Back to Journals » Infection and Drug Resistance » Volume 16
Intra-Abdominal Hypertension Contributes to the Development of Ventilator-Associated Pneumonia from Intestinal Bacteria
Authors Zheng R, Jiang Y, Yan C, Li Y, Song X, Zheng P
Received 19 January 2023
Accepted for publication 15 March 2023
Published 31 March 2023 Volume 2023:16 Pages 1913—1921
DOI https://doi.org/10.2147/IDR.S403714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Rui Zheng,1,* Yaxian Jiang,1,* Cheng Yan,2,* Yikun Li,1 Xiaozhou Song,3 Pengcheng Zheng4
1Department of Clinical Laboratory, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China; 2Medical School, Kunming University of Science and Technology, The First People’s Hospital of Yunnan, Kunming, People’s Republic of China; 3Department of Infection Control, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China; 4Department of Pharmacy, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pengcheng Zheng, Department of Pharmacy, The First People’s Hospital of Yunnan Province, No. 157 of Jingbi Road, Kunming, People’s Republic of China, Tel +86 013888116045, Email [email protected] Xiaozhou Song, Department of Infection Control, The First People’s Hospital of Yunnan Province, No. 157 of Jingbi Road, Kunming, People’s Republic of China, Tel +86 013888144965, Email [email protected]
Introduction: Ventilator-associated pneumonia (VAP) is an ICU (intensive care unit)-acquired pulmonary parenchymal infection that is complicated by mechanical ventilation and is associated with high morbidity and mortality. Klebsiella pneumoniae (KPN) is known to asymptomatically colonize the gastrointestinal tract and may increase the incidence of corresponding VAP. Our study aims were to investigate the exact origin of the carbapenem-resistant Klebsiella pneumoniae (CRKP) causing VAP in our patient.
Methods: Various environmental samples, including the patient’s anal swab, were collected in order to find the source of the bacteria. Minimum inhibitory concentrations (MICs) for antimicrobial agents were determined according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI); resistant genes were detected by using PCR and sequencing; clone relationships were analyzed by using multilocus-sequence typing (MLST) and pulsed field gel electrophoresis (PFGE). The IAP values were obtained via urinary catheter.
Results: One CRKP strain was detected in the patient’s anal swab; this strain was confirmed with the same gene type as the strain isolated from the sputum. We found that the patient’s intra-abdominal pressure (IAP) was 29.41, 27.06, 24.12, and 22.66 mmHg; the IAP was either equal to or above 12 mmHg, on the operation day and the following three days. Intra-abdominal hypertension (IAH) occurred during the patient’s hospitalization and was considered to be caused by the surgical procedure. Meanwhile, we found that there was a correlation between IAH and the detection of CRKP in the sputum. The findings suggested that his VAP was caused by intestinal colonial KPN, and not from the environment.
Discussion: Our research illustrated that the ST11 KPC-2-producing strain colonized the intestinal tract and caused the development of VAP when the IAP was elevated. Routine screening for the intestinal carriage of CRKP, among patients in ICUs, can limit and prevent current and future outbreaks.
Keywords: ventilator-associated pneumonia, intra-abdominal pressure, intra-abdominal hypertension, Klebsiella pneumoniae, healthcare-associated infection
Introduction
Mechanical ventilation has been widely applied for critically ill patients and can lead to nosocomial infections, especially in intensive care units (ICUs). Ventilator-associated pneumonia (VAP) is an ICU-acquired pulmonary parenchymal infection that is complicated by mechanical ventilation lasting over two days and which is associated with high morbidity and mortality.1 Previous studies suggest that IAH is an independent risk factor for increased VAP incidence in critically ill patients.2–4 Human and animal experiments physiological studies suggest that IAH can impair respiratory function.2,4 Increasing attention to intra-abdominal pressure (IAP) and changes in the clinical management of patients who are critically ill or injured have led to an increase in research relating to IAH.5 IAH may induce physiological changes that could increase VAP frequency in ICU patients, but clinical data are very limited.4
Enterobacteriaceae are the most common pathogenic bacteria causing VAP.6 Klebsiella pneumoniae (KPN), an Enterobacteriaceae species, is known to asymptomatically colonize the skin, mouth, and respiratory and gastrointestinal tracts. About 50% of KPN infections arise from patients’ own microbiota.7 KPN colonization may increase the incidence of corresponding infections in critically ill patients. Carbapenems are antibiotics that are frequently used to treat KPN infections. The emergence of carbapenem-resistant KPN (CRKP) poses a challenge for the treatment of KPN infections, especially among ICU patients. Antimicrobial resistance in these pathogens may impact the outcome of patients with VAP, as it limits antibiotic treatment to harsher drugs, such as ceftazidime-avibactam (CAZ/AVI).
The risk factors associated with ICU-acquired CRKP among patients who were negative for CRKP colonization at the time of admission included previous exposure to carbapenems, β-lactam/β-lactamases inhibitor, and invasive processes or surgical operations.8
Here, we show that IAH is a risk factor for VAP that is caused by the intestinal colonial microbiota ST11 KPC-2-producing KPN. We analyzed the gut microbiota of a patient with a pulmonary KPN infection to uncover the relationship between IAH and KPC-2-producing, KPN-induced VAP. Our findings can be used to help prevent or reduce the risk of CRKP infection in critical patients by allowing clinicians to design more effective therapeutic approaches.
Materials and Methods
Bacterial Isolates
To identify the source of KPC-2-producing KPN, we screened the environmental swabs of the ward in which patient G was hospitalized on the day the first sputum sample that contained CRKP was collected, including swabs of the bed linens, the door knob of the isolation ward, the surface of the call button, the ward’s automatic faucet, the ward’s mop pool the surface of ventilator, the surface of microinjection pump, the inspiratory and expiratory ports of the ventilator, the moisture trap of ventilator, the surface of the gas valve, the pump of bottles with hand-washing-free disinfectant inside and outside the isolation ward, all doctors’ white coats, all nurses’ white coats, the hand swab of patient’s son, the care workers’ nasal swabs, the care workers’ throat swabs, and the care workers’ anal swabs. Two ST641 CSKP isolates were obtained from care worker Z’s throat swab and mop pool, with both a genotype and a phenotype completely different from those of previously isolated strains G1-G6.
Ward Investigation
The ICU in the General Surgery Department of the First People’s Hospital of Yunnan Province consists of one ward with nine beds and an isolation ward with one bed.
VAP Diagnosis
Clinical criteria for the suspicion of VAP include a new and persistent (48h) or progressive radiographic infiltrate plus two of the following: temperature of 38°C or 36°C, blood leukocyte count of 10,000 cells/mL or 5000 cells/mL, purulent tracheal secretions, and gas exchange degradation.9
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility was determined using the disk diffusion method and the automated VITEK 2 Compact system with gram-negative bacteria cards (bioMérieux). The microdilution susceptibility testing method was employed to verify the minimal inhibitory concentrations (MICs) of the antibiotics, and the results were interpreted based on Clinical & Laboratory Standards Institute (CLSI) guidelines.10 The antibiotics tested using microdilution included imipenem, meropenem, ceftriaxone, aztreonam, tigecycline, tetracycline, ciprofloxacin, gentamicin, and ceftazidime-avibactam. Escherichia coli (ATCC 25922) was used as the quality-control strain for antimicrobial susceptibility testing.
Detection of Phenotypes
The production of carbapenemases was evaluated in all isolates using Modified Carbapenem Inactivation Methods according to CLSI-M100.10 Klebsiella pneumoniae (ATCC BAA-1705, ATCC BAA-1706 and ATCC BAA-2146) were used as the quality-control strain.
Detection of Drug‑Resistant Genes
Bacterial chromosomal DNA was obtained with a TIANamp Bacterial DNA Kit according to the manufacturer’s instructions (TIANGEN BIOTECH, Beijing, China). PCR and DNA sequence analysis were performed to confirm the presence of drug-resistant genes, including carbapenemase, extended spectrum β-lactamases, and plasmid-mediated AmpC genes. The primers used in this study were described previously.11–17 The β-lactamase genes included Ambler class A (blaCTX-M, blaTEM, blaSHV, blaKPC, and blaGES), class B (blaNDM and blaIMP), class C (blaCMY and blaDHA), and class D (blaOXA-48). All amplicon sequences were compared with those in the GenBank database (www.ncbi.nlm.nih.gov/blast/).
Molecular Typing
All nine isolates were genotyped using multilocus sequence typing (MLST) and pulsed-field gel electrophoresis (PFGE). Seven housekeeping genes (aroC, dnaN, hemD, hisD, purE, sucA, thrA) were amplified according to the protocol described on the MLST website (https://pubmlst.org). Genotyping was carried out by referring to the PFGE molecular typing method used for Salmonella serotypes for the PulseNet China platform. Salmonella was entrapped with SeaKem Gold Agarose and digested with the restriction enzyme XbaI. The obtained DNA fragments underwent PFGE and were then classified by the CHEF Mapper XA system (Bio-Rad, Hercules, California, United States). Finally, cluster analysis was performed with BioNumerics (bioMérieux).
Measurement of Intra-Abdominal Pressure
An IAH diagnosis is based only on the IAP value, which can be obtained via urinary catheter because urinary blood pressure is a close approximate of IAP.
Results
Bacterial Isolates
Nine KPN isolates were identified by simultaneously using the VITEK 2 Compact and VITEK MS systems (bioMérieux, Lyon, France). Six of nine KPN isolates were isolated from the sputum of patient G on postoperative days 5, 6, 7, 8, 9, and 10, and were numbered G1 to G6. The other three KPN isolates were isolated from an anal swab of patient G (isolate number PW3), care worker Z’s throat swab (isolate number PW1), and from the mop pool (isolate number PW2).
Antimicrobial Susceptibility Testing
The drug-resistance profiles of G1, G2, G3, G4, G5, G6, and PW3 showed high resistance to third-generation cephalosporins, carbapenems, and monobactam. The MIC values of aminoglycoside and tetracycline were also high. The other two isolates (PW1 and PW2) were susceptible to β-lactam drugs, including carbapenems. These results are summarized in Table 1.
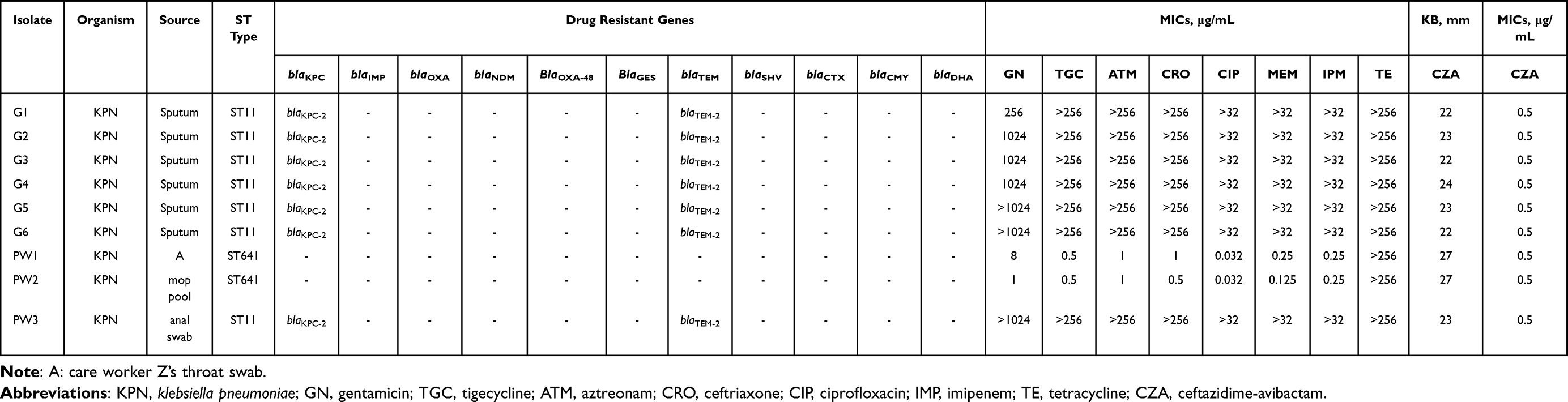 |
Table 1 Molecular Characteristics of Isolated KPN |
Intra-Abdominal Pressure
IAP is a steady-state pressure within the abdominal cavity, and the normal range is 0–5 mmHg. Our patient’s IAP was measured on the day of operation and on postoperative days 1, 4, 6, 9, 12, and 14, yielding measurements of 29.41, 27.06, 24.12, 22.66, 12.21, 7.33, and 5.23 mmHg, respectively (Table 2). The first four testing values were beyond 12 mmHg, which is the threshold for IAH.
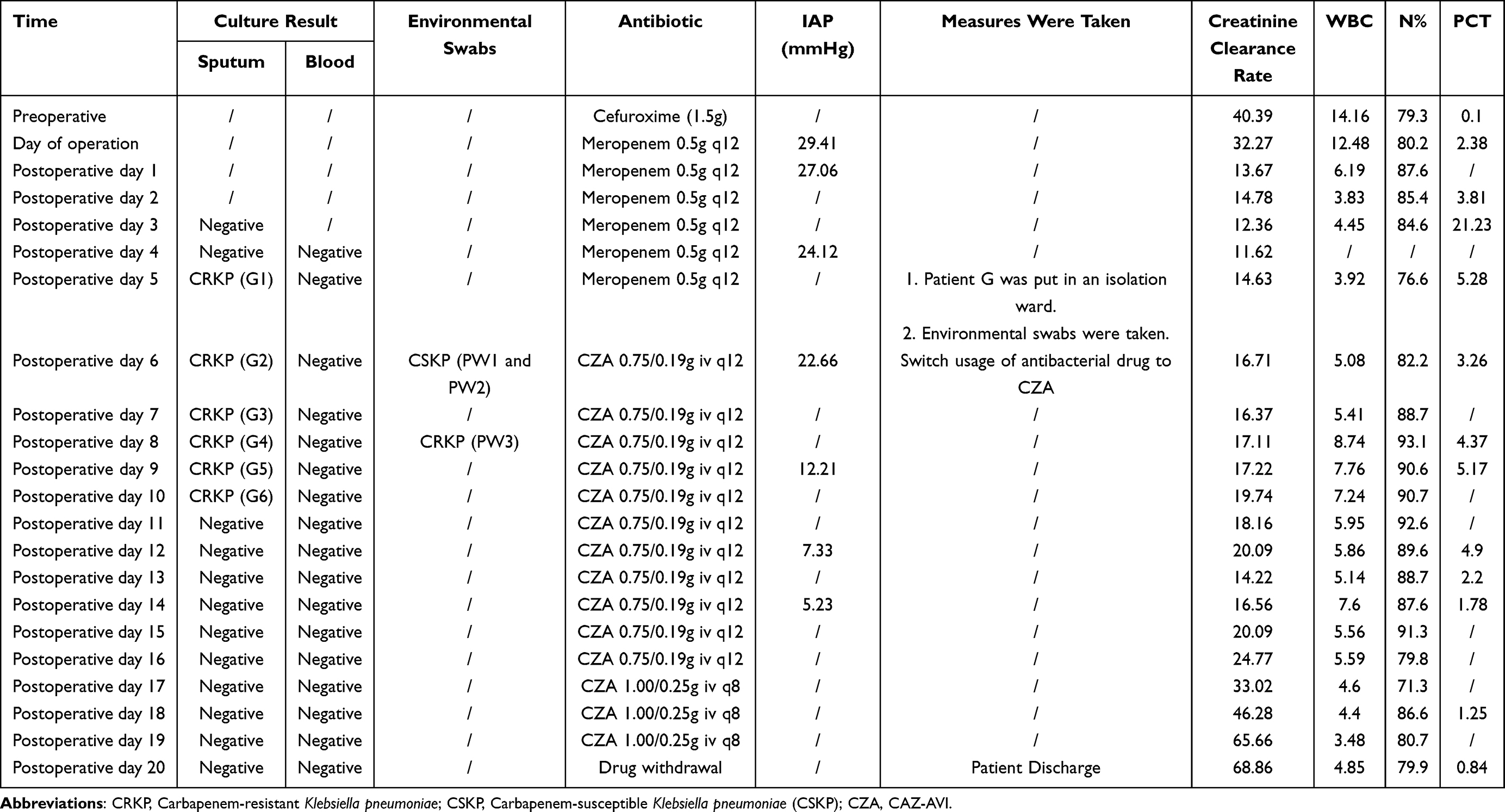 |
Table 2 Clinical Treatment Course of Patient G |
Detection of Phenotypes
G1-G6 and PW3 showed positive results for mCIM test and negative results for eCIM (EDTA-modified carbapenem inactivation method) which suggested these strains produce serine carbapenemase.
Drug-Resistant Genes
A total of 11 drug-resistant genes were amplified. The six strains isolated from sputum and one strain isolated from the anal swab produced KPC-2 carbapenemase and all had a 989-bp positive band. No carbapenemase gene was found in the two KPN isolates from the mop pool and the care worker’s throat swab. Other β-lactamase-resistance genes blaTEM-1 were detected. These results are summarized in Table 1.
Gene Type
All nine isolates were subjected to PFGE and MLST typing. Two PFGE genotypes were identified. Seven KPN isolates from patient G were classified into the same PFGE cluster and sequence type 11 (ST11). Another two KPN isolated from the mop pool and the nursing worker’s throat swab were in the same PFGE cluster and belonged to sequence type 641 (Figure 1).
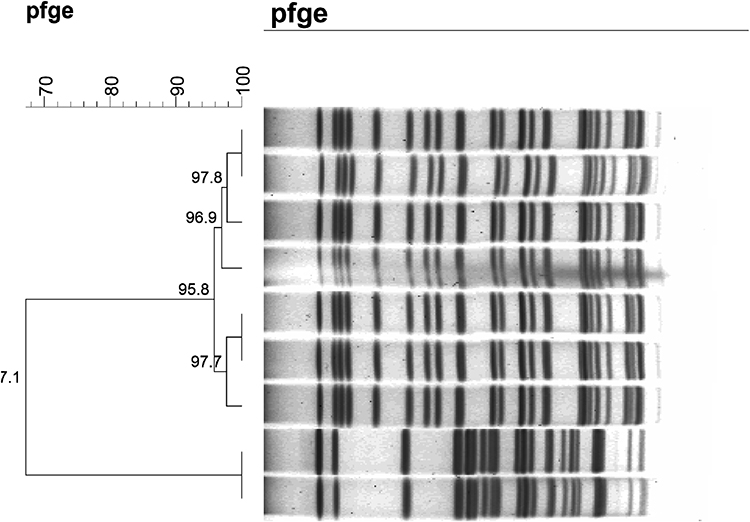 |
Figure 1 Dendrogram of PFGE patterns of chromosomal DNA restriction fragments from 9 K. pneumoniae isolates in present study. |
Discussion
VAP is one of the most frequent ICU-acquired infections associated with prolonged mechanical ventilation and ICU stays. The organisms associated with VAP vary due to factors including cumulative exposure to antimicrobials and the local ecology. Multivariable analysis showed that ICU stays longer than seven days, β-lactamase inhibitor antibiotics, and carbapenems are independent risk factors for VAP that is caused by carbapenem-resistant Enterobacteriaceae.1 More specifically, KPC-2-producing KPN leads to prolonged hospitalization, which in turn increases the risk of developing VAP. Our patient had two of these risk factors because they were in the ICU for over seven days and they were treated with meropenem, which is carbapenem. KPN was isolated from the patient’s sputum on six consecutive days. All the blood cultures sent to the laboratory were negative for KPN; we speculate that this may be due to continuous administration of antimicrobial agents. All six KPN isolates isolated from sputum carried blaKPC-2 and were resistant to carbapenems. Patient G’s pulmonary CT scan appeared normal upon the emergency visit to the hospital, which verifies that this patient developed pneumonia during their hospitalization.
Gut colonization is a critical first step for many pathogens that cause both intestinal and extra-intestinal infection. The risk factors associated with acquiring CRKP colonization during an ICU stay among patients who are negative for CRKP colonization at admission included undergoing invasive processes or surgical operations and previous exposure to carbapenem, tigecycline, or β-lactam/β-lactamases inhibitor.8 Intestinal colonization by CRKP is consistently associated with subsequent infection, and patients are predominantly infected with their colonizing strain.18–20 In this study, patient G’s anal swab was screened for rectal carriage of KPN after isolation of KPC-2-producing KPN. After ST11 KPC-2-producing KPN (PW3) was obtained from patient G’s anal swab, PFGE was performed and confirmed that PW3 was the same strain as strains G1-G6, which were isolated from patient G’s sputum. CRKP was found in patient G’s anal swab, indicating that the gut is a reservoir of infectious KPN.
Animal experiments21 have shown that increased IAP could cause severe intestinal ischemia, and significant decreases in mesenteric artery and portal vein blood flow, bacterial translocation, and gut-induced lung injury occurred from intestinal sites as IAP increased from 10 to 15 mmHg. IAH in humans is defined as a sustained increase in IAP equal to or above 12 mmHg. The highest incidence of IAH is observed in ICU patients who have undergone an emergency laparotomy.22,23 Our patient G was diagnosed with a bilateral iliac aneurysm and a ruptured iliac aneurysm, and underwent a surgical operation that involved endovascular abdominal aortic aneurysm repair, balloon dilation of the abdominal aorta, right internal iliac artery embolization, and balloon dilation of the right iliac artery. The patient’s IAP was 29.41, 27.06, 24.12 and 22.66 mmHg on the operation day and the next three days. The IAP data show that our patient presented with IAH during his stay in the ICU. Meanwhile, the same PFGE clone was isolated from both the patient’s sputum and their intestinal tract, confirming that the ST11 KPC-2-producing strain colonized the intestinal tract of patient G, causing the development of VAP when IAP was elevated.
Carbapenem‐resistant Enterobacterales (CRE)-induced HAP is associated with a significantly higher infection-related mortality rate than that observed in CRE infections at other sites (61.4% versus 34.6%). Microbiological confirmation of VAP infection is crucial, and antibiotic treatments should be based on in vitro drug sensitivity tests. Ceftazidime-avibactam (CAZ-AVI) is a promising option for the treatment of carbapenem-resistant, gram-negative bacteria, has been approved by the US Food and Drug Administration (FDA) and European Medicines Agency for the treatment of HAP/VAP owing to its attractive bactericidal broad-spectrum activity, linear pharmacokinetics with a moderate degree of lung penetration, and low risk of serious adverse events. According to CRKP detection, we use CAZ-AVI at a dosage of 1.00/0.25g IV q8hr, based on creatinine clearance rate (Table 2). In our patient, CAZ-AVI maintain a good antibacterial effect of KPC-2-producing KPN, given its low mortality and recurrence rates even following monotherapy. Patient G improved and was discharged after a 14-day course of CAZ-AVI treatment.
Because KPN colonization may serve as a reservoir for ICU-acquired infections,8 routine screening for intestinal carriage of CRKP among patients in ICUs could limit and prevent current and future outbreaks. In the near future, the use of bacteriophages to control pathogens may offer a non-antibiotic-based approach to treat multidrug-resistant infections such as CRKP.24
Conclusion
Our research illustrated that the ST11 KPC-2-producing strain colonized the intestinal tract and caused the development of VAP when the IAP was elevated. Ceftazidime-avibactam has a positive effect in the treatment of KPC-2-producing KPN-induced VAP even when used as monotherapy. Routine screening for the intestinal carriage of CRKP, among patients in ICUs, can limit and prevent current and future outbreaks.
Ethics Statement
The clinical isolates in this study were specifically isolated for this research. Ethical approval was obtained from the Institutional Ethics Committee (The First People’s Hospital of Yunnan Province, Kunming, Yunnan, China). Written informed consent was received from patient G’s son, aged 40, and care worker Z before sample collection that the study participants gave consent to publish.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82160403), the Yunnan Science and Technology Commission (202101AY070001-247) of the Yunnan provincial Science and Technology Department and Kunming Medical University, the Health Commission of Yunnan Province Talent Program, Grant No. H-2017027, Young and middle-aged academic and technical leaders talent project, Grant No. 202305AC160023, and the Respiratory Clinical Medical Center of Yunnan, Grant No. 2020LCZXKF-HX01.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gao B, Li X, Yang F, et al. Molecular epidemiology and risk factors of ventilator-associated pneumonia infection caused by carbapenem-resistant enterobacteriaceae. Front Pharmacol. 2019;10:262. doi:10.3389/fphar.2019.00262
2. Papakrivou E, Makris D, Manoulakas E, et al. Intra-abdominal hypertension causes bacterial growth in lungs: an animal study. Biomed Res Int. 2017;2017:4601348. doi:10.1155/2017/4601348
3. Papakrivou E, Makris D, Manoulakas E, Karvouniaris M, Zakynthinos E. Intra-abdominal hypertension is a risk factor for increased VAP incidence: a prospective cohort study in the ICU of a tertiary hospital. J Intensive Care Med. 2018;885066618779369. doi:10.1177/0885066618779369
4. Papakrivou E, Manoulakas E, Zakynthinos E, Makris D. Is intra-abdominal hypertension a risk factor for ventilator-associated pneumonia? Ann Transl Med. 2018;6(21):419. doi:10.21037/atm.2018.08.27
5. Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013;39(7):1190–1206. doi:10.1007/s00134-013-2906-z
6. Rouze A, Martin-Loeches I, Nseir S. Airway devices in ventilator-associated pneumonia pathogenesis and prevention. Clin Chest Med. 2018;39(4):775–783. doi:10.1016/j.ccm.2018.08.001
7. Gorrie CL, Mirceta M, Wick RR, et al. Gastrointestinal carriage is a major reservoir of Klebsiella pneumoniae infection in intensive care patients. Clin Infect Dis. 2017;65(2):208–215. doi:10.1093/cid/cix270
8. Qin X, Wu S, Hao M, et al. The colonization of carbapenem-resistant klebsiella pneumoniae: epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Supplement_2):S206–S214. doi:10.1093/infdis/jiz622
9. Koenig SM, Truwit JD. Ventilator-associated pneumonia: diagnosis, treatment, and prevention. Clin Microbiol Rev. 2006;19(4):637–657. doi:10.1128/CMR.00051-05
10. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 29th Ed. CLSI Supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2019.
11. Hong SS, Kim K, Huh JY, Jung B, Kang MS, Hong SG. Multiplex PCR for rapid detection of genes encoding class A carbapenemases. Ann Lab Med. 2012;32(5):359–361.
12. P¨¦rez-P¨¦rez FJ, Hanson ND. Detection of plasmid-mediated AmpC beta-lactamase genes in clinical isolates by using multiplex PCR. J Clin Microbiol. 2002;40(6):2153–2162. doi:10.1128/JCM.40.6.2153-2162.2002
13. Pagani L, Dell’Amico E, Migliavacca R, et al. Multiple CTX-M-type extended-spectrum beta-lactamases in nosocomial isolates of Enterobacteriaceae fr om a hospital in northern Italy. J Clin Microbiol. 2003;41(9):4264–4269. doi:10.1128/JCM.41.9.4264-4269.2003
14. Poirel L, H¨¦ritier C, Tol¨¹n V, Nordmann P. Emergence of oxacillinase-mediated resistance to imipenem in Klebsiella pneumoniae. Antimicrob Agents Chemother. 2004;48(1):15–22. doi:10.1128/AAC.48.1.15-22.2004
15. Robicsek A, Strahilevitz J, Sahm DF, Jacoby GA, Hooper DC. qnr prevalence in ceftazidime-resistant Enterobacteriaceae isolates from the United States. Antimicrob Agents Chemother. 2006;50(8):2872–2874. doi:10.1128/AAC.01647-05
16. Weldhagen GF, Poirel L, Nordmann P. Ambler class A extended-spectrum beta-lactamases in Pseudomonas aeruginosa: novel developments and cl inical impact. Antimicrob Agents Chemother. 2003;47(8):2385–2392. doi:10.1128/AAC.47.8.2385-2392.2003
17. Wolter DJ, Khalaf N, Robledo IE, et al. Surveillance of carbapenem-resistant Pseudomonas aeruginosa isolates from Puerto Rican Medical Center Hospitals: dissemination of KPC and IMP-18 beta-lactamases. Antimicrob Agents Chemother. 2009;53(4):1660–1664. doi:10.1128/AAC.01172-08
18. Rao K, Seekatz A, Bassis C, Sun Y, Mantlo E, Bachman MA. Enterobacterales infection after intestinal dominance in hospitalized patients. mSphere. 2020;5(4). doi:10.1128/mSphere.00450-20
19. Vornhagen J, Bassis CM, Ramakrishnan S, et al. A plasmid locus associated with Klebsiella clinical infections encodes a microbiome-dependent gut fitness factor. PLoS Pathog. 2021;17(4):e1009537. doi:10.1371/journal.ppat.1009537
20. Christos Doudakmanis RS, Makri A, Loutsou M, et al. Relationship Between Intra-Abdominal pressure and microaspiration of gastric contents in critically ill mechanically ventilated patients. J Crit Care. 2023;74:154220.
21. Yagci G, Zeybek N, Kaymakcioglu N, et al. Increased intra-abdominal pressure causes bacterial translocation in rabbits. J Chin Med Assoc. 2005;68(4):172–177. doi:10.1016/S1726-4901(09)70244-8
22. Ivatury RR, Porter JM, Simon RJ, Islam S, John R, Stahl WM. Intra-abdominal hypertension after life-threatening penetrating abdominal trauma: prophylaxis, incidence, and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J Trauma. 1998;44(6):1016–21;discussion 1021–3. doi:10.1097/00005373-199806000-00014
23. Malbrain ML, De Laet IE. Intra-abdominal hypertension: evolving concepts. Clin Chest Med. 2009;30(1):45–70. doi:10.1016/j.ccm.2008.09.003
24. Tan D, Zhang Y, Cheng M, et al. Characterization of Klebsiella pneumoniae ST11 isolates and their interactions with lytic phages. Viruses. 2019;11(11). doi:10.3390/v11111080
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characterization of ST11 and ST15 Carbapenem-Resistant Hypervirulent Klebsiella pneumoniae from Patients with Ventilator-Associated Pneumonia
Song S, Zhao S, Wang W, Jiang F, Sun J, Ma P, Kang H
Infection and Drug Resistance 2023, 16:6017-6028
Published Date: 8 September 2023