Back to Journals » Journal of Pain Research » Volume 15
Intrathecal Drug Delivery Systems Survey: Trends in Utilization in Pain Practice
Authors Abd-Sayed A, Fiala K, Weisbein J ![]() , Chopra P, Lam C
, Chopra P, Lam C ![]() , Kalia H
, Kalia H ![]() , Jassal N, Gulati A, Sayed D
, Jassal N, Gulati A, Sayed D ![]() , Deer T
, Deer T ![]()
Received 30 December 2021
Accepted for publication 14 April 2022
Published 3 May 2022 Volume 2022:15 Pages 1305—1314
DOI https://doi.org/10.2147/JPR.S344409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Alaa Abd-Sayed,1 Kenneth Fiala,1 Jacqueline Weisbein,2 Pooja Chopra,3 Christopher Lam,4 Hemant Kalia,5 Navdeep Jassal,6 Amitabh Gulati,7 Dawood Sayed,4 Timothy Deer8
1Department of Anesthesiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, 53792-3272, USA; 2Napa Valley Orthopedic Medical Group, Napa, CA, 94558, USA; 3Bux Pain Management, Danville, KY, 40422, USA; 4Department of Anesthesiology, University of Kansas, Kansas City, KS, 66160, USA; 5Rochester Regional Health, Rochester, NY, 14626, USA; 6Excel Pain and Spine, Lakeland, FL, 33805, USA; 7Department of Anesthesiology and Critical Care, Memorial Sloan Kettering Cancer Center, NY, NY, 10604, USA; 8Department of Anesthesiology, University of West Virginia, Charleston, WV, 25301, USA
Correspondence: Alaa Abd-Sayed, Email [email protected]
Background: The use of intrathecal drug delivery for chronic and cancer pain medicine has been established for decades. However, optimization and utilization of this technique still lag behind other modalities for pain control. Some of this may be due to variability of surgical technique, medication usage and education. It is currently unclear on whether or not practitioners follow available algorithms for the use of intrathecal drug delivery systems.
Methods: A survey developed by the American Society of Pain and Neuroscience (ASPN) was sent to its members via email using the cloud-based SurveyMonkey. After 30 days of being available, 159 different providers responded to the survey that consisted of 31 various multiple choice and free response questions. Each question was not required and the number of responses to each varied from 128 to 159.
Results: Approximately 9% of those who successfully received and opened the email containing the survey responded, likely due to a small number of providers working with intrathecal drug delivery systems. Eighty-six of respondents practice medicine in the United States, and 87% of the respondents were attending physicians. A majority of respondents, approximately 74%, were board certified in pain medicine with 69% of respondents being train in anesthesiology. The first and second most used medications for intrathecal pump trial were morphine and fentanyl, respectively. Most respondents, approximately 96%, provide pre-operative/intra-operative antibiotics. The most common first-choice medication for implanted intrathecal pumps was also morphine with the most common implanted location being the abdomen.
Conclusion: Interestingly, there is currently fairly substantial variation in the way providers utilize intrathecal pump delivery for both chronic and cancer pain. There is variation from the training background of the providers providing care, to the pre-implantation trial medications, to where the pump is implanted for each patient, to if the patient has the option to give themselves boluses once implanted. Further research is needed to elucidate current and best practices for intrathecal drug delivery system trials, implantations, and utilization.
Keywords: pain management, intrathecal, chronic pain, cancer pain, neuromodulation, analgesia
Corrigendum for this paper has been published.
Introduction
Intrathecal Drug Delivery has been widely utilized to treat a myriad of chronic conditions including malignant pain, low back pain, neck pain, neuropathic pain, as well as spasticity. These conditions affect a large portion of society, constituting an economic societal burden. Intrathecal drug delivery systems offer a relatively safe, cost-effective, and effective mechanism of drug delivery into the CSF, thereby allowing for more efficacious improvement in pain and spasticity while also minimizing potential adverse effects when compared to other drug administration routes.1,2 With the emergence of intrathecal pump therapies in the 1980s, early treatments were done with fixed continuous intrathecal infusion rates.3 Over the last 40 years, proceduralists have adopted technical variations, divergence, and, at times, questionable intrathecal choices for medications when performing intrathecal pump trials and permanent pump therapy.
Due to this variability, the Polyanalgesic Consensus Conference (PACC) panel was created with the purpose of publishing evidence-based best practice guidelines relating to the safety and efficacy of intrathecal pump therapy.4 This panel has since reconvened multiple times to discuss updates and improvements regarding patient safety and analgesia.5,6 Through this article, the American Society of Pain and Neuroscience (ASPN) aims to demonstrate the differences in practice and discuss their relation to PACC guidelines regarding optimal patient safety and efficacy with regards to intrathecal pump therapy. A survey-based approach was used to gather information that will improve the scope of practice and implementation of intrathecal drug delivery for chronic pain and spasticity patients.
Methods
A survey developed by ASPN was attempted to be sent to 4503 members of the American Society of Pain and Neuroscience (ASPN). The survey was sent via email on April 28th, 2021 using a cloud-based tool called SurveyMonkey to each member of the ASPN with an email on file. The estimated number of members who successfully received and opened the email was 1801. This may have been limited due to inaccurate/unused/unupdated emails for ASPN members along with only a portion of ASPN members working with intrathecal pump delivery systems. The survey was designed to identify respondent’s demographics and background, information about their practices with intrathecal pump trials, pump implantation, and post-implantation information. The survey consisted of 31 different multiple-choice and free response questions. The questionnaire was approved via waiver (does not involve human subjects and patient history information) by the University of Wisconsin Health Sciences IRB.
Each recipient of the survey was only allowed to respond a single time and they were unable to edit their responses once they submitted the survey. Any member of the ASPN who answered a question in the survey was then identified as a respondent. Some respondents who did not answer a specific question in the survey was marked as “skipped” for that question. Once distributed, 30 days were allotted for ASPN members to respond to the survey before the survey was closed and the data was analyzed. Also of note, any respondents who did not submit the survey after starting it were excluded from data analysis.
A total of 159 providers responded to the survey. Participants were not required to answer every question, so there were a variable number of responses to each question ranging from N = 128 to N=159. Data from the survey was extracted from SurveyMonkey and further translated into excel for consolidation of each questions result. The questions were further broken into 4 categories for presentation in the presentation of the results. No statistical analysis was performed due to the nature of this report addressing differences in practice rather than statistical discrepancies.
Results
Response rate of ASPN members who successfully received and opened the email with the link to the survey was estimated to be approximately 9%. However, given that a much smaller percent of ASPN members perform intrathecal pump trials and/or implants, we estimate the response rate of those directly working with intrathecal pump delivery systems to be much higher. Of these 159 respondents, 131 identified as being male, 27 as female, and 1 preferred not to say. There was a variety of provider types including attending physicians, physicians in training, nurse practitioners, and physician assistants, however, the most of respondents were attending physicians (about 87%). Of the physicians, just under 85% were board certified, 72.5% of them completed an ACGME accredited Pain Management Fellowship, and their primary board specialties included anesthesiology, physical medicine and rehabilitation, neurology, neurosurgery, and others including family medicine, neuromusculoskeletal medicine, radiology, orthopedics, and palliative medicine. More than three quarters (76.6%) of respondents attributed pain management to be dedicated to over 80% of their practice. The majority of providers, approximately 70%, fell between the ages of 31 and 50, with all but one of the remaining being 51 years old or older (Table 1). There was a wide range of years each provider has been in practice ranging from being in training now to over 25 years, (Table 1). Twenty-two of the respondents practiced medicine outside of the United States, each of the countries represented is further described in Table 1.
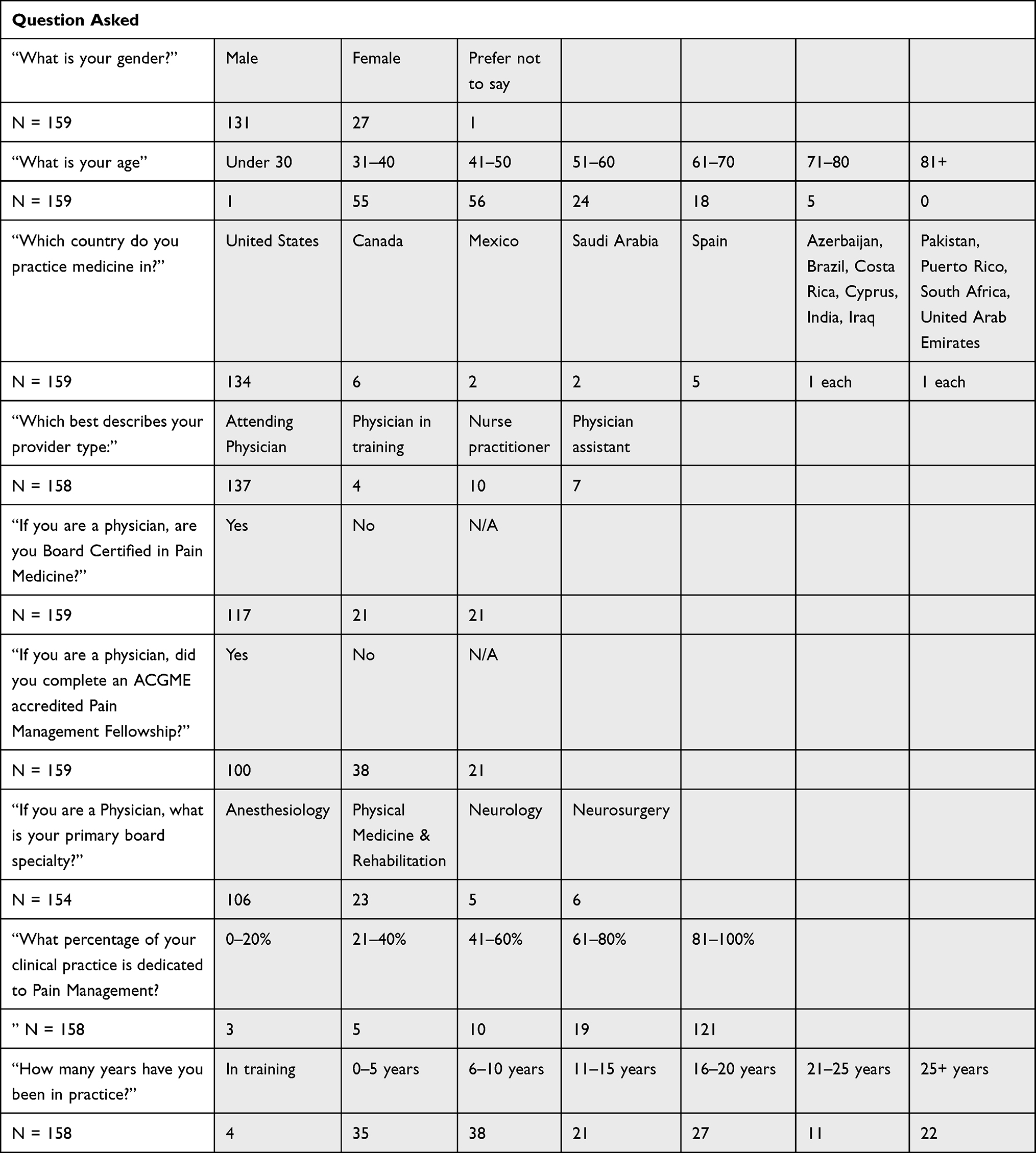 |
Table 1 Provider Demographics and Practice Background |
When specifically asked about intrathecal pump therapy, including trials, implants, interrogation, and/or refills, a total of 135 of the 159 respondents said they performed one or more of these. One hundred sixteen, or 73%, respondents perform intrathecal pump trials. However, when asked how trials of intrathecal pumps were performed, there were 138 responses with 78.3% utilizing the single shot approach and the following 21.7% utilizing techniques described in Table 2. Almost three-quarters (73.9%) of respondents never find respiratory depression after a trial for an intrathecal pump, 21% responded between 1% and 10% of the time, and the remaining respondents selected answers over 11% of the time which is further broken down in Table 2. When asked about weaning opioids prior to an intrathecal pump trial, 55.6% of respondents answered that they do wean prior to the trial and 44.4% answered that they do not wean opioids prior to the trial – for those that do wean down, there was a range of answers including a wean to 10–20%, 30%, 50%, 80%, for 48 hours, for one week without opioids, over the course of 2 months, to always below 50MEQ (milliequivalents) for non-cancer and not for cancer, with some weaning completely off. Furthermore, there were 135 responses answering what type of medications and dose that respondents typically used during the trial, answers included: morphine (MS/MSO4) ranging from 0.05mg–0.5mg, fentanyl ranging from 15mcg–100mcg, hydromorphone ranging from 50mcg–0.4mg, prialt ranging from 2mcg–5mcg, “opioids”, baclofen at 50mcg, dilaudid dosing at “100 mcg–5000mcg/day” and “0.3 mg in 2 mL volume”, ziconotide ranging from 2–8mcg and sometimes in addition to fentanyl, and a few respondents not using meds for trials. More than three-quarters (80.3%) of the providers who answer the question on giving antibiotics during an intrathecal pump trial answered that they did not give them, in addition to this 89.8% of responding providers do not prescribe oral antibiotics after the intrathecal pump trial.
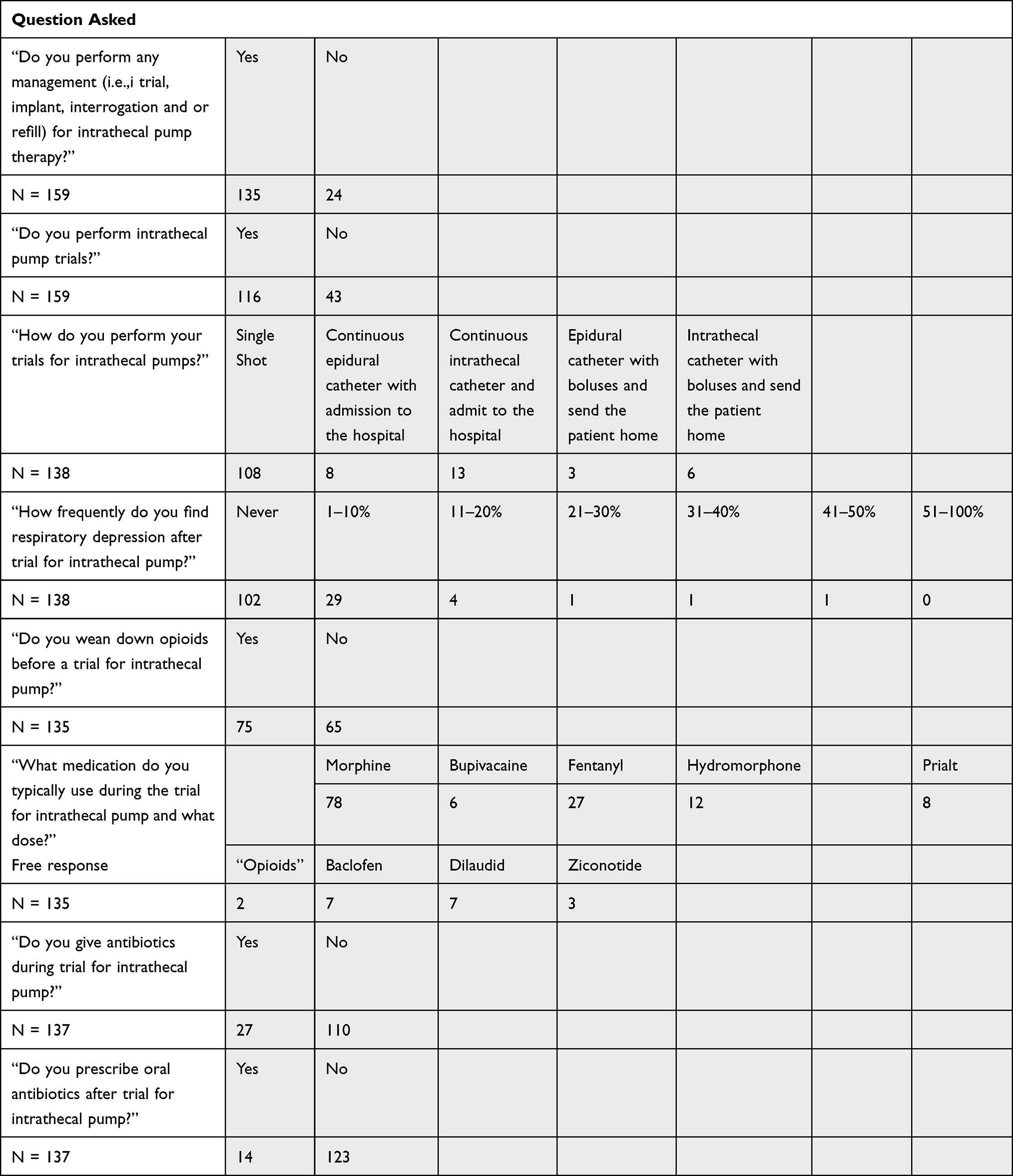 |
Table 2 Intrathecal Pump Trial |
The most common main indication for an intrathecal reported from respondents was non-cancer, chronic pain at 66.9% followed by cancer pain at 21.6%, spasticity at 7.9% and others including equal indication with pain and spasticity, both cancer and non-cancer pain, and neuropathic pain at 3.6%. More than half (66.9%) of the providers who responded to the questions asking if they implant intrathecal pumps answered yes and independently to neurosurgery, and 7.4% answered yes and in conjunction with neurosurgery. Morphine was the first-choice medication in an intrathecal pain pump for 63.3% of respondents with others using drugs described in Table 3 and mixtures of each of those drugs; as of note, one participant mentioned they used Buprenorphine since morphine was not readily available in their country. Most respondents (77.4%) surgically implant the pump in the abdomen, with a lower percentage implanting in the low back, buttock, and other locations. The most commonly used sized intrathecal pump across the respondents was 20mL mostly at 56.6% with 40mL at 27.9% and using both equally at 15.4%. Medtronic was selected by 74.5% of respondents when asked which pump brand they typically used, Flowonix was selected by 6.6% of respondents, and both Medtronic and Flowonix was selected by 16.8% of respondents. The majpority (96.3%) of the respondents selected that they give intraoperative/preoperative antibiotics during the implantation of intrathecal pumps.
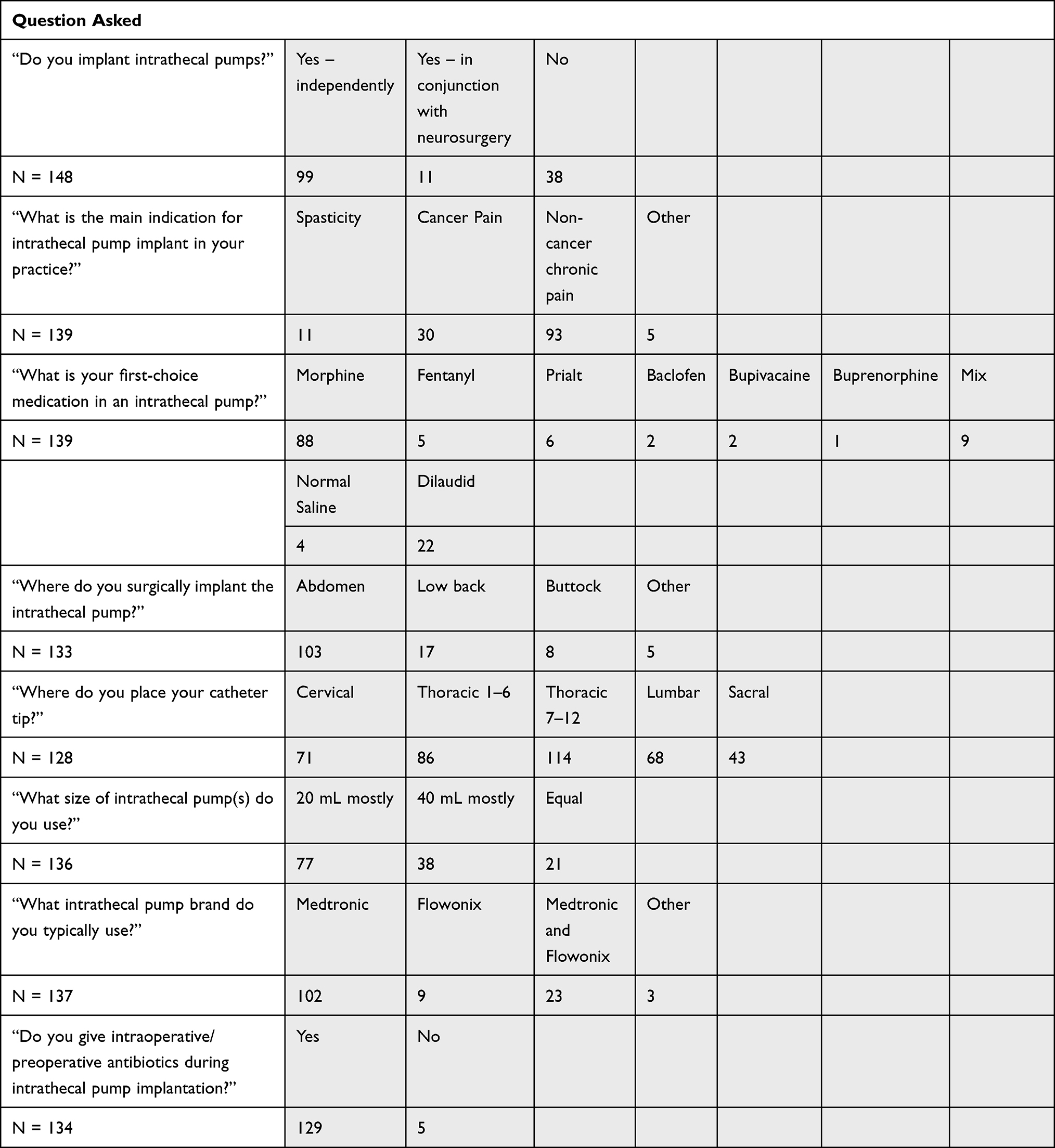 |
Table 3 Intrathecal Pump Implantation |
As shown in Table 4, 30.2% of respondents answered that they admit patients overnight after an intrathecal pump implant while 53.7% said they did not and only 16.2% answered that they only admit patients overnight if there is a comorbidity. The number of respondents who never saw respiratory depression as a side effect of intrathecal medication after implantation was 70.4%, 26.7% said they see it 1–10% of the time, two respondents said they see it 11–20% of the time, one said 21–30% of the time and one said 31–40% of the time. When asked a about what complications respondents commonly encounter after intrathecal pump implantation, 33.6% selected skin infection, 3% selected meningitis, 26.1% selected medication related complications, 29.9% selected urinary retention, 42.5% selected itching, 6% selected that they have never seen a complication, and 14.9% specified other complications including: seroma, CSF leak, pump infection, catheter dislodge secondary to injury or lifestyle, infections around the pump, postdural puncture headache (PDPH), urinary retention, pump failure, sexual insufficiency, and bruising. More than half (59.4%) of respondents answered that they do prescribe oral antibiotics prophylactically after intrathecal pump implant while 40.6% said they do not. When asked if providers typically activated the patient controlled blousing option on the intrathecal pump, 32.9% of respondents said yes, 27% said no, 31.4% said sometimes, and 12 respondents specified if there were episodes of severe pain, if needed for better coverage of episodic pain, patient dependent, if the patient wants more control, if the continuous infusion and programmed boluses are not sufficient, for an active patient, and only for cancer pain if they answered “yes or sometimes”. A few (12.4%) respondents do not perform intrathecal pump refills; of those who do perform refills, 57.9% do by palpation, 20% using ultrasound (US), and 9.7% using fluoroscopy.
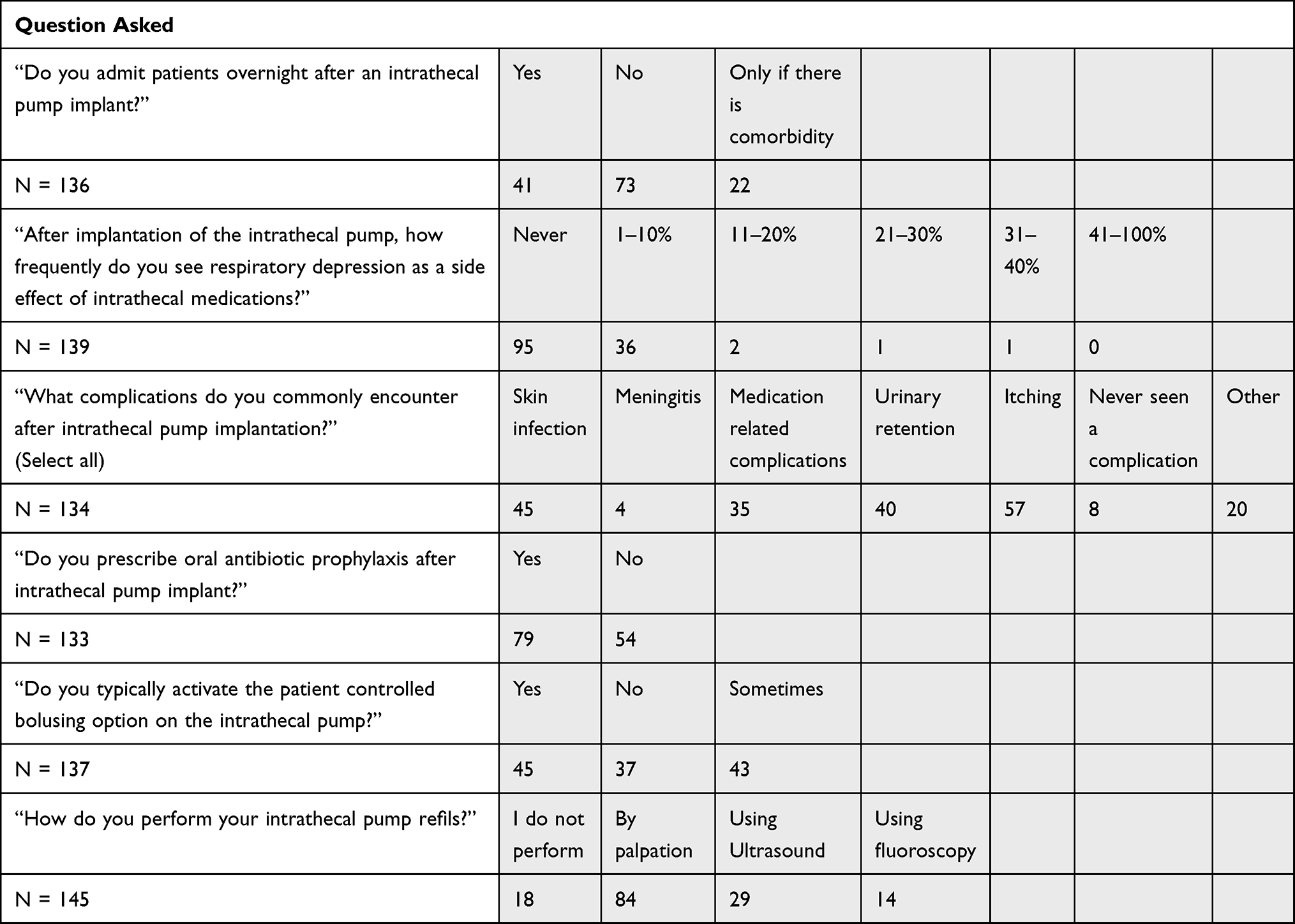 |
Table 4 Post-Intrathecal Pump Implantation |
Discussion
The ASPN IDDS survey yielded a response from 159 providers with representation from greater than 5 specialties including anesthesiology, physiatry, neurosurgery, and neurology. Female representation constituted 16.9% of all survey responders while 82.4% were male. Most survey responders were within the age range of 31–60 years of age (84.8%) with 29.5% of responders being over the age of 50. This matches closely with the national trends of trainee and provider demographics in the United States. Of the 104 accredited pain medicine fellowships representing 372 fellowship positions, 21.8% of these positions were filled by female physicians with 1.6% being non-responders and 76.6% being male. Similarly, of the 115 neurosurgical residency programs with 1462 total residency positions, 17.3% of the positions were filled by female physicians while 82.0% were male and 0.7% not responding.7 A review of the 2019 Association of American Medical Colleges data show that female providers make up 19% of all active pain medicine physicians and 9.3% of all neurosurgeons.8 Further, the percentage of active physicians greater than 55 years of age, averaged across all specialties was 44.9%.9 Deviations from these numbers may be explained by the range of international responders (Canada 3.8%, Spain 3.1%, Mexico 1.3%, Saudi Arabia 1.3%) though most survey responses were from within the United States (84.3%). Approximately 48.5% of those surveyed have practiced for fewer than 10 years while 51.5% have practiced for greater than 10 years reflecting a wide spectrum of practice preferences.
In those surveyed, 84.9% of providers incorporate IDDS in their practice to some degree with 72.9% of providers performing intrathecal trials. Of those that do trials, the majority of providers perform a single shot intrathecal injection (78.3%) while 21.7% perform an indwelling epidural or intrathecal catheter for trial. The type of trial medication used and the admission status of single shot trial patients were not surveyed. Previous studies have found no superiority among trialing methods though the consensus recommendation was trials using opioids require inpatient overnight monitoring and single dose opioid trial is not considered best practice.10
Interestingly, of those that perform a continuous catheter trial, 70% admit the patient to the hospital while 30% send the patient home the same day. The American Society of Regional Anesthesia published a 2016 practice guidelines for prevention, detection, and management of respiratory depression associated with neuraxial opioid administration.11 Though not specific for IDDS and was more reflective of perioperative neuraxial opioid use, it was recommended for patients receiving lipophilic opioids to be monitored for at least 2 hours after administration with further monitoring as indicated by patient presentation. Twenty four hour monitoring was recommended for patients who were treated with hydrophilic opioids though no differences in frequency of respiratory depression, ventilatory response to carbon dioxide, somnolence or sedation was seen when single injection morphine was compared to fentanyl or sufentanil.11
Prior to trial, 55.6% of providers wean patients of systemic opioids. Though direct recommendations for oral opioid wean prior to trial or implant were not provided in the PACC guidelines, it was recommended to not use IDDS as a salvage therapy, implicating the need to avoid IDDS use as means of pain management when patients are refractory to care by high dose oral opioids.6 Future reviews have since taken a stronger stance to recommend preprocedural opioid wean to improve post implant IDDS outcomes.12
In those that perform trials, 19.7% of providers administer peri-procedural antibiotics and 10.2% prescribed post trial antibiotics. Best practices guidelines for IDDS were published by Prager et al in 2014 do not provide recommendations for periprocedural antibiotics use or post trial antibiotic course. In 2016, the Polyanalgesic Consensus Conference (PACC) published by Deer et al compiled recommendations to improve patient safety and IDDS efficacy.6 These guidelines do recommend antibiotic administration around the time of trials based on Center of Disease Control (CDC) grade IA and National Institute for Health and Care Excellence (NICE) recommendations but no post trial antibiotics beyond 24 hours.6 The variation in peri-trial antibiotic administration may reflect the prevalence of single shot trials over indwelling catheters.
Respiratory depression was never seen in the practice of 73.9% of the providers from trials while 21.0% has seen respiratory depression in less than 10% of all the trials they performed. Little data is available regarding respiratory depression after IDDS trial with opioids. In non-obstetric populations receiving neuraxial morphine (not specific for IDDS trial), the incidence of respiratory depression was quoted as 0.01–7.0%.13,14 The findings from this survey reflect this incidence though the breakdown of trialed medication used by providers were not reported here. Further, early respiratory depression (respiratory depression within 2 hours of administration) from intrathecal morphine have not been reported, though rare instances of delayed respiratory depression from cephalad migration of intrathecal morphine has been reported.15 Though formal studies have not been published, case reports have been reported detailing respiratory depression after intrathecal fentanyl administration, and a case series has been published detailing decreased respiratory rate with increased intrathecal fentanyl dosing though literature related to IDDS trial dosing is sparse.16,17
Independent pump implants are performed in 66.9% of those surveyed while 7.4% of responders implant in conjunction with neurosurgery. The predominant first choice medication utilized was morphine (63.3%) followed by hydromorphone (15.8%). This is similar to recommendations from PACC guidelines though ziconotide or baclofen use was not captured by this survey.5,6 The pump reservoir pocket was typically implanted in the abdomen (77.4%), low back (12.8%), or buttock (6.0%). Most providers (56.6%) only implant 20 mL pumps while 27.9% implant 40 mL pumps, and 15.4% implant both. The majority of those surveyed implant peristaltic rotor pump systems only (74.5%) or both the peristaltic rotor system and the valve gated bellow system (16.8%) in their practice while 6.6% only utilize the valve gated bellow system. There is no recommendation on pump or surgeon choice based on the survey responses.
Peri-implant antibiotics during surgical implant were used in 96.3% of providers which echo the trends and recommendations from the PACC guidelines and the CDC.6 Meanwhile oral post-operative antibiotics were utilized in 59.4% of those surveyed. This practice goes against the Surgical Care Improvement Project of the Joint Commissions (SCIP) recommendations that post-operative antibiotics are not needed 24 hours after the time of implant.18 Previous studies have shown that the rate of perioperative infection for implanted pain devices to range from 2.8% to 6%.19–21 Many IDDS are utilized in cancer patients who may have concomitant immunotherapy and may be immunocompromised. Studies have shown contrary to this belief, the rates of surgical site infection for pain implants are not greater in cancer patients compared to patients without cancer.19,22 However, a study by Hoelzer et al evaluating spinal cord stimulator implants did have a statistically significant decrease in incidence of surgical site infection with use of post-operative antibiotics for 7 days in non-cancer patients.23 This practice may reflect provider preference based on these findings.
Following implantation only 30.2% of patients are admitted for overnight monitoring while 16.2% of survey responders require overnight admission if patient comorbidities indicate this. Explanation for this trend was not provided by surveyors and only 2.9% of pumps were discharged with saline. The survey did not ask about concomitant naloxone prescriptions after implant but may explain the lower-than-expected overnight admission of chronic pain pumps. Further, not all implanted pumps were for pain. Approximately 7.9% of pumps were implanted for spasticity and 3.6% were implanted for category designation “other” which can further explain the discrepancy in actual admission rate compared to prior recommendations.6,10 Additionally, 70.4% of providers have never seen post implant respiratory depression while 16.7% have seen respiratory depression in less than 10% of patients with IDDS. This clinical experience may provide and influence survey responder’s decision against post implant 24-hour admission.
Common complications seen include pruritus (42.5%), skin infection (33.6%), and urinary retention (26.1%). These results vary from those published by Kamran et al where decreased libido was the most common complication followed by constipation and pruritus.24 Interestingly, superficial wound infection constituted only 3.1% of all complications in this study and urinary hesitancy was found in 9.2% of their patient complication cohort. Medication associated complications were noted by 26.1% of surveyed providers. These findings may reflect the prevalence of the complication seen across surveyed practices but not the true incidence of the complication in the surveyed cohort’s practice.
Once implanted, patient therapy manager or patient therapy controller was activated by 32.9% of providers while 31.5% activate this device “sometimes.” The variation in practice may reflect the question as it is vague whether activation refers to activation at the time of implant or activation over lifetime of the device. Thus, a larger percentage of providers may have selected “no” in reference for time of implant rather than lifetime of the device. The majority of providers that do refill their own IDDS (87.6%) do so by palpation (57.9%) or US (20.0%) while fluoroscopy was seldomly used (9.7%). It does appear education may be helpful to improve use of intrathecal boluses, especially for the management of pain.
The goal of this survey was to evaluate variations in intrathecal drug delivery systems practice characteristics across all providers. This was further achieved through various members of the interdisciplinary team being respondents, importantly so due to the pain management team built upon the collaboration of all providers represented in this survey.25
Limitations
Interpretation of the information from this survey should be performed with care. This survey’s small sample size needs to be considered as it consisted of only 159 participants and this could lead to potential response bias. The large difference in those who were sent the email and those who successfully received and opened the email may be partially attributed to incorrect or unused emails being on file for their ASPN accounts. Furthermore, the small response percentage, 9%, of those who successfully received and opened the email and completed the survey may reflect the small fraction of ASPN members who work with intrathecal drug delivery systems consistently as a part of their practice. Only 73.6% of survey respondents were board certified in pain medicine while 62.9% completed an ACGME accredited pain management fellowship and this also needs to be taken into consideration. These numbers can be partially explained by the 13.3% responder made up by non-attending physician providers (including physicians in training, APRN-NP’s, and PAs) who participated in this survey.
Conclusion
Many interventional pain physicians utilize some form of intrathecal drug delivery in their practice, however, this may only be a fraction of all pain management providers and ASPN members. There is variation most all aspects of intrathecal drug delivery systems from the health professionals providing the care to the actual pump used itself. The most common response for intrathecal drug delivery system main indication was chronic non-cancer pain, although cancer pain spasticity, and “other” were noted. The most reported first-choice medication in an intrathecal drug delivery system was morphine with the most common implant location of the pump being in the abdomen. Although this was a small sample size, a majority of the responding providers did not report serious complications; such as most having never seen respiratory depression as a side effect. This may add to current literature supporting the safety of intrathecal drug delivery systems. It must be noted that it is possible for response bias to be present due to the voluntary nature and small sample size of this survey. Further research into intrathecal drug delivery system practices should be sought out as this could help develop a more precise standard of care for the patients for needing this for adequate pain control.
Disclosure
Dr Jacqueline Weisbein received fees for consulting and research form Medtronic, Abbott, Saluda, and Boston Scientific, outside the submitted work. Dr Pooja Chopra reports personal fees from Flowonix, outside the submitted work. Dr Amitabh Gulati reports personal fees from Medtronic, personal fees from Flowonix, personal fees from AIS Healthcare, personal fees from Tremeau medical, personal fees from SPR therapeutics, personal fees from Nalu Medical, during the conduct of the study. Dr Dawood Sayed reports personal fees from Medtronic, personal fees from Flowonix, outside the submitted work. Dr Timothy Deer reports personal fees from Medtronic, during the conduct of the study; personal fees from Abbott fees, Vertos, Flowonix, SpineThera, Saluda, Mainstay, Nalu, Cornerloc, Ethos, SPR Therapeutic, SI Bone, Nevro, Boston Scientific, PainTeq, Tissue Teq, and Avanos, outside the submitted work. In addition, Dr Timothy Deer has a patent Abbott pending to Abbott & Tim Deer.
References
1. Duarte RV, Lambe T, Raphael JH, Eldabe S, Andronis L. Intrathecal drug delivery systems for the management of chronic noncancer pain: a systematic review of economic evaluations. Pain Pract. 2018;18(5):666–686. doi:10.1111/papr.12650
2. Stearns LJ, Narang S, Albright RE, et al. Assessment of health care utilization and cost of targeted drug delivery and conventional medical management vs conventional medical management alone for patients with cancer-related pain. JAMA Netw open. 2019;2(4):e191549. doi:10.1001/jamanetworkopen.2019.1549
3. Wallace M, Yaksh TL. Long-term spinal analgesic delivery: a review of the preclinical and clinical literature. Reg Anesth Pain Med. 2000;25(2):117–157.
4. Deer TR, Pope JE, Hayek SM, et al. The Polyanalgesic Consensus Conference (PACC): recommendations for intrathecal drug delivery: guidance for improving safety and mitigating risks. Neuromodulation. 2017;20(2):155–176. doi:10.1111/ner.12579
5. Deer TR, Pope JE, Hanes MC, McDowell GC. Intrathecal therapy for chronic pain: a review of morphine and ziconotide as firstline options. Pain Med. 2019;20(4):784–798. doi:10.1093/pm/pny132
6. Deer TR, Pope JE, Hayek SM, et al. The Polyanalgesic Consensus Conference (PACC): recommendations on intrathecal drug infusion systems best practices and guidelines. Neuromodulation. 2017;20(2):96–132.
7. Accreditation Council for Graduate Medical Education. Data resource book: academic year 2018–2019; 2019.
8. AAMC. Active physicians by sex and speciality. physician specialty data report; 2019. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-sex-and-specialty-2019.
9. AAMC. 2020 physician specialty report data highlights. physician specialty data report; 2020. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/2020-physician-specialty-report-data-highlights.
10. Prager J, Deer T, Levy R, et al. Best practices for intrathecal drug delivery for pain. Neuromodulation. 2014;17(4):
11. An Updated Report by the American Society of Anesthesiologists Task Force on Neuraxial Opioids. Practice guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid administration: an updated report by the American Society of Anesthesiologists Task Force on Neuraxial Opioids and the American So. Anesthesiology. 2016;124(3):535–552. doi:10.1097/ALN.0000000000000975
12. Abd-Elsayed A, Karri J, Michael A, et al. Intrathecal drug delivery for chronic pain syndromes: a review of considerations in practice management. Pain Physician. 2020;23(6):E591–617.
13. Carvalho B. Respiratory depression after neuraxial opioids in the obstetric setting. Anesth Analg. 2008;107(3):956–961. doi:10.1213/ane.0b013e318168b443
14. Shapiro A, Zohar E, Zaslansky R, Hoppenstein D, Shabat S, Fredman B. The frequency and timing of respiratory depression in 1524 postoperative patients treated with systemic or neuraxial morphine. J Clin Anesth. 2005;17(7):537–542. doi:10.1016/j.jclinane.2005.01.006
15. Ruan X. Drug-related side effects of long-term intrathecal morphine therapy. Pain Physician. 2007;10(2):357–366. doi:10.36076/ppj.2007/10/357
16. Belzarena SD. Clinical effects of intrathecally administered fentanyl in patients undergoing cesarean section. Anesth Analg. 1992;74(5):653–657.
17. Cornish PB. Respiratory arrest after spinal anesthesia with lidocaine and fentanyl. Anesth Analg. 1997;84(6):1387–1388. doi:10.1213/00000539-199706000-00041
18. Rosenberger LH, Politano AD, Sawyer RG. The surgical care improvement project and prevention of post-operative infection, including surgical site infection. Surg Infect. 2011;12(3):163–168. doi:10.1089/sur.2010.083
19. Engle MP, Vinh BP, Harun N, Koyyalagunta D. Infectious complications related to intrathecal drug delivery system and spinal cord stimulator system implantations at a comprehensive cancer pain center. Pain Physician. 2013;16(3):251–257.
20. Scanlon MM, Gazelka HM, Moeschler SM, et al. Surgical site infections in cancer patients with intrathecal drug delivery devices. Pain Med. 2017;18(3):520–525.
21. Malheiro L, Gomes A, Barbosa P, Santos L, Sarmento A. Infectious complications of intrathecal drug administration systems for spasticity and chronic pain: 145 patients from a tertiary care center. Neuromodulation. 2015;18(5):421–427. doi:10.1111/ner.12265
22. Sindt JE, Larsen SD, Dalley AP, Collier WH, Brogan SE. The rate of infectious complications after intrathecal drug delivery system implant for cancer-related pain is low despite frequent concurrent anticancer treatment or leukopenia. Anesth Analg. 2020;131(1):280–287. doi:10.1213/ANE.0000000000004639
23. Hoelzer BC, Bendel MA, Deer TR, et al. Spinal cord stimulator implant infection rates and risk factors: a multicenter retrospective study. Neuromodulation. 2017;20(6):558–562. doi:10.1111/ner.12609
24. Kamran S, Wright BD. Complications of intrathecal drug delivery systems. Neuromodulation. 2001;4(3):111–115. doi:10.1046/j.1525-1403.2001.00111.x
25. Adler JA, Lotz NM. Intrathecal pain management: a team-based approach. J Pain Res. 2017;10:2565–2575. doi:10.2147/JPR.S142147
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.