Back to Journals » Clinical Interventions in Aging » Volume 18
Investigating the Feasibility, Acceptability, and Impact of a Brief Dementia Awareness for Caregivers (DAC) Course: A Mixed Methods Study
Authors Patel R ![]() , Evans I
, Evans I ![]() , Stoner CR, Spector A
, Stoner CR, Spector A
Received 4 August 2023
Accepted for publication 5 November 2023
Published 21 November 2023 Volume 2023:18 Pages 1923—1935
DOI https://doi.org/10.2147/CIA.S429556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Ria Patel,1,* Isabelle Evans,1,* Charlotte R Stoner,2 Aimee Spector1
1Faculty of Brain Sciences, Division of Psychology and Language Sciences, Research Department of Clinical, Educational and Health Psychology, University College London, London, WC1E 6BT, UK; 2Centre for Chronic Illness and Ageing, Institute of Life Course Development, School of Human Sciences, University of Greenwich, Old Royal Naval College, London, SE10 9LS, UK
*These authors contributed equally to this work
Correspondence: Aimee Spector, Faculty of Brain Sciences, Division of Psychology and Language Sciences, Research Department of Clinical, Educational and Health Psychology, University College London, Gower Street, London, WC1E 6BT, UK, Tel +44 020 7679 1844, Email [email protected]
Aim: Informal caregivers are vital in assisting people with dementia. However, this role can significantly impact caregivers’ lives and interventions to support them are crucial. This study aimed to develop a United Kingdom version of the Dementia Awareness for Caregivers (DAC) course and to investigate the feasibility, acceptability, and impact of delivering the course online to informal dementia caregivers.
Methods: This study comprised a mixed-methods pre-post intervention parallel group design. Fifty-one informal dementia caregivers were randomized into either an experimental (receiving the DAC course) or control group (treatment as usual). Outcomes relating to perceived burden, attitude, competence, relationship quality and positive caregiving aspects were measured at baseline and follow-up, alongside statistics relating to recruitment, retention, attendance, and adherence. Semi-structured interviews were conducted to explore qualitative acceptability and impact among caregivers who completed the DAC course.
Results: The study found high retention and attendance rates with low levels of unexplained attrition. Analysis indicated positive change for four of the outcome measures in favor of the DAC course, however this was not statistically significant. Qualitative analysis generated 11 subthemes organized into four overarching main themes; “acceptability of course”, “impact of course on caregivers”, “using skills from course” and “outcome measures”.
Conclusion: Findings provide promising evidence for the feasibility, acceptability and impact of the Dementia Awareness for Caregivers course when delivered online to informal caregivers in the United Kingdom.
Keywords: dementia, informal caregivers, intervention, support, psychoeducation
Introduction
Nearly a million people have been diagnosed with dementia in the United Kingdom (UK), and this number is continuing to rise.1 Many of these individuals are cared for by informal caregivers,2 defined as unpaid family, friends, or community members. Estimates suggest that there are currently 670,000 informal dementia caregivers in the UK contributing to the equivalent economic value of £11 billion and providing over 1.34 billion hours of unpaid care.3
When provided with appropriate support, the dementia caregiving role has been found to have a positive impact.4 However, support is often not provided, and many informal dementia caregivers experience psychological concerns, high levels of stress, and a loss of independence.5,6 Nearly 50% of dementia caregivers report considerable levels of burden and roughly a third report symptoms of anxiety and depression.7,8 Furthermore, stigma regarding dementia is prevalent in the UK.9 Without support, the impact of caregiving can lead to earlier institutionalization of the individual with dementia as well as poorer outcomes for the caregiver themselves, who often become the “invisible second patient”.10
Despite this undisputedly significant role, there is currently no standardized caregiver support policy in the UK.11 There have been worldwide and UK specific initiatives to increase support for caregivers,12,13 however reviews of these have highlighted that care often falls short, with great variability in what is offered.14
Across the UK, third sector organizations such as charities and social enterprises can offer support to caregivers.15 However, not all services are easily accessible and often have long waiting lists.6 To address this, research has investigated structured interventions. Research interventions such as the Resources for Enhancing Alzheimer’s Caregiver Health (REACH) project developed in America, and the Strategies for Relatives (START) project developed in the UK, found engaging in interventions can lead to a reduction in burden, case level depression, and a higher quality of life.16,17 However, both interventions had limitations. The REACH project was six months in length, requiring caregivers to use their already limited time to be able to attend. Furthermore, caregivers had to report distress at baseline to be eligible, highlighting the intervention to be more of a reactive approach rather than preventative, with the latter potentially more beneficial for caregivers.18 Within the START project, it was noted that baseline scores of depression and anxiety were already high, increasing the likelihood of a post-test score change.19 Online interventions have also been developed and trialed among dementia caregivers, such as the iSupport program, trialed in India.20 The program comprises 23 independently accessed lessons for caregivers to complete within a three-month period. Findings reported a positive change in attitudes towards dementia, however no significant changes in burden, depression, or self-efficacy. Furthermore, the intervention was reported as having low levels of retention and adherence. A brief or single session intervention for caregivers would require reduced caregiver time-commitment and fewer professional and financial resources, making it more feasible to implement in the National Health Service (NHS).21
Responding to this need, an internationally adaptable Dementia Awareness for Caregivers (DAC) course template was designed for informal caregivers,22 to provide accessible educational information within a one-off half-day session, informed by the biopsychosocial model of dementia.23 Results from initial field tests among dementia caregivers in Brazil, India, and Tanzania indicated the DAC course was acceptable, feasible and well received.22 Whilst these initial results are promising, to establish whether the course can be utilized on a wider scale, further testing in other countries is required.
Following the COVID-19 pandemic, many services transitioned to using online means of support.24 Given the limited time and health concerns that informal dementia caregivers experience, many find attending face-to-face interventions challenging.25 Therefore, this study aimed to adapt the DAC course for online delivery to informal dementia caregivers across the UK, exploring the feasibility, acceptability, and impact of the intervention.
The key aims were to:
- Adapt the international DAC course template thus creating a UK version.
- Evaluate the feasibility of the DAC course.
- Assess and explore the acceptability and impact of the DAC course.
Method
Design
The study used a mixed-methods, pre-post intervention parallel group design with a treatment and control group. The trial was registered under identifier: NCT05887063 (ClinicalTrials.gov), and ethical approval was obtained by University College London research committee (Project ID: 22375.001). The study also complied with the Declaration of Helsinki. The treatment group engaged in the DAC course and the control group was defined as treatment as usual (TAU), meaning that participants were not offered the DAC course but could access their usual support outside of the study.
Participants
The inclusion criteria consisted of participants being over 18 years of age, an unpaid dementia caregiver, able to communicate and understand English, have access to the internet and able to attend pre-specified course dates. The exclusion criteria included professional caregivers and caregivers of those residing in dementia residential care. Participants were recruited via an online dementia research database, “Join Dementia Research” (www.joindementiaresearch.nihr.ac.uk). A study advert was placed on their website, and participants were sent opt-in emails. Study recruitment took place over three months between June and August 2022 and covered four regions across England, Wales, Scotland, and Northern Ireland. As the study was an initial feasibility trial, the sample size was not powered to detect a clinically significant effect. A sample size of 50–60 participants was selected in alignment with recommendations for feasibility studies.26,27 This sample size also allowed for possible attrition and subsequent participant ineligibility.
Procedure
All participants were provided with an information sheet which informed them of the purpose of the study. Participants then provided informed consent to engage in the study as well as publication of anonymized responses by completing an online consent form. Following this, participants were randomly allocated, on a 1:1 basis, to either the DAC or TAU group by the researchers using online randomization software. In the week prior to the delivery of the DAC, all participants were emailed and asked to complete an online questionnaire comprising demographic information and the five outcome measures. The email to the treatment group also included confirmation of the date and time of the course and a course video link.
Following course completion, participants in the treatment group were sent an email containing the relevant handouts and signposting materials. One month after the DAC course, all participants from both the TAU and treatment group completed the same five outcome measures that were completed at baseline. All those in the treatment group were also invited to and took part in a remote interview over Zoom. Interviews were conducted by the researcher who did not run the DAC course for that participant to allow them to feedback honestly. Interviews were semi-structured and lasted 30 minutes. Questions and prompts covered acceptability and impact of the course (see Appendix A). All participants had access to a debriefing form which included signposting.
Intervention
The DAC course was delivered online via video-conferencing software by one trainee clinical psychologist as a one-off, four-hour course. The course was run on three separate occasions and delivered to groups of six to ten caregivers each time. Participants that cancelled and did not attend were re-offered another course date and a fourth course was therefore run. All the courses were delivered within three months of recruitment.
The course was initially created using a four-stage iterative process using literature reviews and stakeholder involvement. Specific modules were agreed upon and from this, an international version of the course was created.22 The international template included a course guide consisting of seven sections and a 75-slide presentation. In line with the guidelines,22 the international template was adapted by the research team, creating a local version including UK specific dementia myths, facts, examples, activities, medication information and support offered across the UK. No core components of the DAC course were changed, and a member of the original DAC course development team reviewed and approved the final UK version. The course structure comprised six sections including a welcome, three course modules (what is dementia, positive engagement, caring for someone with dementia), reflections on the course and an ending (see Table 1).
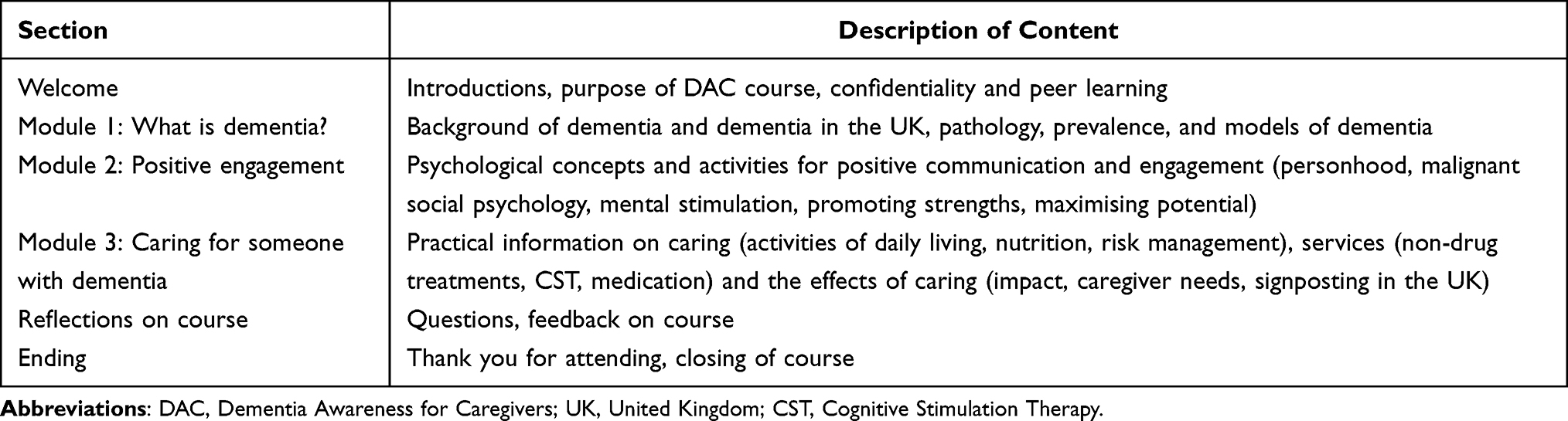 |
Table 1 Overview of Content Included in Dementia Awareness for Caregivers Course |
Six stakeholders were recruited through personal contacts to review the local version of the DAC course and provide feedback via email. Two dementia caregivers, two professionals working in dementia care and two individuals diagnosed with dementia provided feedback on the course. The stakeholders were reimbursed with a £10 voucher. All individuals felt the adaptations were applicable to the UK, found the course content relevant and felt no changes were needed.
Quantitative Analysis
Primary – Feasibility and Acceptability of the DAC Course
Recruitment and retention rates, intervention attendance and adherence, alongside outcome measure completion rates were collected. The DAC course was considered feasible if recruitment of the target sample within six months was successful, and if there was a retention rate of at least 75% of participants at follow-up. The intervention was considered acceptable if overall attendance and retention rates were over 60% and completion of the outcome measures was higher than 75%. This aligns with thresholds set in other studies.28,29
Secondary – Impact of the DAC Course on Caregivers
Although this study was not powered, all participants completed the same battery of five outcome measures at baseline and follow-up, to explore the possible impact of the intervention on these outcomes. The measures were administered via Qualtrics, an online survey platform, with participants completing them independently. Participants completed the:
- Approaches to Dementia Questionnaire (ADQ-19)30 – A 19-question survey measuring attitudes toward people with dementia. The ADQ-19 has good reliability (α=0.76 for hope, α=0.85 for person-centeredness) and validity.30
- Quality of the Caregiver Patient Relationship (QCPR): Carer version31 – a 14-item measure capturing positive and negative aspects of the caregiving relationship. Reliability and validity of the QCPR have been found to be high.31
- Short-Form Zarit Burden Interview (ZBI-12)32 – A 12-item questionnaire measuring caregiver’s perceived burden as a result of their role and has been shown to have high levels of validity and reliability.33
- Short Sense of Competence Questionnaire (SSCQ)34 – a 7-item questionnaire measuring sense of competence in their caregiving role. The SSCQ has been found to have high construct validity (r = 0.88) and reliability (α = 0.76).34
- Gain in Alzheimer’s Care Instrument (GAIN)35 – a 10-item measure covering positive aspects of caregiving in terms of the relationship with the person with dementia, self-reflection, and personal development. This tool has been found to be valid and reliable.35
Higher scores on the ADQ-19, QCPR, SSCQ and GAIN reflect positive outcomes, whereas lower scores on the ZBI-12 reflect positive outcomes. Independent samples t-tests for the five outcome measures were carried out to ascertain that the two groups were not significantly different at baseline. Descriptive statistics of demographics data were computed at baseline.
Pre-post change scores were calculated, for each participant, for each of the five outcome measures. These scores were then analyzed via a between-subjects MANOVA, comparing the two conditions.
Qualitative Analysis
Acceptability and impact were also measured through participants’ qualitative feedback, from those in the treatment group, during their semi-structured interviews following completion of the DAC course.
All 15 interviews were recorded and uploaded to Scrintal (online transcription service). Whilst Scrintal assists with transcription, it is still necessary for researchers to re-read and check the accuracy of transcription, leading to familiarization of the data. A data-driven inductive approach and a deductive a priori template of codes approach16,36 were applied to interpret and understand the data. Data were systematically coded and organized into meaningful groups. Following reviewing and refining of the coded data, visual tables were used to gain a sense of how coded extracts may be sorted into overarching and sub-themes (see Appendix B). A second researcher provided credibility checks on a random sample (20%) of the transcripts by reviewing and providing feedback on initial codes. Any disagreements were discussed and resolved, and final main and sub-themes were developed.
Results
Quantitative
Primary – Feasibility and Acceptability
Recruitment and Retention
Fifty-one participants were recruited to the trial with 26 randomized to the DAC condition and 25 randomized to the control (TAU) condition (Figure 1). All recruited participants identified as White British with a mean age of 60.56 years. The majority of participants were female (74.36.%) and a large proportion of the sample were caring for a parent (43.59%) (see Table 2 for further demographics). All participants were recruited within a 3-month period.
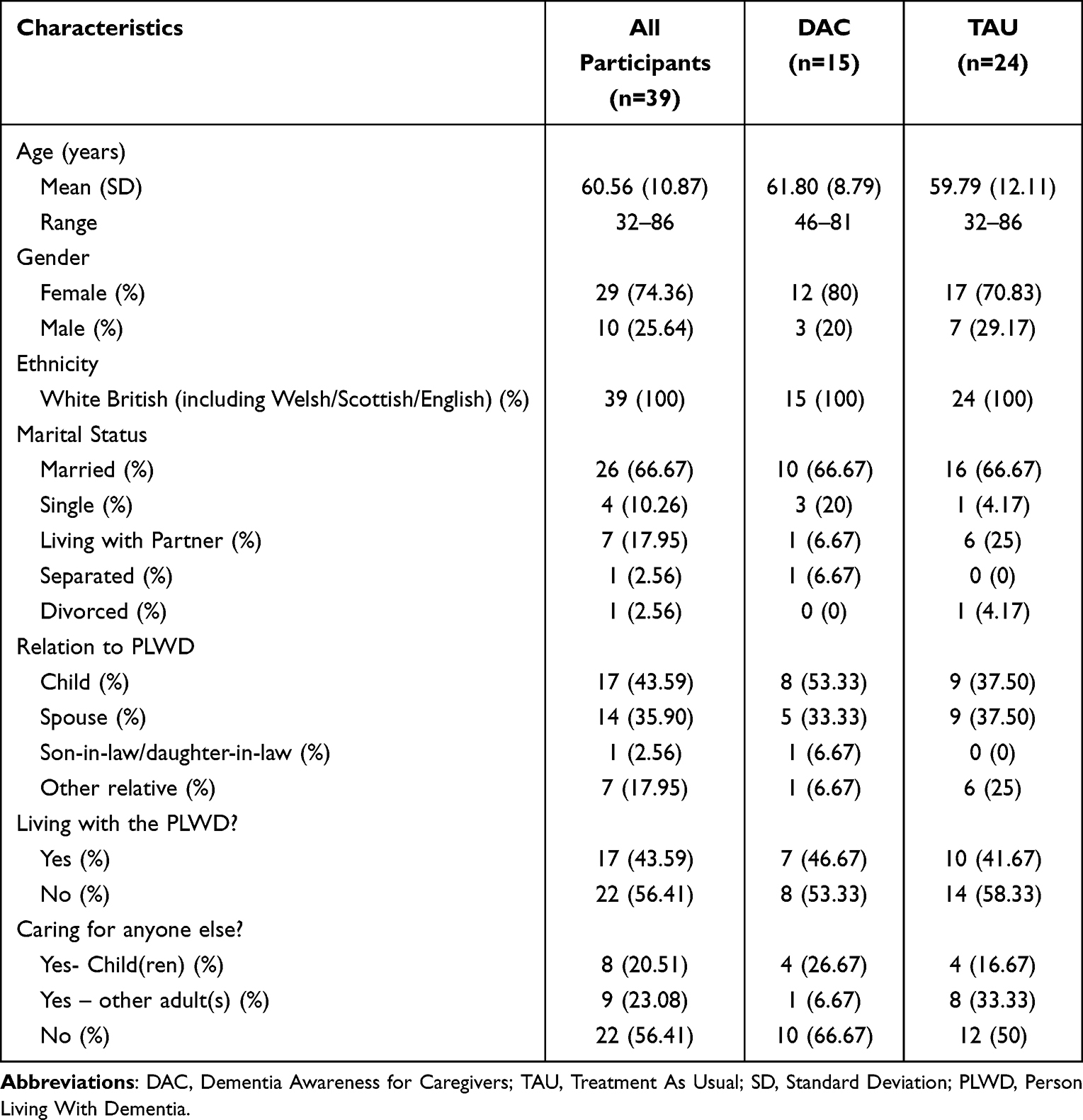 |
Table 2 Participant Demographics |
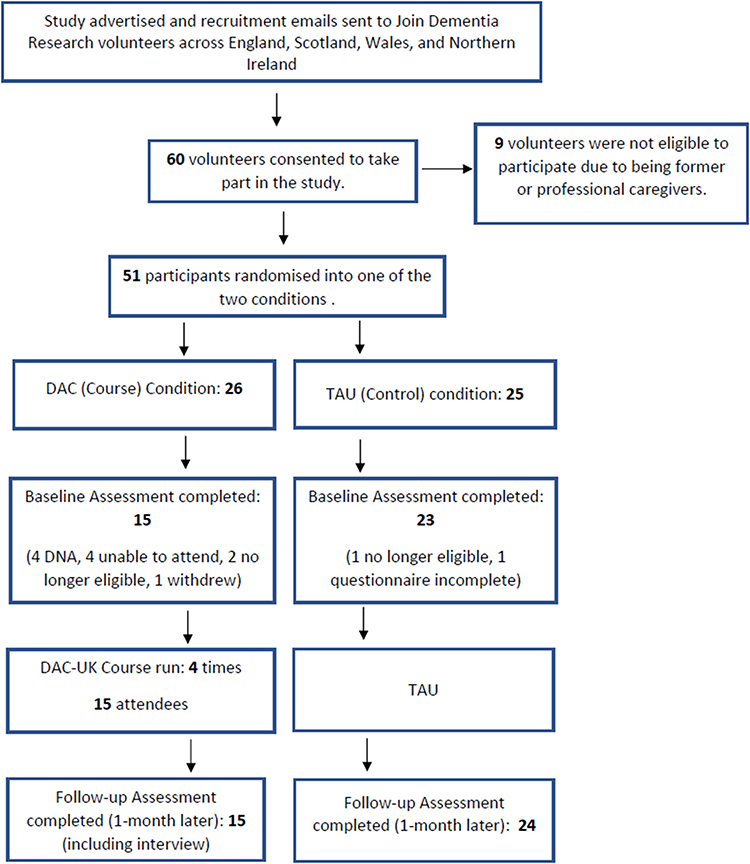 |
Figure 1 Study recruitment and retention flow-chart. Abbreviations: DAC, Dementia Awareness for Caregivers; TAU, Treatment As Usual; DNA, Did Not Attend; DAC-UK, Dementia Awareness for Caregivers-United Kingdom. |
Of the 26 participants in the DAC condition, two were no longer eligible to attend the course due to a change in circumstances (person with dementia moving into care or passing away). Another withdrew from the study citing caring needs. Of the remaining 23 participants, all were invited to attend the course, with 12 invited on two different occasions due to many being unable to attend the first date at short notice due to work changes, other commitments, or caring needs. The researchers introduced telephone calls confirming attendance and reminder emails for the remaining courses, following these cancellations. Fifteen participants (65%) attended the online course, with all these participants completing the baseline and follow-up measures. Four caregivers did not attend without providing a reason and did not respond when contacted following this. The remaining four participants did not attend but contacted the researchers prior to delivery with three referencing work commitments and the other citing health problems.
In the control group, 23 participants (92%) fully completed the baseline measures, of which all were retained at follow-up. One participant was no longer eligible as they were no longer a caregiver. One other participant did not fully complete the baseline outcome measures; however, they were retained and completed the follow-up outcome measures. Their data were included in the primary (feasibility), but not secondary (outcome measures) analysis. Overall, of the 47 participants remaining at follow-up, 39 (83%) were retained and completed follow-up assessments. Of the 39 participants, the 15 participants from the treatment group also completed interviews.
Attendance and Adherence
Fifteen of the 23 (65%) eligible participants attended the DAC course. Fourteen (93%) completed the full course and one completed the first two modules but then had to leave due to an appointment.
Feasibility of Outcome Measures
Both the SSCQ and the ADQ-19 measures had 100% completion rates with no missing data. The ZBI, QCPR and GAIN had a completion rate of 97% at baseline and 100% at follow-up.
Secondary – Outcome Measures
Analysis was conducted only for the 38 participants who completed both baseline and follow-up questionnaires.
Independent samples T-tests indicated that the average baseline scores for the five measures did not differ significantly between the groups: ADQ-19 (p = 0.225), GAIN (p = 0.431), QCPR (p = 0.527), SSCQ (p = 0.635), ZBI (p = 0.060). At baseline both groups showed reasonable positive attitudes to dementia (TAU mean = 69.96; treatment group mean = 73.33), reasonable experiences of positive aspects of caregiving (TAU mean = 27.96; treatment group mean = 26.00), a standard level of caregiver–patient relationship (TAU mean = 51.52; treatment group mean = 49.73), a reasonable level of sense of competence (TAU mean = 23.61; treatment group mean = 22.80), and high levels of burden (TAU mean = 20.57; treatment group mean = 25.40).
Using Pillai’s trace, there was no significant effect of treatment condition on the pre-post change scores for any of the five outcome measures, V = 0.07, F(5, 32) = 0.49, p = 0.783. There were non-significant positive changes in the pre-post change score means in favor of the DAC course, compared to TAU, for the ADQ-19, the GAIN, the SSCQ and the ZBI. There was no indication of positive change in the pre-post change score for the QCPR. Follow-up score means and pre-post change score means for the conditions alongside separate adjusted univariate ANOVAs are presented in Table 3.
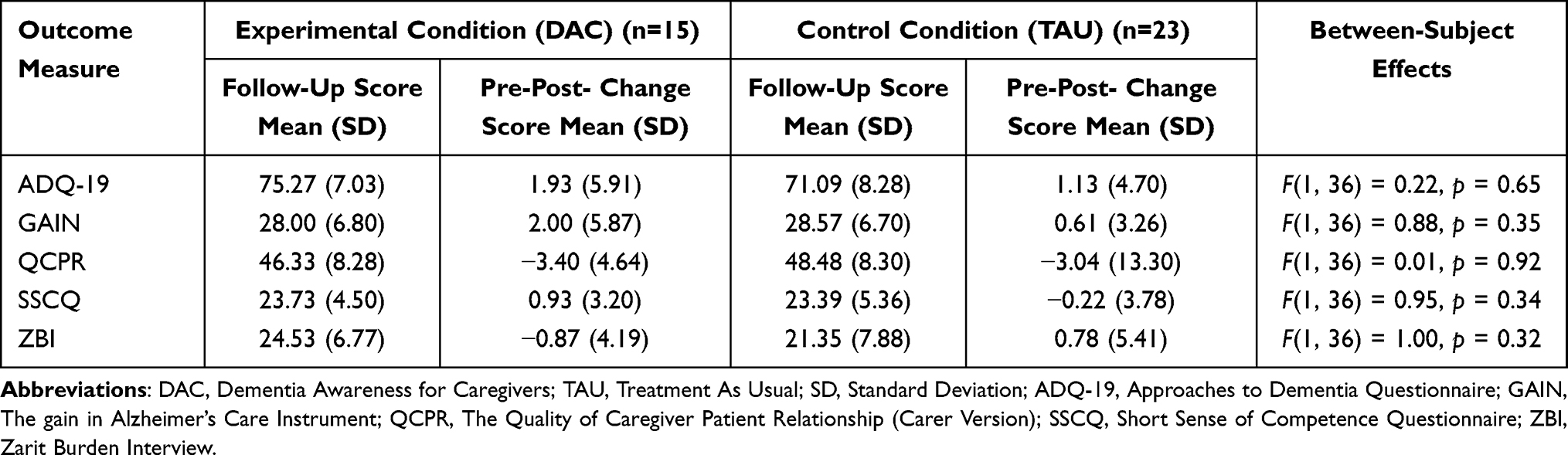 |
Table 3 Between-Subject Effects at Follow-Up |
Qualitative
The final analysis of the 15 interviews conducted generated 11 sub-themes relating to the research aims. These sub-themes were organized into four overarching main themes (see Table 4).
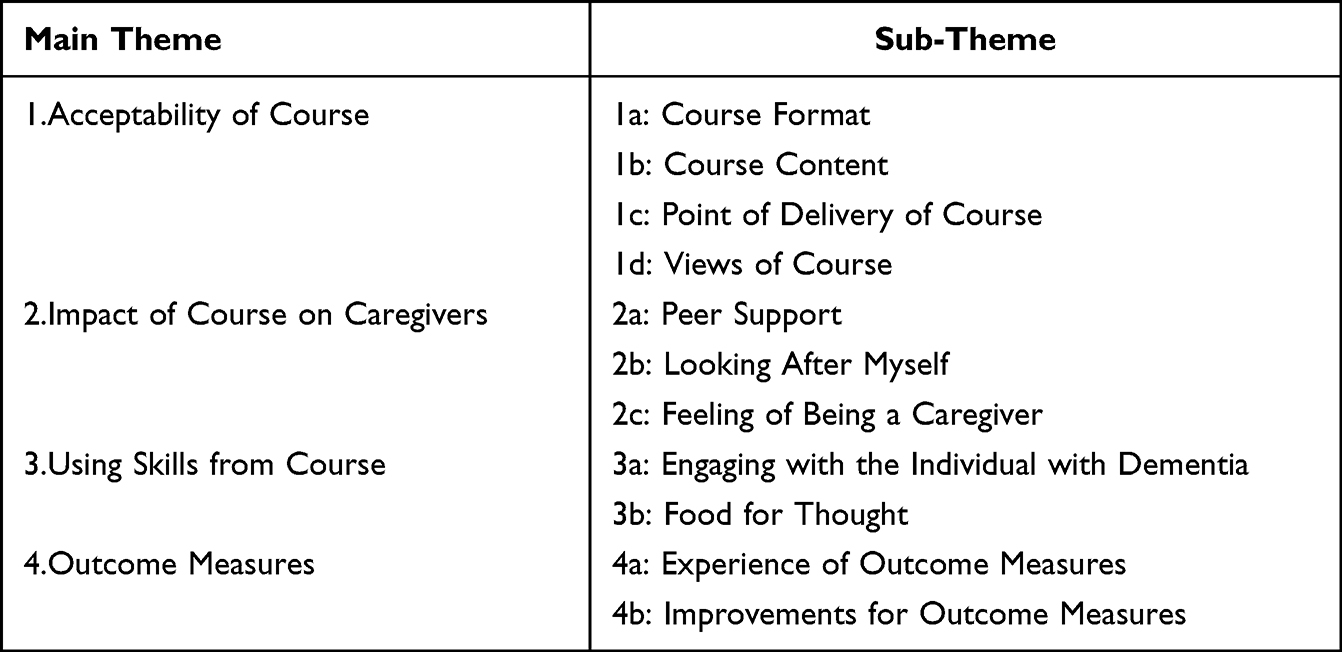 |
Table 4 Thematic Framework |
Acceptability of Course
Course Format
For course length, a minority of participants felt it was “quite a long session” (P3) and that it could be “shortened so it’s like an hour shorter” (P6). However, most individuals found the length of the course appropriate, “I learned a lot. And, the time went so quickly, I couldn’t believe it was over” (P7).
No participants had concerns about the DAC course being run online. Nearly all reported they preferred the online delivery due to it saving on travel time:
it’s much easier to do it on the screen than face-to-face. It makes it easier for people to attend because they don’t have to worry about travelling (P14).
Even participants who had reservations around attending online appeared to have found it manageable
I’m not so keen on talking online, but it was alright once I got started. It wasn’t too full on, and I enjoyed it (P15).
Individuals reported having no concerns with the size of the group. One participant who was part of a group of six stated, “it was a good number; I think you could even have more” (P11). All participants found listening to other caregivers’ experiences “useful” (P2) and “powerful” (P9).
“…the relationships just get birthed even during just a short training…when the course builds into a little community, and you have that support” (P13)
Course Content
Participants reported finding the course content “thought-provoking” (P10) and “helpful” (P15). Various aspects of the course appealed to different individuals for example participants referenced, “the myth busting, I think that was quite helpful” (P1),
talking about psychological models, social interaction and promoting strengths, as opposed to just focusing on medical models, like other courses do, was very informative and interesting (P8)
and “the information about, dementia itself…that was really interesting and helpful” (P9).
The activities and hand-outs were described as “fun and useful” (P4). Individuals stated, “the activities that made us think and share after a bit of information, that was for me was the best thing” (P11) and “there was a lot of good signposting” (P4). One participant stated, “there was nothing about new technology…it would’ve been nice to hear a bit more about that” (P3).
Point of Delivery of Course
A majority of individuals commented on the lack of support they received when the person was diagnosed with dementia.
“The doctors kind of go to you…here’s a leaflet and they go, and you literally have no clue what to do because they say go and talk to the Alzheimer’s society. Okay, right. Where do I start? Where do I get the information?” (P10)
These experiences led participants to reflect on at which point in the dementia journey they felt it would be helpful to receive the DAC course. All individuals felt having the course offered at point of diagnosis would be “really helpful” (P7).
“If everyone could access it, that needed to, they would find it very beneficial…if they got a diagnosis and then automatically get offered your course, maybe even record it to go back to as well, that would be really helpful” (P4)
Views of the Course
Some participants reported feeling thankful for being offered the course stating, “it was amazing to be offered this course” (P3) and “I feel glad that I got offered this course, because I’ve learned so much” (P1).
All participants reported that they would recommend the course to other dementia caregivers.
“You know, sometimes as carers, you don’t have time to read a great big book on dementia, and you wouldn’t understand it half the time. A lot of people who were carers might not have the capacity to be able to do that kind of learning. So having this course shown to them is really valuable, I’d definitely recommend it” (P6)
Impact of Course on Caregivers
Peer Support
Following completion of the DAC course, participants commented on “joining a few groups” (P13), “going to social groups” (P5), “reaching out for support from others” (P7) and “using helplines” (P9).
A couple of participants noted that they had not sought peer support following the course due to having other forms of support, “because I have the regular contact with my siblings and I use that as really my sounding board” (P3).
Looking After Myself
Individuals reported that following engaging with the DAC course they were “paying more attention in looking after myself” (P3), “putting down a few more boundaries than I did before” (P8), and “taking care of myself, having time where I try to just focus on me” (P4). One participant reported the discussion of self-care within the DAC course as being valuable, “Even speaking about it…it just made me think that actually this is really hard, and I do need to take time to look after myself” (P7).
Feeling of Being a Caregiver
Many individuals felt the course provided them with “a bit more hope in knowing I can do this” (P13). They felt it “definitely gives you that insight and I think I’m more empathic, understanding and patient now as a carer” (P1) and “I feel more confident and knowledgeable…Definitely more prepared” (P10). Participants also commented on the course as helping them to not feel “isolated as a caregiver” (P2) and “reminded me there are others out there” (P7).
Using Skills from Course
Engaging with the Individual with Dementia
The majority of individuals reported giving the person with dementia more independence following course completion.
“I’ve learnt from the course the importance of letting him do more things on his own…and I’ve already noticed a bit of a difference in him since doing that”. (P5)
Participants also reported using other skills such as “not contradicting him” (P2), “involving her more in the decision-making” (P11), “keeping him active and including more hobbies” (P6) as well as “changing the way I speak to him, you know the part of the course we went through ways of saying things, I’ve really taken that on board” (P5).
Some noted not having used the skills from the course and all felt if they had received the course at an earlier point this may have been different.
“[X] is quite unwell at the moment, so I don’t think I’ve done anything different but if we were at an earlier stage and I had this course, then I would have done things differently after the course, that’s why I think it’s helpful to have it early on”. (P4)
Food for Thought
Participants stated the course, “really just got me thinking” (P8) and “it helped in getting me thinking about dementia generally and how it doesn’t mean dad can’t do anything anymore” (P2).
“I guess after the course, I’m just more aware of what I’m doing and how I’m caring for him…I notice myself thinking back to the course and being like, oh maybe we should change the way we do that” (P13)
Outcome Measures
All participants in the treatment group were asked of their experience in completing the outcome measures and any improvements they felt could be made.
Experience of Outcome Measures
All treatment group participants described the questions asked in the outcome measures as being “relevant” (P1).
“I found it pretty simple to complete and found all the questions relevant. It does make you think, day to day you go along and then someone asks you a question…it actually makes you think about things” (P7)
Improvements for Outcome Measures
One individual commented on the wording of questions stating “one of the questions that we got…said is it important not to become too attached to residents? I mean, is that what my husband is, a resident?” (P4). Another felt the measures did not consider the individual’s relationship with the person with dementia pre-diagnosis.
“It really depends what relationship you have with that person before they become unwell. I’ve said it didn’t change but that’s because it was great before not because the course wasn’t helpful”. (P4)
Discussion
Findings indicate that the online UK DAC course is both feasible and acceptable and is also feasible to be tested within an RCT design. It has also demonstrated that engaging in the DAC course can have a beneficial impact on various aspects of the caregiving role.
Feasibility
The course met all feasibility criteria established at the beginning of this study, with some limitations in terms of attendance.
Sample recruitment was achieved within half of the pre-set six-month time frame and 83% of the participants who remained eligible were retained at follow-up, surpassing the pre-set 75% threshold. In contrast, the iSupport program had a retention rate of 36.42%, suggesting that the DAC course is more feasible as an online intervention.20 The five outcome measures were also shown to be highly acceptable with completion rates of between 97% and 100% across both conditions. This suggests that investigating the DAC course in a research trial context is feasible and future randomised control trials could allow the DAC course to have a comparable evidence-base to other research.16,17
In terms of the intervention’s feasibility, 65% of the caregivers in the DAC course condition attended the course, which is below the feasibility threshold of 75%. However, 17% of the participants in this condition stated that they were unable to attend the course due to legitimate reasons such as work commitments, alerting the researchers prior to the course date. It is likely that they would have attended had there been another course date available. This suggests that 83% of the participants in the DAC course condition were engaged and willing to participate but the limitations of the research study prevented this.
Acceptability
Ninety-three percent of participants who attended the DAC course completed the full intervention and 100% were retained at follow-up, indicating a high level of course acceptability. This is in positive contrast to the iSupport program which found only 31% of participants completed the recommended five or more of 23 online lessons.20
All who engaged in qualitative interviews reported they would recommend the DAC course to others and had no concerns with regard to the course being run online, with reasons including saving on travel cost and not taking up too much of caregivers’ already limited free time, in line with previous findings.25 Whilst some participants felt the course was too long, the majority felt the length was appropriate. This is important qualitative evidence to support the idea that a brief intervention is well received by caregivers, and that interventions do not need to be longer term as seen in other programs such as START, REACH and iSupport.16,17,20
All participants felt that the DAC course as a group intervention was beneficial. Caregivers mentioned the group aspect helped individuals feel less alone and hearing others’ experiences was powerful, with some individuals requesting to keep in touch with each other. These findings highlight how the group format of the DAC course enables caregivers to feel supported despite being held online. This is consistent with research that has suggested online relationships are able to be formed in similar ways to in-person relationships.37
Qualitative feedback indicated a high level of acceptability with regard to course content. The focus on psychological principles as well as social aspects of dementia was appreciated by participants in providing a different narrative of dementia. Furthermore, the activities and handouts included were deemed helpful.
Impact
As an unpowered feasibility trial, this study was not expected to detect a significant effect.38 There were, however, non-significant changes in favour of the intervention, which are worthy of further assessment. In contrast, other interventions such as the START and REACH programs reported significant effects within their powered trials.16,17 It would be interesting for future powered trials of the DAC course to be conducted and compared to these other intervention findings.
Qualitative feedback highlighted that the course had a positive impact on caregivers and, in turn, care recipients. Caregivers commented on how the course helped provide them with hope, insight, reduced feelings of isolation and served as a reminder to engage in self-care. Participants also reported feeling more confident and prepared in being able to utilise skills they had learnt on the DAC course and to seek peer-support. Equipping caregivers with such skills can also assist with reducing risk of early residential admission of care recipients.18,39 Given the well-documented psychological concerns and lack of independence that can result from caregiving,40 the above findings provide support for the vital impact of the DAC course not only on caregivers but also on individuals with dementia.
Strengths and Limitations
Stakeholder consultation was undertaken before the trial, which is crucial when developing new interventions.41 The course was also delivered to caregivers across the UK to increase the generalisability of the findings to a wider UK audience, with the possibility of public health implementation held at the forefront of this decision.
Despite these strengths, some limitations are noted. All participants were of White British ethnicity making it challenging to generalise findings to caregivers from minority ethnic backgrounds. Furthermore, all participants were recruited via an online dementia research base, which may have resulted in caregivers who are more confident using technology and therefore contributed to the acceptability of the online format. It is also worth noting that the TAU group was not interviewed within this study. As such, qualitative data regarding the TAU group participants’ experience of the outcome measures, the impact of the study period, and/or whether any behaviour change occurred, were not captured. It would be worthwhile for future studies to interview both the TAU and treatment group, in order to ascertain the impact of the DAC course specifically. Some participants were unable to attend the DAC course, most often due to practical reasons. By nature of the intensity of the informal caregiving role, often falling alongside work and other commitments, flexibility is crucial when offering interventions. However, given the small-scale research context, limited course dates were offered. If implemented in a public health setting or a large-scale research project, with more regular and variable times, it is likely that attendance would be higher. In addition, participants in the control condition were not interviewed to explore the acceptability of randomisation in the trial. However, the high levels of retention and outcome measure completion in this condition indicate that randomisation is feasible and acceptable.
Implications
The findings from the current study suggest that the delivery of the DAC course in the UK is feasible, acceptable and can positively impact caregivers and their care recipients. As such, the current study presents a foundation for a larger randomized control trial (RCT) to establish the efficacy and cost-effectiveness of the DAC course on a larger and more diverse sample. Whilst the study explored five different outcome measures, which participants reported to be acceptable in the interviews, it would be beneficial to further consider other outcomes that may be impacted by the DAC course. Furthermore, future research into the DAC course may also need to consider facilitator fidelity to the course manual and slides, in order to increase the validity and reliability of the data collected.
Although most individuals felt the DAC course length was acceptable, some felt it was too long and suggested trialing the course with frequent shorter breaks or as three separate sessions. Furthermore, this study has indicated that flexible and regular delivery would likely be the most effective means of dissemination. Findings also highlighted the lack of support and information caregivers felt they received at the point of diagnosis. Many felt that being offered the course as part of a standard package of care following diagnosis would have been beneficial and would have enabled them to utilize more of the skills discussed at earlier stages. Running an RCT at point of diagnosis within the NHS, utilizing findings from the current study, would assist in further identifying the practical, clinical, and cost implications of the DAC course among informal caregivers.
Conclusion
As dementia diagnoses continue to increase, it is vital that suitable evidence-based caregiver interventions are offered throughout the UK. This study provides promising evidence that the DAC course can provide a brief and proactive intervention for informal caregivers that is feasible and acceptable. Qualitative findings also indicate the DAC course as having a positive impact on caregivers and, in turn, care recipients. Additional research on a larger scale and at point of diagnosis will assist in building on the current study’s findings. Doing so will allow for public health implementation of high-quality evidence-based care among dementia caregivers.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wittenberg R, Hu B, Barraza-Araiza L, Rehill A. Projections of older people with dementia and costs of dementia care in the United Kingdom, 2019–2040. Care Policy and Evaluation Centre, London School of Economics, CPEC Working Paper 5; 2019.
2. Gallagher-Thompson D, Tzuang YM, Au A, et al. International perspectives on nonpharmacological best practices for dementia family caregivers: a review. Clin Gerontol. 2012;35:316–355. doi:10.1080/07317115.2012.678190
3. Prince M, Knapp M, Guerchet M, et al. Dementia UK: second edition - overview. Alzheimer’s Society; 2014.
4. Doris SF, Cheng ST, Wang J. Unravelling positive aspects of caregiving in dementia: an integrative review of research literature. Int J Nurs Stud. 2018;79:1–26. doi:10.1016/j.ijnurstu.2017.10.008
5. Lindeza P, Rodrigues M, Costa J, Guerreiro M, Rosa MM. Impact of dementia on informal care: a systematic review of family caregivers’ perceptions. Br Med J Support Palliat Care. 2020:bmjspcare-2020–002242. doi:10.1136/bmjspcare-2020-002242
6. Or R, Kartal A. Influence of caregiver burden on well-being of family member caregivers of older adults. Psychogeriatrics. 2019;19:482–490. doi:10.1111/psyg.12421
7. Collins RN, Kishita N. Prevalence of depression and burden among informal caregivers of people with dementia: a meta-analysis. Ageing Soc. 2020;40:2355–2392. doi:10.1017/S0144686X19000527
8. Kaddour L, Kishita N. Anxiety in informal dementia carers: a meta-analysis of prevalence. J Geriatr Psychiatry Neurol. 2020;33:161–172. doi:10.1177/0891988719868313
9. Alzheimer’s Disease International. World Alzheimer Report 2019: attitudes to dementia. London: Alzheimer’s Disease International; 2019.
10. Brodaty H, Donkin M. Family caregivers of people with dementia. Dialogues Clin Neurosci. 2009;11:217–228. doi:10.31887/DCNS.2009.11.2/hbrodaty
11. National Institute for Health and Clinical Excellence. Dementia: assessment, management and support for people living with dementia and their carers. NICE clinical guideline 97. London: NICE. Reilly & Newton; 2018.
12. Department of Health Prime ministers challenge on dementia 2020; 2015 [cited June 07, 2023]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/507981/PM_Dementia-main_acc.pdf.
13. World Health Organization. Global action plan on the public health response to dementia 2017–2025; 2017.
14. Schmachtenberg T, Monsees J, Thyrian JR. Structures for the care of people with dementia: a European comparison. BMC Health Serv Res. 2022;22:1372. doi:10.1186/s12913-022-08715-7
15. Amador S, Rapaport P, Lang I, et al. Implementation of START (STrAtegies for RelaTives) for dementia carers in the third sector: widening access to evidence-based interventions. PLoS One. 2021;16:e0250410. doi:10.1371/journal.pone.0250410
16. Wisniewski SR, Belle SH, Coon DW, et al. The Resources for Enhancing Alzheimer’s Caregiver Health (REACH): project design and baseline characteristics. Psychol Aging. 2003;18:375. doi:10.1037/0882-7974.18.3.375
17. Livingston G, Barber J, Rapaport P, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: pragmatic randomised controlled trial. Br Med J. 2013;347:f6276. doi:10.1136/bmj.f6276
18. Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: systematic review and meta‐analysis of randomised controlled trials. Int J Geriatr Psychiatry. 2015;30:130–143. doi:10.1002/gps.4208
19. Livingston G, Barber J, Rapaport P, et al. Long-term clinical and cost-effectiveness of psychological intervention for family carers of people with dementia: a single-blind, randomised, controlled trial. Lancet Psychiatry. 2014;1:539–548. doi:10.1016/S2215-0366(14)00073-X
20. Baruah U, Varghese M, Loganathan S, et al. Feasibility and preliminary effectiveness of an online training and support program for caregivers of people with dementia in India: a randomized controlled trial. Int J Geriatr Psychiatry. 2021. doi:10.1002/gps.5502
21. Christie HL, Boots LMM, Tange HJ, Verhey FRJ, de Vugt ME. Implementations of evidence-based eHealth interventions for caregivers of people with dementia in municipality contexts (myinlife and partner in balance): evaluation study. JMIR Aging. 2021;4:e21629. doi:10.2196/21629
22. Stoner CR, Lakshminarayanan M, Mograbi DC, et al. Development and acceptability of a brief, evidence-based dementia awareness for caregivers course in low- and middle-income countries. Dementia-Int J Soc Res Pract. 2022;21:598–617, Article 14713012211055316.
23. Spector A, Thorgrimsen L, Woods B, et al. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: randomised controlled trial. Br J Psychiatry. 2003;183:248–254. doi:10.1192/bjp.183.3.248
24. Giebel C, Lord K, Cooper C, et al. A UK survey of COVID-19 related social support closures and their effects on older people, people with dementia, and carers. Int J Geriatr Psychiatry. 2021;36:393–402. doi:10.1002/gps.5434
25. Dai R, Spector A, Wong G. e-mental health care for people living with dementia: a lesson on digital equality from COVID-19. Alzheimers Dement. 2020;12:e12100.
26. Browne RH. On the use of a pilot sample for sample size determination. Stat Med. 1995;14:1933–1940. doi:10.1002/sim.4780141709
27. Sim J, Lewis M. The size of a pilot study for a clinical trial should be calculated in relation to considerations of precision and efficiency. J Clin Epidemiol. 2012;65:301–308. doi:10.1016/j.jclinepi.2011.07.011
28. Blok AC, Blonquist TM, Nayak MM, et al. Feasibility and acceptability of “healthy directions” a lifestyle intervention for adults with lung cancer. Psycho-Oncology. 2018;27:250–257. doi:10.1002/pon.4443
29. Galea S, Salvaris CA, Yap MBH, Norton PJ, Lawrence KA. Feasibility and acceptability of an enhanced cognitive behavioural therapy programme for parent–child dyads with anxiety disorders: a mixed-methods pilot trial protocol. Pilot Feasibility Stud. 2021;7. doi:10.1186/s40814-021-00846-8
30. Lintern TC. Quality in Dementia Care: Evaluating Staff Attitudes and Behaviour [Doctor of Philosophy Thesis]. Bangor University; 2001.
31. Spruytte N, Audenhove C, Lammertyn F, Storms G. The quality of the caregiving relationship in informal care for older adults with dementia and chronic psychiatric patients. Psychol Psychother. 2002;75:295–311. doi:10.1348/147608302320365208
32. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20:649–655. doi:10.1093/geront/20.6.649
33. Higginson IJ, Gao W, Jackson D, Murray J, Harding R. Short-form Zarit Caregiver Burden Interviews were valid in advanced conditions. J Clin Epidemiol. 2010;63:535–542. doi:10.1016/j.jclinepi.2009.06.014
34. Vernooij-Dassen MJ, Felling AJ, Brummelkamp E, Dauzenberg MG, Van Den Bos GA, Grol R. Assessment of caregiver’s competence in dealing with the burden of caregiving for a dementia patient: a Short Sense of Competence Questionnaire (SSCQ) suitable for clinical practice. J Am Geriatr Soc. 1999;47:256–257. doi:10.1111/j.1532-5415.1999.tb04588.x
35. Yap P. Gain in Alzheimer care instrument—a new scale to measure caregiving gains in dementia. Am J Geriatr Psychiatry. 2010. doi:10.1097/JGP.0b013e3181bd1dcd
36. Boyatzis RE. Transforming Qualitative Information: Thematic Analysis and Code Development. Sage; 1998.
37. Lomanowska AM, Guitton MJ. Online intimacy and well-being in the digital age. Internet Interv. 2016;4:138–144. doi:10.1016/j.invent.2016.06.005
38. Button KS, Ioannidis JPA, Mokrysz C, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14:365–376. doi:10.1038/nrn3475
39. Pinquart M, Sörensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr. 2006;18:577–595. doi:10.1017/S1041610206003462
40. Kuo LM, Huang HL, Hsu WC, Shyu YIL. Health-related quality of life and self-efficacy of managing behavior problems for family caregivers of vascular dementia and Alzheimer’s disease patients. Dement Geriatr Cogn Disord. 2014;38:310–320. doi:10.1159/000360414
41. Duncan E, O’Cathain A, Rousseau N, et al. Guidance for reporting intervention development studies in health research (GUIDED): an evidence-based consensus study. British. Med J Open. 2020;10:e033516.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multidomain Intervention Program for Older People with Dementia: A Pilot Study
Xuan Nguyen T, Thi Thanh Vu H, Nguyen T, Esterman A, Viet Tran L, Thillainadesan J, Naganathan V, Brodaty H, Trung Nguyen A
Open Access Journal of Clinical Trials 2023, 15:1-10
Published Date: 17 April 2023
The Post-Traumatic Growth Experience in Family Caregivers of People with Dementia: A Descriptive Qualitative Study
Wang Y, Gu Y, Qiu R, Long D, Sun N
Psychology Research and Behavior Management 2025, 18:1495-1507
Published Date: 26 June 2025
A Scoping Review of Psychoeducational Interventions for Managing Type 2 Diabetes Mellitus in Asian Countries
Setyowati R, Haroen H, Yosep I, Agustina HR
Journal of Multidisciplinary Healthcare 2025, 18:8333-8350
Published Date: 30 December 2025