")
Back to Journals » Infection and Drug Resistance » Volume 16
Investigation of a Mask Fitness Test Based on Self-Efficacy and Diversified Training in the Assessment System for Nosocomial Infection Training
Authors Xiao B, Sun LL, Yuan J, Xiao WL, Liu Y, Cai MY, Liao QH
Received 5 September 2022
Accepted for publication 14 December 2022
Published 17 January 2023 Volume 2023:16 Pages 313—322
DOI https://doi.org/10.2147/IDR.S388784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Bing Xiao,1 Lu-Lu Sun,2 Jing Yuan,3 Wan-Ling Xiao,1 Ying Liu,4 Man-Yuan Cai,5 Qiao-Huo Liao2
1Department of Outpatient, the Third People’s Hospital of Shenzhen, Shenzhen, 518000, People’s Republic of China; 2Department of Pediatric, the Third People’s Hospital of Shenzhen, Shenzhen, 518000, People’s Republic of China; 3Department of Infectious Diseases, the Third People’s Hospital of Shenzhen, Shenzhen, 518000, People’s Republic of China; 4GI Medicine Department, the Third People’s Hospital of Shenzhen, Shenzhen, 518000, People’s Republic of China; 5Science and Education Department, the Third People’s Hospital of Shenzhen, Shenzhen, 518000, People’s Republic of China
Correspondence: Lu-Lu Sun, Department of Pediatric, the Third People’s Hospital of Shenzhen, No. 29 of Bulan Road, Longgang District, Shenzhen, 518000, People’s Republic of China, Tel +86 13510332310, Email [email protected]
Objective: To explore a mask fitness test based on self-efficacy and diversified training in the assessment system for nosocomial infection training.
Methods: From March 15 to April 5, 2022, 442 staff members (272 male and 170 female) of the Third People’s Hospital of Shenzhen who planned to enter the quarantine ward for secondary protection skill training assessment were selected. They comprised 56 doctors, 31 medical technicians, 72 nurses, and 283 property logistics staff. During the mask fitness test, a diversified training model based on self-efficacy was adopted to observe the passing status, the identification and selection of mask models, the method of mask-wearing, the fit between the mask and the face, and the changes in self-efficacy.
Results: In the assessment system for nosocomial infection training, the passing rate of the mask fitness test was correlated with the identification and selection of mask models, the method of wearing masks, the fit between the mask and the face, and the diversified training, and the differences were statistically significant (P < 0.05). The difference in the self-efficacy in the test takers between those before and after the mask fitness test was statistically significant (P < 0.05).
Conclusion: In the assessment system for nosocomial infection training, the mask fitness test based on self-efficacy and diversified training might improve the passing rate, the rate of correct mask model identification and selection, the rate of correct mask-wearing, and the degree of facial fit, thus to enhance the awareness of protection and improve self-efficacy.
Keywords: self-efficacy, mask fitness test, training mode
Introduction
According to the data concerning the coronavirus disease 2019 (COVID-19) issued by the World Health Organization (WHO) as of February 22, 2022, there have been more than 424 million confirmed cases of COVID-19 infection worldwide, resulting in 5,890,312 deaths.1 Respiratory droplets and close contact are the main transmission routes of the virus leading to COVID-19.2 Previous meta-analysis have provided the latest state-of-art evidence on the efficacy of masks in preventing the transmission of COVID-19 and reducing the risk of infection. The protective effects of masks against COVID-19 were not only significant for healthcare workers, but also population.3,4 However, protective masks are effective respiratory protective equipment. The fitness of this protective equipment directly determines the protective effect on the respiratory tract.5
It is required by WHO, the United States, and the European Union that a fitness test should be conducted when wearing respiratory protective equipment. Studies from abroad have shown that in the absence of the fitness test, the average exposure rate of the test takers is reduced to 33% of the environmental level. While through the fitness test, the protection obtained is much higher than that from the normally expected level (the average exposure rate is reduced to 4% of the environmental level).6 Currently, China also has relevant national and industry standards, which clearly stipulate the requirements for the fitting of the mask to the face as well as the measurement of the fitness of respiratory protective equipment and medical protective masks.7,8
In actual clinical practice, front-line medical staff generally wear masks directly provided by the hospitals, with a lack of relevant training on fitness and relevant testing methods.9 Facing the global pandemic of Omicron mutants, the dynamic zero-clearing policy faces huge challenges in China.10–13 To cope with the dual requirements of the wartime state of the epidemic and the normalization of epidemic prevention and control, a mask fitness tester was adopted by the staff in this study during the mask fitness test assessment.14 The tests of self-efficacy, objective mask fitness, and diversified training modes were adopted to improve protection skills and achieved satisfactory results.
Study Subjects
From March 15 to April 5, 2022, 442 staff members (272 male and 170 female) who would be working at the designated hospital for the treatment of patients with COVID-19 in the Third People’s Hospital of Shenzhen and would enter the quarantine ward for the second-level protection skill training assessment were enrolled. There were 56 doctors, 31 medical technicians, 72 nurses, and 283 property logistics staff (Table 1).
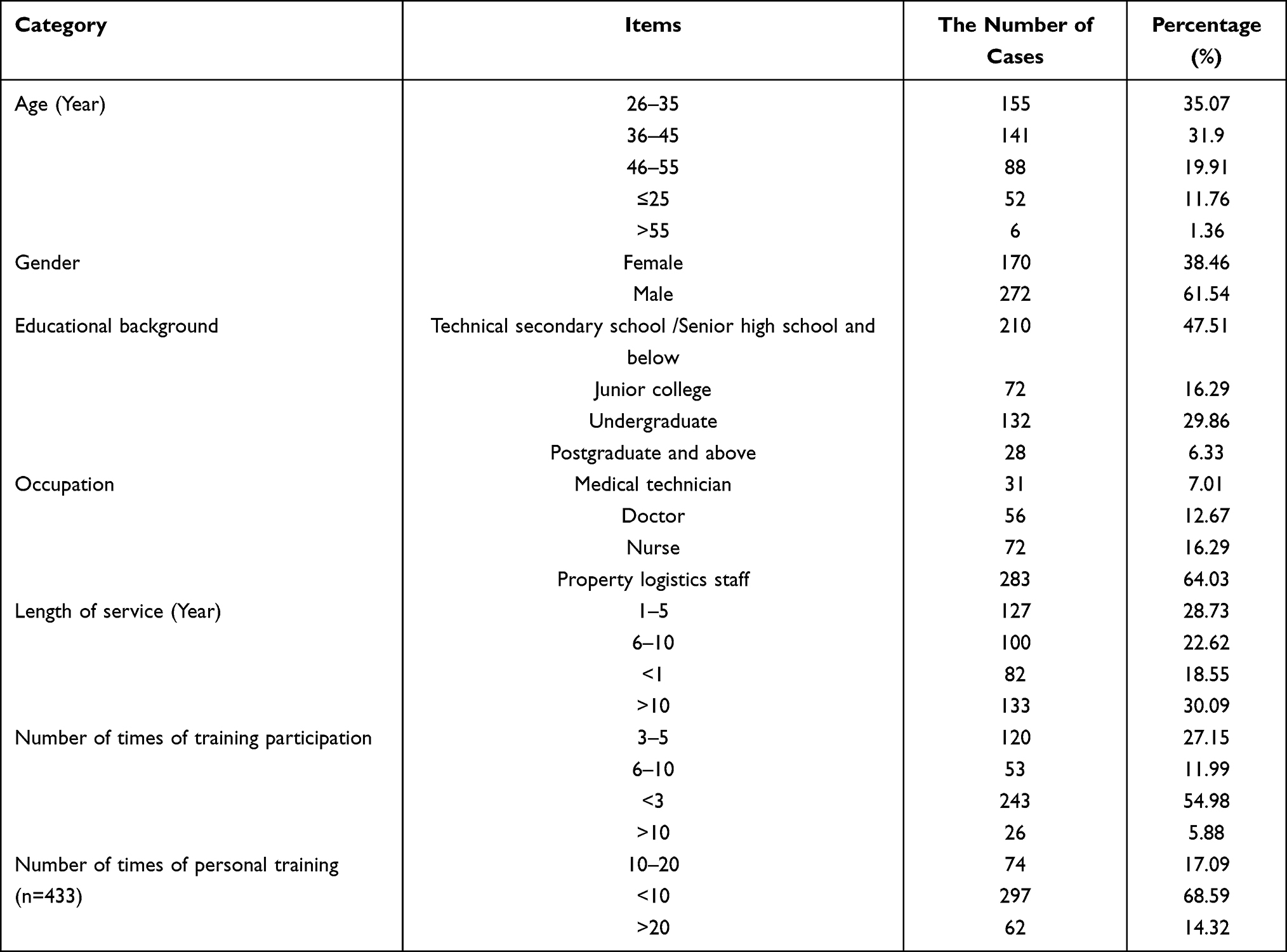 |
Table 1 The General Data of the Staffs Who Planned to Enter the Quarantine Ward for the Training and Assessment of Secondary Protection Skills (n=442) |
The inclusion criteria were as follows: (1) staff in good health, including those who were asymptomatic and with stable underlying diseases (hypertension, diabetes mellitus, cardiovascular disease, etc.) and those without respiratory infectious diseases (tuberculosis, influenza, COVID-19, etc.); (2) staff who were not pregnant; (3) staff without beards; (4) staff who had not smoked within 30 min before the test; (5) staff who had participated in theoretical knowledge training, simulated scene training, and nosocomial infection and secondary protection theory assessment in the skills training center and had achieved 100 points; (6) staff who had completed three doses of the novel coronavirus vaccine for at least 14 d; and (7) staff who voluntarily signed a commitment and entered the quarantine ward.
The exclusion criteria were as follows: (1) staff with symptomatic disease or a history of other serious medical conditions, (2) staff with a height <145 or >185 cm, (3) staff with a weight < 35 or >95 kg, or (4) staff who were illiterate.
Methods
Assessment Team Training
The team consisted of 34 staff from the Infection Control Department, the Nursing Department, the Medical Department, the General Affairs Department, and the Skills Training Center. They were divided into the infection control supervision team, the scenario-based simulation team, the teaching guidance team, the logistics support team, the assessment team, and the appointment review team (Figure 1). All members were included after passing the examinations for the homogenized secondary protection skill training. The members were very familiar with the theoretical knowledge of nosocomial infection and secondary protection, operation procedures, mask fitness test, pipeline disinfection, and training methods.
 |
Figure 1 The structure diagram of the training and assessment team. |
Secondary Protection Skill Training and Assessment Process
According to the “Guidelines for the Usage Scope of Common Medical Protective Equipment in the Prevention and Control of COVID-19 (Trial)”,15 the “Secondary Protection Skill Assessment Form” was formulated (Figure 2), and those with an assessment score of 100 points were considered as qualified. The assessed person should scan the code on the mobile terminal to make an appointment in advance, scan the site code to punch in the card on the day of the assessment, fill in the paper version of the assessment form, and receive onsite operation training, guidance, and practice of the secondary protection skill.
 |
Figure 2 Flow chart of the training and assessment procedures for the secondary protection skills. Abbreviations: OSCE, objective structured clinical examination; SPOC, Small Private Online Course; CBL, case-based learning; PBL, problem-based learning. |
Diversified Training Mode
The scenario-based simulation teaching mode of the objective structured clinical examination (OSCE) was adopted before the assessment of the mask fitness test. The OSCE is a tool for the evaluation of clinical practice ability and scenario-based simulation, which may provide the trainees with a simulated real practice scene, allowing them to complete tasks during the process of experiencing the role.16 First, the scenario-based simulation team completed the onsite arrangement under the guidance of the infection control supervision team. Then the scenario was set as follows: (1) hand hygiene, selection of protective equipment, donning, and doffing; (2) emergency management of occupational exposure after contact with a patient with COVID-19; and (3) protective equipment removal and medical waste disposal. The student would undergo onsite training and drills in sequence, and the instructor would make a preliminary evaluation according to the secondary protection skill assessment form and provide targeted guidance.
Those who failed the first assessment of the mask fitness test would be trained by drawing a mind map and one-on-one skill guidance mode. Mind mapping is an approach of visualizing human thinking. With the adoption of the technique of paying equal attention to both pictures and text, hierarchical diagrams or mutual affiliation are used to express themes at all levels.17 First, the assessment team would provide feedback to the teaching guidance team regarding the secondary protection skill assessment form and the reasons for failing the test. The teaching team would help the student draw a mind map according to the problems found, as follows: (1) determine the central keywords; (2) disperse multiple knowledge points according to the keywords; and (3) one-on-one skill guidance to strengthen the weak points and easily overlooked parts, thereby enhancing self-confidence.
For those who failed the second assessment of the mask fitness test, a teaching mode of a small-scale restricted online course was adopted. This mode was to organically combine online courses with modern classroom teaching, while using flipped classroom teaching to improve the teaching quality.18 The teaching guidance team would send the strengthening operation video to the student through WeChat. The video comprised narration, action decomposition, assessment standard explanation, error-prone analysis, and an online interaction section. The teaching team would demonstrate errors on the spot and raise questions to the student, asking them to answer the mistaken points and explain emergencies to strengthen standardized operation memory and improve their ability to deal with emergencies.
For those who failed the mask fitness test three or more times, case-based learning and problem-based learning19 combined with peer-to-peer teaching were adopted. Students were divided into groups by the teaching team, with 2–3 subjects in each group. The teaching group arranged occupational exposure cases in the quarantine ward according to the specific problems. The group members would discuss and analyze the cases, and the teaching group would answer the questions. Team members acted as examiners for each other and conducted scenario-based simulation for specific problems to guide each other and strengthen the knowledge points. The teaching team would provide appropriate psychological adjustments according to the psychological status and occupational characteristics of the examinees to improve their enthusiasm and self-identity.
Mask Fitness Test
During the assessment of conventional secondary protection skills, all the assessed personnel routinely wore N95 masks of the same brand, following the training requirements. These were that the assessed personnel chose the type of mask they considered being suitable and wore it according to the conventional method of wearing masks, which involved the index fingers of both hands pressing the metal strip along the upper edge of the mask onto the bridge of the nose and adjusting the tightness of the strap. The test method was to cover the mask with both hands and then exhale vigorously. If air came from the edge of the mask, this indicated improper wearing, and the strap and metal strip on the bridge of the nose should be adjusted until no air escaped when exhaling vigorously. During the test, no one was given guidance or instruction. In this study, in addition to the routine mask-wearing by the examinees, the mask fitness test was conducted with the adoption of the TSI 8048 type respirator fitness tester. The specific operation procedures were as follows:
Dual air tubes and the power supply were installed before starting the instrument, and TSI FitPro Ultra software was installed on the computer;
The system was powered on and routine quality control testing was conducted;
The mask sampling probe was installed on the N95 mask and tightly connected with the dual airline interface;
The examinee was instructed to follow the animation displayed on the screen to complete the testing actions in sequence: bend deeply for 30s, speak loudly for 30s, swing head left and right for 30s, look up and down for 30s, with the total test time of 2.5 min;
When the test was completed, the software interface would display green to indicate success and red to indicate failure. For those who failed, the tester helped them analyze the reasons for the failure, such as whether the mask model was suitable, whether the method of mask-wearing was correct, as well as the face shape, etc. The teaching team would provide them with different training modes to conduct improved training, and re-test as required until they passed.
After each student completed the test, the mask and sampling probe were unplugged from the dual gas pipeline, and then a special pipeline sterilizer was adopted to sterilize the dual gas pipeline and quickly dry it for repeated use.
Observation Indicators
The observation indicators were mask model identification and selection, mask-wearing method, facial fitness, passing status of the mask fitness test, and evaluation of self-efficacy.
Statistic Methods
Double entry was adopted for data input and SPSS™ Statistics v25.0 software was used for statistical analysis. The measurement data were expressed as means ± standard deviations ( ) and tested for normality and homogeneity of variance. The t-test was adopted for data that conformed with the normal distribution. The countable data were expressed as the number of cases (n) (percentages %), and the χ²-test was adopted for comparison between groups. A value of P < 0.05 was considered statistically significant.
) and tested for normality and homogeneity of variance. The t-test was adopted for data that conformed with the normal distribution. The countable data were expressed as the number of cases (n) (percentages %), and the χ²-test was adopted for comparison between groups. A value of P < 0.05 was considered statistically significant.
Results
Comparison of the Results of Mask Fitness Test with Diversified Training
The passing status of the mask fitness test was correlated with the identification and selection of mask models, the method of mask-wearing, and the fit between the mask and the face, and the differences were statistically significant (P < 0.05) (Table 2).
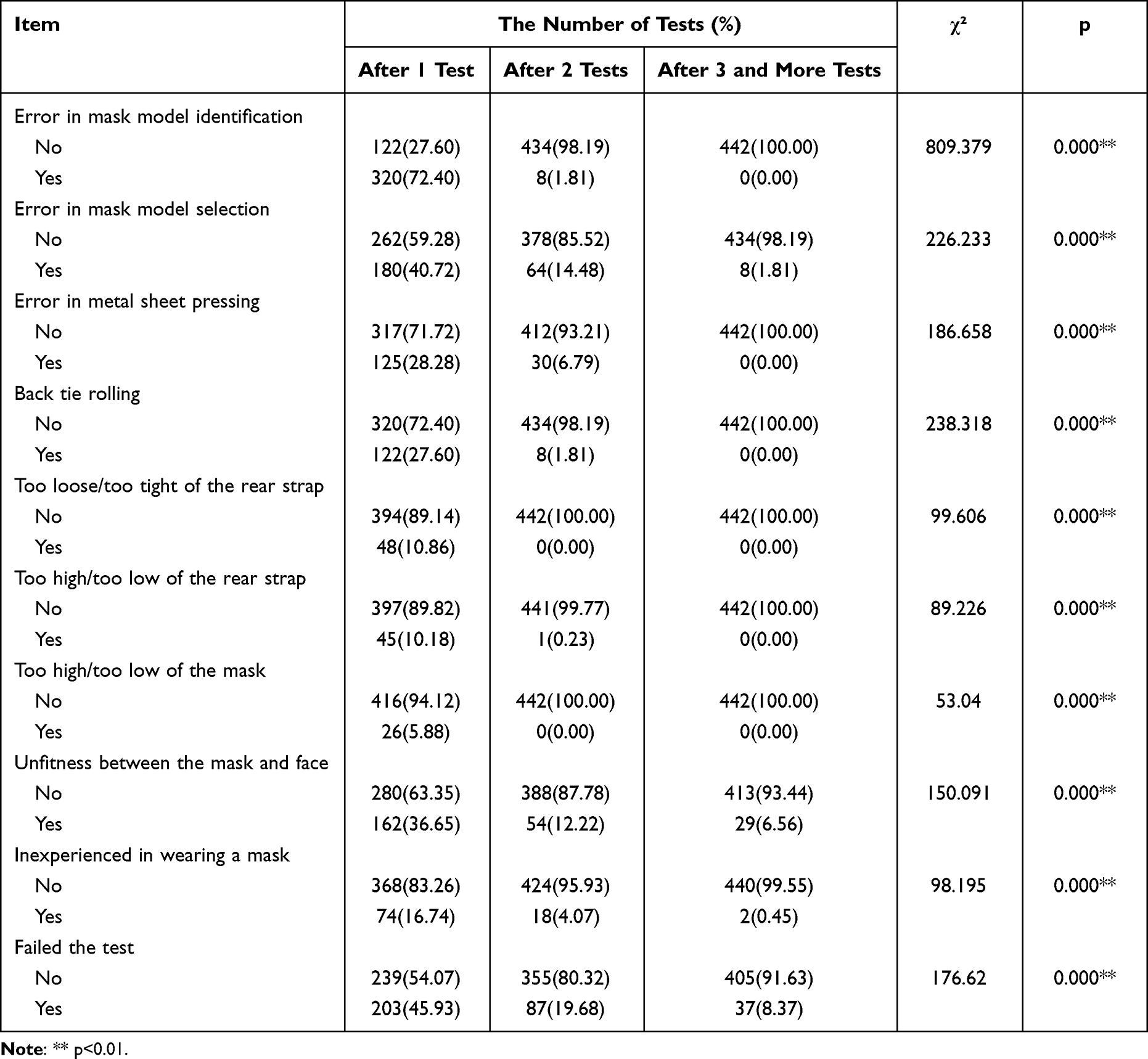 |
Table 2 Comparison of the Results of Mask Fitness Test with Diversified Training |
Comparison of the Self-Efficacy of the Test Takers Before and After the Mask Fitness Test Based on the Self-Efficacy Theory
The general self-efficacy scale (GSES) was prepared by Schwarzer et al,20 with a total of 10 items and adoption of the Likert four-point scale, ranging from completely incorrect (one point) to completely correct (four points) for the assessment. According to the score, it could be divided into three levels: low (10–20 points), medium (21–30 points), and high (31–40 points). The higher the score, the higher the self-efficacy. The Cronbach’s alpha coefficient of the internal consistency was 0.81. The comparison of the self-efficacy of the test takers before and after the mask fitness test is shown in Table 3.
 |
Table 3 Comparison of General Self-Efficacy Before and After the Mask Fitness Test(n=442) |
Discussion
Improve Self-Efficacy
Self-efficacy theory was first proposed by American psychologist Bandura21 in 1977. It refers to an individual’s subjective evaluation of whether he/she can complete a certain task or job, and it can also be considered as the belief or judgment of organizational and executive ability of an individual’s behavioral process for completing a given behavioral goal.22 Strengthening self-efficacy is of great significance to work motivation enhancement and work attitude improvement,23 and is helpful for changing behavior.24 In the present study, the difference in the GSES scores before and after the mask fitness test was statistically significant (P < 0.05). The mask fitness test could quickly evaluate the protective effect and safety of the tested subject regarding correct mask-wearing. The diversified training could strengthen the application of protection knowledge and the proficiency in protection skills of the students. The self-efficacy of the students became higher with reduced tension, a more positive work attitude, and enhanced confidence in completing the task, therefore better protecting the physical and mental health of staff. During this investigation, positive feedback and recognition from the test takers was continuously received.
Mask Fitness Test
The mask fitness test relies on the instrument to detect whether there is air leakage around the contact between the mask and face. It does not rely on personal subjective feelings and judgments, thus has better accuracy and authenticity. During the fitness test, it was found that when the students completed various tests according to the instructions, the selection of mask model, whether hemmed, the position and tightness of the strap, the position of the mask, and the proficiency in mask-wearing all affected the passing rate to varying degrees. Therefore, the training and assessment team was committed to continuously improving the mask-wearing and mask-removing skills, the proficiency, and protection awareness of the students through a diversified training mode to continuously improve their protection skills and the test passing rate. During the process, the self-efficacy of the test takers was improved, and they adapted better to work in the quarantine ward. It was found in the present study that the more working experience in the quarantine ward and duration of training and practice, the stronger the awareness of protection, the higher the proficiency, and the easier it was for the students to pass the mask fitness test.
The Mask Tightness Test
The fitness test is to detect the sealing performance between the edge of the mask and the wearer’s face. It mainly depends on whether the shape, size, nose clip, and mask strap of the mask matches the wearer’s face.25,26 As illustrated in Table 2, before the mask fitness test in this study, 72.4% of the test takers did not know how to distinguish the mask model, and 40.72% of them did not know which type of mask was suitable for them to wear. Combined with the reasons for the failure of the students in each fitness test, it was conducted again after applying diversified training. Therefore, all the test takers knew how to distinguish the mask model and could determine the mask model that was suitable for themselves. Studies have shown that different testers had great differences in the fitness test of the same type of protective mask.27 With the help of the mask fitness test under the diversified training mode, the medical staff could choose the most suitable type of protective mask for personal use, and the test takers could master the correct methods and the details concerning mask-wearing. As demonstrated in Table 2, before the fitness test in this study, 28.28% of the test takers did not use the index fingers of both hands to press the metal piece along the upper edge of the mask onto the bridge of the nose but used their thumb and index finger, making an acute angle of the metal piece, and the mask could not be completely attached to the face, which resulted in air leakage, thereby reducing the fitness of the mask. In addition, 6.56% of the test takers passed the fitness test after multiple attempts even though the mask was worn correctly; details are shown in Table 2. The reason might be due to the fixed specifications of the mask, and it was impossible to make the mask fit perfectly with each subject’s face, resulting in insufficient facial fitness with reduced protective performance.28 In the present study, the same brand of mask was adopted for each student, so there are certain limitations.
Disinfection Management in the Mask Fitness Test
When the test takers completed the mask fitness test, the pipeline in the test instrument was sterilized before further use. However, currently, there is no dedicated pipeline sterilizer on the market. During the test, the mask was connected to the environment inside the pipeline. With normal breathing, there would be residual viruses transmitted through the respiratory tract in the pipeline, and there was a risk of cross-infection in the case of repeated use without disinfection. In the present study, the application of a pipeline sterilizer was explored, and the pipelines were perfused and sterilized with 75% alcohol and dried quickly to ensure they were quickly sterilized one at a time with a reduction in the risk of cross-infection.
Sampling Probe
In addition, a sampling probe should be installed on the test mask when conducting the mask fitness test, and the test mask should not be worn anymore. Considering the cost of testing equipment and test masks together with the workforce required to complete the test, it was recommended that during the process of high-risk aerosol exposure environments and operations (pathogenic microorganism laboratories, respiratory infectious disease areas, viral nucleic acid sampling, dust environments, etc.), attention should be paid to the mask fitness test based on self-efficacy and diversified training mode to ensure the health and safety of staff.
Conclusion
In summary, in the assessment system for nosocomial infection training, the mask fitness test based on self-efficacy and diversified training could improve the correct rate of mask model identification and selection, the correct rate of mask-wearing, and the facial fit for the staff, thereby enhancing the protection awareness and strengthening the protection skills with higher self-efficacy and good effect.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of the Third People’s Hospital of Shenzhen. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Shenzhen Key Medical Discipline Construction Fund. Supported by Shenzhen Fund for Guangdong Provincial High-level Clinical Key Specialties (No:SZGSP011).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Baj A, Novazzi F, Pasciuta R, et al. Breakthrough infections of E484K-harboring SARS-CoV-2 delta variant, lombardy, Italy. Emerg Infect Dis. 2021;27(12):3180–3182. doi:10.3201/eid2712.211792
2. The General Office of the National Health Commission, The Office of the State Administration of Traditional Chinese Medicine. 新型冠状病毒肺炎诊疗方案(试行第九版 [COVID-19 diagnosis and treatment program (Trial Ninth Edition)]. 2022.3.14. Medical letter from the National Health Office; 2022. Chinese.
3. Liang M, Gao L, Cheng C, et al. Efficacy of face mask in preventing respiratory virus transmission: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;36:101751. doi:10.1016/j.tmaid.2020.101751
4. Li Y, Liang M, Gao L, et al. Face masks to prevent transmission of COVID-19: a systematic review and meta-analysis. Am J Infect Control. 2021;49(7):900–906. doi:10.1016/j.ajic.2020.12.007
5. Hon CY, Danyluk Q, Bryce E, et al. Comparison of qualitative and quantitative fit-testing results for three commonly used respirators in the healthcare sector. J Occup Environ Hyg. 2017;14(3):175–179. doi:10.1080/15459624.2016.1237030
6. Laboratory performance evaluation of N95 filtering facepiece respirators. Available from: http://www.cdc.gov/mmwr/preview/mmwrhtml/00055954.htm.
7. State Administration of Quality Supervision, Inspection and Quarantine, PRC, Standardization Administration of China. GB19038-2010医用防护口罩技术要求. [GB19038-2010 Medical Protective Mask Technical Requirements]. Beijing: China Standards Press; 2011. Chinese.
8. The National Health and Family Planning Commission of the PRC. WS233-2017病原微生物实验室生物安全通用准则 [WS233-2017 General Guidelines for Biosafety of the Pathogenic Microbiology Laboratory]. Beijing: China Standards Press; 2017. Chinese.
9. Bai F, Guo JL, Yang HY. 影响医用 N95 防护口罩使用性能的障碍因素研究进展 [Progress on obstacle factors affecting the performance of medical N95 protective masks]. Chine Remedies Clin. 2021;21(4):592–594. Chinese.
10. Lu H. More effective vaccines and oral antivirals: keys for the battle against Omicron. Biosci Trends. 2022;16(1):1–3. doi:10.5582/bst.2022.01062
11. Yao CL, Wei WL, Zhang JQ, et al. Traditional Chinese medicines against COVID-19: a global overview. World J Tradit Chin Med. 2022;8:279–313. doi:10.4103/2311-8571.353502
12. Song ZJ, Nik Nabil WN, Xi ZC, Xu HX. Current global status and future development of traditional Chinese medicine in the prevention and treatment of coronavirus disease 2019. World J Tradit Chin Med. 2021;7:155–166. doi:10.4103/wjtcm.wjtcm_43_20
13. Li MX, Yang YY, Liu Y, et al. Progress of traditional Chinese medicine treating COVID-19. World J Tradit Chin Med. 2021;7:167–183. doi:10.4103/wjtcm.wjtcm_68_20
14. Li JS, Zhang K, He CL, et al. 呼吸道防护装备佩戴密合度测定仪的研制 [Development of tightness tester for respiratory tract protective equipment]. China Med Equip. 2018;15(9):1–4. Chinese.
15. National Health Commission. 新型冠状病毒感染的肺炎防控中常见医用防护用品使用范围指引(试行) [Guidelines on the use scope of common medical protective equipment in the prevention and control of novel coronavirus pneumonia (trial)]; 2020. Chinese.
16. Li SW, Yang MY, Mao Y, et al. OSCE模式情景模拟教学法在新冠疫情期间低年资护士院感防控培训中的应用. [The application of OSCE model scenario simulation teaching method for young nurses in hospital fever prevention and control training in period of COVID-19 outbreak]. Med Pharm Yunnan. 2021;42(2):186–187. Chinese.
17. Song CX, Li WM, Liu CZ. 思维导图在护理文书书写及质量控制中的应用 [Application of mind mapping in nursing document writing and quality control]. Mod Hospitals. 2020;20(4):510–515. Chinese.
18. Cai JP, Zhou DL, Liu WJ, et al. SPOC 教学模式在血液科护理教学中的应用 [Application of SPOC teaching in hematology nursing teaching]. China Higher Med Educ. 2021;12:65–79. Chinese.
19. Sun Y, Zhang QJ, Liu LL. 对分课堂融合CBL+PBL模式在妇产科护理学教学中的应用效 [The application effect of integrating CBL + PBL model in the nursing teaching of obstetrics and gynecology]. Health Vocat Educ. 2018;36(20):93–94. Chinese.
20. Swhwarze R, Raristi B. Optimistic self-beliefs assessment of general perceived self-efficacy in thirteen cultures. World Psychol. 1997;3(1–2):177–190.
21. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295x.84.2.191
22. Zeng J, Zhang Q, Xu H. 改良式正念减压法对头颈部鳞癌放疗患者自我效能和正念水平的影响 [Effect of modified MBSR on self-efficacy and mindfulness level in patients with HNSCC radiotherapy]. J Nurs. 2021;28(2):65–68. Chinese.
23. Zhou WX, Guo GP. 自我效能感 概念、理论和应用 [Self-efficacy: the conception, theory and applications]. J Renmin Univ China. 2006;1:91–97. Chinese.
24. Gao CR, Xu DM, Cao DF. 基于自我效能理论的康复护理模式在首发脑卒中恢复期患者中的应用 [Application of rehabilitation nursing model based on self-efficacy theory in patients with first stroke]. J Qilu Nurs. 2018;24(13):83–86. Chinese.
25. Zhang K, Hu LF, Jin AJ, et al. Quantitative face fit test and comparison of five types of protective masks. Chine Med Biotechnol. 2018;13(2):117–121.
26. Liu ZY, Ke JC, Zheng YY, et al. Analysis of the performance of protective face mask for medical use. China Personal Protect Equip. 2017;1:28–32.
27. Zhang XY, Li YZ, Jia N, et al. 颗粒物防护口罩适合因子的影响因素研究 [Research on factors affecting particulate respirator fit factor]. China Safety Sci J. 2015;25(3):121–125. Chinese.
28. Li M, Tian MY. Technical standards and prospects of medical masks. Shandong Sci. 2020;33(3):28–34.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.