Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 13
Interventions to Improve Quality of Life in Multiple Sclerosis: New Opportunities and Key Talking Points
Authors Faraclas E ![]()
Received 20 May 2023
Accepted for publication 5 September 2023
Published 19 September 2023 Volume 2023:13 Pages 55—68
DOI https://doi.org/10.2147/DNND.S395733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Müller
Erin Faraclas
Physical Therapy Department, Johnson & Wales University, Providence, RI, USA
Correspondence: Erin Faraclas, DPT. PhD, MSCS, Physical Therapy Department, Johnson & Wales University, Providence, RI, USA, 8 Abbott Park Place, Providence, RI, 02903, USA, Tel +1 413-896-5686, Email [email protected]
Background: Today, living well with multiple sclerosis (MS) is often measured by a person’s overall quality of life rather than being limited to the more traditional metrics of reduced frequency of relapses or progression of disability. This change in focus, to a more holistic view of health, such as overall quality of life, has shifted the views of what both providers and people with multiple sclerosis view as essential for living well with MS.
Purpose: This narrative review aims to examine the relevant literature on existing and emerging non-pharmacological interventions shown to improve the quality of life for people with multiple sclerosis across all health domains.
Methods: A literature search was conducted on MEDLINE, CINAHL, and Scopus electronic databases using the following search terms: quality of life, health-related quality of life, life quality, life satisfaction, non-pharmacological intervention, non-drug, and intervention. After screening the abstracts, 24 were selected for this review.
Results: Common non-pharmacological interventions were used for fatigue and sleep, mental and emotional health, cognition, physical health, and chronic pain. Several non-pharmacological interventions included in this review positively improved the overall quality of life for people with multiple sclerosis. These interventions included exercise, cognitive behavior therapy, and cognitive rehabilitation.
Conclusion: Non-pharmacological interventions such as exercise and cognitive behavioral therapy improve the quality of life for people with MS. These interventions should be prescribed more during routine medical care. Translating this research into standard clinical practice should be one area of focus. In addition, higher quality studies, such as randomized control trials, need to be conducted on emerging nonpharmacological interventions to assess effectiveness.
Keywords: multiple sclerosis, quality of life, health and wellness, health-related quality of life
Introduction
Multiple sclerosis (MS) is a progressive neurodegenerative autoimmune disease characterized by demyelination and axonal loss throughout the central nervous system. This demyelination causes motor, cognitive, and sensory impairments of varying levels of severity.1 Most individuals are diagnosed between the ages of 20 and 50, making MS the most common non-traumatic neurological disease affecting young adults in the United States, with an estimated one million individuals living with MS nationwide.2–6 MS’s annual costs in the US are in the seven to twelve-billion-dollar range.7
It is established in the literature that people with MS (pwMS) have a lower quality of life (QOL) than the general population.8–10 This is due to the myriad of symptoms pwMS encounter, such as; visual changes, weakness, spasticity, paresthesia, impaired proprioception, balance difficulties, pain, fatigue, bladder/bowel changes, and cognitive impairments, among others.11–14 Health-related quality of life is a multi-dimensional construct that includes physical, mental, emotional, and social health.11,15,16 Health-related quality of life is notably also lower in pwMS than population norms.
The increased attention to health-related quality of life has facilitated a notable shift in the views of what both providers and pwMS view as living well with MS.17–19 In 2018, after exploring the traffic coming onto the National MS Society’s website and noticing that individuals were going to the website for health and wellness strategies, the National MS Society formed a wellness research group to foster research promoting optimal health for pwMS. Today living well with MS is measured not just by an absence of relapses or progression of disability but rather by the measure of a person’s overall quality of life living with MS.12,20,21
Numerous studies of varied rigor have aimed to measure the influence of non-pharmacological interventions on quality of life or health-related quality of life for pwMS.22–27 Non-pharmacological interventions include physical activity, dietary changes, psychosocial support, cognitive behavioral therapy, exercise, and fatigue management. This narrative review presents relevant literature on existing and emerging non-pharmacological interventions that positively influence the quality of life for pwMS across different dimensions of health throughout the disability spectrum.
Methods
Data Sources and Search Strategy
A literature search was conducted on MEDLINE, CINAHL, and Scopus electronic databases using the following search terms: quality of life, health-related quality of life, life quality, life satisfaction, non-pharmacological intervention, intervention, and non-drug (Figure 1). Additional search parameters included publication within the last five years (2017–2023) and available in English. MEDLINE retrieved 16 studies, CINAHL 4, and Scopus 40. Duplicate titles, 18, were removed. The remaining abstracts were screened to determine if the articles were related to non-pharmacological interventions to improve the quality of life in pwMS (Table 1). After screening the abstracts for inclusion criteria, 24 were deemed appropriate for this review.
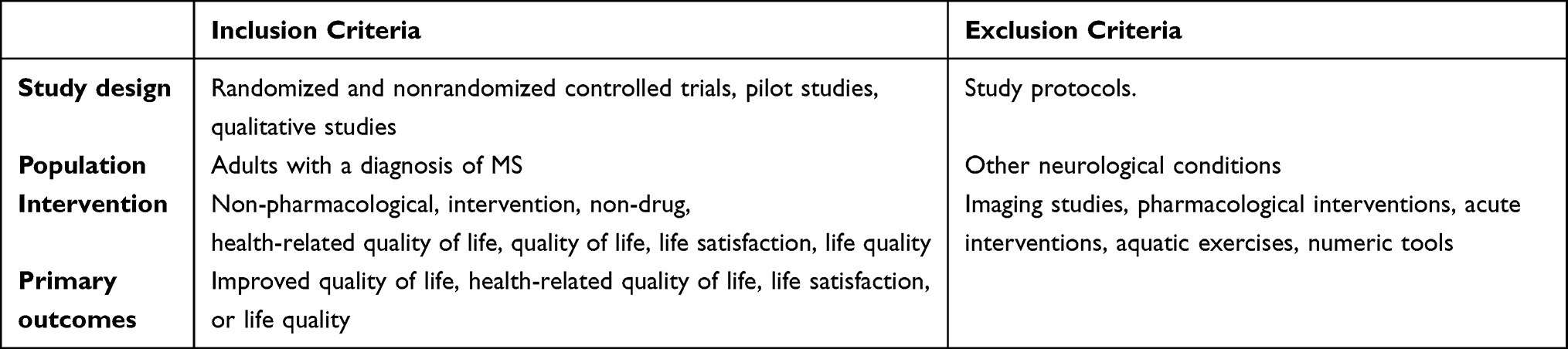 |
Table 1 Inclusion Criteria |
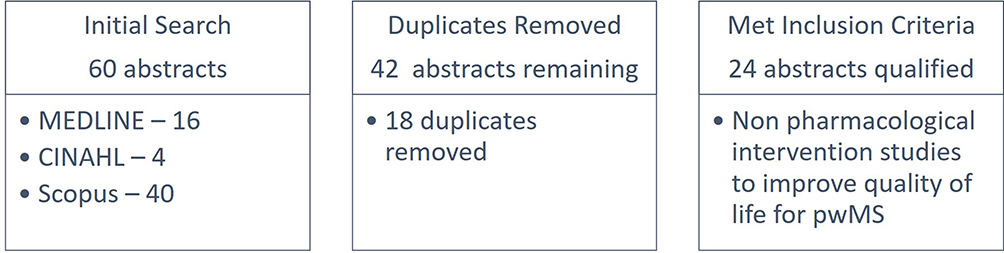 |
Figure 1 Search Strategy. |
Data Extraction and Analysis
Randomized and non-randomized control trials, quasi-experimental, comparison, qualitative, and pilot studies were included. This review also included nonpharmacological intervention studies with future use prospects. All articles were reviewed by the principal investigator and categorized into common themes related to symptoms reported by pwMS. The common themes included; fatigue and sleep, mental and emotional health, cognition, physical health, and chronic pain. Once all articles were categorized into broad themes, each article within a theme was reviewed for its level of evidence, methodological quality, and effectiveness at improving quality of life using the PEDdro Scale or a scale more appropriate for the type of study.28 Each theme then summarized the available for this review (Table 2).
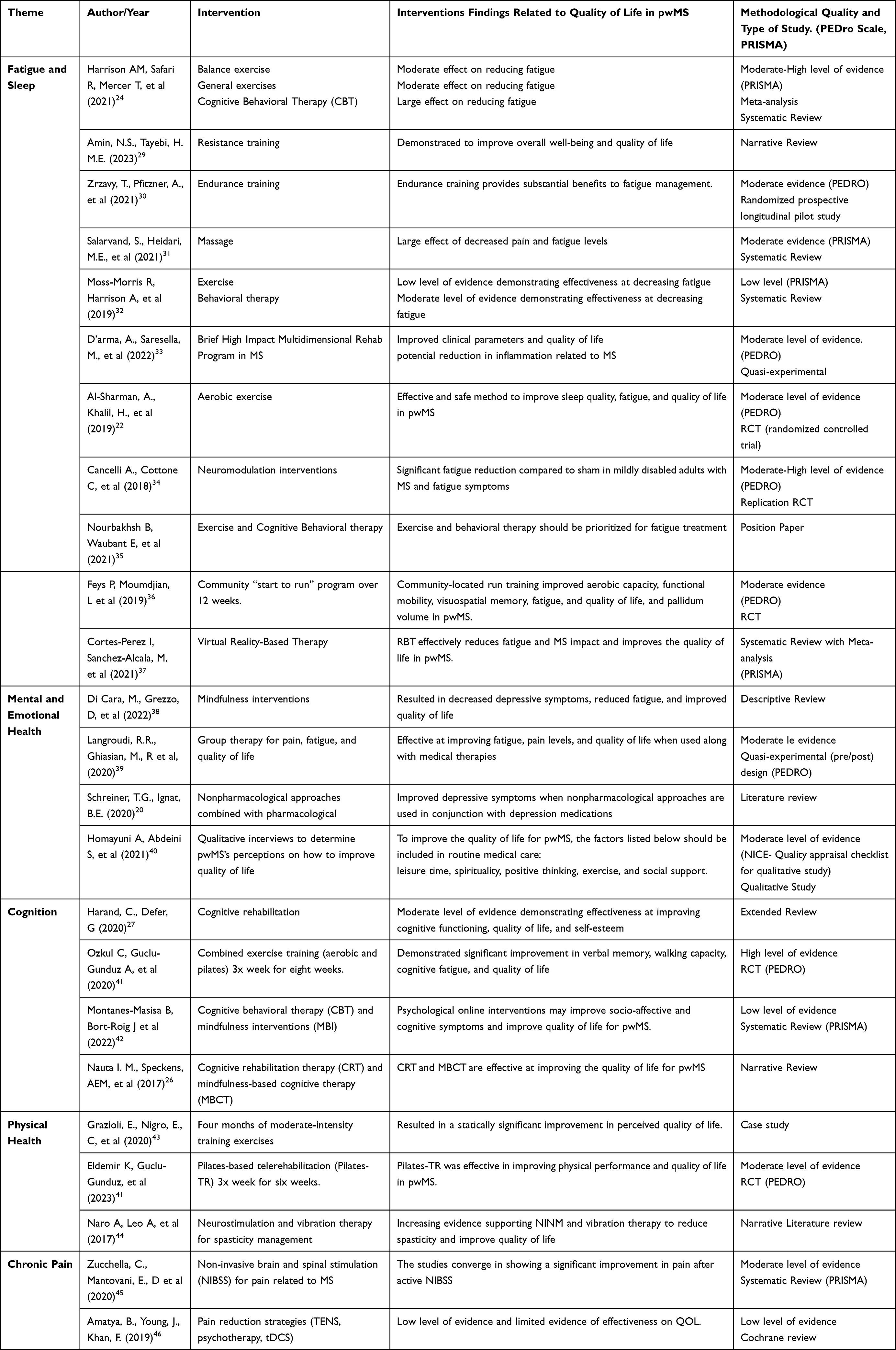 |
Table 2 Summary of Evidence Organized by Theme |
Results
Fatigue
Fatigue affects 80% or more of pwMS, and often fatigue directly impacts a person’s overall quality of life.30,47,48 Fatigue is commonly associated with a lower quality of life, even when researchers control for MS disease severity in their studies.24 Routine fatigue is one of the primary reasons for pwMS to leave the workforce and go on disability services.49 Over the last twenty years, numerous RTCs, quasi-experimental, and other types of research have focused on non-pharmacological interventions, like exercise and cognitive behavioral therapy (CBT), as fatigue management strategies.22,24,25,30,50,51 Literature within the last five years has experienced an increase in the number of studies on non-pharmacological interventions and quality of life. Modifiable lifestyle factors have been explored as a means to improve fatigue management and other MS-oriented outcomes.19,31,39
Exercise is an evidence-based intervention with significant evidence demonstrating exercise as an effective strategy to improve quality of life, mobility, and fatigue for pwMS.18,23,52–54 For this review, ten articles meeting the inclusion criteria focused on fatigue reduction and overall quality of life. Of these ten articles, eight centered on exercise as a highly effective intervention for managing fatigue and overall quality of life for pwMS. The remaining three articles investigated massage therapy, neuromodulation, and virtual reality-based therapy as possible interventions to improve fatigue and overall quality of life. CBT was included in two of the exercise articles focused on fatigue management.
Weakness, impaired balance, limited mobility, decreased physical activity, and overall deconditioning contribute to fatigue-related symptoms for pwMS.29 Limited physical activity can cause fatigue levels to increase, further limiting mobility, and the cycle persists indefinitely. Exercise or routine physical activity can break the cycle and is often a primary intervention to maintain or restore aerobic fitness, strength, balance, mobility, and fatigue.29,54,55 Although medication for fatigue management is routinely prescribed, there is a lack of evidence demonstrating a drug’s effectiveness in controlling MS-related fatigue.56,57 There are non-pharmacological interventions with recent and notable evidence demonstrating effectiveness with fatigue management through exercise, CBT, massage, and neuromodulation therapies.22,24,29–37
Intervention studies in this review included three RCTs, one quasi-experimental trial, and a randomized prospective longitudinal pilot study. Four studies specifically looked at some form of exercise and its impact on fatigue and overall quality of life.22,30,33,36 A RCT performed by Feys B et al investigated the effects of a remotely supervised 12-week community “start-to-run” program on fatigue levels, quality of life, and cognitive function.36 The authors reported a large effect on decreasing fatigue, improving quality of life, and improving memory at 8 and 12 weeks post-program.
An RCT by d’Arma et al looked at the effects of a 12-week personalized training program, the brief high-impact multidimensional rehabilitation program (b-HIPE), on quality of life, aerobic capacity, and fatigue levels on pwMS compared to standard of care.33 The b-HIPE program includes physical therapy, mindfulness, and promoting other healthy lifestyle behaviors. Clinical parameters measured beta-endorphin and catecholamines concentrations pre-and post-participation in the b-HIPE program because of the relationship between these hormones and the immune system in neurodegenerative diseases like MS. The physical therapy intervention focused on aerobic exercise and strength training. The results demonstrated that after the b-HIPE program, clinical parameters and quality of life were improved.33 All study participants in this RTC experienced significant gains in quality of life and improved fatigue levels.
Another randomized prospective pilot study comparing the effects of endurance training under hypoxic and normoxic conditions on fatigue, mobility, and spasticity in pwMS reported that endurance training under hypoxic or normoxic conditions substantially benefits individuals in neurological rehabilitation programs.30 Endurance training under hypoxic conditions influenced walking endurance more than in normoxic conditions. This intervention needs further research with high-level evidence to determine its effectiveness and safety in improving fatigue and mobility. This study does demonstrate that physical activity and endurance training is clinically meaningful when measuring the quality of life for pwMS. More information on this modality and similar innovations can be expected in the future.58
Sleep disorders are common in MS and are regularly associated with fatigue, depression, pain, and a decreased quality of life.22 Sleep is vital for memory consolidation, motor learning, and cognitive function, which are critical to the quality of life for pwMS.22 A recent RCT explored the effects of a six-week moderate-intensity aerobic exercise program on sleep and fatigue levels in pwMS.22 Participants were randomly allocated to either a moderate-intensity aerobic exercise program (MAE, n=20) or a home exercise program (HEP, n=20). Participants were assessed several times throughout the study. Compared to the HEP group, people with MS who participated in moderate-intensity aerobic exercise experienced significant improvements in sleep and quality, ultimately improving fatigue.22
This study’s systematic reviews, narratives, and positional paper all appeared to echo the findings of the above RCTs. Exercise and physical activity clinically improve fatigue levels and overall quality of life for pwMS.24,29,32,35,37 A systematic review with a meta-analysis recently reported that balance exercises and general exercises have a moderate effect on reducing fatigue in pwMS.24 In the same study, cognitive behavioral therapy (CBT) was said to have a large effect on reducing fatigue24 Amin, N. et al, in a 2023 narrative review on resistance training, reported that overall well-being and quality of life increases when pwMS engage in resistance training, again demonstrating the benefits of exercise.29 One position paper summed up the evidence by concluding that exercise and cognitive behavioral therapy should be prioritized for fatigue treatment in all pwMS.35
There is a notable lag in translating this large body of evidence on exercise and quality of life into clinical practice. Discussing exercise, cognitive behavioral therapy, and physical therapy are often topics not discussed during routine healthcare visits for pwMS.59 Integrating exercise prescription into routine medical care is where attention needs to be focused on now.
Mental and Emotional Health
Depression and mental health concerns occur in over half of pwMS.20,60 Depression is the most common psychiatric disorder in pwMS, with rates of depression overall increased for pwMS compared to the general population.9,60,61 Anxiety is three times more prevalent in the MS population than in the general population.62 Suicidal ideation and suicide are two times higher in pwMS than in the general population.62–64 These statistics establish the need for more attention and access to mental and emotional healthcare for pwMS. Mental and emotional health influences the quality of life for all people, especially those with MS.27,38 Evidence has been growing, and four studies in this search are related to nonpharmacological treatments for mental and emotional health. In the last five years, more research studies have explored lifestyle behaviors and emotional health as effective non-pharmacological interventions for improving depression in pwMS.20,21,60 Despite these numbers, pwMS report receiving little or no treatment for their mental or emotional health.27
A recent descriptive review on mindfulness and its impact on depressive symptoms and overall quality of life concluded that mindfulness interventions could decrease depressive symptoms and fatigue levels while increasing the quality of life for pwMS.38 The review noted that mindfulness, cognitive behavioral therapy (CBT), and other similar strategies effectively improve the mental and emotional health of pwMS.38 CBT, a non-pharmacological intervention, has accumulated a moderate amount of evidence demonstrating its effectiveness at improving depression symptoms, difficulty sleeping, and anxiety in pwMS effectively.24,65
For this review, two intervention studies assessed if a more significant improvement in mental health occurred when medical therapies were combined with nonpharmacological interventions compared to medical therapies alone. One quasi-experimental study paired group therapy sessions with medical therapies for improving mental health.39 The sample of participants that participated in both medical therapy and group therapy had a significantly greater improvement in mental health, fatigue levels, and quality of life compared to participants only receiving medical therapies.39 The other study examined CBT and mindfulness strategies as nonpharmacological interventions. The authors came to the same conclusion as the group therapy study, non-pharmacological interventions like CBT combined with medical therapies versus medical therapies alone improve fatigue levels, sleep quality, and quality of life.20
Cognition
Nonpharmacological intervention studies to treat cognitive impairments include a fair amount of evidence strongly suggesting nonpharmacological interventions like CBT, mindfulness, and exercise are effective for treating cognitive impairments. More than 50% of pwMS report cognitive impairments that they perceive as impacting their abilities to complete activities of daily living (ADLs) and overall quality of life.26,27 Common cognitive impairments include difficulty with information processing, memory, visuospatial processing, executive function, and learning ability.66–68 These cognitive changes can impact an individual’s quality of life, such as job loss, reduced social interaction, and diminished independence. According to McNicholas et al,68 cognitive impairments contribute more than physical impairments to withdrawal from the workplace for pwMS.68,69 Notably, only 55% of pwMS are employed seven years out from initial diagnosis.68
It is vital to note that cognitive impairments often do not correlate with disease duration and appear to surface at any time throughout the disease course.70 Recent evidence suggests cognitive impairments can begin very early in the disease course and can be present with or without physical impairments.11,70 Despite the high prevalence of cognitive impairments, these symptoms appear to be detected less than the more “visible” physical impairments.68 The connection between cognitive impairments and quality of life in the MS population has yet to be fully developed in the existing body of literature; however, what is available indicates that identifying and treating cognitive impairments in pwMS will positively impact quality of life.27
Nonpharmacological intervention studies for cognitive impairments have focused on three primary strategies, cognitive behavioral therapy (CBT), mindfulness, and physical exercise. For this review, four articles meeting the inclusion criteria are about cognition and quality of life.26,27,41,42 One extended review examined the effectiveness of psychosocial interventions for improving health-related quality of life and fatigue for pwMS.27 After a comprehensive review of evidence published in 2020, the authors concluded that CBT, mindfulness, and physical exercise were effective and appropriate cognitive strategies to improve the quality of life for pwMS.27
A dual-center, single-blind randomized control trial completed in 2023 on cognitive rehabilitation therapy (CRT) and mindfulness-based cognitive therapy (MBCT) concluded these therapies to be highly effective interventions for treating cognitive impairments and improving quality of life for pwMS.26 Cognitive rehabilitation focuses on restorative and compensatory strategies to improve cognitive function. However, this study notes that cognitive rehabilitation therapies’ benefits may not persist after six months.26 These results suggest ongoing treatment may sometimes be required for some cognitive impairments.
Mindfulness is a form of meditation focusing on awareness and attention to the present moment.26 Mindfulness as a strategy to improve an individual’s quality of life often appears in the literature when searching for interventions to enhance quality of life for pwMS. In this review, two articles specifically explored mindfulness as a strategy to improve cognitive function and quality of life.26,42 Montanes-Masisa et al published a systematic review on cognitive behavioral therapy and mindfulness as interventions for cognitive impairments and quality of life. The systematic review had a relatively low amount and quality of available evidence. The authors indicated that psychological online interventions may improve socio-affective health, cognitive dysfunction, and quality of life for pwMS.42 Although the evidence is still evolving, and notably, there is not enough high-quality evidence to support psychological online interventions as effective, the available evidence is promising, and higher quality studies are needed to draw conclusions.
Physical Health
A large body of evidence supports exercise and physical activity as effective non-pharmacological interventions to improve quality of life, cognition, functional mobility, and psychosocial well-being in pwMS.18,23,25,32,41 In 2019, Dalgas et al made a compelling evidence-based argument demonstrating that initiating an exercise program at the time of diagnosis is optimal for treating the many symptoms of MS before they occur. The authors also found that exercise may act as a disease-modifying intervention by providing neuroprotective effects.18 These findings suggest that exercise can also be considered a secondary prevention strategy.18 High quality research on exercise as a disease-modifying intervention is significantly limited. Additional evidence is needed to draw clear conclusions about using exercise as a neuroprotective prevention strategy for pwMS. The type of research requires significant time as the primary outcome is minimal disease progression over the course of MS.18,54,71 It is also important to note that exercise training doesn’t appear to cause an increase in the risk or rate of MS relapses or adverse events throughout the disease course.72,73
For this review, three articles specifically looked at exercise as an intervention to improve physical health and quality of life for pwMS.43,44,74 An additional ten studies looked at exercise as positively impacting pwMS; these ten studies have already been discussed in the previous sections of this review. All studies for this review indicated exercise was effective at improving either fatigue, physical health, cognition, quality of life, or a combination of the four.24,32,41
One case study explored exercise as an intervention to improve functional (physical), cognitive, and psychological health parameters for pwMS, associated with increased quality of life and decreased disease severity.43 This case study aimed to evaluate the effects of a four-month training program at moderate intensity [65% heart rate reserve (HRR)] on BMI, adiponectin, and quality of life in a person with secondary progressive MS.43 The parameters were evaluated before participating in the program, at the end of the program, and then six months after the end of training. The authors found a slight reduction in BMI, improved perceived quality of life, a reduced expression of total adiponectin, and decreased MS disability level as measured by an expanded disability status scale (EDSS).43 Despite the limitations of a case study, this study provides the foundation for future studies to explore exercise more.
Neurostimulation and vibration therapy for spasticity management in pwMS has recently appeared in the literature. In a narrative review by Naro et al, the authors explored neurostimulation and vibration as an intervention for spasticity management and quality of life.44 The authors presented compelling evidence supporting noninvasive neurostimulation (NINM) and vibration therapy as appropriate interventions for spasticity and improving physical performance. NINM and vibration therapy’s impact on the quality of life for pwMS showed similar results.44
The last study for this review on physical function was an RCT that explored Pilates-based telerehabilitation. This study aimed to assess if a telerehabilitation Pilates program delivered 3x a week for six weeks was an effective intervention to decrease spasticity, improve physical performance, and improve the quality of life for pwMS.74 This Pilates intervention was completed via telerehabilitation, an alternative setting for Pilates-based therapy. The authors concluded that a telerehabilitation-based Pilates program effectively decreases spasticity and improves physical performance and quality of life.74 Walking speed, muscle strength, balance, core endurance, and fatigue measures showed statistically significant improvements.
Pain
Neuropathic and nociceptive pain frequently affect people with multiple sclerosis, with a prevalence of close to 90%.46 Pain can influence the general health and overall quality of life of a pwMS. Pharmacological strategies are widely used to treat pain in MS; however, the efficacy of many of these drugs and their side effects often leaves pwMS seeking non-pharmacological interventions. Determining the best non-pharmacological intervention to treat chronic pain is challenging because many studies are of low quality and rigor.
Some examples of pain interventions include transcutaneous electrical nerve stimulation (TENS), psychotherapy (telephone, self-management, hypnosis, and electroencephalogram (EEG) biofeedback), transcranial random noise stimulation (tRNS), transcranial direct stimulation (tDCS), hydrotherapy and reflexology.46 A 2019 Cochrane review on pain reduction strategies using TENS, psychotherapy, and DCS found minimal evidence existed on these pain interventions, and what was available was mostly low-level evidence.46 It is still unclear if these pain modalities influence the quality of life for pwMS.
In addition to the study above, this review’s search yielded a recent systematic review investigating the evidence of non-invasive brain and spinal stimulation (NIBSS) for pain management for pwMS.45 The evidence on NIBSS is at a moderate level, indicating NIBSS is potentially beneficial for pain reduction in pwMS and should be considered as an emerging non-pharmacological intervention for pain control.45 No clear conclusions can be drawn until more evidence, such as an RCT comparing NIBSS to the standard of care, becomes available.
Discussion
The World Health Organization defines quality of life as “an individual’s perception of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns”.75 This narrative review aimed to examine the literature published in the last five years related to existing and emerging non-pharmacological interventions that demonstrate effectiveness at improving the quality of life for pwMS. This review included various studies and reviews, including RCTs, quasi-experimental studies, systematic reviews, meta-analyses, and qualitative studies to meet this review’s aim. There is variability in how each study was assessed for quality and methodological rigor due to the different types of studies included in this review. This method ensured that all new literature on nonpharmacological intervention studies and reviews for MS having quality of life as a primary outcome was included.
Different quality-of-life tools were used to measure the quality of life for pwMS in the studies for this review. Some tools used were general quality of life scales that can be used on individuals with or without MS, while other studies used MS-specific tools to measure quality of life. This variability in quality of life measurement is a limitation of this review. It is important to note that a single quality-of-life assessment tool has yet to be agreed upon as the gold standard for pwMS. However, all studies in this review indicated that physical, mental, and social aspects of life must be a part of any quality-of-life assessment used with the MS population.76–78 Notably, not all studies in this review had all of these aspects encompassed in the quality of life tool used. Many studies used multiple tools or scales to look at overall quality of life in pwMS.
The non-pharmacological intervention with the most amount of evidence was exercise. Exercise was overwhelmingly shown to reduce fatigue and facilitate improved sleep quality, which are necessary for pwMS to have an overall good quality of life. Exercise was recommended routinely as a non-pharmacological intervention to treat physical, balance, and cognitive impairments. None of the articles in this review reported any adverse events occurring during their respective studies.
According to the literature for this study, exercise is beneficial and should be prescribed; failure to do so goes against the best available evidence. Exercise was shown to be an appropriate intervention to prescribe to pwMS to improve overall quality of life by decreasing fatigue, improving cognition, and enhancing physical strength. The finding from this review is in congruence with past studies.18,54,79–81 Guidance from a physical therapist or another trained professional is highly recommended to ensure safety when pwMS are starting any exercise plan.18,25,52 Past and present evidence demonstrates that exercise should be essential to a healthcare plan for pwMS. The literature in this review included varied forms of exercise such as resistance training, aerobic exercise, endurance training, Pilates, balance activities, and virtual reality. In addition, the safety profile of exercise in the MS population is especially good. Regardless of the specific exercise or study type in this review, the benefits of exercise were all similarly positive and successfully demonstrated exercise as a highly effective intervention to improve quality of life in pwMS.22,33,41
Exercise is a safe and effective intervention to manage many symptoms of MS and specifically to improve the overall quality of life for pwMS. Given the consistent evidence supporting exercise, it is hard to understand why exercise is often not discussed or under-emphasized during routine medical care visits. Focusing on translating this evidence into standard clinical practice for providers such as advanced care providers and medical doctors should be emphasized more. Understanding the barriers or current challenges to exercise and exercise prescription is recommended. This review focused specifically on interventions to improve the quality of life for pwMS, which leads to another limitation of this review. This review did not include studies focused on the implementation of the evidence into clinical practice.
CBT is a non-pharmacological intervention for depression, cognitive impairments, and fatigue, with promising results. Several studies reported CBT as an effective intervention for improving the quality of life for pwMS.24,32,35,42 CBT was shown to be effective both in parallel with pharmacological options or as a stand-alone therapy. CBT is used in these studies to improve quality of life and treat depression, cognitive challenges, and fatigue. The studies included in this review are consistent with other available literature.58,66,82 The range of symptoms CBT can treat suggests CBT should be considered an option for pwMS. Looking outside this review at the larger body of literature, CBT is shown to be effective; however, it is not widely used as an intervention for pwMS. Studies indicate many pwMS have yet to be offered therapies such as CBT as part of their care.26,83,84 Considerations when using CBT are that it might not have long-lasting effects and, therefore, may need to be employed throughout the disease course multiple times.
It is well established in the literature that mental and emotional health can substantially impact the quality of life pwMS experience. Mental and emotional health concerns can occur anytime throughout the disease course. Current research also indicates that pwMS seldom report having their mental and emotional health needs addressed during routine medical visits.59 CBT was a cited therapy in this review, as stated above, to treat depression and anxiety, but currently, this therapy is not commonly offered in clinical practice. This again shifts the need from exploring interventions to how best to integrate these intervention strategies into routine medical practice. The research is available to support CBT, but recent studies indicate a lag in translating mental health and CBT into regular practice.
Conclusion
This article aimed to summarize non-pharmacological interventions for people with multiple sclerosis that have been shown to improve the quality of life for people with multiple sclerosis over the last five-year period. Several nonpharmacological interventions had evidence to support their use to promote physical, cognitive, and mental health, which ultimately influences the quality of life pwMS experience.52,85 What appears to be lagging for non-pharmacological interventions is the implementation of these interventions into clinical practice. Several studies discussed in this review concluded that exercise and CBT are safe and essential interventions that are shown to improve the quality of life for pwMS. Unfortunately, some of these studies also reported that these interventions are not commonly reported to be used in routine healthcare visits. Non-pharmacological interventions such as exercise and cognitive behavioral therapy improve the quality of life for pwMS, yet, these interventions are not prescribed as much as they should be.
Taking a biopsychosocial approach to healthcare is essential for optimal health and especially important if you have a chronic disease like MS. Integrating nonpharmacological interventions into routine care for pwMS is shown to improve quality of life. Several nonpharmacological interventions are effective, safe, and complementary to medical therapies. Exercise has clear evidence to back its use, but exercise is not widely prescribed as an intervention to improve the quality of life for pwMS directly. Integrating exercise into routine clinical practice must be explored and understood more. Translating the knowledge of exercise and CBT into regular MS care is essential to achieve broad adoption of exercise and CBT interventions.
There is also a notable need for more rigorous RTCs and primary studies. Many studies used for this review and available are systematic reviews and meta-analyses. This is causing the systematic reviews to be of lower quality due to minimal RTCs, with a few less rigorous studies only being present for nonpharmacological interventions. This may be due to funding and time concerns. Fortunately, we have strong evidence to conclude that exercise and CBT therapies can improve the quality of life for pwMS. Exercise and CBT can improve physical, cognitive, and mental health for pwMS.
Key Points
- Multiple Sclerosis can cause various symptoms that impact the overall quality of life for the pwMS.
- Non-pharmacological interventions are available to treat various symptoms related to MS.
- Exercise, cognitive behavioral therapy, and cognitive rehabilitation can improve physical, cognitive, and mental health for pwMS. Moderate to strong levels of evidence support using these nonpharmacological interventions to improve the quality of life for pwMS.
Summary
Some health and wellness needs in the MS population are not routinely addressed in regular medical visits. These health needs can significantly affect those individuals’ quality of life. While exercise and CBT are well supported in the literature as effective interventions, commonly, they are not discussed during routine medical visits. Research attention must focus on translating this knowledge into practice and on high-quality RTCs to clearly show the benefit of nonpharmacological interventions for pwMS. Non-pharmacological interventions do not remove the importance of disease-modifying agents or other medications but increase the number of interventions available to pwMS.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cuerda-Ballester M, Martínez-Rubio D, García-Pardo MP, et al. Relationship of motor impairment with cognitive and emotional alterations in patients with multiple sclerosis. Int J Environ Res Public Health. 2023;20(2):1387. doi:10.3390/ijerph20021387
2. Immune-Mediated Disease. National multiple sclerosis society. Available from: http://www.nationalmssociety.org/What-is-MS/Definition-of-MS/Immune-mediated-disease.
3. Nelson LM, Wallin MT, Marrie RA, et al. A new way to estimate neurologic disease prevalence in the United States: illustrated with MS. Neurology. 2019;92(10):469–480. doi:10.1212/WNL.0000000000007044
4. Giovannoni G, Fole JF, Brandes DW. Hidden disabilities in multiple sclerosis? The impact of multiple sclerosis on patients and their caregivers. Eur Neurol Rev. 2013;8(1):2. doi:10.17925/ENR.2013.08.S1.2
5. Browne P, Chandraratna D, Angood C, et al. Atlas of multiple sclerosis 2013: a growing global problem with widespread inequity. Neurology. 2014;83(11):1022–1024. doi:10.1212/WNL.0000000000000768
6. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10):e1029–e1040. doi:10.1212/WNL.0000000000007035
7. Newsome SD, Aliotta PJ, Bainbridge J, et al. A Framework of Care in Multiple Sclerosis, Part 1: updated Disease Classification and Disease-Modifying Therapy Use in Specific Circumstances. Int J MS Care. 2016;18(6):314–323. doi:10.7224/1537-2073.2016-051
8. Somerset M, Campbell R, Sharp DJ, Peters TJ. What do people with MS want and expect from health‐care services?. Health Expect Int J Public Particip Health Care Health Policy. 2001;4(1):29–37. doi:10.1046/j.1369-6513.2001.00111.x
9. Rezapour A, Almasian Kia A, Goodarzi S, Hasoumi M, Nouraei Motlagh S, Vahedi S. The impact of disease characteristics on multiple sclerosis patients’ quality of life. Epidemiol Health. 2017;39. doi:10.4178/epih.e2017008
10. Barin L, Salmen A, Disanto G, et al. The disease burden of Multiple Sclerosis from the individual and population perspective: which symptoms matter most?. Mult Scler Relat Disord. 2018;25:112–121. doi:10.1016/j.msard.2018.07.013
11. Faraclas E, Lynn J, Lau JD, Merlo A. Health-Related Quality of Life in people with Multiple Sclerosis: how does this Population Compare to Population-based Norms in Different Health Domains?. J Patient-Rep Outcomes. 2022;6(1):12. doi:10.1186/s41687-022-00415-4
12. Faraclas E, Merlo A, Lynn J, Lau JD. Perceived facilitators, needs, and barriers to health related quality of life in people with multiple sclerosis: a qualitative investigation. J Patient-Rep Outcomes. 2022;6(1):89. doi:10.1186/s41687-022-00496-1
13. Disanto G, Berlanga AJ, Handel AE, et al. Heterogeneity in Multiple Sclerosis: scratching the Surface of a Complex Disease. Autoimmune Dis. 2011;2011. doi:10.4061/2011/932351
14. Contrò V, Schiera G, Macchiarella A, Sacco A, Lombardo G, Proia P. Multiple sclerosis: physical activity and well-being. Mult Scler. 2017;2:6.
15. Weeks J. Foundation Health Measure Report, Health-Related Quality of Life and Well-Being. Washington: Office of Disease Prevention and Health Promotion; 2020.
16. Healthy People 2030 Framework - Healthy People 2030 | health.gov. Available from: https://health.gov/healthypeople/about/healthy-people-2030-framework.
17. Motl RW, Mowry EM, Ehde DM, et al. Wellness and multiple sclerosis: the National MS Society establishes a Wellness Research Working Group and research priorities. Mult Scler Houndmills Basingstoke Engl. 2018;24(3):262–267. doi:10.1177/1352458516687404
18. Dalgas U, Langeskov-Christensen M, Stenager E, Riemenschneider M, Hvid LG. Exercise as Medicine in Multiple Sclerosis—Time for a Paradigm Shift: preventive, Symptomatic, and Disease-Modifying Aspects and Perspectives. Curr Neurol Neurosci Rep. 2019;19(11):88. doi:10.1007/s11910-019-1002-3
19. Mendozzi L, Tovo A, Grosso C, et al. Changing Lifestyle of Persons With Multiple Sclerosis: development, Feasibility and Preliminary Results of a Novel High-Impact Collaborative Intervention in Leisure Environments. Int J Phys Med Rehabil. 2018;06(02). doi:10.4172/2329-9096.1000461
20. Department N, Rehabilitation Hospital C, Iasi R, Schreiner TG. “Gr.T. Popa” University of Medicine and Pharmacy, Iasi, Romania, et al. New insights on depression in multiple sclerosis – a literature review. Romanian J Neurol. 2020;19(4):237–243. doi:10.37897/RJN.2020.4.4
21. Silva MD, Cavalcanti DB. Evaluation of quality of life in multiple sclerosis patients: impact of fatigue, anxiety and depression. Int J Med. 2019;26:339. doi:10.6084/m9.figshare.11312930.v1
22. Al-Sharman A, Khalil H, El-Salem K, Aldughmi M, Aburub A. The effects of aerobic exercise on sleep quality measures and sleep-related biomarkers in individuals with Multiple Sclerosis: a pilot randomised controlled trial. NeuroRehabilitation. 2019;45(1):107–115. doi:10.3233/nre-192748
23. Tollár J, Nagy F, Tóth BE, et al. Exercise Effects on Multiple Sclerosis Quality of Life and Clinical–Motor Symptoms. Med Sci Sports Exerc. 2020;52(5):1007. doi:10.1249/MSS.0000000000002228
24. Harrison AM, Safari R, Mercer T, et al. Which exercise and behavioural interventions show most promise for treating fatigue in multiple sclerosis? A network meta-analysis. Mult Scler Houndmills Basingstoke Engl. 2021;27(11):1657–1678. doi:10.1177/1352458521996002
25. Farrell JW, Merkas J, Pilutti LA. The effect of exercise training on gait, balance, and physical fitness asymmetries in persons with chronic neurological conditions: a systematic review of randomized controlled trials. Front Physiol. 2020;11:585765. doi:10.3389/fphys.2020.585765
26. Nauta IM, Bertens D, Fasotti L, et al. Cognitive rehabilitation and mindfulness reduce cognitive complaints in multiple sclerosis (REMIND-MS): a randomized controlled trial. Mult Scler Relat Disord. 2023;71:104529. doi:10.1016/j.msard.2023.104529
27. Harand C, Defer G. Psychological interventions in multiple sclerosis: improving cognition and quality of life. Ann Phys Rehabil Med. 2020;63(2):148–153. doi:10.1016/j.rehab.2018.10.002
28. PEDro scale – pEDro; 2016. Available from: https://pedro.org.au/english/resources/pedro-scale/.
29. Amin NS, Tayebi HME. More gain, less pain: how resistance training affects immune system functioning in multiple sclerosis patients: a review. Mult Scler Relat Disord. 2023;69. doi:10.1016/j.msard.2022.104401
30. Zrzavy T. Effects of normobaric hypoxic endurance training on fatigue in patients with multiple sclerosis: a randomized prospective pilot study. J Neurol. 2021;268(12):4809. doi:10.1007/s00415-021-10596-5
31. Salarvand S, Heidari ME, Farahi K, Teymuri E, Almasian M, Bitaraf S. Effectiveness of massage therapy on fatigue and pain in patients with multiple sclerosis: a systematic review and meta-analysis. Mult Scler J Exp Transl Clin. 2021;7(2):20552173211022780. doi:10.1177/20552173211022779
32. Moss-Morris R, Harrison AM, Safari R, et al. Which behavioural and exercise interventions targeting fatigue show the most promise in multiple sclerosis? A systematic review with narrative synthesis and meta-analysis. Behav Res Ther. 2021;137:103464. doi:10.1016/j.brat.2019.103464
33. d’Arma A, Saresella M, Rossi V, et al. Increased levels of beta-endorphin and noradrenaline after a brief high-impact multidimensional rehabilitation program in multiple sclerosis. Life. 2022;12(5):755. doi:10.3390/life12050755
34. Cancelli A, Cottone C, Giordani A, et al. Personalized, bilateral whole-body somatosensory cortex stimulation to relieve fatigue in multiple sclerosis. Mult Scler Houndmills Basingstoke Engl. 2018;24(10):1366–1374. doi:10.1177/1352458517720528
35. Nourbakhsh B, Waubant E, Evers AWM, Solomon AJ. Ethical considerations in the treatment of multiple sclerosis fatigue. Mult Scler Relat Disord. 2021;54:103129. doi:10.1016/j.msard.2021.103129
36. Feys P, Moumdjian L, Van Halewyck F, et al. Effects of an individual 12-week community-located “start-to-run” program on physical capacity, walking, fatigue, cognitive function, brain volumes, and structures in persons with multiple sclerosis. Mult Scler Houndmills Basingstoke Engl. 2019;25(1):92–103. doi:10.1177/1352458517740211
37. Cortés-Pérez I, Sánchez-Alcalá M, Nieto-Escámez FA, Castellote-Caballero Y, Obrero-Gaitán E, Osuna-Pérez MC. Virtual reality-based therapy improves fatigue, impact, and quality of life in patients with multiple sclerosis. a systematic review with a meta-analysis. Sensors. 2021;21(21):7389. doi:10.3390/s21217389
38. Di Cara M, Grezzo D, Palmeri R, et al. Psychological well-being in people with multiple sclerosis: a descriptive review of the effects obtained with mindfulness interventions. Neurol Sci off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2022;43(1):211–217. doi:10.1007/s10072-021-05686-1
39. Rezaian Langroudi R, Ghiasian M, Roozbehani M, Shamsaei F. Comparison of the Effectiveness of Group Therapy Based on Acceptance and Commitment and Amantadine on Pain, Fatigue and Quality of Life in Patients with Multiple Sclerosis. Avicenna J Nursing Midwifery Care. 2020;28(3):251–262. doi:10.30699/ajnmc.28.3.251
40. Homayuni A, Abedini S, Hosseini Z, Etemadifar M, Ghanbarnejad A. Explaining the facilitators of quality of life in patients with multiple sclerosis: a qualitative study. BMC Neurol. ;21(1):193. doi: 10.1186/s12883-021-02213-9
41. Ozkul C, Guclu-Gunduz A, Eldemir K, Apaydin Y, Yazici G, Irkec C. Combined exercise training improves cognitive functions in multiple sclerosis patients with cognitive impairment: a single-blinded randomized controlled trial. Mult Scler Relat Disord. 2020;45:102419. doi:10.1016/j.msard.2020.102419
42. Montañés‐Masias B, Bort‐Roig J, Pascual JC, Soler J, Briones‐Buixassa L. Online psychological interventions to improve symptoms in multiple sclerosis: a systematic review. Acta Neurol Scand. 2022;146(5):448–464. doi:10.1111/ane.13709
43. Grazioli E, Nigro E, Cerulli C, et al. Case Report: concurrent Resistance and Aerobic Training Regulate Adiponectin Expression and Disease Severity in Multiple Sclerosis: a Case Study. Front Neurosci. 2020;14. doi:10.3389/fnins.2020.567302
44. Naro A, Leo A, Russo M, et al. Breakthroughs in the spasticity management: are non-pharmacological treatments the future?. J Clin Neurosci off J Neurosurg Soc Australas. 2017;39:16–27. doi:10.1016/j.jocn.2017.02.044
45. Zucchella C, Mantovani E, De Icco R, Tassorelli C, Sandrini G, Tamburin S. Non-invasive Brain and Spinal Stimulation for Pain and Related Symptoms in Multiple Sclerosis: a Systematic Review. Front Neurosci. 2020;14:547069. doi:10.3389/fnins.2020.547069
46. Amatya B, Young J, Khan F. Non-pharmacological interventions for chronic pain in multiple sclerosis: a Cochrane systematic review. Ann Phys Rehabil Med. 2018;61:e106. doi:10.1016/j.rehab.2018.05.227
47. Krupp L. Fatigue is intrinsic to multiple sclerosis (MS) and is the most commonly reported symptom of the disease. Mult Scler Houndmills Basingstoke Engl. 2006;12(4):367–368. doi:10.1191/135248506ms1373ed
48. Weiland TJ, Jelinek GA, Marck CH, et al. Clinically Significant Fatigue: prevalence and Associated Factors in an International Sample of Adults with Multiple Sclerosis Recruited via the Internet. PLoS ONE. 2015;10(2):e0115541. doi:10.1371/journal.pone.0115541
49. Kobelt G, Langdon D, Jönsson L. The effect of self-assessed fatigue and subjective cognitive impairment on work capacity: the case of multiple sclerosis. Mult Scler Houndmills Basingstoke Engl. 2019;25(5):740–749. doi:10.1177/1352458518769837
50. Mikuľáková W, Klímová E, Kendrová L, Gajdoš M, Chmelík M. Effect of rehabilitation on fatigue level in patients with multiple sclerosis. Med Sci Monit Int Med J Exp Clin Res. 2018;24:5761–5770. doi:10.12659/MSM.909183
51. Razazian N, Yavari Z, Farnia V, et al. Exercising impacts on fatigue, depression, and paresthesia in female patients with multiple sclerosis. Med Sci Sports Exerc. 2016;48(5):796–803. doi:10.1249/MSS.0000000000000834
52. Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017;17(1):185. doi:10.1186/s12883-017-0960-9
53. Pilutti LA, Edwards T, Motl RW, Sebastião E. Functional electrical stimulation cycling exercise in people with multiple sclerosis: secondary effects on cognition, symptoms, and quality of life. Int J MS Care. 2019;21(6):258–264. doi:10.7224/1537-2073.2018-048
54. Proschinger S, Kuhwand P, Rademacher A, et al. Fitness, physical activity, and exercise in multiple sclerosis: a systematic review on current evidence for interactions with disease activity and progression. J Neurol. 2022;269(6):2922–2940. doi:10.1007/s00415-021-10935-6
55. Motl RW. Physical Activity and Healthy Aging with Multiple Sclerosis?Literature Review and Research Directions. US Neurol. 2016;12(01):29. doi:10.17925/USN.2016.12.01.29
56. Zielińska-Nowak E, Włodarczyk L, Kostka J, Miller E. New Strategies for Rehabilitation and Pharmacological Treatment of Fatigue Syndrome in Multiple Sclerosis. J Clin Med. 2020;9(11):3592. doi:10.3390/jcm9113592
57. Sahu M, Tripathi R, Jha NK, Jha SK, Ambasta RK, Kumar P. Cross talk mechanism of disturbed sleep patterns in neurological and psychological disorders. Neurosci Biobehav Rev. 2022;140:104767. doi:10.1016/j.neubiorev.2022.104767
58. Gravesteijn AS, de Groot V, Hulst HE. The future for non-pharmacological treatments in MS: looking back and moving forward. Mult Scler J. 2021;27(11):1640–1642. doi:10.1177/13524585211005344
59. Ysrraelit MC, Fiol MP, Gaitán MI, Correale J. Quality of life assessment in multiple sclerosis: different perception between patients and neurologists. Front Neurol. 2017;8:729. doi:10.3389/fneur.2017.00729
60. Patten SB, Marrie RA, Carta MG. Depression in multiple sclerosis. Int Rev Psychiatry Abingdon Engl. 2017;29(5):463–472. doi:10.1080/09540261.2017.1322555
61. Feinstein A, Magalhaes S, Richard JF, Audet B, Moore C. The link between multiple sclerosis and depression. Nat Rev Neurol. 2014;10(9):507–517. doi:10.1038/nrneurol.2014.139
62. Newsome SD, Aliotta PJ, Bainbridge J, et al. A framework of care in multiple sclerosis, part 2. Int J MS Care. 2017;19(1):42–56. doi:10.7224/1537-2073.2016-062
63. Chwastiak LA, Ehde DM. Psychiatric Issues in Multiple Sclerosis. Psychiatr Clin North Am. 2007;30(4):803–817. doi:10.1016/j.psc.2007.07.003
64. Pompili M, Forte A, Palermo M, et al. Suicide risk in multiple sclerosis: a systematic review of current literature. J Psychosom Res. 2012;73(6):411–417. doi:10.1016/j.jpsychores.2012.09.011
65. Kidd T, Carey N, Mold F, et al. A systematic review of the effectiveness of self-management interventions in people with multiple sclerosis at improving depression, anxiety and quality of life. PLoS ONE. 2017;12(10):e0185931. doi:10.1371/journal.pone.0185931
66. Islas MÁ M, Ciampi E. Assessment and Impact of Cognitive Impairment in Multiple Sclerosis: an Overview. Biomedicines. 2019;7(1). doi:10.3390/biomedicines7010022
67. Foley FW, Benedict RHB, Gromisch ES, DeLuca J. The need for screening, assessment, and treatment for cognitive dysfunction in multiple sclerosis. Int J MS Care. 2012;14(2):58–64. doi:10.7224/1537-2073-14.2.58
68. McNicholas N, O’Connell K, Yap SM, Killeen RP, Hutchinson M, McGuigan C. Cognitive dysfunction in early multiple sclerosis: a review. QJM Mon J Assoc Physicians. 2018;111(6):359–364. doi:10.1093/qjmed/hcx070
69. Cadden M, Arnett P. Factors Associated with employment status in individuals with multiple sclerosis. Int J MS Care. 2015;17(6):284–291. doi:10.7224/1537-2073.2014-057
70. Migliore S, Ghazaryan A, Simonelli I, et al. Cognitive impairment in relapsing-remitting multiple sclerosis patients with very mild clinical disability. Behav Neurol. 2017;2017:7404289. doi:10.1155/2017/7404289
71. Negaresh R, Motl RW, Zimmer P, Mokhtarzade M, Baker JS. Effects of exercise training on multiple sclerosis biomarkers of central nervous system and disease status: a systematic review of intervention studies. Eur J Neurol. 2019;26(5):711–721. doi:10.1111/ene.13929
72. Pilutti LA, Platta ME, Motl RW, Latimer-Cheung AE. The safety of exercise training in multiple sclerosis: a systematic review. J Neurol Sci. 2014;343(1–2):3–7. doi:10.1016/j.jns.2014.05.016
73. Rooney S, Riemenschneider M, Dalgas U, et al. Physical activity is associated with neuromuscular and physical function in patients with multiple sclerosis independent of disease severity. Disabil Rehabil. 2021;43(5):632–639. doi:10.1080/09638288.2019.1634768
74. PRIME PubMed | effects of Pilates-based telerehabilitation on physical performance and quality of life in patients with multiple sclerosis. Available from: https://www.unboundmedicine.com/medline/citation/37147864/Effects_of_Pilates-based_telerehabilitation_on_physical_performance_and_quality_of_life_in_patients_with_multiple_sclerosis.
75. Canavarro M, Serra A, Simões M, et al. The World Health Organization Quality of Life Assessment (WHOQOL). Development and psychometric properties. Int J Behav Med. 2009;16(2):116–124. doi:10.1007/s12529-008-9024-2
76. Kefaliakos A, Pliakos I, Diomidous M. Managing the quality of life in patients with multiple sclerosis: a literature review. In: Unifying the Applications and Foundations of Biomedical and Health Informatics. IOS Press; 2016:220–221. doi:10.3233/978-1-61499-664-4-220
77. Opara J, Jaracz K, Brola W. Quality of life in multiple sclerosis. J Med Life. 2010;3(4):352–358.
78. Nortvedt MW, Riise T. The use of quality of life measures in multiple sclerosis research. Mult Scler J. 2003;9(1):63–72. doi:10.1191/1352458503ms871oa
79. Crank H, Carter A, Humphreys L, et al. Qualitative investigation of exercise perceptions and experiences in people with multiple sclerosis before, during, and after participation in a personally tailored exercise program. Arch Phys Med Rehabil. 2017;98(12):2520–2525. doi:10.1016/j.apmr.2017.05.022
80. Learmonth YC, Motl RW. Physical activity and exercise training in multiple sclerosis: a review and content analysis of qualitative research identifying perceived determinants and consequences. Disabil Rehabil. 2016;38(13):1227–1242. doi:10.3109/09638288.2015.1077397
81. Learmonth YC, Adamson BC, Balto JM, et al. Multiple sclerosis patients need and want information on exercise promotion from healthcare providers: a qualitative study. Health Expect Int J Public Particip Health Care Health Policy. 2017;20(4):574–583. doi:10.1111/hex.12482
82. Solaro C, Gamberini G, Masuccio FG. Depression in Multiple Sclerosis: epidemiology, Aetiology, Diagnosis and Treatment. CNS Drugs. 2018;32(2):117–133. doi:10.1007/s40263-018-0489-5
83. Hind D, Cotter J, Thake A, et al. Cognitive behavioural therapy for the treatment of depression in people with multiple sclerosis: a systematic review and meta-analysis. BMC Psychiatry. 2014;14(1):5. doi:10.1186/1471-244X-14-5
84. Gomes KE, Ruiz JA, Raskin SA, et al. The Role of Cognitive Impairment on Physical Therapy Attendance and Outcomes in Multiple Sclerosis. J Neurol Phys Ther. 2022;46(1):34–40. doi:10.1097/NPT.0000000000000375
85. Malcomson KS, Lowe-Strong AS, Dunwoody L. What can we learn from the personal insights of individuals living and coping with Multiple Sclerosis?. Disabil Rehabil. 2008;30(9):662–674. doi:10.1080/09638280701400730
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent Aphthous Stomatitis Affects Quality of Life. A Case-Control Study
Rivera C, Muñoz-Pastén M, Núñez-Muñoz E, Hernández-Olivos R
Clinical, Cosmetic and Investigational Dentistry 2022, 14:217-223
Published Date: 26 July 2022
Assessing Quality-of-Life of Patients Taking Mirabegron for Overactive Bladder
Shaw C, Gibson W
Therapeutics and Clinical Risk Management 2023, 19:27-33
Published Date: 10 January 2023
Factors Associated with Therapeutic Adherence in Multiple Sclerosis in Spain
Soria C, Prieto L, Lázaro E, Ubeda A
Patient Preference and Adherence 2023, 17:679-688
Published Date: 14 March 2023
Influence of Disease Acceptance on the Quality of Life of Patients with Ankylosing Spondylitis – Single Centre Study
Wysocki G, Czapla M, Uchmanowicz B, Fehler P, Aleksandrowicz K, Rypicz, Wolska-Zogata I, Uchmanowicz I
Patient Preference and Adherence 2023, 17:1075-1092
Published Date: 18 April 2023
Preferences, Adherence, and Satisfaction: Three Years of Treatment Experiences of People with Multiple Sclerosis
Hoffmann O, Paul F, Haase R, Kern R, Ziemssen T
Patient Preference and Adherence 2024, 18:455-466
Published Date: 22 February 2024