Back to Journals » International Journal of General Medicine » Volume 16
Invasive Candidiasis in Patients with Solid Tumors: A Single-Center Retrospective Study
Received 3 March 2023
Accepted for publication 30 May 2023
Published 13 June 2023 Volume 2023:16 Pages 2419—2426
DOI https://doi.org/10.2147/IJGM.S411006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xueying Bai, Ji Luo
Department of Thoracic Surgery, The First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
Correspondence: Xueying Bai, Email [email protected]
Background: Invasive candidiasis (ICs) is one of the common causes of death in patients with solid tumors. However, studies on the clinical characteristics of ICs with solid tumors are limited.
Methods: The purpose of this study was to retrospectively analyse the clinical characteristics, laboratory results and risk factor prediction of inpatients with ICs and solid tumors. We reviewed the clinical data and candida specimen information of hospitalized patients diagnosed with solid tumors combined with ICs at the First Hospital of China Medical University from January 2016 to December 2020. Multivariate logistic regression analysis was used to assess the prognostic factors associated with mortality in these patients.
Results: A total of 243 ICs patients with solid tumors were included in this study. The average ± SD age was 62.8 ± 11.7 (range: 27– 93 years old), of which nearly 41% were ≥ 65 years old (99/243, 40.7%), and most were male (162/243, 66.6%). Most patients had malignant tumors of the digestive system. The most common candida was Candida parapsilosis (101/243, 41.5%), followed by Candida guilliermondii (83/243, 34.1%), Candida albicans (32/243, 13.1%), Candida glabrata (17/243, 6.9%), Candida tropicalis (7/243, 2.8%) and Candida krusei (3/243, 1.2%). Multivariate logistic regression analysis showed that the length of stay in the ICU, urinary catheter, total parenteral nutrition, stay in the ICU, renal failure and neutrophil count were prognostic factors related to death.
Conclusion: In this study, based on the clinical data of solid tumor patients with ICs in the past 5 years, the results showed that the length of stay in the ICU, urinary catheter, total parenteral nutrition, stay in the ICU, renal failure and neutrophil count were identified as the main prognostic factors. This study can be used to help clinicians carry out early intervention for high-risk patients.
Keywords: invasive candidiasis, solid tumors, epidemic, single center, prognosis
Introduction
Invasive candidiasis (ICs) is one of the most common hospital bloodstream infections1,2 and easily occurs in patients who have been hospitalized for a long time, immunotherapy and organ transplantation.3–5 The infection rate of ICs in patients with solid tumors continues to increase due to a more active multidrug chemotherapy scheme, increased use of antibiotics and use of high-dose immunosuppressants.6–8 According to research reports from different cohorts of solid tumor patients, the invasive candidiasis infection rate of solid tumor patients ranges from 1.3% to 38.0%.6 In patients with solid tumors, immune deficiency and disruption of gastrointestinal mucosal integrity are the reasons for the increased risk of invasive candidiasis infection.9 In healthy individuals, candida and other microorganisms mainly play physiological functions and contribute to individual homeostasis, however, in patients with solid tumors, candida and other microorganisms play different roles and may play a role in promoting the progression of solid tumors.10 And patients with solid tumors may develop neutropenia, further leading to poor prognosis.11 According to previous research results, the most common invasive candida infection in patients with solid tumors is Candida albicans, followed by Candida parapsilosis, tropical Candida and Candida glabrata, but it is changing like non Candida albicans infection.12 For the selection of anticandida drugs, changes in candida species have clinical significance, as non Candida albicans are often resistant to fluconazole.13
The mortality of ICs patients is very high, which has attracted increasing attention in the medical field. Due to the limited number of studies, many aspects of ICs are still poorly understood. In this study, we collected the data of 243 solid tumor patients with ICs, described their clinical characteristics and biochemical tests in detail, and finally used multivariate logistic regression to identify the prognostic factors related to death.
Method
Patient Selection
The data come from the electronic medical record system of the ward and are extracted from the period from January 2016 to December 2020 of the First Hospital of China Medical University. The clinical data and candida specimen information of inpatients with solid tumors and ICs were collected. The information collected and recorded included age, sex, length of stay, antibiotic application, chemotherapy, surgery, basic diseases, admission to the intensive care unit (ICU) and other relevant clinical information.
Criteria for Study Inclusion
We collected all Candida isolates recovered from sterile body fluids and blood for inclusion in this study (EORTC/MSG 2008). The data collected included the tumor type, baseline characteristics, hematological diagnosis and chemotherapy, risk factors for ICs, clinical characteristics of ICs, candida detection results, anticandida prevention and treatment, and survival status at discharge. Document the management of patients receiving anticandida prophylaxis and treatment. Including the date and nature of treatment changes and survival status at discharge. Each inpatient represents a case.
Microbiological Test
Sterile body fluid samples (8–10 mL) were collected and incubated for 5 days. Transfer the positive sample to the blood agar plate and then pass the bacterial and candida isolates at 35 °C for 48–72 hours. Gram staining and microscopic examination were performed simultaneously. Strain identification (bacterial isolates and candida isolates) was carried out on a VITEK 2 Compact (Bio Merieux SA, Marcy l’etoile, France).
ATB FUNGUS 3 (Bio Merieux SA, Marcy l’etoile, France) was used for the drug sensitivity test. The drug sensitivity test was performed by applying ATB Fungus 3 yeast-like fungi to the drug sensitivity test box in strict accordance with the National Clinical Trial Operating Procedures and reagent instructions. The standard anticandida susceptibility testing was performed according to CLSI M27-A3. Essential agreement (EA) is defined as the percent of all Sensititre™ YeastOne™ MIC results within one 2-fold dilution of the CLSI MIC result. Candida krusei ATCC 6258 and Candida parapsilosis ATCC 22019 were selected for quality control. The epidemiological cutoff values (ECV) and clinical breakpoints of anticandida against C. duobushaemulonii in vitro have been established by the CLSI. Among them, fluconazole MICs of greater than 32 μg/mL is considered as non-WT for C. duobushaemulonii and C. auris. Flucytosine MIC values (≥32 μg/mL) were interpreted according to the CLSI document M27-S3. In addition, MIC of ≥2 μg/mL was used for interpreting “resistance” of amphotericin B.
Definition
Prolonged hospitalization was defined as a hospital stay longer than 10 days.
Statistical Analysis
MedCalc software 19.3.1 (MedCalc Software Ltd, Ostend, Belgium) was used for statistical analysis. The quantitative data with a nonnormal distribution are expressed as the median and quartile range [M (P25, P75)], and the Mann‒Whitney test was used for comparative analysis between groups. Qualitative data are described by relative numbers and compared between groups by χ^2 Inspection. Logistic regression analysis was used for multivariate analysis. p < 0.05 was required for differences to be considered statistically significant.
Result
General Information
A total of 243 ICs patients with solid tumors were included in this study. The average ± SD age was 62.8 ± 11.7 (range: 27–93 years old), of which nearly 41% were ≥ 65 years old (99/243, 40.7%), and most were male (162/243, 66.6%). Most patients had malignant tumors of the digestive system, such as gastric cancer (66/243, 27.2%), colon cancer (46/243, 18.9%), rectal cancer (34/243, 14.0%), pancreatic cancer (22/243, 9.1%), duodenal carcinoma (19/243, 7.8%), bile duct cancer (15/243, 6.2%), liver cancer (8/243, 3.3%), and esophageal cancer (6/243, 2.5%).
The most common candida in our sample was Candida parapsilosis (101/243, 41.5%), followed by Candida guilliermondii (83/243, 34.1%), Candida albicans (32/243, 13.1%), Candida glabrata (17/243, 6.9%), Candida tropicalis (7/243, 2.8%) and Candida krusei (3/243, 1.2%). In addition, 184 (75.7%) patients received recent surgery (within 2 weeks) before data collection, 100 (39.1%) patients stayed in the ICU during hospitalization, 95 (39.0%) patients had bacterial blood infections, 82 (33.7%) patients had persistent invasive candidiasis, and 33 (13.5%) patients died within 30 days. During hospitalization, 92 (37.8%) patients used three or more types of antibiotics, and 223 (91.7%), 156 (64.1%), and 156 (64.1%) patients used catheters, gastric tubes, and central venous catheters, respectively. Supplementary Table 1 contains a summary of the clinical characteristics and inducing factors of patients included in this study.
In vitro Anticandida Susceptibility Test
The sensitivity test results of 243 isolates to five anticandida drugs are shown in Supplementary Table 2. Among the isolates tested, 27/243 (11.1%) were resistant to at least one anticandida agent. For fluconazole, 226/243 (93.0%) Candida strains were found to be susceptible. The susceptible of Candida glabrata isolates to fluconazole was the highest in non-susceptible (12/17, 70.6%).
Risk Factors for Candida albicans and Non-Candida albicans Infection
The comparison of demographic and clinical characteristics of patients with Candida albicans and non-C. albicans infection is summarized in Table 1. The presence of total parenteral nutrition (78.1% vs 97.6%, P=0.0002), recent surgery (59.3% vs 78.1%, P=0.0271), gastric tube (40.6% vs 67.7%, P=0.0049) and drainage catheter (59.3% vs 89.0%, P<0.0001) was more common in patients with non-C. albicans infection. Compared with patients with non-C. albicans infection, patients with C. albicans infection had longer hospitalization times (59 days vs 37.7 days, P=0.001). In terms of laboratory examination, the leukocyte count and neutrophil counts of Candida albicans patients were higher, and the median white blood cell and neutrophil counts exceeded the normal values.
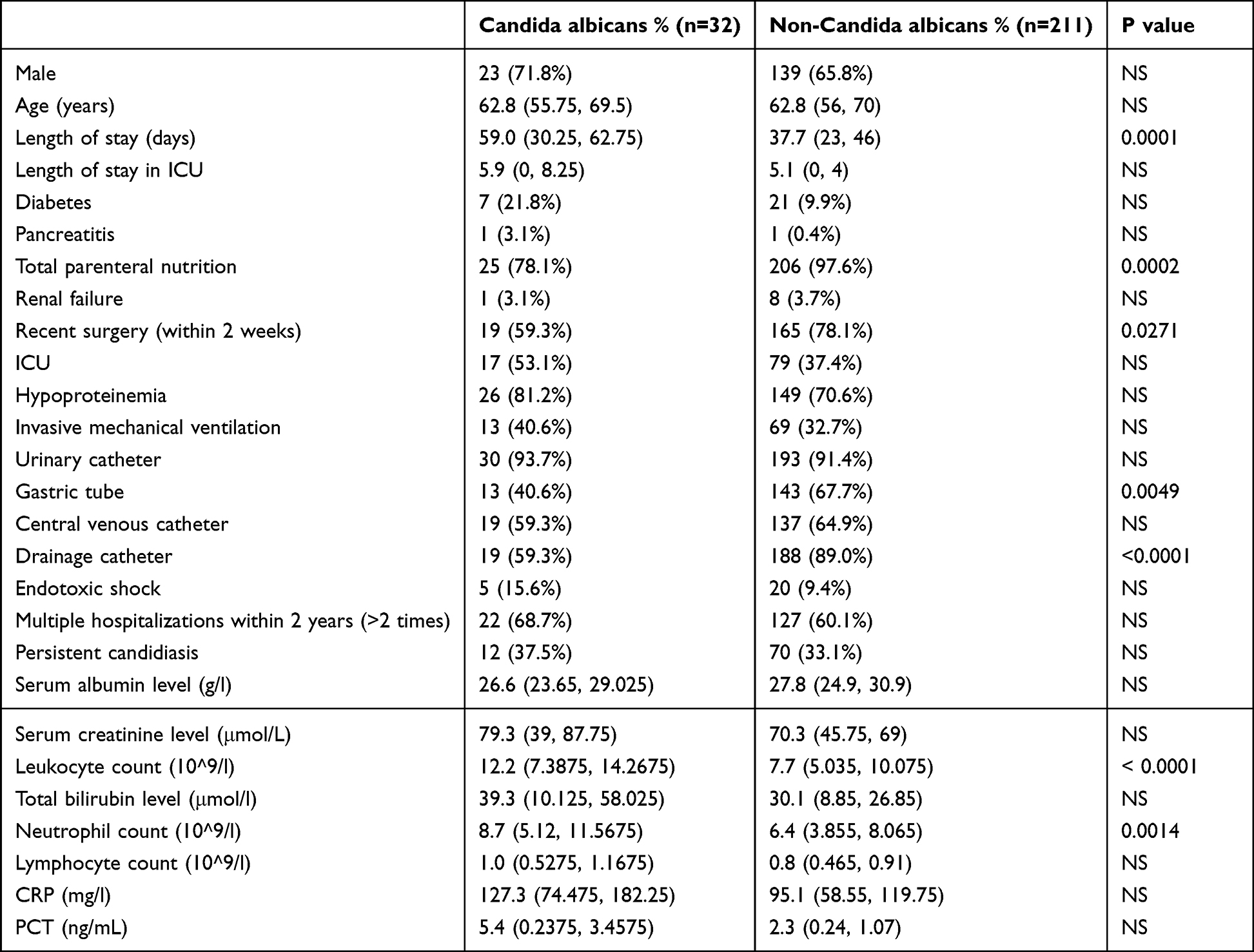 |
Table 1 Risk Factors for Candida albicans and Non-Candida albicans Infections |
Analysis of Risk Factors for Survived - Deceased in Patients
The demographic and clinical characteristics of survived - deceased of patients are listed in Table 2. Surviving patients are usually those who stay in the ICU for a longer time, and they are less often accompanied by renal failure, invasive mechanical ventilation, endotoxic shock, multiple hospitalizations within 2 years, and persistent candidiasis. Surviving patients had lower serum creatinine levels, leukocyte counts, total bilirubin levels, neutrophil counts and PCT (procalcitonin) levels. Patients who passed away tended to have a higher usage of total parenteral nutrition, urinary catheters, and drainage catheters, as well as having undergone more recent surgeries.
 |
Table 2 Comparisons of Patients That Survived versus Died |
Prognostic Factors Associated with Deceased
In solid tumors patients with ICs, in univariate analysis, death was the dependent variable (0=survived, 1=deceased), length of ICU stay, total parenteral nutrition, renal failure, recent surgery, admission to ICU, invasive mechanical ventilation, urinary catheter, drainage catheter, endotoxic shock, multiple hospitalizations within 2 years, persistent candidiasis, serum creatinine level, leukocyte count, total bilirubin level, neutrophil count, and PCT were used as independent variables for logistic regression analysis. The results showed that hospitalization time in the ICU, urinary catheters, total parenteral nutrition, admission to the ICU, renal failure and neutrophil count were prognostic factors related to death (Table 3). Next, we conducted factor analysis on the 6 results obtained from logistic regression analysis, and obtained a risk score of Logit (P): +for each patient based on the 6 factors of “Length of stay in ICU”, “Urinary Catheter”, “Total parental nutrition”, “ICU”, “Renal failure”, and “Neutral count” for diagnosis of “whether to die”. Logit (P): + represents a greater tendency towards deceased, - represents a smaller tendency towards deceased, resulting in the model:
 |
Table 3 Logistic Regression Analysis of Prognostic Factors Associated with Death |
Logit(P) = 2.504 + 0.029 * (Length_of_stay_in_ICU) + 0.191 * (Neutrophil_count) + 3.257 * (Renal_failure) + 3.213 * (Stay_in_ICU) - 5.330 * (Total_parenteral_nutrition) - 4.067 * (Urinary_catheter).
Conclusion
In ICs patients with solid tumors, stay in ICU is a common complication that is associated with poor prognosis. This study aimed to investigate the clinical characteristics, pathogen distribution, and risk factors for death in 243 solid tumor patients with ICs. The average age of these patients was 62.8 ± 11.7 years, with nearly 41% being ≥ 65 years old. Most of the patients were male (66.6%) and had malignant tumors of the digestive system, such as gastric, colon, rectal, pancreatic, duodenal, bile duct, liver, and esophageal cancers. Candida parapsilosis was found to be the most common pathogen, followed by Candida guilliermondii, Candida albicans, Candida glabrata, Candida tropicalis, and Candida krusei. These findings are consistent with those of recent studies conducted in Italy and the United States.14–16
Amphotericin B was the most sensitive anticandida agent in our study. According to the anticandida susceptibility test, candida strains isolated from 243 patients were not resistant to amphotericin B, which was consistent with another study on anticandida susceptibility of candida.17,18 Although fluconazole is the most commonly used anticandida drug, our results show that 7.4% (18/243) of candida are resistant to fluconazole, which is the drug with the strongest resistance. This is similar to the results of a recent study on candida resistance.19
According to the results of logistic regression analysis in this study, we found that the most important predictors of death in solid tumor patients with ICs included the length of stay in the ICU, urinary catheters, total parenteral nutrition, admission to the ICU, renal failure and neutrophil count. Length of stay in ICU, Stay in ICU, Renal failure, and Neutral count are factors that can increase the risk of patient mortality. Total parental nutrition and Urinary Catheter can prevent patient death. Some studies have shown that the overall mortality of hospitalized patients increases with increasing length of stay in the ICU, which may be due to the complications caused by long-term intensive care.20,21 In patients with candidemia, the mortality rate of hospitalized patients increases with the increase in the use rate of urinary catheters. Some recent studies have also proven our view.22,23 Total parenteral nutrition is also an important risk factor for candidiasis. The results of two multicenter prospective controlled clinical trials show that total parenteral nutrition is an independent risk factor for candidiasis.24,25 Although there is no direct literature proving that the death rate of solid tumors patients with ICs will increase when they stay in the ICU during hospitalization, there are studies proving that the prolonged stay in the ICU will lead to the risk of invasive candidiasis.21,26 Perhaps this is one of the reasons for the increase in mortality. Patients with renal failure are often accompanied by dialysis or renal transplantation, which is also a risk factor for candidaemia infection and may lead to an increase in mortality.27 In a study on bloodstream infection in patients with hematological malignancies, neutropenia was the most common risk factor, and infection will develop rapidly, leading to poor prognosis.28
The mortality rate of invasive candidiasis varies in different regions. In a study in Brazil, the mortality rate of cancer patients with invasive candidiasis was 49.4%.29 In a study in Europe, the mortality rate of patients with invasive candidiasis associated with cancer was 39%.30 Our data shows that the mortality rate of patients with solid tumors accompanied by invasive candidiasis is 13.6%. And the mortality rate of infection varies among different types of Candida. In a French study, cancer patients infected with Candida krusei had the highest mortality rate, while those infected with Candida parapsilosis had the lowest mortality rate.31 This is similar to our research results. Our data shows that the mortality rate from high to low is Candida krusei (2/3, 66.67%), Candida tropicalis (3/7, 42.86%), Candida albicans (9/32, 28.13%), Candida glabrata (4/17, 23.53%), Candida parapsilosis (9/101, 8.91%), and Candida guilliermondii (6/83, 7.23%).
However, this study has some limitations. First, this was a single-center study. The results may be affected by geographical location, hospital management strategies, infection control policies and other factors. Second, limited samples and regional differences may reveal some key factors. Therefore, a large-scale, multicenter prospective study should be further carried out to verify the results of this study.
Conclusion
We have reported for the first time the epidemiological data of solid tumors combined with invasive candidiasis in patients over the past 5 years. Although available clinical data is limited, these findings will greatly assist clinical healthcare workers in identifying, preventing, and treating ICs in patients with solid tumors.
Data Sharing Statement
The data supporting the findings of this study from the corresponding author upon request.
Ethical Approval
The study was conducted in accordance with the declaration of Helsinki. This study was approved by The Human Ethics Review Committee of the First Hospital of China Medical University (no. 2021-260). The ethics review board of the First Hospital of China Medical University exempted the acquisition of informed consent because this was a retrospective study. Patients’ data confidentiality was fully respected during data collection and the preparation of the manuscript.
Consent Procedures
Written informed consent from the patients was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Acknowledgments
The authors thank the reviewers for their helpful comments on our report.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Li Y, Gao Y, Niu X, et al. A 5-year review of invasive fungal infection at an academic medical center. Front Cell Infect Microbiol. 2020;10:553648. doi:10.3389/fcimb.2020.553648
2. Enoch DA, Yang H, Aliyu SH, et al. The changing epidemiology of invasive fungal infections. Methods Mol Biol. 2017;1508:17–65. doi:10.1007/978-1-4939-6515-1_2
3. Ferrarese A, Cattelan A, Cillo U, et al. Invasive fungal infection before and after liver transplantation. World J Gastroenterol. 2020;26(47):7485–7496. doi:10.3748/wjg.v26.i47.7485
4. Badiee P, Hashemizadeh Z. Opportunistic invasive fungal infections: diagnosis & clinical management. Indian J Med Res. 2014;139(2):195–204.
5. Gavaldà J, Meije Y, Len Ó, et al. Infección fúngica invasora en el trasplante de órgano sólido [Invasive fungal infection in solid organ transplant]. Enferm Infecc Microbiol Clin. 2012;30(10):645–653. Spanish. doi:10.1016/j.eimc.2012.09.004
6. Ruijters VJ, Oosterom N, van der Perk M, et al. Clinical characteristics of invasive fungal infections in pediatric oncology patients with solid tumors. J Pediatr Hematol Oncol. 2021;43(3):e408–e413. doi:10.1097/MPH.0000000000001761
7. Li Y, Wu Y, Gao Y, et al. Machine-learning based prediction of prognostic risk factors in patients with invasive candidiasis infection and bacterial bloodstream infection: a singled centered retrospective study. BMC Infect Dis. 2022;22(1):150. doi:10.1186/s12879-022-07125-8
8. Dandachi D, Wilson Dib R, Fernández-Cruz A, et al. Invasive pulmonary aspergillosis in patients with solid tumours: risk factors and predictors of clinical outcomes. Ann Med. 2018;50(8):713–720. doi:10.1080/07853890.2018.1518581
9. Zirkel J, Klinker H, Kuhn A, et al. Epidemiology of Candida blood stream infections in patients with hematological malignancies or solid tumors. Med Mycol. 2012;50(1):50–55. doi:10.3109/13693786.2011.587211
10. Pfisterer N, Lingens C, Heuer C, et al. The microbiome in PDAC-vantage point for future therapies. Cancers. 2022;14(23):5974. doi:10.3390/cancers14235974
11. Koçak U, Rolston KV, Mullen CA. Fever and neutropenia in children with solid tumors is similar in severity and outcome to that in children with leukemia. Support Care Cancer. 2002;10(1):58–64. doi:10.1007/s005200100277
12. De Rosa FG, Busca A, Capparella MR, et al. Invasive candidiasis in patients with solid tumors treated with anidulafungin: a post hoc analysis of efficacy and safety of six pooled studies. Clin Drug Investig. 2021;41(6):539–548. doi:10.1007/s40261-021-01024-7
13. Pfaller MA, Diekema DJ, Gibbs DL, et al. Results from the ARTEMIS DISK Global Antifungal Surveillance Study, 1997 to 2007: a 10.5-year analysis of susceptibilities of Candida Species to fluconazole and voriconazole as determined by CLSI standardized disk diffusion. J Clin Microbiol. 2010;48(4):1366–1377. doi:10.1128/JCM.02117-09
14. Li J, Li Y, Gao Y, et al. Prediction of prognostic risk factors in patients with invasive candidiasis and cancer: a single-centre retrospective study. Biomed Res Int. 2022;2022:7896218. doi:10.1155/2022/7896218
15. Orsetti E, Brescini L, Mazzanti S, et al. Central venous catheter unrelated candidemia influences the outcome of infection in patients with solid tumors. Eur J Clin Microbiol Infect Dis. 2019;38(8):1499–1505. doi:10.1007/s10096-019-03578-z
16. Tattevin P, Revest M, Lefort A, et al. Fungal endocarditis: current challenges. Int J Antimicrob Agents. 2014;44(4):290–294. doi:10.1016/j.ijantimicag.2014.07.003
17. Marak MB, Dhanashree B. Antifungal susceptibility and biofilm production of candida spp. isolated from clinical samples. Int J Microbiol. 2018;2018:7495218. doi:10.1155/2018/7495218
18. Gao Y, Tang M, Li Y, et al. Machine-learning based prediction and analysis of prognostic risk factors in patients with candidemia and bacteraemia: a 5-year analysis. PeerJ. 2022;10:e13594. doi:10.7717/peerj.13594
19. Tortorano AM, Prigitano A, Morroni G, et al. Candidemia: evolution of drug resistance and novel therapeutic approaches. Infect Drug Resist. 2021;14:5543–5553. doi:10.2147/IDR.S274872
20. Pintado MC, Villa P, Luján J, et al. Mortality and functional status at one-year of follow-up in elderly patients with prolonged ICU stay. Med Intensiva. 2016;40(5):289–297. doi:10.1016/j.medin.2015.08.002
21. Zhang Z, Zhu R, Luan Z, et al. Risk of invasive candidiasis with prolonged duration of ICU stay: a systematic review and meta-analysis. BMJ Open. 2020;10(7):e036452. doi:10.1136/bmjopen-2019-036452
22. Wang K, Hsueh K, Kronen R, et al. Creation and assessment of a clinical predictive model for candidaemia in patients with candiduria. Mycoses. 2019;62(7):554–561. doi:10.1111/myc.12917
23. Zatta M, Di Bella S, Giacobbe DR, et al. Clinical features and mortality of nosocomial candidemia in very old patients: a multicentre Italian study. Gerontology. 2020;66(6):532–541. doi:10.1159/000510638
24. Poissy J, Damonti L, Bignon A, et al. Risk factors for candidemia: a prospective matched case-control study. Crit Care. 2020;24(1):109. doi:10.1186/s13054-020-2766-1
25. Yalçın N, Sürmelioğlu N, Özkan-Kuşcu Ö, et al. Evaluation of the effect of antibiotics used during parenteral nutrition treatment on Candidemia. Rev Assoc Med Bras. 2021;67(10):1448–1453. doi:10.1590/1806-9282.20210650
26. Cataldo MA, Tetaj N, Selleri M, et al. Incidence of bacterial and fungal bloodstream infections in COVID-19 patients in intensive care: an alarming “collateral effect”. J Glob Antimicrob Resist. 2020;23:290–291. doi:10.1016/j.jgar.2020.10.004
27. Patel MH, Patel RD, Vanikar AV, et al. Invasive fungal infections in renal transplant patients: a single center study. Ren Fail. 2017;39(1):294–298. doi:10.1080/0886022X.2016.1268537
28. Carvalho AS, Lagana D, Catford J, et al. Bloodstream infections in neutropenic patients with haematological malignancies. Infect Dis Health. 2020;25(1):22–29. doi:10.1016/j.idh.2019.08.006
29. Pasqualotto AC, Rosa DD, Medeiros LR, et al. Candidaemia and cancer: patients are not all the same. BMC Infect Dis. 2006;6:50. doi:10.1186/1471-2334-6-50
30. Viscoli C, Girmenia C, Marinus A, et al. Candidemia in cancer patients: a prospective, multicenter surveillance study by the invasive fungal infection group (IFIG) of the European Organization for Research and Treatment of Cancer (EORTC). Clin Infect Dis. 1999;28(5):1071–1079. doi:10.1086/514731
31. Lortholary O, Renaudat C, Sitbon K, et al. The risk and clinical outcome of candidemia depending on underlying malignancy. Intensive Care Med. 2017;43(5):652–662. doi:10.1007/s00134-017-4743-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.