Back to Journals » Patient Preference and Adherence » Volume 20
Investigating the Risk Factors for Medication Nonadherence in Myasthenia Gravis Patients: Establishing a Nomogram Model
Authors Liu C, Ning S, Lu P, Jia W, Zhang X, Qi G
Received 2 April 2026
Accepted for publication 17 June 2026
Published 9 July 2026 Volume 2026:20 614156
DOI https://doi.org/10.2147/PPA.S614156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Chaoying Liu,1– 3 Simei Ning,1 Ping Lu,1,2 Wenli Jia,1 Xiaohe Zhang,1– 3 Guoyan Qi1– 3
1Treatment Center of Myasthenia Gravis, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, People’s Republic of China; 2Hebei Provincial Key Laboratory of Myasthenia Gravis, Shijiazhuang, Hebei, People’s Republic of China; 3Hebei Provincial Clinical Research Center for Myasthenia Gravis, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Guoyan Qi, Email [email protected]
Objective: Many studies have shown that MG patients often show poor adherence to their medications. Poor adherence may affect disease control, and also put a heavy burden on patients’ physical functions and medical costs. Therefore, this study aimed to develop and verify a nomogram for predicting medication adherence in MG patients.
Methods: We prospectively reviewed clinical information, demographic data, and medication adherence records for MG patients at Shijiazhuang People’s Hospital from January to December 2025. Logistic regression models were used to analyse risk factors related to medication nonadherence among MG patients; based on this analysis, we constructed a nomogram. Internal validation involved the Bootstrap method, while discrimination and accuracy of the nomogram were evaluated through the C-index, area under the receiver operating characteristic (ROC) curve (AUC), and calibration curves. Potential clinical use was confirmed by decision curve analysis (DCA) and clinical impact curves.
Results: Our study included 376 patients; 194 (51.60%) had poor compliance. There were 263 MG patients in the training cohort, of which 136 (51.71%) had poor compliance. We included five factors in our model: disease recurrence, insurance type, BMQ necessity, BIPQ cognition, and BIPQ emotion. Our model showed an area under the ROC curve of 0.94 (95% CI: 0.91– 0.97), with a sensitivity of 87.5% and specificity of 85.8%. Additionally, DCA and clinical impact curves confirmed the effectiveness of the developed model for predicting medication adherence in MG patients.
Conclusion: A successful development and validation of a decision curve model based on five risk factors was achieved, which can be utilised for the home management of MG patients.
Keywords: myasthenia gravis, nomogram, clinical prediction model, medication adherence
Background
Myasthenia gravis (MG) is a chronic autoimmune disorder of the neuromuscular junction characterized by fluctuating muscle weakness and fatigability. It is primarily mediated by autoantibodies against the acetylcholine receptor (AChR), muscle-specific kinase (MuSK), or other proteins associated with AChR function at the postsynaptic membrane.1 MG is a chronic illness that frequently necessitates the long-term use of corticosteroids and immunosuppressants in order to control symptoms.2 Consequently, treatment adherence emerges as a critical factor influencing disease management and patient prognosis.
Medication compliance means the degree to which patients take medicine according to the dosage, frequency, and duration prescribed by doctors.3 Studies have shown that low compliance is one of the most important reasons for poor chronic disease management, which leads to poor disease control, increased risk of recurrence, and great waste in the health care economy.4 Patients with MG may reduce or interrupt medication without prior consultation because they are worried about the side effects of drugs, lack of knowledge about the disease, a complicated drug regimen, and insufficient communication between doctors and patients.5 It has been reported that non-adherence is relatively common among patients with MG (38%-65%), which increases the risk of relapse, hospitalization, and crisis.5–7 This contributes to increased healthcare costs.
Although several studies have examined medication adherence in patients with MG and its related factors, most were limited to descriptive research or univariate analysis.5,6,8 Prospective cohort-based models for predicting poor medication adherence are still lacking. In clinical practice, early identification of patients at high risk for poor adherence may allow timely and targeted interventions. This may help reduce relapse and myasthenic crisis.
In recent years, clinical prediction models based on methods such as logistic regression have been widely used in the management of chronic neurological diseases. These models combine multidimensional variables and generate quantitative tools for clinical decision-making.7
Therefore, in this prospective cohort study, we systematically identified factors associated with medication adherence in patients with MG from both physiological and psychological perspectives. We also built a predictive model for poor adherence to prescribed medications. Such a prediction tool could facilitate the early detection of at-risk patients and aid patient-tailored medication management.
Methods
Study Design
This was a prospective cross-sectional study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Shijiazhuang People’s Hospital (2025143).
Participants
Inclusion Criteria
(1) confirmed diagnosis of MG;9 (2) age ≥18 years; (3) receiving medication for MG at discharge; and (4) voluntary participation and provision of written informed consent.
Exclusion Criteria
(1) Patients with severe cognitive impairment unable to complete questionnaires; (2) Patients with other concurrent neurological disorders affecting adherence assessment; (3) Patients with incomplete medical records.
Sample Size
A total of 376 adult patients with MG were selected from the Shijiazhuang People’s Hospital from January 2025 to December 2025.
According to the sample size estimation method for logistic regression analysis, the sample size should be 10–15 times the number of independent variables, accounting for a 10% non-response rate.10 This study encompassed 23 predictive factors. Participants were randomly allocated to the model development cohort and model validation cohort in a 7:3 ratio. Ultimately, data from 376 patients who completed the questionnaire validly were collected, comprising 263 cases in the development cohort and 113 cases in the validation cohort. The study satisfied the required sample size.
Instruments
Sociodemographic Characteristics
The following demographic data were collected: sex, age, education level, employment status, and method of health insurance payment. Disease-related data were also collected, including disease duration, Myasthenia Gravis Foundation of America (MGFA) classification, thymic status, number of relapses, duration of medication use, history of myasthenic crisis, and comorbidities.
Chinese Version of the General Medication Adherence Scale (GMAS-C)
The scale was developed by Naqvi et al11 in 2018. It includes 3 dimensions and 11 items: patient behavior–related adherence (5 items), additional disease and pill burden (4 items), and cost-related adherence (2 items). Each item is scored as 0, 1, 2, or 3 for “always”, “mostly”, “sometimes”, and “never”, respectively. The total score ranges from 0 to 33. A score of 30–33 indicates high adherence, 27–29 indicates good adherence, 17–26 indicates moderate adherence, 11–16 indicates low adherence, and 0–10 indicates poor adherence.
In 2021, Wang et al12 translated the English version of the GMAS into Chinese. The Chinese version showed good reliability and validity, with an overall Cronbach’s α of 0.781 and a test–retest reliability coefficient of 0.883. Lan et al13 study found that 26.5 was the optimal cutoff score for the GMAS in patients with chronic diseases. In the present study, a GMAS score >26.5 was defined as good adherence, whereas a score ≤26.5 was defined as poor adherence.
Brief Illness Perception Questionnaire, BIPQ
The BIPQ14 was used to assess patients’ illness perceptions. The questionnaire includes three dimensions: cognitive representation, emotional representation, and illness comprehensibility. These dimensions contain 5, 2, and 1 items, respectively. Each item is scored on a scale from 0 to 10, giving a total score range of 0 to 80. Higher scores indicate more negative illness perceptions and greater perceived disease severity. Cronbach’s alpha values ≥0.70 indicate acceptable internal consistency.15 In this study, the Cronbach’s α coefficient was 0.712.
The Beliefs About Medicines Questionnaire, BMQ
The BMQ,16 originally developed and validated by Horne et al for patients with chronic diseases, was used in this study. The questionnaire includes two dimensions: necessity beliefs and concern beliefs. Each dimension contains 5 items, giving a total of 10 items. All items are scored on a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The overall medication belief score is calculated as the necessity score minus the concern score. Higher scores indicate stronger beliefs in the necessity of medication relative to concerns about it. In this study, the Cronbach’s α coefficient was 0.791.
Data Collection
Three trained interviewers with relevant experience administered the questionnaires through face-to-face interviews on the day of admission or outpatient consultation. Written informed consent was obtained before the survey. Patients completed the questionnaires independently whenever possible. If a patient was unable to do so, a researcher assisted and recorded the responses accurately according to the patient’s answers. All questionnaires were distributed and collected on-site. Questionnaires with errors, incomplete responses, or obvious response patterns were excluded. To ensure an adequate number of valid samples for the final analysis, 270 questionnaires were distributed in the modeling set, of which 263 were valid (97.41%). In the validation set, 120 questionnaires were distributed, and 113 were valid (94.16%).
Statistical Methods
Statistical analysis was performed using SPSS 24.0 and R 4.5.1. All continuous variables underwent a Shapiro‒Wilk normality test. Continuous variables conforming to a normal distribution are expressed as the means ± standard deviations, and t-tests were used for intergroup comparisons. Nonnormally distributed data are expressed as medians and interquartile ranges, and the Mann–Whitney U-test was used for intergroup comparisons. Enumeration data are expressed as frequencies and percentages, and the chi-square test or rank sum test was used for intergroup comparisons. Binary logistic regression analysis was employed for univariate and multivariate analyses of each variable to screen predictive factors for the risk of MG medication nonadherence, and nomogram models were constructed using statistically significant variables. Variables with P < 0.10 in the univariate analysis were entered into the multivariate logistic regression model. Logistic regression analysis was performed using the “glm” function in R, and the nomogram was constructed using the “lrm” and “nomogram” functions in the ”rms”package. Internal validation was performed using patient data. The internal validation of the nomogram was conducted using bootstrap resampling with 1000 repetitions. Calibration was assessed using calibration plots generated with the “calibrate” function in the rms package with 1000 bootstrap resamples, together with the Hosmer–Lemeshow goodness-of-fit test using the “hoslem.test”function in the “ResourceSelection”package. ROC curves were used to measure the discriminatory performance of the nomogram on both the training and validation sets, and the area under the curve was calculated using the “roc”function in the “pROC” package. The optimal cutoff value was determined according to the maximum Youden index using the “coords” function. DCA was further employed to assess the clinical utility of the model using the “decision_curve”function in the “rmda” package. The significance level was set at α=0.05.
Results
Patient Demographic Characteristics
This study included 376 patients, with 194 (51.60%) exhibiting poor compliance. The training cohort comprised 263 MG patients, of whom 136 (51.71%) demonstrated poor compliance, detailed results are shown in Table 1; The validation cohort included 113 patients, with 58 (51.33%) showing poor compliance. Balance testing of baseline characteristics between the training and validation cohorts revealed no statistically significant differences in any indicators between the two groups (P > 0.05), detailed results are shown in Supplementary Material 1. This indicates that patients in the training and validation cohorts exhibit good homogeneity and are suitable for analysis.
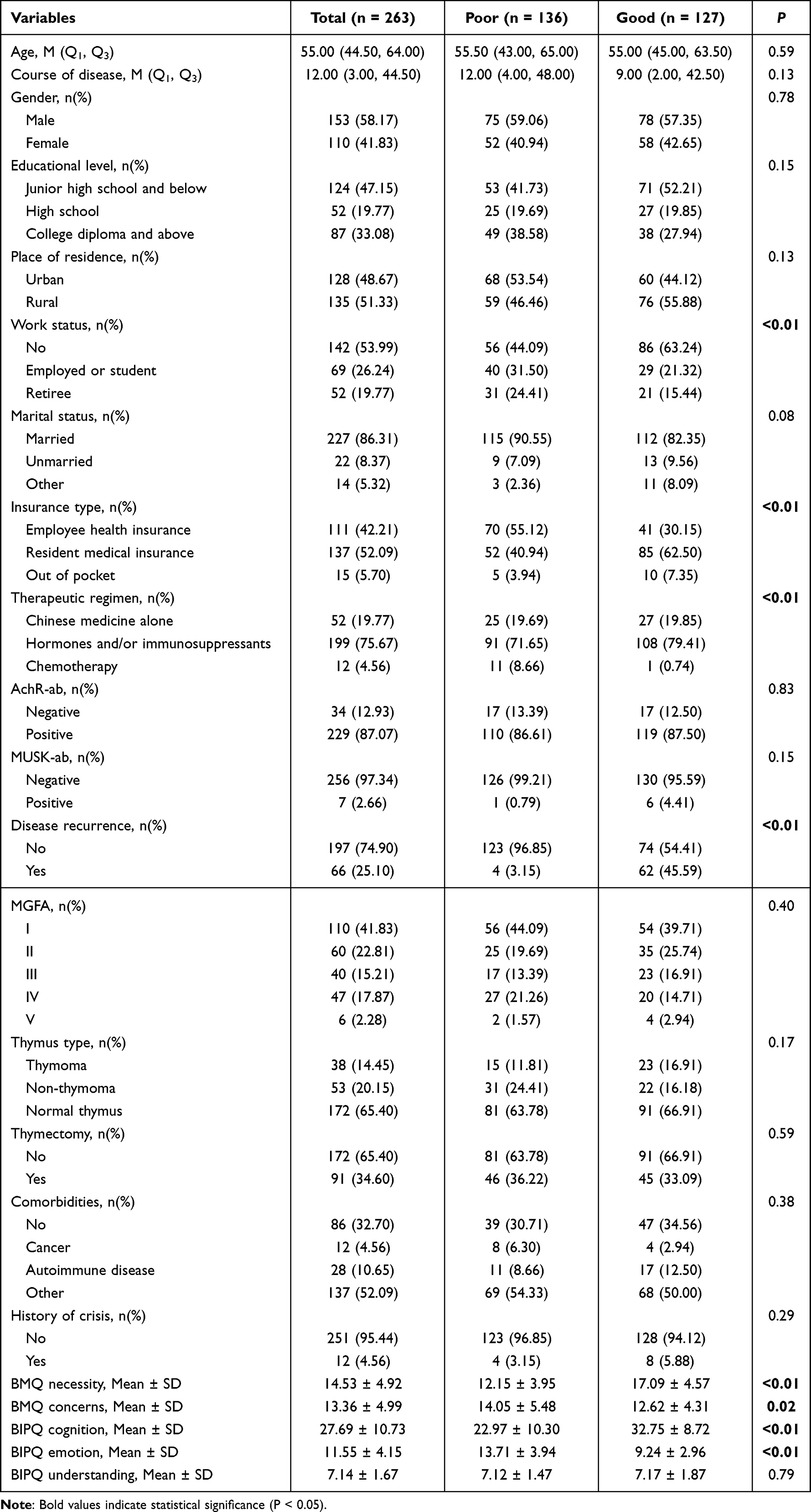 |
Table 1 The Participant Characteristics of the Training Set |
Univariate Analysis of Medication Nonadherence in MG Patients
Using medication adherence as the grouping variable, we performed univariate analyses of all demographic characteristics, clinical variables, and scale scores. To avoid excluding potentially relevant predictors, variables with P < 0.1 in the univariate analyses were entered into the multivariable analysis. The univariate analyses showed significant differences (P < 0.05) in disease recurrence, employment status, insurance type, treatment regimen, BMQ necessity, BMQ concerns, BIPQ cognition, and BIPQ emotion. Marital status was also included in the subsequent analysis because it met the threshold of P < 0.1. Detailed results are shown in Table 2.
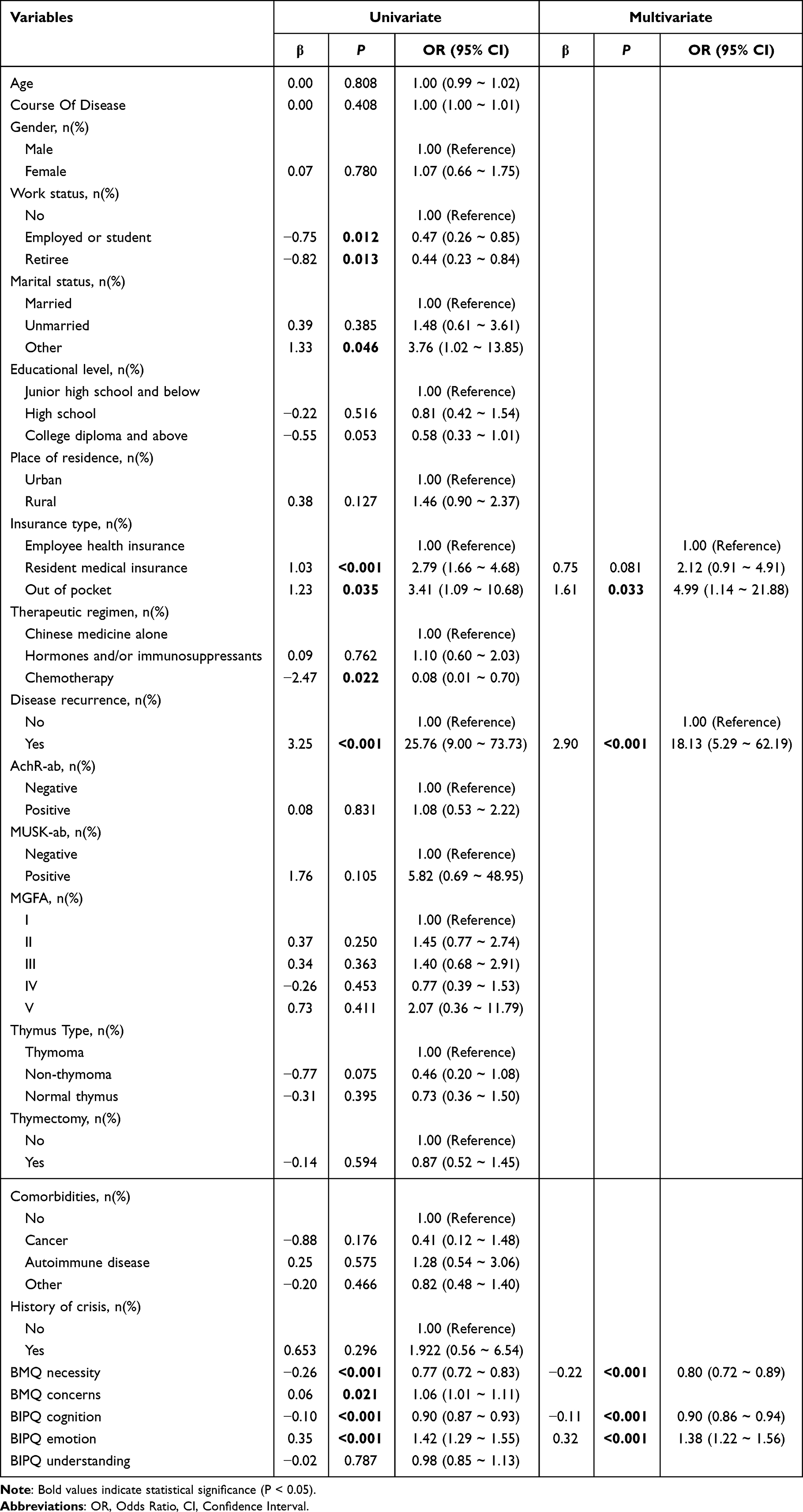 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Factors in the Training Set |
Multivariate Logistic Regression Analysis of MG Patients’ Medication Nonadherence
In order to evaluate multicollinearity between predictor variables, we conducted multicollinearity tests. Multicollinearity was considered to be present when variance inflation factors (VIFs) exceeded 10.0. Our data showed that the VIFs of the nine potential predictors ranged between 1.043 and 1.780, suggesting none of the VIFs exceeded our cut-off value, so multicollinearity did not occur. Subsequently, we carried out multivariate logistic regression analyses to examine whether the five patient characteristics (demographic, clinical, psychological, and social factors) were independent predictors of MG patients’ medication nonadherence. The results indicated that disease recurrence, insurance type, BMQ necessity, BIPQ cognition, and BIPQ emotion were significant predictors of MG patients’ medication nonadherence (P < 0.01) (Table 2).
Construction of a Risk Prediction Regression Model for Medication Nonadherence in MG Patients
Based on the multivariable analysis, a prediction model was constructed using five factors: disease recurrence, insurance type, BMQ necessity, BIPQ cognition, and BIPQ emotion, as shown in Figure 1 (nomogram). To use the nomogram, for each predictor, find the value on its line, then go straight up to the “Points” line to get points. Add all points. Then go from “Total Points” straight down to “Risk of nonadherence” to read the predicted risk.
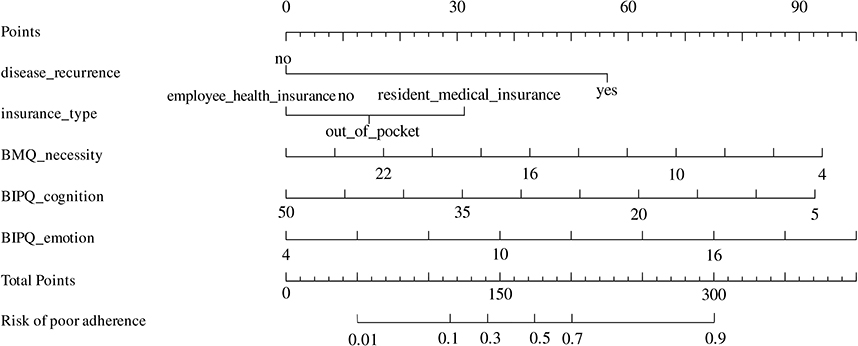 |
Figure 1 Nomogram for analgesic medication nonadherence in MG patients. |
The area under the ROC curve was 0.94 (95% CI: 0.91–0.97), with a sensitivity of 87.5% and a specificity of 85.8% (Figure 2). The calibration curve closely approximated the reference line, indicating good agreement between predicted and observed outcomes (Figure 3A). The Hosmer–Lemeshow goodness-of-fit test (χ2 = 3.303, P = 0.913) indicated a good model fit.
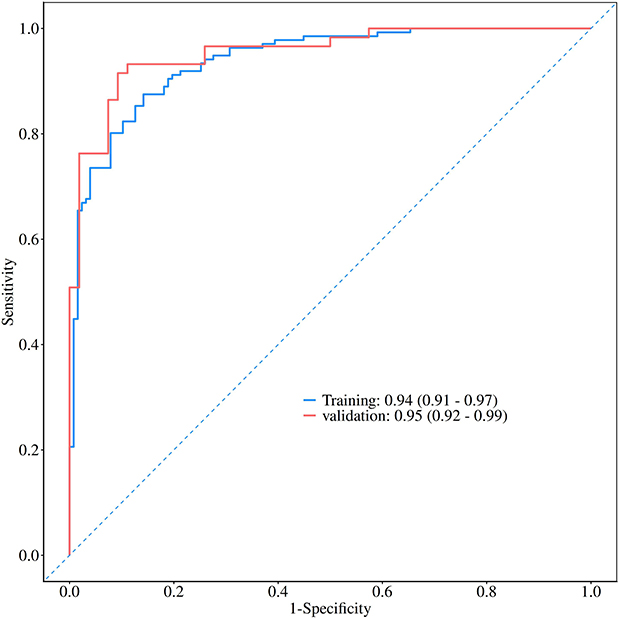 |
Figure 2 Receiver operating characteristic (ROC) curves of the predictive model to predict medication nonadherence in MG patients. |
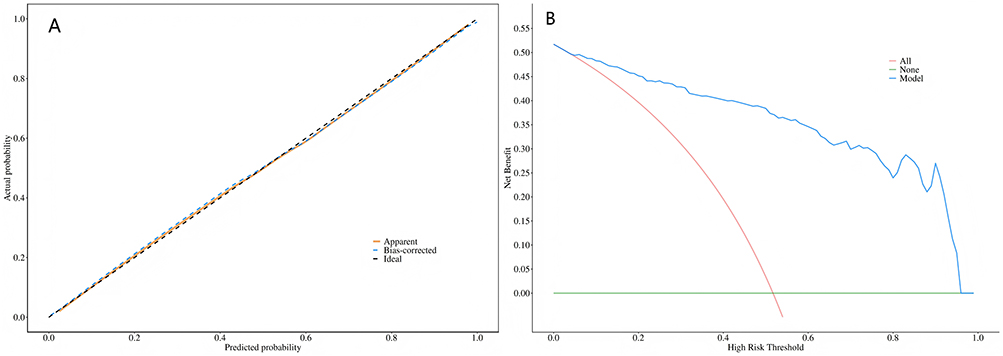 |
Figure 3 Medication nonadherence of nomogram evaluation and clinical use in MG patients. (A) Calibration plots for nomogram. (B) Decision curve analysis for the nonadherence nomogram. |
Validation of the Medication Nonadherence Prediction Model in MG Patients
The ROC analysis of prediction models was performed. For the training group and validation group, respectively, their ROC curves and AUCs were plotted. In the validation group, the AUC of the model was 0.954 (95% CI: 0.919–0.990), which had a very good discrimination effect. When the cut-off value of the prediction model in the validation group was 0.482, the sensitivity was 0.932, the specificity was 0.889, and the accuracy was 0.912. Therefore, this model has a very good discrimination effect for predicting medication nonadherence of MG patients in both the training group and the validation group, indicating that the model has relatively good reliability and can be used to predict the medication nonadherence of MG patients. The ROC curves of the training group and the validation group are shown in Figure 2. Decision curve analysis (DCA) was used to evaluate the clinical usefulness of the model in the training set. In Figure 3B, the green line represents the “intervene in none” strategy, with a net benefit of 0 across all threshold probabilities, while the red line represents the “intervene in all” strategy, whose net benefit decreases rapidly as the threshold probability increases. The blue line represents our prediction model. The model curve remained above the “intervene in none” line across a wide range of threshold probabilities, indicating that use of the model could provide a positive net benefit in clinical decision-making. This suggests that the model may help identify patients who truly need intervention more accurately, while reducing unnecessary intervention in low-risk patients.
Discussion
Medication adherence plays an important role in disease management and treatment outcomes among MG patients. Poor adherence could lead to increased frequency of relapse, reduced quality of life, higher economic burden, as well as increased psychological burden. In this study, we found that 51.7% of the patients had poor medication adherence, which suggested that there was still a large proportion of patients who had poor medication adherence. This result is similar to the result of previous studies conducted by Su et al5 Therefore, early identification of factors associated with poor medication adherence was necessary, and the development of predictive tools for individualized risk assessment was very important for designing targeted interventions to promote medication adherence. This study showed that disease recurrence, insurance type, BMQ necessity, BIPQ cognition, and BIPQ emotion were associated with medication nonadherence in patients with MG.
We found that insurance type was independently associated with medication nonadherence in MG patients. Furthermore, economic status was another important determinant of medication adherence. This finding was similar to those of previous studies.7 In China, basic medical insurance was the major way for payment and covered 67.4% of patients,17 but the financial burden still remained high in MG patients.
Myasthenic crisis usually requires hospitalization. Admission to an intensive care unit may be necessary, which will increase the medical cost.18 Novel targeted therapies for MG, such as efgartigimod,19 rozanolixizumab,20 and batoclimab,21 have shown strong efficacy. However, these treatments are also very expensive. In addition, worsening symptoms may cause patients to lose their ability to work. This can further affect family finances. Because MG is a chronic disease with fluctuating symptoms, patients may also need long-term care from family members. This increases the burden on both families and society.22
This study found that disease recurrence was an independent factor associated with medication nonadherence in patients with MG. While disease recurrence is a strong predictor of nonadherence, part of this effect may be mediated by disease severity; In response, we re-examined the data by selecting patients with generalized MG and thymoma or thymic hyperplasia, yielding a total of 78 patients for an exploratory subgroup analysis. Recurrence remained independently associated (OR = 3.55, 95% CI: 1.06–11.19), suggesting a direct psychological impact. Patients who experience recurrence may lose confidence in treatment or face more complex regimens, leading to poorer adherence.
Hou et al23 reported that, compared with persistent adherence, persistent nonadherence was associated with significantly higher risks of adverse clinical outcomes in patients with cardiovascular disease. Earla et al24 reported that nonadherent patients with multiple sclerosis had a higher relapse rate than fully adherent patients. In the present study, poor medication adherence was also closely related to disease recurrence in patients with MG. One possible explanation is that some patients do not fully understand the chronic and complex nature of MG. They may mistakenly believe that the disease can be completely cured with a single treatment regimen or medication. As a result, when symptoms improve, they may reduce or stop their medication without medical advice, which can lead to recurrence. In contrast, some patients may still experience fluctuating symptoms despite regular treatment. This may cause them to doubt the effectiveness of their medication. It may also increase anxiety and further reduce adherence. Therefore, healthcare professionals should provide early and effective interventions for patients with recurrent disease to improve medication adherence.
Medication beliefs were among the most important factors associated with adherence in this study. Binary logistic regression showed that the perceived necessity of medication was a protective factor for adherence. Patients with stronger beliefs in the necessity of medication had better adherence. In contrast, medication concerns were a risk factor for poor adherence.
In the BMQ, the concerns dimension reflects a patient’s worries about the negative effects of medication and its impact on daily life. The necessity dimension reflects a patient’s belief in the role of medication in disease control and in maintaining current and future health.25 Previous studies have shown that patients’ trust in treatment and their expectations of its benefits directly affect adherence. Positive expectations about drug efficacy are associated with better adherence.26
The participants perceived pharmacotherapy as important for managing MG, but they were also concerned about potential problems. This ambivalence could have been due to their lack of knowledge regarding MG and dissatisfaction with treatment outcomes. Due to MG being a rare disease, most patients did not have sufficient understanding of the chronicity and refractoriness of MG, which might lead them to unrealistic expectations of a complete cure. Furthermore, their hesitant attitudes towards treatments were mainly caused by concerns over adverse drug reactions, financial burden, and unsatisfactory treatment outcomes. Therefore, our study suggested there was a need for educational intervention to reinforce patients’ perception of treatment necessity and reduce their concerns. Healthcare providers may improve adherence through interventions designed to help patients feel more confident in their treatments.
According to this study’s binary logistic regression analysis, BIPQ cognition and BIPQ emotion are both independent factors affecting MG patients’ medication nonadherence; BIPQ cognition has a positive correlation with medication compliance; BIPQ emotion has a negative correlation with medication adherence. This conclusion is consistent with the research conclusions about many chronic diseases at home and abroad.
In addition, Liu et al27 found that the level of understanding of the illness had the greatest impact on the persistence of COPD patients (OR = 5.739). For patients with atrial fibrillation, there was a negative correlation between the degree of emotional reactivity and persistence measured by the BIQQ scale.28 Previous literature has indicated that patients’ levels of disease understanding and perception of treatment necessity have been associated with higher persistence rates.29 Patients with chronic disease often suffer from negative emotions due to its ongoing and unpredictable course, which may lead to lower persistence because of rejection towards treatment. Some may even stop taking medication out of unnecessary worry regarding potential side effects.30 Given that MG is a chronic disease and has the possibility of relapse, if patients have a low level of understanding or anxiety regarding their condition, they are likely to be non-adherent to their medications. Therefore, healthcare providers need to pay attention to this aspect and give individualized help to patients who are considered to be at risk of developing low persistence.
Research has shown that when the AUC value of a prediction model’s ROC curve exceeds 0.9, it indicates high accuracy; a value between 0.9 and 0.7 indicates moderate accuracy, suggesting the model’s predictive performance is satisfactory.31 This study developed a risk stratification model for predicting medication nonadherence in MG patients based on disease recurrence, BMQ necessity, BIPQ cognition, and BIPQ emotion. Both internal and external validation demonstrated excellent consistency and stability, with high predictive efficacy, effectively identifying the risk of poor medication adherence in MG patients.
Limitations
First, external validation of the model is still needed. This study included samples from only one center. Although the nomogram demonstrated a high AUC, its predictive performance may have been overestimated because of potential overfitting and the conceptual overlap between some predictors, such as medication beliefs and illness perception, and medication adherence itself. Therefore, this model should be regarded as a preliminary internally validated tool, and further external validation in independent cohorts is required before clinical application.
Secondly, machine-learning approaches might be applied to improve prediction accuracy. Moreover, this study did not fully investigate long-term changes of medication adherence and their sustained association with clinical outcomes. Therefore, future work could consider including data across longer durations of follow-up.
Moreover, the adherence measure and questionnaire mainly depend on the patients themselves, which may lead to recall bias. Adherence and psychological variables were measured simultaneously, which prevents establishing causality. In future studies, we can use more objective evaluation methods to improve prediction models.
In conclusion, randomized controlled trials should be performed to assess interventions for patients with low adherence. These trials may test if personalization according to the prediction model can improve adherence.
Conclusions
Disease recurrence, BMQ necessity, BIPQ cognition, and BIPQ emotion had a significant effect on medication nonadherence in patients with MG; the prediction model based on those factors performed well and could be used as a reference for improving medication adherence in patients with MG.
Abbreviations
MG, Myasthenia Gravis; BIPQ, Brief Illness Perception Questionnaire; OR, Odds Ratio; AUC, Area Under the Curve; ROC, Receiver Operating Characteristic; AchR-ab,anti-acetylcholine receptor antibody; MuSK-ab,anti-muscle-specific kinase receptor antibody; MGFA,Myasthenia Gravis Foundation of America; CI, Confidence interval.
Data Sharing Statement
The datasets generated and analyzed are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Shijiazhuang People’s Hospital (2025143).Each study participant provided written informed consent.
Acknowledgments
We thank the participants of the study.
Funding
This study was financially supported by grants from the Key Medical Disciplines of Hebei Province, and Key Research of Medical Science Research of Hebei Province (No. 20242107).
Disclosure
The authors declare no conflicts of interest.
References
1. Iorio R. Myasthenia gravis: the changing treatment landscape in the era of molecular therapies. Nat Rev Neurol. 2024;20(2):84–12. doi:10.1038/s41582-023-00916-w
2. Casasnovas C, Claeys KG, Vissing J. Long-term patient outcomes: the role of sustained treatment efficacy in myasthenia gravis. EMJ Neurol. 2025;13(Suppl 1);2–7. doi:10.33590/emjneurol/kilj9296
3. Abeysekara CM, Prasanthi KKN, Jeyassuthan K, et al. Review article on medication adherence. Sri Lankan J Med Admin. 2024;24(2):126–128. doi:10.4038/sljma.v24i2.5436
4. Kardas P. From non-adherence to adherence: can innovative solutions resolve a longstanding problem? Eur J Internal Med. 2024;119:6–12. doi:10.1016/j.ejim.2023.10.012
5. Su Y, Wang X, Xing Y, et al. The analysis of factors affecting medication adherence in patients with myasthenia gravis: a cross-sectional study. Therapeutic Adv Neurolog Disord. 2024;17. doi:10.1177/17562864231206877
6. Vitturi BK, Pellegrinelli A, Valerio BCO. Medication adherence in patients with myasthenia gravis in Brazil: a cross-sectional study. Acta Neurologica Belgica. 2019;120(1):83–89. doi:10.1007/s13760-019-01209-0
7. Yu J, Xie L, Chen S, et al. Social support and medication adherence among adult myasthenia gravis patients in China: the mediating role of mental health and self-efficacy. Orphanet J Rare Dis. 2024;19(1). doi:10.1186/s13023-024-03145-6
8. Ranukusuma CM, Kariasa IM, Arista L. Factors associated with medication adherence among patients with myasthenia gravis: a cross-sectional study. Jurnal Keperawatan Respati Yogyakarta. 2025;12(2):132–138. doi:10.35842/jkry.v12i2.830
9. Narayanaswami P, Sanders DB, Wolfe G, et al. International consensus guidance for management of myasthenia gravis: 2020 update. Neurology. 2021;96(3):114–122. doi:10.1212/WNL.0000000000011124
10. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
11. Naqvi AA, Hassali MA, Rizvi M, et al. Development and validation of a novel General Medication Adherence Scale (GMAS) for chronic illness patients in Pakistan. Front Pharmacol. 2018;9:1124. doi:10.3389/fphar.2018.01124
12. Wang Y, Wang X, Wang X, et al. Translation and validation of the Chinese version of the general medication adherence scale (GMAS) in patients with chronic illness. Curr Med Res Opin. 2021;37(5):829–837. doi:10.1080/03007995.2021.1901680
13. Lan KY, Zhang Q, Shen YH. Comparison of the effectiveness of GMAS, MMAS-8, and SEAMS in assessing medication adherence in patients with chronic diseases. Chin Nurs res. 2023;37(13).
14. Broadbent E, Petrie KJ, Main J, et al. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
15. Schweizer K. On the changing role of Cronbach’s α in the evaluation of the quality of a measure. Euro Jo Psycholog Assess. 2011;27:143–144. doi:10.1027/1015-5759/a000069
16. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
17. Chen J, Tian DC, Zhang C, et al. Incidence, mortality, and economic burden of myasthenia gravis in China: a nationwide population-based study. Lancet Reg Health West Pac. 2020;5:100063. doi:10.1016/j.lanwpc.2020.100063
18. Reyes Leiva D, Carbayo Á, Vesperinas Castro A, et al. Persistent symptoms, exacerbations and drug side effects despite treatment in myasthenia gravis. Eur J Neurol. 2024;32(1). doi:10.1111/ene.16463
19. Fuchs L, Shelly S, Vigiser I, et al. Real-world experience with efgartigimod in patients with myasthenia gravis. J Neurol. 2024;271(6):3462–3470. doi:10.1007/s00415-024-12293-5
20. Matic A, Alfaidi N, Bril V. An evaluation of rozanolixizumab-noli for the treatment of anti-AChR and anti-MuSK antibody-positive generalized myasthenia gravis. Expert opin biol ther. 2023;23(12):1163–1171. doi:10.1080/14712598.2023.2296126
21. Li J, Wu X, Chu T, et al. The efficacy and safety of FcRn inhibitors in patients with myasthenia gravis: a systematic review and meta-analysis. J Neurol. 2024;271(5):2298–2308. doi:10.1007/s00415-024-12247-x
22. Papus M, Dima AL, Viprey M, et al. Motivational interviewing to support medication adherence in adults with chronic conditions: systematic review of randomized controlled trials. Patient Educ Couns. 2022;105(11):3186–3203. doi:10.1016/j.pec.2022.06.013
23. Hou Q, Zhao Y, Wu Y. Medication adherence trajectories and clinical outcomes in patients with cardiovascular disease: a systematic review and meta-analysis. J Glob Health. 2025;15:4145. doi:10.7189/jogh.15.04145
24. Earla JR, Li J, Hutton GJ, et al. Association of oral disease-modifying agents and their adherence trajectories with annual relapses in multiple sclerosis. Mult Scler Relat Disord. 2024;85:105539. doi:10.1016/j.msard.2024.105539
25. Pereira MDGA, Ferreira G, Machado JC, et al. Beliefs about medicines as mediators in medication adherence in type 2 diabetes. Int J Nurs Prac. 2019;25(5):e12768. doi:10.1111/ijn.12768
26. Wang Q, Zhu R, Cao Y, et al. Sublingual immunotherapy adherence in patients with allergic rhinitis: effects of an intervention based on the information-motivation-behavioral skills model. Heliyon. 2023;9(12):e22929. doi:10.1016/j.heliyon.2023.e22929
27. Liu YR, Wang Y, Wang J, et al. Association between illness perception and adherence to inhaler therapy in elderly Chinese patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2024;21:211256139. doi:10.1177/14799731241286837
28. Miyazaki M, Nakashima A, Nakamura Y, et al. Association between medication adherence and illness perceptions in atrial fibrillation patients treated with direct oral anticoagulants: an observational cross-sectional pilot study. PLoS One. 2018;13(9):e204814. doi:10.1371/journal.pone.0204814
29. García-Gutiérrez I, Medellín DR, Noguerado-Mellado B, et al. Treatment with lipid transfer protein sublingual immunotherapy: slowing down new sensitizations. Asia Pacific Allergy. 2021;11(1):e6. doi:10.5415/apallergy.2021.11.e6
30. Patel HR. Prescription medication adherence and compliance in chronic disease patients. Int J Pharmaceut Qual Assur. 2025;16(1):69–71 doi:10.25258/ijpqa.16.1.8
31. Swets JA. Measuring the accuracy of diagnostic systems. Science. 1988;240(4857):1285–1293. doi:10.1126/science.3287615
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Construction and Validation of a Nomogram Model for Predicting Pulmonary Hypertension in Patients with Obstructive Sleep Apnea
Zhang R, Liu Z, Li R, Ai L, Li Y
Nature and Science of Sleep 2025, 17:1049-1066
Published Date: 24 May 2025