Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Investigating the Added Value of a Culturally Tailored Peer Support Intervention for Black Adults with Diabetes: A Randomized Mixed Methods Pilot Trial
Authors Maurer M, Wen MJ ![]() , Deheck J, Szymanski S, Hansen MA
, Deheck J, Szymanski S, Hansen MA ![]() , Pickard AL, Onchiri LK, Quinn T, Kansariwala T, Shiyanbola OO
, Pickard AL, Onchiri LK, Quinn T, Kansariwala T, Shiyanbola OO ![]()
Received 2 July 2025
Accepted for publication 1 December 2025
Published 15 December 2025 Volume 2025:18 Pages 4609—4629
DOI https://doi.org/10.2147/DMSO.S548440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hillary Keenan
Martha Maurer,1 Meng-Jung Wen,2 Jacob Deheck,3 Sierra Szymanski,3 Makenzie A Hansen,3 Annika Louise Pickard,2 Lorraine K Onchiri,3 Tegan Quinn,3 Tina Kansariwala,1 Olayinka O Shiyanbola4
1Sonderegger Research Center for Improved Medication Outcomes, School of Pharmacy, University of Wisconsin-Madison, Madison, WI, USA; 2Social and Administrative Sciences Division, School of Pharmacy, University of Wisconsin-Madison, Madison, WI, USA; 3School of Pharmacy, University of Wisconsin-Madison, Madison, WI, USA; 4Department of Clinical Pharmacy, College of Pharmacy, University of Michigan, Ann Arbor, MI, USA
Correspondence: Olayinka O Shiyanbola, University of Michigan, Department of Clinical Pharmacy, 428 Church Street, Ann Arbor, MI, 48109, USA, Tel +1 734 647 8396, Email [email protected]
Purpose: This randomized controlled mixed methods pilot study evaluated the preliminary signal of effectiveness of a culturally tailored intervention embedded within a standard Diabetes Self-Management Education (DSME) program.
Patients and Methods: Fourteen Black adults with uncontrolled diabetes (A1C ≥ 7.5) enrolled in the study. The study was conducted at a community center and over the phone within a US Midwestern State. All participants participated in a 6-week evidence-based DSME program, with a subset of participants (n=7) randomized to the intervention receiving additional education sessions and race-congruent phone-based peer support throughout the 6-month intervention. Changes in Hemoglobin A1c (A1C) (primary outcome) and self-reported medication adherence (secondary outcome), and other psychosocial outcomes (beliefs about diabetes, self-efficacy, diabetes empowerment, etc.) were assessed at 3 and 6 months using paired t-tests. Between-group differences were analyzed using the Mann–Whitney U-test and within-group differences were analyzed using Wilcoxon signed-rank test. Qualitative data on participant’s perceived impact of the intervention on primary and secondary outcomes were collected through semi-structured interviews and analyzed to identify themes. Subsequently, a mixed methods analysis was conducted to compare quantitative and qualitative findings.
Results: At 6-months, A1C was statistically significantly lower in the intervention group (7.9% (SD =0.4; 95% CI [7.6– 8.2]); n=7) compared to the control group (10.6% (SD =0.7; 95% CI [9.9– 11.2]); p =0.01; d=0.73; n = 6). There were no significant between-group differences (p =0.22) in medication adherence between the 2 groups. Qualitative themes related to beliefs about medicines, diabetes distress, etc. were identified, and integrated with quantitative psychosocial outcomes further explaining the findings.
Conclusion: The findings suggest a signal of evidence for a future adequately powered, randomized controlled trial, testing whether the addition of the theory and evidence-informed culturally specific components of the intervention improve outcomes compared to the DSME program alone.
Keywords: type 2 diabetes, medication adherence, diabetes self-management
Introduction
In comparison to other racial and ethnic groups, diabetes affects Black adults in the US at a disproportionately higher rate, with the prevalence of diagnosed diabetes among non-Hispanic Black adults (12.1%) being the second highest among all reported racial and ethnic groups, and nearly double the prevalence for non-Hispanic White adults (6.9%).1 Black adults with diabetes are also more likely to experience a greater number of complications and disability, 50% more likely to develop diabetic retinopathy, 1.5 times more likely to be hospitalized, and 2.7 times more likely to die from diabetes.2,3 Prior research has demonstrated that even with equal access to medications, Black adults are less adherent to prescribed medications than non-Hispanic white adults.4 When controlling for quality of care and insurance coverage, Black adults were found to be 25% less likely to adhere to their diabetes medication regimen than non-Hispanic white participants.4,5 Research suggests that factors underlying medication adherence disparities among Black adults could be in part due to low self-efficacy and limited engagement during patient-provider interactions, which may be influenced by discrimination experiences and provider distrust5–7 as well as diabetes and medicine misbeliefs.7
Studies document that medication nonadherence is one of the strongest predictors of elevated hemoglobin A1c (A1C)8–10 which increases the risk for diabetes complications such as diabetic retinopathy, nephropathy, and neuropathy.11 Therefore, targeting improvement of adherence may lead to a reduction in A1C5,9,12,13 which may, in turn, reduce the prevalence of diabetes disparities that affect Black adults. To reduce morbidity and mortality in this population, diabetes self-management interventions that address medication nonadherence and other self-management objectives are vital.4,5,7,14,15
Currently available diabetes self-management (DSME) programs are inadequate to improve outcomes for Black adults because they lack sufficient focus on medication adherence, do not explicitly tailor their content to psychosocial contributors to Black adults’ diabetes disparities,16 such as racial discrimination/distrust in healthcare17,18 and do not focus on health misperceptions.19 For example, the widely disseminated, 6-week Diabetes Self-Management Program - Healthy Living with Diabetes (HLWD) program endorsed by the American Diabetes Association addresses self-management broadly but includes only minimal content about medication adherence and is not culturally tailored for Black adults with diabetes.20,21 HLWD does not address sociocultural barriers associated with Black adults’ medication adherence and diabetes management.17
A recent systematic review of 16 randomized controlled trials found that culturally adapted DSME interventions for Black adults were associated with improvements in glycemic control.22 However, the interventions varied in scope, were not evidence-based or widely disseminated, and none of them focused on improving medication adherence. The review highlights the promising evidence of the positive impact culturally adapted DSME generally can have on diabetes health outcomes. This study uniquely focuses on enhancing the medication adherence content of an evidence-based, broadly implemented DSME program for Black adults.
Among racial and ethnic minority groups, peer education is known to be effective in addressing negative beliefs.23,24 Enhancing engagement in medication-taking behaviors among Black adults may be achieved through peer support from someone who is successfully managing their diabetes. For example, community and church based culturally adapted diabetes self-management programs for Black adults use storytelling to provide self-management education based on cultural appropriateness,25 traditional values,26 and diet and food preferences, and have used trusted community members to lead the intervention.27
Our prior research, which was guided by the extended self-regulatory model28 has demonstrated that improvements in medication-taking behaviors are possible when Black peers provide culturally appropriate support to other Black adults.29,30 The conceptual model suggests that a person’s beliefs about their illness and medications can be modified by enhancing information, which is necessary to change health behaviors, increasing motivation via peer support, and improving behavioral skills, which can help Black adults enhance problem-solving skills that improve their medication taking behaviors in ways providers cannot via typical clinic interactions alone.31,32 In particular, race-congruent peer support is effective at addressing experiences of mistreatment by providers, feelings of distrust in the healthcare system, and reframing misperceptions regarding medications influenced by family or culture.33,34 Therefore, we hypothesize that participants randomized to receive race congruent peer support will have greater improvements in A1C and medication adherence than individuals not receiving support, because race congruent peer support will address culturally specific beliefs and misperceptions regarding diabetes and medicines. Race congruent peers will reflect on and share their own experiences as a member of the same culture enhancing the connection and helping to increase motivation, self-efficacy, activation and communication with providers.
To enhance existing evidence-based DSME and tailor it to increase effectiveness for Black adults, we developed and pilot tested a theory and evidence-informed intervention, Peers’ Experiences in Communicating and Engaging in Healthy Living (Peers EXCEL), which embeds educational sessions led by a pharmacist and provider addressing misperceptions and barriers to medication adherence and race-congruent peer support from adults with well-controlled type 2 diabetes.30 In a prior single-arm pilot study, we evaluated the feasibility of implementing Peers EXCEL.30 We found a signal of effect of the intervention, with a clinically meaningful improvement in A1C, nonadherence and diabetes and medicine misperceptions. The current trial – Living Well & Empowered – builds on our prior non-randomized study to pilot the intervention by using a randomized controlled mixed methods two-arm design. The Living Well & Empowered trial protocol was described in detail in a prior publication.35 The trial feasibility and intervention acceptability data which showed high adherence and retention among participants and qualitative data demonstrating participants satisfaction and acceptability is reported elsewhere.36
This companion paper reports on the exploratory outcomes of the Living Well & Empowered trial to assess if there is a signal of change in the A1C for randomized intervention participants at baseline, 3 months, and 6 months, including self-reported medication adherence at 6 months. We hypothesized that, in comparison with the control group, the intervention group would have a greater signal of change in mean hemoglobin A1C that is clinically meaningful (0.6 reduction) as well as show an improvement in self-reported medication adherence and other psychosocial outcomes.
Materials and Methods
Ethical Statement
This randomized controlled mixed methods study was approved by the University of Wisconsin-Madison Minimal Risk Research Institutional Review Board (Study ID: 2020–1061). A written informed consent form was obtained from each participant prior to the trial, which included a consent to publish quotes from qualitative interviews. No identifiers were retained after data transcription. This clinical trial is registered at: https://clinicaltrials.gov/study/NCT05527847.
Design and Setting
This was a randomized controlled mixed methods pilot trial, conducted from March-August 2023 in a community site within a Midwestern State in the United States.
Intervention
All individuals who enrolled in the study participated in Healthy Living with Diabetes (HLWD). HLWD is an evidence-based, 6-week DSME program for community settings with 2.5-hour weekly in-person group sessions led by 2 trained facilitators addressing standardized topics such as diet, exercise, stress, medication use, skin and foot care, action plans, communicating with healthcare providers, and having discussions with family members. All participants received the program resource book37 that contained the HLWD topics covered in the classes. In this trial, weekly sessions were held on weeknight evenings at a community center. Transportation and childcare support were provided to participants who needed it, and meals were provided during the sessions.
Additionally, all participants were provided the opportunity to work with a community health worker (CHW), who offered support and resources related to social determinants of health (SDOH)-related barriers (eg, housing, transportation, food insecurity). The CHW attempted to engage with each participant for an initial discussion and continued working with participants who expressed a need for follow-up resources.
Control Arm (HLWD Only)
Participants in the control arm only participated in the 6-week HLWD program. Figure 1 illustrates the control and intervention components.
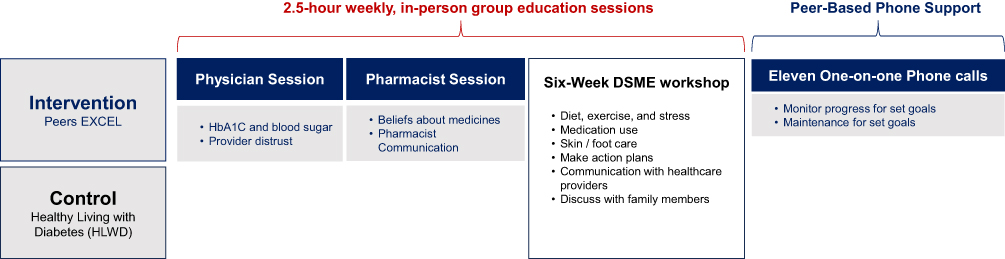 |
Figure 1 Intervention and control sessions. |
Intervention Arm (Peers EXCEL)
The intervention adds the following to the HLWD 6-week session: (1) two group sessions facilitated by a pharmacist and a physician, introduced prior to starting HLWD, and (2) race-congruent peer support from Ambassadors. The two group sessions focused on culturally tailored content. The first session facilitated by a physician focused on racial discrimination and provider mistrust, understanding hemoglobin A1C and blood sugar, and building positive relationships with providers for enhanced communication. The second session with the pharmacist covered diabetes and medication beliefs, sociocultural barriers to medication nonadherence among Black adults, and how to improve communication with pharmacists. The second added component – peer support - was delivered by Ambassadors, who were Black adults with diabetes who self-reported being adherent to their medicines and had well-controlled diabetes control (A1c of <7.5%). Ambassador interactions with participants occurred during HLWD group education sessions that they attended together, and through follow-up phone support. In total, Ambassadors completed 11 calls with the participants, including two preliminary calls with participants at the beginning of the program as they were attending the HLWD sessions together, five weekly calls after the 6-week session ended, to address specific intervention topics (eg, medicine and diabetes perceptions, managing family and cultural relationships, and building positive relationships with healthcare providers), then two bi-weekly calls for 1 month, and then two monthly calls for the last 2 months to support participant’s progression towards their action plans and set goals.
Patient Involvement
Patients were not involved in the development of the current trial; however, our foundational prior studies that directly led to this study, involved patients in the development of the intervention being tested. In a prior study, the intervention content and design were informed by discussions with Black adult patients participating in community-based focus groups.38,39 Additionally, the prior research was informed by continuous feedback from community-based patient advisory boards.40,41 For the current trial, study results were shared with participants at a community-based event led by the PI.
Participants
We enrolled 14 Black adults and randomized them into the intervention and control groups. Figure 2 shows the CONSORT flowchart of participant recruitment and retention.42 Inclusion criteria for participants included: (1) identifying as a Black/African American adult aged 18 to 90 years old diagnosed with type 2 diabetes who can speak and/or read English, (2) having a prescription for at least one oral or injectable diabetes medication, (3) living in the geographical area during the study, (4) having an A1C value of 7.5% or greater, and (5), Self-reporting medication nonadherence. Exclusion criteria for participants included: (1) Current participation in another diabetes management program focused on medication adherence, (2) being an older adult with a previous episode of hypoglycemia that required medical assistance or administration of glucagon, and (3) Self-reported schizophrenia, dementia, untreated bipolar disorder, or active substance use disorder.
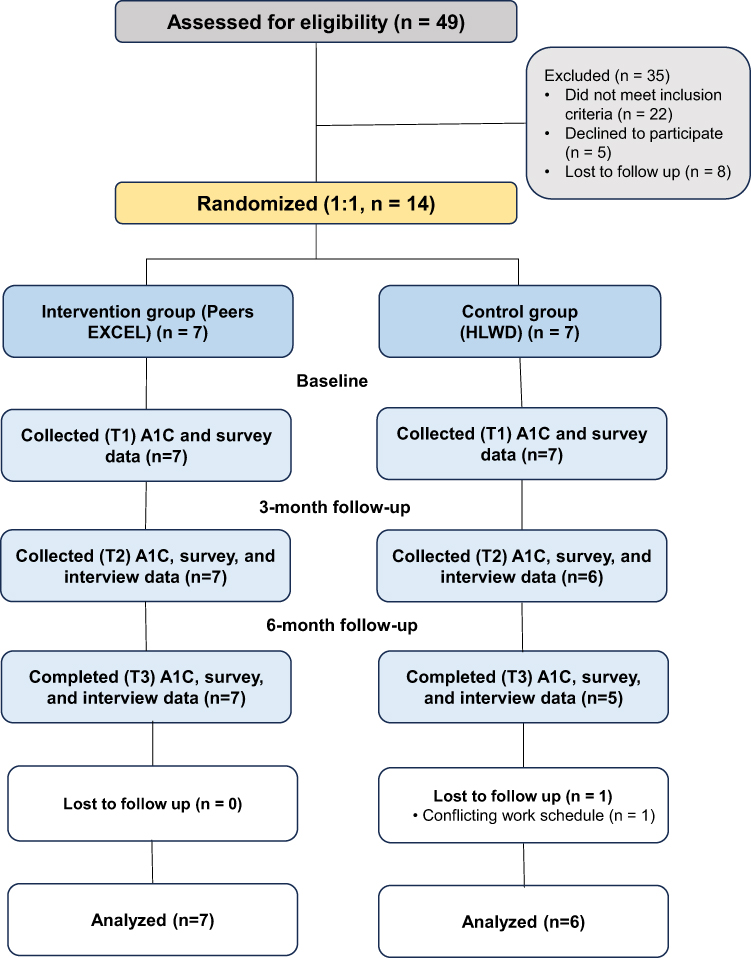 |
Figure 2 Living Well & Empowered trial Consolidated Standards of Reporting Trials diagram of participants at each assessment period. |
Interventionists
In addition to participants, there were several individuals involved in delivering components of the DSME program and the intervention. Three ambassadors provided peer support to the Black adults in the intervention arm. The same two HLWD facilitators led the weekly diabetes self-management sessions for both the intervention and control groups, a physician and pharmacist led the additional intervention sessions on beliefs and provider distrust, and a CHW was available to support all participants in addressing barriers related to social determinants of health, such as access to healthy food and transportation to medical appointments.
Inclusion criteria for ambassadors included: (1) Identifying as a Black adult aged 18 to 90 years old diagnosed with type 2 diabetes mellitus who can speak and/or read English, (2) Having a prescription for at least one oral or injectable diabetes medication, (3) Living in the geographical area during the study, (4) Having a diagnosis of type 2 diabetes for at least one year, (5) Controlled diabetes (A1C <7.5%) and self-reporting being adherent to medications (6) Being able to provide peer support and track phone conversations, and (7) being prepared to attend all training sessions and meetings.
Inclusion criteria for being a HLWD Facilitator included: (1) Identifying as a Black/African American adult, (2) Completing the required HLWD training, and (3) having a diabetes diagnosis or personal lived experience with diabetes.
The pharmacist and physician delivering the additional two intervention sessions identified as Black and Asian, respectively, and had extensive clinical experiences interacting with underrepresented patients, including Black adults with diabetes.
Procedures
Recruitment
Purposive sampling was used for the recruitment of participants in a midwestern city with a population of about 270,000. From January through March 2023, we employed a combination of passive and active approaches for recruitment. Passive approaches included posting study flyers in food pantries and community centers, radio advertisements, and word of mouth communications. Active approaches included community center presentations by the PI, inviting participants from past studies to inform others about the study, and speaking with potential participants.
Participant Screening and Randomization
A two-step screening process was completed by all eligible participants and consisted of a (1) preliminary phone screening to ensure the individual met the initial inclusion criteria (ie, identifying as Black/African American adult, aged 18–90, diagnosed with Type 2 diabetes, etc.) and a subsequent (2) point-of-care A1C test to confirm their A1C was 7.5% or greater. If study eligibility was confirmed, participants enrolled in the study, and completed the intervention, they were compensated with $200. At baseline enrollment, participants attended a prerequisite orientation session that discussed study timeline and study procedures as well as brief health literate presentation about the meaning of clinical trials, randomization, and the rationale for study completion. Informed consent was obtained following the orientation and baseline data was collected using A1CNow+ point-of-care testing kits43 and self-administered surveys with validated scales. A study team member, who was not involved in enrollment, generated a random allocation sequence using computer software. Allocation concealment was ensured by using sequentially numbered sealed envelopes, which were given to participants immediately after completion of the consent form. Outcome assessors were blinded to the randomization as all participants, regardless of group assignment, attended the data collection session together and were instructed not to discuss their group with the data collectors.
Interventionist Training and Fidelity Assessment
All individuals delivering the intervention completed human subjects training and were added to the Minimal Risk IRB protocol of the PI’s prior University.
Ambassadors
The three ambassadors who provided peer support for this trial participated in our prior study30 as peer supporters in a similar role and therefore did not need to repeat the full training in delivering the intervention. To prepare for the current trial, they attended a 1-hour orientation with the PI and the study team prior to initiation of the trial to be reacquainted with the goals of the study and learn about important differences in study design and procedures. They also attended a 1-hour virtual refresher training on delivering the phone-based peer support component of the intervention to review the topics to address and to remind them about the tools provided for conducting the phone calls. Intervention fidelity was assessed via weekly phone calls with a study team member to document phone call completion and problem solve any challenges.
HLWD Facilitators
Both facilitators completed the required training to deliver the evidence-based HLWD program. One facilitator participated in a virtual 32-hour facilitator training provided by the state agency licensing the program and the other facilitator who had previous training in a similar evidence-based program related to living with chronic conditions, participated in a 3-hour virtual cross-training provided by the national program developers. Both facilitators met with the PI and study team for a 1-hour virtual study orientation prior to beginning the program. The two facilitators implemented the DSME workshop for both the intervention and control group. Intervention fidelity was assessed by an HLWD Master Trainer who attended and observed the third weekly session completing a fidelity checklist and discussing feedback with the facilitators.
Additional Session Facilitators
The pharmacist and physician delivering the additional two intervention sessions had discussions with the PI about the standardized intervention content and script to be used to lead the sessions. The PI was present at the two sessions allowing her to assess whether the sessions were facilitated as intended.
Community Health Worker
The study team held an informational orientation meeting with the community health worker (CHW) to describe the study and discuss the CHW’s role. The study team periodically checked in with the CHW throughout the trial.
Data Collection
Quantitative and Qualitative Data
Quantitative data was collected at baseline, 3 months, and 6 months. The primary outcome, Hemoglobin A1c (A1C) was tested using the A1CNow+ testing kits,43 and the secondary outcome, self-reported medication adherence, was assessed with the Adherence to Refills and Medications-Diabetes measure.44 Other psychosocial outcomes were measured with 25 minute-self-reported surveys which included diabetes health beliefs assessed using the Brief Illness Perception Questionnaire,45 beliefs about diabetes medications (Beliefs about Medicines Questionnaire),46 self-efficacy with taking medications (Self-Efficacy for Adherence to Medication Use Scale),47 diabetes empowerment (Diabetes Empowerment Scale – Short Form),48 and perceived quality of patient-provider communication (Patient’s Perceived Involvement in Care Scale),49 and diabetes distress (Diabetes Distress Scale).50
Qualitative data were collected via 60-minute semi-structured virtual interviews with study participants at 3 and 6 months. The interviews aimed to understand their experiences with the intervention and gather feedback on the program. Qualitative data were also collected from the interventionists, including through two focus groups with the Ambassadors at 3 and 6 months, a group discussion with the two HLWD facilitators, and a debrief with the CHW, both at 3 months. The purpose was to elicit their experiences facilitating the program, learn about challenges they encountered and learn about suggestions for improving program delivery.
Participant harms defined as emergency room visits and hospitalizations, were assessed by research team members making frequent, brief phone calls to check-in with participants to assess for harms. These were reported to the PI who determined if further follow-up was appropriate.
Data Analysis
Quantitative
For this analysis, we examined pre- vs post-intervention changes in A1C, self-reported medication adherence, and other psychosocial outcomes at 3 and 6 months using paired t-tests. Between-group differences were analyzed using the Mann–Whitney U-test and within-group differences were analyzed using Wilcoxon signed-rank test.
Qualitative
We conducted transcription and coding of audio-recorded participant interviews and Ambassador focus groups. Transcripts were coded by research assistants using NVivo v 14 (Lumivero)51 Prior to coding, the transcripts were read line-by-line for data immersion. A team of three research assistants coded the transcripts independently – (investigator triangulation), discussed similarities and differences, and reached consensus. The group discussion with the facilitators and debrief with the CHW were analyzed by trained research assistants who identified key messages relevant to the research question.
Mixed
A mixed methods analysis was conducted after analyzing the quantitative and qualitative data separately. A comparison in the context of primary and secondary outcomes was interpreted using a joint display including themes, subthemes, quotes, and meta inferences. Integration was achieved using a joint display, which allowed for advanced interpretation: qualitative insights were examined to contextualize the quantitative findings, and discrepancies or convergences across datasets were explored. This process facilitated the development of meta-inferences, where combined insights not only clarified observed patterns but also provided actionable implications for future program design and intervention tailoring.
Results
Quantitative Results
Participant Demographic and Clinical Characteristics
A total of 14 participants enrolled in the trial and were randomized into the intervention (n = 7) and control group (n = 7). Thirteen participants completed the 6-month program, with one participant in the control group dropping out because of schedule conflicts. The mean age of participants was 54.6 years old (SD = 17.4) and seven (54%) identified as female. The average years of diabetes diagnosis was 14.7 (SD = 9.6) and the average number of diabetes medications taken was 1.9 (SD = 1.2). Table 1 shows the participant demographic information in the intervention and control groups. There was no significant difference in participant characteristics between groups. There was some missing outcome data due to one participant withdrawing from the study prior to the 3-month outcome assessment and another participant not attending the final study visit, (Figure 2). No participants in either the intervention or control group reported harms related to study participation.
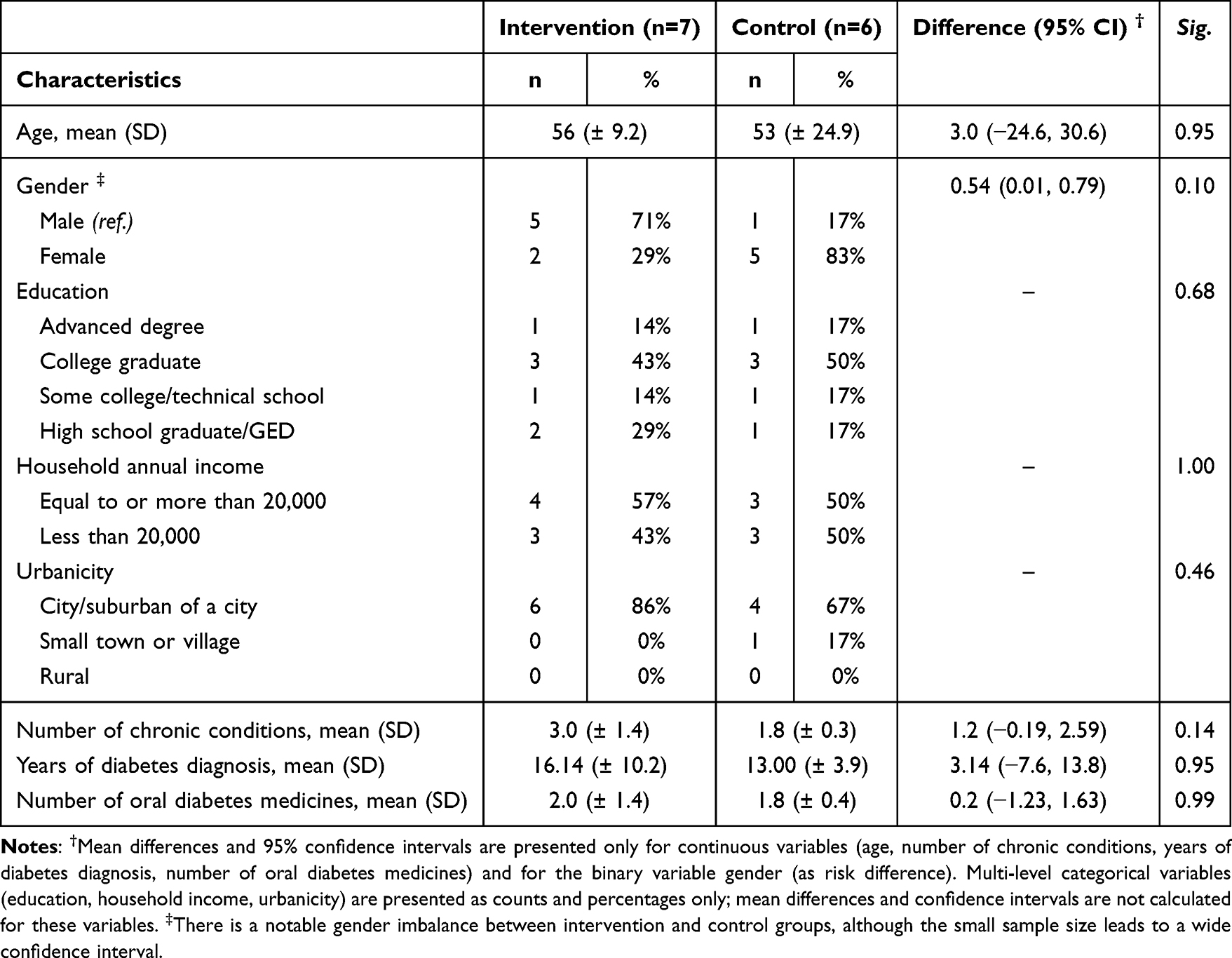 |
Table 1 Demographic and Clinical Characteristics Between Groups at Baseline |
Exploratory Outcomes
Comparison of A1C and Self-Reported Medication Adherence Between Groups
At baseline and 3 months, there were no differences in mean A1C, medication adherence and psychosocial outcomes between the intervention and control group (Table 2). At the end of the 6-month program, the primary outcome, A1C level, was 2.7% (SD = 0.7) statistically significantly lower in the intervention group (7.9% (SD =0.4); 95% CI [7.6–8.2]); n=7) compared to the control group (10.6% (SD =0.7); 95% CI [9.9–11.2]); p =0.01; d=0.73; n = 6).
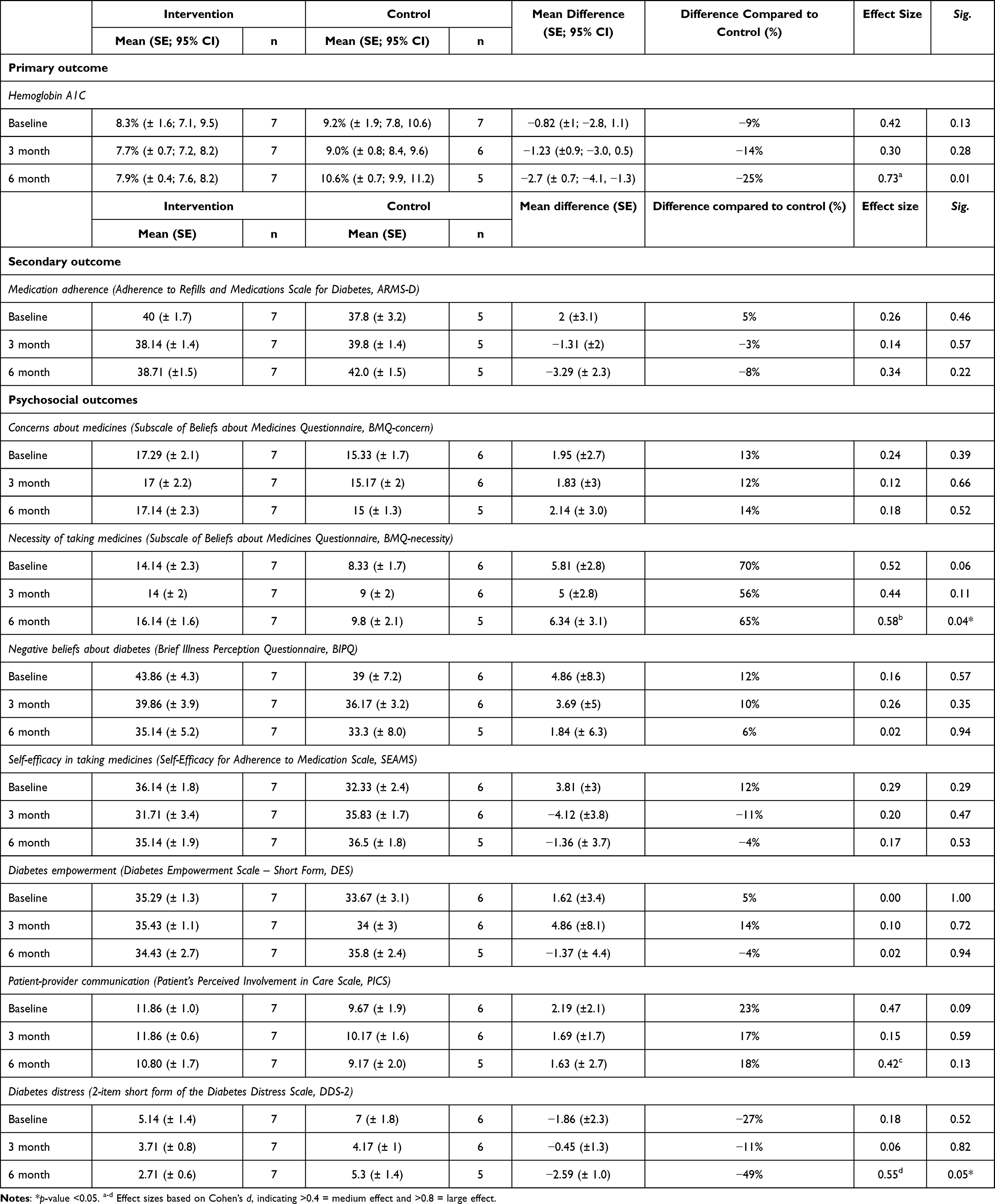 |
Table 2 Comparison of Hemoglobin A1C, Self-Reported Medication Adherence, and Psychosocial Outcomes Between Groups Over Three Time Points (Baseline, 3 Months and 6 Months) |
Figure 3 shows the trends in the change in A1C between groups over three time points. As for medication adherence, we did not find any significant between-group differences (p =0.22).
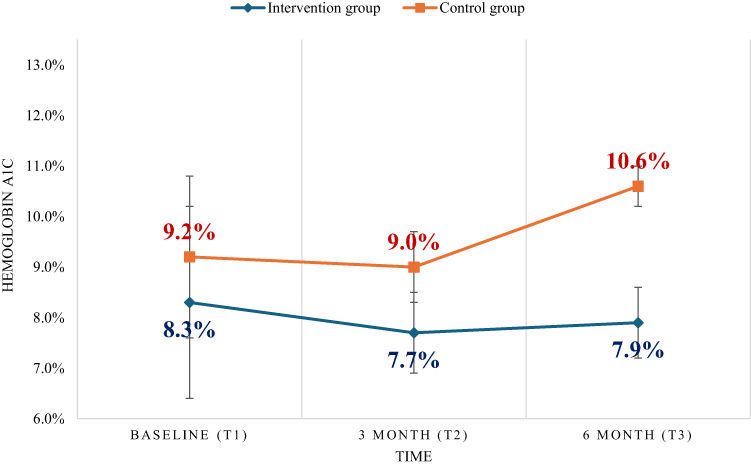 |
Figure 3 The trends in the change in Hemoglobin A1c between the control and intervention groups over time; Intervention group (n=7); Control group (n=6); Between-group differences were analyzed using the Mann–Whitney U-test. |
Comparison of Other Psychosocial Outcomes Between Groups
For the psychosocial outcomes, the intervention group showed a 65% significantly higher perception of the necessity of taking medicines (p =0.04; d =0.58), 18% higher mean score on the Patient’s Perceived Involvement in Care measure, representing better patient-provider communication (p =0.13; d =0.42), and 49% significantly lower diabetes distress (p =0.05; d =0.55) compared to the control group, each with medium effect sizes (Table 2).
Outcomes within the Intervention Group
Within the intervention group, we found a signal of change at 3 months from baseline, with a clinically meaningful decrease (−.6%, d =0.24) in mean A1C.52 Additionally, from baseline to 6 months, there was a 20% reduction in participants’ negative perceptions about diabetes (d =0.64) and a 47% reduction in diabetes distress (d =0.69), each with medium effect sizes (Supplementary Table 1).
Qualitative Results
Participant Experiences
In semi-structured interviews, participants shared their personal experiences with having diabetes and how the intervention supported them in enhancing their diabetes self-management. Seven themes provide additional rich insight into the psychosocial domains. Table 3 provides representative quotes for each theme.
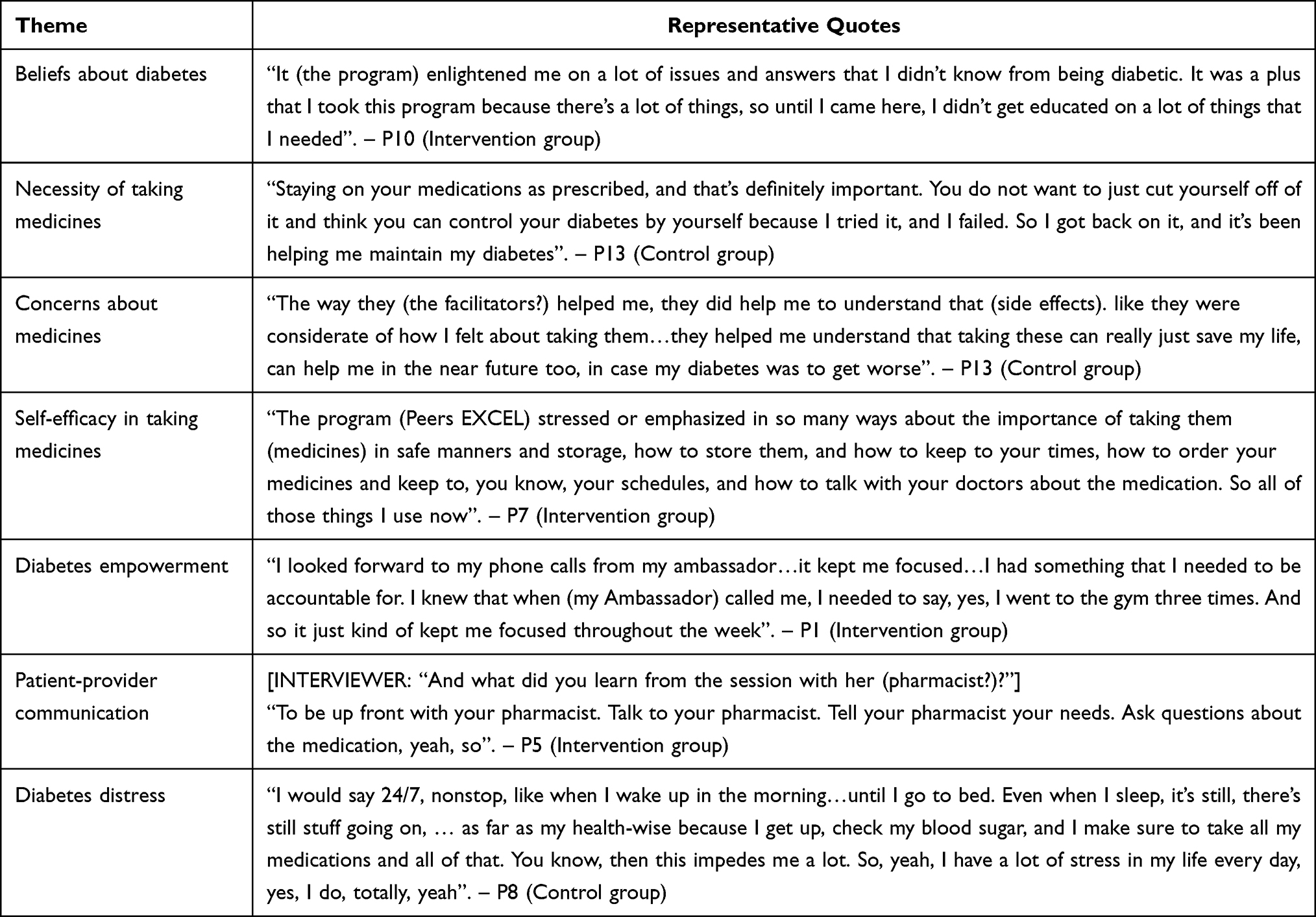 |
Table 3 Themes and Representative Quotes from Participant Interviews |
Beliefs About Diabetes
Participants reported having a lack of understanding about their illness prior to participating in the study. They shared that this deficit was addressed by the program through enhancing their understanding of their disease through which they learned to avoid the consequences of diabetes, (eg, diabetes complications). For example, a participant in the intervention group (Table 3) reported gaining a better understanding of what it meant to live with diabetes through the program, which filled a need for information that was not met before program participation.
Necessity of Taking Medicines
Participants learned about the necessity and importance of taking diabetes medications. Despite not receiving the Peers EXCEL intervention, participants in the control group shared that through the group education classes, they learned the importance and necessity of taking their diabetes medications properly.
Concerns About Medicines
Participants in both the intervention and control groups expressed concerns about medication side effects and the burden of using medicines. Yet, the qualitative data are consistent with the quantitative data which suggests that for all participants, there was a trend towards participants having fewer concerns about medicines at 6 months. Qualitatively, participants shared that the program helped them to address their concerns about their diabetes medicines and how addressing those concerns positively impacted their lives. For example, a participant in the control group expressed that the program helped them to have a better understanding of medication side effects which addressed their concerns and reinforced the importance of taking the medicines.
Self-Efficacy in Taking Medications
Participants in both the intervention and control groups acknowledged the programs’ impact in providing individuals with the necessary knowledge and skills to communicate with healthcare providers and manage their diabetes medications safely and effectively. This suggests that the intervention facilitated improvements in participants’ self-efficacy through promoting open dialogue with providers about medicines, safe diabetes medication storage, and adhering to proper dosing schedules.
Diabetes Empowerment
While participants in both groups reported goal setting activities, which motivated them to manage their diabetes, participants in the intervention group specifically mentioned that consistent interactions with their ambassador provided them accountability and empowered them to take charge of managing diabetes and maintain healthy habits.
Patient-Provider Communication
Participants in the intervention group reported that the encouragement to actively engage with providers empowered them to ask their providers for clarification regarding diabetes medications and express any needs or concerns to their provider or pharmacist. In contrast, participants in the control group expressed a desire to learn how to initiate conversations about medications with their healthcare providers.
Diabetes Distress
Participants in both groups expressed their feelings of constant distress and the continuous burden their diabetes imposes on their physical and mental health. From adhering to diabetes medication regimens to regularly checking their blood sugar levels, the overall demands of diabetes management heightened their stress levels and resulted in a constant state of distress. The qualitative findings do not differentiate between the levels of diabetes distress experienced by participants in the control versus the intervention groups, suggesting that individual difficulties in managing their diabetes during the program still existed and caused certain challenges for participants in both groups.
Perceptions and Experiences of Those Delivering the Intervention
The Ambassadors, HLWD Facilitators, and the CHW shared their perceptions about the program and experiences of delivering it, including suggestions for improving the program in the future.
Ambassadors
Two key themes related to Ambassadors’ perceptions and experiences delivering the intervention emerged from the focus groups (Table 4). They reported that they were proud to be advocates for minoritized groups by serving as an Ambassador providing support to other Black adults in the Peers EXCEL program, which they viewed as valuable. The second theme identified was that open and inclusive group dynamics in the program group sessions led to stronger connections among people in the program, including facilitators, health professionals, ambassadors and participants. Ambassadors appreciated that the facilitators fostered this positive dynamic through the non-judgmental discussion about their living experiences and through tailoring the program information to acknowledge individual variation.
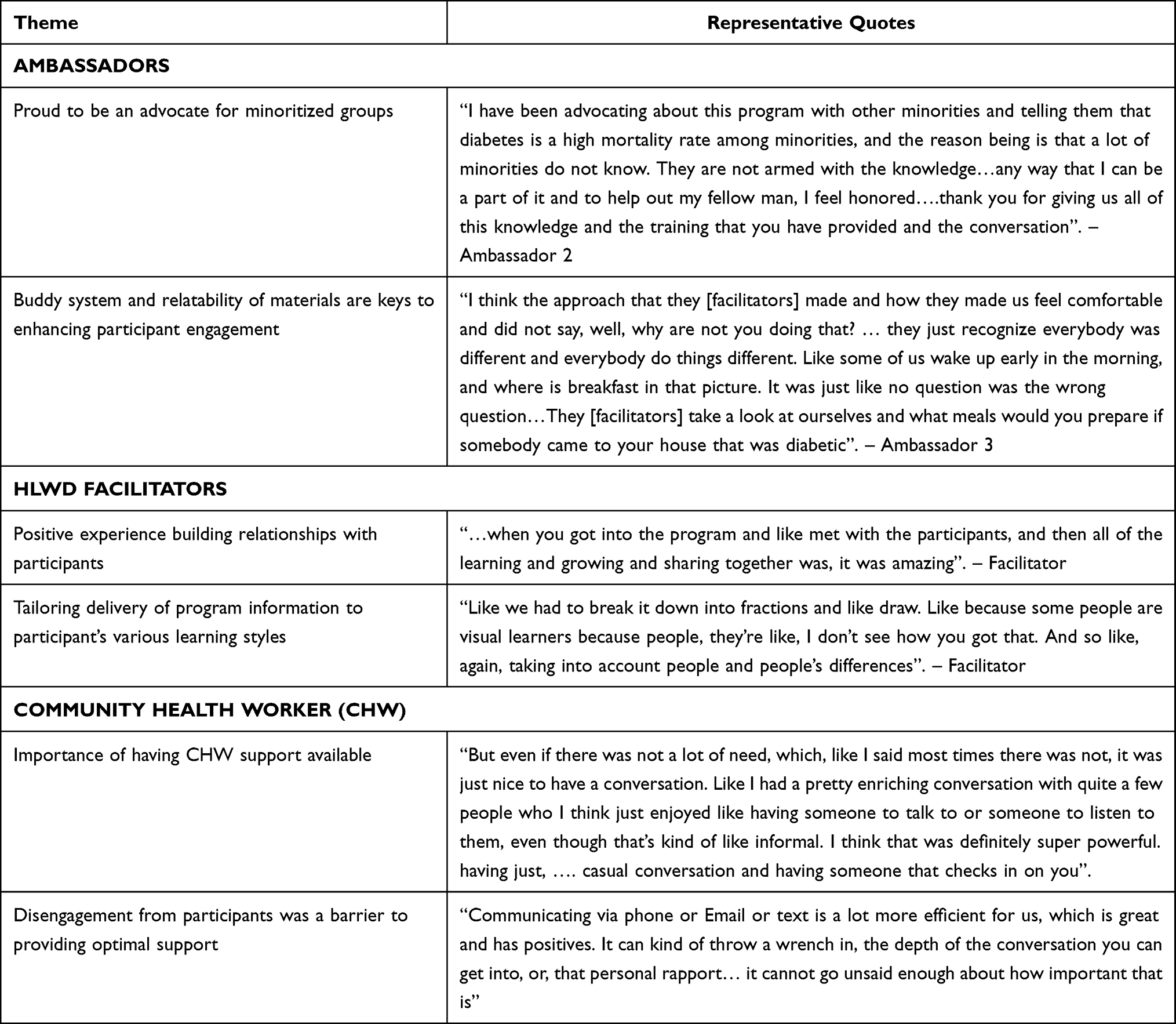 |
Table 4 Interventionists’ Perceptions of the Program |
Ambassadors suggested that the process of being paired with participants could be improved in future programs by incorporating a mechanism to match participants with ambassadors who shared similar interests, beyond characteristics like age and gender. They also suggested adding more opportunities to be active as a group, such as a group exercise activity during the break so participants could stay focused during the long sessions. Ambassadors also shared the suggestion for facilitators to allow additional time for participants to share stories about experiencing systemic racism in healthcare and provide ideas for how to handle those situations, such as a list of questions participants could ask their providers.
HLWD Facilitators
Two key messages derived from the debrief with the HLWD facilitators were positive experiences building relationships and engaging with the participants and tailoring the delivery of the DSME evidence-based content to participant’s individual learning styles (Table 4) The HLWD facilitators provided suggestions for improving future programs (Table 5) suggesting that community partners supporting the workshops could be more engaged and share information about their own health and wellness programming.
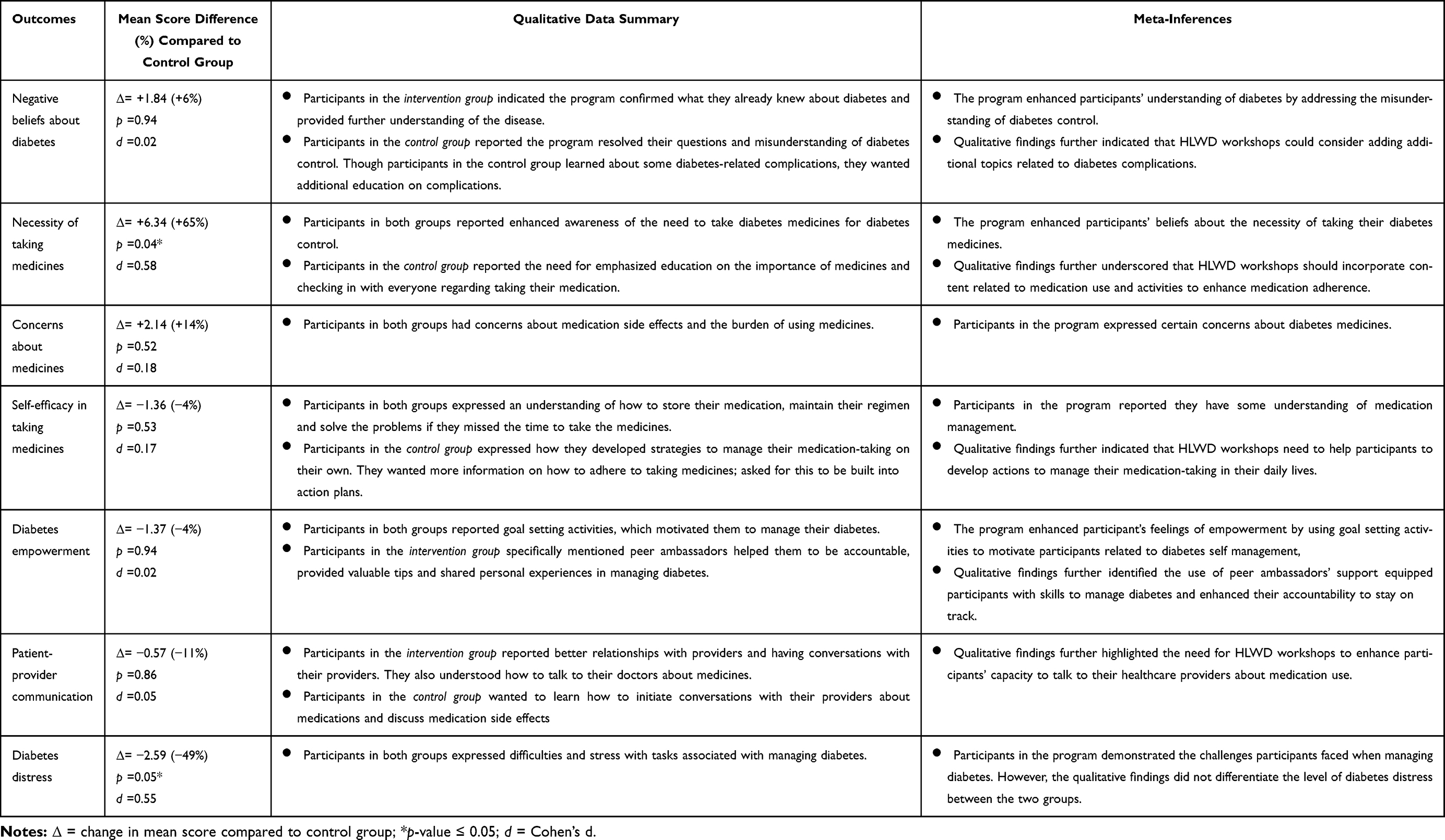 |
Table 5 Joint Display of Psychosocial Outcomes Between the Intervention Group (Peers EXCEL) and the Control Group (Healthy Living with Diabetes, HLWD) at 6 Months |
Community Health Workers
In a debrief with the research team, the community health worker shared his perceptions of the program (Table 4), reflecting on the overall importance of participant’s having an opportunity to connect with another paraprofessional, even when immediate help with a particular social determinant of health was not needed. The community health worker also reported on specific resources requested by program participants. He shared that communicating with participants primarily by phone vs in-person made the interaction more disengaged and felt it was a barrier to providing optimal support. The community health worker provided suggestions for better integrating CHW support in future programs by having a community health worker with a similar racial and ethnic background.
Mixed Methods Integration of Quantitative Results and Qualitative Findings
The joint display demonstrates quantitative psychosocial outcomes with qualitative themes and quotes corresponding to the outcomes in Table 5 to explain and integrate the findings. The qualitative findings of participant perceptions of the necessity of taking medicines were found to further confirm and explain the quantitative results. Increased awareness of the importance of taking diabetes medicines was reported qualitatively in both groups. However, in the control group, participants expressed that they needed more motivation to take medicines by regularly checking in through the group sessions. The additional education session led by the pharmacist focused on medication use received by the intervention group may have enhanced the intervention group’s beliefs about the importance of diabetes medicines strengthening their beliefs about the necessity of taking medicines.
Both groups of participants reported the benefits of using goal-setting activities to motivate diabetes control. In the intervention group, participants further accredited peer support as empowering them with self-management skills and being more accountable On the other hand, though participants in the intervention group reported significantly lower diabetes distress at 6 months, individual difficulties in managing their diabetes during the program still exist and cause certain challenges for participants in both groups.
Due to the exploratory nature of psychosocial outcomes, there are some areas where the qualitative data had discordance with the quantitative data. Though there were no significant differences in negative beliefs about diabetes, concerns about medicines, self-efficacy in taking medicines and patient-provider communication, participants in the control group wanted more topics added to the education sessions. The diabetes-related topics include avoiding diabetes complications and strategies to adhere to diabetes medication. In addition, participants in the control group struggled to initiate conversations with healthcare providers, reporting the need to learn how to discuss medication side effects.
Discussion
This pilot randomized controlled mixed-methods study (Living Well & Empowered trial) explored the benefit of adding a culturally tailored intervention (Peers EXCEL) to a standard diabetes self-management program (HLWD) for Black adults with uncontrolled type 2 diabetes. After 6 months, participants who were randomized to receive the Peers EXCEL intervention reported a clinically meaningful improvement in their A1C, which was statistically significantly lower than for those in the control group. Additionally, when comparing the two groups, the intervention group reported statistically significant higher perception of the necessity of taking medicines and reductions in diabetes distress. However, we did not find statistically significant changes in medication adherence, our secondary outcome, for either group or when comparing the two groups.
Our findings suggest a signal of improvement in A1C after participation in a culturally tailored intervention embedded into a diabetes self-management program. Clinically meaningful reductions in A1C are associated with improvements in numerous health outcomes, including reducing diabetes complications such as diabetic retinopathy, nephropathy, and neuropathy.11 The potential for the Peers EXCEL culturally tailored intervention to contribute to improvements in A1C suggests a promising approach to addressing poor health outcomes among Black adults with diabetes, which is urgently needed. This is consistent with our prior research that has shown that race-congruent Black adult peers with diabetes can provide culturally appropriate informational support and contribute to a signal of improvement in A1C and other psychosocial outcomes.29,30 These results add to the literature on the benefits of race-congruent peer support in which peers can use their own personal, lived experiences with the disease to help others learn successfully.33,53
Inconsistent with our prior research,29,30 we did not find a signal of improvement in medication adherence among either group. This could have been related to potential biases due to the use of a self-reported measure for medication adherence, which depends on respondents accurately recalling behaviors and potentially responding in a socially desirable way. These concerns can lead to overestimating adherence and can contribute to ceiling effect biases in scoring the measure where an unrealistic majority of respondents report very high adherence.54 In semi-structured interviews, participants shared challenges with diabetes distress, which may have affected their medication adherence. This suggests that medication adherence may not have been the pathway through which we saw a signal of change in A1C. Improvements in other factors reported by intervention group participants, such as enhanced patient provider communication and reduced diabetes distress, may have contributed to improvements in other self-management activities, such as nutrition and physical activity, which in turn, may have improved their A1C.
Notable changes in quantitative psychosocial outcomes, including perceptions of the necessity of taking diabetes medicines and diabetes distress were further supported and confirmed by the qualitative findings.
Participants in both groups reported an improved awareness of the necessity of diabetes medicines, yet qualitative findings suggest that participants in the intervention group had a greater awareness of the necessity of taking medicines than those in the control group. This suggests that participation in the diabetes self-management program may have contributed to some improvement in awareness of the necessity of diabetes medicines for all participants, but the added content and peer support for the intervention group likely contributed to their greater awareness about medicines. This is an important finding related to improving glycemic control because race-congruent peer support is especially important and effective for Black adults, who may have fatalistic perceptions about diabetes and medicines influenced by culture, family experiences, and a history of mistreatment and distrust.55 Beliefs about the necessity of prescribed medicines are associated with adhering to treatments,56–58 which in turn can contribute to improvements in glycemic control. This suggests that enhanced awareness of the necessity of medicines may have contributed to better medication adherence and ultimately lowering A1C. This is consistent with several studies which have found that patients who perceive their treatments as necessary are more prone to follow their healthcare provider agreed upon recommendations.57
There was an improvement in diabetes distress within the intervention group from baseline to 6 months, and at 6 months, the intervention group showed a signal of lower diabetes distress compared to the control group. However, the qualitative findings did not differentiate the level of diabetes distress between the two groups. Participants in both groups expressed difficulties and stress with tasks associated with managing diabetes. It could be that intervention participants were expressing similar diabetes related stressors as the control group participants, but through the intervention they were able to find ways of coping with these stressors, so they reported lower diabetes distress after participating in the intervention. It is not realistic that the intervention will eliminate all diabetes-related stressors but rather support individuals in finding ways of coping with those stressors. Indeed, studies have demonstrated that diabetes distress can negatively affect self-care behaviors leading to worse diabetes outcomes.59–61 Our findings suggest that reducing diabetes distress led to enhanced medication adherence and eventual improvement in diabetes health outcomes, such as A1C.
Valuable feedback was elicited from those delivering the HLWD program and the intervention components. Notably, two key points were made about having racially congruent interventionists. First, the Ambassadors reflected on how their role of providing race-congruent peer support for other Black adults living with type 2 diabetes positioned them as advocates for this minoritized group and recognized that was an important initial step towards addressing a dire need in their community, but that this model of support needed to be scaled up. Evidence supports that race-congruent peer support, which is a nonhierarchical, reciprocal relationship created through sharing similar experiences and is aligned with the individual’s cultural and social beliefs,62 is effective at addressing experiences of mistreatment by and feelings of distrust in the healthcare system, and reframing misperceptions regarding medications influenced by culture. For Black adults who may have experienced mistreatment and distrust in the healthcare system, or have misperceptions regarding medications influenced by culture, race-congruent peer support is effective in providing education to target these beliefs.63,64 Second, the CHW noted that CHW support ideally should be provided by someone from the participant’s community. This is consistent with recognized best practices that CHWs ideally should be similar to the communities they work with in terms of demographics and primary language spoken as well as have shared social and structural experiences and challenges.65 This alignment of characteristics and experiences between the CHW and the individuals they are working with facilitates trust building, improves the relevance of information provided, and serves as a bridge to healthcare resources.66
This pilot study has some notable strengths and a few limitations. This study builds on our prior single-arm research designs29,30 by testing Peers EXCEL using a randomized controlled trial design, which is regarded as the gold standard of clinical trial design.67 Our prospective randomization of participants sought to minimize differences in characteristics of the intervention and control groups that may have influenced the outcomes, which is regarded as providing the most definitive evidence for the impact of an intervention on outcome.67 Outcomes related to the feasibility of the trial, such as recruitment and retention rates are reported elsewhere.36 Another strength of our study was the mixed-methods approach involving semi-structured interviews of participants in addition to collecting clinical and quantitative outcomes. Reporting the integration of the quantitative and qualitative findings provides a rich, nuanced interpretation of the study outcomes. Eliciting feedback from the interventionists about their experiences implementing the program was another strength of this trial. Considering their valuable perceptions and suggestions for enhancements to the program can inform future trials as well as future translation of the intervention to real-world settings.
This study also had some limitations. We showed a signal of change in the exploratory outcomes of A1C. However, the results should be interpreted with caution as we had a small sample. The findings may not be generalizable beyond the Midwestern urban setting within which the pilot trial took place. However, future studies could test the same intervention with modest contextual adaptations to better fit a different setting. There was a noteworthy difference in the proportion of males and females in the intervention and control groups, with the intervention group having a large majority of males and the control group having a large majority of females. Because gender could have been associated with other variables such as number of medications taken, this may have been a confounding factor distorting the true effect of the intervention. Our future research will consider stratification approaches to ensure a more equal distribution of males and females within each group. Another potential limitation is that the two HLWD facilitators led the DSME program for both the control and intervention groups. It was not possible to blind the facilitators as to which group was the control and the intervention because the Ambassadors were participants in the intervention group DSME sessions. Having the same facilitators lead each group enhances the likelihood that the session content was standardized across the groups, but their delivery may have been impacted by the awareness of which was the control vs intervention group and they may have inadvertently exposed participants in the control group to elements of the intervention. However, because the peer support was primarily phone based and occurred outside of the DSME weekly sessions, it is less likely that contamination occurred. Future studies will ensure that there are different HLWD facilitators for the control and intervention groups.
This study advances the field towards meeting the long-term goal of reducing diabetes morbidity for Black adults by addressing an unmet critical need to focus on health misperceptions and distrust by providing culturally tailored content and peer support to a population historically beset by harms related to uncontrolled diabetes. The intervention builds upon a widely used evidence-based program, which increases the likelihood that it can be widely disseminated to reduce diabetes-related mortality and morbidity in Black adults in the future. Future adequately powered randomized controlled trials are needed to evaluate the efficacy of Peers EXCEL in improving diabetes outcomes compared to HLWD alone. Once efficacy is established, there is the potential for such an intervention to be scaled up through non-profit agencies licensed to provide the DSME programs, state Departments of Health Services could potentially integrate elements of Peers EXCEL into existing chronic disease self-management partnerships and initiatives, as well as it would be eligible for federal funding for the dissemination/implementation and scalability of evidence-based programs.
Conclusion
The findings from this pilot randomized controlled trial provide a signal of evidence to evaluate the efficacy in a future adequately powered, randomized controlled trial, testing the question of whether the addition of the theory and evidence-informed culturally specific components of Peers EXCEL improve outcomes compared to HLWD alone.
Data Sharing Statement
Deidentified participant data are available upon reasonable request from the corresponding Author and reuse is only permitted with permission.
Ethics Approval and Informed Consent
This randomized controlled mixed methods study was approved by the Minimal Risk Institutional Review Board of the University of Wisconsin-Madison (Study ID: 2020-1061). A written informed consent form was obtained from each participant prior to the trial, which included a consent to publish quotes from qualitative interviews. No identifiers were retained after data transcription. This clinical trial is registered at: https://clinicaltrials.gov/study/NCT05527847. This study complies with the Declaration of Helsinki.
Author Contributions
MM: Writing – Conceptualization, Methodology, Writing - original draft, Writing - review & editing. MW: Formal analysis, Writing – original draft, Writing – review & editing. JD: Formal analysis, Writing – original draft. SS: Formal analysis, Writing – original draft. MAH: Formal analysis, Writing – original draft. AP: Formal analysis, Writing – original draft. LO: Formal analysis, Writing – original draft. TQ: Formal analysis, Writing – original draft. TK: Formal analysis, Writing – original draft. OS: Conceptualization, Methodology, Funding acquisition, Writing – review & editing, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the University of Wisconsin Center for Demography of Health and Aging (CDHA).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. US Centers for Disease Control and Prevention. National Diabetes Statistics Report. 2024. Available from: https://www.cdc.gov/diabetes/php/data-research/index.html.
2. US Department of Health and Human Services, Office of Minority Health. Minority population profile-diabetes. Diabetes and African Americans: US Department of Health and Human Services. 2023. Available from: https://minorityhealth.hhs.gov/diabetes-and-blackafrican-americans.
3. Chow EA, Foster H, Gonzalez V, McIver L. The disparate impact of diabetes on racial/ethnic minority populations. Clin Diabetes. 2012;30(3):130–133. doi:10.2337/diaclin.30.3.130
4. Patel I, Erickson SR, Caldwell CH, et al. Predictors of medication adherence and persistence in Medicaid enrollees with developmental disabilities and type 2 diabetes. Res Soc Admin Pharm. 2016;12(4):592–603. doi:10.1016/j.sapharm.2015.09.008
5. Schectman JM, Nadkarni MM, Voss JD. The association between diabetes metabolic control and drug adherence in an indigent population. Diabetes Care. 2002;25(6):1015–1021. doi:10.2337/diacare.25.6.1015
6. Mann DM, Ponieman D, Leventhal H, Halm EA. Predictors of adherence to diabetes medications: the role of disease and medication beliefs. J Behav Med. 2009;32(3):278–284. doi:10.1007/s10865-009-9202-y
7. Shenolikar RA, Balkrishnan R, Camacho FT, Whitmire JT, Anderson RT. Race and medication adherence in Medicaid enrollees with type-2 diabetes. J Nat Med Assoc. 2006;98(7):1071–1077.
8. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med. 2006;166(17):1836–1841. doi:10.1001/archinte.166.17.1836
9. Lawrence DB, Ragucci KR, Long LB, Parris BS, Helfer LA. Relationship of oral antihyperglycemic (Sulfonylurea or Metformin) medication adherence and hemoglobin A1c goal attainment for HMO patients enrolled in diabetes disease management program. J Manage Care Pharm. 2006;12(6):466–471.
10. Rozenfeld Y, Hunt JS, Plauschinat C, Wang KS. Oral antidiabetic medication adherence and glycemic control in managed care. Am J Manage Care. 2008;14(2):71–75.
11. ElSayed NA, Aleppo G, Bannuru RR; American Diabetes Association. Professional Practice Committee. 6. Glycemic goals and hypoglycemia: standards of care in Diabetes—2024. Diabetes Care. 2024;47(Suppl1):S111–S125. doi:10.2337/dc24-S006
12. Hill-Briggs F, Gary TL, Bone LR, Hill MN, Levine DM, Brancati FL. Medication adherence and diabetes control in urban African Americans with type 2 diabetes. Health Psychol. 2005;24(4):349–357. doi:10.1037/0278-6133.24.4.349
13. Krapek K, King K, Warren SS, et al. Medication adherence and associated hemoglobin A1c in type 2 diabetes. Ann Pharmacother. 2004;38(9):1357–1362. doi:10.1345/aph.1D612
14. Heisler M. Overview of peer support models to improve diabetes self-management and clinical outcomes. Diabetes Spect. 2007;20(4):214–221. doi:10.2337/diaspect.20.4.214
15. Hu D, Juarez DT, Yeboah M, Castillo TP. Interventions to increase medication adherence in African-American and Latino populations: a literature review. Hawai J Med Pub Health. 2014;73(1):11–18.
16. Gonzalez JS, Tanenbaum ML, Commissariat PV. Psychosocial factors in medication adherence and diabetes self-management: implications for research and practice. Amer Psychol. 2016;71(7):539–551. doi:10.1037/a0040388
17. Cunningham AT, Crittendon DR, White N, Mills GD, Diaz V, LaNoue MD. The effect of diabetes self-management education on HbA1c and quality of life in African-Americans: a systematic review and meta-analysis. BMC Health Serv Res. 2018;18(1):367. doi:10.1186/s12913-018-3186-7
18. Lynch EB, Mack L, Avery E, et al. Randomized trial of a lifestyle intervention for urban low-income African Americans with type 2 diabetes. J Gen Int Med. 2019;34(7):1174–1183. doi:10.1007/s11606-019-04894-y
19. Hawkins J, Mitchell J, Piatt G, Ellis D. Older African American men’s perspectives on factors that influence type 2 diabetes self-management and peer-led interventions. Geriatrics. 2018;3(3):38. doi:10.3390/geriatrics3030038
20. Lorig K, Ritter PL, Turner RM, English K, Laurent DD, Greenberg J. Benefits of diabetes self-management for health plan members: a 6-month translation study. J Med Internet Res. 2016;18(6):e164. doi:10.2196/jmir.5568
21. Lorig K, Ritter PL, Turner RM, English K, Laurent DD, Greenberg J. A diabetes self-management program: 12-month outcome sustainability from a nonreinforced pragmatic trial. J Med Internet Res. 2016;18(12):e322. doi:10.2196/jmir.6484
22. Wadi NM, Asantewa-Ampaduh S, Rivas C, Goff LM. Culturally tailored lifestyle interventions for the prevention and management of type 2 diabetes in adults of Black African ancestry: a systematic review of tailoring methods and their effectiveness. Public Health Nutr. 2022;25(2):422–436. doi:10.1017/S1368980021003682
23. Peterson EB, Chou W-YS, Rising C, Gaysynsky A. The role and impact of health literacy on peer-to-peer health communication. Stud Health Technol Inform. 2020;269:497–510. doi:10.3233/SHTI200058
24. Salud MA, Gallardo JI, Dineros JA, et al. People’s initiative to counteract misinformation and marketing practices: the Pembo, Philippines, breastfeeding experience, 2006. J Hum Lact. 2009;25(3):341–349. doi:10.1177/0890334409334605
25. Williams IC, Utz SW, Hinton I, Yan G, Jones R, Reid K. Enhancing diabetes self-care among rural African Americans with diabetes: results of a two-year culturally tailored intervention. Diabetes Educ. 2014;40(2):231–239. doi:10.1177/0145721713520570
26. Peña-Purcell NC, Jiang L, Ory MG, Hollingsworth R. Translating an evidence-based diabetes education approach into rural African-American communities: the “wisdom, power, control” program. Diabetes Spectr. 2015;28(2):106–115. doi:10.2337/diaspect.28.2.106
27. Samuel-Hodge CD, Keyserling TC, France R, et al. A church-based diabetes self-management education program for African Americans with type 2 diabetes. Prev Chronic Dis. 2006;3(3):A93.
28. Fisher W, Fisher J, Harman J. The informational-motivation-behavioral skills model as a general model of health behavior change: theoretical approaches to individual level change. In: Suls J, Wallston K, editors. Social Psychological Foundations of Health and Illness. Blackwell Publishing; 2003:127–153.
29. Shiyanbola OO, Maurer M, Mott M, et al. A feasibility pilot trial of a peer-support educational behavioral intervention to improve diabetes medication adherence in African Americans. Pilot Feasibility Stud. 2022;8(1):240. doi:10.1186/s40814-022-01198-7
30. Shiyanbola OO, Maurer M, Schwerer L, et al. A culturally tailored diabetes self-management intervention incorporating race-congruent peer support to address beliefs, medication adherence and diabetes control in African Americans: a pilot feasibility study. Patient Prefer Adherence. 2022;16:2893–2912. doi:10.2147/PPA.S384974
31. Tang TS, Funnell MM, Gillard M, Nwankwo R, Heisler M. Training peers to provide ongoing diabetes self-management support (DSMS): results from a pilot study. Patient Educ Couns. 2011;85(2):160–168. doi:10.1016/j.pec.2010.12.013
32. Dennis CL. Peer support within a health care context: a concept analysis. Int J Nurs Stud. 2003;40(3):321–332. doi:10.1016/S0020-7489(02)00092-5
33. Ruddock JS, Poindexter M, Gary-Webb TL, Walker EA, Davis NJ. Innovative strategies to improve diabetes outcomes in disadvantaged populations. Diabet Med. 2016;33(6):723–733. doi:10.1111/dme.13088
34. Williams EM, Hyer JM, Viswanathan R, et al. Peer-to-peer mentoring for African American women with Lupus: a feasibility pilot. Arthritis Care Res. 2018;70(6):908–917. doi:10.1002/acr.23412
35. Shiyanbola OO, Maurer MA, Wen MJ. Protocol for a pilot randomized controlled mixed methods feasibility trial of a culturally adapted peer support and self-management intervention for African Americans. Pharmacy. 2023;11(1):2.
36. Wen MJ, Maurer M, Pickard AL, Hansen M, Shiyanbola OO. A pilot mixed methods randomized control trial investigating the feasibility and acceptability of a culturally tailored intervention focused on beliefs, mistrust and race-congruent peer support for Black adults with diabetes. Front Public Health. 2025;13:1474027. doi:10.3389/fpubh.2025.1474027
37. Lorig K, Laurent D, González V, Sobel D, Minor M, Gecht-Silver M. Living a Healthy Life with Chronic Conditions: Self-Management of Heart Disease, Arthritis, Diabetes, Depression, Asthma, Bronchitis, Emphysema and Other Physical and Mental Health Conditions.
38. Shiyanbola OO, Brown CM, Ward EC. “I did not want to take that medicine”: African-Americans’ reasons for diabetes medication nonadherence and perceived solutions for enhancing adherence. Patient Prefer Adherence. 2018;12:409–421. doi:10.2147/PPA.S152146
39. Shiyanbola OO, Ward E, Brown C. Sociocultural influences on African Americans’ representations of type 2 diabetes: a qualitative study. Ethn Dis. 2018;28(1):25–32. doi:10.18865/ed.28.1.25
40. Shiyanbola OO, Kaiser BL, Thomas GR, Tarfa A. Preliminary engagement of a patient advisory board of African American community members with type 2 diabetes in a peer-led medication adherence intervention. Res Involv Engagem. 2021;7(1):4. doi:10.1186/s40900-020-00245-y
41. Maurer MA, Shiyanbola OO, M ML, M J. Engaging patient advisory boards of African American community members with type 2 diabetes in implementing and refining a peer-led medication adherence intervention. Pharmacy. 2022;10(2):37. doi:10.3390/pharmacy10020037
42. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 Statement: updated guideline for reporting randomised trials. BMJ. 2025;388:e081123. doi:10.1136/bmj-2024-081123
43. PTS Diagnostics. A1CNow+. Available from: https://www.ptsdiagnostics.com/a1cnow-plus-system/.
44. Mayberry LS, Gonzalez JS, Wallston KA, Kripalani S, Osborn CY. The ARMS-D out performs the SDSCA, but both are reliable, valid, and predict glycemic control. Diabet Res Clin Pract. 2013;102(2):96–104. doi:10.1016/j.diabres.2013.09.010
45. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
46. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
47. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the Self-efficacy for appropriate medication use scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Measure. 2007;15(3):203–219. doi:10.1891/106137407783095757
48. Anderson RM, Fitzgerald JT, Gruppen LD, Funnell MM, Oh MS. The diabetes empowerment scale-short form (DES-SF). Diabetes Care. 2003;26(5):1641–1642. doi:10.2337/diacare.26.5.1641-a
49. Lerman CE, Brody DS, Caputo GC, Smith DG, Lazaro CG, Wolfson HG. Patients’ perceived involvement in care scale. J Gen Intern Med. 1990;5(1):29–33. doi:10.1007/BF02602306
50. Fisher L, Glasgow RE, Mullan JT, Skaff MM, Polonsky WH. Development of a brief diabetes distress screening instrument. Ann Fam Med. 2008;6(3):246–252. doi:10.1370/afm.842
51. Lumivero. NVivo (Version 12). 2018. Available from: https://community.lumivero.com/s/topic/0TOJw0000000SabOAE/nvivo?language=en_US.
52. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect of glycemic control. Patient Educ Couns. 2016;99(6):926–943. doi:10.1016/j.pec.2015.11.003
53. Heisler M, Vijan S, Makki F, Piette JD. Diabetes control with reciprocal peer support versus nurse care management: a randomized trial. Ann Intern Med. 2010;153(8):507–515. doi:10.7326/0003-4819-153-8-201010190-00007
54. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/s13142-015-0315-2
55. Long JA, Jahnle EC, Richardson DM, Loewenstein G, Volpp KG. Peer mentoring and financial incentives to improve glucose control in African American veterans: a randomized trial. Ann Int Med. 2012;156(6):416–424. doi:10.7326/0003-4819-156-6-201203200-00004
56. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
57. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
58. Cea-Calvo L, Marín-Jiménez I, de Toro J, et al. Association between non-adherence behaviors, patients’ experience with healthcare and beliefs in medications: a survey of patients with different chronic conditions. Curr Med Res Opin. 2020;36(2):293–300. doi:10.1080/03007995.2019.1676539
59. Owens-Gary MD, Zhang X, Jawanda S, Bullard KM, Allweiss P, Smith BD. The importance of addressing depression and diabetes distress in adults with type 2 diabetes. J Gen Intern Med. 2019;34(2):320–324. doi:10.1007/s11606-018-4705-2
60. Brown SA, García AA, Brown A, et al. Biobehavioral determinants of glycemic control in type 2 diabetes: a systematic review and meta-analysis. Patient Educ Couns. 2016;99(10):1558–1567. doi:10.1016/j.pec.2016.03.020
61. Walker RJ, Gebregziabher M, Martin-Harris B, Egede LE. Understanding the influence of psychological and socioeconomic factors on diabetes self-care using structured equation modeling. Patient Educ Couns. 2015;98(1):34–40. doi:10.1016/j.pec.2014.10.002
62. Perry E, Swartz J, Brown S, Smith D, Kelly G, Swartz R. Peer mentoring: a culturally sensitive approach to end-of-life planning for long-term dialysis patients. Am J Kidney Dis. 2005;46(1):111–119. doi:10.1053/j.ajkd.2005.03.018
63. Armstrong K, McMurphy S, Dean LT, et al. Differences in the patterns of health care system distrust between blacks and whites. J Gen Intern Med. 2008;23(6):827–833. doi:10.1007/s11606-008-0561-9
64. Gamble VN. Under the shadow of Tuskegee: African Americans and health care. Am J Public Health. 1997;87(11):1773–1778. doi:10.2105/AJPH.87.11.1773
65. Cervantes L, Robinson BM, Steiner JF, Myaskovsky L. Culturally concordant community-health workers: building sustainable community-based interventions that eliminate kidney health disparities. J Am Soc Nephrol. 2022;33(7):1252–1254. doi:10.1681/ASN.2022030319
66. Ross R, Goldstein N. Enhancing care for diverse communities: the role of community health workers. Center to Advance Palliative Care Health Equity Blog; 2024. Available from: https://www.capc.org/blog/enhancing-care-for-diverse-communities-the-role-of-community-health-workers/.
67. Zabor EC, Kaizer AM, Hobbs BP. Randomized controlled trials. Chest. 2020;158(1S):S79–S87. doi:10.1016/j.chest.2020.03.013
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.