Back to Journals » Patient Preference and Adherence » Volume 18
Interventions to Improve Endoscopic Screening Adherence of Cancer in High-Risk Populations: A Scoping Review
Authors Sun YX ![]() , Tang T, Zou JY
, Tang T, Zou JY ![]() , Yue QQ, Hu LF, Peng T, Meng XR, Feng GH, Huang LL, Zeng Y
, Yue QQ, Hu LF, Peng T, Meng XR, Feng GH, Huang LL, Zeng Y
Received 8 October 2023
Accepted for publication 7 March 2024
Published 20 March 2024 Volume 2024:18 Pages 709—720
DOI https://doi.org/10.2147/PPA.S443607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ying-Xue Sun,1,* Tian Tang,1,* Jin-Yu Zou,1,* Qian-Qian Yue,1 Li-Feng Hu,1 Tong Peng,1 Xin-Ru Meng,1 Ge-Hui Feng,1 Li-Li Huang,1 Ying Zeng1– 3
1Department of International and Humanistic Nursing, School of Nursing, Hengyang Medical School, University of South China, Hengyang, People’s Republic of China; 2Hunan Province Key Laboratory of Tumor Cellular & Molecular Pathology, Cancer Research Institute, Hengyang Medical School, University of South China, Hengyang, People’s Republic of China; 3Hunan Engineering Research Center for Early Diagnosis and Treatment of Liver Cancer, Cancer Research Institute, Hengyang Medical School, University of South China, Hengyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Zeng, Department of International and Humanistic Nursing, School of Nursing, Hengyang Medical School, University of South China, Hengyang, People’s Republic of China, Tel +86 17773486339, Fax + 86 0734-8281344, Email [email protected]
Background: Colorectal, and gastric cancers have the second, and fourth mortality rates worldwide, respectively. Endoscopic screening is a crucial diagnostic tool for colorectal, and gastric cancers. Effective interventions can improve adherence to endoscopic screening in high-risk populations, which is important for cancer prevention and mortality reduction. This study aimed to identify interventions that could improve adherence to endoscopic screening for cancer in high-risk populations.
Methods: Combination keywords including colorectal cancer, gastric cancer, screening adherence, and interventions were used to search for articles in PubMed, Web of Science, Cochrane Library, and MEDLINE Complete. The review methodology was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-SCR).
Results: A total of 12 articles were included in this review: 9 randomized controlled trials(RCT) and 3 quasi-experimental studies(QEDs). Among the extracted studies, 11 were about colorectal cancer, and 1 was about gastric cancer. Most studies used lecture-based or Information Technology-based health education interventions. Narrative interventions have proven to be novel and effective approaches for promoting adherence to endoscopic screening. Health education interventions included cancer epidemiology, cancer risk factors, warning symptoms, and screening methods.
Conclusion: All interventions involved were effective in increasing individual knowledge of cancer-related endoscopic screening, willingness to undergo screening, and screening behaviors. These findings provide a reference for designing endoscopy-related cancer screening interventions.
Keywords: colorectal cancer, gastric cancer, screening adherence, high-risk population
Introduction
Cancer is the second leading cause of death worldwide.1 According to the World Health Organization in 2019, there were an estimated 19.3 million new cases and 10 million deaths worldwide in 2020.2 Colorectal, and gastric cancers have the second, and fourth highest mortality rates worldwide, respectively.2 Studies show that the five-year survival rate is 85% for stage I and 30% for stage IV in colorectal cancer,3 94.9% for stage I and 8.1% for stage IV in gastric cancer,4 Colorectal, gastric cancers have poor survival rates at late stages.
Endoscopy is an effective screening tool for colorectal, and gastric cancer. Asia is a region with a high incidence of gastric cancer, and Korea and Japan have conducted nationwide gastric cancer screening programs. The Korean gastric cancer screening guidelines recommend that the asymptomatic general population between the ages of 40 and 74 years undergo gastric cancer screening once every two years.5 Japanese gastric cancer screening guidelines recommend gastric cancer screening for the general population over 50 years of age.6 China guidelines for gastric cancer screening recommend annual gastric cancer screening for high-risk individuals.7 2021 American Gastroenterological Association colorectal cancer screening guideline recommend colorectal cancer screening for the general risk population between the ages of 50 and 75.8 General endoscopy is expensive, and due to national gastric cancer screening programs in Japanese and Korean countries,9 screening is less of a financial burden, with high rates of participation in gastroscopy and high five-year survival rates for gastric cancer compared to other Asian countries. Colonoscopy is expensive, requires bowel preparation and anesthesia, is invasive, and causes discomfort, resulting in a low screening rate. Overall, compliance with endoscopic screening is low, early diagnosis of cancer is low, and patients cannot be treated promptly, resulting in low survival rates.
Screening can increase the chances of early detection and treatment, thus improving survival rates.10,11 However, the current endoscopic screening adherence is low, at 12.9%,12 17.4%13 in high-risk populations for colorectal, gastric cancers, respectively, in China. The factors associated with poor endoscopy screening rates are complex and similar. Economic status is the most important factor influencing endoscopy screening adherence, and uninsured individuals are less likely to undergo screening.14 Low education level is a hindrance to endoscopy screening15 and insufficient knowledge can hinder endoscopy screening.12,13 Difficulty getting an appointment is a significant barrier to endoscopy.15 Fear of screening procedures and fear of endoscopic complications are important reasons for not attending screening.16 An effective way to improve cancer survival is by improving endoscopic screening adherence in high-risk populations.
Studies have developed various interventions to improve adherence to endoscopic screening in high-risk populations. Health education brochures, face-to-face health education, individualized narrative care, appointment reminders, invitation letters, phone calls, and text messages are generally used to communicate information to participants.17 Targeted interventions using intervention programs for people at high risk for colorectal, gastric cancers together with regular appointment reminders have been shown to be cost-effective and time-efficient in increasing screening rates.18 Given the limited number of studies that have cumulatively evaluated the effectiveness of interventions to improve endoscopic screening adherence of cancer in high-risk populations, the purpose of this scoping review was to conclude the interventions used to improve endoscopic screening adherence and determine the effectiveness of these interventions.
Methods
Overview
This review was based on the PRISMA guidelines19 and their structured approach provided by the guidelines. This review was based on the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-SCR). The study protocol was registered with the International Prospective Registry of Systematic Reviews (PROSPERO) on 15 July 2022 (registration number: CRD42022343319).
Search Strategy
Searches were performed using PubMed, Cochrane Library, MEDLINE Complete, and Web of Science electronic databases. This review was conducted by combining the terms “gastric cancer”, “colorectal cancer”, “mass screening”, “early cancer diagnosis”, “adherence”, “intervention”, “trial”, and “experimental trial”. The search was conducted at the beginning of 30 June 2022. See Appendix 1 for the complete database search strategy.
Inclusion Criteria
Papers were included if they satisfied all of the following criteria: (1) articles of randomized controlled trials and quasi-experimental designs; (2) interventions related to cancer screening adherence (this article focused on endoscopy-related cancer screening adherence interventions, excluding other screening interventions); (3) described the effectiveness and implementation of interventions on outcomes related to endoscopy-related cancer screening; and (4) were published in English in peer-reviewed journals from inception up to 30 June 2022. Articles on multiple mixed cancers were excluded from the analysis.
Selection of Article
Two researchers conducted the literature search by referring to the above search strategies and one researcher removed duplicates using Endnote. Two independent investigators screened the retrieved studies based on their titles and abstracts using eligibility criteria. Subsequently, the same two researchers conducted a full-text screening. The screening process is shown in the PRISMA flowchart (Figure 1).
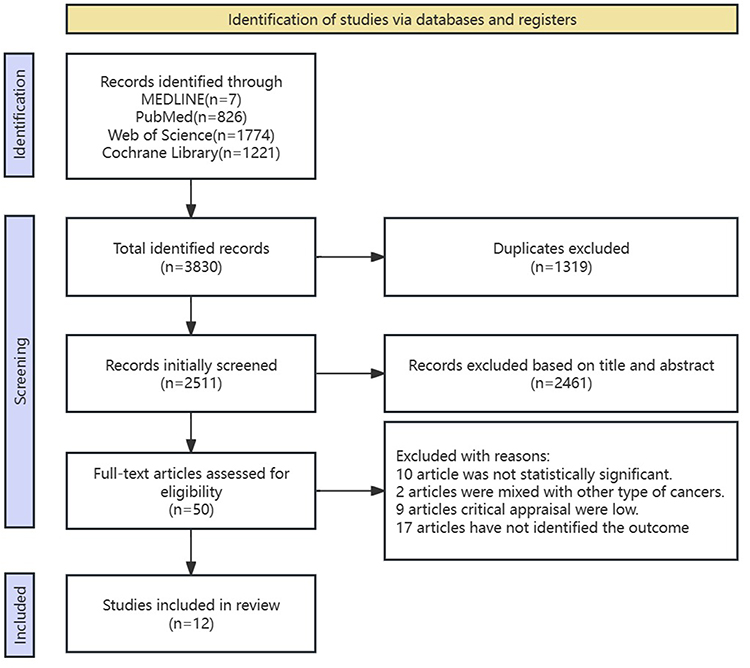 |
Figure 1 The PRISMA flow diagram. |
Data Extraction and Charting
The following data were extracted from each selected article:
- Article identifiers (author, year, country, study design, sample size/age, outcome measure timeline, and main findings)
- Types of cancer
- Intervention content and methods
- Outcome measures (awareness, knowledge, or attitude; screening rate; and implementation-related outcomes)
Results
Overview of Studies
Table 1 presents an overview of these 12 studies. Nine studies used a randomized controlled trial (RCT) design20–28 and three were QEDs.29–31 Of the QEDs, one was two-group pre- and post-experimental comparisons studies,31 and two were one-group pre/post-test comparative studies.29,30 Regarding the countries involved in the studies, 7 studies were from the United States,21–25,29,30 one study from South Korea,20 one study from Iran,26 one study from Turkey,28 one study from the United Kingdom,27 and one study from Jordan.31 The types of cancer involved in 11 on colorectal cancer21–31 and 1 on gastric cancer.20
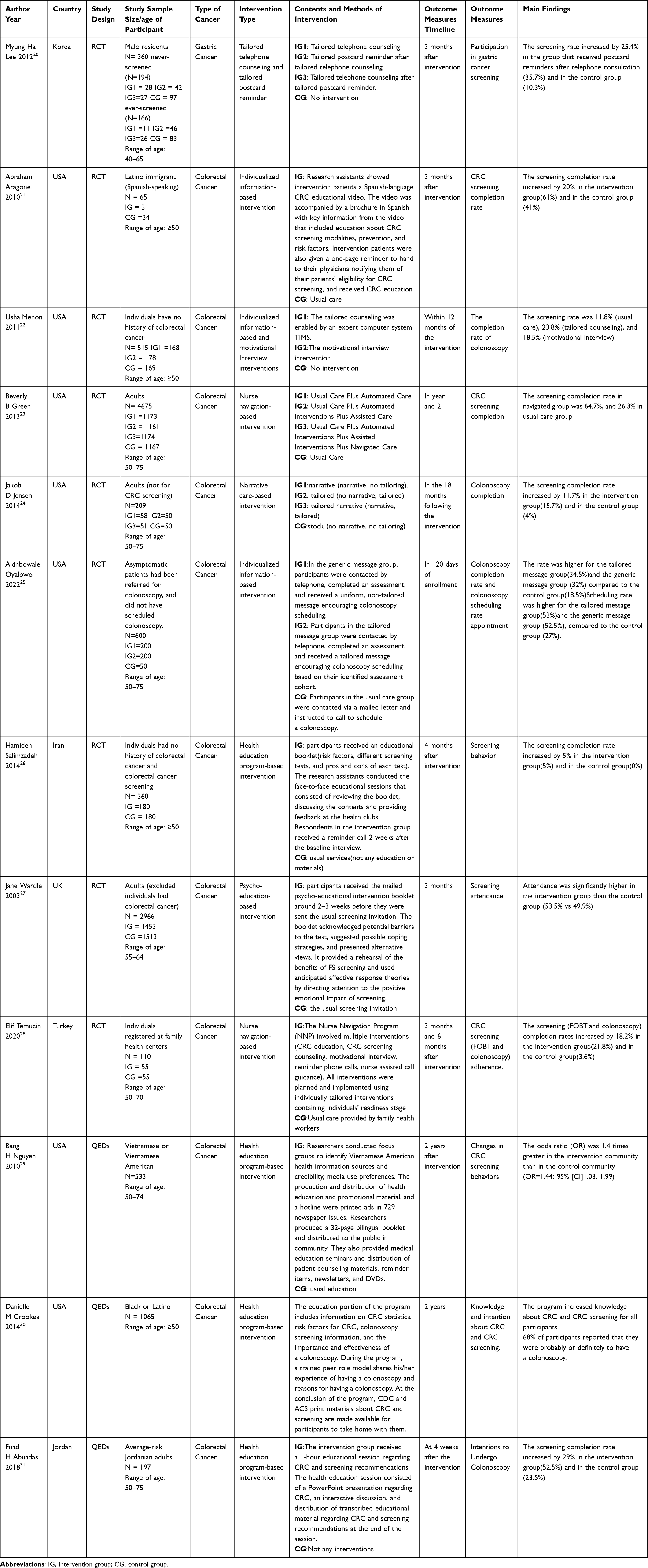 |
Table 1 Description of the Selected Articles |
Structure and Outcomes of Endoscopic-Related Cancer Screening Adherence Intervention
Gastric Cancer
One study20 was designed as an RCT and the intervention adopted individualized telephone counseling and postcard reminders to intervene in screening adherence. Individualized telephone counseling focused on targeting study participants to encourage them to attend gastric cancer screening based on their survey baseline status, assisting men at a high risk of gastric cancer in making appointments, and explaining the entire process of gastric cancer screening. Individualized postcard reminders were primarily text reminders for gastric cancer screening based on the baseline status of the study participants, including information on gastric cancer screening, nearby screening units (name, location, and phone number), and instructions for scheduling gastric cancer screening. The results revealed a significant increase in gastric cancer screening participation among men who had never undergone gastric cancer screening after the intervention. The participation rate in gastric cancer screening increased by 25.4% in the group that received postcard reminders after telephone consultation (35.7%) and in the no-intervention group (10.3%).
Colorectal Cancer
Eight studies were RCTs,21–28 two were single-group before-and-after controlled class experimental studies,29,30 and one was a two-group before-and-after class experimental design.31 Four studies were health education program-based interventions,26,29–31 three were individualized information-based interventions,21,22,25 two were nurse navigation-based interventions,23,28 one was a psycho-education-based intervention,27 and one was a narrative care-based intervention.24
The health education program intervention26,29–31 consisted of face-to-face health education lectures conducted by the researchers. These lectures included distributing educational brochures, discussing relevant content, providing timely feedback on questions, and addressing barrier factors. Each lecture lasted approximately 60 min. The content of the educational brochures included risk factors for colorectal cancer; warning symptoms; prevention methods; and the selection, advantages, and disadvantages of screening methods. The health booklet provides information on the preparation and precautions to be taken before and after colorectal screening based on colorectal cancer screening guidelines. Individualized information-based intervention21,22,25 means that researchers contact people at high risk for colorectal cancer by telephone to complete an initial information assessment and a one-on-one targeted information intervention to guide the study population through colonoscopy based on the initial information assessment of the study population. The nurse navigation-based intervention23,28 consisted of nurses following and guiding the study participants throughout the entire process, educating them about colorectal cancer health knowledge, providing colorectal cancer screening counseling, conducting motivational interviews based on the study participants’ information, and regularly reminding them of screening telephone guidance. Psychoeducational intervention27 focuses on identifying the barrier factors for performing colorectal screening according to the basic conditions of the study participants and using psychological theory to guide the study participants to develop positive psychology toward screening. Narrative care-based intervention24 focuses on individualized story sharing based on information about gender, age, and race.
All of the colorectal cancer screening adherence interventions addressed in the literature were effective in increasing colorectal cancer screening rates from 3.6% to 38.4%. Three of the RCT trials used individualized information-based interventions. One included developed brochures and educational videos based on basic information about the participant and had a physician refer them for CRC screening, with a 20% higher screening rate in the intervention group (61%) than in the control group (41%). Two assessed participants’ basic information, tailored one-on-one phone coaching to needs, provided screening information, and encouraged colonoscopy, with a 12% higher screening rate in the intervention group (23.8%) than in the control group (11.8%) and a 16% higher screening rate in the intervention group (34.5%) than in the control group (18.5%). Two of the RCT trials used nurse navigation-based interventions, in which nurses provided participants with health education and assisted with referrals, appointments, and preparation for colonoscopy throughout the process, with a 38.4% higher screening rate in the intervention group (64.7%) compared to the control group (26.3%) and an 18.2% higher screening rate in the intervention group (21.8%) compared to the control group (3.6%). One of the RCT trials used narrative care-based intervention, where stories were tailored to the participant’s baseline information to facilitate colonoscopy, with an 11.7% higher screening rate in the intervention group (15.7%) compared to the control group (4%). One of the RCT trials used health education talk to encourage colonoscopy, and the screening rate was 5% higher in the intervention group (5%) than in the control group (0%). One of the RCT trials used psychoeducation to encourage participant participation in screening through the theory of anticipatory affective response, and the screening rate was 3.6% higher in the intervention group (53.5%) than in the control group (49.9%). All three of the QEDs used health education program-based interventions. The intervention group had an increased screening participation rate compared to the control (OR=1.44 and OR=1.792).
The result shows that nurse navigation-based intervention was the most significant, followed by individualized information-based intervention and narrative care-based intervention, and health education program-based intervention and psycho-education-based intervention were not significant.
Discussion
This review highlights 12 publications with results demonstrating the role of multiple interventions in increasing compliance with endoscopic screening and the level of knowledge about screening in individuals at high risk for cancer. The results of the included studies were consistent.
Individualized Information and Health Education Program Intervention
The most commonly used interventions in the study were individualized information-based interventions and four health education program-based interventions. The study included four individualized information-based interventions and four health education program-based interventions. The results of the above studies found that the individualized information-based interventions had significant effects, and the health education program-based interventions had mixed results, which may be the individualized information-based interventions were RCT, and the three education program-based interventions were QEDs. The use of RCT reduces interfering factors and makes the effects of the interventions more stable Secondly, it may be because health education lectures are for crowed who receive broad knowledge, and individualized information-based intervention is for individuals, and participants get more specific knowledge information and thus are more willing to follow the recommendations. There are some differences in the effectiveness of the interventions when using the same interventions. Using the same individualized information-based intervention, face-to-face instruction by a nurse combined with advice from a physician was more effective than instruction by telephone, which suggests that one-on-one instruction to study participants is more effective, and also suggests that advice from a physician plays a role in facilitating screening. This study only included one gastric cancer study and the subjects were men. Studies have shown that gender, age, and education level are influential factors in gastric cancer screening,32 so there is some interference with the results. Individualized intervention methods are effective in other areas. A study in the UK applied individualized health education lectures to improve medication adherence in patients with chronic obstructive pulmonary disease.33 Current studies have explored the effects of culture-based individualized educational interventions. An individualized education intervention based on American culture significantly increased cancer screening knowledge among men.34 Therefore, individualized information interventions tailored to the different needs of participants are effective. Individualized education followed by group discussions on cancer-related knowledge was more helpful in increasing cancer awareness and cancer screening participation, possibly because this format has a synergistic effect on cancer prevention and cancer screening behaviors when conveying information. In addition, it is recommended that interventions be developed not only for hospital-based individualized cancer education lectures but also for community-based individualized cancer education lectures for the general population.
Narrative Care and Motivational Interviewing Interventions
Narrative care and motivational interviewing are novel and useful approaches to promote screening behaviors. Narrative care is generally used in interventions for chronic diseases, and some studies have shown that it improves the quality of life of cancer survivors and patients with diabetes.35–37 The application of narrative care to endoscopic screening is relatively new, and more studies are needed to verify its effectiveness. Motivational interviewing has been widely used as a clinical method to promote behavioral changes in patients. Motivational interviewing interventions have shown positive effects in improving endoscopic screening compliance and good intervention effects in cardiac rehabilitation.38 Narrative care and motivational interviewing are more interesting than traditional interventions and may be more likely to make participants receive cancer-related information, increase their awareness of the importance of cancer screening, and thus be more willing to undergo screening. Two new forms of intervention should be considered in future intervention development.
Nurse Navigation-Based Interventions
The intervention with the most significant effect included in this study was the nurse navigation-based intervention. Both nurse navigation interventions had significant effects. The nurse navigation intervention had a more significant effect than the individualized information intervention, which may be due to the integration of the individualized information intervention into the nurse navigation intervention process, with the nurse following the study participant throughout the process, educating the participant one-on-one about colorectal cancer health, providing colorectal cancer screening counseling, assisting with colonoscopy appointments and preparations, and following up on completion of the exam. There were also differences in the effectiveness of the two nurse navigation interventions, with nurse navigation-assisted telephone-guided follow-up being more effective than the nurse navigation intervention alone. We can combine multiple interventions to maximize compliance rates. Study has shown that nurse navigation interventions can increase the uptake of early cancer detection, cancer knowledge, beliefs about early detection, and detection of cases of precancerous lesions.39 Nurse navigation implementation has limitations and is more commonly applied to hospital outpatients, and individualized information interventions are more easily implemented on a large scale in the community for at-risk community residents. There is existing research exploring the effect of lay health educators in primary care provider practices on participants’ increased willingness to screen for cancer and acceptance of cancer screening, with some effect.40 Endoscopic screening interventions in the community may consider training lay health educators for large-scale interventions.
This review revealed that multiple interventions can improve endoscopy screening rates, with varying effects. The endoscopy-related cancer screening results were similar. Therefore, interventions which improve adherence to endoscopic screening can be used as references. Comprehensive interventions combining multiple modalities are worth promoting and implementing. When designing an intervention program for endoscopic screening adherence, it is suggested that the format combines traditional medicine and mobile medicine, such as new-style health education lectures combined with telephone text messages. We can also draw on literature to gradually increase the cumulative intervention method, and the intervention content can incorporate narrative care, motivational interviewing, and psychological care. Phone and text reminders, invitation letters, health education, or nurse navigation services, are more effective than interventions that include only one approach. Study showed that m-Health interventions can be effective in improving cancer screening rates and early diagnosis, but a combination of modalities is more effective.11 Therefore, when designing interventions for endoscopic screening adherence, it is important to consider a combination of multiple interventions to optimize their effectiveness. In the Internet era, m-Health has been commonly used in public health care as well as primary health care,41 with a positive impact on treatment care adherence and health behavior change.42 The use of chat applications, such as WeChat, to send messages to participants, share pictures and videos, and chat in real time,43 has made interventions more effective. Engagement with social media apps varies by age group.44 Community workers can use traditional medicine for cancer screening and health education for older adults.
Conclusion
Multiple interventions were effective in increasing endoscopy screening participation rates and the level of knowledge about screening among people at high risk of colorectal, gastric cancer. Combining multiple interventions may be more effective in improving screening adherence for endoscopy-related cancers.
Acknowledgments
The authors thank all the participants in this study. We are grateful to Professor De-liang Cao and Professor Xi Zeng for their advice on manuscript writing. We also gratefully acknowledge Dr. Qi Liu for her advice on projecting revising.
Funding
Natural Science Foundation of Hunan Province: Grant/Award number: 2023JJ30521; Postgraduate Research Innovation Project of Hunan Province, Grant/Award number: CX20221031; Hunan Provincial Innovation Foundation for Undergraduate, Grant/Award number: S202310555248; Hunan Provincial Innovation Foundation for Undergraduate, Grant/Award number: S202210555264; The University of South China Innovation & Entrepreneurship Foundation for Undergraduate, Grant/Award: D202305171152150199; Aid Program for Science and Technology Innovative Research Team in Higher Educational Institutions of Hunan Province.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mortality GBD.; Causes of Death C. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1459–1544.
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Wang R, Lian J, Wang X, et al. Survival rate of colorectal cancer in China: a systematic review and meta-analysis. Front Oncol. 2023;13:1033154. doi:10.3389/fonc.2023.1033154
4. Wenzhe K, Hongmei Z, Jianping X, et al. Survival of patients with gastric cancer surgically treated at the national cancer center of China from 2011 to 2018 according to stage at diagnosis. J Nat Can Cent. 2022;2:3.
5. Group DW, Panel R. Erratum: Korean practice guideline for gastric cancer 2018: an evidence-based, multi-disciplinary approach. J Gast Can. 2019;19(3):372–373. doi:10.5230/jgc.2019.19.e32
6. Hamashima C. Update version of the Japanese guidelines for gastric cancer screening. Japan J Clin Oncol. 2018;48(7):673–683. doi:10.1093/jjco/hyy077
7. He J, Chen WQ, Li ZS, et al. 中国胃癌筛查与早诊早治指南(2022)北京) [China guideline for the screening, early detection and early treatment of gastric cancer (2022, Beijing)]. Zhonghua Zhong Liu Za Zhi. 2022;44(7):634–666. Chinese. doi:10.3760/cma.j.cn112152-20220617-00430
8. Shaukat A, Kahi CJ, Burke CA, Rabeneck L, Sauer BG, Rex DK. ACG clinical guidelines: colorectal cancer screening 2021. Am J Gastroenterol. 2021;116(3):458–479. doi:10.14309/ajg.0000000000001122
9. Leung WK, Wu M-S, Kakugawa Y, et al. Screening for gastric cancer in Asia: current evidence and practice. Lancet Oncol. 2008;9(3):279–287. doi:10.1016/S1470-2045(08)70072-X
10. Clegg-Lamptey J-NA, Vanderpuye V, Dedey F. Late presentation of breast cancer in lower- and middle-income countries. Curr Brea Can Rep. 2019;11(3):143–151. doi:10.1007/s12609-019-00312-8
11. Schliemann D, Tan MM, Hoe WMK, et al. mHealth interventions to improve cancer screening and early detection: scoping review of reviews. J Med Inter Res. 2022;24(8):e36316. doi:10.2196/36316
12. Huang R-L, Liu Q, Wang Y-X, et al. Awareness, attitude and barriers of colorectal cancer screening among high-risk populations in China: a cross-sectional study. BMJ Open. 2021;11(7):e045168. doi:10.1136/bmjopen-2020-045168
13. Liu Q, Zeng X, Wang W, et al. Awareness of risk factors and warning symptoms and attitude towards gastric cancer screening among the general public in China: a cross-sectional study. BMJ Open. 2019;9(7):e029638. doi:10.1136/bmjopen-2019-029638
14. Jolidon V, De Prez V, Willems B, Bracke P, Cullati S, Burton-Jeangros C. Never and under cervical cancer screening in Switzerland and Belgium: trends and inequalities. BMC Public Health. 2020;20(1):1517. doi:10.1186/s12889-020-09619-z
15. Al-Azri M, Al-Kindi J, Al-Harthi T, Al-Dahri M, Panchatcharam SM, Al-Maniri A. Awareness of stomach and colorectal cancer risk factors, symptoms and time taken to seek medical help among public attending primary care setting in Muscat governorate, Oman. J Can Educ. 2019;34(3):423–434. doi:10.1007/s13187-017-1266-8
16. Lidofsky A, Miller A, Jorgensen J, et al. Development and Implementation of a Culturally Appropriate Education Program to Increase Cervical Cancer Screening among Maasai Women in Rural Tanzania. Anna Global Health. 2019;85(1):127. doi:10.5334/aogh.2503
17. Bhochhibhoya S, Dobbs PD, Maness SB. Interventions using mHealth strategies to improve screening rates of cervical cancer: a scoping review. Preventive Med. 2021;143:106387. doi:10.1016/j.ypmed.2020.106387
18. Broberg G, Gyrd-Hansen D, Miao Jonasson J, et al. Increasing participation in cervical cancer screening: offering a HPV self-test to long-term non-attendees as part of RACOMIP, a Swedish randomized controlled trial. Internat J Can. 2014;134(9):2223–2230. doi:10.1002/ijc.28545
19. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
20. Lee MH, Lee YY, Jung DW, et al. Effectiveness of interventions to increase the participation rate of gastric cancer screening in the Republic of Korea: a pilot study. Asian Pacific J Can Prev. 2012;13(3):861–866. doi:10.7314/APJCP.2012.13.3.861
21. Aragones A, Schwartz MD, Shah NR, Gany FM. A randomized controlled trial of a multilevel intervention to increase colorectal cancer screening among Latino immigrants in a primary care facility. J Gen Intern Med. 2010;25(6):564–567. doi:10.1007/s11606-010-1266-4
22. Menon U, Belue R, Wahab S, et al. A randomized trial comparing the effect of two phone-based interventions on colorectal cancer screening adherence. Anna Behavl Med. 2011;42(3):294–303. doi:10.1007/s12160-011-9291-z
23. Green BB, Wang C-Y, Anderson ML, et al. An automated intervention with stepped increases in support to increase uptake of colorectal cancer screening: a randomized trial. Ann Internal Med. 2013;158(5):301–311. doi:10.7326/0003-4819-158-5-201303050-00002
24. Jensen JD, King AJ, Carcioppolo N, Krakow M, Samadder NJ, Morgan S. Comparing tailored and narrative worksite interventions at increasing colonoscopy adherence in adults 50–75: a randomized controlled trial. Soc Sci Med. 2014;104:31–40. doi:10.1016/j.socscimed.2013.12.003
25. Oyalowo A, Forde KA, Lamanna A, Kochman ML. Effect of patient-directed messaging on colorectal cancer screening: a randomized clinical trial. JAMA network open. 2022;5(3):e224529. doi:10.1001/jamanetworkopen.2022.4529
26. Salimzadeh H, Eftekhar H, Majdzadeh R, Montazeri A, Delavari A. Effectiveness of a theory-based intervention to increase colorectal cancer screening among Iranian health club members: a randomized trial. J Behav. 2014;37(5):1019–1029. doi:10.1007/s10865-013-9533-6
27. Wardle J, Williamson S, McCaffery K, et al. Increasing attendance at colorectal cancer screening: testing the efficacy of a mailed, psychoeducational intervention in a community sample of older adults. Health Psychol. 2003;22(1). doi:10.1037/0278-6133.22.1.99
28. Temucin E, Nahcivan NO. The effects of the nurse navigation program in promoting colorectal cancer screening behaviors: a randomized controlled trial. J Can Educ. 2020;35(1):112–124. doi:10.1007/s13187-018-1448-z
29. Nguyen BH, McPhee SJ, Stewart SL, Doan HT. Effectiveness of a controlled trial to promote colorectal cancer screening in Vietnamese Americans. Am J Public Health. 2010;100(5):870–876. doi:10.2105/AJPH.2009.166231
30. Crookes DM, Njoku O, Rodriguez MC, Mendez EI, Jandorf L. Promoting colorectal cancer screening through group education in community-based settings. J Can Educ. 2014;29(2):296–303. doi:10.1007/s13187-013-0599-1
31. Abuadas FH, Petro-Nustas WJ, Abuadas MH. The effect of a health education intervention on Jordanian participants’ colorectal cancer knowledge, health perceptions, and screening practices. Cancer Nursing. 2018;41(3):226–237. doi:10.1097/NCC.0000000000000480
32. Ma K, Chen X, Xiang X, et al. Willingness to undergo gastroscopy for early gastric cancer screening and its associated factors during the COVID-19 pandemic - a nationwide cross-sectional study in China. Pat Prefere Adher. 2023;17:505–516. doi:10.2147/PPA.S400908
33. Janjua S, Pike KC, Carr R, Coles A, Fortescue R, Batavia M. Interventions to improve adherence to pharmacological therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2021;9(9):CD013381. doi:10.1002/14651858.CD013381.pub2
34. Dougherty B, Fisher JL, Adeyanju T, Paskett E. Impact of a culturally tailored education intervention for African-American and Appalachian Men in Ohio. J Can Educ. 2022;37(5):1389–1400. doi:10.1007/s13187-021-01970-y
35. Murphy-Banks R, Blanch-Hartigan D, Boehm L, Hamel PC, Parsons SK. Personal narrative: raising awareness of adolescent and young adult cancer survivors in similarly aged university students. J Adol Young Adult Oncol. 2019;8(4):434–441. doi:10.1089/jayao.2018.0131
36. Reaney M, Gladwin T, Chmiel N, Churchill S. Encouraging foot care in people with and without diabetes through narrative communication. J Health Psychol. 2022;27(9):1993–2012. doi:10.1177/13591053211017206
37. Sebire SJ, Toumpakari Z, Turner KM, et al. ”I’ve made this my lifestyle now”: a prospective qualitative study of motivation for lifestyle change among people with newly diagnosed type two diabetes mellitus. BMC Public Health. 2018;18(1):204. doi:10.1186/s12889-018-5114-5
38. Bohplian S, Bronas UG. Motivational strategies and concepts to increase participation and adherence in cardiac rehabilitation: AN INTEGRATIVE REVIEW. J Cardiopulm Rehabil Prev. 2022;42(2):75–83. doi:10.1097/HCR.0000000000000639
39. Li C, Liu Y, Xue D, Chan CWH. Effects of nurse-led interventions on early detection of cancer: a systematic review and meta-analysis. Internat J Nurs Stud. 2020;110:103684. doi:10.1016/j.ijnurstu.2020.103684
40. Lofters AK, Vahabi M, Prakash V, et al. Lay health educators within primary care practices to improve cancer screening uptake for South Asian patients: challenges in quality improvement. Pat Prefere Adher. 2017;11:495–503. doi:10.2147/PPA.S127147
41. World Health Organization. 2019.
42. Marcolino MS, Oliveira JAQ, D’Agostino M, Ribeiro AL, Alkmim MBM, Novillo-Ortiz D. The impact of mHealth interventions: systematic review of systematic reviews. JMIR mHealth and uHealth. 2018;6(1):e23. doi:10.2196/mhealth.8873
43. Petkovic J, Duench S, Trawin J, et al. Behavioural interventions delivered through interactive social media for health behaviour change, health outcomes, and health equity in the adult population. Cochrane Database Syst Rev. 2021;5(5):CD012932. doi:10.1002/14651858.CD012932.pub2
44. Soto M, Martinez-Gutierrez J, Momany M, et al. Preferences of underserved Chilean women on a mobile technology intervention for cervical cancer screening: qualitative study. JMIR mHealth and uHealth. 2018;6(11):e196. doi:10.2196/mhealth.9494
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.