Back to Journals » Infection and Drug Resistance » Volume 19
Intestinal Colonization and Subsequent Nosocomial Infection with Carbapenem-Resistant Organisms in a PICU: Risk Factors and Molecular Homology Analysis
Authors Yan G ![]() , Yang Y, Liu L, Yang W, He L, Wang Y, Zhou J, Chen W, Zhang Y, Zhang C, Fu P, Wang C, Lu G
, Yang Y, Liu L, Yang W, He L, Wang Y, Zhou J, Chen W, Zhang Y, Zhang C, Fu P, Wang C, Lu G
Received 20 January 2026
Accepted for publication 8 May 2026
Published 28 May 2026 Volume 2026:19 597676
DOI https://doi.org/10.2147/IDR.S597676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Gangfeng Yan,1,* Yuxia Yang,1,* Ling Liu,1,* Weili Yang,1 Leiyan He,2 Yixue Wang,1 Jinlan Zhou,1 Weiming Chen,1 Yingying Zhang,1 Caiyan Zhang,1 Pan Fu,2 Chuanqing Wang,2 Guoping Lu1
1Department of Pediatric Intensive Care Unit, Children’s Hospital of Fudan University, Shanghai, People’s Republic of China; 2Department of Nosocomial Infection Control, Children’s Hospital of Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guoping Lu, Department of Pediatric Intensive Care Unit, Children’s Hospital of Fudan University, No. 399 Wanyuan Road, Minhang District, Shanghai, 201102, People’s Republic of China, Tel +86 13788904150, Email [email protected] Chuanqing Wang, Department of Nosocomial Infection Control, Children’s Hospital of Fudan University, No. 399 Wanyuan Road, Minhang District, Shanghai, 201102, People’s Republic of China, Tel +86 18017591167, Email [email protected]
Background: Rates of carbapenem-resistant organism (CRO) colonization and infection are rising in pediatric intensive care units (PICUs), mainly due to underlying comorbidities, frequent invasive procedures, prolonged hospitalization, and extensive use of broad-spectrum antibiotics. Colonized patients can act as reservoirs for nosocomial transmission of drug-resistant bacteria, posing a serious threat to other children and healthcare workers. Prevention and control of CRO are therefore of urgent clinical importance.
Methods: Based on active screening measures, we analyzed risk factors for intestinal CRO colonization and subsequent nosocomial infection in critically ill children. Pulsed-field gel electrophoresis (PFGE) was used to determine molecular homology between colonizing and infecting strains isolated from the same patient.
Results: A total of 1069 children were admitted to our PICU between January 2021 and September 2022. Seventy-seven cases of intestinal CRO colonization were detected, with a colonization rate of 7.2%. Of these colonized children, 15 developed subsequent CRO infection, and PFGE confirmed that the infecting strains were homologous to the colonizing ones. Independent risk factors for CRO colonization included underlying neuromuscular disease (OR 7.048, 95% CI 3.003– 16.545, P< 0.001) and longer hospital stay (OR 1.063, 95% CI 1.034– 1.092, P< 0.001). Among colonized children, independent risk factors for subsequent nosocomial infection were carbapenem exposure (OR 4.041, 95% CI 1.310– 12.470, P=0.014), absence of contact isolation (OR 0.033, 95% CI 0.002– 0.496, P=0.010), and longer hospital stay (OR 1.083, 95% CI 1.002– 1.170, P=0.045).
Conclusion: Intestinal CRO colonization significantly increases the risk of subsequent homologous nosocomial infection in PICU children. Rational carbapenem use,aprompt contact isolation following colonization and shorten hospitalization time are crucial strategies to reduce CRO-related nosocomial infections.
Keywords: carbapenem-resistant organisms, intestinal colonization, active screening, homology analysis, nosocomial infections
Introduction
Since the first identification of carbapenem-resistant Enterobacteriaceae (CRE) in 1996, these pathogens have evolved into a formidable global public health threat, entrenched in healthcare settings worldwide due to their extraordinary capacity for transmission and persistence.1 Carbapenem-resistant organisms (CROs) stand as the leading cause of nosocomial infections, conferring prohibitively high mortality rates, prolonged hospital stays, and substantial economic burdens, primarily owing to the dwindling armamentarium of effective therapeutic agents.2–5 Central to the clinical challenge is the observation that CRO colonization—whereby bacteria persist asymptomatically within the host, most commonly the intestinal tract—represents a critical, reversible precursor to subsequent invasive infection.6–8 This process is governed by complex biological interplay: while the intestinal microbiota provides a physical barrier to colonization, dysbiosis induced by broad-spectrum antibiotics, combined with immune compromise, creates an ecological niche enabling CRO expansion, translocation across the mucosal barrier, and the development of clinical disease.9,10
Epidemiologically, the global landscape of CRO is marked by disturbing trends. The widespread and often empiric use of carbapenems has driven a continuous upward trend in CRO prevalence.11 In China, national surveillance data highlights Escherichia coli and Klebsiella pneumoniae as the predominant CRE species, with reported carbapenem resistance rates of 1.5% and 10.1%, respectively.12 More alarmingly, pediatric populations, particularly critically ill children in intensive care units (ICUs), face disproportionately high risks. Their immature immune systems, frequent exposure to invasive procedures, and higher antibiotic exposure frequency render them a vulnerable high-risk group for both colonization and subsequent nosocomial transmission.13
Despite this, a critical research gap persists. While the clinical consequences of CRO are well-documented, fundamental questions regarding the biological drivers of colonization-to-infection transition in the pediatric ICU (PICU) context remain underexplored. Specifically, the specific ecological and immunological factors that tip the balance from asymptomatic carriage to active disease in this unique population are poorly defined. Furthermore, although active CRO screening and isolation precautions have been gradually implemented in adult tertiary hospitals, such strategies are still in their infancy in most pediatric institutions.14 Currently, only a handful of pediatric tertiary care centers conduct routine CRO screening in neonatal ICUs (NICUs) or hematology/oncology wards, and large-scale, prospective studies systematically linking CRO intestinal colonization to subsequent nosocomial infection in PICUs are exceedingly rare.13 This dearth of high-quality epidemiological evidence hinders the development of targeted, evidence-based prevention and control strategies for Chinese children.
To address this gap, our study employed a multifaceted approach. First, we conducted active CRO screening via rectal swabs in a large cohort of PICU patients, leveraging the well-established high sensitivity of this method for CRE detection (49.3%).9,11 Second, we utilized pulsed-field gel electrophoresis (PFGE), a gold-standard molecular typing technique, to perform a rigorous homology analysis of colonizing and subsequent infecting CRO strains isolated from individual patients. This allowed us to definitively establish the clonal relationship between colonization and infection, a key step in confirming the causal link. Finally, we employed rigorous univariate and multivariate regression analyses to systematically identify independent risk factors for both CRO acquisition and the progression from colonization to clinical infection. By integrating these epidemiological, molecular, and clinical dimensions, our study aims to provide in-depth biological insights, fill critical knowledge gaps, and generate actionable evidence to guide the prevention and control of CRO in the PICU.
Materials and Methods
Study Design and Definitions
This was a single-center, cross-sectional, prospective study performed at the pediatric intensive care unit (PICU) of the Children’s Hospital of Fudan University. CRO intestinal colonization screening and CRO surveillance were conducted in all patients who were admitted to the PICU from January 1, 2021, to September 30, 2022. The inclusion criteria included: 1) age between 29 days and 18 years; 2) admitted to PICU with acute onset in one week. The exclusion criteria included: 1) admitted to PICU after surgical operations and was transferred to a general ward; 2) died, discharged, or transferred to a general ward within 48 hours after admission; 3) correction of preterm infants with gestational age less than 38 weeks.
To analyze the risk factors of CRO colonization, we compared the groups of patients with CRO colonization to those whose screening results were negative during the whole time during admission. We determined the candidate range for the non-colonization group based on age, gender, and weight as matching conditions, and randomly selected 77 patients with negative CRO screening results during hospitalization as the non-colonization group using the RANDBEATWEEN function in Microsoft Excel 2018.
To analyze the risk factors of subsequent nosocomial CRO infection, we compared the group of patients with clinical infections to those whose screening results were positive but developed no infection after the CRO colonization. Furthermore, we ran a homological analysis to confirm whether the CRO colonization was the reservoir of the subsequent CRO infection.
CRO Surveillance
Intestinal CRO colonization was screened within 48 hours of admission and monitored weekly throughout hospitalization. For patients with clinical signs of infection, appropriate clinical specimens were collected for bacterial culture and antimicrobial susceptibility testing.Bacterial identification was performed using a Bruker MALDI Biotyper Sirius system (Bruker Daltonics, Bremen, Germany) with the MALDI Biotyper 4.0 software platform. Antimicrobial susceptibility testing (AST) was performed using the bioMérieux VITEK 2 Compact automated system. Interpretation of susceptibility results was performed according to the breakpoints recommended by the CLSI M100-S27 documents (2017 and 2018 editions). All clinical and laboratory data of CRO-positive patients were extracted from electronic medical records by the study authors.
Pulsed-Field Gel Electrophoresis (PFGE)
The concentration of the bacterial suspension was controlled with a bioMérieux DENSIMAT turbidimeter to ensure that its turbidity did not exceed 3.8–4.2. Gel blocks were made by adding 1% Seakem Gold:1% SDS gel to achieve homogeneity. The pellet was digested by cell lysis buffer (CLB) containing proteinase K for 2 h, and then washed twice with purified water to avoid residue of lysate, and washed four times with TE (10 mmol/L Tris:1 mmol/L EDTA, pH 8.0). The lysate was digested by XbaI endonuclease and incubated at 37°C for 4 h. The standard strain H9812 was digested by XbaI. The standard strain H9812 was digested with XbaI. Pulsed-field gel electrophoresis was performed in a CHEF-DRIII (BioRad, CA, USA) electrophoresis apparatus. At the end of electrophoresis, staining was performed with GelRed nucleic acid dye. Gel was imaged in a gel reader and converted to TIFF image format for storage. PFGE images of Salmonella H9812 were processed in BioNumerics (Version 8.1, Applied Maths, Belgium) software and calibrated using a molecular weight standard. Similarity coefficients between each image were calculated using the Dice coefficient, and clustering was performed using the unweighted pair group method with arithmetic mean (UPGMA) to construct a clustering tree. The SD value reflects the degree of similarity between PFGE images of different strains and ranges between 0 and 1, with 0 representing completely different and 1 representing completely the same. Different band patterns were recognized as different types.
Data Collection
The clinical information collected as possible risk factors for CRO intestinal colonization were age, weight, type of primary disease, criticality score, hormone/immunosuppressant use, Carbapenem antibiotic administration, invasive procedures (surgery, catheterization, tracheoscopy, etc), ventilation, duration of hospital stay.
Statistical Methods
Univariable analysis of risk factors was done using χ2/Fisher and unpaired Student’s t-test to identify the risk factors for CRO colonization and subsequent nosocomial infection. Statistically significant risk factors for CRO colonization and infection were considered where P < 0.05. Multivariable logistic regression analysis was performed on statistically significant risk factors for CRO intestinal colonization and infection to identify independent risk factors.
Risk of Bias Assessment
This study adopted a prospective observational nested case-control design, so randomization and blinding of participants or treating clinicians were not applicable. To minimize detection bias, laboratory technicians performing bacterial identification, AST, and PFGE were blinded to patients’ clinical status and group assignment (colonized vs. non-colonized, infection vs. non-infection). Selection bias was reduced by frequency matching of controls to cases by age, gender, and weight, and information bias was minimized by standardized data extraction from electronic medical records by independent investigators.
Results
CRO Intestinal Colonization Incidence
A total of 1069 children were admitted to our PICU between January 1, 2021, and September 30, 2022. Seventy-seven cases of CRO intestinal colonization were identified, with a colonization rate of 7.2%. The isolated strains comprised 38 Escherichia coli, 25 Klebsiella pneumoniae, 10 Acinetobacter baumannii, 2 Stenotrophomonas maltophilia, 1 Pseudomonas aeruginosa, and 1 Enterobacter aerogenes. Of the CRO-colonized patients, 70.1% first tested positive within two weeks after admission, and 77.9% tested positive by the third week. Enrollment flowchart (Figure 1).
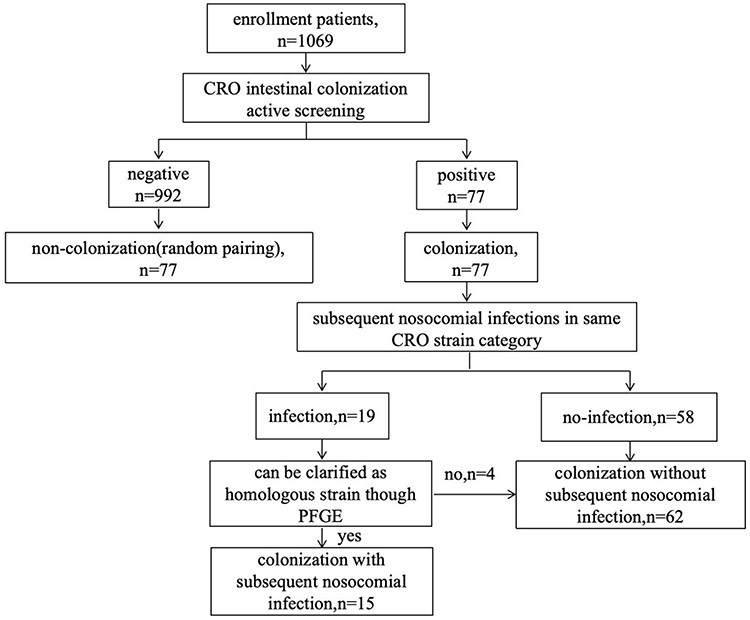 |
Figure 1 Enrollment Flowchart. |
CRO Subsequent Nosocomial Infection Incidence
Of the children with CRO intestinal colonization, 19 developed subsequent clinical infections caused by the same CRO category. PFGE was used to analyze colonization and infection strains from the same patients. Homology analysis confirmed that 15 pairs were of the same strain origin, corresponding to a subsequent nosocomial infection rate of 19.5% (Figures 2 and 3).
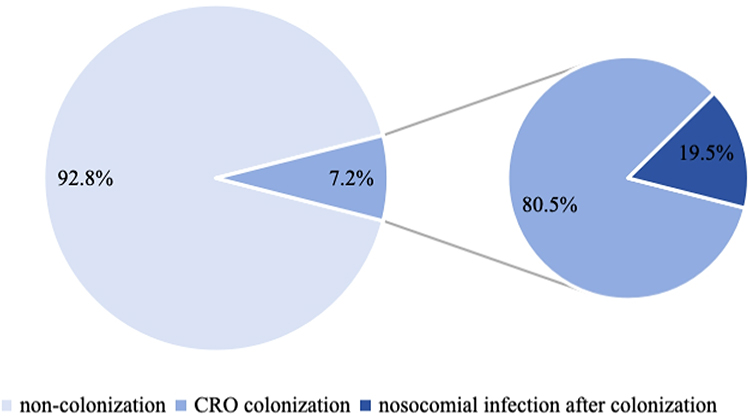 |
Figure 2 Proportion of CRO Intestinal Colonization and Post-colonization Infections Among Children in PICU. |
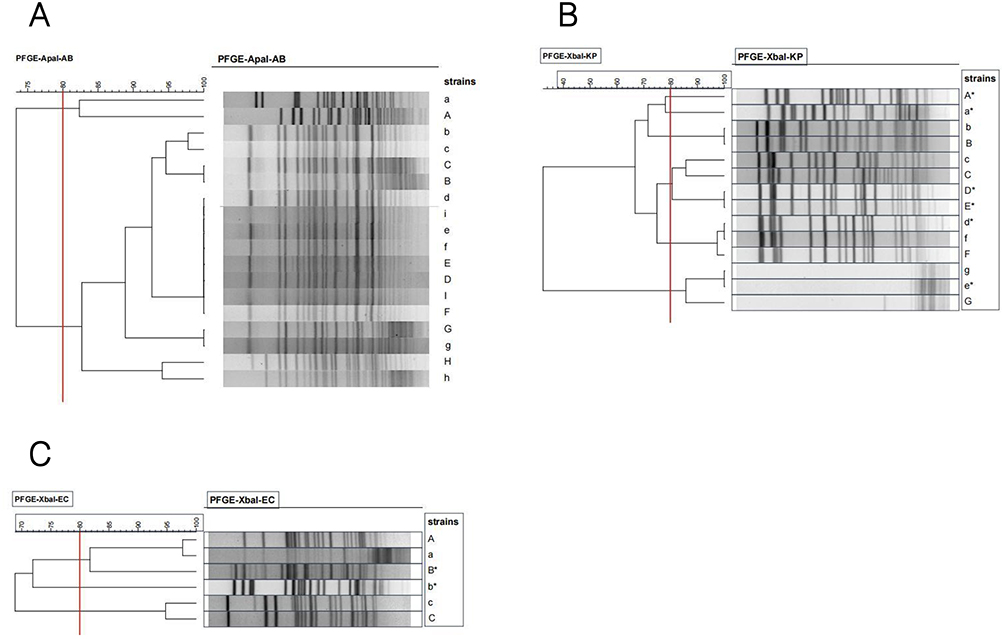 |
Figure 3 PFGE Analysis of Colonization and Infection Strains Isolated from The Same Patients. The upper case letter indicates the intestinal colonizing bacteria, and the lower case letter indicates the CRO strain isolated from the clinical specimen. The upper and lower case of the same letter indicates that both strains originate from the same patient, and the colonizing bacteria and the infecting pathogenic bacteria have a sequential time order, and “*” indicates that the colonizing bacteria from the same patient and the clinical pathogenic bacteria are confirmed to be different typed strains by homology analysis. (A) Acinetobacter baumannii. (B) Klebsiella pneumonia. (C) Escherichia coli. |
In the infection group, 9 cases were Acinetobacter baumannii (Appendix Table 1), 4 were Klebsiella pneumoniae (Appendix Table 2), and 2 were Escherichia coli (Appendix Table 3).
Among these patients, 60.0% first tested positive within two weeks of admission, and 80.0% tested positive by the third week.
Risk Factors of CRO Intestinal Colonization and Subsequent Nosocomial Infection
Clinical data were compared between colonized and non‑colonized children. Univariate analysis showed that neuromuscular underlying diseases, surgery, puncture procedures (including lumbar puncture, thoracentesis, paracentesis, bone marrow aspiration, pericardiocentesis, etc)., invasive procedures such as indwelling catheters or drainage tubes, length of hospital stay, and duration of mechanical ventilation were potential risk factors for CRO intestinal colonization in PICU children (Table 1).
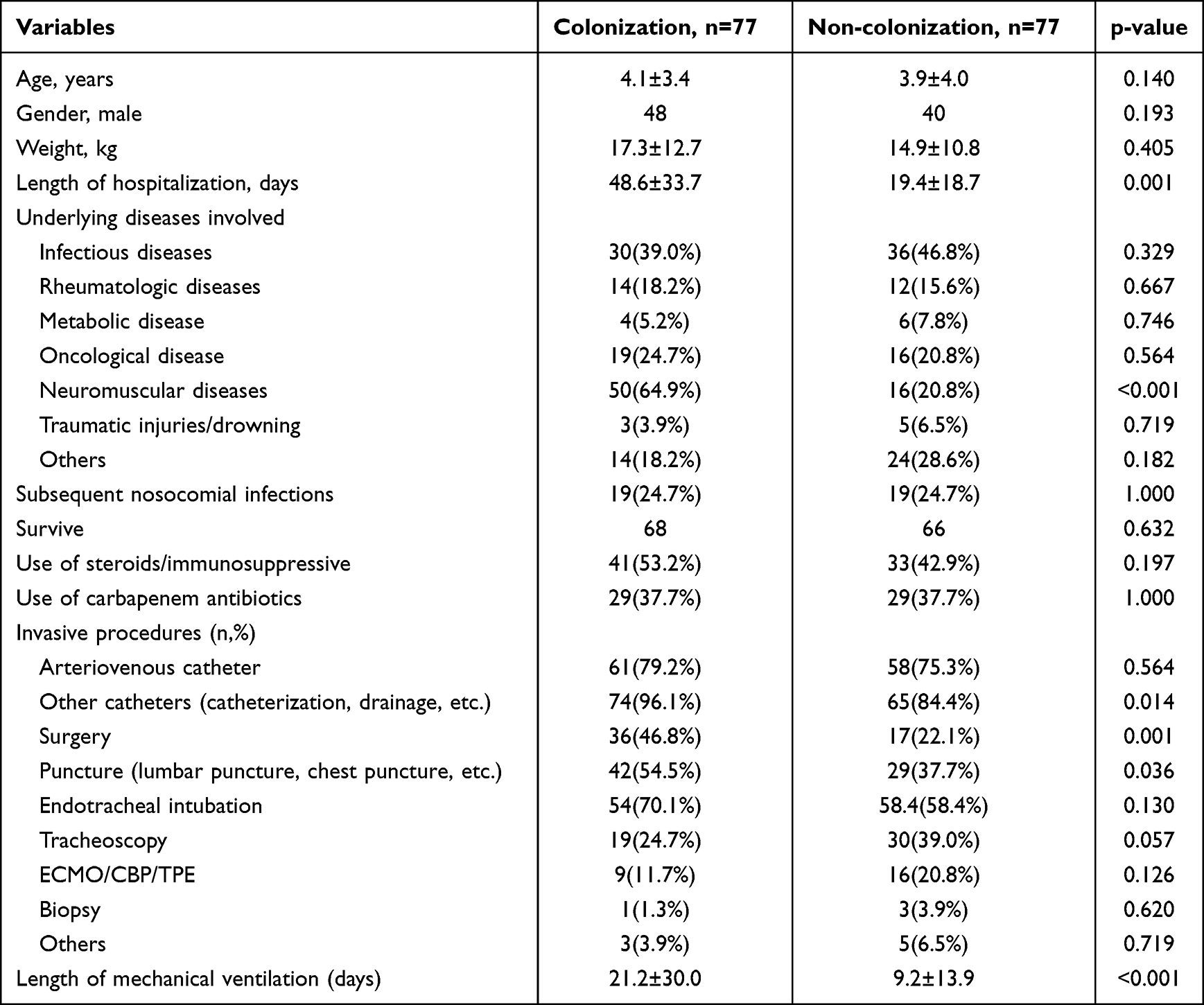 |
Table 1 Results of Single-Factor Analysis of CRO Intestinal Colonization |
Among children with CRO intestinal colonization, use of steroids or immunosuppressive agents, use of carbapenem antibiotics, absence of contact isolation following colonization, age at first CRO screening, length of hospital stay, duration of mechanical ventilation, and concurrent respiratory failure, circulatory failure, or digestive failure were potential risk factors for subsequent CRO infection (Table 2).
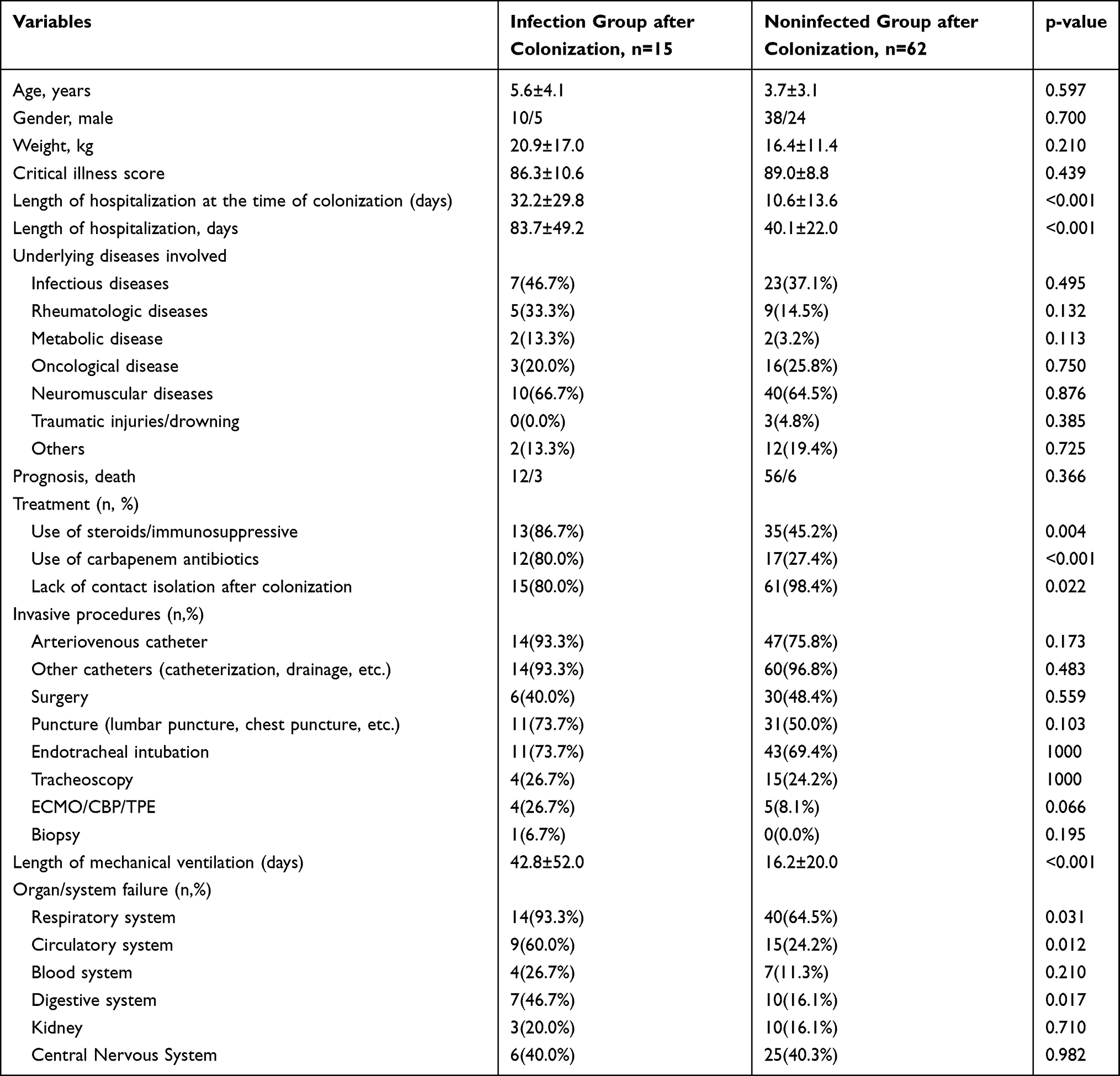 |
Table 2 Results of Single-Factor Analysis of Indicators Related to Nosocomial Infection After CRO Colonization |
Multivariate analysis identified neuromuscular underlying disease and length of hospital stay as independent risk factors for CRO intestinal colonization. In colonized children, use of carbapenem antibiotics, absence of contact isolation after colonization, and length of hospital stay were independent risk factors for subsequent CRO infection (Table 3 and Table 4).
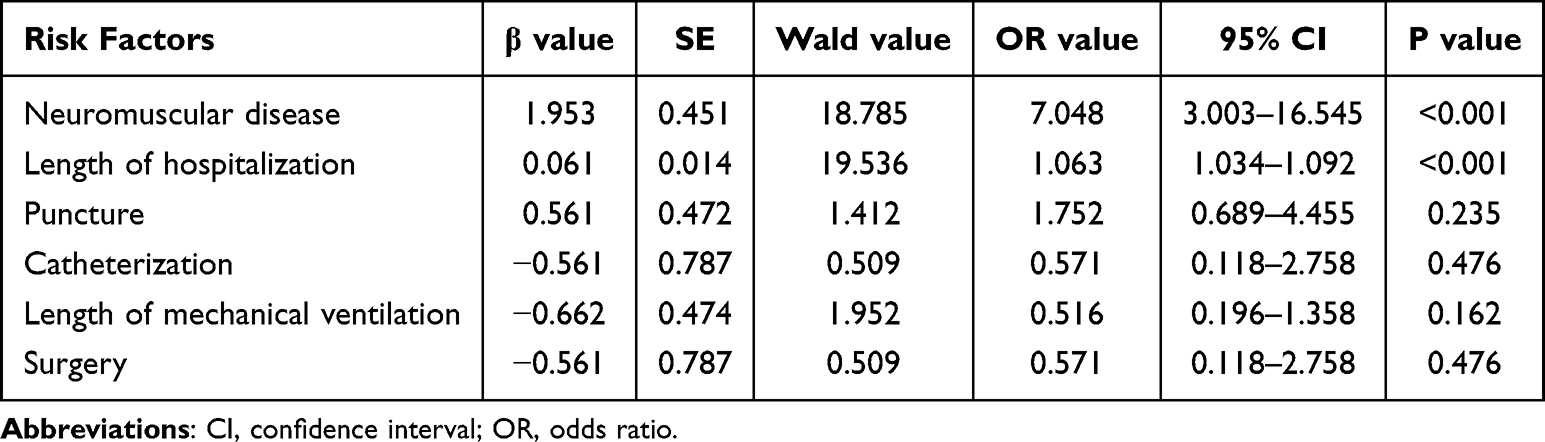 |
Table 3 Results of Multifactorial Analysis of CRO Intestinal Colonization |
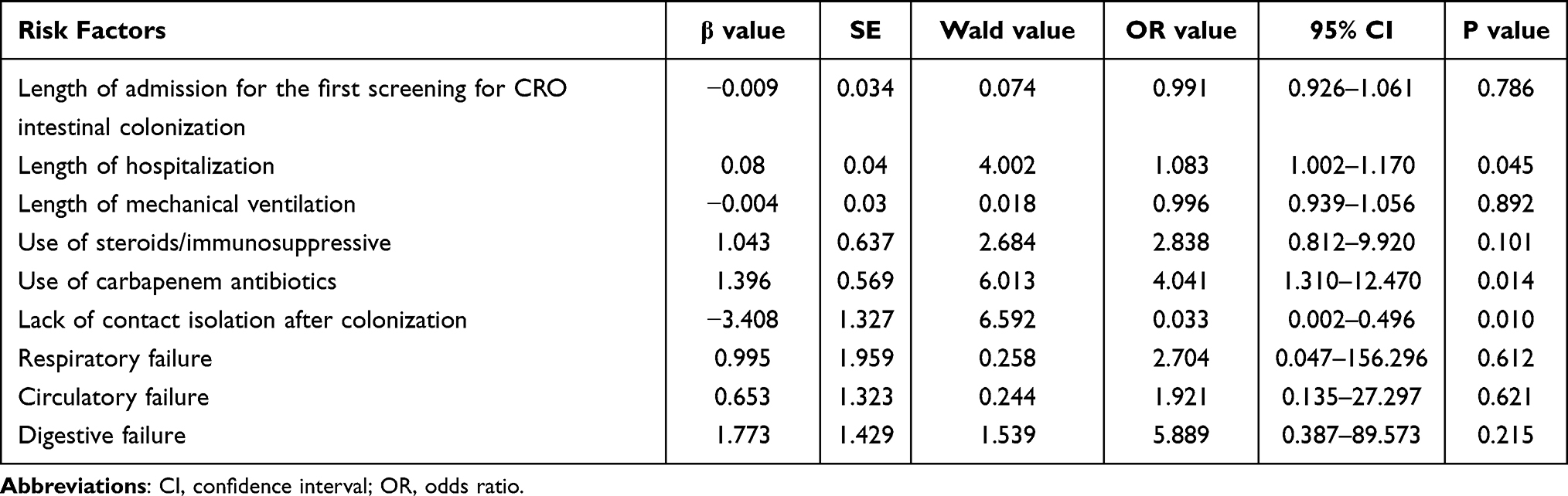 |
Table 4 Results of Multifactorial Analysis of Indicators Related to Nosocomial Infection After CRO Colonization |
Discussion
Effect of Length of Hospitalization on Intestinal Colonization and Subsequent Nosocomial Infection in CRO
In this study, we observed that the proportion of children with CRO intestinal colonization and infection detected increased significantly with the duration of hospitalization. In addition, 70.1% of all children with CRO intestinal colonization were detected for the first time within 2 weeks of hospitalization, making it important to initiate proactive screening within 2 weeks of admission for children at high risk of CRO colonization and infection. In addition, 80.0% of children with CRO intestinal colonization developed subsequent infections within 3 weeks of the first detection of colonized bacteria, so it is important to strengthen the monitoring and management of clinical infections in children with CRO intestinal colonization within 3 weeks.
In the univariate analysis, the differences in length of stay between the colonized and non-colonized groups and between the post-colonization infected and non-infected groups were statistically significant, suggesting that the colonized and infected CRO strains may have originated in the inpatient setting. Children are often treated with different types of broad-spectrum antimicrobials from the time they are admitted to the PICU ward, so the colonized strains in the gut are susceptible to pan-resistance, while CRO strains are more likely to spread epidemically in the ward as the length of stay increases. Irregular disinfection of clinical operations by medical staff and incomplete disinfection of the ward environment are among the causes of CRO colonization and dissemination in the in-hospital environment, and some studies have shown that the incidence of CRO infections in ICU wards can be effectively reduced by strengthening hand hygiene education of medical staff and environmental disinfection measures.15–17 In addition, as the length of stay increases, children receive more invasive operations in the PICU, which may also contribute to the increase in the rate of CRO colonization and infection. In this study, univariate analysis showed that the length of mechanical ventilation was one of the risk factors for increased risk of CRO colonization and infection. Previous literature has reported that risk factors for CRO infections include invasive procedures, but few studies have pointed out the specific effects of different invasive procedures on increasing the risk of CRO infections. Invasive procedures commonly performed in PICU include surgery, tracheal intubation, bronchoscopy, arteriovenous placement, various types of punctures, indwelling catheters or drainage tubes, etc. Most of these invasive procedures involve the reuse of medical devices, such as bronchoscopy, ventilators, etc. Even if this part of the reused equipment is cleaned and disinfected, the disinfection efficacy can be substantially reduced by the formation of bacterial biofilm and will be easily contaminated by various types of bacteria.18–20 In addition, the skin and intestinal barriers of children are less developed than those of adults, so repeated invasive operations or prolonged mechanically assisted ventilation will cause varying degrees of damage to the child, thus increasing the risk of CRO colonization and infection.21,22
Effect of Neuromuscular Diseases on CRO Intestinal Colonization and Subsequent Hospital Infections
Neuromuscular disease was significantly associated with an increased risk of intestinal colonization by carbapenem-resistant organisms (CRO) and subsequent nosocomial infection. Patients with neuromuscular disorders frequently present with impaired swallowing, weakened cough reflex, recurrent aspiration, and impaired gastrointestinal motility, all of which disrupt the normal intestinal flora and compromise intestinal mucosal barrier function. These pathophysiological changes provide favorable conditions for CRO to colonize the intestinal tract. In addition, such patients often require prolonged hospital stays, frequent invasive procedures, including mechanical ventilation, tracheal intubation, and indwelling catheters, as well as long-term use of broad-spectrum antibiotics, especially carbapenems. These factors further promote the selection and overgrowth of resistant strains, increase the risk of exogenous transmission, and facilitate the transition from intestinal colonization to clinical infection. Therefore, neuromuscular disease can be regarded as an important risk factor for CRO intestinal colonization and subsequent nosocomial infection, and patients with such conditions should be prioritized for active screening and enhanced infection control measures.
Impact of Carbapenem Antibiotic Use on Subsequent Nosocomial Infections in CRO
Carbapenem antibiotics have a broad antibacterial spectrum and are outstanding in antibacterial and bactericidal performance, mainly because of their ability to block bacterial cell wall mucopeptide synthase. Drugs such as imipenem, meropenem, and ertapenem, all belong to this type. In the multifactorial analysis of this study, the presence of children with CRO colonization, followed by secondary homologous infection and non-infected children showed a statistically significant difference in the rate of carbapenem antibiotic use between the two groups, suggesting that carbapenem antibiotics induce secondary infectious events in children with CRO intestinal colonization, without the involvement of other factors throughout the process. Previous literature has shown that carbapenem antibiotics increase the resistance rate of pathogenic bacteria and make it easier to develop CRO intestinal invasion when the original intestinal flora balance is disrupted, making a history of carbapenem antibiotic use a high-risk factor for CRO infection.23–25
Timing of Active Screening for CRO Intestinal Colonization
There is no international consensus on the optimal timing and frequency of active screening, and it is common for healthcare institutions to initiate active screening for CRO within 24 hours of new admission and to follow up with those at high risk of infection with regular testing (eg., weekly) during subsequent hospitalization.13,26,27 It is evident that 77.9% of children had their first detection of CRO intestinal colonization within three weeks of admission, and the proportion of CRO intestinal colonization detected by active screening continued to increase with the duration of hospitalization. Therefore, active screening for CRO intestinal colonization within the first 3 weeks of admission is essential for all children admitted to the PICU, and regular screening throughout the hospital stay thereafter is still necessary, but the frequency of screening can be reduced according to the economic conditions of the ward.
Conclusion
Intestinal colonization with CRO may be associated with an increased risk of subsequent CRO-related nosocomial infection in the PICU. Carbapenem antibiotic use, lack of contact isolation following colonization, and longer length of hospitalization were significantly associated with the development of subsequent nosocomial CRO infection. However, given the small number of confirmed homologous infection cases (only 15 cases) and the resulting wide confidence intervals indicating unstable odds ratio estimates, as well as the correlational observational design and potential confounding factors including underlying disease severity, these findings should be interpreted with considerable caution, and further large-scale prospective studies are warranted to verify these relationships.
Ethics Approval
The study protocol was approved by the Ethics Committee of the Children’s Hospital of Fudan University [(2021) 111]. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all parents or legal guardians of the enrolled patients. Assent was obtained from older children where applicable according to institutional guidelines. Attending physicians were informed of the patients’ screening and test results to guide appropriate clinical management and treatment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Shanghai Municipal Science and Technology Major Project (ZD2021CY001), Xiamen Municipal Health Commission Health Science and Technology Program (2025CXA065), National Key R&D Program of China (2021YFC2701800, 2021YFC2701805), National Natural Science Foundation of China (82372168), Natural Science Foundation of Shanghai (23ZR1461600, 25ZR1401032), Shanghai Municipal Health System Key Supporting Discipline Project (2023ZDFC0103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guh AY, Bulens SN, Mu Y. et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in 7 US Communities, 2012-2013. JAMA. 2015;314(14):1479–11. doi:10.1001/jama.2015.12480
2. Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, et al. Predictors of carbapenem-resistant Klebsiella pneumonia acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52(3):1028–1033. doi:10.1128/AAC.01020-07
3. Bratu S, Landman D, Haag R, et al. Rapid spread of carbapenem-resistant Klebsiella pneumonia in New York City: a new threat to our antibiotic armamentarium. Arch Intern Med. 2005;165(12):1430–1435. doi:10.1001/archinte.165.12.1430
4. Bonten MJ, Slaughter S, Ambergen AW, et al. The role of “colonization pressure” in the spread of vancomycin-resistant enterococci: an important infection control variable. Arch Intern Med. 1998;158(10):1127–1132.
5. Peter DM, Edwin VDV, Miranda L, et al. Enterobacter Species in a Pediatric Hospital: horizontal Transfer or Selection in Individual Patients? J Infec Dis. 2001;184(2):211–214. doi:10.1086/322014
6. Dickstein Y, Edelman R, Dror T, et al. Carbapenem-resistant Enterobacteriaceae colonization and infection in critically ill patients: a retrospective matched cohort comparison with non-carriers. J Hosp Infect. 2016;94(1):54–59. doi:10.1016/j.jhin.2016.05.018
7. Giannella M, Bartoletti M, Morelli MC, et al. Risk factors for infection with carbapenem-resistant Klebsiella pneumonia after liver transplantation: the importance of pre-and post-transplant colonization. Am J Transplant. 2015;15(6):1708–1715. doi:10.1111/ajt.13136
8. CDC. Guidance for control of infections with carbapenem-resistant or carbapenemase-producing Enterobacteriaceae in acute care facilities. MMWR Morb Mortal Wkly Rep. 2009;58(10):256–260.
9. Zaidah AR, Mohammad NI, Suraiya S, et al. High burden of carbapenem-resistant Enterobacteriaceae (CRE) fecal carriage at a teaching hospital: cost-effectiveness of screening in a low-resource setting. Antimicrob Resist Infect Control. 2017;6:42. doi:10.1186/s13756-017-0200-5
10. Podschun R, Ullmann U. Klebsiella spp. as nosocomial pathogens: epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin Microbiol Rev. 1998;11(4):589–603. doi:10.1128/CMR.11.4.589
11. Gupta N, Limbage BM, Patel JB, et al. Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention. Clin Infect Dis. 2011;53(1):60–67. doi:10.1093/cid/cir202
12. Zhang FF, Wang XL, Qu HP, et al. Prevalence and genotypes of carbapenemase-producing Enterobacteriaceae. Chin J Infect Chemother. 2024;14:521–525.
13. Yin L, He L, Miao J, et al. Carbapenem-resistant Enterobacteriaceae (CRE) colonization and subsequent infection in a neonatal intensive care unit in Shanghai, China. Infect Prev Pract. 2021;3(3):100147. doi:10.1016/j.infpip.2021.100147
14. Gao S, Yan R, Zhang S, et al. Rectal culture could predict carbapenem-resistant organism bloodstream infection and reduce the mortality in hematological patients: a retrospective cohort study. J Glob Antimicrob Resist. 2024;36:96–104. doi:10.1016/j.jgar.2023.12.007
15. Karampatakis T, Tsergouli K, Losifidis E, et al. Effects of an active surveillance program and enhanced infection control measures on carbapenem-resistant gram-negative bacterial carriage and infections in pediatric intensive care. Microb Drug Resist. 2019;25(9):1347–1356. doi:10.1089/mdr.2019.0061
16. Ho KW, Ng WT, Ip M, et al. Active surveillance of carbapenem-resistant Enterobacteriaceae in intensive care units: is it cost-effective in a nonendemic region? Am J Infect Control. 2016;44(4):394–399. doi:10.1016/j.ajic.2015.10.026
17. Martin ET, Tansek R, Collins V, et al. The carbapenem-resistant Enterobacteriaceae score: a bedside score to rule out infection with carbapenem-resistant Enterobacteriaceae among hospitalized patients. Am J Infect Control. 2013;41(2):180–182. doi:10.1016/j.ajic.2012.02.036
18. Huang J, Chen EZ, Qu HP, et al. Sources of multidrug-resistant Acinetobacter baumannii and its role in respiratory tract colonization and nosocomial pneumonia in intensive care unit patients. Chin Med J. 2013;126(10):1826–1831. doi:10.3760/cma.j.issn.0366-6999.20122358
19. Barnes SL, Morgan DJ, Harris AD, et al. Preventing the transmission of multidrug-resistant organisms: modeling the relative importance of hand hygiene and environmental cleaning interventions. Infec Control Hosp Epidemiol. 2014;35(9):1156–1162. doi:10.1086/677632
20. Mataseje LF, Bryce E, Roscoe D, et al. Carbapenem-resistant gram-negative bacilli in Canada 2009-10: results from the Canadian Nosocomial Infection Surveillance Program (CNISP). J Antimicrob Chemother. 2012;67(6):1359–1367. doi:10.1093/jac/dks046
21. Aguilera-Alonso D, Escosa-García L, Saavedra-Lozano J, et al. Carbapenem-resistant gram-negative infections in children. Antimicrob Agents Chemother. 2020;64(3):e02183–19. doi:10.1128/AAC.02183-19
22. Kapoor K, Jain S, Jajoo M, et al. Risk factors and predictors of mortality in critically ill children with extensively-drug resistant Acinetobacter baumannii infection in a pediatric intensive care unit. Iran J Pediatr. 2014;24(5):569–574.
23. Chiotos K, Tamma PD, Flett KB, et al. Multicenter study of risk factors for colonization or infection with carbapenem-resistant enterobacteriaceae in children: a multicenter study. Antimicrob Agents Chemother. 2017;61(12):e01440–17. doi:10.1128/AAC.01440-17
24. Borer A, Saidel-Odes L, Eskira S, et al. Risk factors for developing clinical infection with carbapenem-resistant Klebsiella pneumonia in hospital patients initially only colonized with carbapenem-resistant K pneumonia. Am J Infect Control. 2012;40(5):421–425. doi:10.1016/j.ajic.2011.05.022
25. Hsu AJ, Tamma PD. Treatment of multidrug-resistant gram-negative infections in children. Clin Infect Dis. 2014;58(10):1439–1448. doi:10.1093/cid/ciu069
26. Richter SS, Marchaim D. Screening for carbapenem-resistant Enterobacteriaceae: who, when, and how? Virulence. 2017;8(4):417–426. doi:10.1080/21505594.2016.1255381
27. Yin L, He L, Miao J, et al. Active surveillance and appropriate patient placement in contact isolation dramatically decreased carbapenem-resistant Enterobacterales infection and colonization in pediatric patients in China. J Hosp Infect. 2020;31(S0195–6701(20)30130–4).
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.