")
Back to Journals » Journal of Pain Research » Volume 8
Intrathecal morphine attenuates acute opioid tolerance secondary to remifentanil infusions during spinal surgery in adolescents
Authors Tripo P, Kuestner M, Poe-Kochert C, Rubin K, Son-Hing J, Thompson G, Tobias J
Received 16 May 2015
Accepted for publication 30 July 2015
Published 22 September 2015 Volume 2015:8 Pages 637—640
DOI https://doi.org/10.2147/JPR.S88687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michael Schatman
Paul A Tripi,1 Matthew E Kuestner,1 Connie S Poe-Kochert,2 Kasia Rubin,1 Jochen P Son-Hing,2 George H Thompson,2 Joseph D Tobias3
1Division of Pediatric Anesthesiology, 2Division of Pediatric Orthopaedic Surgery, Rainbow Babies and Children's Hospital, University Hospitals Case Medical Center, Case Western Reserve University, Cleveland, 3Department of Anesthesiology and Pain Medicine, Nationwide Children's Hospital, Columbus, OH, USA
Introduction: The unique pharmacokinetic properties of remifentanil with a context-sensitive half-life unaffected by length of infusion contribute to its frequent use during anesthetic management during posterior spinal fusion in children and adolescents. However, its intraoperative administration can lead to increased postoperative analgesic requirements, which is postulated to be the result of acute opioid tolerance with enhancement of spinal N-methyl-D-aspartate receptor function. Although strategies to prevent or reduce tolerance have included the coadministration of longer acting opioids or ketamine, the majority of these studies have demonstrated little to no benefit. The current study retrospectively evaluates the efficacy of intrathecal morphine (ITM) in preventing hyperalgesia following a remifentanil infusion.
Methods: We retrospectively analyzed 54 patients undergoing posterior spinal fusion with segmental spinal instrumentation, to evaluate the effects of ITM on hyperalgesia from remifentanil. Patients were divided into two groups based on whether they did or did not receive remifentanil during the surgery: no remifentanil (control group) (n=27) and remifentanil (study group) (n=27). Data included demographics, remifentanil dose and duration, Wong–Baker visual analog scale postoperative pain scores, and postoperative intravenous morphine consumption in the first 48 postoperative hours.
Results: The demographics of the two study groups were similar. There were no differences in the Wong–Baker visual analog scale pain scores in the postanesthesia care unit and on postoperative days 1 and 3. Pain scores were higher in the remifentanil group on postoperative day 2 (2.9 vs 3.8). Postoperative morphine requirements were similar between the two groups (0.029 vs 0.017 mg/kg/48 h for the control group and the study group, respectively).
Conclusion: In patients receiving preincisional ITM during spinal surgery, intraoperative remifentanil does not increase postoperative analgesic requirements.
Keywords: remifentanil, intrathecal morphine, idiopathic scoliosis, posterior spinal fusion, opioid tolerance, segmental spinal instrumentation
Introduction
Posterior spinal fusion (PSF) and segmental spinal instrumentation (SSI) for the treatment of idiopathic scoliosis result in significant postoperative pain.1 Strategies for managing postoperative pain include patient-controlled analgesia with intravenous (IV) opioids, epidural administration of local anesthetic agents and/or opioids, and the administration of intrathecal morphine (ITM).2 We have previously reported that the preincisional administration of ITM provides effective and safe analgesia during the postoperative period.3 Regardless of the analgesic approach, a remifentanil infusion combined with a propofol infusion is often administered intraoperatively to facilitate neurophysiological monitoring, including somatosensory- and motor-evoked potentials.
Remifentanil is an ultrashort-acting synthetic opioid with a context sensitive half-life that is unaffected by length of infusion, which contributes to its frequent use during anesthetic management during PSF and SSI.4 However, remifentanil has been associated with increased postoperative analgesic requirements thought to be secondary to acute opioid tolerance.5–8 Crawford et al5 reported that the use of a remifentanil infusion during scoliosis surgery in adolescents resulted in significantly increased postoperative morphine consumption by patient-controlled analgesia device during the first 24 postoperative hours.
The mechanism for the development of acute opioid tolerance following remifentanil may be enhancement of spinal N-methyl-d-aspartate (NMDA) receptor function.9 In an animal model, it has been demonstrated that recordings of NMDA current in cultured dorsal horn neurons are increased in the presence of clinically significant concentrations of remifentanil. Strategies to attenuate remifentanil-induced opioid tolerance during scoliosis surgery have included pretreatment with longer acting opioids or ketamine, a partial NMDA antagonist. However, a prospective, blinded study examining low-dose intraoperative ketamine infusion versus placebo in adolescents receiving remifentanil infusion during scoliosis surgery did not show a reduction in postoperative opioid requirements in patients receiving ketamine.10 Additionally, McDonnell et al11 reported that pretreatment with IV morphine did not prevent remifentanil-induced hyperalgesia following spinal surgery.
The use of both ITM and remifentanil infusions in our patient population provides a unique opportunity to assess whether postoperative acute opioid tolerance occurs in patients with idiopathic scoliosis receiving remifentanil following pretreatment with ITM. We maintain a Pediatric Orthopedic Spine Database (1992–2015), containing information including, but not limited to, demographics, visual analog scale (VAS) pain scores, and postoperative IV morphine consumption. Until 2010, patients received ITM without remifentanil, and since then, our practice has changed to include both ITM and a remifentanil infusion. We hypothesized that the administration of intraoperative remifentanil infusion would not increase postoperative pain scores and analgesic requirements in patients who had received ITM. To verify this, we conducted a retrospective review of patients undergoing spine surgery over a 3–4-year period.
Methods
Following institutional review board approval by Case Western Reserve University, we retrospectively reviewed data regarding patients with idiopathic scoliosis, who underwent PSF with SSI from December 2008 until May 2011. Patients with neuromuscular or other forms of scoliosis were excluded as were patients with idiopathic scoliosis who had same-day or staged anterior and posterior spinal fusions or anterior fusion and instrumentation only. Our Pediatric Orthopedic Spine Database and anesthesia records were our primary sources of information. After the induction of general anesthesia, all patients received preincisional ITM at a dose of 15 μg/kg (maximum dose of 1 mg). Maintenance of general anesthesia included a propofol infusion, with or without an intraoperative infusion of remifentanil. Patients also received <0.5 minimum alveolar concentration (MAC) of a volatile anesthetic agent ± nitrous oxide according to the discretion of the attending anesthesiologist. No long-acting IV opioids were administered intraoperatively, and postoperative analgesia in the first 48 hours was provided using a continuous IV morphine infusion titrated to keep Wong–Baker VAS pain scores at ≤5.12 Demographic and patient data collected included patient age at the time of surgery (years), sex, weight (kilograms), duration of surgery (hours), remifentanil infusion duration (minutes), remifentanil dose (μg/kg/min), postoperative morphine consumption (mg/kg/48 h), and VAS pain scores (range: 0–10) in the postanesthesia care unit, and on postoperative days 1, 2, and 3.
Data were analyzed using a statistical software package (SPSS Inc., version 8.0, Chicago, IL, USA). Continuous variables between two groups were analyzed using Student’s t-test. All significance levels were set at P<0.05.
Results
There were 54 patients who met inclusion criteria. All of the patients received ITM. They were further divided into two groups, those who did not receive remifentanil (control group, n=27) and those who received remifentanil (study group, n=27). There were no significant differences in the demographic variables between the two groups. Demographic data, pain scores, and opioid use are listed in Table 1. In the patients who received remifentanil, the mean infusion duration was 236 minutes and the mean remifentanil rate was 0.14 μg/kg/min. No difference was noted in postoperative opioid requirements between the two groups (0.029 mg/kg/48 h in the patients who did not receive remifentanil and 0.017 mg/kg/48 h in those who received remifentanil, P=0.068). No difference was noted in average postoperative pain scores in the postanesthesia care unit and on postoperative days 1 and 3 (Table 1). The mean pain scores were statistically higher on postoperative day 2 in patients who received remifentanil when compared to those who did not (2.9 vs 3.8, P=0.04).
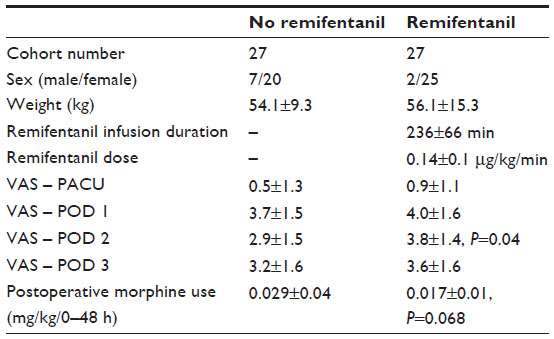 | Table 1 Demographic data of the two cohort groups |
Discussion
Patients with idiopathic scoliosis undergoing PSF and SSI experience significant postoperative pain. In a prior study, we found that preincisional administration of ITM produced safe and effective postoperative analgesia following PSF and SSI for correction of idiopathic scoliosis.3 Followed by the addition of a continuous IV morphine infusion, analgesia was extended for the first 48 postoperative hours.13 With the advent of intraoperative spinal cord monitoring using both somatosensory- and motor-evoked potentials, it is now common practice to include a remifentanil infusion, often in combination with a propofol infusion, for the intraoperative anesthetic management of such patients. Remifentanil has been associated with postoperative opioid tolerance and increased opioid requirements.5–8
In our current study, we noted that the administration of preincisional ITM blunted the hyperalgesia that has been previously reported with remifentanil, as we noted no difference in the postoperative morphine requirements between patients who received remifentanil and those who did not. In fact, although it did not meet statistical significance, the postoperative morphine requirements were lower in the patients who received ITM and remifentanil. Furthermore, the only difference noted in pain scores was a slightly higher score during postoperative day 2 in the patients receiving remifentanil. Despite the pain score being acceptable (average score of 3.8), considering the magnitude of the surgical procedure, our finding suggests that acute opioid tolerance does not develop in the first 48 postoperative hours when remifentanil is infused intraoperatively in patients receiving preincisional ITM.
There are several possible explanations as to why we did not observe acute opioid tolerance in our patients who received remifentanil after ITM. It is possible that ITM produces such profound analgesia in the early postoperative period that it overwhelms the impact of any hyperalgesia produced by remifentanil. Previous studies have suggested that patients receiving ITM do not typically require IV morphine for supplemental analgesia until 17 hours after the administration of ITM.3 Although long-term administration of ITM has been shown to produce increasing opioid requirements, this is unlikely since we showed in our prior study that ITM administration resulted in decreased morphine requirements in the first 48 postoperative hours when compared to those patients who did not receive ITM.2,3,14,15 However, it must also be recognized that nonopioid mechanisms may also be responsible for the hyperalgesia induced by remifentanil. Further work is required to clearly define the cellular mechanisms responsible for this phenomenon.
There is evidence that opioid rotation can reduce opioid requirements.16 Perhaps the rotation from ITM to remifentanil to IV morphine either increases an antinociceptive pathway or decreases a pronociceptive pathway in a manner that does not occur when only ITM and IV morphine are used. If this were true, it is possible that the study group (remifentanil + ITM) experienced both increased opioid requirements due to remifentanil and decreased requirements due to rotation, minimizing any overall impact of remifentanil on postoperative opioid requirements. Finally, over the time period of this study, our approach for maintaining general anesthesia evolved from a balanced inhalational technique with limited use of propofol to a total IV technique using remifentanil and propofol. Propofol has been shown to interact with the NMDA receptor and potentially modulate the hyperalgesia after a remifentanil infusion.17,18
This study has several limitations. It is retrospective with modest sample sizes. The anesthetic approach was not standardized among patients, and patients in the study group (remifentanil) generally received care later in the study period than those in the control group (no remifentanil). Sample sizes were modest due to the relatively recent introduction of remifentanil into our clinical practice. We did not collect data after May 2011 due to the introduction of a pain service and concurrent changes in postoperative pain management. The only significant difference between groups was the postoperative day 2 pain score in patients receiving remifentanil versus those who did not. Since most current scoliosis surgery includes spinal cord monitoring, it may be difficult to perform a prospective study where remifentanil is eliminated from the anesthetic regimen. The inclusion of propofol in the anesthetic technique may also have impact on the results, as it has been suggested that propofol may have antihyperalgesic effects on opioid-induced hyperalgesia due to inhibition of the NMDA system.19 The intent of the study was only to evaluate the acute effects of ITM on the postoperative course. As such, we cannot comment on the potential long-term implications in modulating chronic pain syndromes, which may occur following these surgical procedures.
With those caveats in mind, we noted that the administration of intraoperative remifentanil does not increase postoperative morphine requirements in patients who receive preincision ITM for PSF and SSI. Given prior data showing ITM to be safe and effective in this patient population, clinicians concerned with acute opioid tolerance secondary to remifentanil may consider preincision ITM as a postoperative pain management strategy.
Disclosure
The authors report no conflicts of interest in this work.
References
Katzer AM. Factors predicting postoperative pain in children and adolescents following spine fusion. Issues Compr Pediatr Nurs. 2000;23:83–102. | |
Son-Hing JP, Poe-Kochert C, Thompson GH, Potzman J, Tripi PA. Intrathecal morphine analgesia in idiopathic scoliosis surgery: does sex or racial group affect optimal dosing? J Pediatr Orthop. 2011;31:489–495. | |
Tripi PA, Poe-Kochert C, Potzman J, et al. Intrathecal morphine for postoperative analgesia in patients with idiopathic scoliosis undergoing posterior spinal fusion. Spine. 2008;33:2248–2251. | |
Sammartino M, Garra R, Sbaraglia F, et al. Remifentanil in children. Pediatr Anesth. 2010;20:246–255. | |
Crawford MW, Hickey C, Zaarour C, et al. Development of acute opioid tolerance during infusion of remifentanil for pediatric scoliosis surgery. Anesth Analg. 2006;102:1662–1667. | |
Guignard B, Bossard AE, Coste C, et al. Acute opioid tolerance. Anesthesiology. 2000;93:409–417. | |
Komatsu R, Turan AM, Orhan-Sungur M, et al. Remifentanil for general anaesthesia: a systematic review. Anesthesia. 2007;62:1266–1280. | |
Sharma S, Balireddy RK, Vorenkamp KE, et al. Beyond opioid patient controlled analgesia: a systemic review of analgesia after major spine surgery. Reg Anesth Pain Med. 2012;37:79–98. | |
Zhao M, Joo DT. Enhancement of spinal n-methyl-d-aspartate receptor function by remifentanil action at delta-opioid receptors as a mechanism for acute opioid-induced hyperalgesia or tolerance. Anesthesiology. 2008;109:308–317. | |
Englehardt T, Zaarour C, Naser B, et al. Intraoperative low dose ketamine does not prevent a remifentanil-induced increase in morphine requirement after pediatric scoliosis surgery. Anesth Analg. 2008;107:1170–1175. | |
McDonnell C, Zaarour C, Hull R, et al. Pre-treatment with morphine does not prevent the development of remifentanil-induced hyperalgesia. Can J Anesth. 2008;55:813–818. | |
Wong DI, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs. 1988;14:9–17. | |
Poe-Kochert C, Tripi PA, Potzman J, et al. Continuous intravenous morphine infusion for postoperative analgesia following posterior spinal fusion for idiopathic scoliosis. Spine. 2010;35:754–757. | |
Ali NM. Hyperalgesic response in a patient receiving high concentrations of spinal morphine. Anesthesiology. 1986;65:449–450. | |
Arner S, Rawal N, Gustafsson LL. Clinical experience of long-term treatment with epidural and intrathecal opioids – a nationwide survey. Acta Anaesthesiol Scand. 1988;32:253–259. | |
Koppert W. Opioid-induced hyperalgesia – pathophysiology and clinical relevance. Acute Pain. 2007;9:21–34. | |
Singler B, Troster A, Manering N, et al. Modulation of remifentanil induced postinfusion hyperalgesia by propofol. Anesth Analg. 2007;104:1397–1403. | |
Ben-David B, Chelly JE. Propofol alters ketamine effect on opiate-induced hyperalgesia. Anesth Analg. 2009;108:1353–1356. | |
Bandschapp O, Filitz J, Ihmsen H, et al. Analgesic and antihyperalgesic properties of propofol in a human pain model. Anesthesiology. 2010;113:421–428. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.