Back to Journals » Journal of Pain Research » Volume 18
Interpreting the Evidence for Laser Acupuncture in Knee Osteoarthritis Management: A Call for Methodological Rigor and Nuance [Letter]
Authors Zhao FY ![]() , Fu QQ
, Fu QQ ![]() , Ho YS
, Ho YS
Received 25 August 2025
Accepted for publication 10 September 2025
Published 14 September 2025 Volume 2025:18 Pages 4787—4790
DOI https://doi.org/10.2147/JPR.S562822
Checked for plagiarism Yes
Editor who approved publication: Professor Michael Überall
Fei-Yi Zhao,1–4 Qiang-Qiang Fu,5 Yuen-Shan Ho6
1Department of Nursing, School of International Medical Technology, Shanghai Sanda University, Shanghai, 201209, People’s Republic of China; 2School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, 3083, Australia; 3Sydney School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, 2050, Australia; 4Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200071, People’s Republic of China; 5Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China; 6School of Nursing, Faculty of Health and Social Sciences, the Hong Kong Polytechnic University, Hong Kong, SAR, People’s Republic of China
Correspondence: Yuen-Shan Ho, School of Nursing, Faculty of Health and Social Sciences, the Hong Kong Polytechnic University, Hong Kong, SAR, People’s Republic of China, Tel +8522766-6410, Fax +8522364-9663, Email [email protected] Qiang-Qiang Fu, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China, Tel +86021-6569 0520, Fax +86021-65696249, Email [email protected]
View the original paper by Miss Zeng and colleagues
A Response to Letter has been published for this article.
Dear editor
Pain is a primary reason for individuals to seek acupuncture treatment.1 Laser acupuncture (LA), which preserves the conceptual foundations of acupuncture while being non-invasive,2 garners increasing research attention as a potential modality for pain management. A recent systematic review and meta-analysis (SR/MA) by Zeng et al evaluates the analgesic efficacy of LA for knee osteoarthritis (KOA).3 While their work contributes valuable clinical evidence, we have methodological concerns and hold differing perspectives on certain aspects of the study. We welcome the opportunity to further discuss these issues with the authors.
Accuracy Considerations in Trial Reporting and Interpretation
First, Zeng et al’s SR/MA incorporates five randomized controlled trials (RCTs).3 In their results, the authors state that “Two trials were conducted in China,4,5 and the remaining ones in Australia,6 the UK,7 and India”.8 However, verification shows that the trial attributed to the UK is actually conducted at the Security Forces Hospital in Saudi Arabia,7 and the trial ascribed to India is performed at Cipto Mangunkusumo Hospital in Indonesia.8
Second, an inaccuracy pertains to the “Length of Follow-Up” presented in Table 1 of the aforementioned SR/MA. Re-examination of the original RCTs indicates that the reported values likely correspond to the intervention periods rather than follow-up durations. To enhance precision and clinical relevance, both the intervention and follow-up periods of the included studies are recompiled (see our Table 1).
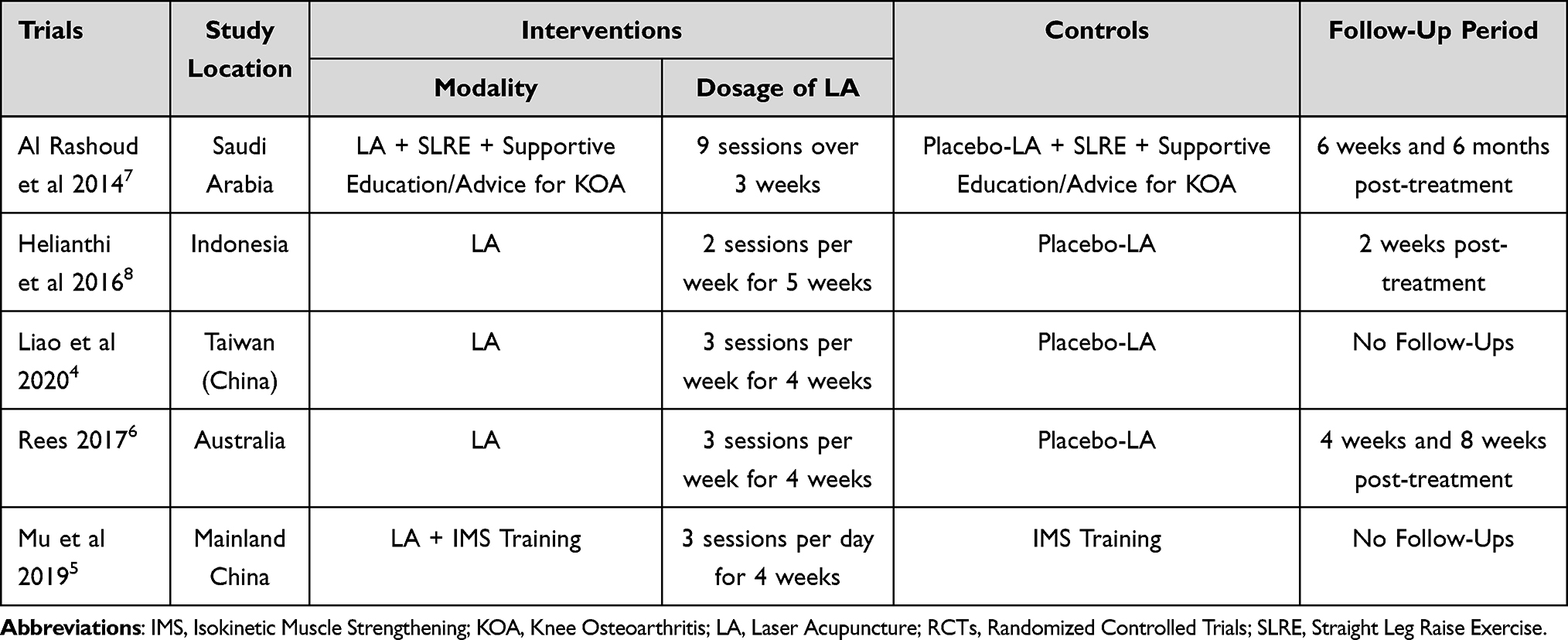 |
Table 1 Re-Extraction of Characteristics from the Five RCTs Included in Zeng et al’s Study |
Third, in the same table, the intervention modality of the 2014 RCT by Al Rashoud et al7 is described as “Laser & Exercise versus Exercise and Exercise.” In reality, the intervention group receives LA combined with straight leg raise exercises and supportive health education/advice for coping with KOA, whereas the control group underwent the same exercise and education/advice protocol along with placebo-LA (see our Table 1).
Finally, a notable inconsistency exists between the statements in the “Overall Findings” and “Conclusion” sections. The former states that LA has “little to no effect” compared to exercise therapy, while the latter concludes that patients undergoing LA “may experience a greater reduction in pain intensity.” This interpretation appears primarily based on a single trial,5 in which the between-group difference [WMD −0.84 cm, 95% CI (−1.12 to −0.56)] does not exceed the pre-specified 1 cm minimal important difference (MID) in Visual Analogue Scale. We respectfully caution against an overly rigid application of the MID in this context, as its clinical relevance can vary based on population, baseline severity, and, notably, the choice of comparator.9 Given that exercise itself is an effective, guideline-recommended management for KOA,10 achieving an additional mean reduction of 0.84 cm (with a lower confidence interval of 0.56 cm) with LA represents a potentially meaningful incremental benefit. This could constitute an important option for patients who have contraindications, poor tolerance, or an inadequate response to exercise.
Discrepancy Between Predefined and Applied Inclusion Criteria
Zeng et al specify that eligible RCTs should “randomize participants to laser needle versus placebo laser, exercise therapy, or no treatment”,3 implying that the intervention arm comprises LA alone, while the control arm consists solely of placebo laser, exercise therapy, or no treatment. However, two of the five included RCTs do not meet this criterion: their interventions combine LA with supportive education/advice for KOA and/or exercise,5,7 and in one trial, the control group also incorporates supportive education/advice for KOA7 (see our Table 1).
Exclusion of Short-Duration Trials Without Justification
Zeng et al stipulate that only RCTs with a treatment duration of ≥4 weeks are eligible for inclusion,3 leading to the exclusion of two shorter-duration trials.11,12 Two associated issues arise.
First, the Saudi Arabian trial referenced earlier involves only nine sessions over three weeks,7 falling short of the four-week threshold, yet it is nonetheless included.
Second, the rationale for excluding RCTs with treatment durations shorter than four weeks is not provided. We speculate that the authors consider shorter duration indicative of an insufficient therapeutic dose. However, dosage depends not only on treatment length but also on session frequency and laser exposure time per session. For instance, while the included Indonesian trial administers ten sessions over five weeks (two sessions per week), with 80 seconds per acupoint,8 the excluded Turkish trial delivers ten sessions within two weeks (five sessions per week), applying LA for 20 minutes per session.12 The total exposure in the Turkish trial is therefore comparable to—or even greater than—that of the included Indonesian8 and Saudi trials.7
In the absence of clear justification, the exclusion of studies with <4 weeks of treatment appears questionable, reduces the number of eligible trials, and potentially weakens the reliability of the meta-analytic synthesis.
Pooling of Heterogeneous Trials and Outcomes at Inconsistent Time Points
Two methodological concerns arise in the pooling of effect sizes.
First, Zeng et al combine the Saudi Arabian RCT (Intervention: LA + Exercise + Education/Advice for KOA; Control: Placebo-LA + Exercise + Education/Advice for KOA)7 with three trials comparing LA versus placebo-LA alone, without subgroup analysis. This approach is methodologically questionable due to fundamental differences in trial designs and objectives. The Saudi trial evaluates whether LA confers additional benefits to routine KOA management, whereas the other three trials assess LA as a stand-alone alternative therapy and whether its effects are specific or nonspecific. Pooling these clinically heterogeneous trials risks introducing statistical heterogeneity and complicating interpretation.
Second, the synthesis of outcome data from temporally inconsistent time points further introduces significant heterogeneity, as visually evidenced by the forest plots (Zeng et al’s Figures 4 and 5). Four of the five included RCTs report end-of-treatment outcomes, whereas the Indonesian trial, which involves 10 sessions over 5 weeks, reports outcomes only after the ninth treatment session and at a 2-week follow-up after treatment cessation.8 Pooling follow-up data from one trial with immediate post-treatment data from others confounds the treatment effect estimate and challenges the interpretation of the pooled result.
Inadequate Investigation of Heterogeneity and Publication Bias
In their meta-analysis, Zeng et al report substantial heterogeneity (I² = 83.95%),3 a critical consideration for interpretation. With only five RCTs included, identifying sources of heterogeneity through meta-regression or similar models is not feasible; the authors’ avoidance of such analyses thus reflects methodological prudence. Nevertheless, leave-one-out sensitivity analyses and limited subgroup analyses (eg, separating trials of LA plus routine care from LA alone) remain both viable and informative. While statistical power is limited, their value lies in generating hypotheses regarding potential sources of heterogeneity. Supplementing these with descriptive comparisons of study characteristics and an L’Abbé plot13 can further strengthen interpretation.
Publication bias is also not assessed. With only five studies, the Doi plot and Luis Furuya-Kanamori Index14 offer viable alternatives to conventional funnel plots for evaluating potential bias.
Lastly, the authors’ assertion that “all studies show that the pain scores in the laser acupuncture treatment group are notably lower compared to the control group, and this high heterogeneity does not compromise the validity of the results” appears overly definitive. Although the direction of effect consistently favors LA or LA combined with routine care, the considerable variation in effect magnitudes (95% CI −1.09 cm to −3.57 cm) is itself notable. This suggests inconsistent treatment responses and implies that the efficacy of LA may be moderated by additional, unexamined factors. Accordingly, the range of effect sizes should be acknowledged as reflecting uncertainty in the magnitude of benefit, rather than asserting uniform effectiveness.
Uncertainty in Adverse Event Evidence and Safety Assessment
Zeng et al report adverse event data from a single RCT (n = 59),8 yielding a relative risk (RR) of 3.52 (95% CI 0.76 to 6.29), which constitutes very low-certainty evidence due to imprecision. The claim that LA has “fewer adverse reactions” than placebo is unsupported, as the RR suggests a potential increased risk, and the wide confidence interval reflects inconclusive results. The absence of adverse event data from the other four RCTs, along with insufficient details regarding event types or severity, limits the ability of the SR/MA to evaluate the safety profile of LA—a critical determinant of its application in KOA. Future trials should prioritize standardized adverse event reporting, such as using the Common Terminology Criteria for Adverse Events (CTCAE),15 to better characterize the safety of LA.
Conclusion and Recommendations
In summary, while Zeng et al’s SR/MA provides valuable reference regarding LA for pain management in KOA, its methodological limitations need to be addressed to yield more robust and clinically translatable results. Future research should focus on meticulous data verification and clearer exploration of heterogeneity, objectively and separately evaluating LA as an alternative therapy and as an adjunct to conventional KOA management, to provide more reliable guidance to inform clinical decision-making.
Abbreviations
CTCAE, Common Terminology Criteria for Adverse Events; KOA, Knee Osteoarthritis; LA, Laser Acupuncture; MID, Minimally Important Difference; RCT(s), Randomized Controlled Trials; RR, Relative Risk; SR/MA, Systematic Review and Meta-Analysis.
Author Contributions
Fei-Yi Zhao: Conceptualization, Investigation, Formal analysis, Writing – original draft. Qiang-Qiang Fu: Formal analysis, Validation, Writing – review and editing; Yuen-Shan Ho: Conceptualization, Methodology, Formal analysis, Writing – review and editing.
All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
No funding was received.
Disclosure
The authors declare no competing interests in this communication.
References
1. Kelly RB, Willis J. Acupuncture for pain. Am Family Phys. 2019;100(2):89–96.
2. Chon TY, Mallory MJ, Yang J, Bublitz SE, Do A, Dorsher PT. Laser acupuncture: a concise review. Med Acupunct. 2019;31(3):164–168. doi:10.1089/acu.2019.1343
3. Zeng DH, Yuan DN, Zhou QQ, Liu YY, Ma WB, Lan L. Laser acupuncture for the pain of knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. J Pain Res. 2025;18:3833–3841. doi:10.2147/JPR.S517994
4. Liao FY, Lin CL, Lo SF, Chang CC, Liao WY, Chou LW. Efficacy of acupoints dual-frequency low-level laser therapy on knee osteoarthritis. Evid Based Complement Alternat Med. 2020;2020(1):6979105. doi:10.1155/2020/6979105
5. Mu ZY, Li YJ, Wang CY, Zhu MH, Li QB. Observation on the therapeutic effect of laser acupuncture combined with isokinetic muscle strength training in the treatment of knee osteoarthritis. Shanghai. J Acupuncture Moxibustion. 2019;38(12):1409–1413.
6. Rees MKL. Evaluation of the Effectiveness of Laser Acupuncture on Osteo-arthritic Knee Pain: A Randomised, Double-blind, Placebo-controlled Clinical Research Trial [Doctorate thesis]. University of Technology Sydney (Australia); 2017.
7. Al Rashoud AS, Abboud RJ, Wang W, Wigderowitz C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: a randomised double-blind comparative trial. Physiotherapy. 2014;100(3):242–248. doi:10.1016/j.physio.2013.09.007
8. Helianthi DR, Simadibrata C, Srilestari A, Wahyudi ER, Hidayat R. Pain reduction after laser acupuncture treatment in geriatric patients with knee osteoarthritis: a randomized controlled trial. Acta Med Indones. 2016;48(2):114–121.
9. King MT. A point of minimal important difference (MID): a critique of terminology and methods. Expert Rev Pharmacoecon Outcomes Res. 2011;11(2):171–184. doi:10.1586/erp.11.9
10. Zhao FY, Fu QQ, Ho YS. Does thunder-fire moxibustion really augment therapeutic efficacy in knee osteoarthritis? Methodological critique of a recent pairwise meta-analysis. J Pain Res. 2025;18:3717–3722. doi:10.2147/JPR.S551887
11. Mezaal AL, Tajali SB, Olyaei G, Jalaie S, Alwatifi ST. Effects of low-level laser versus laser acupuncture in patients with knee osteoarthritis: a randomized controlled trial. J Mod Rehabil. 2018;12(3):181–194.
12. Yurtkuran M, Alp A, Konur S, Ozçakir S, Bingol U. Laser acupuncture in knee osteoarthritis: a double-blind, randomized controlled study. Photomed Laser Surg. 2007;25(1):14–20. doi:10.1089/pho.2006.1093
13. Song F. Exploring heterogeneity in meta-analysis: is the L’Abbé plot useful? J Clin Epidemiol. 1999;52(8):725–730. doi:10.1016/s0895-4356(99)00066-9
14. Furuya-Kanamori L, Xu C, Lin L, et al. P value-driven methods were underpowered to detect publication bias: analysis of Cochrane review meta-analyses. J Clin Epidemiol. 2020;118:86–92. doi:10.1016/j.jclinepi.2019.11.011
15. Shah S. Common terminology criteria for adverse events. Nat Cancer Instit. 2022;784:785.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.