")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Interpersonal Psychotherapy for Late-life Depression and its Potential Application in China
Authors Xu H , Koszycki D
Received 1 February 2020
Accepted for publication 27 July 2020
Published 7 August 2020 Volume 2020:16 Pages 1919—1928
DOI https://doi.org/10.2147/NDT.S248027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Hua Xu,1,2 Diana Koszycki2,3
1Department of Psychiatry, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Faculty of Education and Faculty of Medicine, University of Ottawa, Ottawa, Ontario, Canada; 3Institut du Savoir Montfort, Hôpital Montfort, Ottawa, Ontario, Canada
Correspondence: Hua Xu; Diana Koszycki Email [email protected]; [email protected]
Abstract: Interpersonal psychotherapy (IPT) is a time-limited, structured, interpersonally oriented psychotherapy, with demonstrated efficacy for the treatment of major depression across the lifespan. IPT uses a medical model of illness and links depressed mood to four research-informed interpersonal problem areas: complicated grief, role transitions, role disputes, and interpersonal deficits/sensitivity. The IPT model of vulnerability to depression nicely dovetails with interpersonal issues that are faced by older adults, and this article focuses on the application of IPT for late-life depression in China. The group format of IPT may be a practical and efficient method of improving access to an established depression-focused treatment for China’s rapidly aging population and has the advantage of providing important social support for patients who feel lonely, isolated, and stigmatized. Short-term interventions like IPT are more cost-effective from a public health perspective and can easily be delivered in primary care facilities, where many elderly patients receive care. IPT is effective in different cultures, and possible cultural adaptations of IPT for older adults in China are discussed herein.
Keywords: interpersonal psychotherapy, late-life depression, cultural adaptation, China
Interpersonal psychotherapy (IPT) is a brief, manualized psychotherapy with demonstrated efficacy for the treatment of major depression.1 Introduced in the 1970s, IPT is recognized as a first-line psychosocial treatment for major depressive disorder2–4 and has been adapted and shown to be effective in treating depression across the lifespan, as well as other disorders such as bipolar disorder, eating disorder, and post-traumatic stress disorder.5,6 In the current article, we focus on IPT for the treatment of late-life depression (LLD) and its potential application in China.
Brief Overview of IPT for Depression
IPT was developed by Weissman et al as a manualized, time-limited (usually 12–16 weekly sessions) intervention for adult outpatients with unipolar depression. Influenced by attachment, interpersonal, and social theories of the 1940s and 1950s, as well as empirical research demonstrating a link between adverse life events and depressed mood and the protective effect of social supports against depression, IPT is concerned with the bidirectional interaction between interpersonal events and depressed mood.1,7 Thus, when bad things happen to people mood is affected and when mood is depressed people do not handle their interpersonal world effectively, causing further interpersonal adversity and worsening of mood. IPT conceptualizes depression as a medical illness and adopts the concept of the “sick role”.7 Comparing depression to other medical illnesses and giving the patient the sick role are intended to reduce blame associated with developing depression, reduce demoralization and feelings of guilt associated with impairment caused by depressive symptoms (eg, making mistakes at work due to poor concentration), instill a sense of hope that depression is treatable, motivate the patient to work hard in therapy so they can recover as quickly as possible, and facilitate combining psychotherapy and pharmacotherapy if medication is considered necessary.7
IPT is a focal intervention that links the depressive episode to one or two interpersonal problem areas that are considered salient to the onset and maintenance of the patient’s symptoms: complicated grief following the death of an important attachment; role transitions, which involve difficulty adjusting to changed life circumstances that affect people’s feelings about themselves and others; role disputes, which involve nonreciprocal expectations between the patient and a significant other; and interpersonal deficits/sensitivity, which involves difficulty forming and maintaining interpersonal relationships.7 Reduction of depressive symptoms is achieved by facilitating resolution of these interpersonal problems and helping patients build and strengthen social supports. Maintaining the interpersonal focus of treatment is important in IPT as this prevents the therapy from becoming too diffuse and pushes the therapist and patient to use their time efficiently and discuss material that is relevant to the identified interpersonal problem area and treatment objectives.7
The therapy is structured and includes three phases (beginning, middle, and end), with each phase associated with specific therapeutic tasks. A summary of these tasks is provided in Table 1. The therapeutic strategies and techniques used in IPT are designed to help the patient master interpersonal difficulties associated with current depressive symptoms and prevent depression relapse. Some of the key techniques used in IPT include communication analysis, encouragement and exploration of affect, exploration of options for change, decision analysis, clarification, role play, and use of the therapeutic relationship. A full description of IPT techniques can be found in the updated and expanded version of the IPT manual by Weissman et al.7 This updated manual has been translated into Chinese.
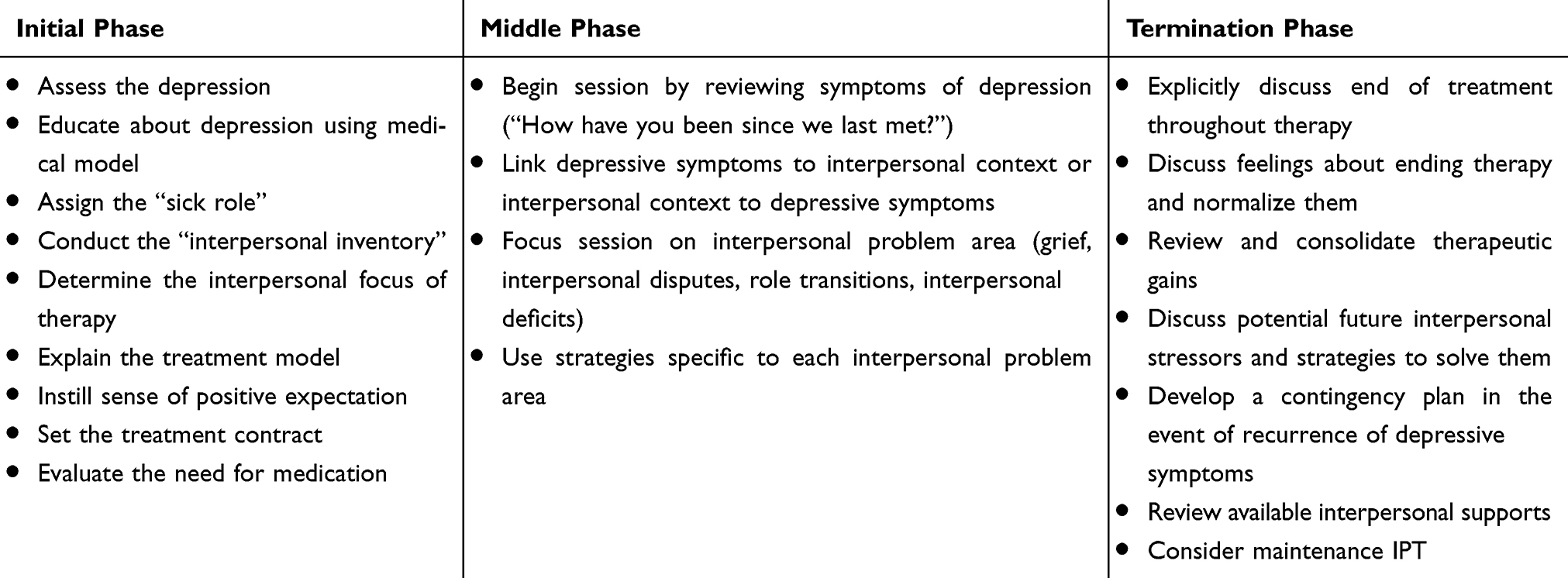 |
Table 1 Main Tasks of Three Phases of IPT |
Since the publication of the initial trials of IPT in the 1970s and findings from the landmark National Institute of Mental Health Treatment of Depression Collaborative Research Program,8 which demonstrated that IPT was superior to pill placebo, similar to imipramine for mild to moderate depression, and slightly better than cognitive behavior therapy (CBT) for severe depression, research on IPT for depression has flourished both in the US, where it was conceived and initially tested, and internationally. A recent meta-analysis involving 11,434 participants concluded that IPT is equally as effective as CBT,6 and as effective as antidepressant drugs in treating mild to moderately severe depression.9 These psychological interventions also appear to have more durable effects than medication. For some adult and elderly patients with chronic depression, the combination of medication and psychotherapy produces the best outcome.10
IPT for Late-life Depression
Depression is a common psychiatric disorder in older adults and is associated with reduced quality of life, disability, risk of suicide, and mortality.11,12 Nearly 10–25% of people 60 years and older suffer from depression worldwide.13–15 Studies report that on average, 22.6% of the elderly in China suffer from depressive symptoms, with prevalence varying as a function of gender, geographic regions, socioeconomic status, and education levels.16–19 Irrespective of culture, depressive symptoms in late life are often atypical compared to younger patients, and include irritability, apathy, somatic symptoms, and cognitive decline.20–22 Variants of depression in late life have also been described and include depression without sadness, depletion syndrome, and depression-executive function.23 Cognitive impairment is relatively common in LLD and involves deficits in executive function, attention, and memory.24 A neuropathological link between LLD and dementia has been proposed,25,26 with depression considered both a risk factor for and symptom of cognitive decline.24
Despite the high prevalence of LLD and associated impairment, elderly patients in China underutilize mental health services because of stigma of mental illness in traditional Chinese culture and poor mental health literacy.27,28 Although Chinese elderly are more inclined to seek treatment for mental health problems in primary care as less stigma is associated with primary care treatment,28 the majority of elderly patients treated in primary care or in the community receive inadequate or no treatment for their depression.27 Depression in the elderly in China and elsewhere is often underdetected,28,29 and once identified treatment is not always optimal, with more than 60% of patients remaining depressed at 12-month follow-up.29 Pharmacotherapy is often the first choice of treatment for LLD worldwide, however, the efficacy of antidepressant medication tends to be modest and a substantial number of patients require additional treatment.30 Further, concomitant drug therapies for medical comorbidities and adverse effects may limit the extent to which antidepressant drugs are suitable for elderly patients, especially those who are frail.31 Psychotherapy is a valuable alternative for older depressed patients who cannot tolerate antidepressant medications, for those who may benefit from combination medication and psychotherapy, and for those who prefer a nonpharmacological approach for symptom relief.9,32 Indeed, older depressed patients often express a preference for psychotherapy over medication,33,34 and mental health specialists endorse psychotherapy, including IPT, as an important frontline treatment option for LLD.3
The IPT model of vulnerability to depression nicely dovetails with interpersonal issues that are faced by older adults and that increase risk for depression. Examples include difficulty adjusting to changes in social roles brought about by retirement and other life circumstances; loss of independence due to medical illness, disability, and diminished mobility; disputes with significant others; and loss of network supports and attachments due to death and relocation.35–37 Further, a meta-analysis confirmed that social support, quality of relations, and presence of confidants can decrease risk for depression in late life.38 Studies conducted in older people in China similarly report that social support, especially support from family members, is protective against depression39 and that interpersonal stressors increase depression vulnerability;40 these include poor marital status, childlessness, social isolation and loneliness, medical illness, bereavement, and having impious offspring.16,17,41,42 Family conflict is one of the strongest predictors of suicide in elderly Chinese,42 and a case–control psychological autopsy study of completed suicides in elderly Chinese living in rural areas43 found that being left behind by offspring who migrated to urban areas elevated risk for suicide; this association was mediated through increased life stress, presence of depressive symptoms and other mental disorders, and decreased social supports. Overall, these findings highlight the relevance of evidence-based psychosocial treatments that specifically target interpersonal processes in LLD and risk for suicide.
IPT has been extensively evaluated in cognitively intact elderly depressed patients. While the effects of acute treatment are generally modest, IPT is comparable in efficacy to antidepressant medications but without the associated adverse events.44,45 In primary care settings, IPT delivered by mental health practitioners produced a better outcome than physician usual care and supportive clinical management.34,46 However, among older patients with bereavement-related depression, IPT works best when combined with medication.47 In contrast to acute IPT treatment, the evidence for maintenance IPT is less clear, with some studies reporting that maintenance treatment confers protection against depression relapse35,36 and others reporting no demonstrable benefit in preserving well-being achieved with acute and continuation treatment.47 Lack of response to maintenance IPT may be a function of age, with higher relapse rates found in those with advanced age (ie, those >70 years old) vs younger age (ie, those <70 years).48 Chronic poor health, residual anxiety, sleep disturbance, cognitive difficulties, and continual loss of psychosocial resources may contribute to increased risk for relapse in older patients,48,49 who may benefit more from a combination of maintenance IPT and medication than monotherapy.48
While IPT for LLD does not require substantive adaptation for patients who are cognitively intact, working with older patients who are cognitively impaired may present important challenges in psychotherapy. These patients may have more difficulty engaging in psychotherapy and are more dependent on their caregivers for activities of daily living.50 Miller adapted IPT for depressed older patients with mild cognitive impairment (IPT-CI),50 and found the therapy could be successfully implemented with this patient population and improve depressive symptoms.51–53 In this adaptation of IPT, caregivers are integrated in the therapeutic process; this is intended to educate the caregiver about depression and cognitive impairment, provide them with an opportunity to discuss challenges they face with their own “role transition” as a caregiver, provide a forum for discussing interpersonal role disputes between the patient and caregiver, and promote engagement of caregivers to improve patient treatment adherence.50 Although IPT-CI is a promising intervention for cognitively impaired depressed older patients, its efficacy has not been rigorously evaluated in randomized trials.
In addition to individual therapy, IPT has been adapted for delivery in a group format. Group IPT (IPT-G) for LLD may be especially relevant in China, a country with the world’s largest aging population. Indeed in 2018, older people accounted for 17.9% of the total population in China54 and it is estimated that by 2040, one in four people will be 60 years and older.55 Considering this trend and reported economic burden of depression in China, IPT-G represents a cost-effective format of delivering evidence-based psychosocial care to elderly depressed patients and one that can be delivered in the community or primary care centers, where depressed elderly people are initially screened and treated. IPT-G was initially developed by Wilfley et al for the treatment of bulimia.56 The fundamental structure of IPT-G is similar to the individual format of IPT and an individual session with the therapist is integrated before, midway, and after the group intervention. Therapists also provide patients with written group summaries after each session which are intended to stimulate patient reflection after each session and encourage them to work on their identified problem area. Scocco et al developed a slightly adapted version of Wilfley’s IPT-G manual for depressed elderly patients. In this version of IPT-G, pre- and postgroup individual meetings are scheduled but there is no mid-treatment individual session and weekly group summary reports are not provided.57 There are no randomized controlled trials of IPT-G for LLD with or without cognitive impairment. Nevertheless, this IPT modality may be of particular benefit to elderly patients who are socially isolated and lonely, and provides a forum for patients to practice adaptive communication and interpersonal skills that can be transferred to real life interpersonal circumstances.57 Although concerns about perceived stigma and discomfort sharing personal problems with strangers may reduce willingness of elderly people in China to participate in group therapy, research suggests that elderly Chinese have a generally positive attitude toward group interventions and they show good treatment engagement.58
In addition to the group format of IPT described above, a simplified version of group IPT has been developed for countries where access to trained mental health specialists is limited.7 The intervention can be delivered by supervised lay therapists with little or no formal training in mental health, and is endorsed by the World Health Organization to improve the scalability of effective psychological interventions in low-to-middle-income countries. There are no published trials of this group version of IPT in depressed elderly, however, randomized controlled trials conducted in Uganda have demonstrated that IPT delivered by nonexpert facilitators is superior to a control intervention in reducing depressive symptoms and dysfunction.59,60 Despite positive findings from the Ugandan studies, it remains unclear if group IPT delivered by nonspecialist providers would be perceived as a credible and acceptable treatment option by the depressed elderly in China. Nevertheless, similar to many other countries, access to evidence-based psychotherapies remains problematic in China, especially in rural and remote regions where there is a grave shortage of mental health specialists. Developing innovative models of mental health care that scales up the provision of effective and affordable short-term psychotherapies like IPT should be an important priority for the management and care of the depressed elderly in China.
Selection of Suitable Candidates for IPT and IPT vs Other Psychotherapies for Late-life Depression
Although patient selection is an important issue related to treatment success, limited research exists regarding what type of psychological intervention works best for a particular individual with LLD. A systematic review of studies comprising mainly nonelderly patients found that few reproducible patient and clinical characteristics moderated IPT’s effects relative to other treatments.61 However, there is some evidence that efficacy of IPT may be less effective than CBT in depressed patients with avoidant personality disorder. While depressed patients with personality pathology can be difficult to treat, many patients with depression, especially chronic depression, present with cluster C personality features that are partly due to the depression itself. Although IPT does not directly address personality change, its emphasis on resolving interpersonal problems and building adaptive interpersonal skills has been found to reduce cluster C and other personality disorder symptoms in patients who received maintenance IPT.62 Thus, consideration of IPT as a treatment option for depressed elderly with personality pathology is warranted, although longer duration of treatment and use of adjunctive treatment may be necessary.
In addition, older patients with varying levels of cognitive impairment may not fully benefit from IPT compared to noncognitively impaired patients due to their difficulties engaging in psychotherapy, maintaining attention during sessions, or recalling discussions from prior sessions. An important issue, therefore, is to determine what level of cognitive impairment severity would render a patient unsuitable for IPT. Recommendations for providing IPT to cognitively impaired elderly patients have been proposed and include: the ability to communicate with others, awareness that a problem exists, motivation to resolve the problem, and some capacity for retention.63
In addition to IPT other short-term manualized therapies have shown efficacy for LLD including CBT and problem-solving therapy (PST).44,45,64 Although these therapies are based on different theoretical models of depression, a common feature is that they focus primarily on current rather than historical issues, as is the case with psychodynamic therapy. CBT and IPT are the best researched psychological therapies for depression and good candidates for cultural adaptation based on their strong empirical support.65,66 PST was developed more recently and is a variant of CBT that focuses on learning adaptive problem-solving skills. There is growing evidence supporting its beneficial effects on mood and cognitive function in older adults.67,68, Although there are no head-to-head comparisons of IPT vs other psychotherapies for LLD, meta-analyses of psychotherapy studies for depression in nonelderly patients suggest that IPT works as well as other psychotherapies,69,70 with one analysis suggesting a slight advantage of IPT.70 Based on these findings, one might expect IPT to work as well as other established psychotherapies for LLD. As no one treatment works for everyone, having multiple effective psychological approaches to choose from is important for the care of depressed elderly patients. Recommendation of IPT over other effective approaches to treating depression should be based on the presence of social and interpersonal problems that are temporally linked to the development of depressive symptoms,6 the availability of trained IPT therapists, and importantly, on patients’ goals and treatment preference.
Cultural Considerations in the Application of IPT for LLD in China
With the opening-and-reform policies initiated in the 1980s, China has re-entered the global environment, experimenting with theories and concepts of psychotherapies that were originally developed within the context of Western culture. Research on the cultural aspects of psychological interventions suggest that culture may influence the practice and processes of psychotherapy in subtle ways.71 The prototype of interpersonal relations in China is rooted in Confucian philosophy that advocates harmony, moderation, and balance. This philosophy continues to influence popular beliefs and social behavior of contemporary Chinese.72,73 Researchers in multiculturalism in psychotherapy have proposed that culturally competent psychotherapy requires three levels of adjustments: technical adjustments, theoretical modifications, and philosophical reorientation.74 Treatment modalities that take into account traditional Chinese values and history from a broad perspective, and include modifications that meet the cultural needs and preferences of patients, may improve therapeutic outcome. For example, the efficacy of CBT for Chinese people has been found to be more robust when the intervention is culturally adapted than when it is not.75 Nevertheless, it is important not to overgeneralize cultural differences or assume that elderly Chinese are a homogeneous group that share the same kind of cultural beliefs and values. The theories and techniques of mainstream psychotherapies are universally applicable and depressed elderly Chinese have been found to respond well to psychotherapies developed in Western countries without adaptation.76
Generally, researchers and clinicians agree that interpersonal problem areas of IPT are universal and that the intervention makes clinical sense regardless of geography.7 IPT research conducted in China77,78 and other non-Western cultures7 seems to suggest few modifications are required and that the core elements of IPT are well preserved. Still, IPT may need to be culturally adapted to enhance its relevance, meaningfulness, and effectiveness.79,80 For example it may be preferable to rename the four interpersonal problem areas into colloquial expressions.7 Another example of possible cultural consideration relates to family interdependence and filial piety. Unlike some cultures in North America and elsewhere that socialize offspring to become independent and autonomous, Chinese culture is prototypically collectivistic and the centrality of the family unit makes family interdependence acceptable and desirable throughout the individual’s lifespan. At the same time, family interdependence can lead to interpersonal conflict. The one-child policy established in China in 1979 has also altered the dynamic of parent–child relationships, creating potential burdens and conflicts within families that can lead to psychological distress.81
Relatedly, children are an important source of emotional, instrumental and financial support to elderly parents. Filial piety (xiao) is highly valued in Chinese culture, especially among elderly rural Chinese who are more likely to adhere to traditional family cultural values than their urban counterparts. However, attitudes towards filial obligations have changed in contemporary China and a lack of congruence between what the elderly parent and adult offspring and grandchildren considered as filial behavior may strain intergenerational relationships. China has also witnessed important transformations of family ties and residential patterns,55 particularly in rural China, where migration of adult workers to urban centers has eroded the traditional intergenerational family support mechanism that is vital to the well-being of elderly.81 Difficulty adjusting to changes in traditional family living arrangements can increase risk for depression in the elderly, especially if there is loss of tangible and intangible supports, added burdens, and lost social roles and status. Risk for disruption in support patterns and increased negative parent–child interactions may be particularly high if caring for the elderly parent becomes an inconvenience or a financial burden for adult migrant children.82,83 Approximately 50% of Chinese rural older adults are empty nesters or “left behind” and rates of depression in this subgroup of elderly is higher than the general elderly population in China.84
In working with intergenerational interpersonal disputes, the therapist can frame IPT goals (eg, developing more flexible expectations of others, accepting that which cannot change, focusing on more positive aspects of the relationship and modifying faulty communication) as a means to restore and maintain harmony in relationships and achieve an acceptable balance between the needs of the self and those of others. For those facing changes in traditional family structure or other life circumstances, exploring feelings of loss associated with the change and identifying positive aspects of change and opportunities are important IPT strategies. Examining viable options to maintain a satisfactory level of contact and support from family members would also be a key focus of IPT, as family support is pivotal for the well-being of Chinese elderly and preferred over other forms of support.85 Although elderly Chinese may be reticent to seek support outside the family unit, establishing a broader network of support that includes friends, neighbors, and community resources should be encouraged, especially from those who share the patient’s experience and who can provide emotional support. As dependent patterns are often observed in elderly women raised in traditional Chinese culture, enhancing self-efficacy may be an important therapeutic goal, especially for women who are widowed or live alone.86 Incorporating culturally rooted proverbs or traditional Chinese philosophy may also help foster a better understanding of the relational and social context of depressive symptoms and facilitate effective coping with interpersonal disputes and changes in life circumstances.79
Chinese culture also needs to be considered for the IPT problem area of complicated bereavement. Every culture has its unique attitudes concerning death and grieving rituals and Chinese culture is no different in this regard.87 Unfortunately, very little research on grief in general and pathological grief in particular has been conducted in China.88 Despite the limited research base, preliminary data on spousal bereavement suggests that elderly Chinese respond better to a grief intervention that focuses both on grief work and restorative-oriented coping (ie, reconstructing identity, seeking social supports, dealing with family, friends, and neighbors) than an intervention that focuses mainly on grief work.89 Thus, IPT’s dual goals of facilitating the mourning process and re-establishing interests and social supports fits well with this model. Because avoidance of expression of grief is common among Chinese90 and may result in failure to successfully integrate the loss, the early sessions of IPT should focus on grief feelings and the loss, with later sessions focusing on restoration of interests and supports. While discussing negative or ambivalent feelings towards the deceased is encouraged in IPT, this may require modification in working with bereaved elderly Chinese as honoring the deceased is important in Chinese culture. Certain culture-related grief beliefs may also contribute to greater levels of depression and grief severity in Chinese elderly and these beliefs should also be addressed in therapy. For example, the bereaved may experience intense guilt and self-blame if they were unable to facilitate a “good death” for the deceased.91
In general, studies suggest Chinese people tend to prefer time-limited, directive, goal-oriented, and pragmatic approaches,80 which generally fits well with IPT. Although the therapist-patient relationship in IPT is collaborative and the patient is encouraged to generate their own options for resolving interpersonal issues and strengthening social supports, the therapist can take an active and directive therapeutic stance if needed and maintain the role of expert. This therapeutic stance aligns well with the more hierarchical provider–patient relationship preferred by many elderly Chinese patients.80 Chinese elderly also report a preference for words such as stress or wellness instead of depression, and may require more psychoeducation about problems related to distress, mood, mind–body connection, and the collaborative nature of the therapist–patient relationship.80 Cultural differences in expression of affect also need to be considered. While IPT is an affect-focused intervention and encouragement of affect is a key technique that facilitates therapeutic change, many Chinese people are uncomfortable talking about difficult emotions and tend to express their distress somatically. The IPT therapist must therefore gently encourage patients to talk about difficult feelings within the supportive therapeutic relationship, normalize and validate feelings, and help them find appropriate ways to communicate their needs and feeling with others. It should be mentioned that much of what we know about the impact of Chinese culture on psychotherapy is generally based on therapist impressions rather than on the patient’s own experience and perception of psychotherapy. More research is therefore needed to obtain a clearer picture of how Chinese culture can inform adaptations of IPT for LLD.
Conclusion
In summary, LLD is common in elderly Chinese patients and is associated with significant morbidity and mortality. Available research makes a strong case for the role of interpersonal factors in precipitating and maintaining depressive symptoms in elderly Chinese and the interpersonal focus of IPT makes it an ideal intervention for depressed older adults, even for those with some mild cognitive impairment. IPT works for people from diverse cultural backgrounds and can easily be adapted to accommodate Chinese cultural values. The strong empirical base for the efficacy of IPT for depression can also address issues related to perception of treatment credibility and acceptability by elderly patients and their families, leading to better treatment uptake, adherence, and response. Considering China’s rapidly aging population, the group format of IPT delivered by trained therapists may be a practical and efficient method of improving access to an established treatment for LLD, and has the advantage of providing important social support for patients who feel lonely, isolated, and stigmatized. Although long-term psychodynamic therapy has a long history in China and is still a widely practiced treatment modality, Chinese people tend to prefer short-term approaches. Further, from a public health perspective, short-term interventions like IPT are more cost-effective and can also be easily delivered in primary care facilities where the majority of elderly patients are treated. As no treatment benefits all depressed patients, it is advantageous to have an array of effective therapies and psychotherapists in China and competencies should be developed in more than one of them.
Interest in evidence-based therapies is growing in academic and clinical communities in China. Several academic hospitals have organized IPT workshops for mental health specialists (eg, Renji Hospital and Shanghai Mental Health Center, Shanghai) and advanced training via distance supervision by IPT supervisors from the US, Canada, and elsewhere is currently underway with clinicians working in academic centers (eg, Xiangya Second Hospital, Central South University, Changsha, Hunan). Developing IPT trainers and supervisors in China is an important initiative as this will contribute to the training and development of competent IPT therapists and help promote the dissemination of IPT in China. Finally, rigorously designed research of IPT needs to be carried out in China, and it is our hope that innovative research on the efficacy and mechanisms of different formats of IPT for LLD will be developed in this country.
Author Contributions/Acknowledgments
Hua Xu drafted the manuscript. Diana Koszycki supervised Dr Xu and made critical revisions of the manuscript for important intellectual content. We would also like to thank Jacques Bradwejn (University of Ottawa, University of Montreal, and Shanghai Jiao Tong University School of Medicine) for helpful comments. All authors made substantial contributions to conception and design, took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Markowitz JC, Weissman MM. Interpersonal psychotherapy: past, present and future. Clin Psychol Psychother. 2012;19(2):99–105. doi:10.1002/cpp.1774
2. Karasu TB, Gelenberg A, Wang P, et al. Practice guideline for the treatment of patients with major depressive disorder (revision). Am J Psychiatry. 2000;157(4 Suppl):1–45.
3. Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry. 2010;71(Suppl):e04. doi:10.4088/JCP.9058se1c.04gry
4. Parikh SV, Quilty LC, Ravitz P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 2. Psychological treatments. Can J Psychiatry. 2016;61(9):524–539. doi:10.1177/0706743716659418
5. Ravitz P, Watson P, Lawson A, et al. Interpersonal psychotherapy: a scoping review and historical perspective (1974–2017). Harv Rev Psychiatry. 2019;27(3):165–180. doi:10.1097/HRP.0000000000000219
6. Cuijpers P, Donker T, Weissman MM, et al. Interpersonal psychotherapy for mental health problems: a comprehensive meta-analysis. Am J Psychiatry. 2016;173(7):680–687. doi:10.1176/appi.ajp.2015.15091141
7. Weissman MM, Markowitz JC, Klerman GL, et al. The Guide to Interpersonal Psychotherapy: Updated and Expanded Edition. Oxford University Press; 2018.
8. Elkin I, Shea MT, Watkins JT, et al. National institute of mental health treatment of depression collaborative research program. General effectiveness of treatments. Arch Gen Psychiatry. 1989;46(11):971–982. doi:10.1001/archpsyc.1989.01810110013002
9. Cuijpers P, Geraedts AS, van Oppen P, et al. Interpersonal psychotherapy for depression: a meta-analysis. Am J Psychiatry. 2011;168(6):581–592. doi:10.1176/appi.ajp.2010.10101411
10. Hollon SD, Jarrett RB, Nierenberg AA, et al. Psychotherapy and medication in the treatment of adult and geriatric depression: which monotherapy or combined treatment? J Clin Psychiatry. 2005;66(4):455–468. doi:10.4088/JCP.v66n0408
11. Morimoto SS, Kanellopoulos D, Manning KJ, et al. Diagnosis and treatment of depression and cognitive impairment in late life. Ann N Y Acad Sci. 2015;1345:36–46. doi:10.1111/nyas.12669
12. Vaughan L, Corbin AL, Goveas JS. Depression and frailty in later life: a systematic review. Clin Interv Aging. 2015;10:1947–1958.
13. Forlani C, Morri M, Ferrari B, et al. Prevalence and gender differences in late-life depression: a population-based study. Am J Geriatr Psychiatry. 2014;22(4):370–380. doi:10.1016/j.jagp.2012.08.015
14. Blazer D, Williams CD. Epidemiology of dysphoria and depression in an elderly population. Am J Psychiatry. 1980;137(4):439–444.
15. Niino N, Ihara K, Suzuki T, et al. Prevalence of depressive symptoms among the elderly: a longitudinal study. Geriatr Gerontol Int. 2003;3:27–30. doi:10.1111/j.1444-0594.2003.00093.x
16. Zhong BL, Xu YM, Xie WX, et al. Depressive symptoms in elderly chinese primary care patients: prevalence and sociodemographic and clinical correlates. J Geriatr Psychiatry Neurol. 2019;32(6):312–318. doi:10.1177/0891988719862620
17. Chou KL, Chi I. Prevalence and correlates of depression in Chinese oldest-old. Int J Geriatr Psychiatry. 2005;20(1):41–50. doi:10.1002/gps.1246
18. Woo J, Ho SC, Lau J, et al. The prevalence of depressive symptoms and predisposing factors in an elderly Chinese population. Acta Psychiatr Scand. 1994;89(1):8–13. doi:10.1111/j.1600-0447.1994.tb01478.x
19. Yu J, Li J, Cuijpers P, et al. Prevalence and correlates of depressive symptoms in Chinese older adults: a population-based study. Int J Geriatr Psychiatry. 2012;27(3):305–312. doi:10.1002/gps.2721
20. Ismail Z, Fischer C, McCall WV. What characterizes late-life depression? Psychiatr Clin North Am. 2013;36(4):483–496. doi:10.1016/j.psc.2013.08.010
21. Campos C, Nogueira CH, Fernandes L. Aging, circadian rhythms and depressive disorders: a review. Am J Neurodegener Dis. 2013;2(4):228–246.
22. Vilalta-Franch J, Planas-Pujol X, López-Pousa S, et al. Depression subtypes and 5-years risk of mortality in aged 70 years: a population-based cohort study. Int J Geriatr Psychiatry. 2012;27(1):67–75. doi:10.1002/gps.2691
23. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5:363–389. doi:10.1146/annurev.clinpsy.032408.153621
24. Taylor WD. Clinical practice. Depression in the elderly. N Engl J Med. 2014;371(13):1228–1236. doi:10.1056/NEJMcp1402180
25. Leyhe T, Reynolds CF
26. Kim HK, Nunes PV, Oliveira KC, et al. Neuropathological relationship between major depression and dementia: A hypothetical model and review. Prog Neuropsychopharmacol Biol Psychiatry. 2016;67:51–57. doi:10.1016/j.pnpbp.2016.01.008
27. Li X, Xiao Z, Xiao S. Suicide among the elderly in mainland China. Psychogeriatrics. 2009;9(2):62–66. doi:10.1111/j.1479-8301.2009.00269.x
28. Chen S, Conwell Y, Vanorden K, et al. Prevalence and natural course of late-life depression in China primary care: a population based study from an urban community. J Affect Disord. 2012;141(1):86–93. doi:10.1016/j.jad.2012.02.027
29. Barry LC, Abou JJ, Simen AA, et al. Under-treatment of depression in older persons. J Affect Disord. 2012;136(3):789–796. doi:10.1016/j.jad.2011.09.038
30. Kok RM, Nolen WA, Heeren TJ. Efficacy of treatment in older depressed patients: a systematic review and meta-analysis of double-blind randomized controlled trials with antidepressants. J Affect Disord. 2012;141(2–3):103–115. doi:10.1016/j.jad.2012.02.036
31. Nelson JC, Delucchi K, Schneider LS. Efficacy of second generation antidepressants in late-life depression: a meta-analysis of the evidence. Am J Geriat Psychiatry. 2008;16(7):558–567. doi:10.1097/01.JGP.0000308883.64832.ed
32. de Mello MF, de Jesus Mari J, Bacaltchuk J, et al. A systematic review of research findings on the efficacy of interpersonal therapy for depressive disorders. Eur Arch Psychiatry Clin Neurosci. 2005;255(2):75–82. doi:10.1007/s00406-004-0542-x
33. van Schaik DJ, van Marwijk H, Beekman A, et al. Interpersonal psychotherapy (IPT) for late-life depression in general practice: uptake and satisfaction by patients, therapists and physicians. BMC Fam Pract. 2007;8:52. doi:10.1186/1471-2296-8-52
34. van Schaik A, van Marwijk H, Adèr H, et al. Interpersonal psychotherapy for elderly patients in primary care. Am J Geriatr Psychiatry. 2006;14(9):777–786. doi:10.1097/01.JGP.0000199341.25431.4b
35. Reynolds CF
36. Reynolds CF
37. Hinrichsen GA. Interpersonal psychotherapy: a treatment for late-life depression. Psychiatr Ann. 2009;39(9):838–843. doi:10.3928/00485713-20090821-05
38. Schwarzbach M, Luppa M, Forstmeier S, et al. Social relations and depression in late life-a systematic review. Int J Geriatr Psychiatry. 2014;29(1):1–21. doi:10.1002/gps.3971
39. Chen R, Wei L, Hu Z, et al. Depression in older people in rural China. Arch Intern Med. 2005;165(17):2019–2025. doi:10.1001/archinte.165.17.2019
40. Li N, Pang L, Chen G, et al. Risk factors for depression in older adults in Beijing. Can J Psychiatry. 2011;56(8):466–473. doi:10.1177/070674371105600804
41. Yang K, Victor CR. The prevalence of and risk factors for loneliness among older people in China. Ageing Soc. 2008;28(3):305–327. doi:10.1017/S0144686X07006848
42. Li M, Katikireddi SV. Urban-rural inequalities in suicide among elderly people in China: a systematic review and meta-analysis. Int J Equity Health. 2019;18(1):2. doi:10.1186/s12939-018-0881-2
43. Zhou L, Wang G, Jia C, et al. Being left-behind, mental disorder, and elderly suicide in rural China: a case–control psychological autopsy study. Psychol Med. 2018;49(3):458–464. doi:10.1017/S003329171800106X
44. Pinquart M, Duberstein PR, Lyness JM. Treatments for later-life depressive conditions: a meta-analytic comparison of pharmacotherapy and psychotherapy. Am J Psychiatry. 2006;163(9):1493–1501. doi:10.1176/ajp.2006.163.9.1493
45. Cuijpers P, Karyotaki E, Pot AM, et al. Managing depression in older age: psychological interventions. Maturitas. 2014;79(2):160–169. doi:10.1016/j.maturitas.2014.05.027
46. Schulberg HC, Magruder KM, deGruy F. Major depression in primary medical care practice. Research trends and future priorities. Gen Hosp Psychiatry. 1996;18(6):395–406. doi:10.1016/S0163-8343(96)00093-X
47. Reynolds CF
48. Reynolds CF
49. Dombrovski AY, Mulsant BH, Houck PR, et al. Residual symptoms and recurrence during maintenance treatment of late-life depression. J Affect Disord. 2007;103(1–3):77–82. doi:10.1016/j.jad.2007.01.020
50. Miller MD. Clinician’s Guide to Interpersonal Psychotherapy in Late Life: Helping Cognitively Impaired or Depressed Elders and Their Caregivers. Oxford University Press; 2009.
51. Reynolds CF
52. Kok RM, Reynolds CF
53. Miller MD, Reynolds CF
54. Population distribution by broad age group in China. 2019. Available from: https://www.statista.com/statistics/251524/population-distribution-by-age-group-in-china/.
55. Zhang Y, Goza FW. Who will care for the elderly in China?: a review of the problems caused by China’s one-child policy and their potential solutions. J Aging Stud. 2006;20(2):151–164. doi:10.1016/j.jaging.2005.07.002
56. Wilfley DE, Frank ML, Welch R, et al. Adapting Interpersonal Psychotherapy to a Group Format (IPT-G) for binge eating disorder: toward a model for adapting empirically supported treatments. Psychother Res. 1998;8(4):379–391. doi:10.1093/ptr/8.4.379
57. Scocco P, Leo DD, Frank E. Is interpersonal psychotherapy in group format a therapeutic option in late-life depression? Clin Psychol Psychother. 2002;9(1):68–75. doi:10.1002/cpp.301
58. Chong A. Reminiscence group for Chinese older people-a cultural consideration. J Gerontol Soc Work. 2000;34(2):7–22. doi:10.1300/J083v34n02_03
59. Bolton P, Bass J, Betancourt T, et al. Interventions for depression symptoms among adolescent survivors of war and displacement in northern Uganda: a randomized controlled trial. JAMA. 2007;298(5):519–527. doi:10.1001/jama.298.5.519
60. Bolton P, Bass J, Neugebauer R, et al. Group interpersonal psychotherapy for depression in rural Uganda: a randomized controlled trial. JAMA. 2003;289(23):3117–3124. doi:10.1001/jama.289.23.3117
61. Bernecker SL, Coyne AE, Constantino MJ, et al. For whom does interpersonal psychotherapy work? A systematic review. Clin Psychol Rev. 2017;56:82–93. doi:10.1016/j.cpr.2017.07.001
62. Cyranowski JM, Frank E, Winter E, et al. Personality pathology and outcome in recurrently depressed women over 2 years of maintenance interpersonal psychotherapy. Psychol Med. 2004;34(4):659–669. doi:10.1017/S0033291703001661
63. Hinrichsen GA. Interpersonal psychotherapy for late life depression: current status and new applications. J Ration Emot Cogn Behav Ther. 2008;26(4):263–275. doi:10.1007/s10942-008-0086-5
64. Kirkham JG, Choi N, Seitz DP. Meta-analysis of problem solving therapy for the treatment of major depressive disorder in older adults. Int J Geriatr Psychiatry. 2016;31(5):526–535. doi:10.1002/gps.4358
65. Comas-Díaz L. Latino healing: the integration of ethnic psychology into psychotherapy. Psychotherapy (Chic). 2006;43(4):436–453. doi:10.1037/0033-3204.43.4.436
66. Munoz RF, Mendelson T. Toward evidence-based interventions for diverse populations: the San Francisco General Hospital prevention and treatment manuals. J Consult Clin Psychol. 2005;73(5):790–799. doi:10.1037/0022-006X.73.5.790
67. Alexopoulos GS, Raue PJ, Kiosses DN, et al. Problem-solving therapy and supportive therapy in older adults with major depression and executive dysfunction: effect on disability. Arch Gen Psychiatry. 2011;68(1):33–41. doi:10.1001/archgenpsychiatry.2010.177
68. Alexopoulos GS, Raue PJ, Kanellopoulos D, et al. Problem solving therapy for the depression-executive dysfunction syndrome of late life. Int J Geriatr Psychiatry. 2008;23(8):782–788. doi:10.1002/gps.1988
69. Jakobsen JC, Hansen JL, Simonsen S, et al. Effects of cognitive therapy versus interpersonal psychotherapy in patients with major depressive disorder: a systematic review of randomized clinical trials with meta-analyses and trial sequential analyses. Psychol Med. 2012;42(7):1343–1357. doi:10.1017/S0033291711002236
70. Cuijpers P, van Straten A, Andersson G, et al. Psychotherapy for depression in adults: a meta-analysis of comparative outcome studies. J Consult Clin Psychol. 2008;76(6):909–922. doi:10.1037/a0013075
71. Tung M. Insight-oriented psychotherapy and the Chinese patient. Am J Orthopsychiatry. 1991;61(2):186–194. doi:10.1037/h0079249
72. Fan Y, Pool B. A classification of Chinese culture. Int J Cross Cult Manag. 2000;7(2):3–10. doi:10.1108/13527600010797057
73. Li MG, Duan C, Ding BK, et al. Psychotherapy integration in modern china. J Psychother Pract Res. 1994;3(4):277–283.
74. Tseng WS. Culture and psychotherapy: asian perspectives. J Ment Health. 2009;13(2):151–161.
75. Ng TK, Wong DF. The efficacy of cognitive behavioral therapy for Chinese people: a meta-analysis. Aust N Z J Psychiatry. 2018;52(7):620–637. doi:10.1177/0004867417741555
76. Dai B, Lie J, Cuijpers P. Psychological treatment of depressive symptoms in Chinese elderly inpatients with significant medical comorbidity: a meta-analysis. BMC Psychiatry. 2011;11:92. doi:10.1186/1471-244X-11-92
77. Jiang RF, Tong HQ, Delucchi KL, et al. Interpersonal psychotherapy versus treatment as usual for PTSD and depression among Sichuan earthquake survivors: a randomized clinical trial. Confl Health. 2014;8:14. doi:10.1186/1752-1505-8-14
78. Tang TC, Jou SH, Ko CH, et al. Randomized study of school-based intensive interpersonal psychotherapy for depressed adolescents with suicidal risk and parasuicide behaviors. Psychiatry Clin Neurosci. 2009;63(4):463–470. doi:10.1111/j.1440-1819.2009.01991.x
79. Tseng WS. Culture and psychotherapy: asian perspectives. J Ment Health. 2004;13(2):151–161.
80. Chu JP, Huynh L, Areán P. Cultural adaptation of evidence-based practice utilizing an iterative stakeholder process and theoretical framework: problem solving therapy for Chinese older adults. Int J Geriatr Psychiatry. 2012;27(1):97–106. doi:10.1002/gps.2698
81. Cheung CK, Kwan AY. The erosion of filial piety by modernisation in Chinese cities. Ageing Soc. 2009;29(2):179–198. doi:10.1017/S0144686X08007836
82. Wu ZQ, Sun L, Sun YH, et al. Correlation between loneliness and social relationship among empty nest elderly in Anhui rural area, China. Aging Ment Health. 2010;14(1):108–112. doi:10.1080/13607860903228796
83. Krause N, Liang J. Stress, social support, and psychological distress among the Chinese elderly. J Gerontology. 1993;48(6):282–291. doi:10.1093/geronj/48.6.P282
84. He G, Xie JF, Zhou JD, et al. Depression in left‐behind elderly in rural China: prevalence and associated factors. Geriatr Gerontol Int. 2016;16(5):638–643. doi:10.1111/ggi.12518
85. Li H, Ji Y, Chen T. The roles of different sources of social support on emotional well-being among Chinese elderly. PLoS One. 2014;9(3):e90051. doi:10.1371/journal.pone.0090051
86. Chen Y, Nettles ME, Chen SW. Rethinking dependent personality disorder: comparing different human relatedness in cultural contexts. J Nerv Ment Dis. 2009;197(11):793–800. doi:10.1097/NMD.0b013e3181be76ae
87. Pressman DL, Bonanno GA. With whom do we grieve? Social and cultural determinants of grief processing in the United States and China. J Soc Pers Relat. 2007;24(5):729–746. doi:10.1177/0265407507081458
88. Chow AY. Death in the family–bereavement and mourning in contemporary China. In: Handbook on the Family and Marriage in China. Edward Elgar Publishing; 2017;373–391.
89. Chow AYM, Caserta M, Lund D, et al. Dual-Process Bereavement Group Intervention (DPBGI) for widowed older adults. Gerontologist. 2019;59(5):983–994. doi:10.1093/geront/gny095
90. Bonanno GA, Papa A, Lalande K, et al. Grief processing and deliberate grief avoidance: a prospective comparison of bereaved spouses and parents in the United States and the People’s Republic of China. J Consult Clin Psychol. 2005;73(1):86–98. doi:10.1037/0022-006X.73.1.86
91. Chan CL, Chow AY, Ho SM, et al. The experience of Chinese bereaved persons: A preliminary study of meaning making and continuing bonds. Death Stud. 2005;29(10):923–947. doi:10.1080/07481180500299287
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.