")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Intravitreal Fluocinolone Acetonide Implant (ILUVIEN®) for the Treatment of Retinal Conditions. A Review of Clinical Studies
Authors Mushtaq Y, Mushtaq MM, Gatzioufas Z, Ripa M , Motta L, Panos GD
Received 13 January 2023
Accepted for publication 22 March 2023
Published 30 March 2023 Volume 2023:17 Pages 961—975
DOI https://doi.org/10.2147/DDDT.S403259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Yusuf Mushtaq,1,* Maryam M Mushtaq,2,* Zisis Gatzioufas,3 Matteo Ripa,4 Lorenzo Motta,5 Georgios D Panos1
1Department of Ophthalmology, Queen’s Medical Centre, Nottingham University Hospitals NHS Trust & School of Medicine, University of Nottingham, Nottingham, UK; 2Department of Acute Medicine, Luton and Dunstable University Hospitals NHS Trust, Luton, UK; 3Department of Ophthalmology, Basel University Hospital & University of Basel School of Medicine, Basel, Switzerland; 4Ophthalmology Unit, “Fondazione Policlinico Universitario A. Gemelli IRCCS”, Rome, Italy; 5Department of Ophthalmology, William Harvey Hospital, East Kent Hospitals University NHS Foundation Trust, Kent, UK
*These authors contributed equally to this work
Correspondence: Georgios D Panos, Department of Ophthalmology, Queen’s Medical Centre, Derby Road, Lenton, Nottingham, NG7 2UH, UK, Tel +44 115 924 9924, Email [email protected] Lorenzo Motta, Department of Ophthalmology, William Harvey Hospital, Kennington Road, Willesborough, Ashford, Kent, TN24 0LZ, UK, Tel +44 1233 633331, Email [email protected]
Abstract: Fluocinolone acetonide (FAc) intravitreal implant (Iluvien®) is a corticosteroid implant indicated for the treatment of diabetic macular oedema (DMO) in patients who have previously received conventional treatment without good response, non–infectious posterior uveitis, and as an off-label treatment of the macular oedema secondary to retinal vein occlusion. FAc is a non-biodegradable 0.19 mg intravitreal implant which is designed to release FAc over 3 years at a rate of approximately 0.2 mcg per day. The aim of this review is to describe the special pharmacological properties of Iluvien and display the outcomes of the most important clinical trials and real-world studies regarding its efficacy and safety for the management of the above retinal disorders.
Keywords: Iluvien, steroid implant, diabetic macular oedema, intravitreal implant, posterior uveitis, retinal vein occlusion
Introduction
Intravitreal injection of pharmacological agents is a valuable tool to efficiently achieve therapeutic levels of medication directly in the vitreoretinal space and treat several retinal conditions.1 This technique has been helpful when treating with corticosteroids, where high oral doses are often needed to achieve therapeutic levels in the eye and therefore increase the risk of adverse systemic side effects.2
With rare but serious complications associated with intravitreal injections, such as endophthalmitis, retinal detachment, and vitreous haemorrhage, sustained-release corticosteroid implants, have emerged to reduce the frequency of repeated intravitreal injections.2 This ultimately reduces risk of complications and increases patient comfort through less frequent hospital visits. The 0.19-mg Fluocinolone acetate (FAc) implant (ILUVIEN®), is an intravitreal glucocorticoid implant that is designed to release fluocinolone acetate at a rate of 0.25μg per day and can have a therapeutic effect lasting 3 years.3 This review will explore the efficacy and safety of FAc in the treatment of retinal conditions, such as diabetic macular oedema (DMO), non-infectious posterior uveitis (NIPU) and retinal vein occlusion (RVO), highlighting important clinical trials and real-world studies.
Short Description of FAc
FAc is a non-erodible implant that is inserted via the pars plana through a 25-gauge injector system as an intravitreal injection. Each implant contains 0.19 mg of the synthetic corticosteroid, FAc, which is practically insoluble in water and is slowly released into the vitreous cavity lasting up to 36 months. The FAMOUS study demonstrated this sustained release in the eye, assessing concentrations of FAc in aqueous humour, with levels of slightly more than 2 ng/mL for approximately the first 3 months followed by a maintained concentration of 0.5–1.0 ng/mL through a period of 36 months. It was also demonstrated that the drug was not detected in the systemic circulation, with FAc plasma concentrations always below the lower limit of quantification of the assay (100 pg/mL).4
FAc is indicated in Europe for the treatment of vision impairment associated with chronic DMO considered insufficiently responsive to available therapies and for prevention of relapse in recurrent NIPU. In 2014, the US Food and Drug Administration approved FAc for the treatment of DMO in patients who have been previously treated with a course of corticosteroids and did not have a clinically significant rise in intraocular pressure (IOP).5
The 0.19mg FAc implant is contraindicated in the presence of pre-existing glaucoma with a cup-to-disc ratio of 0.8 and suspected or active ocular or periocular infections. Also, it is contraindicated in patients that have hypersensitivity to the active substance or any component of the product, such as silicone adhesive, polyvinyl alcohol and polyimide tube.6
Pharmacodynamics
FAc is a synthetic, medium-potency, fluorinated glucocorticoid receptor agonist with no mineralocorticoid activity.7,8 Corticosteroids primary method of action involves stimulating an increase in the synthesis of lipocortins, particularly phospholipase A2. This prevents the formation of prostaglandins and leukotrienes, which are potent inflammatory mediators, through inhibiting the release of their common precursor arachidonic acid from the phospholipid membrane.9,10 Along with their anti-inflammatory activity, glucocorticoids also reduce intravitreal levels of vascular endothelial growth factor (VEGF) through cell and gene inhibition, consequently causing regression of active neovascularisation.8 FAc has been shown to inhibit cell migration; the release of heparin, growth factors, and angiogenic factors; and the secretion of proinflammatory cytokines, which stimulate VEGF production.
In early studies of retinal degeneration in rat models, intravitreal FAc was shown to reduce the levels of neuroinflammation in both anterior and posterior chambers. There was also evidence seen of retinal electro-physiology and morphology preservation, inhibition of cell proliferation, and reduced angiogenesis.7,11,12 In a chick chorioallantoic membrane assay, it was also noted to inhibit tumour necrosis factor a-induced angiogenesis.13 Intravitreal FAc was shown to have positive effects in a human retinal pigment epithelial cell line (ARPE-19) by inhibiting VEGF secretion and mRNA expression. In Phase III trials, FAc at 0.2 mg/day improved best-corrected visual acuity (BCVA) and reduced foveal thickness in patients with DMO. As early as 3 weeks, there was an increase in BCVA of 15 letters (p < 0.05) compared with a placebo, which remained significant throughout the remainder of the trial (36 months).14,15 Reductions in foveal thickness were also sustained and rapid, with the central point thickness significantly lower (p < 0.05) in the treatment arm than in the placebo arm from as early as week 1. This difference remained notable at all measured points through the trial (24 months).14,15 An earlier Phase II study revealed that there was no statistically significant difference between patients receiving FAc at 0.2 versus 0.5 mg/day.7,16 Sustained-release FAc was also more effective in suppressing retinal microgliosis when compared with high-dose FAc.17
Pharmacokinetic Profile
A phase II study assessing the aqueous levels of FAc after administration of inserts/implants in patients with DMO revealed that the steroid is released into the aqueous humour in a sustained manner for a minimum of 36 months.4 This method of delivery of the 0.2mg/day FAc implant causes a steady-state concentration of 0.5 to 1.0 ng/mL to be reached by 6 to 9 months, with the average aqueous concentration reaching its maximum approximately 1 week after administration. The higher 0.5mg/day dose resulted in significantly higher aqueous levels for the first month, but no statistically significant difference in doses was noted after that time.18 For both lower (0.2mg/day) and higher-dose (0.5mg/day) implants, the plasma concentrations of FAc remained below the lower limit (100 pg/mL) from week 1 until completion of the trial at 36 months.8
Retinal Conditions and Their Management
The principal effects of corticosteroids are thought to be stabilisation of the blood-retinal barrier (BRB), reduction of exudation and downregulation of inflammatory stimuli.9 These properties make them an attractive therapeutic option for a variety of posterior segment diseases such as DMO, NIPU and RVO.
Diabetic Macular Oedema (DMO)
DMO is the most common form of sight-threatening retinopathy in people, with more than 20 million cases worldwide.19 Approximately 14% to 25% of patients diagnosed with diabetes appear to develop DMO within 10 years of presentation.20 Disruption of the BRB due to an inflammatory cascade of events, involving chronic hyperglycaemia, oxidative stress and upregulation of anti-VEGF, results in the accumulation of fluid in the extravascular space. Corticosteroid intravitreal injections have been proven to inhibit the inflammatory cascade and can effectively treat this macular oedema.21 However, some patients can develop chronic DMO, with oedema persisting despite treatment. This is problematic as repeated injections (anti-VEGF or steroid) or macular laser sessions are required to attempt to stabilise visual acuity with a suboptimal response. The long-acting therapeutic effect of FAc aims to provide a solution to these challenging cases and has obtained approval for use in Europe and the USA following recent clinical trials and studies. The FAME clinical trial, which compared a total of 768 patients given varied strength doses of the FAc implant to 185 patients receiving a sham injection, demonstrated a mean improvement in BCVA and foveal thickness (FT) at 24 months’ post administration.15 The mean improvement in BCVA letter score was 4.4 and 5.4 in the low- and high-dose groups, respectively, compared with 1.7 in the sham group (P = 0.02 and P = 0.016). This has also been highlighted in the ICE-UK study, which analysed 233 eyes treated with the FAc implant. In the 12 months prior to the implant, the visual acuity (VA) of these patients declined. However, in the 12 months’ post implant, there was improvement of VA from a median of 0.66 LogMAR units or 52.0 ETDRS letters to 0.60 (0.38–0.90) LogMAR units or 55.0 letters (p < 0.001).22 Similar results were reported by El-Ghrably et al with a mean increase of 5.1 letters in BCVA at month 12.23
A reduction in retinal thickness following FAc implants is acknowledged in many literatures and was noticed as early as 7 days after implantation and maintained for up to 3 years after the injection, with an average 20% to 30% reduction in macular oedema.24–26 A case report by Bertelmann et al showed how bilateral FAc implants in a phakic patient with a 20-year history of refractory DMO (left eye at baseline, right eye at month 6), resulted in a decrease in central retinal thickness (CRT) in the left eye from 642 to 372µm at month 13 and from 473 to 334µm in the right eye at month 6.27 Elaraoud et al investigated earlier outcomes in 22 eyes across three different UK sites, which demonstrated a mean reduction in CRT of 148.9µm at 3 months and a mean visual gain of 6.4L.28 In patients with bilateral implants and DMO, later data at 6 and 23 months established a sustained CRT reduction at months 6 and 12.29,30 Massin et al conducted a prospective Phase IV study in France, whereby participants were divided into two groups: chronic DMO insufficiently responsive to laser (group 1) with or without anti-VEGF (group 2), and given the FAc implant. A decrease in CRT was seen as early as week 1, with a mean reduction of 239 and 147µm at month 1 for groups 1 and 2, respectively.31 This effect was seen to be maintained at every 3-monthly interval, up to 12 months where a 299µm (group 1) and 251µm (group 2) reduction was established.
Greater oedema (>400 μm) is linked to a higher implant efficacy, with a thickness reduction of up to 50% in 21% of treated eyes.32 In a certain study, the results were noticeably better, with a decrease from 960 to 246 μm in just 3 months.28 There is substantial debate regarding the relationship between reduced macular thickness and increased visual acuity; in some studies, visual improvement was less significant than structural improvement. This is probably because of other factors that affect vision in diabetic patients besides macular thickness, like ischaemia, DMO duration, or structural retinal damage.31–33
A recent real-world study from East London reported worse VA and CRT results, compared to the other published studies, in a predominantly BAME (black, Asian and minority ethnic) population.33 Interestingly, in comparison to white subjects, BAME patients were found to respond less favourably in terms of VA gains, CRT improvement, and the need for additional treatment.
Although FAc has been found to be efficient in improving patient vision for up to 3 years in real-world studies, ophthalmic practitioners should remember that typically more than one injection or supplementary treatment with anti-VEGF or steroid injections is needed. The second FAc injection is typically given at 12 months.24 In the FAME studies, approximately two-third of patients needed additional treatment.14 In the MEDISOFT study 44% of patients required additional therapy within a 2-year follow-up period and more specifically 6.4% received additional macular laser, 1.2% received bevacizumab, 13.6% received aflibercept, 17.7% received ranibizumab, 2.3% received intravitreal dexamethasone and the same percentage received intravitreal triamcinolone, while 0.53% received another FAc implant.25 According to published studies, the proportion of patients requiring supplementary treatment range from 44% to 83%.14,24,25,33,34
A summary of the studies on Iluvien in the treatment of DMO is depicted in Table 1. Important side-effects that have been associated with Iluvien usage are also included.
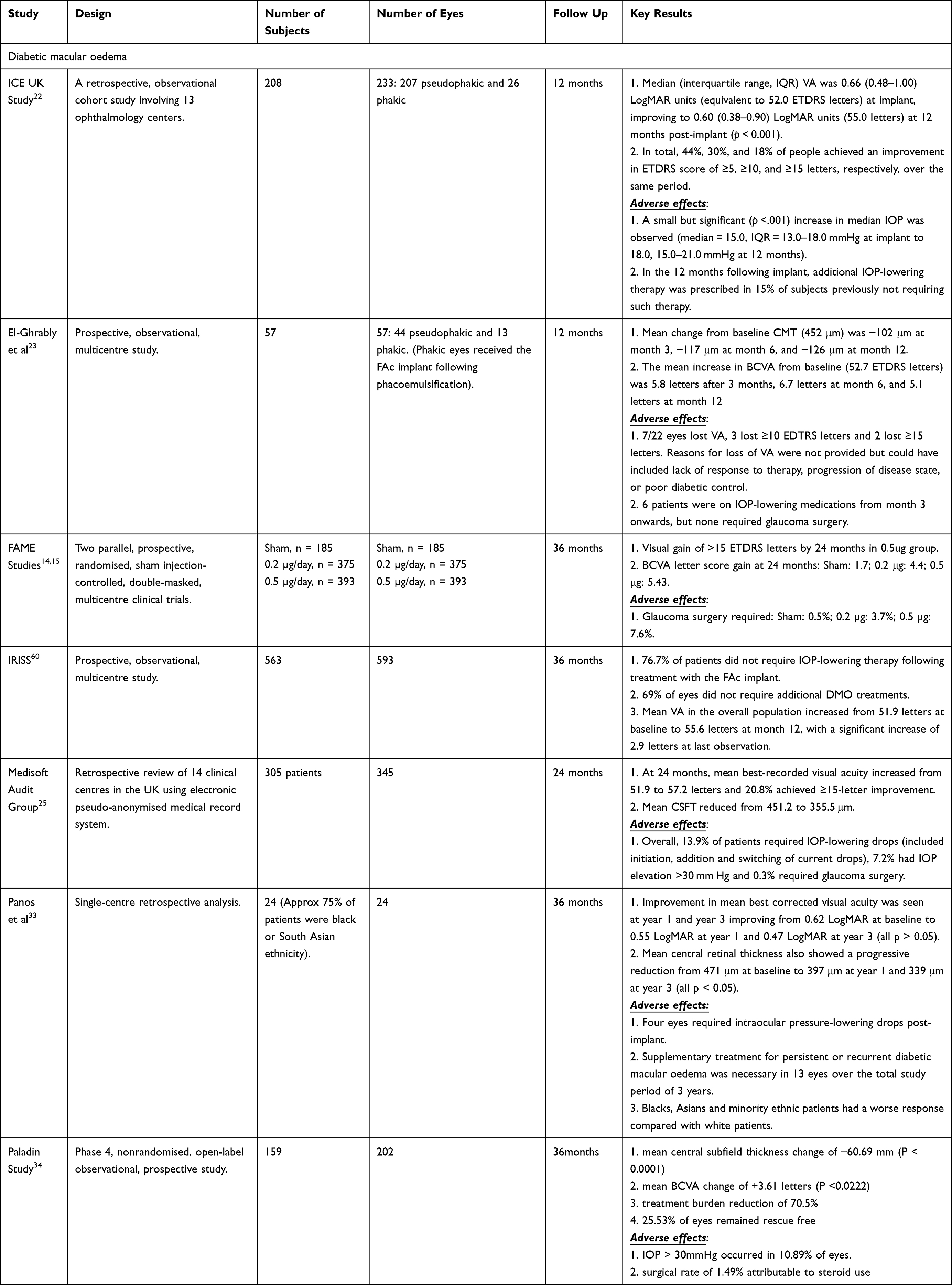 |
Table 1 Summary of Most Important Studies of ILUVIEN and DMO |
Non-Infectious Posterior Uveitis (NIPU)
There are several treatment options available to improve visual outcomes for those with posterior uveitis, including systemic corticosteroids and immunomodulatory therapy (IMT).35 However, corticosteroids are associated with many side effects and direct intravitreal therapy offers promise to provide therapeutic levels directly to the eye while avoiding systemic complications. Until recently, there have been no intravitreal treatments offering sustained therapeutic effect for more than 6 months.36
Bodaghi et al stresses the importance of avoiding cumulative damage in uveitis by preventing recurrent episodes of inflammation.37 It has been hypothesised that the total insult to a uveitic eye from repeated inflammatory attacks may be greater than the sum of the individual insults and the consequences can be irreversible.18 FAc can provide sustained long-term treatment directly to the eye and reduce the cycle of treat, recur and treat.37
Recent studies have shown that FAc is effective in treating NIPU. Jaffe et al performed a randomised controlled trial in 11 eyes with a history of recurrent noninfectious intermediate uveitis, posterior, or panuveitis.38 Participants were randomized to receive either a low- or a high-dose FAc. Eyes were observed on day 0 (day the implant was injected) and then at regular intervals through 2 years. The average number of inflammation recurrences in the 12 months before implantation was 1.54 episodes per eye. During the follow-up period, none of the study eyes experienced a recurrence. None of these eyes also required a dose of posterior sub-tennon triamcinolone acetonide (PSTA) injection, which was given an average of 1.5 times preceding implantation in 5 of the 11 eyes.
Pavesio and Heinz also carried out a prospective, randomised, double-masked, multicentre comparison of FAc and control-treated (sham injection plus standard of care) participants.39 Eligible subjects had over a one-year recurrent NIPU history and either at least two separate recurrences requiring treatment or corticosteroid therapy (systemic or ocular) in the 12 months preceding study entry. Bilateral disease was present and analysed in 59/87 FAc-treated participants. In these patients, the more severely affected eye was treated with the FAc implant. Over 36 months, more FAc treated than fellow eyes remained recurrence-free (28.8% vs 5.1%, P = 0.001; mean 1.9 vs 4.7 recurrences, respectively, P < 0.0001). Topical corticosteroid use was also lower in FAc-treated than fellow eyes (27.1% vs 52.5%, P = 0.0041). However, cataract surgery occurred in 72.0% of FAc-treated and 37.0% of fellow eyes. Although it appears to be relatively common for phakic eyes treated with FAc needing to undergo cataract surgery at some point in the follow-up, Weber et al demonstrated in 11 eyes with non-infectious uveitic macular oedema, treated with FAc implant, that intraocular pressure increases did not require additional treatment and no major ophthalmic complications occurred.40
Jaffe and Pavesio on behalf of the Study Investigators conducted a Phase 3, prospective, double-masked, multicenter study on 129 participants (n = 87 FAc-treated; n = 42 sham-treated) over 36 months.41 In comparison to sham-treated eyes, Fac-treated eyes had significantly lower rates of uveitis recurrence over the course of the study (65.5% vs 97.6%; P < 0.001), significantly longer periods without recurrence (median 657.0 vs 70.5 days; P < 0.001), fewer recurrence episodes among those who had recurrences (mean 1.7 vs 5.3; P < 0.001), less adjunctive therapy (57.5% vs 97.6%), and an acceptable side-effect profile.
A number of real-world studies demonstrated favourable functional and anatomical outcomes of FAc in patients with NIPU. More specifically, two retrospective studies showed a mean CRT reduction of approximately 150μm with a complete resolution of the macular oedema in about 70% of the cases over 12 months.42,43 Battista et al found that the area under the curve (AUC) of BCVA after FAc correlates with the BCVA at the time of injection but not with macular thickness, whereas the AUC of central macular thickness (CMT) correlates with baseline CMT and may be negatively associated with uveitis duration.44
A recent large retrospective study on 57 patients with NIPU treated with Fac 0.19mg from a tertiary referral centre in Germany specialising in uveitis reported a significant CRT reduction of approximately 54μm over 12 months and a reduction in intraocular inflammation over the first 9 months of the follow-up without significant adverse events.45
More real-world studies with patients of different racial and ethnic backgrounds are expected with great interest.
A summary of the studies on Iluvien in the treatment of NIPU is depicted in Table 2.
 |
Table 2 Summary of Most Important Studies of ILUVIEN and NIPU |
Retinal Vein Occlusion (RVO) and Irvine – Gass Syndrome
RVO is one of the main causes of sudden, painless vision loss in adults older than 50 years old. It is the occurrence of macular oedema in RVO that most frequently leads to visual loss.46 Thrombosis within a retinal vein can lead to partial obstruction of blood flow from the eye. Sufficiently high increased intraluminal pressure can cause transudation of blood products into the retina resulting in increased interstitial fluid and protein. This can increase interstitial oncotic pressure, worsening tissue oedema and vascular perfusion, ultimately leading to ischaemia. Several chemical factors are involved in this inflammatory process, with Yoshimura et al finding significantly elevated vitreous levels of the soluble cytokines interleukin (IL) 6 and 8, monocyte chemoattractant protein-1, and VEGF in RVO, and especially in central RVO (CRVO).47 This makes corticosteroids a useful class for their treatment.
With macular oedema persisting for a long time post CRVO, the prolonged therapeutic effect of FAc could be helpful and reduce the burden of multiple intravitreal injections.48 Coelho et al reported a case of non-ischaemic CRVO that was successfully treated with a single intravitreal FAc implant.49 Initially, repeated injections of shorter-acting dexamethasone were given, but resulted in fluctuations of vision between 20/32 and 20/200, based on the presence of macular oedema. This constant fluctuation on visual acuity was very uncomfortable for the patient being a frequent complaint. The FAc implant was successful in providing sustained improvement in visual acuity from 20/200 to 20/25.
The FAc implant has been demonstrated by Ribeiro et al to be effective in a case of ischaemic CRVO and BRVO. The patient with the ischaemic CRVO presented a baseline BCVA of 29 letters and a CRT of 664 µm.50 In the absence of response to anti-VEGF (bevacizumab and aflibercept) and triamcinolone intravitreal injections, she was proposed to a dexamethasone implant (OZURDEX). She showed an anatomical improvement (CRT of 364 µm), although not sustained, despite a total of 5 implants. After the FAc implant was administered, a significant and sustained functional (BCVA of 38 letters) and anatomical (CRT of 271 µm) improvement was noted. This was similarly proven in the patient with BRVO, with sustained resolution of macular oedema at 12 months following the FAc implant.
Despite these clinical case studies, the volume of data regarding the use of FAc for RVO remains limited, and therefore its use is “off-label.” Further studies with longer follow-ups and sample sizes are needed to improve the confidence in the efficacy and safety of the FAc implant in these patients.
The post-operative macular oedema or Irvine – Gass syndrome is a common complication following intraocular surgery and can potentially lead to reduced visual acuity. The pathogenesis of this condition is related to postoperative inflammation and inflammatory mediator release and, therefore, steroids play an important role in the treatment and prevention.51 Miguel-Escuder et al presented four clinical cases of vitrectomised eyes with post-operative CMO irresponsive to conventional treatment including dexamethasone implant (Ozurdex).52 After treatment with Iluvien, macular oedema resolved in three cases, while one patient required additional treatment with Ozurdex. A recent study from Germany showed favourable outcomes in terms of visual and anatomical improvement in patients with refractory post-op CMO treated with a single Iluvien implant.53
The volume of published data regarding the use of FAc for post-operative CMO remains limited and and therefore its use is “off-label.” Further larger studies are needed to reliably assess the efficacy and safety of the FAc implant in these cases.
A summary of the reports on Iluvien in the treatment of RVO and Irvine – Gass syndrome is depicted in Table 3.
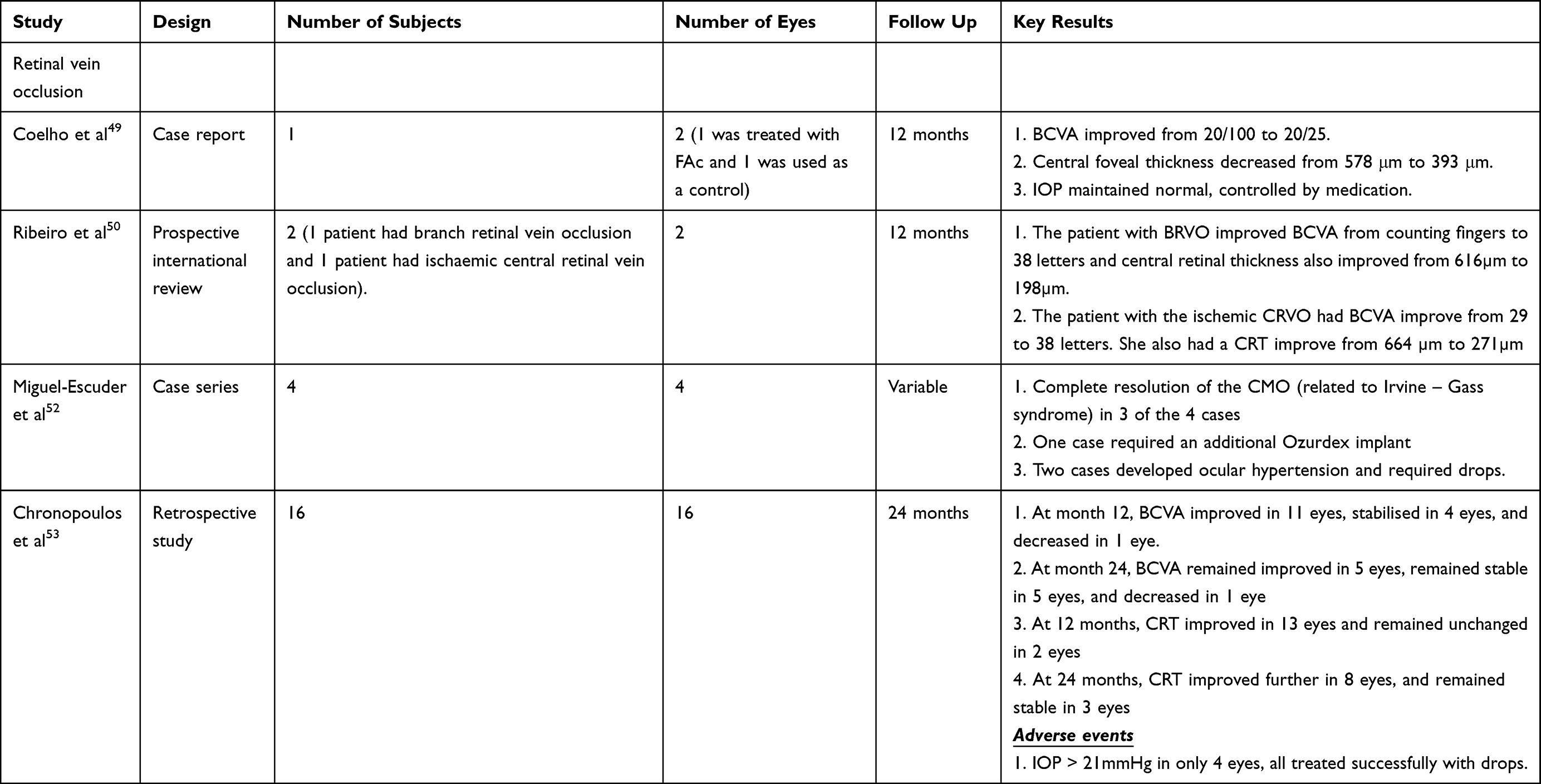 |
Table 3 Summary of Most Important Studies of ILUVIEN and RVO & Irvine – Gass Syndrome |
Safety
The most significant concerns surrounding intravitreal injection of steroids revealed by the FAME trials, were the development of visually significant cataract and ocular hypertension, or glaucoma. During the trials, four cases of endophthalmitis occurred, in which half of these were considered secondary to FAc injection (days 13 and 16 post-injection).25 Surprisingly, there have only been a few reported cases of endophthalmitis that have been published in real-world studies to date, despite steroid injections known to be immunosuppressive in already compromised patients, such as those with diabetes.54 This also highlights the need for increased caution with steroid use in patients with a history of herpetic or viral eye disease, as these injections may lead to a higher recurrence rate.
Ocular hypertension is one of the most common adverse events associated with the use of intraocular steroids; with up to 13% of patients potentially developing an IOP of >30 mmHg36 (range of occurrence, 7–50%).24,55,56 Comparisons with the untreated eye show no ocular hypertension present when specifically assessed.57 This is echoed in the FAME study, where IOP was raised in 37.1% of patients who received the 0.2-mg/day FAc implant (n = 375), compared to 11.9% of those who received a placebo (n = 185). This pattern remained true with both the overall population, and in those without prior ocular corticosteroid exposure; with a >30-mmHg rise in IOP more frequently seen in patients who received the 0.2-mg/day FAc implant (p < 0.001) than in those who received placebo.14,15
A retrospective study of 26 vitrectomised eyes (with a mean follow-up of 255 days) was performed by Meireles et al, where a mean IOP increase of 1.4 mmHg was found between baseline and the last visit (range, 9.0 to þ8.0 mmHg); with eight eyes (30.7%) initiating or continuing anti-glaucoma drops.58 Pessoa et al also performed a retrospective study with 43 eyes (24 vitrectomised and 19 non-vitrectomised), and a mean follow-up of 8.5 months.59 There was no difference in the IOP changes between the two groups; however, vitrectomised eyes demonstrated a higher mean IOP elevation (1.6 vs 0.8 mmHg). The conclusions of the FAME study were supported in a multicentre study from three European countries (United Kingdom, Germany, and Portugal), published by the IRISS group. They found that roughly 23% of patients required IOP-lowering medication, but with no associated clinically significant changes in their cup-to-disc ratio (CDR).60 The percentage of administered glaucoma drops varied from 0% to 15%, with some larger series having an even higher rate.22,25,55,60 These larger percentages are more in accordance with the FAME study, in which 26% of patients required glaucoma drops. However, 5.2% of patients in IRISS had a baseline IOP of >21 mmHg, which was an exclusion criterion in the FAME trials. Despite appropriate topical treatment, glaucoma surgery was deemed necessary in up to 14.3% of cases.55
From these studies we can conclude that careful patient selection is of high importance in avoiding complications related to ocular hypertension. Currently, the FAc implant is contraindicated in patients with pre-existing glaucoma, and it is not approved for use in steroid responders in the United States.61 An idea to improve safety in administration would be through introducing a steroid provocation test to patients. Such a test could highlight individuals who may require surgical intervention and prevent them from FAc treatment; however, it could not definitely predict the absence of ocular hypertension.62 The PALADIN study showed that 96.92% of eyes with a previous IOP response of <25 mmHg after the steroid challenge, would have a similar outcome to Fac implant.34 In the FAME study, 6.1% of steroid-naıve patients needed IOP-lowering surgery (n = 18), stressing the importance of identifying the individuals who have a strong IOP response to corticosteroid therapy.62 Dosing also needs to be highlighted, with no measured increase found in the CDR with a 0.2-mg/day dose after 36 months, compared to an increase of 0.1 in the 0.5-mg/day group.62 Subsequently, a 0.2-mg/day dose is the implant globally used; however, careful long-term follow-up focusing on IOP is still required.
Besides ocular hypertension, cataract formation is another important issue to tackle when it comes to the use of intraocular corticosteroids. It was discovered that cataracts usually develop within the first year of treatment and in almost all patients receiving implants after 3 years of follow-up.63 The percentages of cataract surgery were 46% and 55% in patients with and without chronic macular oedema, respectively; which correlates to the 21% and 11% in the matched placebo group.64 At the 36-month follow-up in the FAME study, cataracts developed in 81.7% of baseline phakic patients who received the 0.2-mg/day implant (n 1⁄4235), as opposed to the 50.4% of those who received a placebo (n = 121).14,15 The visual outcome, however, following extraction, was measurable, if not better, than that in patients with pseudophakia at baseline.14,15,63 These results demonstrate that patients with chronic DMO are more likely to gain a 15-letter improvement than those without DMO following cataract extraction.14,15
As is the case with all intravitreal injections, adverse events may occur which are not currently reported in the literature. Such events include vitreous haemorrhage, transient ocular hypertension, and retinal tears or detachment.54 Inside the eye, the presence of the steroid implant can also lead to problems in patients who undergo vitreo-retinal surgery, as it can become dislodged into the infusion cannula and cause globe pressurisation difficulties during surgery. These implants also run the risk of alternatively migrating to the anterior chamber.65 The benefit–risk ratio of FAc use should therefore be acknowledged with each patient before use, as there are associated significant risks of adverse events, despite some studies supporting safe bilateral use.29,30,66
Cost-Effectiveness
Retinal conditions, including DMO, can lead to blindness with significant financial impact; the annual cost of blindness for UK patients is more than GBP 5 billion.67 Numerous analyses suggest that the FAc implant is a cost-effective treatment for both phakic and pseudophakic patients with insufficiently responsive DMO.55,68 A recent systematic literature review conducted in Germany over 3 years used a short-term cost–cost model to compare choosing an FA implant as a treatment for insufficiently anti-VEGF responding foveas in patients with DMO over other treatments, including ranibizumab, aflibercept, and a dexamethasone implant (Ozurdex).69 The review concluded that a single FA implant was the most cost-effective (in-label) therapeutic option, with total costs of EUR 10,826, compared to EUR 17,542, EUR 15,896 and EUR 12,365, for ranibizumab, aflibercept, and the dexamethasone implant, respectively. The model determined drug costs as the predominant cost component, followed by the expenses of injections and optical coherence tomography.
In a recent NHS study, Quhill and Beiderbeck analysed the overall cost of treatment over 3 years with a single FAc implant, compared to using an average of 14 ranibizumab as needed.68 The study took into account the expenses of the drugs and administration; along with the costs involved in monitoring patients, any additional interventions needed and management of adverse events. These authors calculated that by using the FAc implant over ranibizumab, and taking into account the added cost of cataract surgery, savings of roughly £6068 in pseudophakic eyes and £5341 in phakic eyes could occur. Therefore, within 3 years following the FAc implant, the need for adjunctive treatment was found to be lower than that needed with average anti-VEGF treatment regimens.24,25
These studies demonstrate that the long-acting efficacy, safety profile and tolerability of the FAc implant allows it to be a considerable cost-saving option when compared to other treatments. Additionally, minimising the number and need for treatments is important for both patients and health-care staff, as department workloads are reduced and treatment time can be made available to other patients who need it. An increase in the frequency of injections has also been shown to decrease patients’ quality of life, causing an increase in work leave and anxiety.70
Conclusion
Overall, most clinical studies discussed have shown that FAc can be useful in the treatment of several retinal diseases. The common thing between DMO, NIPU and RVO is the inflammatory component associated with them and this makes corticosteroids a good therapeutic option. However, one of the biggest challenges faced is the chronicity of these diseases. FAc provides an option for long-term, stabilization of retinal conditions through constant, slow release of therapeutic substance directly to the vitreous cavity of the eye. Other intravitreal therapies, such as anti-VEGF and triamcinolone acetate (TA), have provided good therapeutic outcomes for patients with the mentioned retinal conditions, however the need for multiple injections is inconvenient for patients with an increase in associated risks.71 FAc offers a plausible alternative for patients with persistent or recurrent symptoms despite multiple anti-VEGF injections.15
The most frequently occurring adverse events related to FAc use are cataracts requiring surgery and an increase in IOP. Often, phakic eyes developed cataracts requiring surgery; however, the visual outcomes post-cataract surgery were similar to the outcomes from the already pseudophakic patients used at baseline.15 IOP measurements were also included in most studies and when ocular hypertension occurred, it was often well controlled by topical therapy.
Therefore, there is growing evidence for the use of FAc in many retinal conditions that are not completely responsive to current, short-term therapies, as it offers several advantages over other, and because it is a slow-release implant, patients require fewer injections or appointments with their ophthalmologist, which can reduce the burden of treatment. Additionally, FAC has been shown to be effective in maintaining visual acuity over the long term, making it a valuable option for patients with chronic DMO, recurrent NIPU, and eventually other retinal conditions.
Disclosure
Yusuf Mushtaq and Maryam M Mushtaq are co-first authors for this study. Lorenzo Motta and Georgios D Panos are co-correspondence authors for this study. The authors report no conflicts of interest in this work.
References
1. Peyman GA, Lad EM, Moshfeghi DM. Intravitreal injection of therapeutic agents. Retina. 2009;29(7):875–912. doi:10.1097/IAE.0b013e3181a94f01
2. Falavarjani KG, Nguyen QD. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye. 2013;27(7):787–794. doi:10.1038/eye.2013.107
3. Massa H, Nagar AM, Vergados A, Dadoukis P, Patra S, Panos GD. Intravitreal fluocinolone acetonide implant (ILUVIEN(R)) for diabetic macular oedema: a literature review. J Int Med Res. 2019;47(1):31–43. doi:10.1177/0300060518816884
4. Campochiaro PA, Nguyen QD, Hafiz G, et al. Aqueous levels of fluocinolone acetonide after administration of fluocinolone acetonide inserts or fluocinolone acetonide implants. Ophthalmology. 2013;120(3):583–587. doi:10.1016/j.ophtha.2012.09.014
5. Drugs.com. FDA approves iluvien; 2014. Available from: https://www.drugs.com/newdrugs/fda-approves-iluvien-diabetic-macular-edema-4092.html.
6. Cadth.ca. Clinical review report: fluocinolone acetonide intravitreal implant (Iluvien): (Knight Therapeutics Inc.): indication: for the treatment of diabetic macular edema (DME) in patients who have been previously treated with a course of corticosteroids and did not have a clinically significant rise in intraocular pressure. Ottawa (ON); 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/relatedinfo/sr0608-iIluvien-clinical-review-report.pdf. Accessed
7. Medicine and Healthcare products Regulatory Agency. Iluvien 190 micrograms intravitreal implant in applicator (fluocinolone acetonide): public assessment report; 2016.
8. Alimera Sciences Inc. Iluvien (fluocinolone acetonide intravitreal implant) 0.19 mg for intravitreal injection: US prescribing information; 2014. Available from: http://www.fda.gov.
9. Sarao V, Veritti D, Boscia F, Lanzetta P. Intravitreal steroids for the treatment of retinal diseases. ScientificWorldJournal. 2014;2014:989501. doi:10.1155/2014/989501
10. Kang BS, Chung EY, Yun YP, et al. Inhibitory effects of anti-inflammatory drugs on interleukin-6 bioactivity. Biol Pharm Bull. 2001;24(6):701–703. doi:10.1248/bpb.24.701
11. Holmquist F, Lundin S, Larsson B, Hedlund H, Andersson KE. Studies on binding sites, contents, and effects of AVP in isolated bladder and urethra from rabbits and humans. Am J Physiol. 1991;261(4 Pt 2):R865–874. doi:10.1152/ajpregu.1991.261.4.R865
12. Glybina IV, Kennedy A, Ashton P, Abrams GW, Iezzi R. Photoreceptor neuroprotection in RCS rats via low-dose intravitreal sustained-delivery of fluocinolone acetonide. Invest Ophthalmol Vis Sci. 2009;50(10):4847–4857. doi:10.1167/iovs.08-2831
13. Ayalasomayajula SP, Ashton P, Kompella UB. Fluocinolone inhibits VEGF expression via glucocorticoid receptor in human retinal pigment epithelial (ARPE-19) cells and TNF-alpha-induced angiogenesis in chick chorioallantoic membrane (CAM). J Ocul Pharmacol Ther. 2009;25(2):97–103. doi:10.1089/jop.2008.0090
14. Campochiaro PA, Brown DM, Pearson A, et al. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology. 2012;119(10):2125–2132. doi:10.1016/j.ophtha.2012.04.030
15. Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626–635 e622. doi:10.1016/j.ophtha.2010.12.028
16. Syed YY. Fluocinolone acetonide intravitreal implant 0.19 mg (ILUVIEN((R))): a review in diabetic macular edema. Drugs. 2017;77(5):575–583. doi:10.1007/s40265-017-0722-4
17. Glybina IV, Kennedy A, Ashton P, Abrams GW, Iezzi R. Intravitreous delivery of the corticosteroid fluocinolone acetonide attenuates retinal degeneration in S334ter-4 rats. Invest Ophthalmol Vis Sci. 2010;51(8):4243–4252. doi:10.1167/iovs.09-4492
18. Campochiaro PA. Pharmacokinetics of sustained-delivery fluocinolone acetonide for DMO. Retina Today. 2009;2009:55–56.
19. Tan GS, Cheung N, Simo R, Cheung GC, Wong TY. Diabetic macular oedema. Lancet Diabetes Endocrinol. 2017;5(2):143–155. doi:10.1016/S2213-8587(16)30052-3
20. Klein R, Klein BE, Moss SE, Cruickshanks KJ. The Wisconsin epidemiologic study of diabetic retinopathy. XV. The long-term incidence of macular edema. Ophthalmology. 1995;102(1):7–16. doi:10.1016/S0161-6420(95)31052-4
21. Pacella F, Ferraresi AF, Turchetti P, et al. Intravitreal Injection of Ozurdex((R)) implant in patients with persistent diabetic macular edema, with six-month follow-up. Ophthalmol Eye Dis. 2016;8:11–16. doi:10.4137/OED.S38028
22. Holden SE, Currie CJ, Owens DR. Evaluation of the clinical effectiveness in routine practice of fluocinolone acetonide 190 microg intravitreal implant in people with diabetic macular edema. Curr Med Res Opin. 2017;33(sup2):5–17. doi:10.1080/03007995.2017.1366645
23. El-Ghrably I, Steel DHW, Habib M, Vaideanu-Collins D, Manvikar S, Hillier RJ. Diabetic macular edema outcomes in eyes treated with fluocinolone acetonide 0.2 microg/d intravitreal implant: real-world UK experience. Eur J Ophthalmol. 2017;27(3):357–362. doi:10.5301/ejo.5000929
24. Fusi-Rubiano W, Mukherjee C, Lane M, et al. Treating Diabetic Macular Oedema (DMO): real world UK clinical outcomes for the 0.19mg Fluocinolone Acetonide intravitreal implant (Iluvien) at 2 years. BMC Ophthalmol. 2018;18(1):62. doi:10.1186/s12886-018-0726-1
25. Bailey C, Chakravarthy U, Lotery A, Menon G, Talks J, Medisoft Audit G. Real-world experience with 0.2 mug/day fluocinolone acetonide intravitreal implant (ILUVIEN) in the United Kingdom. Eye. 2017;31(12):1707–1715. doi:10.1038/eye.2017.125
26. Figueira J, Henriques J, Amaro M, Rosas V, Alves D, Cunha-Vaz J. A nonrandomized, open-label, multicenter, phase 4 pilot study on the effect and safety of ILUVIEN(R) in chronic diabetic macular edema patients considered insufficiently responsive to available therapies (RESPOND). Ophthalmic Res. 2017;57(3):166–172. doi:10.1159/000455235
27. Bertelmann T, Schulze S. Long-term follow-up of patient with diabetic macular edema receiving fluocinolone acetonide intravitreal implant. Ophthalmol Ther. 2015;4(1):51–58. doi:10.1007/s40123-015-0028-0
28. Elaraoud I, Andreatta W, Kidess A, et al. Use of flucinolone acetonide for patients with diabetic macular oedema: patient selection criteria and early outcomes in real world setting. BMC Ophthalmol. 2016;16:3. doi:10.1186/s12886-015-0178-9
29. Elaraoud I, Attawan A, Quhill F. Case series investigating the efficacy and safety of bilateral fluocinolone acetonide (ILUVIEN((R))) in patients with diabetic macular edema. Ophthalmol Ther. 2016;5(1):95–104. doi:10.1007/s40123-016-0045-7
30. Elaraoud I, Quhill H, Quhill F. Case series investigating the efficacy and safety of bilateral fluocinolone acetonide (ILUVIEN((R))) in patients with diabetic macular edema: 10 eyes with 12 months follow-up. Ophthalmol Ther. 2016;5(1):105–109. doi:10.1007/s40123-016-0049-3
31. Massin P, Erginay A, Dupas B, Couturier A, Tadayoni R. Efficacy and safety of sustained-delivery fluocinolone acetonide intravitreal implant in patients with chronic diabetic macular edema insufficiently responsive to available therapies: a real-life study. Clin Ophthalmol. 2016;10:1257–1264. doi:10.2147/OPTH.S105385
32. Currie CJ, Holden SE, Owens DR. Patterns of retinal thickness prior to and following treatment with fluocinolone acetonide 190 microg intravitreal implant for diabetic macular edema. Curr Med Res Opin. 2017;33(sup2):33–43. doi:10.1080/03007995.2017.1366662
33. Panos GD, Arruti N, Patra S. The long-term efficacy and safety of fluocinolone acetonide intravitreal implant 190 mug (ILUVIEN((R))) in diabetic macular oedema in a multi-ethnic inner-city population. Eur J Ophthalmol. 2021;31(2):620–629. doi:10.1177/1120672119898414
34. Singer MA, Sheth V, Mansour SE, Coughlin B, Gonzalez VH. Three-year safety and efficacy of the 0.19-mg fluocinolone acetonide intravitreal implant for diabetic macular edema: the PALADIN study. Ophthalmology. 2022;129(6):605–613. doi:10.1016/j.ophtha.2022.01.015
35. Uy HS, Yu-Keh E, Chan PS. Posterior Uveitis. Dev Ophthalmol. 2016;55:163–166.
36. Massa H, Georgoudis P, Panos GD. Dexamethasone intravitreal implant (OZURDEX((R))) for macular edema secondary to noninfectious uveitis: a review of the literature. Ther Deliv. 2019;10(6):343–351. doi:10.4155/tde-2019-0024
37. Bodaghi B, Nguyen QD, Jaffe G, Khoramnia R, Pavesio C. Preventing relapse in non-infectious uveitis affecting the posterior segment of the eye - evaluating the 0.2 mug/day fluocinolone acetonide intravitreal implant (ILUVIEN((R))). J Ophthalmic Inflamm Infect. 2020;10(1):32. doi:10.1186/s12348-020-00225-z
38. Jaffe GJ, Lin P, Keenan RT, Ashton P, Skalak C, Stinnett SS. Injectable fluocinolone acetonide long-acting implant for noninfectious intermediate uveitis, posterior uveitis, and panuveitis: two-year results. Ophthalmology. 2016;123(9):1940–1948. doi:10.1016/j.ophtha.2016.05.025
39. Pavesio C, Heinz C. Non-infectious uveitis affecting the posterior segment treated with fluocinolone acetonide intravitreal implant: 3-year fellow eye analysis. Eye. 2022;36(6):1231–1237. doi:10.1038/s41433-021-01608-9
40. Weber LF, Marx S, Auffarth GU, et al. Injectable 0.19-mg fluocinolone acetonide intravitreal implant for the treatment of non-infectious uveitic macular edema. J Ophthalmic Inflamm Infect. 2019;9(1):3. doi:10.1186/s12348-019-0168-9
41. Jaffe GJ, Pavesio CE, Study I. Effect of a fluocinolone acetonide insert on recurrence rates in noninfectious intermediate, posterior, or panuveitis: three-year results. Ophthalmology. 2020;127(10):1395–1404. doi:10.1016/j.ophtha.2020.04.001
42. Hikal M, Celik N, Auffarth GU, Kessler LJ, Mayer CS, Khoramnia R. Intravitreal 0.19 mg fluocinolone acetonide implant in non-infectious uveitis. J Clin Med. 2021;10(17):3966. doi:10.3390/jcm10173966
43. Pockar S, Leal I, Chhabra R, Jones NP, Steeples LR. Intravitreal fluocinolone 0.19mg implant in the management of chronic non-infectious uveitis: 12-month outcomes from a single tertiary centre. Ocul Immunol Inflamm. 2021;1–7:54.
44. Battista M, Starace V, Cicinelli MV, et al. Efficacy of 0.19 mg fluocinolone acetonide implant in non-infectious posterior uveitis evaluated as area under the curve. Ophthalmol Ther. 2022;11(1):215–224. doi:10.1007/s40123-021-00426-2
45. Buhl L, Thurau S, Kern C. Fluocinolone acetonide 0.19-mg implant for the treatment of noninfectious uveitis with involvement of the posterior segment: a real-world study. Graefes Arch Clin Exp Ophthalmol. 2022. doi:10.1007/s00417-022-05893-2
46. Orskov M, Vorum H, Bjerregaard Larsen T, et al. A review of risk factors for retinal vein occlusions. Expert Rev Cardiovasc Ther. 2022;20(9):761–772. doi:10.1080/14779072.2022.2112667
47. Yoshimura T, Sonoda KH, Sugahara M, et al. Comprehensive analysis of inflammatory immune mediators in vitreoretinal diseases. PLoS One. 2009;4(12):e8158. doi:10.1371/journal.pone.0008158
48. Ford JA, Clar C, Lois N, et al. Treatments for macular oedema following central retinal vein occlusion: systematic review. BMJ Open. 2014;4(2):e004120. doi:10.1136/bmjopen-2013-004120
49. Coelho J, Pessoa B, Meireles A. Long-term management of non-ischemic central retinal vein occlusion with fluocinolone acetonide intravitreal implant 190 mug (ILUVIEN(R)). Ther Adv Ophthalmol. 2019;11:2515841418820755. doi:10.1177/2515841418820755
50. Ribeiro M, Pereira AF, Penas S, Falcão-Reis F, Beato JN. 12-Month Effectiveness of the Fluocinolone Acetonide Implant (ILUVIEN®) in Retinal Vein Occlusions – Two Clinical Cases. EURETINA; 2021.
51. Kessel L, Tendal B, Jorgensen KJ, et al. Post-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: a systematic review. Ophthalmology. 2014;121(10):1915–1924. doi:10.1016/j.ophtha.2014.04.035
52. Miguel-Escuder L, Olate-Perez A, Sala-Puigdoners A, et al. Intravitreal fluocinolone acetonide implant for the treatment of persistent post-surgical cystoid macular edema in vitrectomized eyes. Eur J Ophthalmol. 2021;2021:11206721211046718.
53. Chronopoulos A, Chronopoulos P, Hattenbach LO, et al. Intravitreal fluocinolone acetonide implant for chronic postoperative cystoid macular edema - two years results. Eur J Ophthalmol;2022;11206721221124688. doi:10.1177/11206721221124688
54. Alfaqawi F, Lip PL, Elsherbiny S, Chavan R, Mitra A, Mushtaq B. Report of 12-months efficacy and safety of intravitreal fluocinolone acetonide implant for the treatment of chronic diabetic macular oedema: a real-world result in the United Kingdom. Eye. 2017;31(4):650–656. doi:10.1038/eye.2016.301
55. Ch’ng SW, Brent AJ, Empeslidis T, Konidaris V, Banerjee S. Real-world cost savings demonstrated by switching patients with refractory diabetic macular edema to intravitreal fluocinolone acetonide (Iluvien): a retrospective cost analysis study. Ophthalmol Ther. 2018;7(1):75–82. doi:10.1007/s40123-017-0114-6
56. Schmit-Eilenberger VK. A novel intravitreal fluocinolone acetonide implant (Iluvien((R))) in the treatment of patients with chronic diabetic macular edema that is insufficiently responsive to other medical treatment options: a case series. Clin Ophthalmol. 2015;9:801–811. doi:10.2147/OPTH.S79785
57. Currie CJ, Holden SE, Berni E, Owens DR. Evaluation of the clinical effectiveness of fluocinolone acetonide 190 microg intravitreal implant in diabetic macular edema: a comparison between study and fellow eyes. Curr Med Res Opin. 2017;33(sup2):19–31. doi:10.1080/03007995.2017.1366659
58. Meireles A, Goldsmith C, El-Ghrably I, et al. Efficacy of 0.2 mug/day fluocinolone acetonide implant (ILUVIEN) in eyes with diabetic macular edema and prior vitrectomy. Eye. 2017;31(5):684–690. doi:10.1038/eye.2016.303
59. Pessoa B, Coelho J, Correia N, Ferreira N, Beirao M, Meireles A. Fluocinolone acetonide intravitreal implant 190 mug (ILUVIEN(R)) in vitrectomized versus nonvitrectomized eyes for the treatment of chronic diabetic macular edema. Ophthalmic Res. 2018;59(2):68–75. doi:10.1159/000484091
60. Chakravarthy U, Taylor SR, Koch FHJ, Castro de Sousa JP, Bailey C. Changes in intraocular pressure after intravitreal fluocinolone acetonide (ILUVIEN): real-world experience in three European countries. Br J Ophthalmol. 2019;103(8):1072–1077. doi:10.1136/bjophthalmol-2018-312284
61. ILUVIEN. Summary of product characteristics. Available from: https://www.medicines.org.uk/emc/medicine/27636.
62. Parrish RK, Campochiaro PA, Pearson PA, Green K, Traverso CE. Characterization of intraocular pressure increases and management strategies following treatment with fluocinolone acetonide intravitreal implants in the FAME trials. Ophthalmic Surg Lasers Imaging Retina. 2016;47(5):426–435. doi:10.3928/23258160-20160419-05
63. Yang Y, Bailey C, Holz FG, et al. Long-term outcomes of phakic patients with diabetic macular oedema treated with intravitreal fluocinolone acetonide (FAc) implants. Eye. 2015;29(9):1173–1180. doi:10.1038/eye.2015.98
64. Cunha-Vaz J, Ashton P, Iezzi R, et al. Sustained delivery fluocinolone acetonide vitreous implants: long-term benefit in patients with chronic diabetic macular edema. Ophthalmology. 2014;121(10):1892–1903. doi:10.1016/j.ophtha.2014.04.019
65. Andreatta W, Elaraoud I, Mitra A. Dislodgement of fluocinolone acetonide intravitreal implant into the infusion cannula during vitrectomy for retinal detachment. Retin Cases Brief Rep. 2020;14(3):215–217. doi:10.1097/ICB.0000000000000678
66. de Oliveira Dias JR, Nunes RP, Goldhardt R. New drugs and new posterior delivery methods in CME. Curr Ophthalmol Rep. 2017;5(2):160–168. doi:10.1007/s40135-017-0134-3
67. Royal National Institute of Blind People (UK). Sight loss UK 2013. The latest evidence (2013); 2013. Available from: www.rnib.org.uk/sites/default/files/sight_loss_UK_2013.pdf.
68. Quhill F, Beiderbeck A. Cost advantage of fluocinolone acetonide implant (ILUVIEN) versus ranibizumab in the treatment of chronic diabetic macular oedema. Glob Reg Health Technol Assess. 2017;3(2):25.
69. Neubauer AS, Haritoglou C, Ulbig MW. Kostenvergleich zugelassener intravitrealer Therapien bei nicht ausreichend auf primäre Therapie ansprechendem diabetischem Makulaödem mit fovealer Beteiligung in Deutschland [Cost comparison of licensed intravitreal therapies for insufficiently anti-VEGF responding fovea involving diabetic macular edema in Germany]. Klin Monbl Augenheilkd. 2019;236(2):180–191. German. doi:10.1055/s-0043-125076
70. Sivaprasad S, Oyetunde S. Impact of injection therapy on retinal patients with diabetic macular edema or retinal vein occlusion. Clin Ophthalmol. 2016;10:939–946. doi:10.2147/OPTH.S100168
71. Sampat KM, Garg SJ. Complications of intravitreal injections. Curr Opin Ophthalmol. 2010;21(3):178–183. doi:10.1097/ICU.0b013e328338679a
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.