Back to Journals » Clinical Ophthalmology » Volume 17
Intraoperative Complication Rates in Cataract Surgery After Resuming Surgery Following the COVID-19 Shutdown
Authors Das S, Mehregan C, Richards C ![]() , Schneider M, Le K, Lin X
, Schneider M, Le K, Lin X
Received 5 December 2021
Accepted for publication 15 November 2022
Published 23 February 2023 Volume 2023:17 Pages 641—647
DOI https://doi.org/10.2147/OPTH.S348710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Shibandri Das,1 Christian Mehregan,1 Collin Richards,2 Michael Schneider,1 Kim Le,3 Xihui Lin1
1Kresge Eye Institute Department of Ophthalmology, Visual and Anatomic Sciences, Wayne State University School of Medicine, Detroit, MI, USA; 2Wayne State University School of Medicine, Detroit, MI, USA; 3Department of Ophthalmology, Henry Ford Hospital, Detroit, MI, USA
Correspondence: Xihui Lin, Kresge Eye Institute, Department of Ophthalmology, Visual and Anatomic Sciences, Wayne State University School of Medicine, Detroit, MI, USA, Tel +1 314-359-2691, Fax +1 313 577-9675, Email [email protected]
Purpose: To evaluate surgeon performance and intraoperative complication rates of cataract surgery after resumption of elective surgeries following the operating room (OR) shutdown from the coronavirus disease 2019 (COVID-19) pandemic. Subjective surgical experience is also evaluated.
Methods: This is a retrospective comparative study which analyzes cataract surgeries performed at an inner city, tertiary academic center. Cataract surgeries were categorized into Pre-Shutdown (January 1–March 18, 2020), and Post-Shutdown, for all cases which occurred after surgeries resumed (May 11–July 31, 2020). No cases were performed between March 19 and May 10, 2020. Patients undergoing combined cataract and minimally invasive glaucoma surgery (MIGS) were included, but MIGS complications were not counted as cataract complications. No other combined cataract-other ophthalmic surgeries were included. A survey was used to gather subjective surgeon experience.
Results: A total of 480 cases (n=306 Pre-Shutdown and n=174 Post-Shutdown) were analyzed. Although there was a higher frequency of complex cataract surgeries performed Post-Shutdown (5.2% vs 21.3%; p< 0.00001), complication rates before versus after the shutdown were not statistically significant (9.2% vs 10.3%; p=0.75). Phacoemulsification was the step of cataract surgery in which residents were most concerned about when returning to the OR.
Conclusion: After the surgical hiatus due to COVID-19, significantly more complex cataract surgeries were reported and surgeons reported higher general anxiety level when first returning to the OR. Increased anxiety did not lead to higher surgical complications. This study provides a framework to understand surgical expectations and outcomes for patients whose surgeons faced a prolonged two-month hiatus from cataract surgery.
Keywords: cataract surgery, cataract surgery complication rate, COVID-19 pandemic, simulation training in residency, cataract surgery training, lapse in cataract surgery training
Introduction
Cataract is the most common cause of blindness worldwide.1 Over 9.5 million cataract surgeries are performed across the globe every year, making it one of the most common surgical procedures conducted. This number is expected to grow as the patient population continues to age.2,3 The National Eye Institute expects the rate of cases of cataract in the United States to double from 24.4 million to 50 million between the years 2010 and 2050.4 Cataract extraction has been shown to significantly improve a patient’s vision-related quality of life,5,6 as well as added benefits in the elderly of increased cognitive function,7 decreased depressive symptoms,8 and decreased risk of hip fracture due to fall.9 Furthermore, as second-eye-cataract surgery further increases vision, this has been found to further increase5,9 quality of life in patients.3
The coronavirus disease 2019 (COVID-19) pandemic created a unique situation for surgeons in the USA, in which elective surgeries were suspended anywhere from one to two months based on the institution and specific state of employment.10 For most surgeons in the USA, this represents the longest duration without operating, for the first time, while in or since residency or fellowship training.10 The UK, which had a longer prolonged shutdown of elective cases for six months, twice during the COVID-19 pandemic, has published on the effect of such a shutdown on the long-term complication rates of cataract surgery.11 Theodoraki et al describes the shutdown periods as P2 (June 2020 – January 2021) and P3 (January 2021 to July 2022).11 These authors found that nine months after P3, there was a statistically significant increase in cystoid macular edema as well as posterior capsular rupture (PCR).11 These changes were present irrespective of surgeon seniority level.11 Our own institution underwent a shorter but still significant two month shutdown of elective surgeries to limit the spread of COVID-19 and allow allocation of resources for COVID-19 endeavors; we decided to examine the intraocular complication rate and individual surgeon anxiety to reoperating as this has yet to be examined abroad, or within the USA.
When elective surgeries were restarted in the state of Michigan, there was a backlog of cataract surgeries to be performed at our institution. Similar backlogs have been noted or anticipated in other countries, such as Italy and Switzerland.12,13 Upon the re-opening of the operating room, new challenges have been encountered, such as how to provide a safe environment for cataract surgery to be performed and how to limit the potential spread of COVID-19.14 Surveys on patient attitudes regarding cataract surgery during the COVID-19 pandemic have shown that a sizable portion of them are not willing to return to a healthcare setting.15–17 These two factors led to lower case numbers during this time and from a patient perspective they were more likely to stay at home,16 however we have yet to find a study verifying whether surgeons had a conservative case selection or performed more complex cataract surgeries when surgery first resumed, which is explored in our study.
To our knowledge, no study has looked at the success or intraoperative complication rates of cataract surgery prior to and after the pandemic induced two-month shutdown of elective surgeries in the USA. The goal of this study is to assess the rate of complex cataract surgery before versus after the pandemic and to examine whether the risk of a variety of intraoperative complications prior to versus after the shutdown was higher, potentially due to surgeon “rustiness.” Our study explores the impact of a two-month hiatus on intraoperative complications, and it is important to note that a longer hiatus may lead to differing outcomes. We also administered a survey to surgeons to assess their attitudes and experiences about their return to operating after the pandemic induced layoff. Tzamalis et al (2021) surveyed cataract surgeons to determine the subjective impact of a two-month hiatus on deskilling and found that 37.5% (3/8) surgeons classified the impact as “somewhat” or “a lot” and 62.5% (5/8) surgeons reported being more careful in their initial cases post-lockdown.18 In our study we took a deeper dive to better understand subjective reasoning for deskilling and the number of cases needed to rebuild a surgeon’s subjective confidence.
Methods
Institutional review board (IRB) approval (#20-07-2540) was obtained from Wayne State University (WSU). As a retrospective chart review, our study was granted exempt review status with waiver of consent for all subjects. All subjects in the study were treated in accordance with the Declaration of Helsinki. A review of patient charts who underwent cataract surgeries between January 1, 2020 through July 31, 2020 was conducted. Cataract surgeries were categorized into Pre-Shutdown (January 1, 2020 – March 18, 2020) if they occurred prior to elective surgery suspension on March 18, 2020 and Post-Shutdown, for all cases (May 11, 2020 – July 31, 2020) that occurred after the resumption of elective surgeries on May 11, 2020. No elective cataract surgeries were performed by ophthalmologists between the dates of March 19 to May 10, 2020. This shutdown of 54 days is approximately eight weeks and thus, classified as a two-month hiatus in our study for ease of reference to current studies in the field which also classify shutdown periods in monthly units.
Data gathered retrospectively, both manually and electronically, from patient charts included date of service of cataract surgery, name of operating surgeon, operations performed in addition to simple or complex cataract surgery, and any intraoperative complications which are further detailed in the following paragraphs. Patients over the age of 18 were included if the patient underwent cataract surgery alone, or cataract surgery at the same time as minimally invasive glaucoma surgery (MIGS). For an included cataract-MIGS concurrent procedure, any complications related to the MIGS portion of the procedures such as difficulty with a MIGS device were not recorded as one of the labeled cataract surgery complications. Patient who had MIGS concurrent with cataract surgery were included as their device-related intraocular complications could be easily separated from the intraocular complications consistent with cataract surgery and therefore would not be a confounding factor in the results. Furthermore, there were no cataract-MIGS concurrent procedures with confounding complications such as hyphema or hypotony during the study period; had this occurred those cases would have been excluded. Patients were also excluded if they had any other intraocular procedure, other than already stated, concurrent with cataract surgery.
When deciding the operating surgeon, cataract surgeries were classified as being performed by a resident if the resident was a post-graduate-year-3 (PGY-3) ophthalmology resident who performed greater than 50% of the procedure as the primary surgeon. Otherwise, if the surgeon was an attending or a fellow-in-training, the surgery was considered an attending case. All patients included followed the COVID-19 protocols of our institution at the time, and there was no exclusion based on systemic co-morbidities alone.
Cases were labeled as simple or complex cataract cases. A complex cataract surgery was defined in accordance with the common procedure terminology definition (CPT code) as cases which require iris expansion devices, capsular support devices, capsular stain in the setting of mature cataract, or other techniques not generally used in routine cataract surgery.19 A CPT code of 66982 denoted a complex cataract surgery case, and CPT code of 66984 denoted a simple cataract surgery case, and this was always decided by those attending the case. Data were collected on the usage of capsular tension ring placement for zonular dialysis, occurrence of rhexis run off, posterior capsular rupture, and anterior vitrectomy. Intraoperative complications were defined as posterior capsular rupture, the need for anterior vitrectomy, unanticipated need for capsular tension ring, or unanticipated rhexis run off.
An online survey was administered via SurveyMonkey® to surgeons classified as attending and graduating residents between June 1, 2020 and July 31, 2020. The survey retrospectively assessed their levels of anxiety upon returning to the operating room after the COVID-19 induced shutdown, their individual surgical volume prior to and after the shutdown, and their methods for preparing for their return to operating after the two-month hiatus. We administered the survey to a total of 17 surgeons which comprised of 10 attending and seven graduating residents all of whom completed cases during the study period. A total of 12 surgeons completed the survey, and of those 12, six were graduating ophthalmology residents and six were attending surgeons. Of note, while the surgical cases and data of the seven incoming PGY-3 ophthalmology residents during this study period were included, we did not disseminate the survey to them as our study focused on subjective survey results of surgeons who do not require supervision or will not require supervision soon after the resumption of elective cataract surgery.
All the data were categorical; comparative analysis was performed on Windows version 11 using Fisher’s Exact Test on two-by-two contingency tables. Statistical significance is defined by a p-value of less than 0.05.
Results
A total of 480 cataract surgeries were included. Of those, 306 surgeries were performed in the time period before COVID-19 shutdown from January 1, 2020 – March 18, 2020, and 174 surgeries were performed after elective surgeries were resumed between May 11, 2020 and July 31, 2020. In the Pre-Shutdown group, 220 surgeries were performed by an attending surgeon compared with 86 by residents. In the Post-Shutdown group, 103 surgeries were performed by an attending surgeon vs 71 by residents (p<0.005). Of the 306 cataract surgeries performed in the Pre-Shutdown group, 16 were considered complex, and 37 were concurrent MIGS. Of the 174 cataract surgeries performed in the Post-Shutdown group, 37 were classified as complex (p<0.00001) and 14 were concurrent MIGS (p=0.33). The MIGS performed included Kahook Dual Blade goniotomy, placement of iStent or Xen gel stent implants. Table 1 summarizes the breakdown of cataract surgery numbers by surgeon, complexity, and concurrent performance of MIGS before and after the COVID-19 shutdown.
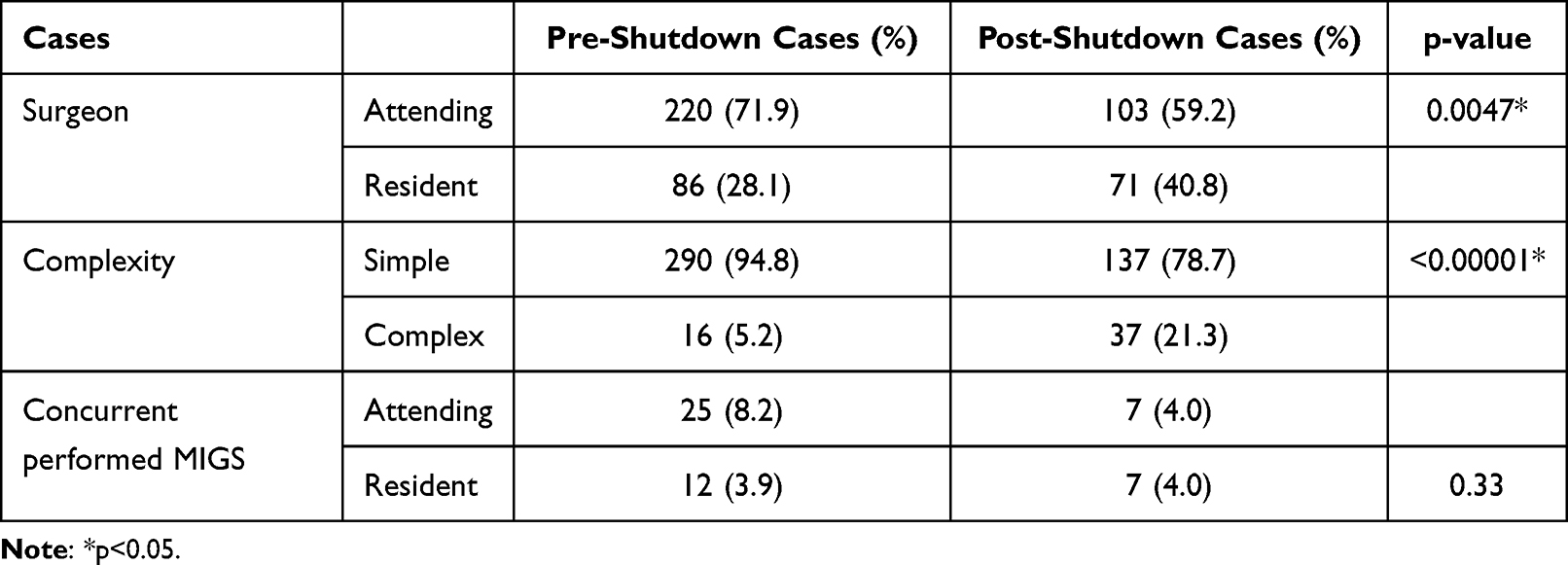 |
Table 1 Breakdown of Cataract Surgery Cases by Surgeon, Complexity, and Concurrent MIGS |
Table 2 shows the difference in cataract complications before and after the shutdown. The complication rates before and after the shutdown was not statistically significant (9.2% vs 10.3%; p=0.75).
 |
Table 2 Cataract Surgery Complication Rates Before and After the COVID-19 Shutdown |
Table 3 shows the complication rates before and after the COVID-19 shutdown, subdivided by attending surgeons versus residents. When looking at all cases, attending surgeons did have significantly lower complication rates (15 of 323; 4.6%) compared with resident surgeons (31 of 157; 19.7%); (p<0.00001). However, there was no statistical difference within each group before and after the COVID-19 shutdown (p>0.12).
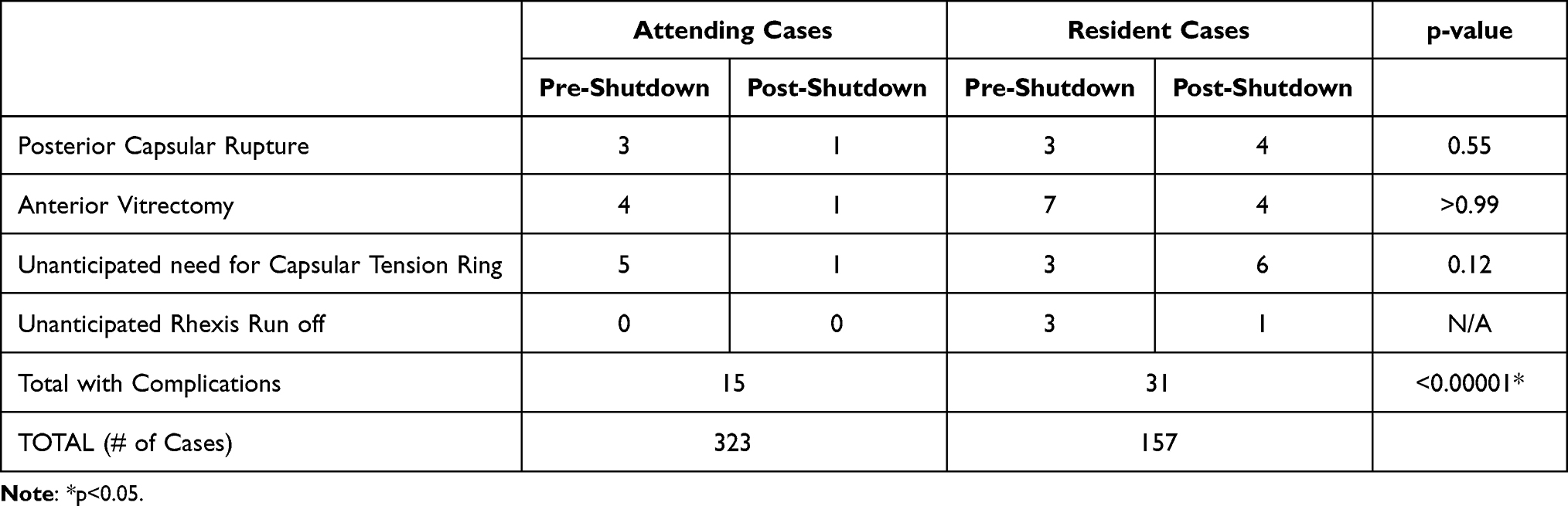 |
Table 3 Cataract Surgery Complication Rates Subdivided by Attending surgeons versus Residents |
Our survey was sent to 17 of 24 surgeons who were involved in operating during the study period. Those seven excluded were the seven incoming PGY-3 residents. Of those who received the survey, 70.6% responded. Of the 12 surgeons who responded to our survey, six were attending surgeons and six were residents. Thus, the response rate was 60% among attending surgeons and 85.7% among residents. Of the surgeons who responded to the survey, a majority felt at least mildly anxious after returning to the operating room with over 80% attributing this to “feeling out of practice on a particular step.” When asked how many cases would be needed to feel comfortable again, 50% reported needing between three to five cases. The full responses to the survey are shown in Supplement.
Discussion
The higher frequency of complex cataract surgeries Post-Shutdown likely reflects the prioritization of patients with more severe visual impairment in the immediate reopening of outpatient surgical centers. Various criteria and methods for prioritization of patients requiring cataract surgery after reopening have been discussed.12,20 Although our academic center did not implement an institution-wide policy for this, individual surgeons did implement personal policies. Of note, in our study, case complexity was viewed as an objective measure as it was quantifiably related to billing by use of CPT code However, it cannot be overlooked that case complexity may be partially influenced by surgeon confidence, and therefore increases in complex cases Post-Shutdown may be a mix of “true” and “perceived” complexity. It is also important to recognize that this study was conducted in the context of a two-month hiatus, and results may vary with a changing length of hiatus and with differing procedures. Overall, there was a trend towards more conservative criteria for cataract surgery selection during this period.
The increased incidence of complex cataract surgeries Post-Shutdown might have led to an increased complication rate. Previous studies have shown that certain preoperative risk factors such as mature cataracts, those deemed to have zonular pathology,21 pseudoexfoliation, small pupil diameter, and long axial length22 put patients at increased risk for complications of cataract surgery including posterior capsular rupture. A study at a Canadian Institution showed that cataract cases deemed to be “simple” preoperatively had a significantly lower complication rate than those deemed to be “complex.”23 A common complication analyzed by the majority of studies investigating cataract surgery complications is rate of PCR.21,23–30 In our study, the incidence of PCR in resident-performed cataract surgeries was 4.5%, which is similar to the incidence found in previous studies at other institutions which have generally shown rates from 0.8–7.6%, though one study24 showed rates as high as 17.3% depending on method of teaching.21,23,25–30 The incidence of PCR in attending-performed cataract surgery was found to be 1.2%. It was not unexpected to see higher complication rates of residents compared with attending surgeons.31 It was however, surprising to see similar complication rates before and after the COVID-19 shutdown.
Although our rate of complications did not increase after the COVID-19 shutdown, the difficulty and outcome of cataract surgeries during this period may not necessarily be the same as prior to COVID-19. One important factor not tracked by our study is the actual difficulty of the cataract surgery during the two periods analyzed. It is possible that the average surgery time may have been longer or the average cataract more dense Post-Shutdown. Tzamalis et al (2021) showed a statistically significant increase in cataract surgery duration post lockdown, from 16.8 ± 5.1 minutes to 19.1 ± 6.1 minutes (p=0.0001).18 This difference was found even when excluding complicated surgeries from the analysis.18 To fully understand the implication of these findings on patient outcomes, further studies on long-term visual acuity and refractive outcomes could be investigated.
In analyzing subjective experience, the majority of the surgeons in the study felt at least mildly anxious when returning to the operating room. While increased case complexity can factor into increased level of anxiousness, the main concern as reflected by our survey was being out of practice for a certain step in the surgery. After a prolonged period without operating, these results are consistent with our expectations. It was comforting to see that none of the surgeons were severely anxious or required more than 10 cases to feel “comfortable” again. A UK study investigating the subjective experience of returning cataract surgeons after a lockdown hiatus (median of 15 weeks) showed that trainees and those with less surgical experience reported a larger deskilling as compared with experienced surgeons.32 Our study helps quantify the number of cases needed to feel comfortable again, at around three to five cases, for the average surgeon. As we blinded ourselves to the survey respondents’ level of skill, we could not reproduce breakdowns in perceptions of deskilling as seen in the UK study.32
The results of this study imply that surgeons who take a two-month long break from surgery are not at a higher risk of causing complications upon their return to the operating room. This is particularly applicable information for recent graduates to know as they often take some amount of time off between graduation and starting their employment. The authors of this study would caution about extrapolating these findings to breaks significantly longer than the two-month break and remind that further studies are needed to assess the difficulty of these cases. It is also notable that 92% of our surveyed surgeons reported doing some sort of preparation for their return to the operating room Post-Shutdown. This extra preparation, such as increased use of simulator training, might have contributed to the similar complication rates from before and after the shutdown. Simulator training has been shown to decrease complication rates in resident cataract surgery.33,34 Furthermore, studies have shown that residents who do extra preparation work did not have increased complication rates in other higher stress situations, such as operating on monocular patients.35
A weakness of this study is the unequal size of the two groups being examined, with 306 surgeries in the Pre-Shutdown group vs 174 surgeries in the Post-Shutdown group. This difference in sample sizes in two time periods of similar length illustrates the lower rate of cataract surgery being performed in the period immediately following the lift of the shutdown of elective surgeries. This limitation is likely due to patient behavior patterns as a result of the COVID-19 pandemic17 and could be a combination of patient and facility-related factors. Facility-related factors include a slow ramp up to maximum volume in the operating room, staffing shortages, and the initial higher threshold for which surgeries could be scheduled. Patient-related factors include the hesitance of patients to come back to the clinic and patients needing COVID testing prior to surgery.17 Both patient-related and facility-related factors added a level of difficulty to organizing care in the Post-Shutdown time period. There was also a significant decrease in cases performed by an attending surgeon as opposed to the residents before versus after lockdown. This difference was due to attending surgeons’ prioritization of PGY-3 performance of cases Post-Shutdown to ensure they would have enough surgical exposure to meet training requirements as the pandemic and its effects were still unknown. With regards to limitations in assessing complications in our study, postoperative complications such as macular edema, corneal decompensation, and endophthalmitis, were not addressed in the study. The former complications would have been diagnosed primarily during follow-up office visits. The goal of our study, however, was more focused on complications and performance of surgeons, and their apprehensions during the surgery after the two-month hiatus. A future study to explore post-operative complications could be a useful next step, helping us identify additional factors correlating with patient outcomes, but a similar study has already been performed in the UK.11 Despite these limitations, the main conclusions of the study are valid and nuanced, especially for trainees who may need to take a similar amount of time off from operating for any reason.
In conclusion, after a prolonged break from surgery due to the COVID-19 mandated shutdown of elective procedures, there was a higher proportion of complex cataract surgeries performed. This did not lead to higher rates of surgical complications during this period. Overall, surgeons are more anxious during the first 10 cases after the pause, but simulator and video review appeared to help prepare the surgeon for a safe return to the operating room. The results of this study likely can be extrapolated to other situations of a two-month hiatus from surgery and reaffirms that surgeons are not at increased risk of intraoperative complications after such a break.
Acknowledgments
This study was supported in part by an unrestricted grant to the Department of Ophthalmology, Visual and Anatomic Sciences from Research to Prevent Blindness, Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
2. Friedman DS, O’Colmain B. Vision problems in the U.S. fifth; 2012.
3. Micieli JA, Arshinoff SA. Cataract surgery. CMAJ Can Med Assoc J. 2011;183(14):1621. doi:10.1503/cmaj.110549
4. Amedo AO, Koomson NY, Pascal TM, Kumah DB, Ocansey JNA, Asare-Bediako B. Quality of life of cataract patients before and after surgery-evidence from four rural communities in Ghana. Mathews J Ophthalmol. 2016;1(1):1–7.
5. Li SS, Misra S, Wallace H, Hunt L, McKelvie J. Patient-reported quality of life for cataract surgery: prospective validation of the “Impact on Life” and Catquest-9SF questionnaires in New Zealand. N Z Med J. 2019;132(1503):34–45.
6. Lin H, Zhang L, Lin D, et al. Visual restoration after cataract surgery promotes functional and structural brain recovery. EBioMedicine. 2018;30:52–61. doi:10.1016/j.ebiom.2018.03.002
7. Ishii K, Kabata T, Oshika T. The impact of cataract surgery on cognitive impairment and depressive mental status in elderly patients. Am J Ophthalmol. 2008;146(3):404–409. doi:10.1016/j.ajo.2008.05.014
8. Tseng VL, Yu F, Lum F, Coleman AL. Risk of fractures following cataract surgery in Medicare beneficiaries. JAMA. 2012;308(5):493–501. doi:10.1001/jama.2012.9014
9. Desai P, Minassian DC, Reidy A. National cataract surgery survey 1997–8: a report of the results of the clinical outcomes. Br J Ophthalmol. 1999;83(12):1336–1340. doi:10.1136/bjo.83.12.1336
10. Lockey SD, Nelson PC, Kessler MJ, Kessler MW. Approaching “Elective” surgery in the era of COVID-19. J Hand Surg. 2021;46(1):60–64. doi:10.1016/j.jhsa.2020.09.006
11. Theodoraki K, Naderi K, Lam CFJ, et al. Impact of cessation of regular cataract surgery during the COVID pandemic on the rates of posterior capsular rupture and post-operative cystoid macular oedema. Eye. 2022:1–6. doi:10.1038/s41433-022-01958-y
12. Tognetto D, Brézin AP, Cummings AB, et al. Rethinking elective cataract surgery diagnostics, assessments, and tools after the COVID-19 pandemic experience and beyond: insights from the EUROCOVCAT Group. Diagn Basel Switz. 2020;10(12):E1035. doi:10.3390/diagnostics10121035
13. Flatharta TÓ, Mulkerrin EC. Back to basics: giant challenges to addressing isaac’s “Geriatric Giants” post COVID-19 crisis. J Nutr Health Aging. 2020;24(7):705–707. doi:10.1007/s12603-020-1425-1
14. Carr F, Agarwal P, Narula H, et al. Restarting cataract surgery during the COVID-19 pandemic; a prospective study analysing 30 day outcomes after elective cataract surgery in the United Kingdom. BMC Ophthalmol. 2021;21(1):167. doi:10.1186/s12886-021-01936-0
15. Mehrotra A, Chernew ME, Linetsky D, Hatch H, Cutler DA. The impact of the COVID-19 pandemic on outpatient visits: a rebound emerges; 2020. doi:10.26099/ds9e-jm36
16. Naderi K, Maubon L, Jameel A, et al. Attitudes to cataract surgery during the COVID-19 pandemic: a patient survey. Eye. 2020;34(12):2161–2162. doi:10.1038/s41433-020-1112-9
17. Sii SSZ, Chean CS, Sandland-Taylor LE, et al. Impact of COVID-19 on cataract surgery- patients’ perceptions while waiting for cataract surgery and their willingness to attend hospital for cataract surgery during the easing of lockdown period. Eye. 2021;35(11):3156–3158. doi:10.1038/s41433-020-01229-8
18. Tzamalis A, Karafotaki K, Karipidi K, et al. The impact of COVID-19 lockdown on cataract surgery: a surgeons’ perspective. Clin Exp Optom. 2021;104(6):705–710. doi:10.1080/08164622.2021.1880866
19. Dotson P. CPT® codes: what are they, why are they necessary, and how are they developed? Adv Wound Care. 2013;2(10):583–587. doi:10.1089/wound.2013.0483
20. Lin PF, Naveed H, Eleftheriadou M, Purbrick R, Zarei Ghanavati M, Liu C. Cataract service redesign in the post-COVID-19 era. Br J Ophthalmol. 2021;105(6):745–750. doi:10.1136/bjophthalmol-2020-316917
21. Rutar T, Porco TC, Naseri A. Risk factors for intraoperative complications in resident-performed phacoemulsification surgery. Ophthalmology. 2009;116(3):431–436. doi:10.1016/j.ophtha.2008.10.028
22. Narendran N, Jaycock P, Johnston RL, et al. The Cataract National Dataset electronic multicentre audit of 55,567 operations: risk stratification for posterior capsule rupture and vitreous loss. Eye Lond Engl. 2009;23(1):31–37. doi:10.1038/sj.eye.6703049
23. Low SAW, Braga-Mele R, Yan DB, El-Defrawy S. Intraoperative complication rates in cataract surgery performed by ophthalmology resident trainees compared to staff surgeons in a Canadian academic center. J Cataract Refract Surg. 2018;44(11):1344–1349. doi:10.1016/j.jcrs.2018.07.028
24. Tzamalis A, Lamprogiannis L, Chalvatzis N, Symeonidis C, Dimitrakos S, Tsinopoulos I. Training of resident ophthalmologists in cataract surgery: a comparative study of two approaches. J Ophthalmol. 2015;2015:932043. doi:10.1155/2015/932043
25. Ellis EM, Lee JE, Saunders L, Haw WW, Granet DB, Heichel CW. Complication rates of resident-performed cataract surgery: impact of early introduction of cataract surgery training. J Cataract Refract Surg. 2018;44(9):1109–1115. doi:10.1016/j.jcrs.2018.06.022
26. Bhagat N, Nissirios N, Potdevin L, et al. Complications in resident-performed phacoemulsification cataract surgery at New Jersey Medical School. Br J Ophthalmol. 2007;91(10):1315–1317. doi:10.1136/bjo.2006.111971
27. Pingree MF, Crandall AS, Olson RJ. Cataract surgery complications in 1 year at an academic institution. J Cataract Refract Surg. 1999;25(5):705–708. doi:10.1016/S0886-3350(99)00017-6
28. Unal M, Yücel I, Sarici A, et al. Phacoemulsification with topical anesthesia: resident experience. J Cataract Refract Surg. 2006;32(8):1361–1365. doi:10.1016/j.jcrs.2006.02.063
29. Rogers GM, Oetting TA, Lee AG, et al. Impact of a structured surgical curriculum on ophthalmic resident cataract surgery complication rates. J Cataract Refract Surg. 2009;35(11):1956–1960. doi:10.1016/j.jcrs.2009.05.046
30. Haripriya A, Chang DF, Reena M, Shekhar M. Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital. J Cataract Refract Surg. 2012;38(8):1360–1369. doi:10.1016/j.jcrs.2012.04.025
31. Puri S, Kiely AE, Wang J, Woodfield AS, Ramanathan S, Sikder S. Comparing resident cataract surgery outcomes under novice versus experienced attending supervision. Clin Ophthalmol Auckl NZ. 2015;9:1675–1681. doi:10.2147/OPTH.S85769
32. Maubon L, Nderitu P, O’Brart DPS. Returning to cataract surgery after a hiatus: a UK survey report. Eye Lond Engl. 2021. doi:10.1038/s41433-021-01717-5
33. Staropoli PC, Gregori NZ, Junk AK, et al. Surgical simulation training reduces intraoperative cataract surgery complications among residents. Simul Healthc. 2018;13(1):11–15. doi:10.1097/SIH.0000000000000255
34. Pokroy R, Du E, Alzaga A, et al. Impact of simulator training on resident cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2013;251(3):777–781. doi:10.1007/s00417-012-2160-z
35. Chen X, Zafar S, Sikder S, et al. National survey and outcomes of resident-performed cataract surgery in monocular patients in the United States. J Cataract Refract Surg. 2019;45(7):939–945. doi:10.1016/j.jcrs.2019.02.018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.