Back to Journals » Journal of Asthma and Allergy » Volume 15
Intracutaneous Skin Tests and Serum IgE Levels Cannot Predict the Grade of Anaphylaxis in Patients with Insect Venom Allergies
Authors Hollstein MM ![]() , Matzke SS, Lorbeer L, Forkel S, Fuchs T
, Matzke SS, Lorbeer L, Forkel S, Fuchs T ![]() , Lex C, Buhl T
, Lex C, Buhl T ![]()
Received 21 March 2022
Accepted for publication 23 June 2022
Published 7 July 2022 Volume 2022:15 Pages 907—918
DOI https://doi.org/10.2147/JAA.S367272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Luis Garcia-Marcos
Moritz M Hollstein,1 Silke S Matzke,1 Lisa Lorbeer,1 Susann Forkel,1 Thomas Fuchs,1 Christiane Lex,2 Timo Buhl1
1Department of Dermatology, Venereology and Allergology, University Medical Centre Göttingen, Göttingen, Germany; 2Department of Pediatric Cardiology, Intensive Care Medicine and Neonatology with Pediatric Pneumology, University Medical Centre Göttingen, Göttingen, Germany
Correspondence: Moritz M Hollstein, Department of Dermatology, Venereology and Allergology, University Medical Centre Göttingen, Robert Koch Str. 40, Göttingen, 37075, Germany, Email [email protected]
Background: Allergies against Hymenoptera venoms are a major cause of severe anaphylaxis. Risk assessment for subjects with suspected allergy is difficult because there are currently no biomarkers that predict the likelihood of high-grade anaphylaxis other than several associated comorbidities.
Objective: We investigated the relationship between the severity of anaphylaxis and the results of intracutaneous skin tests (ICTs) together with serum levels of tryptase, total IgE, and venom-specific IgE, IgG, and IgG4.
Methods: We performed a retrospective evaluation of 194 patients who presented to a single medical center with allergies to bee venoms (Apis mellifera, Bombus spp.; n=24, 12.4%), vespid venoms (Vespula spp., Vespa spp., Polistes spp.; n=169, 87.1%), or both (n=1, 0.5%).
Results: Index bee stings occurred earlier in the year than vespid stings, although the latter were reported more frequently overall. On average, subjects who previously experienced grade IV anaphylaxis required higher dosages of venom to yield positive ICTs than those who exhibited lower grade responses. Patients diagnosed with grade IV anaphylaxis exhibited significantly lower levels of venom-specific IgE and IgG and trended toward elevated levels of tryptase. No significant differences in average levels of venom-specific IgG4 and total IgE were observed.
Conclusion: Our findings reveal that intracutaneous skin testing and levels of venom-specific IgE do not predict the degree of anaphylaxis that develops in patients with venom allergy. Furthermore, the month of the index sting is not a reliable means to differentiate bee from vespid stings in patients presenting with an uncertain history.
Keywords: intracutaneous test, allergy, insect venom allergy, specific IgE
Introduction
Anaphylaxis is a life-threatening condition with an incidence of 1.5 to 7.9 per 100,000 person-years.1 This condition is currently defined as “a severe, potentially fatal, systemic allergic reaction that occurs suddenly after contact with an allergy-causing substance”.2 The causes of anaphylaxis vary with age and exposure to specific allergens. In adults, they are most frequently caused by Hymenoptera venoms followed by drugs and food.3–5
Previous contact with an allergen is a clear prerequisite to an allergic reaction and can result in sensitization. Whilst 56.6% to 94.5% of Europeans have experienced at least one Hymenoptera sting during their lifetimes, sensitization to their venoms occurs in only 9.3% to 28.7% of adults.6,7 Systemic reactions are observed in fewer than 10% of cases, even in populations known to be at elevated risk. In Germany, approximately 3% of the population develops systemic symptoms after a sting.5,8 Likewise, and despite the pathophysiological importance of sensitization to allergic reactions, only 5–17% of previously asymptomatic individuals identified as sensitized by skin-testing or detection of specific IgE go on to develop systemic symptoms in response to a subsequent sting.9,10 Hence, whilst specific IgE antibodies are frequently detected amongst members of the general population and known to mediate allergen-induced mast-cell degranulation via the high affinity IgE receptor11 and downstream via Lyn/Syk,12 they are of only minor diagnostic relevance in the absence of a conclusive patient history.13
An initial evaluation of suspected Hymenoptera venom allergy should include a detailed patient history in addition to clinical tests to document suspected sensitization and estimate the risk of a systemic reaction. The clinical evaluation includes skin tests as well as a determination of levels of total and venom-specific IgEs. The current German guidelines state that patients with systemic sting reactions (SSRs) and proven sensitization to insect venom should be treated with specific immune therapy (SIT).14
The absence of reliable laboratory markers makes it difficult to evaluate patients with inconclusive histories of Hymenoptera stings. These difficulties arise either because the aforementioned clinical tests indicate sensitivity to multiple allergens or because the severity of the response to the index sting reaction cannot be determined in hindsight. In these cases, additional factors are evaluated to help determine the risk of developing potentially fatal anaphylaxis. These factors include the time interval between insect stings, the number of stings, and the type of insect, as well as patient age, sex, the severity of the preceding reaction, concomitant cardiovascular disease and treatments, mastocytosis, and elevated levels of serum tryptase.7 However, most of these factors are either controversial or of only minor importance when used to predict the severity of future anaphylactic reactions.
Symptoms of allergic reactions can be assigned to one of four grades of severity according to overlapping criteria published initially by Mueller15 and Ring and Messmer.16 Grade I includes symptoms limited to the skin, including urticaria, pruritus, or flush. Single or combinations of vital organs are affected at the higher grades of severity. In grade IV anaphylaxis, the reaction to the allergen impedes circulation, oxygenation, and/or consciousness and poses a threat to life.15,16 The most important difference between both anaphylaxis scales is the classification of cardiovascular symptoms. Whilst Mueller15 classifies hypotension (but not tachycardia) as a sign of Grade IV anaphylaxis, Ring and Messmer16 discuss varying degrees of cardiovascular involvement; for example, hypotension (blood pressure < 90 mmHg) is a sign of Grade II anaphylaxis.
We are in great need of reliable predictors to facilitate the clear and accurate diagnosis of insect venom allergies. Our study complements several previous attempts from the early 1990s to identify reliable predictors of SSR severity for both bee and vespid venoms, which are the two most abundant insect allergens.5 However, some changes have occurred since the 1990s, ie changes in venom test extract composition and -quality. Moreover, most preceding studies focused on evaluating skin-prick-tests instead of intracutaneous skin tests (ICTs). Here, we investigated whether the results of ICTs and specific lab tests might help to determine the risks of developing high-grade anaphylaxis.
Materials and Methods
Patients
We screened the files of all patients who initially visited the Allergology Division at the Department of Dermatology, Venereology, and Allergology, University Medical Centre Göttingen, Germany, between July 1990 and July 2011. We identified patients who received SIT following a documented anaphylactic reaction to bee (Apis mellifera; Bombus spp.) or vespid venoms (Vespula spp.; Vespa spp.; Polistes spp.). We excluded patients with missing history. We did not consider any patients evaluated after 2011 because of changes in diagnostic procedures for skin tests and because some clinical tests were discontinued from 2012 onwards. Insect venom allergies were diagnosed by patient history, serological testing, and skin testing in accordance with the German national guidelines.14 Findings from the one patient who received SIT against both bee and vespid venom were included in both patient cohorts. This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki and reviewed and approved by the local ethics committee, approval number [1/11/21]. All included patients gave written informed consent before study inclusion, indicating that their patient data may be used for academic research. Additional written obtained consent to be included in this particular analysis was not deemed necessary by the local ethics committee. Confidentiality of patient related data was maintained at all times.
Personal History
We classified patients according to venom type (bee or vespid venom; insect species listed above), age, sex, comorbidities, other allergies or intolerances, family history, profession, and dates of first and last known Hymenoptera sting. For historical reasons, the severity of anaphylactic reactions was categorized according to Mueller.15 As initially described by Stoevesand et al17 we focused on the following comorbidities that are relevant to anaphylactic reactions: atopy, active malignancy, and mastocytosis, as well as rheumatic, cardiovascular, respiratory, and/or psychiatric diseases.17 We documented specific drug intake based on the guideline “Skin Tests for Diagnostics of Allergic Immediate-Type Reactions”18 complemented with the inclusion of anti-hypertensive medication (beta-blockers and angiotensin-converting enzyme (ACE)-inhibitors, amongst others). We routinely used a questionnaire in combination with laboratory tests to identify the venom type responsible for the allergic reaction in patients who were unable to identify the specific venom type that triggered the anaphylactic response. Subsequently, we matched personal data with respective ICTs and laboratory test results.
Intracutaneous Skin Tests (ICTs)
ICTs were performed for the relevant venoms with histamine dihydrochloride (1.0%) and sodium chloride (NaCl, 0.9%) as positive and negative controls, respectively. We routinely used the allergen preparation Reless® (ALK-Abelló, Hamburg, Germany) to perform ICTs and in rare cases Venomil® (Bencard, Munich, Germany). The ICT protocol began with low doses that were increased until a visible skin reaction (urticaria) ≥5 mm diameter after 15 min was observed. The dose of bee venom increased from 0.001 to 1 µg/mL, whilst the dose of vespid venom was titrated upwards from 0.0001 to 1 µg/mL.
Serological Testing
We analyzed serum samples for venom-specific IgG, IgG4, and IgE, as well as total IgE, tryptase, and IgE against an allergen mixture containing eight common inhalant allergens (Sx1; house dust mite (Dermatophagoides pteronyssinus), cat, dog, birch, timothy (Phleum pratense), rye, ragweed, and Cladosporium herbarum) using the ImmunoCAP® system (Thermo Fisher, Waltham, MA, USA) and following the manufacturer’s instructions. For subjects without documented levels of total IgE, tryptase, or Sx1 before undergoing SIT, we used the first documented values available upon a subsequent visit to our department. At the beginning of the recruitment period, allergen-specific IgE, total IgE, and Sx1-values were reported to be between 0.35 and 100.00 kU/l. The diagnostic range of allergen-specific IgG4 was 2.00 to 30.00 µg/mL. The diagnostic limits for allergen-specific total IgG were 2.00 to 200.00 µg/mL. The diagnostic accuracy of the ImmunoCAP® system improved during the course of the study period and values above and below these limits could ultimately be documented. The new lower and upper limits of IgG4 were 0.15 and 300 µg/mL, respectively; the other parameters were subsequently presented without limits. Values obtained later that were outside the initial limits were set to the corresponding minimum or maximum value of the initial limits. As in most retrospective studies, not all of the aforementioned laboratory results were available for all patients. We supplied the total number of analyzed values in the table provided (Table 1) and the legends of each figure.
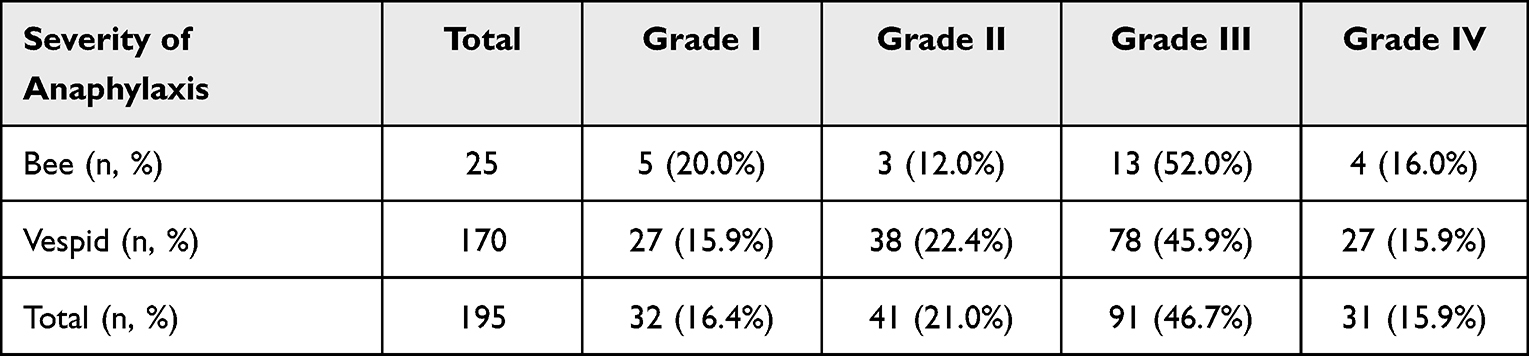 |
Table 1 Severity of Anaphylaxis |
Statistical Analysis
Data were analyzed with Excel (Version 16.44, Microsoft, Redmond, WA, USA), R (Version 1.2.5033, RStudio, USA), and GraphPad PRISM (Version 9, GraphPad Software, San Diego, CA, USA). Differences in proportions between distinct subgroups of patients were tested for significance using Wilcoxon rank-sum test.
Results
History and Demographic Data
We identified 194 individuals who were undergoing SIT because of a documented anaphylactic reaction against bee (n=24, 12.4%) or vespid venoms (n=169, 87.1%). We identified one individual who had undergone SIT against both venoms who was included in both bee and vespid venom groups (n=1, 0.5%). Thus, we evaluated 195 cases of venom allergy in 194 patients. The study population included 96 males (49.5%) and 98 females (50.5%). On average, the patients undergoing SIT against bee venom were younger (mean, 31.5 years) than those treated with SIT against vespid venom (mean, 46.0 years; Table S1). We assessed the number and nature of concomitant diseases and identified atopic diseases as frequent comorbidities in both groups (Table S2). Arterial hypertension was identified in 21.2% of the patients undergoing vespid SIT; 22.9% of the subjects in this group were on antihypertensive medication (Table S3).
Index Sting and Severity of Anaphylaxis
We registered the month of the index sting (ie, the sting that triggered the anaphylactic reaction in each patient). Our findings revealed that bee stings were most prevalent earlier in the calendar year. By contrast, index stings amongst the vespid group peaked in August (Figure 1). The severity of anaphylaxis (ie, the clinical indicator used to select patients for SIT), was comparable amongst both groups (Table 1). Most patients who underwent SIT experienced Grade III anaphylaxis (52.0% of those in the bee sting group and 45.9% for those in the vespid sting group). The proportion of male subjects was higher amongst those exhibiting Grade I and Grade IV anaphylaxis compared to those with Grades II and III in both venom SIT groups (Figure S1).
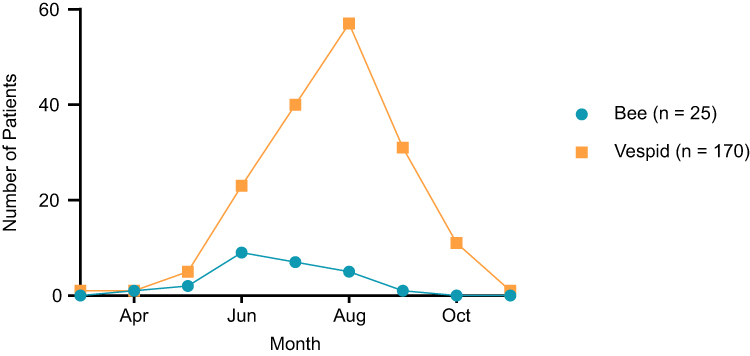 |
Figure 1 The month of the index sting. The number of enrolled patients who were stung by a vespid (orange, n=170) or bee (blue, n=25). The respective months are indicated on the x-axis. No bee or vespid stings that resulted in anaphylaxis were reported from December to February. |
Outcomes of the Intracutaneous Skin Tests (ICTs)
We compared the severity of anaphylaxis to the minimum dosage of venom needed to trigger a positive skin reaction (Figure 2). The results revealed a trend toward decreased responsiveness (ie, in which higher venom concentrations were needed to achieve positive ICTs) with increasing grade of anaphylaxis amongst patients in the vespid venom group, although this finding did not achieve statistical significance. These differences were not detected amongst patients in the bee venom group. However, this may be because only 25 (12.9%) of the patients enrolled in our study were undergoing SIT for anaphylaxis related to bee stings (Table 1).
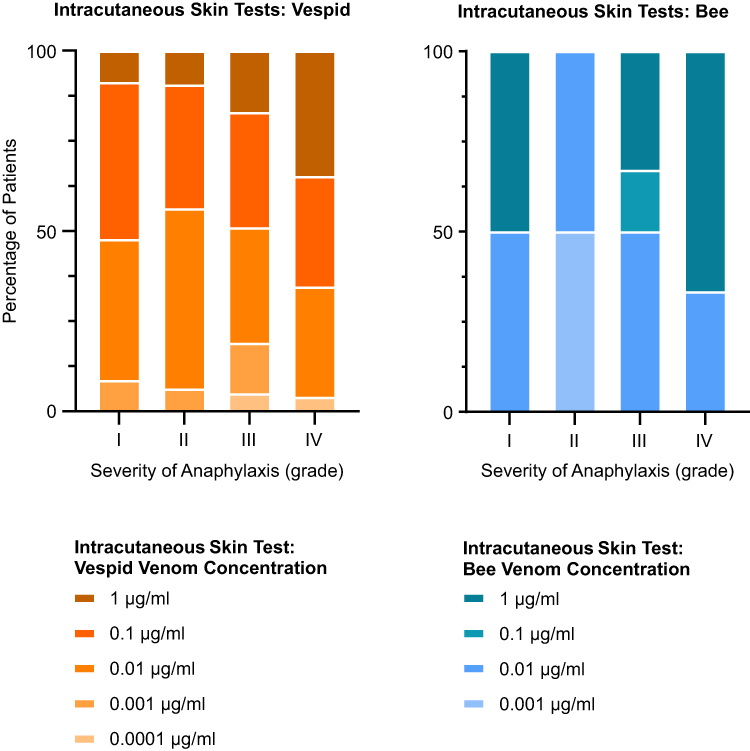 |
Figure 2 The severity of anaphylaxis and results of intracutaneous skin tests (ICTs). Values on the x-axis are severities of anaphylaxis graded I–IV according to Mueller.15 ICTs were performed with increasing concentrations of vespid (left, orange, n=141) or bee (right, blue, n=13) venom until a positive reaction was seen. The colors within each of the bars indicate the venom concentration at which the ICT became positive in each group. Reless® (ALK-Abelló, Hamburg, Germany) and in rare cases Venomil® (Bencard, Munich, Germany) were used as allergen preparations. |
Results of Laboratory Tests
As shown in previous studies, subjects undergoing SIT following Grade IV anaphylaxis exhibited higher serum tryptase levels than those who experienced Grades I–III, although this finding did not reach statistical significance (Figure 3A). Only three values for serum tryptase were available for the group of patients undergoing SIT for Grade IV anaphylaxis secondary to bee stings. Interestingly, we found the opposite to be true in our evaluation of specific IgE against a mixture of eight common aeroallergens (ie, Sx1; Figure 3B). Fifty-six percent of the patients with allergy to bee venom and 53.9% of those allergic to vespid venom were positive for Sx1 (>0.35 kU/l). Levels of Sx1-specific IgE decreased with severity of anaphylaxis; the difference between levels detected amongst those who experienced Grade I versus Grade IV anaphylaxis was statistically significant (p=0.0311). Hence, subjects with evidence of a higher level of aeroallergen sensitization generally had less severe symptoms of anaphylaxis in response to these insect venoms. The severity of anaphylaxis was also related to venom-specific IgE levels detected before the initiation of the respective SITs (Figure 4A). Amongst our findings, the results revealed significantly lower levels of venom-specific IgE in the groups undergoing vespid SIT who experienced Grade IV anaphylaxis (Grades I–III versus Grade IV, p=0.0278). Similar trends were observed in measurements of total IgE, although the differences were small and did not achieve statistical significance (Figure 4B). As noted above, the small number of patients (and only n=4 who experienced Grade IV anaphylaxis) prevents us from drawing any specific conclusions on trends involving total or venom-specific IgE in the bee venom group. Our findings revealed no differences in the levels of venom-specific IgG4 between the groups exhibiting different degrees of SSR severity (Figure 5A). We observed that one subject in the vespid venom group exhibited a serum IgG4 concentration of >300 µg/mL (a mathematical outlier by Grubb’s test). Without this value, our data suggest that Grade IV anaphylaxis might be associated with lower levels of IgG4. Nonetheless, Grade IV anaphylaxis was directly associated with significantly lower levels of total vespid-venom-specific IgG (Grade I versus Grade IV, p=0.0279) (Figure 5B). Taken together, our data indicate an association between Grade IV anaphylaxis and male sex, lower venom-specific antibody titers, and reduced ICT reactivity compared to Grade I anaphylaxis.
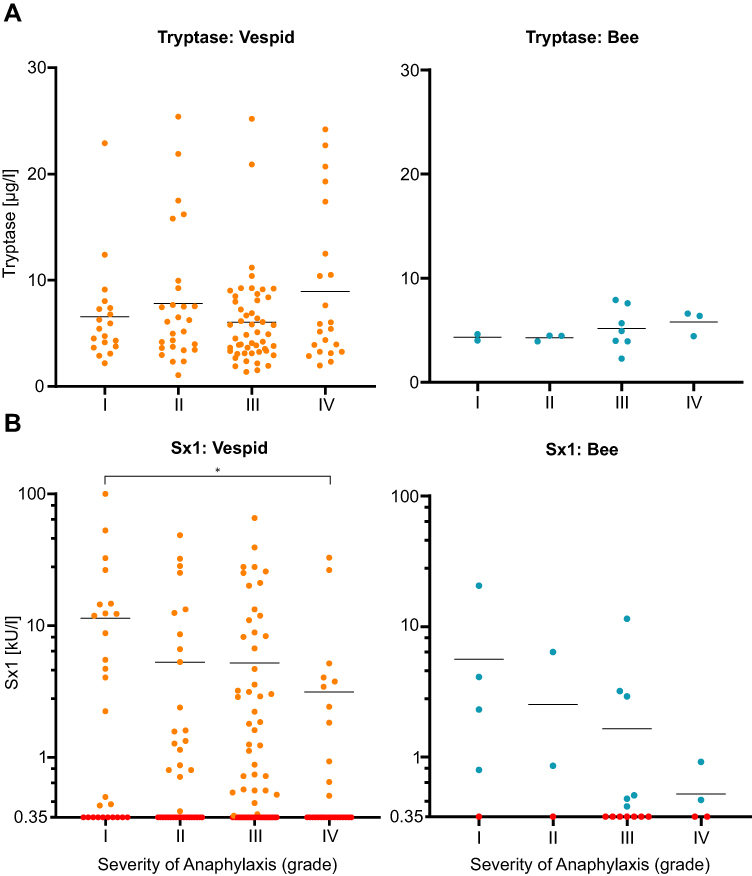 |
Figure 3 The severity of anaphylaxis, serum tryptase, and Sx1 levels. Values on the x-axis are severities of anaphylaxis Grades I–IV according to Mueller.15 The horizontal lines indicate the arithmetic means. (A) Serum tryptase levels (µg/l) in individual patients with vespid (left, orange, n=117) or bee (right, blue, n=15) venom allergies. (B) Sx1 IgE (kU/l) levels in patients with vespid (left, orange, n=165) or bee (right, blue, n=25) venom allergies. The allergen mixture Sx1 was measured using the ImmunoCAP® system (Thermo Fisher, Waltham, MA, USA). Values below the diagnostic cut off according to the manufacturer’s instructions (0.35 kU/l for Sx1) were marked in red color. *Significant at α = 0.05. |
 |
Figure 4 The severity of anaphylaxis and serum IgE levels. Values on the x-axis are severities of anaphylaxis Grades I–IV according to Mueller.15 The horizontal lines indicate the arithmetic means. (A) Serum levels of venom-specific IgE (kU/l) in individual patients with vespid (left, orange, n=166) or bee (right, blue, n=25) venom allergies. (B) Serum levels of total IgE (kU/l) in individual patients with vespid (left, orange, n=168) or bee (right, blue, n=25) venom allergies. Values below the diagnostic cut off according to the manufacturer’s instructions (0.35 kU/l for both specific and total IgE) were marked in red color. *Significant at α = 0.05. |
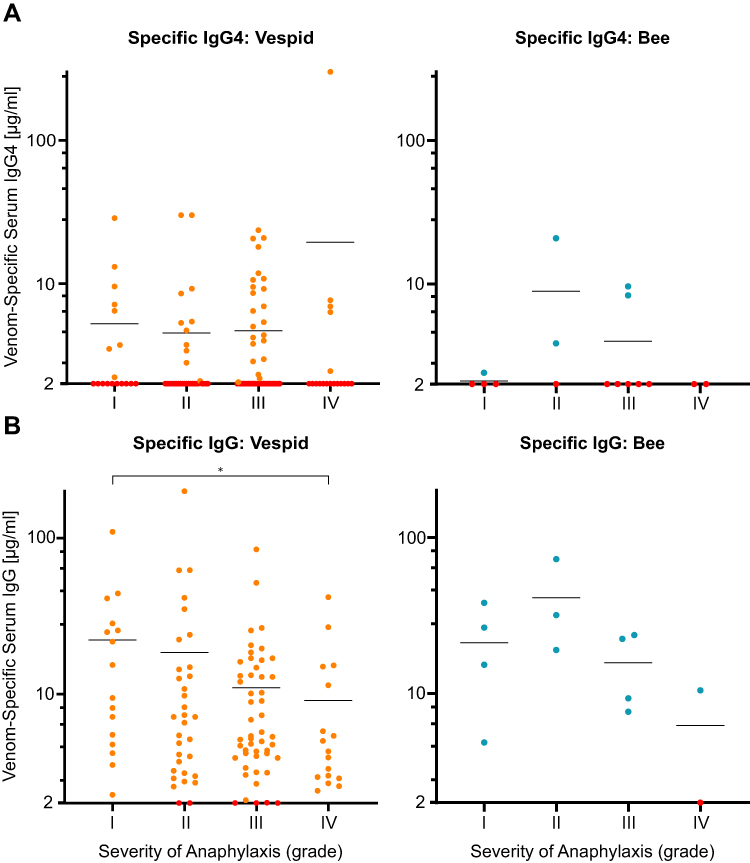 |
Figure 5 The severity of anaphylaxis and venom-specific serum IgG levels. Values on the x-axis are severities of anaphylaxis Grades I–IV according to Mueller.15 The horizontal lines indicate the arithmetic means. (A) Serum levels of venom-specific IgG4 (µg/mL) in individual patients with vespid (left, orange, n=125) or bee (right, blue, n=16) venom allergies. (B) Serum levels of antigen-specific IgG (µg/mL) in individual patients with vespid (left, orange, n=116) or bee (right, blue, n=13) venom allergies. Values below the diagnostic cut off according to the manufacturer’s instructions (2 μg/mL for both IgG and IgG4) were marked in red color. *Significant at α = 0.05. |
Discussion
In this study, we examined retrospective demographic and clinical data from 194 patients with Hymenoptera venom allergies who underwent SIT as part of an effort to identify factors that might predict the likelihood of severe anaphylaxis. Amongst the results, we found that subjects who developed Grade IV anaphylaxis exhibited reduced ICT responses. Since current German guidelines include negative skin test results as one criterion for cessation of a successful SIT,14 one might expect some correlation between the degree of skin reactivity and systemic symptoms. Of note, current European guidelines do not follow this strategy, and instead, highlight the lack of diagnostic significance of differences in ICTs of tolerant patients compared to those with relapses.19 Negative ICTs are of diagnostic value because ICTs are highly sensitive for detecting Hymenoptera allergies.20 However, our findings suggest that the magnitude of a given ICT reaction is overall unrelated to the severity of an SSR (ie, anaphylaxis). This finding is supported by an earlier study that also documented no relationship between skin tests and the severity of recurrent anaphylactic reactions that result from sting challenges.21 This earlier study’s methodology to perform skin tests was based on an earlier publication from 1987.22 However, commercially available venoms have changed in the meantime in composition and -quality, remarkably hampering transferability. Results from several earlier studies focused on systemic symptoms as adverse events during SIT also documented no significant association with the results of ICTs.23,24 To the best of our knowledge, there is only one published smaller study (n=36 patients) that compared ICT reactivity with the severity of the initial SSR. Similar to our current findings, which included a larger patient cohort (n = 194), the results from this earlier study demonstrated no association between the results of ICTs and SSR severity.25
Consistent with previous reports,26,27 a large proportion of patients enrolled in our study had elevated levels of total IgE (ie, over the upper limit of normal at 100 kU/l). Both of these previous studies also showed a tendency for total IgE to decrease with the increasing severity of anaphylaxis. These findings were replicated by our data, although they did not reach statistical significance. Furthermore, our results revealed that higher levels of serum IgE against common aeroallergens (Sx1) were significantly associated with lower severity of anaphylaxis, which also confirmed results reported in previous studies.26,27 These parameters are interpreted similarly as both point toward an atopic predisposition.27–30 Although atopy is generally understood as a risk factor for atopic dermatitis,30,31 evidence suggests that this predisposition may not have any impact on the severity of anaphylactic sting reactions,26,27,32 except amongst beekeepers and their families.33
Results from our study revealed a trend toward higher serum tryptase levels in patients with documented Grade IV anaphylaxis although these findings did not reach statistical significance. Elevated tryptase values are also characteristic of patients diagnosed with mastocytosis, which might also explain its association with severe SSRs.34 Interestingly, numerous earlier studies have described associations between elevated serum tryptase levels with more severe anaphylactic reactions.34–39 Similarly, venom-specific IgE was reported to correlate with levels of total IgE.27 However, studies on the interdependence of venom-specific IgE and the severity of SSRs are scarce. Several studies published before 2000 made efforts to correlate venom-specific IgE levels with the severity of anaphylaxis with contradictory results. Day et al40 reported the existence of a correlation between the severity of anaphylaxis and levels of venom-specific IgE. By contrast, both Wilson et al41 and Reisman and DeMasi42 reported that there were no correlations between individual levels of venom-specific IgE and the incidence of systemic reactions. Another more recent study also reported that levels of bee venom-specific IgE and the rate of serious adverse events during SIT were unrelated to one another.43 In this study, we identified no elevations in venom-specific IgE in patients with Grade IV anaphylaxis. However, we recognize that low specific IgE levels and elevated skin test thresholds may be influenced by numerous factors and may be age-related. Our findings indicate that these results have no negative prospective predictive value with respect to the degree of anaphylaxis that develops in response to insect stings. The notion that IgE levels alone do not explain an individual’s susceptibility to anaphylaxis is further strengthened by the observation that some patients experience near fatal anaphylaxis despite having low or undetectable levels of circulating allergen-specific IgE.44 Conversely, food-allergen-specific IgE can be detected in the plasma of many subjects who do not develop clinical symptoms when exposed to that food-allergen.45 This may also be true for hymenoptera venom, where the vast majority (∼80%) of people with IgE antibodies specific for hymenoptera venoms have no history of systemic reactions to such venoms.27,32 The reason for this may be that the multiple tyrosine kinases, activated after immunoglobulin E binding to the high-affinity receptors for immunoglobulin E (FcεRI), exert both positive and negative regulation on the signaling cascade, which may vary with genetic background or mutations in signaling proteins.
Aside from measuring venom-specific IgE and performing skin tests, molecular diagnosis also permits identification of bee and/or wasp as culprit insect in venom-sensitized subjects. Our study did not include molecular diagnosis. However, current research on this subject has shown that the severity of sting reactions is rather not associated with parameters obtained by molecular diagnosis.46
Molecular analyses of bee and vespid venoms show distinct differences in venom composition between different hymenoptera species with varying allergenic potential.47–49 In our retrospective analysis we analyzed parameters generated by routine-diagnostics and hence correlated SSR severity with composite allergen preparations. A missing correlation of SSR severity with skin tests using composite allergen preparations does not exclude correlations with skin tests using individual venom components. The next step in researching SSR severity may thus be to analyze hymenoptera venom components separately and correlate their induced skin reactions with systemic sting reactions.
Finally, our findings are consistent with previous studies that indicate that bee stings generally occur earlier in the year than vespid stings, at least in central Europe. This result was expected because vespids are typically more abundant than bees during later months of the year.50 However, we identified many more patients who developed anaphylaxis in response to vespid stings (n=170) than in response to bee stings (n=25). This finding is consistent with the previous literature which reports that vespid stings caused many more incidents of anaphylaxis than bee stings.51,52 In our patient cohort, which included individuals with a history of venom-induced anaphylaxis, we found that the absolute frequency of vespid stings was higher than the absolute frequency of bee stings as early as May. This result implies that the current focus on the month of the index sting14 may be of little value in distinguishing between these two insect stings. Bee stings can occur even in late summer (nb: we registered bee stings as late as September). Our results and those of others reveal that anaphylaxis is more likely to be caused by vespids at all times during the year.
Amongst the limitations of this study are its retrospective nature and the changes made to the ImmunoCap® test system over the years. Likewise, to enroll a sufficient number of patients, we needed to include records of anaphylactic patients treated with venom SIT over the course of numerous years. An approach that included only those patients who were evaluated with similar test methods would have resulted in an unjustifiable reduction in statistical power. Furthermore, one can be debate whether rankings of anaphylaxis symptoms should be performed according to criteria developed by Mueller15 or by Ring and Messmer.16 Our allergy department traditionally used the former ranking system for the patients evaluated in this retrospective dataset. Finally, venom-allergic patients that declined SIT were excluded from this analysis because we were unable to trace them through our archived patient files.
Conclusions
In summary, our findings based on a comparatively large cohort of venom-allergic individuals reveal that it is virtually impossible to draw conclusions regarding the grade of anaphylaxis that will develop based on currently available skin and laboratory results. Likewise, patient histories and emergency treatments for anaphylaxis can be difficult to categorize within the current grading system. Given the absence of other objective parameters, the severity of anaphylaxis experienced by a given patient often serves as a guide to the duration of venom SIT. Thus, novel and more effective procedures and parameters for the determination of the duration of a venom SIT are urgently needed.
Study Approval Statement
This study was reviewed and approved by the University Medical Center Göttingen (UMG) ethics committee, approval number [1/11/21].
Data Sharing Statement
Datasets are available on request.
Statement of Ethics
The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate Statement
This is a retrospective study based on the review of patient charts. All included patients gave written informed consent before study inclusion, indicating that their patient data may be used for academic research. Additional written obtained consent to be included in this particular analysis was not deemed necessary by the local ethics committee.
Acknowledgments
We acknowledge support by the Open Access Publication Funds of the Göttingen University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Moritz M Hollstein and Silke S Matzke shared first authorship.
Funding
There is no funding to report.
Disclosure
Prof. Dr. Christiane Lex reports lecture fees paid to institution from Sanofi, during the conduct of the study; lecture fees paid to institution from Sanofi and Novartis, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Panesar SS, Javad S, de Silva D, et al. The epidemiology of anaphylaxis in Europe: a systematic review. Allergy. 2013;68(11):1353–1361. doi:10.1111/all.12272
2. Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117(2):391–397. doi:10.1016/j.jaci.2005.12.1303
3. Tejedor Alonso MA, Moro Moro M, Múgica García MV. Epidemiology of anaphylaxis. Clin Exp Allergy. 2015;45(6):1027–1039. doi:10.1111/cea.12418
4. Grabenhenrich LB, Dölle S, Moneret-Vautrin A, et al. Anaphylaxis in children and adolescents: the European Anaphylaxis Registry. J Allergy Clin Immunol. 2016;137(4):1128–1137.e1. doi:10.1016/j.jaci.2015.11.015
5. Schäfer T. Epidemiologie der Insektengiftallergie. Allergo J. 2009;18(5):353–358. doi:10.1007/BF03362108
6. Antonicelli L, Bilò MB, Bonifazi F. Epidemiology of Hymenoptera allergy. Curr Opin Allergy Clin Immunol. 2002;2(4):341–346. doi:10.1097/00130832-200208000-00008
7. Bilò MB, Bonifazi F. The natural history and epidemiology of insect venom allergy: clinical implications. Clin Exp Allergy. 2009;39(10):1467–1476. doi:10.1111/j.1365-2222.2009.03324.x
8. Langen U, Schmitz R, Steppuhn H. Häufigkeit allergischer Erkrankungen in Deutschland: ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1)[Prevalence of allergic diseases in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. 2013;56(5–6):698–706. German. doi:10.1007/s00103-012-1652-7
9. Golden DB, Marsh DG, Freidhoff LR, et al. Natural history of Hymenoptera venom sensitivity in adults. J Allergy Clin Immunol. 1997;100(6):760–766. doi:10.1016/S0091-6749(97)70270-7
10. Sturm GJ, Kranzelbinder B, Schuster C, et al. Sensitization to Hymenoptera venoms is common, but systemic sting reactions are rare. J Allergy Clin Immunol. 2014;133(6):1635–1643.e1. doi:10.1016/j.jaci.2013.10.046
11. Hazebrouck S, Canon N, Dreskin SC. The effector function of allergens. Front Allergy. 2022;3:818732. doi:10.3389/falgy.2022.818732
12. Siraganian RP, de Castro RO, Barbu EA, Zhang J. Mast cell signaling: the role of protein tyrosine kinase Syk, its activation and screening methods for new pathway participants. FEBS Lett. 2010;584(24):4933–4940. doi:10.1016/j.febslet.2010.08.006
13. Sturm GJ, Schuster C, Kranzelbinder B, Wiednig M, Groselj-Strele A, Aberer W. Asymptomatic sensitization to hymenoptera venom is related to total immunoglobulin E levels. Int Arch Allergy Immunol. 2009;148(3):261–264. doi:10.1159/000161586
14. Przybilla B, Ruëff F, Walker A, et al. Diagnose und Therapie der Bienen und Wespengiftallergie [Skin tests for diagnostics of allergic immediate-type reactions. Guideline of the German Society for Allergology and Clinical Immunology]. Allergo J. 2011;20(6):318–339. German. doi:10.1007/BF03362543
15. Mueller HL. Diagnosis and treatment of insect sensitivity. J Asthma Res. 1966;3(4):331–333. doi:10.3109/02770906609106941
16. Ring J, Messmer K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet. 1977;309(8009):466–469. doi:10.1016/S0140-6736(77)91953-5
17. Stoevesandt J, Sturm GJ, Bonadonna P, Oude Elberink JNG, Trautmann A. Risk factors and indicators of severe systemic insect sting reactions. Allergy. 2020;75(3):535–545. doi:10.1111/all.13945
18. Ruëff F, Bergmann KC, Brockow K, et al. Hauttests zur Diagnostik von allergischen Soforttyp-Reaktionen. Pneumologie. 2011;65(08):484–495. doi:10.1055/s-0030-1256476
19. Sturm GJ, Varga EM, Roberts G, et al. EAACI guidelines on allergen immunotherapy: hymenoptera venom allergy. Allergy. 2018;73(4):744–764. doi:10.1111/all.13262
20. Blank S, Grosch J, Ollert M, Bilò MB. Precision medicine in hymenoptera venom allergy: diagnostics, biomarkers, and therapy of different endotypes and phenotypes. Front Immunol. 2020;11:579409. doi:10.3389/fimmu.2020.579409
21. van der Linden PW, Hack CE, Struyvenberg A, van der Zwan JK. Insect-sting challenge in 324 subjects with a previous anaphylactic reaction: current criteria for insect-venom hypersensitivity do not predict the occurrence and the severity of anaphylaxis. J Allergy Clin Immunol. 1994;94(2):151–159. doi:10.1053/ai.1994.v94.a54889
22. Kampelmacher MJ, Zwan JC. Provocation test with a living insect as a diagnostic tool in systemic reactions to bee and wasp venom: a prospective study with emphasis on the clinical aspects. Clin Exp Allergy. 1987;17(4):317–327. doi:10.1111/j.1365-2222.1987.tb02021.x
23. Lockey RF, Turkeltaub PC, Olive ES, Hubbard JM, Baird-Warren IA, Bukantz SC. The Hymenoptera venom study III: safety of venom immunotherapy. J Allergy Clin Immunol. 1990;86(5):6. doi:10.1016/S0091-6749(05)80182-4
24. Korošec P, Žiberna K, Šilar M, et al. Immunological and clinical factors associated with adverse systemic reactions during the build-up phase of honeybee venom immunotherapy. Clin Exp Allergy. 2015;45(10):1579–1589. doi:10.1111/cea.12582
25. Warrington RJ. Lack of correlation between severity of clinical symptoms, skin test reactivity, and radioallergosorbent test results in venom-allergic patients. Allergy Asthma Clin Immunol. 2006;02(02):62.
26. Przybilla B, Ring J, Grieshammer B. Association of features of atopy and diagnostic parameters in hymenoptera venom allergy. Allergy. 1991;46(8):570–576. doi:10.1111/j.1398-9995.1991.tb00625.x
27. Sturm GJ, Heinemann A, Schuster C, et al. Influence of total IgE levels on the severity of sting reactions in Hymenoptera venom allergy. Allergy. 2007;62(8):884–889. doi:10.1111/j.1398-9995.2007.01413.x
28. Diepgen T, Fartasch M, Hornstein O. Criteria of atopic skin diathesis. Dermatosen Beruf Umw. 1991;39(3):79–83.
29. Diepgen TL, Sauerbrei W, Fartasch M. Development and validation of diagnostic scores for atopic dermatitis incorporating criteria of data quality and practical usefulness. J Clin Epidemiol. 1996;49(9):1031–1038. doi:10.1016/0895-4356(96)00119-9
30. Bieber T. Atopic Dermatitis. N Engl J Med. 2008;358(14):1483–1494. doi:10.1056/NEJMra074081
31. Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–360. doi:10.1016/S0140-6736(20)31286-1
32. Bilò BM, Bonifazi F. Epidemiology of insect-venom anaphylaxis. Curr Opin Allergy Clin Immunol. 2008;8(4):330–337. doi:10.1097/ACI.0b013e32830638c5
33. Müller UR. Bee venom allergy in beekeepers and their family members. Curr Opin Allergy Clin Immunol. 2005;5(4):343–347. doi:10.1097/01.all.0000173783.42906.95
34. Theoharides TC, Valent P, Akin C. Mast cells, mastocytosis, and related disorders. N Engl J Med. 2015;373(2):163–172. doi:10.1056/NEJMra1409760
35. Brockow K, Jofer C, Behrendt H, Ring J. Anaphylaxis in patients with mastocytosis: a study on history, clinical features and risk factors in 120 patients: anaphylaxis in patients with mastocytosis. Allergy. 2008;63(2):226–232. doi:10.1111/j.1398-9995.2007.01569.x
36. Bonadonna P, Zanotti R, Müller U. Mastocytosis and insect venom allergy. Curr Opin Allergy Clin Immunol. 2010;10(4):347–353. doi:10.1097/ACI.0b013e32833b280c
37. Bonadonna P, Zanotti R, Pagani M, et al. How much specific is the association between hymenoptera venom allergy and mastocytosis? Allergy. 2009;64(9):1379–1382. doi:10.1111/j.1398-9995.2009.02108.x
38. Kucharewicz I, Bodzenta-Lukaszyk A, Szymanski W, Mroczko B, Szmitkowski M. Basal serum tryptase level correlates with severity of hymenoptera sting and age. J Investig Allergol Clin Immunol. 2007;17:5.
39. Guenova E, Volz T, Eichner M, et al. Basal serum tryptase as risk assessment for severe Hymenoptera sting reactions in elderly: serum tryptase and Hymenoptera sting reactions in elderly. Allergy. 2010;65(7):919–923. doi:10.1111/j.1398-9995.2009.02302.x
40. Day J, Buckeridge D, Welsh A. Risk assessment in determining systemic reactivity to honeybee stings in sting-threatened individuals. J Allergy Clin Immunol. 1994;93(4):691–705. doi:10.1016/0091-6749(94)90249-6
41. Wilson AB, Deighton J, Lachmann PJ, Ewan PW. A comparative study of IgG subclass antibodies in patients allergic to wasp or bee venom. Allergy. 1994;49(4):272–280. doi:10.1111/j.1398-9995.1994.tb02660.x
42. Reisman RE, DeMasi JM. Relationship of serum venom-specific IgE titers to clinical aspects of stinging insect allergy. Int Arch Allergy Immunol. 1989;89(1):67–70. doi:10.1159/000234925
43. Kopač P, Custovic A, Zidarn M, et al. Biomarkers of the severity of honeybee sting reactions and the severity and threshold of systemic adverse events during immunotherapy. J Allergy Clin Immunol Pract. 2021;9(8):3157–3163.e5. doi:10.1016/j.jaip.2021.04.045
44. Simons F, Frew A, Ansotegui I, et al. Risk assessment in anaphylaxis: current and future approaches. J Allergy Clin Immunol. 2007;120(1):S2–S24. doi:10.1016/j.jaci.2007.05.001
45. Sicherer SH, Sampson HA. Food allergy. J Allergy Clin Immunol. 2010;125(2):S116–S125. doi:10.1016/j.jaci.2009.08.028
46. Gattinger P, Lupinek C, Kalogiros L, et al. The culprit insect but not severity of allergic reactions to bee and wasp venom can be determined by molecular diagnosis. PLoS One. 2018;13(6):e0199250. doi:10.1371/journal.pone.0199250
47. Blank S, Seismann H, McIntyre M, et al. Vitellogenins are new high molecular weight components and allergens (Api m 12 and Ves v 6) of Apis mellifera and Vespula vulgaris Venom. PLoS One. 2013;8(4):e62009. doi:10.1371/journal.pone.0062009
48. Yoon KA, Kim K, Kim WJ, et al. Characterization of venom components and their phylogenetic properties in some aculeate bumblebees and wasps. Toxins. 2020;12(1):47. doi:10.3390/toxins12010047
49. Yoon KA, Kim WJ, Lee SH. Expression profiles of venom components in some social hymenopteran species over different post-capture periods. Comp Biochem Physiol Part C Toxicol Pharmacol. 2022;253:109247. doi:10.1016/j.cbpc.2021.109247
50. Mauss V. Bionomie und Abwehrverhalten der in Deutschland vorkommenden allergologisch bedeutsamen Bienen und Faltenwespen: (Hymenoptera, Apidae, Vespidae) [Bionomics and defensive behaviour of bees and diplopterous wasps (Hymenoptera, Apidae, Vespidae) causing venom allergies in Germany]. Hautarzt. 2008;59(3):184–193. German. doi:10.1007/s00105-008-1472-8
51. Worm M, Eckermann O, Dölle S, et al. Triggers and Treatment of Anaphylaxis. Dtsch Ärztebl Int. 2014;111:367.
52. Arzt L, Bokanovic D, Schwarz I, et al. Hymenoptera stings in the head region induce impressive, but not severe sting reactions. Allergy. 2016;71(11):1632–1634. doi:10.1111/all.12967
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Pragmatic Primary Practice Approach to Using Specific IgE in Allergy Testing in Asthma Diagnosis, Management, and Referral
Demoly P, Liu AH, Rodriguez del Rio P, Pedersen S, Casale TB, Price D
Journal of Asthma and Allergy 2022, 15:1069-1080
Published Date: 16 August 2022