Back to Journals » Journal of Pain Research » Volume 19
Ipsilateral Knee Pain After Total Hip Arthroplasty: Pathogenesis and Intervention Strategies—A Narrative Review
Authors Lin X, Wei Z, Wang Z, Yin G, Cheng Q, Li S
Received 22 December 2025
Accepted for publication 2 April 2026
Published 7 April 2026 Volume 2026:19 590938
DOI https://doi.org/10.2147/JPR.S590938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Xu Lin,1 ZhiLin Wei,1 ZhenYan Wang,1 GuanChen Yin,1 QiSheng Cheng,2 ShuQiang Li1
1Department of Bone and Joint Surgery, First Hospital of Jilin University, Changchun City, Jilin Province, 130021, People’s Republic of China; 2Department of Bone and Joint Surgery, Yantai Sino-French Friendship Hospital, Yantai City, Shandong Province, 264123, People’s Republic of China
Correspondence: ShuQiang Li, Department of Bone and Joint Surgery, First Hospital of Jilin University, No. 1 Xinmin Street, Chaoyang District, Changchun City, Jilin Province, People’s Republic of China, Tel +8618643066177, Email [email protected]
Background: Total hip arthroplasty (THA) is the optimal surgical procedure for treating end-stage hip diseases. However, ipsilateral knee pain after THA, as a relatively insidious and not yet fully recognized complication, affects patient satisfaction and functional recovery. Its etiology is complex, involving the interaction of mechanisms such as biomechanics, neurobiology, surgical technique, and patient population and individual factors, which requires systematic review to guide clinical intervention.
Objective: This review aims to systematically elaborate on the pathogenesis of ipsilateral knee pain after THA and, based on this, propose corresponding intervention strategies.
Methods: A narrative literature review was conducted using the PubMed and Scopus databases, an in-depth analysis was conducted from the following aspects: (1) Based on the pathological basis of developmental dysplasia of the hip (DDH), explore the impact of lower limb biomechanical changes after THA on the ipsilateral knee; (2) Analyze the role of neurobiological mechanisms such as referred pain and central sensitization in this complication; (3) Evaluate the influence of surgery-related factors and patient individual and population factors on this complication; (4) Diagnose this complication based on relevant pain score questionnaires, EOS system, predictive simulation, and other imaging and assessment tools; (5) Integrate management approaches from preoperative intervention to postoperative multimodal analgesia.
Results: Available evidence suggests that ipsilateral knee pain after THA is a multifactorial condition. A key modifiable surgical risk factor identified is excessive limb lengthening (≥ 17mm), which disrupts native knee biomechanics. The pathogenesis further involves neurobiological mechanisms such as referred pain and central sensitization, surgical technical factors, and patient-related factors.
Conclusion: Ipsilateral knee pain after THA arises from a complex interplay of biomechanical, neurobiological, and patient-specific mechanisms. To mitigate this complication, a comprehensive management strategy is recommended, encompassing precise preoperative planning, targeted prehabilitation for high-risk patients, and postoperative multimodal analgesia. Future research should focus on validating specific preventive protocols and management algorithms.
Keywords: total Hip arthroplasty, knee pain, biomechanical phenomena, postoperative complications
Introduction
Total hip arthroplasty (THA) is a highly prevalent procedure for end-stage hip diseases. A key surgical decision involves the choice of implant fixation—cemented, cementless, or hybrid—with registry data indicating a predominant trend towards cementless fixation in contemporary practice (eg., accounting for over 56% of cases with an increasing annual share).1 THA is used to treat end-stage hip diseases, including primary osteoarthritis, osteonecrosis of the femoral head, and secondary causes such as developmental dysplasia of the hip (DDH), and can significantly relieve pain and restore joint function.2 With the popularization and refinement of surgical techniques, patient satisfaction following THA has been widely recognized. However, the management of postoperative complications remains key to affecting surgical outcomes and patient satisfaction. Among the many complications after THA, ipsilateral knee pain, as a relatively insidious yet non-negligible issue, is gradually attracting clinicians’ attention.3,4 Reported incidence rates vary, but studies suggest it affects a subset of patients, with one series reporting an incidence of approximately 7.3%.3 Although THA aims to address the hip lesion and reduce hip pain and functional impairment, the postoperative changes in lower limb biomechanics may lead to symptoms in the ipsilateral knee. Consequently, despite improved hip function, some patients experience knee pain, affecting the surgical outcome and satisfaction.5,6 Importantly, postoperative knee pain may be transient in many patients and often resolves within several months, whereas persistent pain may indicate more complex biomechanical or neurobiological mechanisms.
The pathological mechanism of ipsilateral knee pain after THA is not caused by a single factor but is the result of multiple factors, constituting a typical biopsychosocial medical problem. Firstly, biomechanical changes are the fundamental cause of this complication. For patients with high-dislocation DDH (Crowe III/IV type), to achieve anatomical reduction of the hip joint, intraoperative lengthening of the affected limb is often required.7 THA performed for other reasons, such as femoral head osteonecrosis or femoral neck fracture, may also result in postoperative limb lengthening. Studies have shown that when the limb lengthening amount is ≥17mm, there is a risk of significantly increasing the possibility of anterior knee pain by altering the tibiofemoral rotation angle and patellar tilt angle.3,8 The mechanism may be that the iliotibial band cannot adapt to excessive limb lengthening, leading to increased knee valgus stress and patellofemoral joint subluxation, thereby triggering anterior knee pain.6 Secondly, neuropathic pain mechanisms also play an important role in ipsilateral knee pain after THA. The sensory innervation of the hip and knee joints partially overlaps (eg., the femoral nerve and obturator nerve), which allows for hip-originated pain to be referred to the knee.9 Furthermore, the surgical trauma from THA can induce peripheral and central sensitization, particularly in patients with pre-existing chronic pain or a tendency towards central sensitization (such as fibromyalgia features), who have a higher risk of developing chronic pain and multi-site pain postoperatively.10,11 Details of the surgical technique and prosthesis selection and positioning are also very important. The choice of surgical approach (eg., anterior versus posterolateral approach) and the placement of the prosthesis directly affect the postoperative lower limb alignment and soft tissue tension, subsequently acting on the knee joint and potentially causing pain.12–14 Finally, patient-related factors, divided into individual and population factors, such as age, obesity, diabetes, psychological and emotional state (anxiety, depression, catastrophizing), and socioeconomic factors, can modulate an individual’s susceptibility to pain and postoperative satisfaction.15–17
Currently, significant gaps remain in the research on ipsilateral knee pain after THA. Many studies focus on independent mechanisms, and many mechanisms have not been clearly elucidated; furthermore, there is a lack of discussion on the interactions between the various mechanisms. In terms of clinical intervention, although multimodal analgesic strategies have been increasingly adopted in clinical practice, pain potentially caused by different mechanisms has not been adequately addressed. Future prospective cohort studies and mechanistic investigations are needed to clarify the interactions among biomechanical, neurobiological, and patient-related factors contributing to ipsilateral knee pain after THA.18
Therefore, this review aims to systematically synthesize and integrate the current understanding of the pathogenesis of ipsilateral knee pain after THA. Recognizing the multifactorial nature of this condition, we will provide an integrative (rather than exhaustive) analysis of key contributing perspectives, including post-THA biomechanical changes, neurobiological mechanisms, surgical technical factors, and patient-related factors. To better understand the interplay of these diverse mechanisms, a conceptual model integrating the key factors is presented in Figure 1.Based on this, we will further explore feasible intervention strategies for this complication, including perioperative prehabilitation, optimization of surgical techniques, and postoperative pain management, with the goal of providing guidance for clinical practice, pointing out future research directions, and ultimately improving patients’ overall prognosis and enhancing their surgical satisfaction.
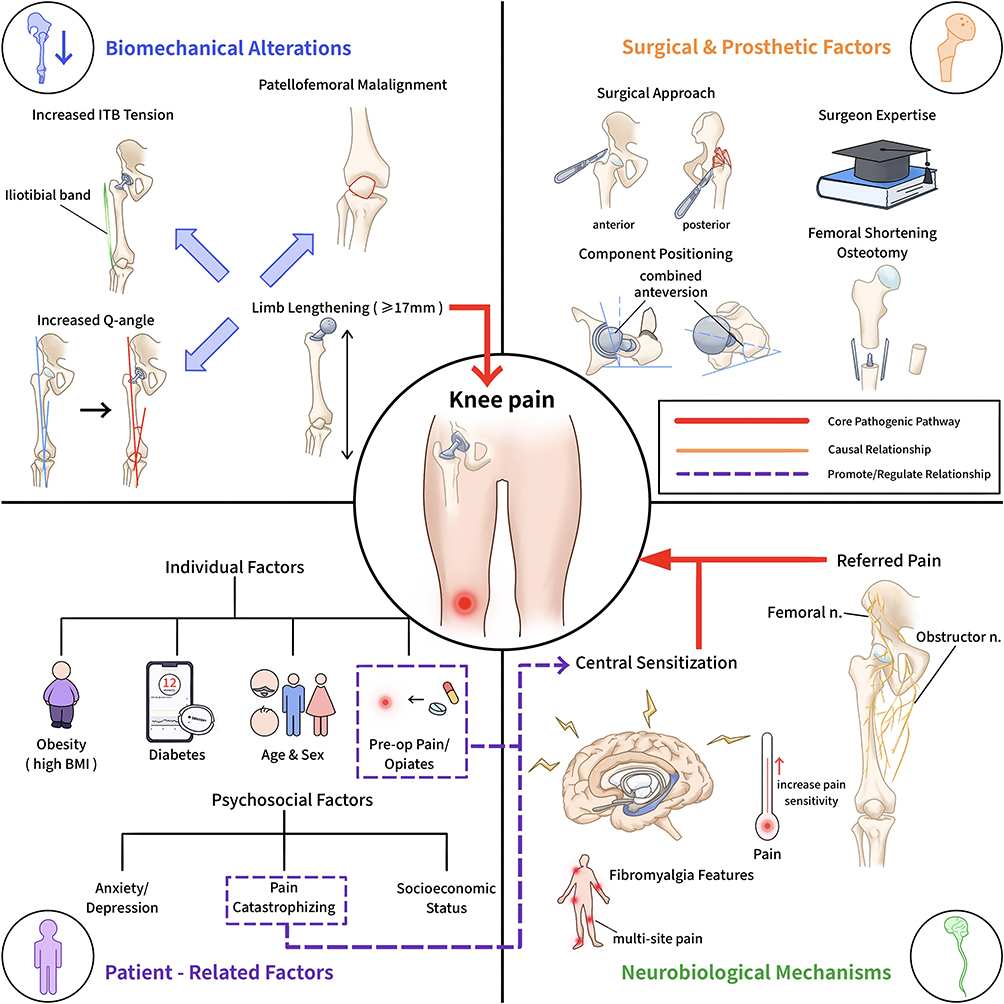 |
Figure 1 Multifactorial pathogenesis and interactions of ipsilateral knee pain following total Hip arthroplasty. |
Methods
This narrative review aimed to provide an overview of the current evidence regarding the mechanisms and management strategies of ipsilateral knee pain following total hip arthroplasty (THA).
Literature Search
A literature search was performed using two major electronic databases, PubMed and Scopus, covering publications from database inception to December 2025. The search strategy combined keywords and controlled vocabulary terms (including Medical Subject Headings in PubMed) related to three core concepts: (1) total hip arthroplasty, (2) knee pain, and (3) the postoperative period. Additional relevant articles were identified through manual screening of reference lists from selected publications.
Study Selection
The initial search identified approximately 800 records. After removing duplicate entries, titles and abstracts were screened to identify studies discussing knee pain in the context of THA. Articles considered potentially relevant were retrieved for full-text evaluation. During this process, particular attention was given to studies investigating biomechanical changes, neurobiological mechanisms, surgical technical factors, and patient-related determinants associated with ipsilateral knee pain after THA.
Eligibility Criteria
Clinical studies (including randomized controlled trials, cohort studies, case–control studies, and case series), as well as systematic reviews and narrative reviews, were considered eligible if they addressed the etiology, diagnosis, or management of knee pain on the side ipsilateral to THA. Articles focusing primarily on intrinsic knee pathology unrelated to THA (eg., primary knee osteoarthritis or traumatic ligament injuries) or pain following unrelated surgical procedures were excluded. Only articles published in English were included.
Given the narrative nature of this review, studies were selected primarily based on their relevance to the topic and their contribution to understanding the mechanisms and clinical management of ipsilateral knee pain following THA. When multiple studies addressed similar topics, preference was given to more recent publications or those with stronger methodological design.
Data Synthesis
The included studies were analyzed using a narrative synthesis approach. Because of heterogeneity in study design, patient populations, outcome measures, and research objectives, a quantitative meta-analysis was not considered appropriate. Instead, findings were summarized and integrated into a thematic framework focusing on four main domains: biomechanical factors, neurobiological mechanisms, surgical technical factors, and patient-related influences. These thematic domains formed the basis for discussing the pathogenesis of ipsilateral knee pain after THA and potential strategies for clinical management.
Related Pathological Mechanisms and Biomechanical Changes
Pathological Basis of the Knee Joint in Developmental Dysplasia of the Hip
Untreated developmental dysplasia of the hip (DDH) in adulthood often leads to progressive anatomical and biomechanical changes.19 Such patients typically suffer from decreased mobility and pain due to issues like joint contractures, limb length discrepancy, and abductor muscle weakness.7 In the Crowe classification used to assess DDH severity, the pathological manifestations of a Crowe type IV hip are diverse, ranging from high dislocation to asymptomatic adult acetabular dysplasia.20 The dysplastic acetabulum is filled with fibrous tissue and fat, and the femoral canal is straight and narrow, accompanied by excessive anteversion.21 Epidemiological data show that 50–70% of DDH patients ultimately develop moderate to severe hip osteoarthritis, most of whom require THA.22 The morphological evolution from Crowe type I to type IV clearly demonstrates a series of progressive changes, including superior migration of the femoral head, the femoral canal becoming straighter, narrower, and excessively anteverted, capsular thickening, and abductor muscle shortening.2 More critically, the impact of DDH extends far beyond the hip joint and is closely related to morphological changes in the knee joint, manifesting as smaller and asymmetric femoral condyles, a shallower trochlea, decreased lateral shift of the patella, an increased patellar tilt angle, and typically valgus lower limb alignment.23 The natural course of the disease can sometimes lead to developmental changes in the knee’s bony anatomy, subsequently causing lower limb valgus deformity and secondary tibiofemoral arthritis.6 The relatively abnormal anatomy of the lower limb in DDH patients provides some guidance for explaining the occurrence of ipsilateral knee pain after THA.
Biomechanical Changes in the Lower Limb After THA
Alterations in the overall biomechanics of the lower limb after THA are a core mechanism of ipsilateral knee pain. Changes in tibiofemoral rotation and patellar tilt post-THA have garnered attention, with some studies reporting external rotation of the tibia after THA;8 furthermore, another study found that the degree of limb lengthening after THA is proportional to the increase in patellar tilt angle and the magnitude of external rotation of the patella relative to the femur.3 Based on this, some research hypothesizes that increased limb lengthening leads to a larger tibiofemoral rotation angle (TFRA),24 which in turn increases the patellar tilt angle (PTA) and worsens postoperative hip function scores (mHHS). The underlying mechanism may be that while muscle tissue can adapt to limb lengthening postoperatively, the iliotibial band (ITB), as a strong tendinous structure, cannot undergo corresponding adaptive changes. Because the ITB inserts on the lateral aspect of the knee, its excessive tension forces the knee into a valgus deformity, leading to abnormal stress on the medial collateral ligament and pain,6 Specifically, a limb lengthening amount of ≥17mm has been identified as a risk factor for provoking anterior knee pain.11
The aforementioned biomechanical changes clinically manifest directly as abnormal knee alignment and pain. Although recent clinical reports on THA for Crowe type IV hips show excellent hip outcomes, corresponding complications still exist, including limited flexion, limping, knee valgus, knee pain, etc.25 Therefore, complications such as periprosthetic fracture, infection, polyethylene liner wear, dislocation, limited range of motion, abnormal gait, knee valgus, knee pain, thigh pain, and hip noise are issues that need to be faced after THA.2 Ipsilateral knee pain after THA, as one of the relatively insidious complications, is gradually being recognized and taken seriously by clinicians.
Clinical observations have found that in some Crowe type III and IV hips, after reducing the hip rotation center to the anatomical position, even the ipsilateral knee that was normal preoperatively exhibits adaptive changes and painful valgus deformity, and this phenomenon still occurs even when femoral shortening is performed.6 This situation is directly related to postoperative limb lengthening. Data analysis shows a significant correlation between the amount of limb lengthening and an increase in the quadriceps Q-angle after THA.26 However, there is no significant correlation between femoral resection length and the postoperative Q-angle, suggesting that knee issues are not directly related to femoral shortening but are indirectly related to the final limb length.6 Excluding knees with pre-existing pathological Q-angle enlargement or valgus deformity makes the results more compelling; one study showed that all knees in their cases were normal preoperatively and demonstrated valgus deformity postoperatively,6 This valgus deformity tends to cause patellofemoral joint subluxation, leading to ipsilateral knee pain. Another important finding is that the postoperative increase in Q-angle is inversely correlated with the Lysholm-Gillquist score used for clinical functional assessment of the knee, meaning that as the Q-angle increases, the knee score decreases,6 which indirectly confirms an association between Q-angle changes and ipsilateral knee pain after THA.
Despite statistically significant improvement in the postoperative Harris Hip Score, the condition of the patient’s knee worsened compared to preoperatively.6 Although the acceptable amount of limb lengthening did not negatively affect the postoperative hip score, it had a negative effect on the ipsilateral knee.6 The above data results explain the clinical phenomenon of observing ipsilateral knee valgus deformity accompanied by medial collateral ligament tenderness, ITB sensitivity, and a sensation of pulling early after THA, and these clinical manifestations are more severe in patients with significant limb lengthening.6
Nevertheless, the overall impact of THA on the coronal and axial plane alignment of the ipsilateral knee in DDH has not been fully elucidated.4 For example, Kocabiyik et al evaluated 25 THAs with femoral osteotomy for Crowe type IV DDH and found that THA neutralized the coronal plane alignment of the knee, femoral parameters changed significantly, but the changes in the hip-knee-ankle angle and mechanical axis were very small.5 Tokuhara et al studied the effects of THA on the ipsilateral patellofemoral joint in 252 DDH patients and found that the incidence of anterior knee pain was approximately 7.3%, and this pain mostly decreased or disappeared within one year; lateral patellar tilt was significantly correlated with limb lengthening and was markedly increased in painful knees, but the association between patellar tilt and anterior knee pain was no longer significant after 3 months.3 The direct biomechanical consequences of achieving anatomical reduction in Crowe IV DDH, particularly limb lengthening, on the ipsilateral knee are depicted in Figure 2.
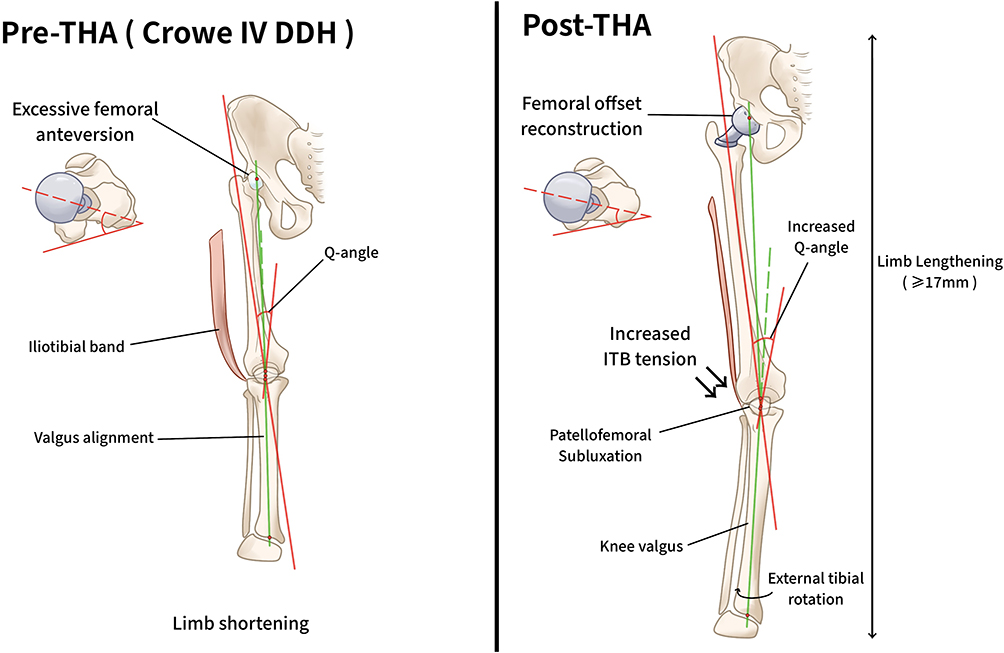 |
Figure 2 Alterations in lower limb biomechanics following total Hip arthroplasty for developmental dysplasia of the hip (DDH). |
Overall, these early findings suggest the importance of in-depth study of such complications, but relevant data remain insufficient, and research is not yet thorough enough.4 Therefore, ipsilateral anterior knee pain and medial collateral ligament tenderness after THA are related to patellofemoral joint abnormalities caused by limb lengthening. This suggests that surgeons performing THA should try to avoid excessive limb lengthening, preferably keeping it to no more than 17mm.
However, in certain complex cases—particularly in patients with high-dislocation developmental dysplasia of the hip—complete restoration of limb length may not always be feasible without introducing excessive soft tissue tension or biomechanical alterations. In such situations, preoperative planning should aim to balance the correction of limb length discrepancy with the risk of secondary complications, including ipsilateral knee pain. Some studies suggest that moderate residual limb length discrepancy may be preferable to excessive limb lengthening, which can increase soft tissue tension and alter knee biomechanics.6,27 Therefore, careful preoperative templating, intraoperative assessment of soft tissue balance, and individualized surgical decision-making are essential to minimize the risk of postoperative knee symptoms.
Referred Pain and Central Sensitization Mechanisms
Referred Pain Mechanism
The pain presentation caused by hip joint pathology possesses a certain complexity. Although this pain is often localized to the hip, it can also be referred to the buttock, thigh, knee, and even the lower leg.28 The prevalence of hip-originated knee pain is reported to be between 2% and 29%.9 Knee pain originating from hip pathology is well-described in pediatric literature, often associated with slipped capital femoral epiphysis or Legg-Calvé-Perthes disease; however, research literature on this symptomatic presentation in adults is very scarce, found only in a small number of small case series.29
Generally, pain caused by hip joint pathology is often felt in the groin area, lumbosacral region, or anterior thigh, while ipsilateral knee pain (especially anterior knee pain) is also a recognized component of hip pain.30 Specific neural pathways underlie the phenomenon of referred pain. Referred pain to the thigh and knee originating from hip joint pathology arises from the sensory distribution of the femoral nerve, obturator nerve, and sciatic nerve.31 The peripatellar soft tissues of the knee joint are in close contact with the patellofemoral joint and are richly innervated.32 It is noteworthy that the presence and distribution of substance-P nerve fibers in the infrapatellar fat pad suggest a nociceptive function in anterior knee pain; Witonski et al found a large number of such fibers in the infrapatellar fat pad of patients with anterior knee pain.33 The imbalance in the state of the balance between sensory and sympathetic nerve fiber densities has certain implications for understanding ipsilateral knee pain after THA. In highly inflammatory diseases such as rheumatoid arthritis, the ratio of sensory substance-P nerve fibers to sympathetic nerve fibers is approximately 8:1, whereas in healthy tissue, the density of sensory and sympathetic nerves is balanced at 1:1.34 Ipsilateral anterior knee pain after THA may be related to referred pain. It is plausible that in patients with long-standing hip pathologies such as DDH or ONFH, chronic alterations in gait and knee biomechanics might create a peripheral sensitization state in the knee. Surgical manipulation during THA may contribute to ipsilateral knee pain through stimulation of shared neural pathways; however, the precise contribution of referred pain to postoperative knee symptoms remains uncertain. Future clinical studies integrating imaging findings and pain phenotyping may help clarify the role of referred pain in this complication.We hypothesize that the surgical trauma and consequent inflammatory milieu of THA may sensitize these pre-existing or newly stimulated substance-P positive nociceptive pathways, potentially lowering the threshold for pain referral from the hip to the knee and contributing to the clinical presentation of ipsilateral knee pain postoperatively.
Central Sensitization Mechanism
Building on the aforementioned referred pain and peripheral nerve mechanisms, the persistence and chronicity of pain often involve changes in the central nervous system. Taking fibromyalgia as an example, as the most “systemic” pain disorder, it is characterized by widespread somatic pain and comorbid somatic symptoms (such as fatigue, poor sleep, depression, and memory difficulties), all of which are considered to originate from the central nervous system.35 Research has identified abnormal central nervous system processing and modulation of pain, as well as comorbid symptoms, in various chronic pain states.36 Indeed, sensitization has multiple clinical manifestations, such as diffuse pain symptoms, sleep disturbances, hyperalgesia, kinesiophobia, or pain catastrophizing. These symptoms presented in patients with knee or hip osteoarthritis are all central nervous system-derived symptoms associated with nociplastic pain conditions.10
Central pain sensitization involves the amplification of neuronal activity occurring at a systemic level, leading to increased sensitivity to nociceptive input distant from the painful area. It is now clear that some patients with painful osteoarthritis have central pain sensitization.37 Such patients may be at higher risk of experiencing chronic pain after joint arthroplasty, as removing the peripheral pain source may not reverse the enhanced central pain processing alterations.37 Some studies have shown that patients with higher fibromyalgia survey scores consumed significantly more opioids during the acute period after TKA and THA.38 Early studies provide additional support for the hypothesis of poorer outcomes in patients with fibromyalgia features. For example, poorer long-term analgesic outcomes after joint arthroplasty are associated with multi-site pain (one of the hallmarks of fibromyalgia).11 Diffuse hyperalgesia is one of the physiological correlates of fibromyalgia and other conditions where pain is considered to have centralized.35 Some studies have demonstrated that patients with anterior knee pain benefit from electroacupuncture treatment, suggesting that central pain inhibition through afferent stimulation is a reasonable explanation,39 providing indirect evidence for the involvement of central mechanisms in pain modulation. In patients with DDH and osteonecrosis of the femoral head, the long duration of disease and chronic pain exposure may predispose individuals to central sensitization, which could contribute to ipsilateral knee pain after THA. This hypothesis requires further confirmation through prospective clinical studies evaluating central sensitization markers and postoperative pain outcomes.
Surgical Technical Factors and Prosthesis Influence
Surgical Approach
The choice of surgical approach may influence clinical outcomes after THA and can affect postoperative lower limb biomechanics, which may indirectly impact the ipsilateral knee. Different approaches involve varying degrees of soft-tissue disruption and muscle preservation, which may influence postoperative joint stability and gait mechanics, and in turn affect overall lower-limb alignment.Previous clinical studies have compared the anterior and posterolateral approaches in THA. For example, Chen et al reported that the anterior approach combined with proximal femoral osteotomy in patients with septic arthritis showed advantages such as reduced intraoperative blood loss and a lower rate of postoperative dislocation compared with the posterolateral approach.40 However, it should be noted that this study involved a highly specific patient population, which may limit the generalizability of its findings to routine THA practice.
In general THA populations, the direct anterior approach is often considered muscle-sparing and may facilitate early postoperative functional recovery. However, it is technically demanding and may require a longer operative time. In contrast, the posterolateral approach remains one of the most commonly used approaches due to its wide exposure and technical familiarity, although it has historically been associated with a relatively higher risk of postoperative dislocation if soft tissue repair is insufficient.41 Because surgical approach selection can influence soft tissue tension, hip stability, and postoperative limb alignment, these factors may subsequently affect knee joint loading and biomechanics. Therefore, careful surgical planning and appropriate approach selection may contribute to minimizing secondary biomechanical effects on the ipsilateral knee after THA.
Prosthesis Positioning and Planning
Accurate prosthesis positioning and selection are core to ensuring the long-term success of THA and avoiding secondary issues in the ipsilateral knee. To effectively prevent postoperative complications, particularly to avoid adverse effects on the ipsilateral knee due to changes in the hip’s mechanical environment, the combined anteversion of the acetabular cup and femoral stem must be comprehensively considered, while carefully assessing the bony coverage of the cup and the native morphological characteristics of the acetabulum, including its natural anteversion and inclination.42 Adult cadaveric morphometric studies show that the normal physiological range of femoral anteversion is wide, ranging from −15° (retroversion) to 30° (anteversion),43 highlighting the importance of precise preoperative assessment and individualized design.
To overcome the limitations of traditional inverse dynamics analysis in predicting postoperative biomechanical changes, predictive dynamic simulation technology provides a feasible solution. This method is based on the fundamental assumption that “human motion tends towards optimization of energy consumption or mechanical efficiency in a given context,” employing optimal control algorithms to predict postoperative patient movement patterns.13 A major advantage of predictive simulation is the ability to perform “what-if” analyses for various clinical scenarios, such as simulating the impact of different patient conditions (eg., limited joint range of motion, weakened muscle strength, etc.) on movement patterns, thereby providing data support for the optimal placement of implants.44 All these technical means help significantly reconstruct lower limb biomechanical offset and appropriate length,45 thereby reducing the incidence of ipsilateral knee pain after THA.In recent years, emerging surgical technologies have been increasingly introduced to improve the precision of implant positioning in THA. Robotic-assisted THA, computer-assisted navigation systems, and patient-specific instrumentation (PSI) have been developed to enhance the accuracy of component placement, restoration of limb length, and femoral offset. These technologies allow surgeons to perform more precise preoperative planning and intraoperative guidance, thereby reducing variability in component alignment.
Several studies have reported that robotic-assisted THA can improve the accuracy of acetabular cup positioning and better control limb length discrepancy compared with conventional techniques.46 Computer navigation systems provide real-time intraoperative feedback on component orientation and limb length changes, which may help optimize lower limb biomechanics.47 Patient-specific instrumentation, based on preoperative imaging and individualized anatomical modeling, also assists surgeons in achieving more accurate component placement.48 Given that postoperative changes in limb length, femoral offset, and lower limb alignment have been associated with ipsilateral knee pain after THA, the application of these technologies may have potential value in reducing this complication. Although current evidence remains limited and further high-quality studies are needed, these technologies represent an important direction for improving surgical precision and postoperative functional outcomes.
Intraoperative Maneuvers (Eg., Adductor Tenotomy)
Beyond the choice of approach and implant planning, the specific technical maneuvers performed during THA are critical determinants of postoperative biomechanics and complication risks. Surgical proficiency plays a key role in executing these maneuvers to optimize outcomes and minimize adverse effects on adjacent joints, such as the knee. Understanding the mechanisms of surgery-related complications is crucial for preventing and managing the complication of ipsilateral knee pain after THA. Lower limb alignment after THA changes dynamically over time. Some studies have shown that hip internal rotation and lateral patellar tilt continue to change for up to two years post-THA, with an average change of about 2°, but inter-individual variation is very large.49 Further analysis revealed that adductor tenotomy was significantly associated with increased hip internal rotation over time; whereas the amount of limb lengthening and a larger preoperative tibiofemoral angle were associated with a decrease in lateral patellar tilt over time.49 These findings suggest that certain potential intraoperative surgical maneuvers (such as adductor release) influence the postoperative biomechanical environment of the ipsilateral knee, potentially leading to the occurrence of anterior knee pain by altering patellofemoral joint stress distribution and lower limb rotational alignment. Therefore, adductor tenotomy—a specific intraoperative maneuver—may inadvertently alter patellofemoral mechanics, representing a modifiable surgical factor that could contribute to the development of ipsilateral anterior knee pain after THA.
Patient-Related Risk Factors
Preoperative Pain Status of the Patient
The patient’s preoperative pain experience is an important predictor of ipsilateral knee pain after THA. Multi-site pain, one of the core diagnostic criteria for fibromyalgia, is closely associated with poorer long-term analgesic outcomes in joint arthroplasty patients. This essentially reflects a sensitized state of pain processing within the central nervous system. This central sensitization phenomenon has been proven in multiple chronic pain studies to be an important biological marker for predicting postoperative pain outcomes.11 Analyzing from a clinical pathophysiological perspective, we can recognize that the functional severity of the joint lesion directly determines the intensity and temporal dimension of peripheral nociceptive stimulation, which to some extent exacerbates central sensitization. Furthermore, comorbid pain in other parts of the body often indicates abnormal widespread pain processing mechanisms. The interaction of these two preoperative pain states leads to a significantly increased incidence of persistent postoperative pain50 and is closely related to the complication of ipsilateral knee pain after THA.
Regarding medication history, preoperative opioid use has been confirmed as a risk factor predicting poor chronic pain outcomes postoperatively, which may be related to mechanisms such as opioid-induced hyperalgesia and drug tolerance.51 The research by Yang et al further expanded this understanding, finding that the use of any type of preoperative analgesic (not limited to opioids) was associated with an increased risk of chronic postoperative pain, suggesting that preoperative opioid analgesic intervention may have a potential impact on ipsilateral knee pain after THA.14 The aforementioned studies indicate that patients with long-term pain and those on preoperative opioid analgesia are more likely to experience ipsilateral knee pain after THA due to central sensitization mechanisms and potential opioid-induced hyperalgesia and tolerance mechanisms. This suggests that surgeons should anticipate this complication based on the patient’s behavioral state during patient management and provide timely intervention postoperatively. In clinical practice, patients with suspected central sensitization or neuropathic pain components may benefit from targeted preoperative screening. Validated tools such as PainDETECT, the Douleur Neuropathique 4 (DN4) questionnaire, or quantitative sensory testing can help identify altered pain processing and guide individualized perioperative pain management strategies.51
Individual and Population Factors
Patients’ metabolic diseases and comorbid status affect postoperative pain outcomes through various pathophysiological pathways. Diabetes mellitus shows a strong association with persistent postoperative pain, the mechanisms of which may be related to peripheral nerve dysfunction caused by the accumulation of advanced glycation end products, oxidative stress damage, and microangiopathy.52 Some studies have shown that linear regression models using individualized metabolic abnormality indicators can predict surgical outcomes more accurately than simply counting the number of risk factors, suggesting the importance of individual metabolic indicators on pain.15 However, most ipsilateral knee pain after THA is not persistent pain (the pain duration is mostly less than 3 months). While diabetes is associated with persistent pain after joint arthroplasty, its mechanism has not been clearly elucidated, and there are no reports linking it to non-persistent postoperative pain. Whether it is relevant to the topic discussed in this review requires future research to investigate.
Psychological and emotional factors play an important role in pain perception and modulation. Negative emotional states such as anxiety and depression affect opioid consumption after THA, and patients with severe negative emotions also experience more pain over time. Mental health is an independent predictor of in-hospital opioid consumption, patient satisfaction at 3 months postoperatively, and treatment effectiveness.53 The mechanisms by which these psychological comorbidities affect joint arthroplasty outcomes involve multiple regulations of the neuroendocrine and even immune networks.54 Individual pain coping strategies have also been proven to be associated with postoperative pain outcomes, suggesting the potential value of cognitive-behavioral intervention.51 Patients with more negative emotions are more likely to feel pain postoperatively and are more likely to have their satisfaction after THA affected. Surgeons should have a general understanding of the patient’s psychological state to be psychologically prepared for the complication of ipsilateral knee pain after THA.
Socioeconomic factors influence patients’ pain experience and healthcare outcomes in multiple ways. Low-income and socially disadvantaged populations are often associated with more severe pain symptoms, highlighting the important role of social determinants in health outcomes.17 In addition, clear social gradient differences exist in healthcare accessibility; individuals from lower socioeconomic groups have fewer opportunities to receive joint arthroplasty procedures, reflecting structural disparities in healthcare resource distribution.17 Regarding treatment outcomes, patients from disadvantaged socioeconomic backgrounds have also been reported to have a higher risk of hospital readmission, suggesting inequalities in postoperative care and follow-up systems.55 Racial disparities in postoperative pain outcomes have also been reported. Some studies have shown that African American patients may have a higher risk of chronic postoperative pain following joint arthroplasty compared with other racial groups.51 However, these differences are likely multifactorial rather than solely attributable to psychosocial factors. Recent studies examining postoperative pain trajectories have suggested that a range of factors—including discharge disposition, access to rehabilitation services, baseline functional status, and perioperative care pathways—may contribute to variations in postoperative recovery and pain outcomes across different populations.56 Furthermore, the availability of social support systems may also affect postoperative pain perception and recovery. A stronger social network can help alleviate perceived pain through emotional support and practical assistance during the recovery process.51 Although employment status has been associated with postoperative pain outcomes in some individual studies, meta-analytic evidence suggests that it may not independently predict pain outcomes after arthroplasty.57 While socioeconomic and demographic factors appear to influence postoperative recovery and patient-reported outcomes, their specific contribution to ipsilateral knee pain after THA remains unclear. Future multicenter cohort studies may help clarify the relative impact of these factors on postoperative knee pain.
Regarding demographic characteristics, several factors show complex associations with postoperative pain outcomes. Firstly, age: although some studies suggest that younger patients may report persistent postoperative pain more easily due to higher functional expectations,58 this association varies significantly across studies, reflecting an interaction between age and research factors (such as occupational demands, psychological expectations, etc).59 Secondly, gender differences are significant in pain biology; female patients exhibit greater sensitivity to acute and chronic pain and poorer analgesic effects, which may be related to the modulation of pain pathways by sex hormones and gender differences in pain coping strategies.60 Obesity, as a global health issue, has multiple negative impacts on joint arthroplasty outcomes. Higher BMI is generally associated with poorer pre- and postoperative scores on various patient-reported outcome measures. The mechanisms involve multiple pathways, including increased biomechanical load, systemic inflammatory state, and adipokine metabolic dysregulation.61 The aforementioned demographic characteristics all have negative effects on satisfaction after THA and are also associated with postoperative pain. However, whether they are relevant to the topic of this review, and if so, to what extent, warrants further research.
Clinical Assessment and Diagnostic Tools
Assessment Tools
Standardized assessment for ipsilateral knee pain after total hip arthroplasty requires the use of validated tools. The pain subscale of the Knee injury and Hip Osteoarthritis Outcome Score is one of the most commonly used scales for assessing pain in patients with osteoarthritis and after joint arthroplasty.62 The Oxford Hip Score, an assessment tool specifically designed for hip replacement patients, systematically quantifies the degree of hip pain and functional limitation on a scale from 0 to 48 (worst to best).63 There are multiple tools for assessing pain, including the Visual Analog Scale for pain (providing a one-dimensional assessment of pain severity), the Brief Pain Inventory (a disease-nonspecific questionnaire containing a pain severity subscale), and the short-form McGill Pain Questionnaire (a disease-nonspecific questionnaire assessing sensory and affective qualities of pain).50 For identifying neuropathic pain, PainDETECT and Douleur Neuropathique 4 (DN4) are commonly used, effective clinical assessment tools,50 Quantitative sensory testing can objectively assess hyperalgesia and central sensitization status. The combined application of these tools enables a comprehensive multi-angle assessment of pain, providing an objective basis for developing individualized treatment plans for ipsilateral knee pain after THA.
Imaging Diagnostic Techniques
Imaging and special diagnostic techniques play a central role in diagnosing the etiology of ipsilateral knee pain after total hip arthroplasty. Ultrasound examination, with its unique advantages of being radiation-free, providing real-time dynamic imaging, and being convenient and low-cost, is particularly suitable for postoperative assessment. It can clearly demonstrate joint effusion, synovial thickening, and changes in periarticular ligaments and tendons.64 Regarding imaging examinations, nuclear medicine studies, such as bone scans, can identify various non-prosthetic causes of pain, including referred pain, fracture, heterotopic ossification, and osteoarthritis progression.16 The EOS two-dimensional and three-dimensional X-ray imaging system holds significant value in assessing biomechanical changes after THA. This technology can simultaneously acquire orthogonal images of both lower limbs under weight-bearing conditions and construct three-dimensional models, intuitively displaying the overall alignment relationship of the spine-pelvis-lower limb chain. Furthermore, this imaging technique is relatively insensitive to metal artifact.65–67 However, a health technology assessment concluded that while EOS provides lower radiation dose and comparable image quality, its high capital cost makes cost-effectiveness highly dependent on very high patient throughput, which may not be achievable in routine practice. Furthermore, evidence on long-term patient health benefits beyond radiation reduction remains limited.68
As traditional imaging techniques (including X-ray and conventional CT) have limitations in fully revealing posture and alignment issues after THA (such as leg length discrepancy, femoral offset, and tibiofemoral rotation, etc),24,69 some research has designed extended CT scanning protocols to compensate for this deficiency. The aim is to with the aim of describe in detail the coronal and axial plane alignment changes of the hip and knee after THA. The hypothesis is that patients undergoing THA will experience significant changes in coronal plane alignment, femoral anteversion, and patellar tracking, and this is planned to be validated through long-term follow-up.4 It is important to acknowledge that such dedicated CT protocols, while offering superior planning accuracy and potentially improving surgical outcomes, are associated with a significantly higher radiation dose (eg., increases of ≥30% or more) compared to conventional radiography. Although the absolute cost of the scan may constitute a small fraction of the total procedure cost, its cost-effectiveness is highly sensitive to equipment utilization rates.70
In summary, the three-dimensional morphological visualization provided by ultrasound, nuclear medicine imaging, EOS, and extended CT assists surgeons in diagnosing ipsilateral knee pain after THA and provides support for precise intervention. The selection of an advanced imaging modality in clinical practice should therefore involve a balanced consideration of its diagnostic yield, against practical constraints including radiation exposure, cost, availability, and the specific clinical question.
Multimodal Intervention Strategies
Preoperative Intervention Strategies
Preemptive intervention before THA plays an important role in reducing ipsilateral knee pain after THA. The core principle is to avoid excessive lengthening of the operated limb through proper preoperative prosthetic measurement and planning, thereby preventing excessive disruption of the lower limb mechanical environment that can lead to knee pain. Preoperative education is an important part of preoperative intervention. Its core elements include: involving the patient and their family together in the planning; ensuring the participation of a team including the surgeon, anesthesiologist, nursing, and physiotherapy teams; informing the patient about the general course of postoperative rehabilitation, including goals and expectations at specific time points; explaining perioperative pain control methods, and setting realistic expectations for postoperative pain levels.71 Simultaneously, individuals at high risk for ipsilateral knee pain after THA (ie., those with the aforementioned potential risk factors, such as patients with high-dislocation DDH, patients suspected of having pre-existing central sensitization, patients with a history of long-term high-dose analgesic use, etc.) should be identified preoperatively. This allows for timely detection and management should this postoperative complication occur. For these identified high-risk patients, implementing targeted prehabilitation is crucial. Such measures may include strengthening exercises for the quadriceps and other peri-articular knee muscles to enhance knee joint stability, thereby helping it withstand altered biomechanics after THA. Concurrently, preoperative pain neuroscience education for high-risk patients is vital to clarify concepts like referred pain and central sensitization. This can reduce maladaptive pain cognitions, such as pain catastrophizing, and alleviate preoperative anxiety. These proactive steps are expected to positively reduce the incidence of this complication.
Postoperative Multimodal Analgesia Regimens
Ipsilateral knee pain after THA is a complication caused by multiple factors, including soft tissue injury around the knee due to postoperative mechanical changes. Referred pain and central sensitization mechanisms may also be involved, alongside other potential risk factors such as the psychosocial factors mentioned above. Addressing the cause accordingly is the best measure for managing ipsilateral knee pain after THA. The concept of multimodal analgesia was first proposed by Wall in 1988 and later promoted by Kehlet and Dahl as “balanced analgesia.” It aims to act on different parts of the pain pathway to reduce postoperative opioid requirements.72 Preemptive analgesia with parecoxib can alleviate acute pain after hip and knee arthroplasty, reduce cumulative opioid consumption, and does not increase the risk of adverse drug events.73 As an injectable COX-2 inhibitor, it reduces central sensitivity and peripheral nociceptor inflammation.73 This makes it a good option when this complication occurs in patients with long-term pain or those on long-term opioid analgesia, although there are no targeted studies proving its efficacy specifically for this condition. Duloxetine, a serotonin and norepinephrine reuptake inhibitor effective for neuropathic pain, significantly reduces VAS scores within 3 months postoperatively.74 Controlled-release opioid formulations can maintain stable blood concentrations, avoiding the fluctuations associated with immediate-release formulations.75 They free patients from the need for as-needed dosing, can improve pain relief, and shorten recovery time.76
Interventional pain management techniques provide important options for patients with inadequate response to medication. Peripheral nerve stimulation targeting branches of the saphenous nerve is a direct, highly selective, and safe technique for treating knee pain.77 Studies show this technique can reduce opioid use and improve quality of life, mood, and sleep.78 Radiofrequency neurolysis of knee nerves has shown preliminary positive effects in reducing pain and improving joint function, representing a promising interventional strategy for treating refractory knee pain.78 Strategies targeting central sensitization primarily aim at the neuropathic pain pathways associated with chronic postoperative pain.78 Recommended medications include tricyclic antidepressants, serotonin and norepinephrine reuptake inhibitors, and gabapentinoids.78 The long-term benefits of multimodal regimens are significant. Non-opioid interventions can reduce opioid-related adverse effects, such as respiratory depression, nausea/vomiting, pruritus, and impaired concentration.79 Individualized pain management, which tailors strategies based on pain mechanisms and psychosocial factors, can improve outcomes in patients with nociplastic pain.80
Conclusion
Ipsilateral knee pain following total hip arthroplasty (THA) is a clinically relevant complication that may impair postoperative functional recovery and patient satisfaction. Current evidence suggests that this condition arises from the interaction of multiple mechanisms rather than a single causative factor. Among these, biomechanical alterations after THA appear to be the most consistently supported contributors, particularly excessive limb lengthening and changes in lower-limb alignment that can alter patellofemoral tracking and knee joint loading. Neurobiological mechanisms such as referred pain and central sensitization may further amplify pain perception in susceptible individuals, while surgical factors and patient-related characteristics may modulate the overall risk.
From a clinical perspective, prevention and management of ipsilateral knee pain after THA should focus on strategies that address these mechanisms. Restoration of appropriate lower-limb biomechanics remains a central goal, emphasizing careful preoperative planning, accurate component positioning, and avoidance of excessive limb lengthening during surgery. Identification of patients with potential vulnerability to persistent postoperative pain—such as those with preexisting chronic pain, high analgesic consumption, or psychosocial risk factors—may allow earlier implementation of targeted perioperative pain management strategies.
Management should also follow a multimodal and mechanism-oriented approach. Pharmacologic treatments targeting inflammatory and neuropathic pathways, combined with rehabilitation strategies aimed at restoring muscle strength and joint stability, may improve postoperative outcomes. In patients with refractory symptoms, interventional pain management techniques may also represent potential treatment options.
Future research should move beyond descriptive studies toward more rigorous investigation of this complication. Prospective cohort studies are needed to better characterize the natural history and risk factors of ipsilateral knee pain after THA. Comparative clinical studies examining surgical techniques and technologies that influence limb length restoration and component positioning may clarify modifiable surgical determinants. In addition, validation of predictive models integrating biomechanical, neurobiological, and patient-related factors may help identify high-risk patients and guide personalized perioperative management strategies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moldovan F, Moldovan L. Fixation methods in primary hip arthroplasty: a nationwide, registry-based observational study in Romania (2001–2024). Healthcare. 2025;13(19):2452. doi:10.3390/healthcare13192452
2. Kawai T, Tanaka C, Kanoe H. Total hip arthroplasty for Crowe IV hip without subtrochanteric shortening osteotomy -a long term follow up study. BMC Musculoskelet Disord. 2014;15:72. (in English). doi:10.1186/1471-2474-15-72
3. Tokuhara Y, Kadoya Y, Kim M, Shoundou M, Kanno T, Masuda T. Anterior knee pain after total hip arthroplasty in developmental dysplasia. J Arthroplasty. 2011;26(6):955–16. (in English). doi:10.1016/j.arth.2010.07.007
4. Lucchini S, Castagnini F, Perdisa F, Filardo G, Pardo F, Traina F. Total hip arthroplasty for low-grade developmental hip dysplasia changes the ipsilateral knee alignment on the axial and coronal planes. J Clin Med. 2023;12(23):7347. (in English). doi:10.3390/jcm12237347
5. Kocabiyik A, Misir A, Kizkapan TB, et al. Changes in hip, knee, and ankle coronal alignments after total hip arthroplasty with transverse femoral shortening osteotomy for unilateral Crowe Type IV developmental dysplasia of the hip. J Arthroplasty. 2017;32(11):3449–3456. doi:10.1016/j.arth.2017.05.044
6. Kilicarslan K, Yalcin N, Cicek H, Cila E, Yildirim H. What happens at the adjacent knee joint after total hip arthroplasty of Crowe type III and IV dysplastic hips? J Arthroplasty. 2012;27(2):266–270. (in English). doi:10.1016/j.arth.2011.04.014
7. Satılmış AB, Cengiz T, Ülker A, Mutlu T. The impact of femoral anteversion correction on clinical outcomes in total hip arthroplasty for adult developmental dysplasia of the hip. J Clin Med. 2025;14(9):3207. (in English). doi:10.3390/jcm14093207
8. Yu DG, Zhang J-W, Xu C, et al. Changes in alignment of ipsilateral knee on computed tomography after total hip arthroplasty for developmental dysplasia of the hip. Orthop Surg. 2019;11(3):397–404. doi:10.1111/os.12462
9. Sakamoto J, Morimoto Y, Ishii S, et al. Investigation and macroscopic anatomical study of referred pain in patients with Hip disease. J Phys Ther Sci. 2014;26(2):203–208. doi:10.1589/jpts.26.203
10. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. The Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
11. Hawker GA, Badley EM, Borkhoff CM, et al. Which patients are most likely to benefit from total joint arthroplasty? Arthritis Rheum. 2013;65(5):1243–1252. doi:10.1002/art.37901
12. Mahure SA, Feng JE, Schwarzkopf RM, Long WJ. The impact of arthroplasty fellowship training on total joint arthroplasty: comparison of peri-operative metrics between fellowship-trained surgeons and non-fellowship-trained surgeons. J Arthroplasty. 2020;35(10):2820–2824. (in English). doi:10.1016/j.arth.2020.05.027
13. Febrer-Nafría M, Nasr A, Ezati M, Brown P, Font-Llagunes JM, McPhee J. Predictive multibody dynamic simulation of human neuromusculoskeletal systems: a review. Multibody Syst Dyn. 2022;1–41.
14. Yang MMH, Hartley RL, Leung AA, et al. Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis. BMJ Open. 2019;9(4):
15. Gandhi R, Razak F, Davey JR, Mahomed NN. Metabolic syndrome and the functional outcomes of Hip and knee arthroplasty. J Rheumatol. 2010;37(9):1917–1922. (in English). doi:10.3899/jrheum.091242
16. Carrilho Vaz S, Ferreira TC, Salgado L, Paycha F. Bone scan usefulness in patients with painful Hip or knee prosthesis: 10 situations that can cause pain, other than loosening and infection. Eur J Orthop Surg Traumatol. 2017;27(2):147–156. doi:10.1007/s00590-016-1884-6
17. Wetterholm M, Turkiewicz A, Stigmar K, Hubertsson J, Englund M. The rate of joint replacement in osteoarthritis depends on the patient’s socioeconomic status: a cohort study of 71,380 patients. Acta Orthopaedica. 2016;87(3):245–251. doi:10.3109/17453674.2016.1161451
18. Keene DJ, Knight R, Bruce J, et al. Chronic pain with neuropathic characteristics after surgery for major trauma to the lower limb: prevalence, predictors, and association with pain severity, disability, and quality of life in the UK WHiST trial. Bone Joint J. 2021;103 B(6):1047–1054. doi:10.1302/0301-620X.103B.BJJ-2020-2204.R1
19. Olesen TH, Torfing T, Overgaard S. MPR realignment increases accuracy when measuring femoral neck anteversion angle. Skeletal Radiol. 2013;42(8):1119–1125. (in English). doi:10.1007/s00256-013-1639-y
20. Sugano N, Noble PC, Kamaric E, Salama JK, Ochi T, Tullos HS. The morphology of the femur in developmental dysplasia of the Hip. J Bone Joint Surg Br. 1998;80(4):711–719. (in English). doi:10.1302/0301-620x.80b4.8319
21. Jia CQ, Wu YJ. Factors associated with complications in 176 Crowe IV hips treated with total hip arthroplasty. Orthop Surg. 2025;17(8):2397–2404. (in English). doi:10.1111/os.70120
22. Papachristou G, Hatzigrigoris P, Panousis K, et al. Total hip arthroplasty for developmental hip dysplasia. Int Orthop. 2006;30(1):21–25. (in English). doi:10.1007/s00264-005-0027-1
23. Imai N, Miyasaka D, Hirano Y, Suzuki H, Tsuchiya K, Endo N. Tibiofemoral rotation is related to differences in the lateral femoral condyle configuration in both normal subjects and women with hip dysplasia: a three-dimensional analysis. BMC Musculoskelet Disord. 2019;20(1):353. (in English). doi:10.1186/s12891-019-2737-3
24. Imai NA-O, Hirano Y, Homma D, Komuta Y, Horigome Y, Kawashima H. Relationship among global femoral offset, leg lengthening, and tibiofemoral rotation after total hip arthroplasty. J Clin Med. 2025;14(9):2893. (in English). doi:10.3390/jcm14092893
25. Liu B, Liu S-K, Wu T, et al. Risk factors for intraoperative periprosthetic femoral fractures in patients with hip dysplasia undergoing total hip arthroplasty with uncemented prostheses. Orthop Surg. 2021;13(6):1870–1881. doi:10.1111/os.13133
26. Krych AJ, Howard JL, Trousdale RT, Cabanela ME, Berry DJ. Total Hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-IV developmental dysplasia. J Bone Joint Surg. 2009;91(9):2213–2221. doi:10.2106/JBJS.H.01024
27. Whitehouse MR, Stefanovich-Lawbuary NS, Brunton LR, Blom AW. The impact of leg length discrepancy on patient satisfaction and functional outcome following total hip arthroplasty. J Arthroplasty. 2013;28(8):1408–1414. (in English). doi:10.1016/j.arth.2012.12.009
28. Nakamura J, Oinuma K, Ohtori S, et al. Distribution of hip pain in osteoarthritis patients secondary to developmental dysplasia of the hip. Modern Rheumatol. 2013;23(1):119–124. doi:10.1007/s10165-012-0638-5
29. Atanda A, Shah SA, O’Brien K. Osteochondrosis: common causes of pain in growing bones. Am Family Phys. 2011;83(3):285–291.
30. Khan AM, McLoughlin E, Giannakas K, Hutchinson C, Andrew JG. Hip osteoarthritis: where is the pain? Ann Royal Coll Surg Engl. 2004;86(2):119–121. doi:10.1308/003588404322827518
31. Hodges DL, McGuire TJ, Kumar VN. Diagnosis of hip pain, an anatomic approach. Orthop Rev. 1987;16(2):109–113. (in English).
32. Wojtys EM, Beaman DN, Glover RA, Janda D. Innervation of the human knee joint by substance-P fibers. Arthroscopy. 1990;6(4):254–263. doi:10.1016/0749-8063(90)90054-H
33. Witoński D, Wagrowska-Danielewicz M. Distribution of substance-P nerve fibers in the knee joint in patients with anterior knee pain syndrome. A preliminary report. Knee Surg Sports Traumatol Arthrosc. 1999;7(3):177–183. doi:10.1007/s001670050144
34. Lehner B, Koeck FX, Capellino S, Schubert TE, Hofbauer R, Straub RH. Preponderance of sensory versus sympathetic nerve fibers and increased cellularity in the infrapatellar fat pad in anterior knee pain patients after primary arthroplasty. J Orthop Res. 2008;26(3):342–350. (in English). doi:10.1002/jor.20498
35. Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. doi:10.1001/jama.2014.3266
36. Brummett CM, Clauw DJ. Fibromyalgia: a primer for the anesthesia community. Curr Opin Anaesthesiol. 2011;24(5):532–539. (in English). doi:10.1097/ACO.0b013e32834a1091
37. King CD, Sibille KT, Goodin BR, et al. Experimental pain sensitivity differs as a function of clinical pain severity in symptomatic knee osteoarthritis. Osteoarthritis Cartilage. 2013;21(9):1243–1252. doi:10.1016/j.joca.2013.05.015
38. Brummett CM, Janda AM, Schueller CM, et al. Survey criteria for fibromyalgia independently predict increased postoperative opioid consumption after lower-extremity joint arthroplasty: a prospective, observational cohort study. Anesthesiology. 2013;119(6):1434–1443. doi:10.1097/ALN.0b013e3182a8eb1f
39. Näslund J, Näslund UB, Odenbring S, Lundeberg T. Sensory stimulation (acupuncture) for the treatment of idiopathic anterior knee pain. J Rehabil Med. 2002;34(5):231–238. doi:10.1080/165019702760279233
40. Chen M, Li G, Luo Z, Zhang X, Shang X. Comparison of clinical efficacy between anterior and posterolateral approaches for total hip arthroplasty combined with proximal femoral reconstruction osteotomy in the treatment of residual high dislocation after pyogenic hip arthritis. Chin J Orthopaedics. 2024;44(16):1077–1084. doi:10.3760/cma.j.cn121113-20231217-00402
41. Lu Z, Chen Q, Lan Y, Xie S, Lin F, Feng E. Subtrochanteric osteotomy in direct anterior approach total hip arthroplasty for Crowe IV dysplasia—surgical technique and literature review. Orthop Surg. 2024;16(3):766–774. doi:10.1111/os.13996
42. Dorr LD, Malik A, Dastane M, Wan Z. Combined anteversion technique for total hip arthroplasty. Clin Orthopaedics Related Res. 2009;467(1):119–127. doi:10.1007/s11999-008-0598-4
43. Maruyama M, Feinberg JR, Capello WN, D’Antonio JA. Morphologic features of the acetabulum and femur: anteversion angle and implant positioning. Clin Orthopaedics Related Res. 2001;393:52–65. doi:10.1097/00003086-200112000-00006
44. Sreenivasa M, Millard M, Kingma I, van Dieën JH, Mombaur K. Predicting the influence of hip and lumbar flexibility on lifting motions using optimal control. J Biomech. 2018;78:118–125. doi:10.1016/j.jbiomech.2018.07.028
45. Bruzzone M, La Russa M, Garzaro G, et al. Long-term results of cementless anatomic total hip replacement in dysplastic hips. La Chirurgia Degli Organi Di Movimento. 2009;93(3):131–136. doi:10.1007/s12306-009-0040-4
46. Abdel Khalik H, Nadeem SM, Cruickshank M, Chalmers BP, Lanting B, Wood TJ. Robotic-assisted total hip arthroplasty using the direct anterior approach: a systematic review and meta-analysis. J Orthop. 2025. (in English).
47. Xu K, Li YM, Zhang HF, Wang CG, Xu YQ, Li ZJ. Computer navigation in total Hip arthroplasty: a meta-analysis of randomized controlled trials. Int J Surg. 2014;12(5):528–533. (in English). doi:10.1016/j.ijsu.2014.02.014
48. Constantinescu DS, Costello JP, Dalling AD, Wagner JD, Al-Hardan W, Carvajal JA. The efficacy of patient specific instrumentation (PSI) in total hip arthroplasty (THA): a systematic review and meta-analysis. J Orthopaedics. 2022;34:404–413. (in English). doi:10.1016/j.jor.2022.10.001
49. Akiyama K, Nakata K, Kitada M, Yamamura M, Owaki H, Fuji T. Chronological changes in axial alignment of the ipsilateral hip and knee after total hip arthroplasty. J Arthroplasty. 2018;33(2):415–422. (in English). doi:10.1016/j.arth.2017.09.012
50. Ghoshal A, Bhanvadia S, Singh S, Yaeger L, Haroutounian S. Factors associated with persistent postsurgical pain after total knee or Hip joint replacement: a systematic review and meta-analysis. Pain Reports. 2023;8(1):E1052. doi:10.1097/PR9.0000000000001052
51. Fernández-de-Las-Peñas C, Florencio LL, de-la-Llave-Rincón AI, et al. Prognostic factors for postoperative chronic pain after knee or hip replacement in patients with knee or hip osteoarthritis: an umbrella review. J Clin Med. 2023;12(20):6624. (in English). doi:10.3390/jcm12206624
52. Rajamäki TJ, Jämsen E, Puolakka PA, Nevalainen PI, Moilanen T. Diabetes is associated with persistent pain after hip and knee replacement. Acta Orthop. 2015;86(5):586–593. (in English). doi:10.3109/17453674.2015.1044389
53. Solomito MJ, Witmer DK, Lucchio P, Kostyun RO. Utility of the patient-reported outcomes measurement information system global mental health T-score to identify patients at risk for poor postsurgical outcomes following total hip arthroplasty. J Arthroplasty. 2025;40(4):929–934. doi:10.1016/j.arth.2024.09.041
54. Galea VP, Rojanasopondist P, Ingelsrud LH, et al. Longitudinal changes in patient-reported outcome measures following total Hip arthroplasty and predictors of deterioration during follow-up: a seven-year prospective international multicentre study. Bone Joint J. 2019;101-b(7):768–778. (in English). doi:10.1302/0301-620x.101b7.Bjj-2018-1491.R1
55. Alvarez PM, McKeon JF, Spitzer AI, et al. Socioeconomic factors affecting outcomes in total knee and hip arthroplasty: a systematic review on healthcare disparities. Arthroplasty Rev. 2022;4(1):
56. Omran KA-O, Waren D, Schwarzkopf R. Postoperative pain trajectories in total Hip arthroplasty. Bone Joint Open. 2024;5(3):174–183. (in English). doi:10.1302/2633-1462.53.BJO-2023-0181.R1
57. Podmore B, Hutchings A, Van Der Meulen J, Aggarwal A, Konan S. Impact of comorbid conditions on outcomes of hip and knee replacement surgery: a systematic review and meta-analysis. BMJ Open. 2018;8(7):
58. Batoz H, Semjen F, Bordes-Demolis M, Bnard A, Nouette-Gaulain K. Chronic postsurgical pain in children: prevalence and risk factors. A prospective observational study. Br J Anaesth. 2016;117(4):489–496. doi:10.1093/bja/aew260
59. Page B, Paterson C, Young D, O’Dwyer PJ. Pain from primary inguinal hernia and the effect of repair on pain. Br J Surg. 2002;89(10):1315–1318. doi:10.1046/j.1365-2168.2002.02186.x
60. Ashoorion V, Sadeghirad B, Wang L, et al. Predictors of persistent post-surgical pain following total knee arthroplasty: a systematic review and meta-analysis of observational studies. Pain Med. 2023;24(4):369–381. doi:10.1093/pm/pnac154
61. Mulford JS, Ackerman I, Holder C, Cashman KS, Graves SE, Harris IA. The association between body mass index and patient-reported outcome measures before and after primary total Hip or knee arthroplasty: a registry. ANZ J Surg. 2023;93(6):1665–1673. (in English). doi:10.1111/ans.18449
62. Neogi T. Structural correlates of pain in osteoarthritis. Clin Exp Rheumatol. 2017;35(5):S75–S78.
63. Murray DW, Fitzpatrick R, Rogers K, et al. The use of the Oxford hip and knee scores. J Bone Joint Surg Series B. 2007;89(8):1010–1014. doi:10.1302/0301-620X.89B8.19424
64. Miller TT. Sonography of joint replacements. Semin Musculoskelet Radiol. 2006;10(1):79–85. doi:10.1055/s-2006-934218
65. Dubousset J, Charpak G, Skalli W, Kalifa G, Lazennec JY. EOS stereo-radiography system: whole-body simultaneous anteroposterior and lateral radiographs with very low radiation dose. Revue de Chirurgie Orthopédique Et Réparatrice de L’appareil Moteur. 2007;93(6 Suppl):141–143. doi:10.1016/S0035-1040(07)92729-4
66. Kobayashi D, Choe H, Kobayashi N, Watanabe S, Inaba Y. Effects of changes in whole-body alignment on ipsilateral knee pain after total Hip arthroplasty. J Orthop Sci. 2023;28(2):398–402. doi:10.1016/j.jos.2021.12.006
67. Laporte S, Skalli W, de Guise JA, Lavaste F, Mitton D. A biplanar reconstruction method based on 2D and 3D contours: application to the distal femur. Comput Methods Biomech Biomed Eng. 2003;6(1):1–6. doi:10.1080/1025584031000065956
68. McKenna C, Wade R, Faria R, et al. EOS 2D/3D X-ray imaging system: a systematic review and economic evaluation. Health Technol Assess. 2012;16(14):1. (in English). doi:10.3310/hta16140
69. Lazennec JY, Rangel A, Baudoin A, Skalli W, Catonne Y, Rousseau MA. The EOS imaging system for understanding a patellofemoral disorder following THR. Orthop Traumatol Surg Res. 2011;97(1):98–101. (in English). doi:10.1016/j.otsr.2010.07.010
70. Huppertz A, Radmer S, Asbach P, et al. Computed tomography for preoperative planning in minimal-invasive total Hip arthroplasty: radiation exposure and cost analysis. Eur J Radiol. 2011;78(3):406–413. (in English). doi:10.1016/j.ejrad.2009.11.024
71. Gaffney CJ, Pelt CE, Gilliland JM, Peters CL. Perioperative pain management in hip and knee arthroplasty. Orthop Clin North Am. 2017;48(4):407–419. doi:10.1016/j.ocl.2017.05.001
72. Dahl JB, Kehlet H. The value of pre-emptive analgesia in the treatment of postoperative pain. Br J Anaesthesia. 1993;70(4):434–439. doi:10.1093/bja/70.4.434
73. Ge Z, Li M, Chen Y, et al. The efficacy and safety of parecoxib multimodal preemptive analgesia in artificial joint replacement: a systematic review and meta-analysis of randomized controlled trials. Pain Ther. 2023;12(4):1065–1078. doi:10.1007/s40122-023-00500-6
74. Lunn MPT, Hughes RAC, Wiffen PJ. Duloxetine for treating painful neuropathy or chronic pain. Cochrane Database Syst Rev. 2008;(2):
75. de Beer JDV, Winemaker MJ, Donnelly GA, et al. Efficacy and safety of controlled-release oxycodone and standard therapies for postoperative pain after knee or hip replacement. Can J Surg. 2005;48(4):277–283.
76. Cheville A, Chen A, Oster G, McGarry L, Narcessian E. A randomized trial of controlled-release oxycodone during inpatient rehabilitation following unilateral total knee arthroplasty. J Bone Joint Surg. 2001;83(4):572–576. doi:10.2106/00004623-200104000-00013
77. Früh A, Sargut TA, Hussein A, et al. Peripheral nerve stimulation for the treatment of chronic knee pain. Sci Rep. 2023;13(1):
78. Murphy J, Pak S, Shteynman L, et al. Mechanisms and preventative strategies for persistent pain following knee and hip joint replacement surgery: a narrative review. Int J Mol Sci. 2024;25(9):
79. Zhao J, Davis SP. An integrative review of multimodal pain management on patient recovery after total hip and knee arthroplasty. Int J Nurs Studies. 2019;98:94–106. doi:10.1016/j.ijnurstu.2019.06.010
80. Ferro Moura Franco K, Lenoir D, Dos Santos Franco YR, Jandre Reis FJ, Nunes Cabral CM, Meeus M. Prescription of exercises for the treatment of chronic pain along the continuum of nociplastic pain: a systematic review with meta-analysis. Eur J Pain. 2021;25(1):51–70. doi:10.1002/ejp.1666
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.