Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Intermanual Transfer Effects on Performance Gain Following Dominant Hand Training in Community-Dwelling Healthy Adults: A Preliminary Study
Authors Beg RA ![]() , Shaphe MA
, Shaphe MA ![]() , Qasheesh M, Ahmad F, Anwer S, Alghadir AH
, Qasheesh M, Ahmad F, Anwer S, Alghadir AH
Received 24 December 2020
Accepted for publication 6 April 2021
Published 30 April 2021 Volume 2021:14 Pages 1007—1016
DOI https://doi.org/10.2147/JMDH.S298991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rashid Ali Beg,1 Mohammad Abu Shaphe,1 Mohammed Qasheesh,1 Fuzail Ahmad,2 Shahnawaz Anwer,3,4 Ahmad H Alghadir3
1Department of Physical Therapy, Jazan University, Jazan, Saudi Arabia; 2Department of Physical Therapy & Health Rehabilitation, College of Applied Medical Science, Majmaah University, Majmaah, Saudi Arabia; 3Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 4Department of Building and Real Estate, Hong Kong Polytechnic University, Hong Kong
Correspondence: Shahnawaz Anwer
Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Building 24, G095-1, P.O. Box. 10219, Riyadh, 11433, Saudi Arabia
Email [email protected]
Purpose: This study aimed to evaluate the intermanual transfer effects of dominant hand training on the functional task of the untrained hand.
Methods: Fifty community-dwelling healthy adults (mean age, 23.4 ± 2.5 Y; females, 60%) were participated. Participants in the experimental group received 15 minutes of right-hand training on a pegboard apparatus twice a week for four weeks. The control group received no training. The Jebsen Taylor test (JTT) and a 16-hole pegboard test were used for the assessment of hand function and dexterity.
Results: Most of the JTT subtests except the writing and simulated feeding subtests and the performance of pegboard task by untrained hand were significantly improved in the experimental group after 4 weeks of training. However, no changes in the untrained hand function after 4 weeks in the control group. There were no significant differences in the pegboard task and JTT subtests found at baseline between the two groups. There were significant differences in the pegboard task between the two groups after dominant hand training. The experimental group took 4.3- and 2.5-second lesser time to complete the pegboard task using the dominant and non-dominant hand, respectively. Similarly, most of the JTT subtests except the writing and simulated feeding subtests were significantly better in the training group than the control group.
Conclusion: This study indicates that the function of the untrained non-dominant hand may be improved after functional training of the dominant hand. Since this study included only healthy young adults, results of this study cannot be generalized to other groups of people such as the elderly. While this study suggests that intermanual transfer could have a therapeutic value in many clinical situations, more longitudinal studies are warranted to examine the intermanual transfer effects of functional gain in different clinical conditions, such as stroke, parkinsonism, rheumatoid arthritis, and so on.
Keywords: intermanual transfer, cross transfer, cross education, dominant hand, hand training, hand function
Introduction
The foundation of transfer of learning is one of the essential factors for learning any task.1 Schmidt et al2 defined transfer as “gain in the ability of performing one task as a result of practice or experience in some other task”. Morton et al3 suggested that the adaptation of a movement could be transferred to the other limb and to different arm configurations within the same limb. Similarly, Fu et al4 have demonstrated an association between the perception produced by the untrained and the trained limb. Therefore, the cross transfer is a circumstance in which an untrained limb improves some performance due to contra lateral limb training.5
The actions of muscles on one side of the body greatly influence the comparable muscles on the contralateral side of the body.6 This effect is known as “cross-education” or more commonly as “cross-transfer”.7 A previous study examined the cross-transfer effects of movement time on the forearm muscles of healthy adults, and they have demonstrated increased performance in both trained and untrained hands.8 Another study reported improved final position accuracy of the nondominant arm following dominant arm training.9 Furthermore, Wang and Sainburg10 showed that dominant arm training significantly improved linearity and initial limb control in the nondominant arm. The mechanism of cross-transfer from the trained limb to the untrained limb can be attributed to bilateral left hemispheric control,11,12 cross-activation, and callosal access of motor engrams stored in the dominant hemisphere via the corpus callosum.13 Various methods are commonly used to minimize the negative effects of long-term immobilization on muscle tissue. One of the possible options could be the use of a healthy limb exercise program to indirectly activate the muscles of the injured limb via a cross-transfer mechanism.14 This is also known as intermanual transfer of training.15
Motor learning is a continuous process, which starts with an acquisition of a task and progresses with the transfer of the task.16 Previous studies have suggested that variability in task and strength training could facilitate the intermanual transfer of motor learning.17–19 Another study reported that the training effects of a pegboard task were demonstrated in untrained hands.20 While some studies indicate that intermanual transfer is only occurring from the dominant to nondominant hands,21–24 others suggest that transfer may occur from nondominant to dominant25–27 or it may transfer equally from both hands.3,28 Therefore, this study aimed to evaluate the intermanual transfer effects of dominant hand training on the functional task of an untrained nondominant hand.
Materials and Methods
Subjects
Fifty community-dwelling healthy adults were participated and randomly divided into two groups (experimental and control) using the computer-generated random numbers (Figure 1). Participants were recruited from the locality of Riyadh and the study was conducted at Rehabilitation research chair, King Saud University between July 5, 2020 and November 10, 2020. The inclusion criteria were as follows: a) age, 20–30 years; b) dominance, right handedness as per the Edinburgh handedness inventory;29,30 and c) individuals free from any medical, surgical, and neurological conditions that may affect upper limb function. The participants were excluded if they had a history of neurological disorders with reduced upper limb function, musculoskeletal disorders of the upper limb, or upper limb injury or surgery. The participants were asked to give written informed consent prior to their participation in the study. The study protocol was approved by the Institutional Ethics Subcommittee, Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia. All the procedures were conducted according to the guidelines given in the Declaration of Helsinki.
 |
Figure 1 Flow diagram for study procedure. |
Instrumentation
The following instruments were used in this study: (a) stopwatch; (b) back supported chair (height, 18 inches); (c) pegboard apparatus with 16 pegs; and (d) Jebsen Taylor test (JTT) board and accessories.31–33
Training
Participants in the experimental group received 15 minutes of right-hand training on a 16-hole pegboard apparatus twice a week for four weeks. The control group received no training. During the training sessions, participants were asked to sit on a wooden chair in front of a pegboard apparatus. The participants were trained to place each peg in the hole one by one using their dominant hand as fast as possible starting from the most distant hole.
Outcomes
Both the outcomes were evaluated by a senior physical therapist who had experience of using the outcomes, which was used in this study. Outcome assessor was blinded to the group allocations.
Jebsen Taylor Test (JTT) for Hand Function
The JTT was designed to assess objective and standardized hand function.31–33 It comprised of seven subtests to evaluate various activities of daily living using both hands. JTT is a reliable and valid test to identify individuals with limited hand function in a variety of health conditions.34–37 Past studies have reported good to excellent inter- and intra-rater reliability of JTT (ICC = 0.82–1.00) in people with stroke37 and elderly populations.36 The seven subtests of JTT are as follows: (a) Subtest 1 – Writing; (b) Subtest 2 – Card turning; (c) Subtest 3 – Small common objects putting; (d) Subtest 4 – Simulated feeding; (e) Subtest 5 – Checkers Stacking; (f) Subtest 6 – Light cans placing; and (g) Subtest 7 – Heavy cans placing. The dominant hand was used for writing the test.29 All tasks in the JTT were performed in a sitting position. A stopwatch was used to measure the time needed to complete each task.37 The participants were asked to complete the JTT test with dominant and non-dominant hands. One familiarization trial was given before two test trials. One minute of rest was given between the two subsets. The time taken to complete each test and to complete the entire JTT were the outcomes. The total time required to complete the task was considered as the outcome (eg, the lower time to complete the task is considered to have a better hand function).33 Likewise, a posttest assessment of JTT subtests was conducted after 4 weeks of training to investigate improvements in hand function after dominant hand training.
Pegboard Task Test for Hand Dexterity
A 16-hole pegboard apparatus, which was used for the training purpose, was also used for the assessment of hand dexterity.38 The participants were asked to place pegs into the holes as fast as possible without dropping the peg. A stopwatch was used to measure the time needed to complete the task. Both hands were assessed separately. One familiarization trial was given before two test trials. The total time required to complete the task was used as the outcome. Similarly, a second assessment of the pegboard task was administered after 4 weeks of training to evaluate changes in hand function after dominant hand training.
Statistical Analysis
Data were analyzed using the statistical program for social studies (SPSS, Window version 22, IBM). Paired and independent t-tests were used to assess within- and between-group differences in outcomes, respectively. Bonferroni corrections were applied for multiple comparisons. Additionally, the effect sizes for pegboard task and JTT tests were calculated using Cohen’s d (d = <0.5, small; d = 0.50 to 0.80, medium; and d >0.80, large) to evaluate clinically meaningful changes.39 A p<0.05 was considered for a statistically significant test.
Results
Fifty healthy adults (male, 20; Female, 30) from the community were participated. The demographic data indicate an insignificant difference in age between the experimental (23.40 ± 2.46 Y) and control (23.32 ± 2.56 Y) groups. Both the dominant and nondominant hand functions measured by the pegboard task and the JTT were significantly improved in the experimental group (Table 1). Participants in the experimental group took 5- and 2.2-second lesser time to complete the pegboard task by dominant and nondominant hands, respectively. Similarly, participants in the experimental group took significantly lesser time to complete most of the JTT tasks except the writing and simulated feeding tasks after dominant hand training (Table 1). However, participants in the control group showed statistically insignificant changes in the dominant and nondominant hand function during the pegboard task and JTT (Table 2).
 |
Table 1 Changes in Hand Functions After Training in Experimental Group |
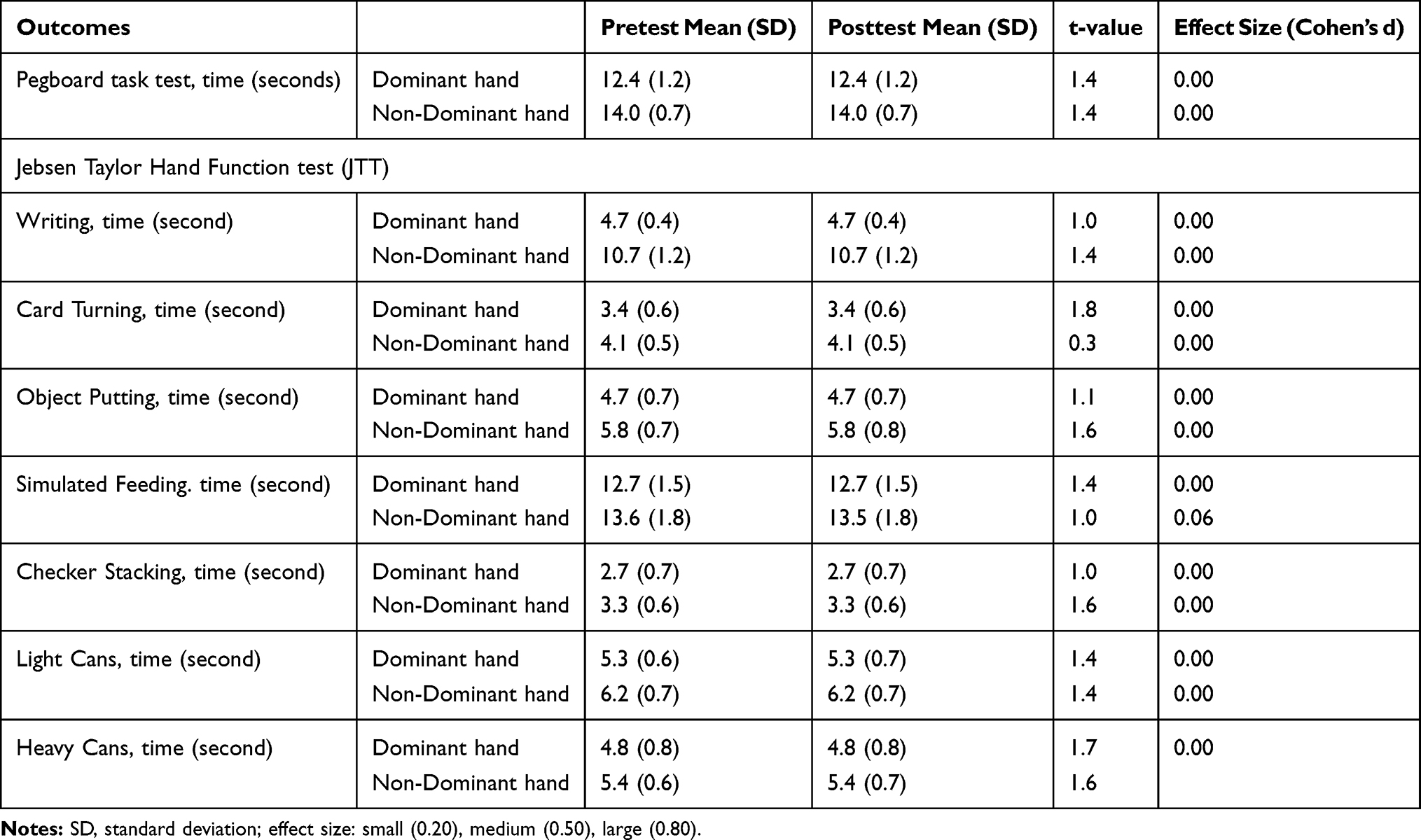 |
Table 2 Changes in Hand Functions After Training in Control Group |
The baseline scores of dominant and nondominant hand functions during the pegboard and JTT tasks are given in Table 3. There were no significant differences in the pegboard and JTT tasks between the groups at baseline (Table 3). There were significant differences in the pegboard task test between the groups after the dominant hand training (Table 4). Participants in the experimental group took 4.3 seconds (dominant hand) and 2.5 seconds (nondominant hand) lesser time to complete the pegboard task as compared to the control group. Similarly, participants in the experimental group completed most of the JTT subtests except the writing and simulated feeding subtests faster than the control group (Table 4). The experimental group took significantly lesser time to complete the card turning (dominant hand, 0.7 sec; nondominant hand, 0.2 sec), object putting (dominant hand, 1.6 sec; nondominant hand, 1.2 sec), checker stacking (dominant hand, 1.6 sec; nondominant hand, 1.2 sec), light cans (dominant hand, 0.7 sec; nondominant hand, 0.6 sec), and heavy cans (dominant hand, 0.5 sec; nondominant hand, 0.3 sec) subtests of JTT than the control group.
 |
Table 3 Intergroup Comparison of Hand Functions at Baseline |
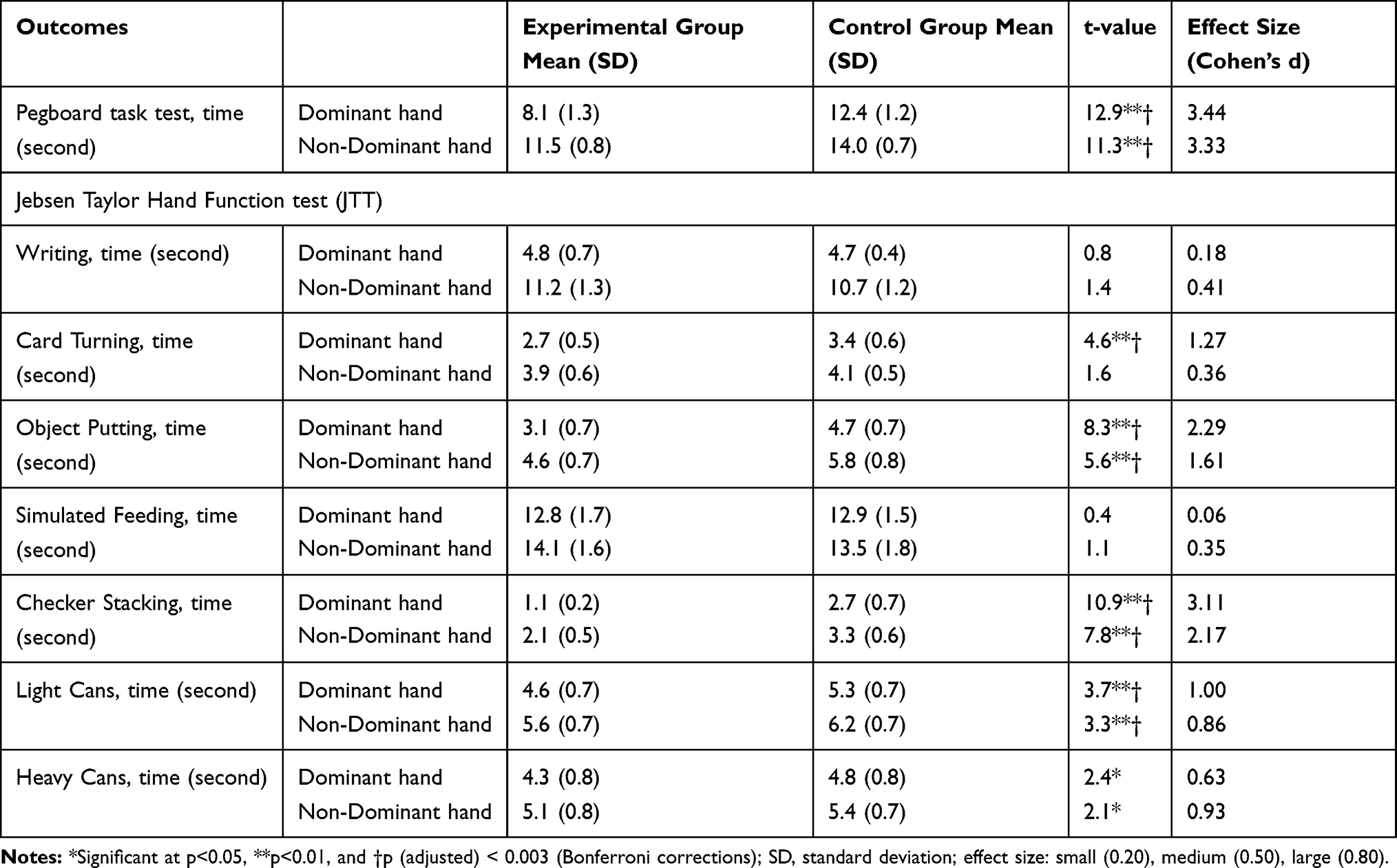 |
Table 4 Intergroup Comparison of Hand Functions After Training (at Posttest) |
Discussion
The current study aimed to evaluate the effects of intermanual transfer of training on the functional task of the untrained hand after 4 weeks of dominant hand training. The results revealed a significant reduction in movement time to complete a pegboard task after an intensive dominant hand training. Transfer of training also occurred to the contralateral nondominant hand as the movement time of the nondominant hand was also reduced to perform the pegboard task. Gain in performance occurred in similar functional tasks in both the trained and untrained hands. Transfers of training were also clinically meaningful as determined by large effect sizes (Cohen’s d > 0.8) for the pegboard task and most of the subsets of JTT in the participants who participated in dominant hand training.
The current study uses a pegboard task that has been extensively used in neuropsychology for the assessment of complex hand functions.40–42 The pegboard task is a type of sensorimotor task that requires a visual stimulus for a specific response to reach, grasp, and place pegs into the specified holes.43 Such visuomotor task training results in progressive changes in hand function, initially slow, inaccurate, and uncoordinated functions to fast, accurate, and coordinated functions. This improvement in hand function may be attributed to changes in underlying processes, for example, motor planning and programming.44 In the current study, training with the dominant hand may produce adaptation in the dominant hemisphere, which was later utilized to perform the task with the nondominant hand.45
The transfer of dominant hand training to an untrained nondominant hand may be explained by three proposed mechanisms of intermanual transfer of training. One of the proposed mechanisms suggests that the same hemisphere may control both the trained and untrained hands and therefore learning of one hand might transfer to the learning of the other hand functions.11 A previous study suggested that the dominant hemisphere may effectively control the nondominant hand.12 Furthermore, another study reported that a lesion in the left cortical area caused marked movement impairment in the contralateral arm with some movement impairment in the ipsilateral arm.46 Another mechanism for transfer of learning to an untrained hand was proposed by Taylor and Heilman and is known as the callosal access model.47 As per this mechanism, motor engrams are originally formed after dominant hand training and stored in the dominant hemisphere. The contralateral hemisphere of the corpus callosum may have access to these engrams. The third mechanism for transfer of learning to untrained hands was proposed by Parlow and Kinsbourne and is known as intermanual transfer of training.48 This mechanism suggests that the copy of learned information for dominant hand training may be synchronously stored in the non-dominant hemisphere.13 Subsequently, the nondominant cortex works independently of the dominant motor cortex and may help improve the function of the untrained nondominant hand.
In the current study, hand functions in both trained and untrained hands were improved in similar tasks. Since grasping is the main task used in the current study, the results of this study may be explained by the internal representations underlying grasping. The pegboard task and JTT subtests used a similar kind of grip, and therefore an internal model for the representation of the type of grip formed during training. This is consistent with the findings which suggest that mechanical properties and behavior of limbs stored in the higher cortex may consequently be used for anticipatory scaling of motor commands during reaching and grasping.4 Another study suggests that intrinsic object properties, including object size, are important for determining the grip along with hand transport and preshaping.49 Similarly, other studies also suggested that the same strategy for applying force is used when handling commonly used objects with a similar grip.4,50 Therefore, the current results are consistent with the evidence that supports internal neural representations of the grip utilized during training and may later be used for performing JTT subtests, such as stacking checkers and putting small objects. The performance of these subtests was also improved in the untrained hand, which could either be explained based upon the formation of an internal mechanism in the dominant cortex and ipsilateral control of the left cortex or transfer of information from the dominant to nondominant cortex.51
Some improvements in the performance of the JTT subtests of turning cards and placing light and heavyweight cans have also been noted in this study, which could be the result of dimensional generalization from learned motions of reaching movements.52 The pegboard task is a visuomotor task that uses reaching, grasping, and placing strategies, which is like card turning and placing of light and heavyweight cans used reaching, grasping, and placing strategies. Therefore, when the practice on a pegboard is learned, an internal map of the desired trajectory is formed. Subsequently, a motor action that produces reaching movements is created by the brain with the help of desired trajectories. However, generalization has been found to occur beyond the region of training.52
Study Limitations and Future Research Directions
This study acknowledges many potential limitations. First, the participants in this study were healthy young adults, which limits the generalizability of the results in other groups of people or clinical conditions, such as the elderly or individuals with immobilized one limb after fracture. Therefore, future studies are required to evaluate the intermanual transfer effects in different populations or clinical conditions, such as individuals with an immobilized upper or lower extremity after fracture. Second, since this study examined intermanual effects on hand function, it remains unknown whether intermanual transfer also occurred on muscle strength gain. Future studies should investigate the intermanual transfer effects of strength training of unaffected upper or lower extremities on muscle strength gain in the affected upper or lower extremities. Such investigation of clinical conditions is important for evaluating the validity and application of intermanual transfer effects during rehabilitation. Finally, the current study uses a similar task for training and evaluating intermanual transfer effects. For example, initially participants were trained on a pegboard task followed by testing the transfer effects using the same pegboard task or JTT test, both of which use the reaching, grasping, and placing strategies. Since the participants became very familiar with the format/use of the pegboard as opposed to truly gaining functional fine motor skills, it remains unknown whether intermanual transfer effects could also occur in different tasks. For instance, range of motion exercise or strength training of one extremity can improve the function of the contralateral extremities. Future studies are warranted to explore the possible application of intermanual transfer effects in different neurological or musculoskeletal disorders.
Clinical Implications
Individuals with immobilized or impaired one upper or lower extremity due to fracture or neurological conditions (eg, stroke) may not be able to use their affected limb during physical exercise or functional training. Consequently, the strength and function of the affected limb gradually diminishes. Therefore, muscles of the affected limb can be indirectly activated via training of the unaffected limbs using the concept of intermanual transfer to prevent muscle weakness and functional impairment of the affected limb.14 Additionally, intermanual transfer training can be used to train prosthetic limbs in people with amputation.15 Individuals with amputated upper or lower limbs often start learning prosthetic skills after getting the prosthesis. However, they could start the prosthetic training immediately after the amputation using the intermanual transfer, so that training of the unaffected limb could enhance the prosthetic skills of the affected limb.53,54 Consequently, the acceptance and handling of the prosthesis would be improved.
Conclusions
This study indicates that the function of the untrained nondominant hand may be improved after functional training of the dominant hand. Since this study included only healthy young adults, results of this study cannot be generalized to other groups of people such as the elderly. While this study suggests that intermanual transfer could have a therapeutic value in many clinical situations, more longitudinal studies are warranted to examine the intermanual transfer effects of functional gain in different clinical conditions, such as stroke, parkinsonism, rheumatoid arthritis, and so on.
Data Sharing Statement
The dataset of this manuscript is available on reasonable request through the corresponding author.
Acknowledgments
The authors are grateful to the Deanship of Scientific Research, King Saud University for funding through Vice Deanship of Scientific Research Chairs.
Disclosure
The authors report no conflicts of interest with respect to authorship, research content, and/or publication of this manuscript.
References
1. Parisi GI, Kemker R, Part JL, Kanan C, Wermter S. Continual lifelong learning with neural networks: a review. Neural Networks. 2019;113:54–71. doi:10.1016/j.neunet.2019.01.012
2. Schmidt SL, Oliveira RM, Krahe TE, Filgueiras CC. The effects of hand preference and gender on finger tapping performance asymmetry by the use of an infra-red-light measurement device. Neuropsychologia. 2000;38(5):529–534. doi:10.1016/S0028-3932(99)00120-7
3. Morton SM, Lang CE, Bastian AJ. Inter-and intra-limb generalization of adaptation during catching. Exp Brain Res. 2001;141(4):438–445. doi:10.1007/s002210100889
4. Fu Q, Shao F, Santello M. Inter-limb transfer of grasp force perception with closed-loop hand prosthesis. IEEE Trans Neural Syst Rehabil Eng. 2019;27(5):927–936. doi:10.1109/TNSRE.2019.2911893
5. Romkema S, Bongers RM, van der Sluis CK. Influence of mirror therapy and motor imagery on intermanual transfer effects in upper-limb prosthesis training of healthy participants: a randomized pre-posttest study. PLoS One. 2018;13(10):e0204839. doi:10.1371/journal.pone.0204839
6. Lee M, Carroll TJ. Cross education. Sports Med. 2007;37(1):1–4. doi:10.2165/00007256-200737010-00001
7. Rider BA. Effects of neuromuscular facilitation on cross transfer. Am J Occup Ther. 1971;25(2):84–89.
8. Nagel MJ, Rice MS. Cross-transfer effects in the upper extremity during an occupationally embedded exercise. Am J Occup Ther. 2001;55(3):317–323. doi:10.5014/ajot.55.3.317
9. Wang J, Sainburg RL. Mechanisms underlying interlimb transfer of visuomotor rotations. Exp Brain Res. 2003;149(4):520–526. doi:10.1007/s00221-003-1392-x
10. Wang J, Sainburg RL. Interlimb transfer of novel inertial dynamics is asymmetrical. J Neurophysiol. 2004;92(1):349–360. doi:10.1152/jn.00960.2003
11. Lee M, Hinder MR, Gandevia SC, Carroll TJ. The ipsilateral motor cortex contributes to cross‐limb transfer of performance gains after ballistic motor practice. J Physiol. 2010;588(1):201–212. doi:10.1113/jphysiol.2009.183855
12. Shadmehr R, Criscimagna-Hemminger SE, Donchin O, Gazzaniga MS. Learned dynamics of reaching movements generalize. J Neurophysiol. 2010;103(4):2275–2284. doi:10.1152/jn.00822.2009
13. Jung D, Park JW, Kim YH, You JS. Neuroplastic and motor behavioral changes after intermanual transfer training of non-dominant hand: a prospective fMRI study. NeuroRehabilitation. 2019;44(1):25–35. doi:10.3233/NRE-182550
14. Green LA, Gabriel DA. The effect of unilateral training on contralateral limb strength in young, older, and patient populations: a meta-analysis of cross education. Phys Therapy Rev. 2018;23(4–5):238–249. doi:10.1080/10833196.2018.1499272
15. Romkema S, Bongers RM, van der Sluis CK. Influence of the type of training task on intermanual transfer effects in upper-limb prosthesis training: a randomized pre-posttest study. PLoS One. 2017;12(11):e0188362. doi:10.1371/journal.pone.0188362
16. Sigrist R, Rauter G, Riener R, Wolf P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: a review. Psychon Bull Rev. 2013;20(1):21–53.
17. Kitago TO, Krakauer JW. Motor learning principles for neurorehabilitation. Handb Clin Neurol. 2013;110:93–103.
18. Censor N, Cohen LG. Using repetitive transcranial magnetic stimulation to study the underlying neural mechanisms of human motor learning and memory. J Physiol. 2011;589(1):21–28. doi:10.1113/jphysiol.2010.198077
19. Carroll TJ, Selvanayagam VS, Riek S, Semmler JG. Neural adaptations to strength training: moving beyond transcranial magnetic stimulation and reflex studies. Acta physiologica. 2011;202(2):119–140. doi:10.1111/j.1748-1716.2011.02271.x
20. Schulze K, Lüders E, Jäncke L. Intermanual transfer in a simple motor task. Cortex. 2002;38(5):805–815. doi:10.1016/S0010-9452(08)70047-9
21. Mostafa AA, Salomonczyk D, Cressman EK, Henriques DY. Intermanual transfer and proprioceptive recalibration following training with translated visual feedback of the hand. Exp Brain Res. 2014;232(6):1639–1651. doi:10.1007/s00221-014-3833-0
22. Taylor JA, Wojaczynski GJ, Ivry RB. Trial-by-trial analysis of intermanual transfer during visuomotor adaptation. J Neurophysiol. 2011;106(6):3157–3172. doi:10.1152/jn.01008.2010
23. Chase C, Seidler R. Degree of handedness affects intermanual transfer of skill learning. Exp Brain Res. 2008;190(3):317–328. doi:10.1007/s00221-008-1472-z
24. Farthing JP. Cross-education of strength depends on limb dominance: implications for theory and application. Exerc Sport Sci Rev. 2009;37(4):179–187. doi:10.1097/JES.0b013e3181b7e882
25. Panzer S, Krueger M, Muehlbauer T, Kovacs AJ, Shea CH. Inter-manual transfer and practice: coding of simple motor sequences. Acta psychologica. 2009;131(2):99–109. doi:10.1016/j.actpsy.2009.03.004
26. Bagesteiro LB, Sainburg RL. Nondominant arm advantages in load compensation during rapid elbow joint movements. J Neurophysiol. 2003;90(3):1503–1513. doi:10.1152/jn.00189.2003
27. Kirsch W, Hoffmann J. Asymmetrical intermanual transfer of learning in a sensorimotor task. Exp Brain Res. 2010;202(4):927–934. doi:10.1007/s00221-010-2184-8
28. Amemiya K, Ishizu T, Ayabe T, Kojima S. Effects of motor imagery on intermanual transfer: a near-infrared spectroscopy and behavioural study. Brain Res. 2010;1343:93–103. doi:10.1016/j.brainres.2010.04.048
29. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 1971;9(1):97–113. doi:10.1016/0028-3932(71)90067-4
30. McMeekan ER, Lishman WA. Retest reliabilities and interrelationship of the Annett hand preference questionnaire and the Edinburgh handedness inventory. Br J Psychol. 1975;66(1):53–59. doi:10.1111/j.2044-8295.1975.tb01439.x
31. Stern EB. Stability of the Jebsen-Taylor Hand Function Test across three test sessions. Am J Occup Ther. 1992;46(7):647–649. doi:10.5014/ajot.46.7.647
32. Sears ED, Chung KC. Validity and responsiveness of the Jebsen–Taylor hand function test. J Hand Surg Am. 2010;35(1):30–37. doi:10.1016/j.jhsa.2009.09.008
33. Jebsen RH, Taylor NE, Trieschmann RB, Trotter MJ, Howard LA. An objective and standardized test of hand function. Arch Phys Med Rehabil. 1969;50(6):311–319.
34. Mak MK, Lau ET, Tam VW, Woo CW, Yuen SK. Use of Jebsen Taylor Hand Function Test in evaluating the hand dexterity in people with Parkinson’s disease. J Hand Therapy. 2015;28(4):389–395. doi:10.1016/j.jht.2015.05.002
35. Alonso CC, de Freitas PB, Pires RS, De oliveira DL, Freitas SM. Accuracy, Sensitivity, and Specificity of Different Tests to Detect Impaired Hand Function in Parkinson's disease. medRxiv. 2020.
36. Hackel ME, Wolfe GA, Bang SM, Canfield JS. Changes in hand function in the aging adult as determined by the Jebsen Test of Hand Function. Phys Ther. 1992;72(5):373–377. doi:10.1093/ptj/72.5.373
37. Bovend Eerdt TJ, Dawes H, Johansen-Berg H, Wade DT. Evaluation of the Modified Jebsen Test of Hand Function and the University of Maryland Arm Questionnaire for Stroke. Clin Rehabil. 2004;18(2):195–202. doi:10.1191/0269215504cr722oa
38. Proud EL, Bilney B, Miller KJ, Morris ME, McGinley JL. Measuring Hand Dexterity in People with Parkinson’s Disease: reliability of Pegboard Tests. Am J Occup Ther. 2019;73(4):7304205050p1–8. doi:10.5014/ajot.2019.031112
39. Gärtner R, Jensen MB, Kronborg L, Ewertz M, Kehlet H, Kroman N. Self-reported arm-lymphedema and functional impairment after breast cancer treatment–a nationwide study of prevalence and associated factors. Breast. 2010;19(6):506–515. doi:10.1016/j.breast.2010.05.015
40. Duffield TC, Trontel HG, Bigler ED, et al. Neuropsychological investigation of motor impairments in autism. J Clin Exp Neuropsychol. 2013;35(8):867–881. doi:10.1080/13803395.2013.827156
41. Buddenberg LA, Davis C. Test–retest reliability of the Purdue Pegboard Test. Am J Occup Ther. 2000;54(5):555–558. doi:10.5014/ajot.54.5.555
42. Bryden PJ, Roy EA. A new method of administering the Grooved Pegboard Test: performance as a function of handedness and sex. Brain Cogn. 2005;58(3):258–268. doi:10.1016/j.bandc.2004.12.004
43. Backman C, Gibson SC, Parsons J. Assessment of hand function: the relationship between pegboard dexterity and applied dexterity. Canadian J Occupational Therapy. 1992;59(4):208–213. doi:10.1177/000841749205900406
44. de Guise E, Del Pesce M, Foschi N, Quattrini A, Papo I, Lassonde M. Callosal and cortical contribution to procedural learning. Brain. 1999;122(6):1049–1062. doi:10.1093/brain/122.6.1049
45. Philip BA, Frey SH. Increased functional connectivity between cortical hand areas and praxis network associated with training-related improvements in non-dominant hand precision drawing. Neuropsychologia. 2016;87:157–168. doi:10.1016/j.neuropsychologia.2016.05.016
46. Wyke M. Effect of brain lesions on the rapidity of arm movement. Neurology. 1967;17(11):1113. doi:10.1212/WNL.17.11.1113
47. Taylor HG, Heilman KM. Left-hemisphere motor dominance in right handersi. Cortex. 1980;16(4):587–603. doi:10.1016/S0010-9452(80)80006-2
48. Parlow SE, Kinsbourne M. Asymmetrical transfer of training between hands: implications for interhemispheric communication in normal brain. Brain Cogn. 1989;11(1):98–113. doi:10.1016/0278-2626(89)90008-0
49. Gentilucci M, Castiello U, Corradini ML, Scarpa M, Umilta C, Rizzolatti G. Influence of different types of grasping on the transport component of prehension movements. Neuropsychologia. 1991;29(5):361–378. doi:10.1016/0028-3932(91)90025-4
50. Jenmalm P, Goodwin AW, Johansson RS. Control of grasp stability when humans lift objects with different surface curvatures. J Neurophysiol. 1998;79(4):1643–1652. doi:10.1152/jn.1998.79.4.1643
51. Gordon AM, Forssberg H, Iwasaki N. Formation and lateralization of internal representations underlying motor commands during precision grip. Neuropsychologia. 1994;32(5):555–568. doi:10.1016/0028-3932(94)90144-9
52. Shadmehr R, Moussavi ZM. Spatial generalization from learning dynamics of reaching movements. J Neurosci. 2000;20(20):7807–7815. doi:10.1523/JNEUROSCI.20-20-07807.2000
53. Malone JM, Fleming LL, Roberson J, et al. Immediate, early, and late postsurgical management of upper-limb amputation. J Rehabil Res Dev. 1971;25(1):33–41.
54. Gaine WJ, Smart C, Bransby-Zachary M. Upper limb traumatic amputees. Review of prosthetic use. J Hand Surg Br. 1997;22:73–76. doi:10.1016/S0266-7681(97)80023-X
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.