")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Investigation and Analysis of the Current Status of Rationality and Standardization of Oxygen Therapy in Hospitalized Adult Patients
Authors Wang J, Zhou L, Liu K, Dou L, Wang R, Chen B
Received 21 March 2023
Accepted for publication 22 May 2023
Published 12 July 2023 Volume 2023:16 Pages 1915—1926
DOI https://doi.org/10.2147/JMDH.S404595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jun Wang,1 Li Zhou,2 Ke Liu,3 Luqun Dou,4 Rui Wang,2 Bing Chen1
1Department of Nursing, Leshan People’s Hospital, Leshan, 614000, People’s Republic of China; 2Department of Intensive Care Unit, Leshan People’s Hospital, Leshan, 614000, People’s Republic of China; 3Department of Gastrointestinal Surgical, Leshan People’s Hospital, Leshan, 614000, People’s Republic of China; 4Department of Cordiovascular Surgery, Leshan People’s Hospital, Leshan, 614000, People’s Republic of China
Correspondence: Bing Chen, Department of Nursing, Leshan People’s Hospital, No. 238 of White Tower Street, Shizhong District, Leshan, 614000, People’s Republic of China, Tel +86 13890655907, Email [email protected]
Objective: To investigate the rationality and standardization of oxygen therapy for hospitalized adult patients, so as to provide a basis for improving the quality of oxygen therapy care.
Methods: Self-designed “Inpatient Oxygen Therapy Status Questionnaire”, using a cross-sectional survey, surveyed 185 oxygen inhalation patients in a tertiary general hospital from August 3– 15, 2020, based on the formulation and promulgation of the Chinese Nursing Association The “Nursing care for adult patient with oxygen therapy” standard evaluates the rationality of clinical oxygen therapy implementation and the standardization of nursing measures.
Results: The reasonable rate of oxygen therapy for hospitalized adult patients was 19.46%, and the standardized rate of nursing measures was 54.52%. The reasonable and standardized rates of medical wards were higher than those of surgical and specialized wards, and were statistically significant (P< 0.05). The incidence of complications of oxygen therapy was positively correlated with the rationality of oxygen therapy and the standardized data of nursing measures.
Conclusion: The clinical oxygen therapy nursing practice and the standard of “Nursing care for adult patient with oxygen therapy” are quite inadequate. There are differences in the quality of oxygen therapy in different wards. Nursing managers should strengthen training and management, standardize nursing behaviors, and improve the quality of oxygen therapy and ensure oxygen therapy for patients’ safety.
Keywords: clinical nursing, cross-sectional survey, oxygen inhalation therapy, rationality, normative
Introduction
Oxygen therapy (oxygen inhalation therapy) is a routine and indispensable treatment for patients with acute hypoxemia caused by various reasons. At present, the clinical oxygen therapy methods include traditional nasal catheter, ordinary mask, oxygen storage mask, nasal high flow oxygen therapy and mechanical ventilation oxygen therapy. Oxygen is the most widely used in clinical medicine and the largest amount of medical gas. It is the key substance of human metabolic activity. It can be used for the treatment and first aid of hypoxic patients, oxygen supplementation in hypoxic environment, health care and fatigue recovery of normal people.1 In daily life, sudden and dangerous emergencies such as heart disease, stroke, asthma attacks, and pregnant women ‘s labor syndrome need to use oxygen for emergency rescue,2 especially patients with chronic obstructive pneumonia need long-term oxygen therapy.3 It can be seen that oxygen, as the first element to maintain life, is a necessary hardware condition for medical institutions at all levels.
In order to standardize clinical oxygen therapy, many countries have issued clinical oxygen therapy guidelines.4–8 The multi-center oxygen therapy study reported by Neves et al9 shows that the clinical implementation of oxygen therapy has poor standardization and rationality, and attempts to improve the quality and safety of oxygen therapy to standardize clinical oxygen therapy practices. At present, there are relevant researches on the rationality and standardization of clinical oxygen therapy orders in China.10 Cao Jie et al11 proposed to avoid the harm of hyperoxia and standardize the target oxygen therapy in order to promote the standardization of clinical oxygen therapy in China.12 China has issued two expert consensuses on oxygen therapy, but there are no normative documents to follow for the comprehensive evaluation, adaptation conditions and observation in the application process before the implementation of oxygen therapy.13,14 Domestic nursing staff still have incomplete understanding and non-standard operation. However, there are few investigations on the current situation of the implementation of clinical oxygen therapy, and there are few investigations on the rationality and standardization of the implementation of oxygen therapy. From the perspective of clinical practice, there is a relatively random phenomenon in the use of clinical oxygen therapy, which should be standardized. Based on the group standard of “adult oxygen inhalation therapy nursing” issued by the Chinese Nursing Association15 (hereinafter referred to as “oxygen therapy standard”), this study used the cross-sectional survey method to investigate the current situation of the implementation of clinical oxygen therapy in our hospital, and preliminarily explored the rationality of the implementation of oxygen therapy and the standardization of nursing measures for adult inpatients in our hospital.
Materials and Methods
Study Subjects
In this study, a cross-sectional survey method was used to select 185 patients with oxygen inhalation admitted to a tertiary general hospital from August 3 to 15, 2020 by convenient sampling. The field investigation site was selected from our hospital (ENT Surgery, Hepatobiliary and Pancreatic Spleen Surgery, Joint Surgery, Spine Surgery, Department of Neurosurgery, Urology, Gastrointestinal Surgery, Cardiothoracic Surgery, Neuro-brain Surgery). Vascular Surgery), Internal Medicine (Cardiovascular Internal Medicine, Neurology, Endocrinology, Respiratory and Critical Care Medicine, Gastroenterology, Rehabilitation / Neurology, Geriatrics, Nephrology), Specialty (Obstetrics, Gynecology, Critical Care Medicine, Oncology Department, Department of Rheumatology and Immunology, Department of Infectious Diseases), and a total of 23 departments and wards for clinical oxygen therapy surveys. Inclusion criteria: (1) Patients who are undergoing oxygen therapy on their beds during the survey period; (2) Patients who are in the interval between two oxygen therapies. Exclusion criteria:(1) Patients who are undergoing hyperbaric oxygen and mechanical ventilation; (2) Patients who have not received oxygen therapy or have stopped oxygen therapy. The research object screening process was shown in Figure 1. This study was approved by the hospital ethics committee and that all participants signed informed consent.
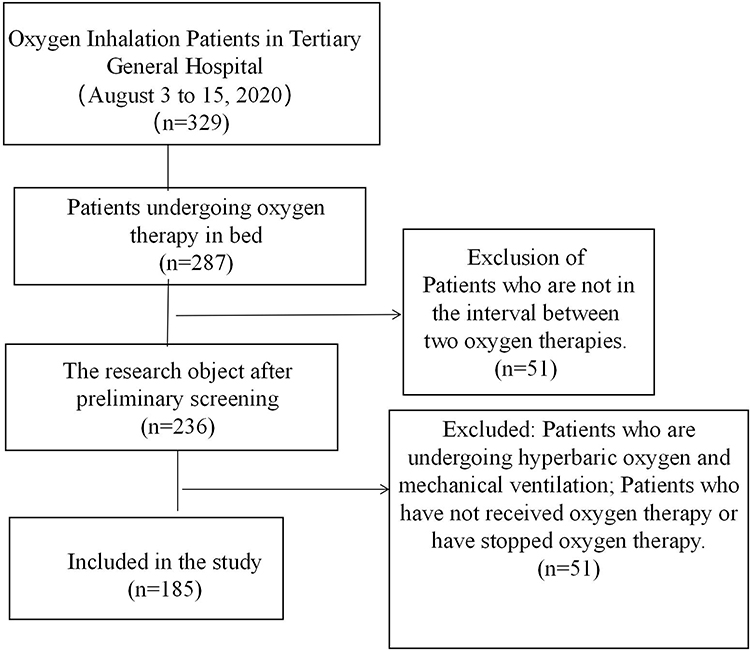 |
Figure 1 Research object screening process. |
Study Methods
Research Tools
This study refers to the research design of Neves et al,9 and is based on the “oxygen therapy standard”, and the “Inpatient Oxygen Therapy Quality Questionnaire” discussed and designed by members of the oxygen therapy quality control project team of our hospital. It includes two parts:
- Basic information of patients;
- Implementation of clinical oxygen therapy: ① Before oxygen therapy, assess whether the patient needs oxygen inhalation, whether there is hypercapnia /hypercapnia risk, whether the oxygen target is determined based on the condition; ② During the implementation of oxygen therapy, whether the choice of oxygen therapy tools and oxygen flow is correct, whether the actual monitoring of blood oxygen saturation reaches the target blood oxygen saturation, whether the oxygen therapy pipeline and oxygen therapy humidification care meet the standards, and whether the health education for patients and their families is effective, etc. In this study, oxygen therapy health education was carried out for patients and their families in the form of bedside education, making brochures and playing oxygen therapy health education videos, and training was carried out from the aspects of oxygen therapy purpose, indications, methods, complications and safety precautions. Through face-to-face interviews, this study understands the oxygen therapy knowledge of patients and their families: ①whether they know the purpose of oxygen use; ②Whether they know that they can not adjust the flow and stop the oxygen automatically; ③Whether they know the complications of oxygen use, and inform the medical staff in time in case of headache, dizziness, dry nasal mucosa and other discomfort; ④Do you know the safety precautions for oxygen use.
Data Collection
The investigators used bedside case-by-case surveys and searched electronic medical orders to determine the oxygen use for all hospitalized adult patients. For the included oxygen therapy patients, with the patients’ consent, consult hospitalization medical records, nursing records, collect blood oxygen saturation data on site, interview responsible nurses and patients, and fill in the “Inpatient Oxygen Therapy Quality Survey Form” one by one.
Quality Control
Before the investigation, the investigators were given a two-day special training. The training contents include “oxygen therapy standard”, specific process of cross-sectional survey, standard filling of questionnaire, simulation survey and data acceptance. After completing the questionnaires, two people checked all the collected data at the investigation site, immediately filled in and modified the missing information and obvious logical errors, and recovered the questionnaires after they were checked. The data of the questionnaires is numbered uniformly and entered into the SPSS software to establish a database. Double-entry method was used to check the consistency of the data, and at the same time set reasonable data boundary values and logical check items. After data entry was completed, logic check was performed, and if there was an error, the original data would be checked for correction.
Evaluation Method
Evaluation of Rationality
The “oxygen therapy standard” was used as the rationality evaluation standard, and the rationality of clinical oxygen therapy indications was evaluated according to the four types of indications recommended in the standard. The evaluation process and standard are shown in Figure 2.
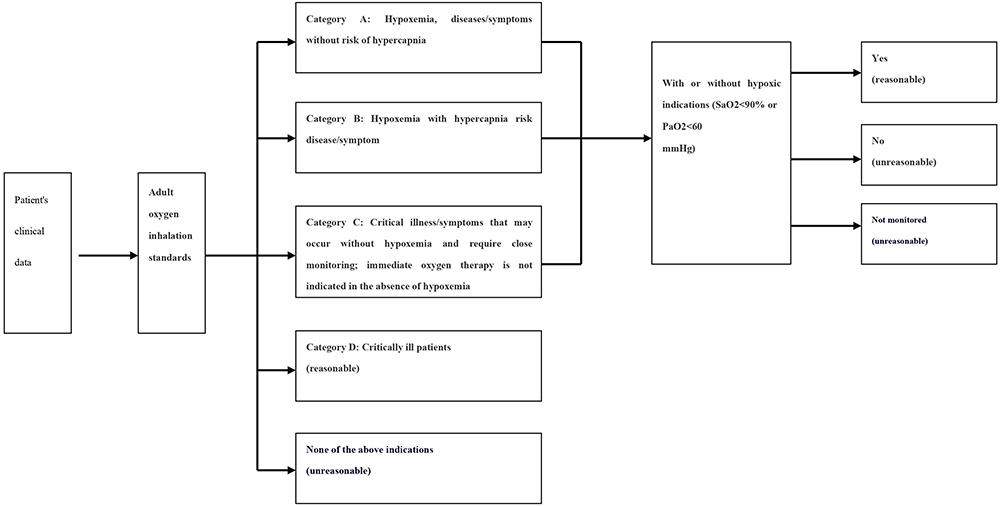 |
Figure 2 Process and criteria for evaluating the reasonableness of oxygen therapy for adults. |
The 4 types of indications are: A: Hypoxemia, diseases/symptoms without risk of hypercapnia; B: Hypoxemia with diseases/symptoms with hypercapnia or hypercapnia risk; C: Critical diseases/symptoms without hypoxemia may appear, requiring close monitoring. Oxygen therapy should not be used to treat critically ill patients without hypoxemia; D: Critically ill patients. The evaluation criteria are as follows: ① If the indications do not meet the above 4 types of oxygen therapy indications, the use of oxygen is judged as unreasonable oxygen use; ② If it is necessary to judge whether there is an indication of hypoxemia in the three indications of A, B, C, if there is hypoxemia, it is reasonable to use oxygen, and if there is no monitoring or no indication of hypoxemia, it is unreasonable use of oxygen. Hypoxemia is defined as PaO2 (arterial partial pressure of oxygen) in the blood <60mmHg and SaO2 (blood oxygen saturation) <90% under standard atmospheric pressure.16 Hypercapnia is defined as the partial pressure of arterial carbon dioxide in the blood>45 mmHg under standard atmospheric pressure.17
Standardized Evaluation
The “oxygen therapy standard” was used as the standard to evaluate the standardization of nursing measures. (1) The standardized evaluation process and standard of nursing evaluation before oxygen therapy are shown in Figure 3. ① Whether the patients’ consciousness, respiratory status, degree of hypoxia and airway patency are evaluated before oxygen therapy, if the evaluation items are more than 75%, it is standardized; ② Before oxygen therapy, evaluate whether the patient is at risk of hypercapnia or has hypercapnia. If the evaluation is completed, it is standardized; ③ Whether the responsible nurse correctly determines the patient’s oxygen target range based on the patient’s condition, knowing the correct range is standardized, knowing the incorrect range or not knowing the concept of oxygen target is not standardized. (2) The standardized evaluation process and standard of nursing measures in the implementation process of oxygen therapy are shown in Figure 4. ① If the correct oxygen therapy tools and oxygen flow are selected according to the patient’s condition during the implementation of oxygen therapy, it is standardized; ② If the examiner monitors that the patient’s actual blood oxygen saturation value is within the target blood oxygen saturation value range, it is standardized; ③ If the wearing of oxygen therapy tools and pipeline management meet the standard, and the humidification of oxygen therapy meets the standard, it is standardized; ④ The patients and their families are interviewed. If the patients or their families know more than 75% of the knowledge about oxygen therapy, it is standardized.
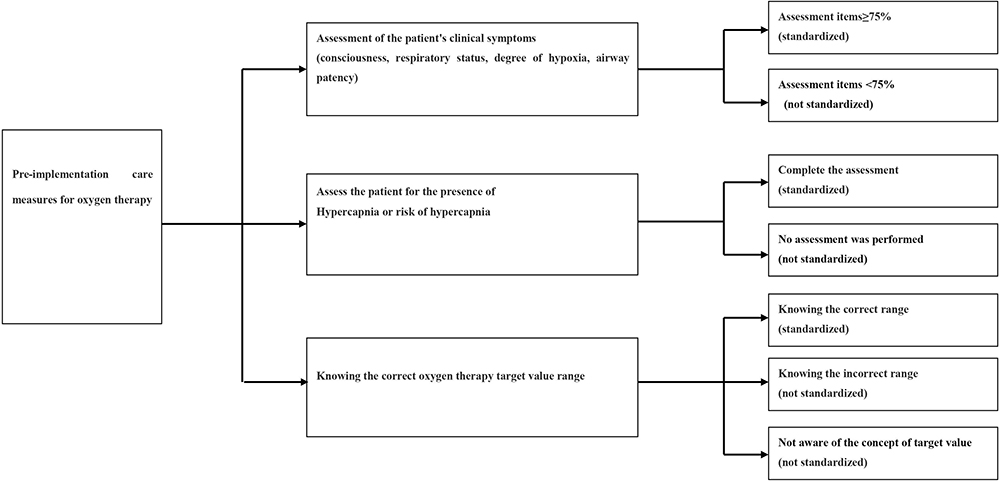 |
Figure 3 Process and criteria for evaluating the standardability of pre-implementation care measures for adult oxygen therapy. |
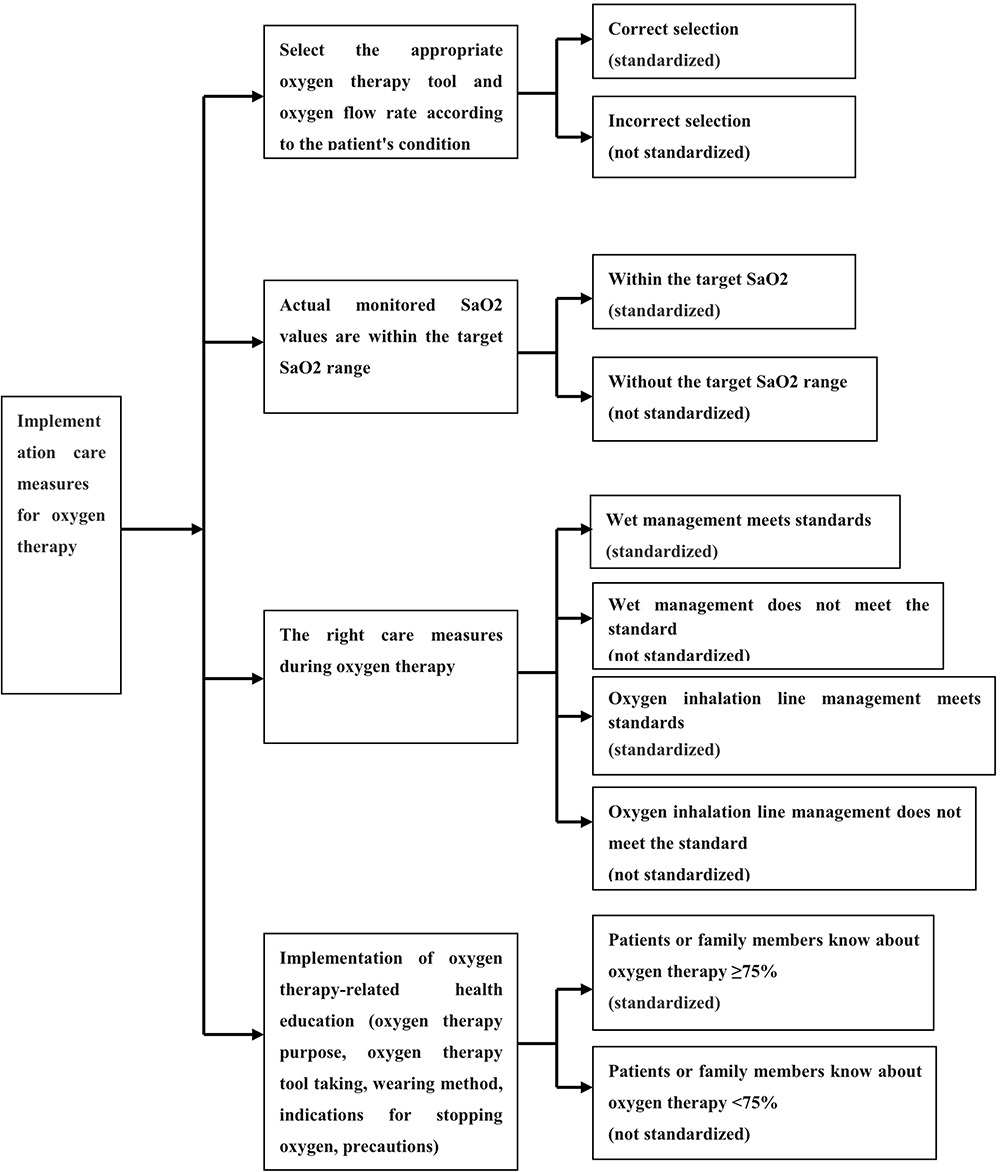 |
Figure 4 Process and criteria for evaluating the standardability of implementation care measures for adult oxygen therapy. |
Standard for Complications of Oxygen Therapy
Complications of oxygen therapy include hypercapnia and hyperoxia.13 In this study, no blood gas analysis and data collection were conducted. The oxygen saturation was monitored by the finger oxygen saturation instrument. The blood oxygen saturation value during the oxygen therapy process was used to evaluate whether the patients had hypercapnia risk or hyperoxia risk. ① Hypercapnia risk: oxygen saturation of patients with chronic obstructive pulmonary disease during oxygen therapy>92%.1,18–20 ② Hyperoxia risk: blood oxygen saturation during oxygen therapy > 98%.21–23 (PaO2 higher than 120mmHg is the diagnostic standard of hyperoxia.24,25 When SaO2 reaches 100%, PaO2 can reach 100–500 mmHg.13 When oxygen saturation of patients with normal oxygen dissociation curve is 98.5%, PaO2 is 160mmHg. In this study, blood oxygen saturation >98% was used as the standard of hyperoxia risk.
Statistical Methods
SPSS22.0 software was used for statistical analysis. Qualitative data (gender, education level and payment method of medical insurance) were described by case (%); The rationality and standardization of clinical oxygen therapy were expressed by case (%); The incidence of complications of oxygen therapy in patients in different wards were expressed by case (%); Comparison of the rationality and standardization of clinical oxygen therapy in different levels of wards and wards of different departments was expressed by the χ2 test, and P<0.05 was statistically significant. If the difference was statistically significant in wards of different disciplines, χ2 segmentation method was further used for pairwise comparison, P < 0.05 was statistically significant.
Results
General Information of Survey Subjects
From August 3 to August 15, 2020, 1703 adult patients were investigated according to the scheduled plan. Of the 1703 adult patients, 235 received adult oxygen therapy. Excluding patients who were receiving hyperbaric oxygen and mechanical ventilation and patients who had stopped oxygen therapy, 185 patients were included in this study, and the oxygen uptake rate was 10.86% (185/1703). The general information of the patients is shown in Table 1.
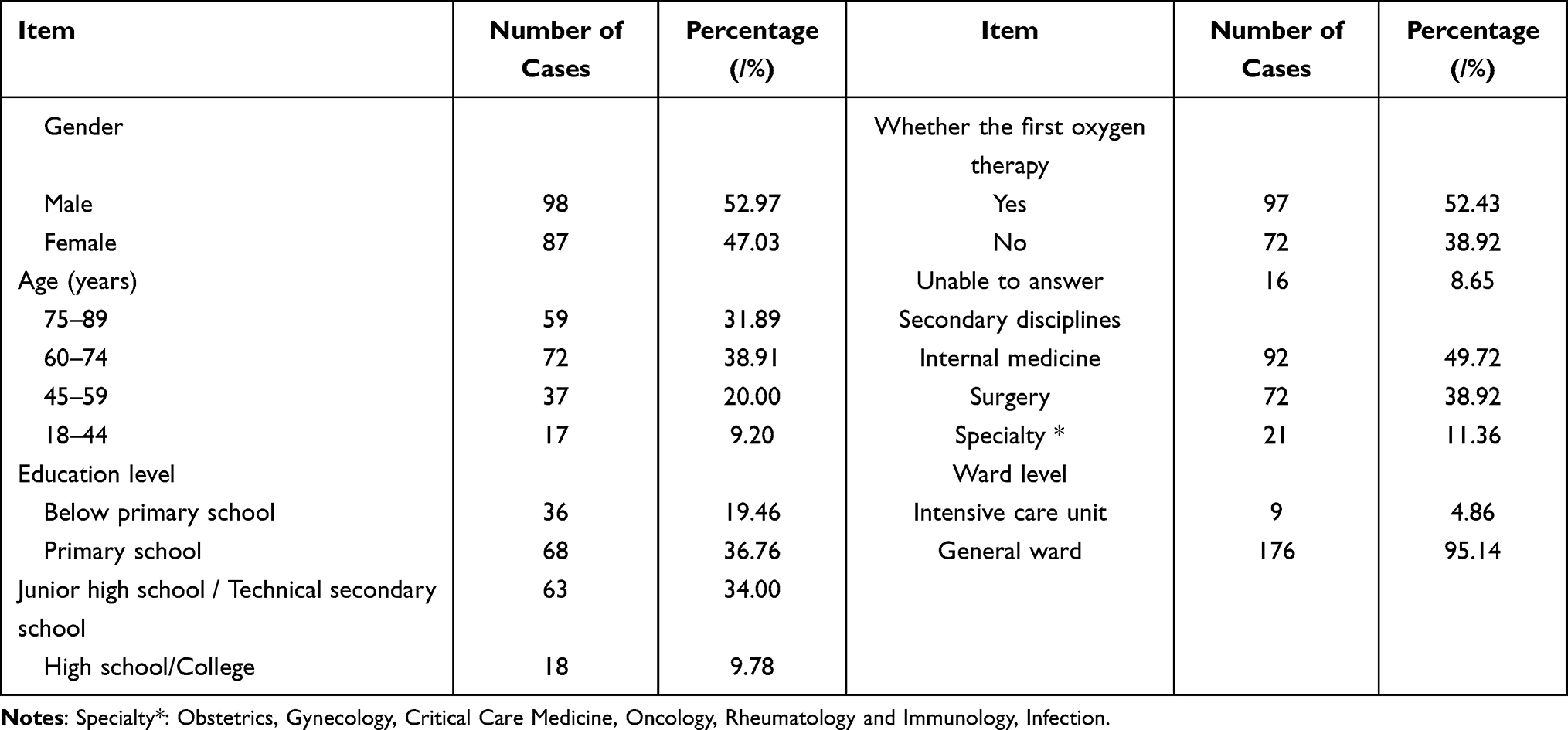 |
Table 1 General Information of Oxygen Therapy Patients [n=185, n(%)] |
Evaluation results of the Rationality of Clinical Oxygen Therapy and the Standardization of Nursing Measures
The results of the Rationality of Clinical Oxygen Therapy
The rationality rate of clinical oxygen therapy for 185 inpatients was 19.46%. See Table 2 for details.
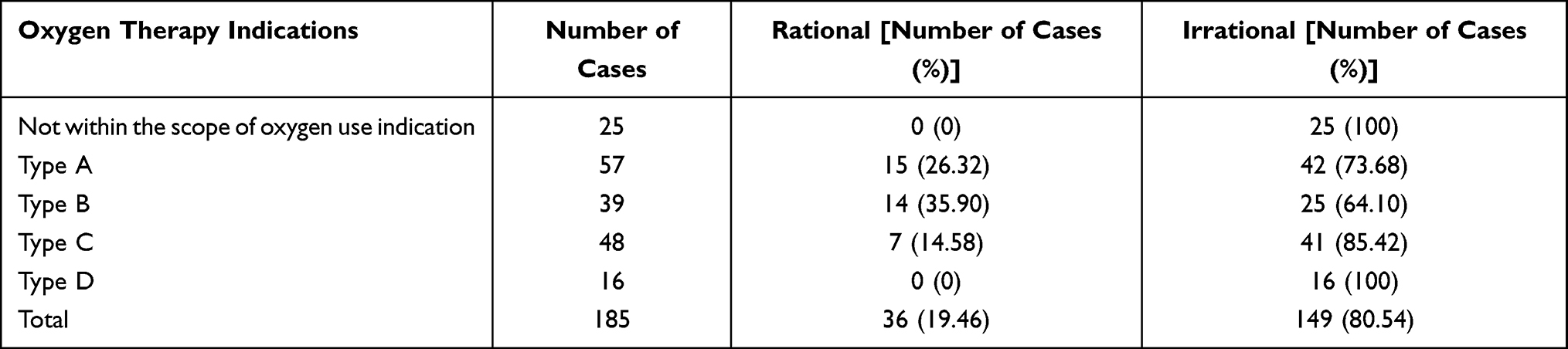 |
Table 2 Rationality Evaluation Results of Clinical Oxygen Therapy for 185 Inpatients |
The results of the the Standardization of Nursing Measures
Oxygen therapy nursing measures for 185 inpatients, combined with 7 standardized indicators, the average standardized rate was 54.52%, see Table 3.
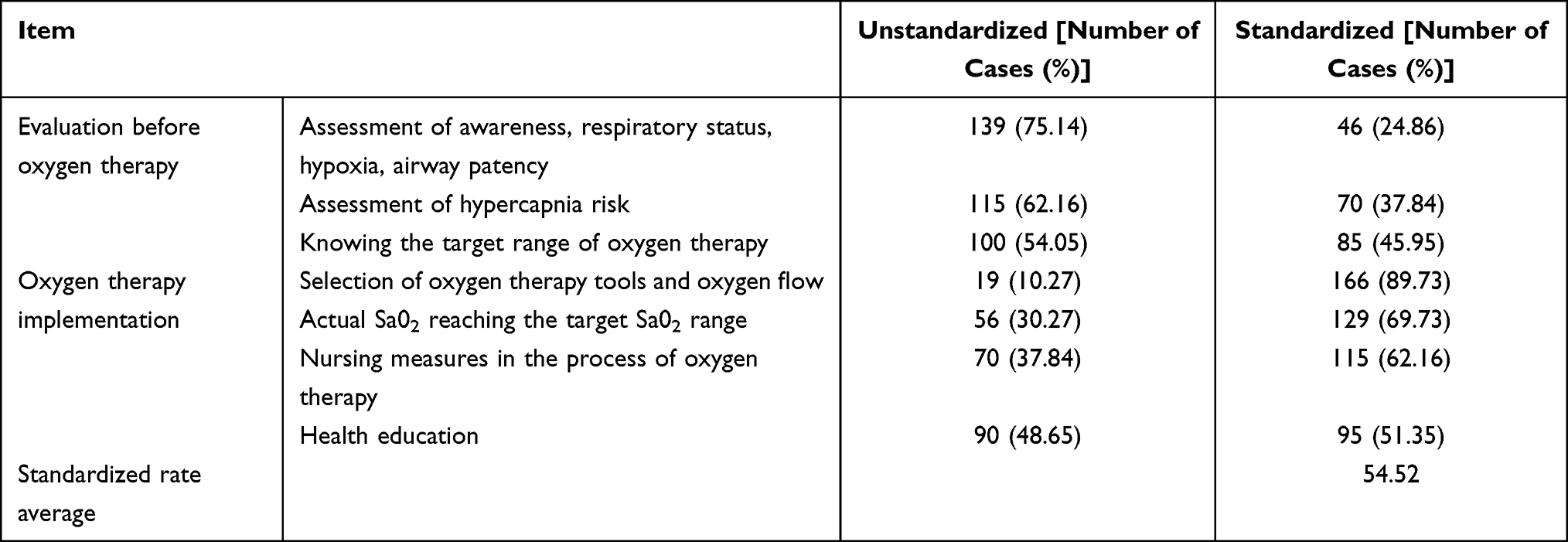 |
Table 3 Standardized Evaluation Results of Clinical Oxygen Therapy Nursing Measures for 185 Inpatients |
Comparison of the Rationality of the Implementation of Oxygen Therapy and the Standardization of Nursing Measures in Different Wards
In terms of the rationality of the implementation of clinical oxygen therapy, the rationality rate of internal medicine wards was higher than that of surgical and specialized wards. The difference between internal medicine wards and surgical wards (χ2 = 20.138, P = 0.000), and the difference between internal medicine wards and specialized wards (χ2 = 7.453, P = 0.004) were statistically significant (P < 0.05), but there was no statistical significance between surgical wards and specialized wards (χ2 = 0.020, P = 1.000). The rationality rate of general wards was higher than that of intensive care unit, but there was no statistical significance between the two (P > 0.05).
In terms of the standardization of nursing measures in the implementation of clinical oxygen therapy, the standardized rate of internal medicine wards was higher than that of surgical and specialized wards. The difference between internal medicine wards and surgical ward (χ2 = 13.141, P = 0.000), and the difference between internal medicine wards and specialized wards (χ2 = 6.592, P = 0.005) were statistically significant (P < 0.05), but there was no statistical significance between surgical wards and specialized wards (χ2 = 0.904, P = 0.460). The standardized rate of general wards was higher than that of the intensive care unit, but there was no statistical significance between the two (P > 0.05). See Table 4.
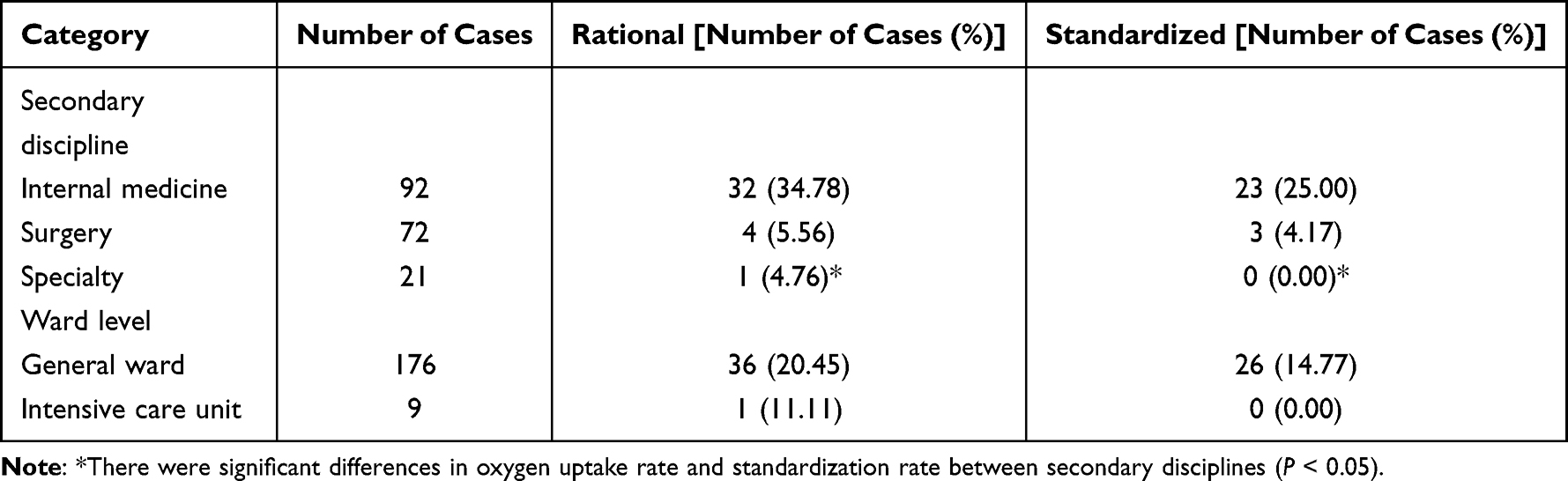 |
Table 4 Comparison of Rationality and Standardization Analysis Results of Clinical Oxygen Therapy in Patients in Different Wards |
Comparison of the Incidence of Complications of Oxygen Therapy in Patients in Different Wards
The incidence of hypercapnia risk in oxygen therapy patients in specialized and surgical wards was higher than that in internal medicine wards (χ2 = 7.801, P = 0.020), and the difference was statistically significant (P < 0.05). The incidence of hyperoxaemia risk in oxygen therapy patients in surgical and specialized wards was higher than that in internal medicine wards (χ2 = 8.083, P = 0.018), and the difference was statistically significant (P < 0.05).
The incidence of hypercapnia risk in oxygen therapy patients in intensive care units was higher than that in general wards (χ2 = 59.805, P = 0.000), which was statistically significant (P < 0.05). There was no statistical significance in the incidence of hyperoxia risk between oxygen therapy patients in intensive care units and general wards (χ2 = 1.550, P = 0.213) (P>0.05). See Table 5.
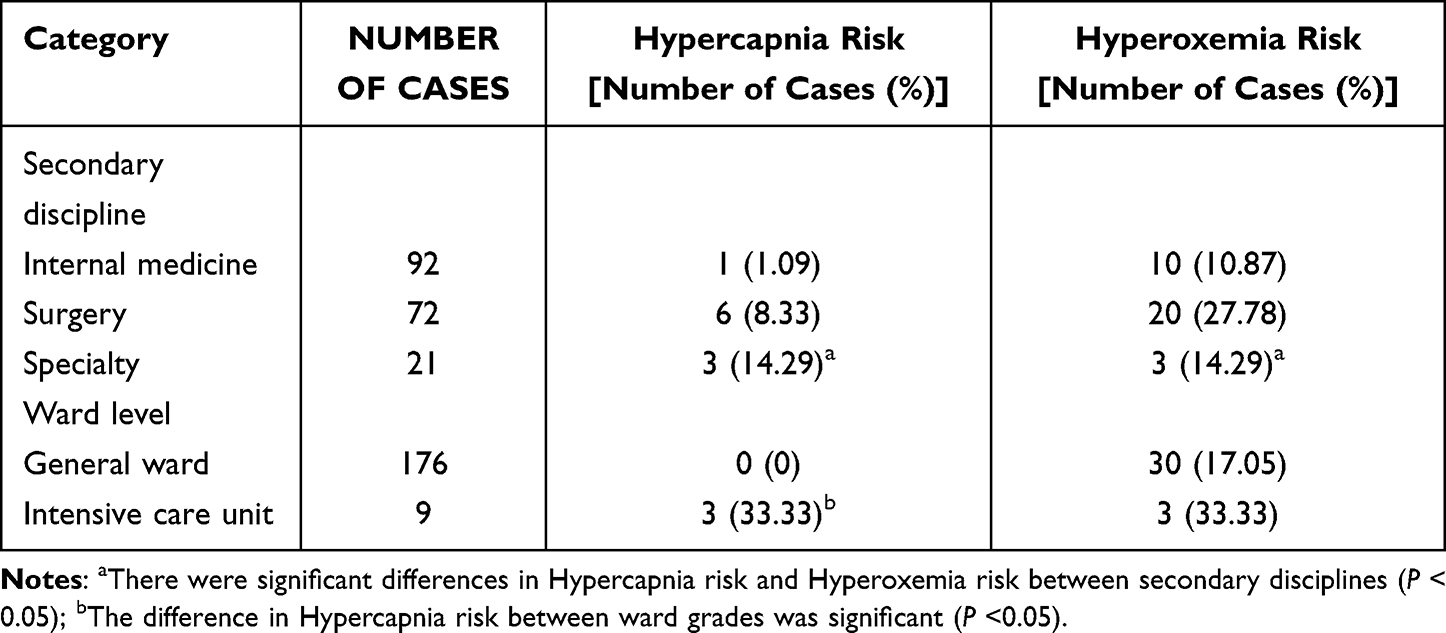 |
Table 5 Comparison of the Results of Complications in the Implementation of Oxygen Therapy in Different Wards |
Discussion
The Rationality of Oxygen Therapy Implementation and the Standard Quality of Oxygen Therapy Nursing Measures Need to Be Improved
The rationality of clinical oxygen therapy in this survey was only 19.46%, and there were many cases of random or excessive use of oxygen, which was higher than the 8% oxygen therapy rationality of Boyle et al.26 The average standardized rate of oxygen therapy nursing measures was 54.52%, which was higher than the 22.4% standardized oxygen therapy rate obtained by Zhu Yijun.27 There were many non-standard behaviors in pre-oxygen therapy evaluation, oxygen therapy target management, oxygen therapy tool use, oxygen therapy humidification effect, health education and other aspects. Oxygen therapy is the primary way to increase the oxygen content of arterial blood and correct various hypoxia, but non-standard assessment and unreasonable oxygen therapy will reduce the effect of oxygen therapy in patients, especially for patients with chronic obstructive pulmonary disease and other restrictive airway obstructions, the occurrence of hypercapnia will cause more or less adverse effects on its prognosis,28 and excessive oxygen therapy will bring irreversible adverse effects on patients.29 This survey suggests that clinical nurses do not have enough knowledge about this. Correct and standardized nursing measures during oxygen therapy are an important guarantee for the safety of oxygen therapy. Monitoring and management of oxygen therapy targets for patients is important in reducing the damage of hyperoxemia and protecting critically ill patients.13 Oxygen therapy is one of the medical activities that doctors, patients and their families participate in together. Patients and their families clearly know the purpose of oxygen therapy and the precautions in the process of oxygen therapy, which can effectively prevent the occurrence of insufficient oxygen therapy and excessive oxygen therapy. However, in this survey, nearly half (48.65%) of oxygen therapy patients and their families’ health education on oxygen therapy is ineffective.
Therefore, in the clinic, oxygen should be strictly managed as a drug, used in accordance with clinical symptoms and medical norms, and its efficacy should be monitored.30 Through the training of oxygen therapy knowledge for nurses, the nurses’ ability to assess the rationality and standardization of oxygen inhalation therapy can be improved, and we should enhance nurses’ awareness of health education, implement oxygen therapy target management and implement correct nursing measures to ensure the effectiveness and safety of oxygen therapy for patients.
Comparison of Differences in the Rationality of Oxygen Therapy Implementation and the Standardization of Nursing Measures in Different Departments
A comparison of the rationality of oxygen therapy implementation and the standardization of nursing measures in different departments shows that the clinical oxygen therapy implementation of internal medicine system, surgical system and specialty system is different, which is statistically significant. The reason may be that different departments pay different attention to oxygen therapy as a medical behavior, and the daily training and management and control are different, which leads to differences in nurses’ oxygen therapy nursing behavior. This also suggests that the importance of training nurses on oxygen therapy-related knowledge and strict oxygen therapy quality management will enable patients to obtain more reasonable and standardized oxygen therapy care. There was no difference in the rationality of oxygen therapy and the standardization of nursing measures between general wards and intensive care units in this study. The reason may be that most of the intensive care patients in the investigated hospital were mechanically ventilated patients, and the number of patients performing adult oxygen inhalation care was small. This survey is a cross-sectional survey. There were only 9 patients who met the inclusion and exclusion criteria, and only 1 patient met the rational standards. There was no difference through statistics. The result of this comparison was of little significance due to the small amount of data.
The Results of Oxygen Therapy Complications are Positively Correlated with the Data of the Rationality of Oxygen Therapy Implementation and the Standardization of Nursing Measures
Comparing the data of patients at risk of hypercapnia and patients at risk of hyperoxaemia during the implementation of oxygen therapy in different departments, it shows that there are differences in the incidence of clinical oxygen therapy complications in the internal medicine system, the surgical system and the specialized system, which is statistically significant. The results of complications are positively correlated with the data of the rationality of oxygen therapy implementation and the standardization of nursing measures in the internal medicine system, the surgical system and the specialized system, indicating that the rationality of oxygen therapy and the implementation of standardized nursing measures will directly affect the occurrence of complications of oxygen therapy. It shows that it is of great significance for clinical medical staff to promote the standardized management of oxygen therapy for the safety of patients.
The “Oxygen Therapy Standard” Has Not Been Effectively Implemented in Clinical Work
Oxygen inhalation technology has long been used as a nursing operation item to train and manage nurses.31,32 The focus of nursing operation items is mainly on the standard of operation behavior. In this survey, the correct rate of nurses’ selection of oxygen therapy tools and flow rate reached 89.73%, which also reflects that nurses have a high degree of mastery of this operation. The “Adult Oxygen Inhalation Therapy Nursing” of the Chinese Nursing Society has comprehensively standardized the six major aspects of oxygen therapy care: preoperational assessment, selection of oxygen supply mode, implementation, oxygen therapy humidification, observation and detection during oxygen therapy, and health education. This standard indicates that appropriate oxygen therapy can be given only when the patient has hypoxemia. The data of this study suggest that nurses have major deficiencies in pre-oxygen therapy operation, observation and testing during oxygen therapy, and oxygen therapy health education, indicating that the “oxygen therapy standard” has not received sufficient attention in medical institutions. There is no good application and promotion in clinical practice.
The Nursing Quality Management of Oxygen Therapy Lacks a Unified Evaluation Standard
Nursing quality evaluation standard is an important tool to carry out nursing quality management and control. It is very important to adopt standardized and homogeneous oxygen therapy evaluation standard to improve the quality of oxygen inhalation nursing. At present, there is no unified management evaluation standard in some hospitals. Taking Sichuan Province as an example, the “Sichuan Hospital Nursing Quality Management Evaluation Standard” published by the Sichuan Nursing Quality Control Center is a code of conduct for nursing staff and a work guide for nursing managers.33,34 The 2014 edition includes 45 quality standards, and the 2018 edition includes 24 quality standards, none of which includes oxygen inhalation therapy items. The results of this study showed that the average standardized rate of oxygen therapy nursing measures for 185 inpatients was 54.52%. The incomplete quality management evaluation standards for the implementation of oxygen therapy will inevitably lead to the lack of attention and standardization of the management and control of this index by some hospitals and nursing managers. It is suggested that after the promulgation of the group standard of “Adult Oxygen Inhalation Therapy Nursing”, hospital management departments in various regions should formulate corresponding management norms and quality evaluation standards according to the standard, so as to guide clinical behavior and promote the implementation of the standard in practice, strengthen the training and update of oxygen therapy knowledge of nursing staff, and normalize the control and supervision of oxygen therapy nursing behavior. Scientific management of clinical oxygen therapy will play a positive role in promoting the further standardization of oxygen therapy in China.
There were some limitations of this study. Firstly, the sample size is relatively small. Secondly, this study collected information through questionnaires, subjective influence may lead to bias.Thirdly, the influence of doctor’s orders on oxygen therapy nursing behavior is not involved in the survey.
Conclusions
There is a big gap between clinical oxygen therapy nursing practice and the requirements of “oxygen therapy standards”, suggesting that hospital managers should pay attention to the training and implementation of standards, and formulate corresponding quality control measures to provide evidence and guidance for promoting standardized and safe oxygen therapy and ensure the safety of patients and practitioners.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval of Studies and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Leshan people’s Hospital. All patients signed an informed consent form for inclusion in the study.
Acknowledgments
We would like to express our gratitude to all those who helped us during the writing of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Leshan City Science and Technology Plan Project (Grant number 20ZD096).
Disclosure
The authors had no personal, financial, commercial or academic conflicts of interest in this work.
References
1. Yue WG, Zhang ZG, Zhang CY, et al. Meta-analysis of the effect of nasal high-flow oxygen therapy on respiratory failure. Chine Critical Care Med. 2017;29(5):396–402. doi:10.3760/cma.j.issn.2095-4352.2017.05.003
2. Smbl H, Yzer AH. Estimating the value of the volume from acceleration on the diaphragm movements during breathing. J Eng Sci Technol. 2018;13(5):1205–1221.
3. Nagata K, Horie T, Chohnabayashi N, et al. Home High-Flow Nasal Cannula Oxygen Therapy for Stable Hypercapnic COPD: a Randomized Clinical Trial. Am J Respir Crit Care Med. 2022;206(11):1326–1335. doi:10.1164/rccm.202201-0199OC
4. American Association for Respiratory Care. AARC (American Association for Respiratory Care) clinical practice guideline. Oxygen therapy in the acute care hospital. Respir Care. 1991;36(12):1410–1413.
5. Buckley T, Dudley J, Eberhart M. AARC clinical practice guideline. Oxygen therapy in the home or extended care facility. American Association for Respiratory Care. Respir Care. 1992;37(8):918–922.
6. O’Driscoll BR, Howard LS, Davison AG, et al. BTS guideline for emergency oxygen use in adults patients. Thorax. 2008;63(6):1–68. doi:10.1136/thx.2007.086215
7. Balfour-Lynn IM, Field DJ, Gringras P, et al. BTS guidelines for home oxygen in children. Thorax. 2009;64:1–26. doi:10.1136/thx.2009.116020
8. O’Driscoll BR, Howard LS, Earis J, et al. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72:1–90. doi:10.1136/thoraxjnl-2016-209170
9. Neves JT, Lobão MJ; Grupo de trabalho EMO. Oxygen therapy multicentric study: a nationwide audit to oxygen therapy procedures in internal medicine wards. Rev Port Pneumol. 2012;18(2):8085.
10. Zhu YJ, Zhou CH, Yiping H, et al. Investigation on the rationality and standardization of clinical oxygen therapy orders in a general hospital in Shanghai. Chine J General Practitioners. 2020;19(2):117–121.
11. Cao J, Dong LX, Chen BY. Avoid hyperoxia hazards and standardize target oxygen therapy. Chine J Tuberculosis Respir. 2015;38(8):629–631.
12. Chen BY, Xie LX, He QY. Promoting standardization of clinical oxygen therapy in China. Chin Med J. 2017;97(20):1523–1525. doi:10.3760/cma.j.issn.0376-2491.2017.20.002
13. Ni Z, Qin H, Li J, et al. Expert consensus on management of high-flow nasal canula oxygen therapy in patients with coronavirus disease 2019. Chin J Respir Crit Care Med. 2020;19(2):110–115.
14. Xie LX; Respiratory Critical Care Group of Respiratory Branch of Chinese Medical Association, Critical Care Medicine Committee of Respiratory Branch of Chinese Medical Doctor Association. Expert consensus of high-flow nasal cannula oxygen therapy on clinical application regularity. Chin J Tuberc Respir Dis. 2019;42(2):83–91.
15. Zhang S. Group Standard T/CNAS08-2019 Adult Oxygen Inhalation Therapy Nursing [S]. Chine Nursing Assoc. 2019;1–7.
16. Liu TT, Feng Z, He Q, et al. Comparison of the therapeutic effects of nasal high-flow oxygen therapy and non-invasive positive pressure ventilation on postoperative hypoxemia. Chine J Phys. 2018;20(2):220–223.
17. Tang DJ, Xue XM, He B, et al. The application progress of nasal high-flow humidification oxygen therapy in patients with hypercapnic respiratory failure. Int J Anesthesiol Resuscitation. 2020;41(1):79–82.
18. Vestbo J, Hurd DD, Rodriguez-Roisin R. 慢性阻塞性肺疾病全球创议(2011年修订版)概述 [An overview of Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (GOLD) (revised 2011)]. Zhonghua Yi Xue Za Zhi. 2012;92(14)937–938. Chinese.
19. Beasley R, Patel M, Perrin K, et al. High-concentration oxygen therapy in COPD. Lancet. 2011;378(9795):969–970. doi:10.1016/S0140-6736(11)61431-1
20. Fan CH, Chen QJ. Oxygen therapy in acute exacerbation of chronic obstructive pulmonary disease. Med Rev. 2012;18(15):2430–2433.
21. Sun JH, Zhao MX, Li RY, et al. Investigation and analysis of hyperoxemia in ICU patients with oxygen therapy. J Nursing Sci. 2020;35(22):8–10.
22. Chen BY, He QY. The standardization of clinical oxygen therapy in China urgently needs to be promoted. J Clin Internal Med. 2019;36(01):1–2.
23. Guo HL, Sun DD, Long Y. Research progress of hyperoxemia in critically ill patients. Chine J Practical Internal Med. 2017;37(02):155–158.
24. Martin DS, Grocott MP. Oxygen therapy in critical illness: precise control of arterial oxygenation and permissive hypoxemia. Crit Care Med. 2013;41(2):423–432. doi:10.1097/CCM.0b013e31826a44f6
25. de Graaff AE, Dongelmans DA, Binnekade JM, et al. Clinicians’ response to hyperoxia in ventilated patients in a Dutch ICU depends on the level of FiO2. Intensive Care Med. 2011;37(1):46–51. doi:10.1007/s00134-010-2025-z
26. Boyle M, Wong J. Prescribing oxygen therapy. An audit of oxygen prescribing practices on medical wards at North Shore Hospital, Auckland, New Zealand. N Z Med J. 2006;119(1238):U2080.
27. Yijun Z. Investigation on the Implementation of Clinical Oxygen Therapy in a General Hospital in Shanghai. Naval Medical University; 2019.
28. Kallet RH, Branson RD. Should oxygen therapy be tightly regulated to minimize hyperoxia in critically Ill patients? Respir Care. 2016;61(6):801–817. doi:10.4187/respcare.04933
29. Cao J, Liu D. The damage of hyperoxia to the body and its mechanism. Chin Med J. 2017;97(20):1537–1539. doi:10.3760/cma.j.issn.0376-2491.2017.20.007
30. Buckley T, Dudley J, Eberhart M. AARC clinical practice guideline. Oxygen therapy in the home or alternate site health care facility-2007 revision & update. Respir Care. 2007;52(8):1063–1068.
31. Wang LD. Clinical Technical Operation Standard. Nursing Volume [M]. People’s Military Medical Publishing House; 2006:49–50.
32. Zhang CF, Ren JK. Guidance of 50 Assessments for Nurse Post Operation Training [M]. People’s Military Medical Publishing House; 2008:39–42.
33. Wen XX. Evaluation Standards for Nursing Quality Management in Sichuan Province (Trial)-2014 Edition [M]. Southwest Jiaotong University Press; 2014:4–87.
34. Wen XX. Evaluation Standards for Nursing Quality Management in Sichuan Province (Revised)-2018 Edition [M]. Sichuan Nursing Quality Control Center; 2018:3–41.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.