")
Back to Journals » Infection and Drug Resistance » Volume 16
Intra-Abdominal Abscess and Bacteremia Due to Stenotrophomonas maltophilia After Total Gastrectomy: A Case Report and Literature Review
Authors Hirai J , Mori N , Sakanashi D, Shibata Y, Asai N, Hagihara M, Mikamo H
Received 30 August 2023
Accepted for publication 4 November 2023
Published 10 November 2023 Volume 2023:16 Pages 7197—7204
DOI https://doi.org/10.2147/IDR.S433564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jun Hirai,1,2 Nobuaki Mori,1,2 Daisuke Sakanashi,2 Yuichi Shibata,2 Nobuhiro Asai,1,2 Mao Hagihara,3 Hiroshige Mikamo1,2
1Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 2Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 3Department of Molecular Epidemiology and Biomedical Sciences, Aichi Medical University, Nagakute, Aichi, Japan
Correspondence: Jun Hirai, Department of Clinical Infectious Diseases, Aichi Medical University Hospital, 1-1, Yazako-karimata, Nagakute, Aichi, 480-1195, Japan, Tel +81-561-62-3311, Fax +81-561-76-2673, Email [email protected]
Abstract: Stenotrophomonas maltophilia (S. maltophilia) is increasingly recognized as a pathogen responsible for nosocomial infections, particularly in immunocompromised patients. The most common types of S. maltophilia infections are pneumonia and catheter-related bloodstream infection, and clinical cases of intra-abdominal abscesses due to S. maltophilia are rare. We present a rare case of intra-abdominal abscess and bacteremia as a surgical site infection (SSI) caused by S. maltophilia in a patient following total gastrectomy. We also reviewed previous literature to elucidate the clinical characteristics of intra-abdominal abscess due to S. maltophilia. The patient, a 75-year-old man with diabetes and polymyositis (treated with prednisolone), developed a fever 17 days after undergoing a total gastrectomy for gastric cancer. Abdominal computed tomography revealed a hypodense solid mass at the esophagojejunostomy site, which appeared to be an intra-abdominal abscess. The culture of both blood and drained abscess pus confirmed only S. maltophilia. Treatment with intravenous trimethoprim-sulfamethoxazole and abscess drainage led to complete resolution. The patient recovered and was discharged and did not experience a recurrence. We reviewed the English literature and found only two additional case reports of intra-abdominal abscesses caused by S. maltophilia. As in our case, the intra-abdominal abscess occurred after abdominal surgery and the source was suspected to be deep SSI. This case highlights the importance of considering S. maltophilia as a potential pathogen in patients with atypical post-surgical abdominal infections. Physicians should be aware that S. maltophilia has the potential to cause intra-abdominal abscesses secondary to SSI, in addition to Enterobacteriaceae, a major causative pathogen of SSI. Further studies are required to elucidate the etiology, epidemiology, and risk factors for SSI caused by S. maltophilia.
Keywords: Stenotrophomonas maltophilia, abdominal abscess, surgical site infection
Introduction
Stenotrophomonas maltophilia (S. maltophilia) is an aerobic, motile, glucose-non-fermentative, gram-negative bacterium that is widespread in aqueous environments including hospitals.1 This pathogen, which was first isolated from a pleural effusion in 1943 and was initially named Bacterium booker, belongs to the family Xanthomonadaceae.2,3 The organism was renamed as Pseudomonas maltophilia and subsequently renamed as S. maltophilia in the genus Stenotrophomonas in 1993.4 A large surveillance investigation of patients with bacteremia revealed that S. maltophilia is the third most common nosocomial pathogen among non-fermentative bacteria after Pseudomonas aeruginosa and Acinetobacter spp.5 Although S. maltophilia is generally not considered highly pathogenic, it has emerged as an important nosocomial pathogen with reported mortality rates ranging from 21% to 69%.6–9
S. maltophilia frequently colonizes humid surfaces such as the medical tubes used in mechanical ventilation and indwelling blood and urinary catheters.4 Therefore, ventilator-associated pneumonia, catheter-related bloodstream infections, and catheter-associated urinary tract infections are the most common clinical manifestations of S. maltophilia infection, particularly in hospitalized immunocompromised patients, such as those taking steroids and receiving chemotherapy for cancer.10,11 Intra-abdominal abscesses caused by S. maltophilia have rarely been reported.12,13 In addition, organ/space surgical site infections (SSI) after total gastrectomy are typically caused by aerobes and anaerobes, such as Streptococcus spp., Enterobacteriaceae, and Prevotella spp., which are found in the flora colonizing the oral cavity and stomach, and isolation of S. maltophilia is rare.14
Given the rarity of intra-abdominal abscesses due to S. maltophilia, it is not possible to conduct large studies, and case reports are the primary source of knowledge about this condition. We share data of a rare case of a postoperative intra-abdominal abscess and bacteremia caused by S. maltophilia. We also summarize what is known about the clinical characteristics of intra-abdominal abscess caused by S. maltophilia from a review of previous literature.
Case Report
A 75-year-old Japanese man with diabetes mellitus and polymyositis underwent a total gastrectomy for gastric adenocarcinoma of the fundic gland. Cefazolin was administered as a perioperative antibiotic and was discontinued the day after surgery. No additional antibiotics were administered thereafter. Seventeen days after the surgery, he developed fever and chills during hospitalization. He had initially been scheduled to undergo a robot-assisted minimally invasive gastrectomy; however, the surgery was changed to laparoscopy-assisted total gastrectomy because of a rupture of the esophageal wall during resection using an ultrasonic energy device. The operation was completed without any other intra-operative complications after a total operation time of 580 minutes. He had experienced an exacerbation of polymyositis 5 weeks before the surgery, which was treated with oral prednisolone, starting with a dose of 20 mg/day (0.5 mg/kg) for 7 days, which was gradually reduced to 5 mg/day by the time of surgery.
His postoperative recovery after gastric surgery was uneventful. A liquid diet was started on postoperative day 6, the abdominal drain was removed on postoperative day 7, and an oral diet was started on postoperative day 9. However, on postoperative day 17, the day before his scheduled discharge, he developed a fever of 38°C and chills.
The physical findings at the time that the patient developed a fever were unremarkable: His lung sounds were clear, there were no heart murmurs, and there was no abdominal tenderness or rebound pain. The abdominal surgical incision wounds did not have any sign of inflammation or discharge. Blood tests revealed an elevated leukocyte count (17,800 cells/µL; normal range: 3300–8600 cells/µL), and C-reactive protein (9.88 mg/dL; normal: ≤0.04 mg/dL), and procalcitonin (1.11 ng/mL; normal: ≤0.05 ng/dL) levels. Abdominal computed tomography showed a 40 mm hypodense solid mass at the site of the esophagojejunostomy (Figure 1). Piperacillin/tazobactam (4.5 g intravenously every 8 hours) was started immediately on the diagnosis of the intra-abdominal abscess after obtaining two sets of blood cultures.
 |
Figure 1 Abdominal CT scan showing a hypo-absorptive area (red circle) of approximately 4 cm in diameter at the esophageal-jejunal anastomosis, suggesting an abscess. |
The following day, two aerobic blood culture bottles and pus obtained by CT-guided drainage confirmed the presence of gram-negative rods using Gram staining (Figure 2). Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) (MALDI Biotyper ver. 9.0.0.0; Bruker Daltonics, Billerica, MA, USA) confirmed that the microorganism isolated from blood culture was S. maltophilia with a spectral score of 2.351. Therefore, we initiated intravenous trimethoprim-sulfamethoxazole (SXT), which is the first-line drug for treating S. maltophilia infection, intravenously (480 mg/2400 mg per day) and inserted a pigtail catheter to drain the abscess. Two days of aerobic and anaerobic cultures of the blood and abscess confirmed only S. maltophilia, and hence, piperacillin/tazobactam was discontinued and the antibiotic was changed to SXT alone (Figure 3). Antimicrobial susceptibility was measured using the MicroScan WalkAway system with an NM2J panel (Beckman Coulter) according to the Clinical and Laboratory Standards Institute guidelines (M-100-ED32:2022). The results revealed that the S. maltophilia isolate was sensitive to SXT, levofloxacin (LVFX), and minocycline (MINO).
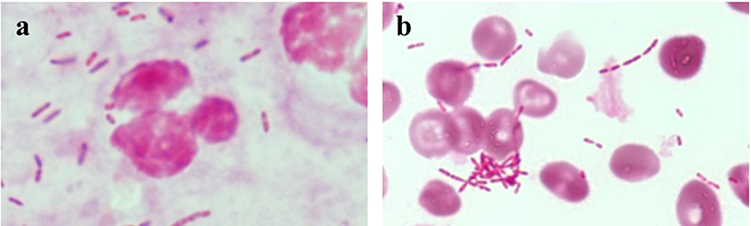 |
Figure 2 Gram-stain of pus obtained by computed tomography-guided abdominal abscess drainage (a) and a positive anaerobic blood culture 20 hours after collection (b). The Gram-stain shows gram-negative rods with phagocytosis of leukemic cells in the pus obtained abdominal abscess (a) and gram-negative rods in the anaerobic blood culture (b) (magnification; ×1000). |
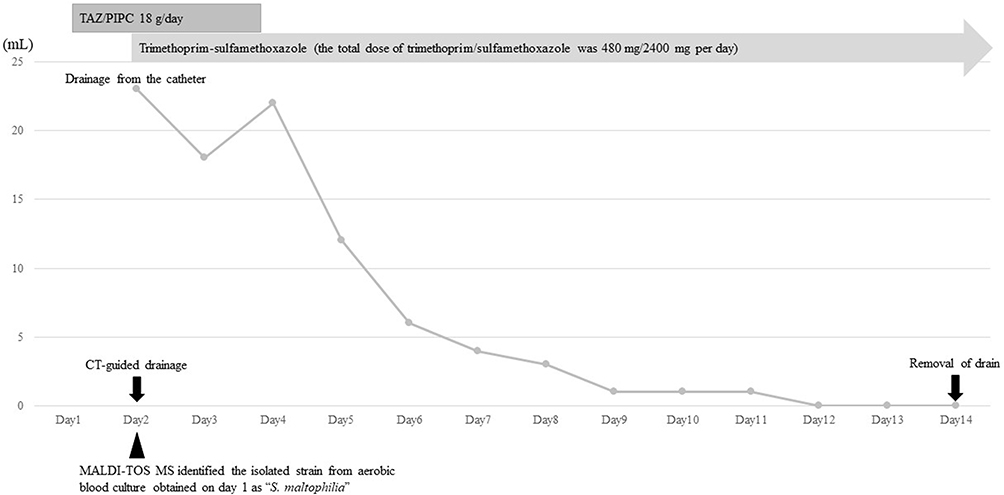 |
Figure 3 Clinical course of the patient after the onset of fever. |
Abdominal CT after 14 days of drainage revealed complete resolution of the abscess. Therefore, the pigtail catheter was removed, and the intravenous SXT was changed to oral SXT (480 mg/2400 mg per day), which was continued for a further 2 weeks (for a total of 4 weeks). The patient recovered without any recurrence and was discharged.
Written informed consent was obtained from the patient accompanying the image, and the present case was in line with the surgical case report guidelines.15
Discussion
This case of intra-abdominal abscess and bacteremia due to S. maltophilia occurred in a patient who had undergone total gastrectomy and was successfully treated with drainage and SXT. Infection due to S. maltophilia typically occurs in severely immunocompromised and debilitated individuals.16 Risk factors for S. maltophilia infection include admission to an intensive care unit, blood and solid tumors, neutropenia, central venous catheters, mechanical ventilation, recent surgery, and previous therapy with broad-spectrum antibiotics, such as carbapenems and cephalosporins, and S. maltophilia isolation within the previous 30 days.17–19 Although our patient was taking a low dose of prednisolone for polymyositis and had recently undergone surgery for a solid tumor, he did not have other major risk factors for S. maltophilia bacteremia. Only a few case reports of intra-abdominal abscesses due to S. maltophilia have been published; therefore, the risk factors for intra-abdominal abscesses due to S. maltophilia are unclear.
The incidence of S. maltophilia hospital-acquired infections is increasing, ranging from 7.1 to 37.7 cases per 10000 discharges.1,3,20,21 S. maltophilia has been reported as a common cause of peritonitis, particularly in patients on peritoneal dialysis.22–26 In patients on continuous ambulatory peritoneal dialysis, predisposing factors for S. maltophilia peritonitis include diabetes mellitus, anemia, and malnutrition.23 However, reports of intra-abdominal abscesses caused by this organism are rare. A search of the PubMed database on July 16, 2023, yielded only two case reports on S. maltophilia-induced intra-abdominal abscesses published in English, one from Japan and one from Korea (Table 1).12,13 One patient was a 68-year-old woman who developed an intra-abdominal abscess caused by S. maltophilia 10 days after a resection of the transverse colon for colon cancer and partial resection of the left kidney for renal carcinoma.12 She was treated with intravenous MINO for 2 weeks and oral LVFX for 2 weeks in addition to drainage of the abscess, which resulted in complete resolution.12 The other case was a 14-year-old boy who developed an intra-abdominal abscess caused by S. maltophilia 14 days after a laparoscopic appendectomy for a perforated appendix. He was treated with percutaneous drainage and 2 weeks of SXT and recovered.13 All three cases of S. maltophilia intra-abdominal abscesses, including our case, occurred after abdominal surgery. Therefore, abdominal surgery may be a risk factor for intra-abdominal abscesses caused by S. maltophilia.
 |
Table 1 Case Reports on Intra-Abdominal Abscesses Caused by Stenotrophomonas maltophilia Published in English |
The presence of two intrinsic, inducible β-lactamase enzymes (L1 and L2) makes β-lactam agents unsuitable as a treatment option.27 Therefore, non-β-lactam drugs such as SXT and fluoroquinolones are the primary antibiotics used, although their activity is limited by the vast array of efflux pumps present in S. maltophilia.28 SXT is generally considered the preferred antibiotic for S. maltophilia infections; however, there is no established PK/PD index or target threshold for effectiveness to optimize its clinical use.29 In addition, the limited clinical data available are from observational studies rather than randomized controlled trials. No prospective trials comparing treatment options for S. maltophilia have been conducted. In this case, we selected SXT as the antibiotic for treating the S. maltophilia intra-abdominal abscesses. Although several clinical studies have been conducted on SXT for pneumonia and bacteremia,30,31 evidence of the clinical effectiveness of SXT for treating intra-abdominal S. maltophilia infections is limited. Further studies, including studies on new antibiotics such as cefiderocol, are essential to identify the optimal antibiotics for treating S. maltophilia abdominal infection.
The origin of the infection in our patient was unclear. One possibility is contamination of the abdominal cavity by S. maltophilia from surgical instruments or the hospital environment during surgery. Our patient had a prolonged operation time because of esophageal rupture, so the S. maltophilia infection may have occurred during the operation. Until the isolation of S. maltophilia in this patient, there had been no instances of postoperative intra-abdominal abscesses caused by S. maltophilia at our hospital. Another possibility is that some patients have S. maltophilia colonization of the gastrointestinal tract,32 because the gastrointestinal tract is the most likely source of infection. The route of S. maltophilia infection was also unclear in the two previous case reports.12,13
The incidence of SSI varies from 5% to 30%, depending on the operative site and wound classification.33 This patient had risk factors for SSI such as prolonged operation time, diabetes, higher age, and use of immunosuppressive drugs.34,35 A recent meta-analysis revealed that the incidence of SSI after laparoscopic gastrectomy was 2.4% (21 events in a total of 869 cases).36 In addition, Kosuga et al37 reported that male sex (odds ratio [OR]: 3.4) and total gastrectomy (OR 3.1) were independent risk factors for deep SSI after laparoscopic gastrectomy for gastric cancer. However, operation time ≥320 min (OR 3.7) was independently associated with incisional SSI rather than deep SSI. The common pathogens isolated from stomach postoperative intra-abdominal infections are Escherichia coli, Klebsiella pneumoniae, Enterobacter spp., Staphylococcus aureus, and Enterococcus faecalis.38,39 In patients with SSI after gastrectomy for gastric cancer, the most common pathogens are E. coli (28 of 64; 36.8%) and K. pneumonia (11 of 64; 15.1%).40 Therefore, S. maltophilia is rarely considered as a potential causative organism in patients with intra-abdominal SSI. SSI due to S. maltophilia is very rare, Ince et al41 reported that the S. maltophilia accounted for only 1.5% (1 of 61) in their 6-year single-center retrospective study in patients with S. maltophilia infection. However, S. maltophilia is resistant to antibiotics, such as piperacillin/tazobactam, meropenem, and ceftriaxone, which are commonly used for abdominal SSI;42 therefore, if S. maltophilia infection is detected, appropriate alternative antibiotics must be selected.
The outcome of this and the two previous cases of intra-abdominal abscesses due to S. maltophilia was favorable, with complete resolution by drainage and use of antibiotics.12,13 The isolate in our patient was sensitive to SXT, MINO, and LVFX. We continued SXT for the treatment of intra-abdominal abscess due to S. maltophilia because both blood and abscess cultures confirmed only S. maltophilia. SXT is the first-line drug for S. maltophilia infection, and there have been no reports of the development of resistance to SXT during treatment, in contrast to reports of resistance to MINO and LVFX.43 Further research is needed to assess the most appropriate antibiotics for the treatment of deep SSI due to S. maltophilia.
This report has some limitations. First, it is a single case and the literature review revealed only two previously reported cases,12,13 so further reports are needed. However, these three cases reveal that S. maltophilia has the potential to cause intra-abdominal abscesses secondary to SSI. Second, we were unable to identify the source of S. maltophilia. To date, no studies regarding risk factors for intra-abdominal abscesses due to S. maltophilia have been published. Further studies are needed to clarify the epidemiology and clinical features of intra-abdominal abscesses caused by S. maltophilia.
Conclusion
In summary, we have described a case of an intra-abdominal abscess due to S. maltophilia after total gastrectomy in a patient with diabetes mellitus, polymyositis, and gastric cancer. Physicians should be aware that in addition to Enterobacteriaceae, a major cause of SSI, S. maltophilia has the potential to cause intra-abdominal abscesses secondary to SSI. Further studies are required to clarify the etiology, epidemiology, and risk factors for S. maltophilia-associated SSI.
Abbreviations
LVFX, levofloxacin; MALDI-TOF MS, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; MINO, minocycline; SSI, surgical site infection; SXT, trimethoprim-sulfamethoxazole.
Data Sharing Statement
The data is available from the corresponding author on reasonable request.
Ethics and Consent
Written informed consent was obtained from the patient for the publication of this case report. The present case did not require ethics committee approval based on the Japanese Ethical Guidelines for Clinical Research to publish case details.
Acknowledgments
We thank Editage for English language editing.
Author Contributions
All authors meet the ICMJE authorship criteria. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors and co-workers did not receive any specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41. doi:10.1128/CMR.00019-11
2. Palleroni NJ, Bradbury JF. Stenotrophomonas, a new bacterial genus for Xanthomonas maltophilia (Hugh 1980) Swings et al. 1983. Int J Syst Bacteriol. 1993;43(3):606–609. doi:10.1099/00207713-43-3-606
3. Denton M, Kerr KG. Microbiological and clinical aspects of infection associated with Stenotrophomonas maltophilia. Clin Microbiol Rev. 1998;11(1):57–80. doi:10.1128/CMR.11.1.57
4. Chang YT, Lin CY, Chen YH, Hsueh PR. Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Front Microbiol. 2015;6:893. doi:10.3389/fmicb.2015.00893
5. Jones RN, Sader HS, Beach ML. Contemporary in vitro spectrum of activity summary for antimicrobial agents tested against 18569 strains non-fermentative gram-negative bacilli isolated in the SENTRY Antimicrobial Surveillance Program (1997–2001). Int J Antimicrob Agents. 2003;22(6):551–556. doi:10.1016/S0924-8579(03)00245-0
6. Paez JI, Costa SF. Risk factors associated with mortality of infections caused by Stenotrophomonas maltophilia: a systematic review. J Hosp Infect. 2008;70(2):101–108. doi:10.1016/j.jhin.2008.05.020
7. Senol E, DesJardin J, Stark PC, Barefoot L, Snydman DR. Attributable mortality of Stenotrophomonas maltophilia bacteremia. Clin Infect Dis. 2002;34(12):1653–1656. doi:10.1086/340707
8. Wang WS, Liu CP, Lee CM, Huang FY. Stenotrophomonas maltophilia bacteremia in adults: four years’ experience in a medical center in northern Taiwan. J Microbiol Immunol Infect. 2004;37(6):359–365.
9. Hashimoto T, Komiya K, Fujita N, et al. Risk factors for 30-day mortality among patients with Stenotrophomonas maltophilia bacteraemia. Infect Dis. 2020;52(6):440–442. doi:10.1080/23744235.2020.1734653
10. Majumdar R, Karthikeyan H, Senthilnathan V, Sugumar S. Review on Stenotrophomonas maltophilia: an emerging multidrug-resistant opportunistic pathogen. Recent Pat Biotechnol. 2022;16(4):329–354.
11. Osawa K, Shigemura K, Kitagawa K, Tokimatsu I, Fujisawa M. Risk factors for death from Stenotrophomonas maltophilia bacteremia. J Infect Chemother. 2018;24(8):632–636. doi:10.1016/j.jiac.2018.03.011
12. Sawai T, Yoshioka S, Matsuo N, Suyama N, Mukae H. Intraabdominal abscess caused by Stenotrophomonas maltophilia: a case report. Int J Surg Case Rep. 2017;41:212–214. doi:10.1016/j.ijscr.2017.10.027
13. Lim DR, Kuk JC, Kim T, Shin EJ. Unusual case of rapid growing intraabdominal abscess caused by Stenotrophomonas maltophilia after laparoscopic appendectomy due to perforated appendicitis: a case report. Medicine. 2017;96(20):e6913. doi:10.1097/MD.0000000000006913
14. Hamza WS, Salama MF, Morsi SS, Abdo NM, Al-Fadhli MA. Benchmarking for surgical site infections among gastrointestinal surgeries and related risk factors: multicenter study in Kuwait. Infect Drug Resist. 2018;11:1373–1381. doi:10.2147/IDR.S167213
15. Agha RA, Fowler AJ, Saetta A, Barai I, Rajmohan S, Orgill DP; SCARE Steering Group. A protocol for the development of reporting criteria for surgical case reports: the SCARE statement. Int J Surg. 2016;27:187–189. doi:10.1016/j.ijsu.2016.01.094
16. Looney WJ, Narita M, Mühlemann K. Stenotrophomonas maltophilia: an emerging opportunist human pathogen. Lancet Infect Dis. 2009;9(5):312–323. doi:10.1016/S1473-3099(09)70083-0
17. Ebara H, Hagiya H, Haruki Y, Kondo E, Otsuka F. Clinical characteristics of Stenotrophomonas maltophilia bacteremia: a regional report and a review of a Japanese case series. Intern Med. 2017;56(2):137–142. doi:10.2169/internalmedicine.56.6141
18. Sumida K, Chong Y, Miyake N, et al. Risk factors associated with Stenotrophomonas maltophilia bacteremia: a matched case-control study. PLoS One. 2015;10(7):e0133731. doi:10.1371/journal.pone.0133731
19. Hotta G, Matsumura Y, Kato K, et al. Risk factors and outcomes of Stenotrophomonas maltophilia bacteraemia: a comparison with bacteraemia caused by Pseudomonas aeruginosa and Acinetobacter species. PLoS One. 2014;9(11):e112208. doi:10.1371/journal.pone.0112208
20. Falagas ME, Valkimadi PE, Huang YT, Matthaiou DK, Hsueh PR. Therapeutic options for Stenotrophomonas maltophilia infections beyond co-trimoxazole: a systematic review. J Antimicrob Chemother. 2008;62(5):889–894. doi:10.1093/jac/dkn301
21. Grupo Andaluz para el Estudio de las Enfermedades Infecciosas, Del Toro MD, Rodríguez-Bano J, Herrero M, et al. Clinical epidemiology of Stenotrophomonas maltophilia colonization and infection: a multicenter study. Medicine. 2002;81(3):228–239. doi:10.1097/00005792-200205000-00006
22. Tzanetou K, Triantaphillis G, Tsoutsos D, et al. Stenotrophomonas maltophilia peritonitis in CAPD patients: susceptibility to antibiotics and treatment outcome: a report of five cases. Perit Dial Int. 2004;24(4):401–404. doi:10.1177/089686080402400418
23. Baek JE, Jung EY, Kim HJ, et al. Stenotrophomonas maltophilia infection in patients receiving continuous ambulatory peritoneal dialysis. Korean J Intern Med. 2004;19(2):104–108. doi:10.3904/kjim.2004.19.2.104
24. Millán-Díaz B, González-Tabarés L, Cobelo-Casas C, López-Vázquez M, Calviño-Varela J. Stenotrophomonas maltophilia: a rare cause of peritonitis in CAPD patients. Nefrologia. 2017;37(6):646–647. doi:10.1016/j.nefro.2017.03.018
25. Rehman A, Ul-Ain Baloch N, Awais M. Severe ovarian hyperstimulation syndrome complicated by Stenotrophomonas maltophilia peritonitis: a case report and literature review. Intern Med. 2015;54(9):1149–1152. doi:10.2169/internalmedicine.54.3564
26. Machuca E, Ortiz AM, Rabagliati R. Stenotrophomonas maltophilia peritonitis in a patient receiving automated peritoneal dialysis. Adv Perit Dial. 2005;21:63–65.
27. Walsh TR, MacGowan AP, Bennett PM. Sequence analysis and enzyme kinetics of the L2 serine beta-lactamase from Stenotrophomonas maltophilia. Antimicrob Agents Chemother. 1997;41(7):1460–1464. doi:10.1128/AAC.41.7.1460
28. Alonso A, Martínez JL. Cloning and characterization of SmeDEF, a novel multidrug efflux pump from Stenotrophomonas maltophilia. Antimicrob Agents Chemother. 2000;44(11):3079–3086. doi:10.1128/AAC.44.11.3079-3086.2000
29. Kullar R, Wenzler E, Alexander J, Goldstein EJC. Overcoming Stenotrophomonas maltophilia resistance for a more rational therapeutic approach. Open Forum Infect Dis. 2022;9(5):ofac095. doi:10.1093/ofid/ofac095
30. Cai B, Tillotson G, Benjumea D, Callahan P, Echols R. The burden of bloodstream infections due to Stenotrophomonas maltophilia in the United States: a large, retrospective database study. Open Forum Infect Dis. 2020;7(5):ofaa141. doi:10.1093/ofid/ofaa141
31. Cho SY, Kang CI, Kim J, et al. Can levofloxacin be a useful alternative to trimethoprim-sulfamethoxazole for treating Stenotrophomonas maltophilia bacteremia? Antimicrob Agents Chemother. 2014;58(1):581–583. doi:10.1128/AAC.01682-13
32. Apisarnthanarak A, Fraser VJ, Dunne WM, et al. Stenotrophomonas maltophilia intestinal colonization in hospitalized oncology patients with diarrhea. Clin Infect Dis. 2003;37(8):1131–1135. doi:10.1086/378297
33. Hedrick TL, Sawyer RG, Friel CM, Stukenborg GJ. A method for estimating the risk of surgical site infection in patients with abdominal colorectal procedures. Dis Colon Rectum. 2013;56(5):627–637. doi:10.1097/DCR.0b013e318279a93e
34. Bratzler DW, Dellinger EP, Olsen KM, et al. American Society of Health-System Pharmacists (ASHP); Infectious Diseases Society of America (IDSA); Surgical Infection Society (SIS); Society for Healthcare Epidemiology of America (SHEA). Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg Infect (Larchmt). 2013;14(1):73–156. doi:10.1089/sur.2013.9999
35. Anderson DJ, Podgorny K, Berríos-Torres SI, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605–627. doi:10.1086/676022
36. Inokuchi M, Sugita H, Otsuki S, Sato Y, Nakagawa M, Kojima K. Laparoscopic distal gastrectomy reduced surgical site infection as compared with open distal gastrectomy for gastric cancer in a meta-analysis of both randomized controlled and case-controlled studies. Int J Surg. 2015;15:61–67. doi:10.1016/j.ijsu.2015.01.030
37. Kosuga T, Ichikawa D, Komatsu S, et al. Clinical and surgical factors associated with organ/space surgical site infection after laparoscopic gastrectomy for gastric cancer. Surg Endosc. 2017;31(4):1667–1674. doi:10.1007/s00464-016-5156-7
38. Takesue Y, Kusachi S, Mikamo H, et al. Antimicrobial susceptibility of common pathogens isolated from postoperative intra-abdominal infections in Japan. J Infect Chemother. 2018;24(5):330–340. doi:10.1016/j.jiac.2018.02.011
39. Li Z, Li H, Lv P, et al. Prospective multicenter study on the incidence of surgical site infection after emergency abdominal surgery in China. Sci Rep. 2021;11(1):7794. doi:10.1038/s41598-021-87392-8
40. Xiao H, Xiao Y, Quan H, Liu W, Pan S, Ouyang Y. Intra-abdominal infection after radical gastrectomy for gastric cancer: incidence, pathogens, risk factors and outcomes. Int J Surg. 2017;48:195–200. doi:10.1016/j.ijsu.2017.07.081
41. Ince N, Yekenkurul D, Danış A, Çalışkan E, Akkaş İ. An evaluation of six-year Stenotrophomonas maltophilia infections in a university hospital. Afr Health Sci. 2020;20(3):1118–1123. doi:10.4314/ahs.v20i3.13
42. Ban KA, Minei JP, Laronga C, et al. American college of surgeons and surgical infection society: surgical site infection guidelines, 2016 update. J Am Coll Surg. 2017;224(1):59–74. doi:10.1016/j.jamcollsurg.2016.10.029
43. Garrison MW, Anderson DE, Campbell DM, et al. Stenotrophomonas maltophilia: emergence of multidrug-resistant strains during therapy and in an in vitro pharmacodynamic chamber model. Antimicrob Agents Chemother. 1996;40(12):2859–2864. doi:10.1128/AAC.40.12.2859
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.