Back to Journals » International Journal of General Medicine » Volume 19
Interleukin-Mediated Inflammatory Pathways and Nerve Injury in Lumbar Disc Herniation: A Narrative Review
Received 30 January 2026
Accepted for publication 24 March 2026
Published 26 March 2026 Volume 2026:19 600123
DOI https://doi.org/10.2147/IJGM.S600123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Dongwei Wang,1 Delai Zhao,2 Xiaoning Li3
1Graduate School, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, 150040,People’s Republic of China; 2Department of Orthopedics, Harbin Fifth Hospital, Harbin, Heilongjiang, 150000, People’s Republic of China; 3Department of Acupuncture and Moxibustion, The Second Affiliated Hospital of Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, 150001, People’s Republic of China
Correspondence: Xiaoning Li, Department of Acupuncture and Moxibustion, The Second Affiliated Hospital of Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, 150001, People’s Republic of China, Email [email protected]
Objective: This is a narrative review aimed to explore the molecular biosciences mechanisms by which interleukin (IL) networks and inflammatory pathways mediate nerve injury in lumbar disc herniation (LDH), providing translational insights for therapy.
Methods: We screened PubMed and Embase databases from January 2010 to January 2026 to search for published studies. The search keywords used are as follows: [“lumbar disc herniation” or “LDH”], [“ interleukin” or “IL” or “Interleukin Network”], [“Nerve Injury”], [“Inflammatory”]. A total of 196 peer-reviewed studies were included, comprising 152 experimental studies (128 animal models, 24 in vitro cell experiments) and 44 human clinical studies, with a human-to-animal study ratio of approximately 1:2.9.
Results: Preclinical mechanistic studies indicate that pro-inflammatory interleukins such as IL-1β, IL-6 and IL-17 lead to nerve root demyelination, axonal degeneration and neuropathic pain by activating NLRP3, JAK-STAT3 and p38MAPK pathways. Anti-inflammatory interleukins including IL-4 and IL-10 produce neuroprotective effects through inducing M2 macrophage polarization. Clinical evidence shows that interleukin levels are related to the severity of radicular pain and neurological deficits. Targeted biologics, TCM and acupuncture can regulate interleukin signaling to relieve symptoms. This review is structured with a three-part framework that includes interleukin characteristics and inflammatory signaling in LDH, interleukin-mediated mechanisms of nerve injury and translational interventions as well as clinical challenges.
Conclusion: In the future, it can be transformed into clinical practice of LDH through the development of targeted biologics, the combination of standardized traditional Chinese and Western medicine protocols, and the evaluation of biomarkers based on interleukin.
Keywords: lumbar disc herniation, interleukins, inflammatory signaling pathway, nerve injury, signal transduction, treatment outcome
Introduction
Lumbar disc herniation (LDH) is a globally prevalent degenerative spinal disorder.1 The prevalence of symptomatic lumbar disc herniation in Finland and Italy is roughly 1% to 3%, and this rate varies by age and gender. The condition is most common among people aged 30 to 50, with an incidence ratio of men to women of 2:1.2 Around 95% of disc herniations in people aged 25 to 55 occur at the lower lumbar spine segments L4/5 and L5/S1, and lumbar disc herniation is also more prevalent in those aged 55 and above.3,4 The chronic radicular pain and sensory-motor dysfunction of the lower extremities caused by LDH have become one of the major contributors to loss of labor capacity.5,6 Current clinical treatments are confronted with a dual bottleneck: conservative therapies only temporarily relieve inflammation without nerve repair;7,8 surgery fails to block residual inflammatory nerve damage, leading to high recurrence and persistent pain.9,10 This clinical dilemma has driven the research focus to shift from a single goal of mechanical decompression to a dual-target strategy encompassing inflammatory regulation and nerve repair.
The core pathological feature of LDH is a vicious cycle of intervertebral disc degeneration–inflammation activation–nerve injury: intervertebral disc degeneration leads to nucleus pulposus herniation, which releases damage-associated molecular patterns (DAMPs) to trigger the activation of local inflammatory networks. As the central hub of the inflammatory network, the interleukin family directly mediates nerve root demyelination, axonal degeneration, and neuronal apoptosis through an imbalance characterized by excessive secretion of pro-inflammatory cytokines and insufficient expression of anti-inflammatory cytokines.11,12 Furthermore, neuropeptides released after nerve injury further activate immune cells, forming a positive amplification loop between inflammation and nerve injury.13,14 The key regulatory node of this pathological loop lies in the interleukin network—interleukins act not only as core mediators of inflammatory responses but also as key signaling molecules regulating nerve injury and repair. This dual role renders them ideal therapeutic targets for breaking the aforementioned vicious cycle.15,16
Previous studies present numerous limitations. Most investigations focus on single interleukins and lack integrated network analysis. The dual roles of interleukins remain controversial.17–19 No review has systematically compared international biologic therapies with domestic TCM interventions.12,20–22 To address these gaps, this review systematically summarizes interleukin-mediated inflammatory and neural mechanisms and makes methodological comparisons between domestic and international research priorities. This review has three unique innovative points that distinguish it from earlier published work. It establishes for the first time a complete cascade framework reflecting interleukin network imbalance inflammatory amplification nerve root injury and repair in LDH. It adopts a standardized parallel comparison method to classify and compare international targeted biologics with domestic interventions including TCM and acupuncture. It directly connects mechanism research results with key clinical translation challenges such as targeted delivery and objective biomarkers to provide feasible stratified treatment strategies. Our research aims to offer translational strategies for precise anti-inflammatory and neuroprotective therapy of lumbar disc herniation.
Methods
Search Strategy
This is a narrative review (not a systematic review or meta-analysis). We conducted a literature search across the PubMed and Embase databases for studies published from January 2010 to January 2026. The search employed the following keywords: (“lumbar disc herniation” or “LDH”), (“interleukin” or “IL” or “Interleukin Network”), (“Nerve Injury”), and (“Inflammatory”). Only English-language publications were included in this search. Initial screening was carried out utilizing the native search tools of each database, and after excluding 285 duplicate records, a total of 783 relevant articles were identified.
Study Selection
Prior to full-text assessment of the shortlisted papers, EndNote software was employed to screen for references relevant to the present study topic. Among these references, 87 articles were without full-text abstracts, 145 were unrelated to lumbar disc herniation (LDH) and interleukins (IL), 257 were review articles or meta-analyses, and 102 were clinical research studies. Ultimately, a total of 196 full-text original research papers pertinent to the research topic were included in the analysis. A flowchart illustrating the entire literature search and selection process is provided in Supplementary Figure 1.
Data Extraction
Data extraction was performed using a pre-specified form focusing on inflammatory phenotypes, signaling pathways, interleukin expression, nerve injury indicators, and intervention efficacy. Extracted items included study type (animal/in vitro/clinical), core interleukin targets, key signaling pathways, pathological outcomes, and therapeutic effects. Two reviewers independently completed data extraction and cross-checked for consistency to ensure accuracy.
Overview of Interleukins and Inflammatory Network Regulation in LDH
Biological Characteristics of Interleukins and Their Secretory Regulation in LDH
As pivotal mediators of immune and neural signaling pathways, the interleukin family is primarily secreted by macrophages, T lymphocytes, glial cells, and intervertebral disc cells in LDH. Its expression is tightly regulated by pathways such as NF-κB, JAK-STAT, and the NLRP3 inflammasome.23,24 Among pro-inflammatory interleukins, IL-1β is predominantly released by M1-polarized macrophages upon stimulation by damage-associated molecular patterns (DAMPs) derived from the nucleus pulposus. It forms a positive feedback loop through activating the NLRP3 inflammasome, resulting in sustained amplification of the inflammatory response.12,25 IL-6 can be secreted by macrophages and astrocytes. Via binding to the gp130 receptor, it activates the STAT3 pathway—promoting inflammatory infiltration in the acute phase while potentially participating in tissue repair during the chronic phase.6,18 IL-17 is mainly derived from Th17 cells, with its expression significantly upregulated in non-contained disc herniation. It accelerates intervertebral disc degeneration and nerve injury by facilitating the secretion of matrix metalloproteinases (MMPs).26–28 IL-21 regulates the differentiation of Th17 cells and exhibits a positive correlation with visual analog scale (VAS) pain scores. Increased IL-21 expression can exacerbate TNF-α-mediated inflammatory responses.15,29 IL-33 activates the JNK/ERK pathway via the ST2 receptor, thereby aggravating central sensitization.30
Among anti-inflammatory interleukins, IL-4 primarily induces macrophage polarization toward the M2 phenotype, enhances IL-10 secretion and suppresses pro-inflammatory cytokine production. Elevated IL-4 levels are associated with the regression of disc herniation.31–33
IL-10 inhibits the excessive activation of immune cells and promotes the expression of brain-derived neurotrophic factor (BDNF). Its serum levels are positively correlated with pain relief, which renders it a key regulatory factor in nerve repair.22,34 The secretory regulation of interleukins in LDH exhibits a distinct hierarchical pattern. It initiates with the release of (DAMPs) such as glycoproteins and nucleic acids from nucleus pulposus herniation, which initially activate TLR4 receptors on the macrophage surface, trigger the NF-κB pathway and thus promote the initial secretion of pro-inflammatory interleukins. Subsequently, pro-inflammatory interleukins activate T cells and glial cells via autocrine/paracrine mechanisms, forming an inflammatory cascade. Meanwhile, insufficient expression of anti-inflammatory interleukins further disrupts the inflammatory balance.11,35
Core Features of Nerve Injury and the Critical Role of Inflammation in LDH
LDH-associated nerve injury primarily targets nerve roots, with its core pathological features encompassing three aspects: first, myelin sheath injury, characterized by the downregulated expression of myelin basic protein (MBP), loose or even disrupted myelin structure. This is closely associated with the inflammation-induced release of matrix metalloproteinases (MMPs), including MMP-3 and MMP-9, which directly degrade myelin proteins and impair the integrity of nerve conduction;36,37 second, axonal degeneration, where mechanical compression from herniated discs combined with inflammatory cytokines jointly causes axonal swelling and rupture, accompanied by decreased expression of neurofilament protein (NF-H), thereby compromising neural signal transmission;38,39 third, neuronal apoptosis, in which dorsal root ganglion (DRG) neurons undergo apoptosis via activating the caspase-3/8 pathway upon stimulation by pro-inflammatory cytokines such as IL-17 and TNF-α, leading to irreversible impairment of neurological function.25,28
Inflammation plays an amplifier role in nerve injury. On the one hand, inflammatory cells (macrophages and neutrophils) infiltrate the periradicular region, and the proteases, nitric oxide (NO) and other mediators they secrete directly induce nerve tissue damage.40,41 On the other hand, inflammatory cytokines indirectly exacerbate nerve injury by regulating the activation of glial cells—activated microglia secrete IL-1βand TNF-α, while astrocyte proliferation leads to the formation of glial scars that impede nerve repair.11,42 Clinical studies have confirmed that the levels of inflammatory cytokines (IL-6, IL-8) in the cerebrospinal fluid (CSF) of LDH patients are positively correlated with the degree of nerve injury (electromyography [EMG] abnormality rate). Furthermore, neurological function scores are significantly improved after anti-inflammatory therapy, which further verifies the critical role of inflammation in nerve injury.43,44
Dual Roles of Interleukins in Regulating the Inflammatory Network in LDH
Interleukins exhibit prominent dual roles in LDH, with their functions being dependent on disease stages, expression levels, and the cellular microenvironment. Pro-inflammatory interleukins exhibit notable dual functions. In acute LDH, IL-6 promotes inflammatory infiltration and exacerbates nerve injury by activating the STAT3 pathway.43 In contrast, during the chronic phase, it may participate in tissue repair by upregulating the expression of neurotrophic factors.18 IL-1βtriggers inflammatory responses to clear necrotic tissues in the early stage of disc herniation. However, its persistent high expression induces excessive inflammatory activation via a positive feedback loop, thereby aggravating neurotoxicity.25 Anti-inflammatory interleukins also feature dual properties. When expressed at appropriate levels, IL-4 induces M2 polarization of macrophages and facilitates nerve repair. Nevertheless, excessive IL-4 expression may inhibit the clearance of necrotic tissues by immune cells and delay tissue remodeling.32,33
The core mechanism underlying these dual roles is associated with the switching of signaling pathways: pro-inflammatory interleukins primarily activate the NF-κB pathway during the acute phase, whereas they may switch to the PI3K/AKT repair pathway in the chronic phase. In contrast, anti-inflammatory interleukins regulate the dynamic balance between inflammation and repair by balancing the activity of the STAT3 and STAT6 pathways.16 This pathway-switching mechanism also explains the controversies observed in different studies (eg., the correlation between IL-6 and pain). Some studies focusing on acute LDH have demonstrated a positive correlation between IL-6 levels and visual analog scale (VAS) pain scores.43 However, other studies enrolling patients with chronic LDH have failed to identify any significant correlation, indicating that the functions of interleukins are stage-specific.19
The Crosstalk Between Inflammatory Network, Interleukin Imbalance and Nerve Root Injury in LDH
Initiating Mechanisms of Inflammatory Network Activation and Interleukin Imbalance
The initiating event for inflammatory network activation in LDH is the foreign body immune response triggered by nucleus pulposus herniation. Under normal physiological conditions, the nucleus pulposus is in an immune-privileged state. When herniated, damage-associated molecular patterns (DAMPs) such as glycoproteins, nucleic acids, and collagens released from the nucleus pulposus are recognized by receptors including TLR4 and CD68 on the surface of macrophages, thereby initiating the innate immune response.45,46
Studies have demonstrated that the number of infiltrating macrophages is significantly increased in herniated disc tissues. Specifically, the degree of macrophage infiltration (proportion of CD68+ cells) in non-contained disc herniation is 2.3-fold higher than that in contained disc herniation.47,48 Once activated, these macrophages secrete large amounts of IL-1β and TNF-α, serving as the primary source of pro-inflammatory interleukins.49,50
Interleukin network imbalance acts as the core driver of inflammatory amplification. Pro-inflammatory interleukins exhibit a cascade-like elevation. Specifically, IL-1β promotes the secretion of IL-6 and IL-17 by activating the NF-κB pathway,51,52 while IL-17 further recruits neutrophil infiltration and induces the release of IL-8 and MMPs.48,53 This process forms an inflammatory cascade that takes IL-1β as the initiator, IL-6/IL-17 as intermediate links and IL-8 as downstream effector molecules. In contrast, anti-inflammatory interleukins show insufficient expression. For instance, serum IL-10 levels in LDH patients are only 58% of those in healthy individuals, and positively correlated with the degree of pain relief.54 Although IL-4 is elevated in some patients, it is insufficient to counteract the damaging effects of pro-inflammatory cytokines.55 This imbalanced state is particularly pronounced in acute LDH. Serum IL-6 and IL-17 levels peak within 12 weeks of onset and then decline gradually.56,57 On the other hand, chronic patients exhibit a low-grade imbalance between pro-inflammatory and anti-inflammatory cytokines.58
Core Pathways of Interleukin-Mediated Nerve Root Injury
We have summarized the relevant research results of interleukin mediated nerve root injury in lumbar disc herniation in recent years, as shown in Table 1. Pro-inflammatory interleukins such as IL-1β and IL-6 directly damage nerve roots by activating glial cells to release toxic mediators. IL-1β binds to interleukin-1 receptors (IL-1R) on the surface of dorsal root ganglion (DRG) neurons and microglia, activating the p38MAPK pathway to promote the secretion of neurotoxic substances including NO and PGE2, which results in loose myelin structure and downregulated myelin basic protein (MBP) expression.59 Clinical studies have confirmed a positive correlation between IL-1β expression levels in DRG tissues of LDH patients and the degree of myelin sheath injury.52,60 IL-6 activates astrocyte proliferation via the gp130/STAT3 pathway, leading to the formation of glial scars that impede nerve axonal regeneration. Meanwhile, it promotes the release of matrix metalloproteinase-9 (MMP-9) to further degrade myelin proteins.58,61 Animal experiments have demonstrated that inhibiting IL-6 can reduce the area of myelin sheath injury in DRG tissues by 41%.60
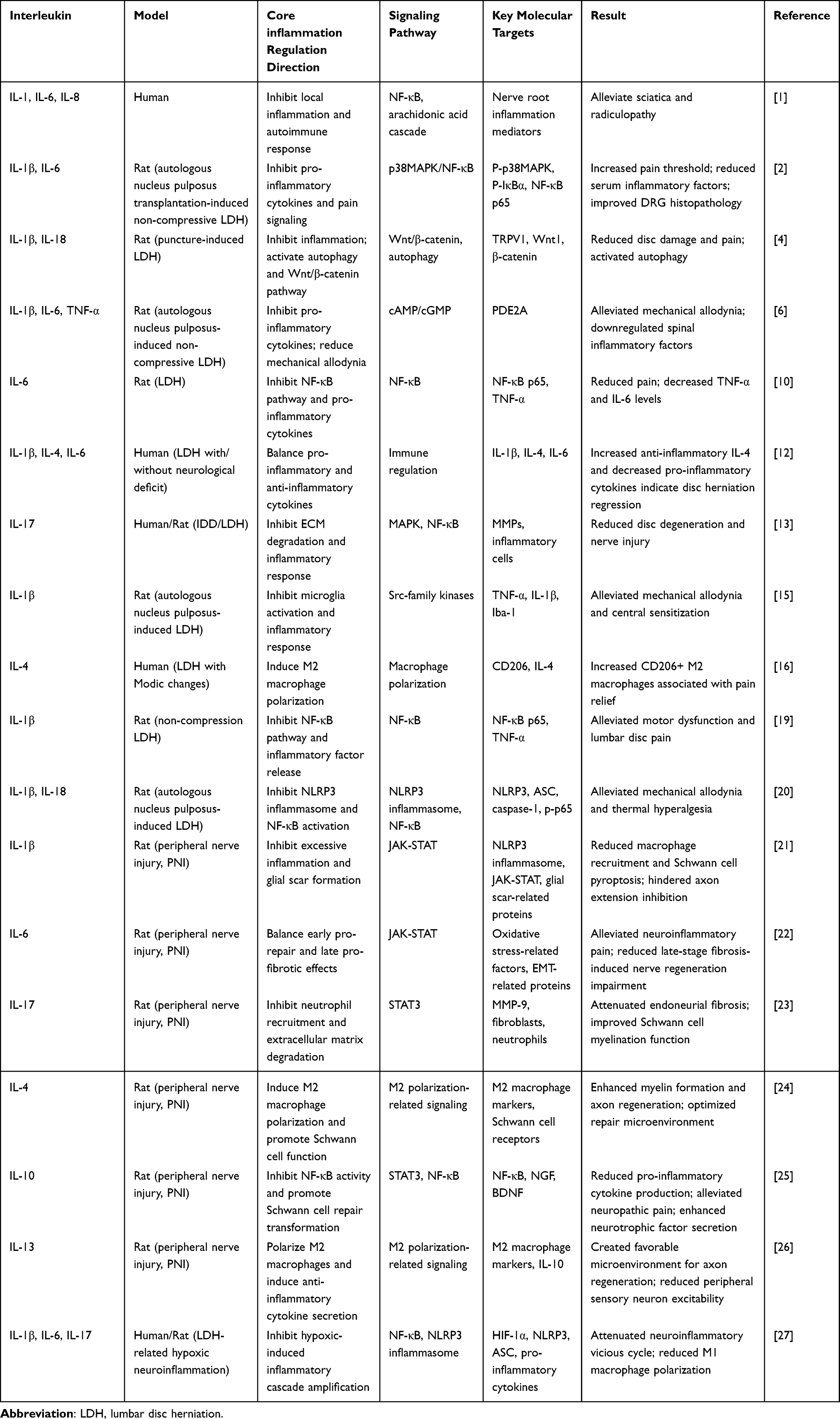 |
Table 1 Related Studies on Interleukin Mediated Nerve Root Injury in Lumbar Disc Herniation |
Pro-inflammatory interleukins such as IL-17 and TNF-α promote the death of nerve root neurons by activating apoptotic pathways. IL-17 binds to interleukin-17 receptors (IL-17R) on the neuronal surface, activates the caspase-3/8 pathway, upregulates the expression of the pro-apoptotic protein Bax, and downregulates the anti-apoptotic protein Bcl-2, resulting in an increased apoptotic rate of DRG neurons.57,62 Immunohistochemical staining has shown that the number of IL-17+ cells in the intervertebral disc tissues of patients with ruptured LDH is 1.8-fold higher than that in patients with non-ruptured LDH, and it is positively correlated with the expression of the neuronal apoptotic marker (cleaved-caspase-3).48 TNF-α exacerbates DRG neuronal apoptosis through the tumor necrosis factor receptor 1 (TNF-R1)-mediated extrinsic apoptotic pathway. Meanwhile, it inhibits neural stem cell proliferation and impedes nerve repair.59,63
Pro-inflammatory interleukins induce chronic neuropathic pain by upregulating the expression of pain-related ion channels and enhancing nociceptive signal transmission. IL-6 upregulates the expression of TRPV1 and Nav1.7 ion channels on the surface of DRG neurons via the JAK2/STAT3 pathway, reducing the pain threshold and triggering abnormal neuronal discharge.64,65 Animal experiments have demonstrated that warm acupuncture and moxibustion can decrease the proportion of TRPV1-positive neurons by 35% through inhibiting IL-6 expression.60 IL-1β activates the PKC pathway in DRG neurons, enhancing ion channel sensitivity and exacerbating mechanical allodynia and thermal hyperalgesia.66 Additionally, IL-8 can directly stimulate nociceptors to induce radiating pain, and its levels are closely correlated with back extension-induced radicular pain.67,68
The Vicious Cycle of Inflammation–Nerve Injury–Interleukin
The chronic progression of LDH is closely associated with a vicious cycle constituted by inflammation, nerve injury, and interleukins. After nerve root injury, neuropeptides such as substance P (SP) and neuropeptide Y (NPY) released from damaged nerves can activate microglia and astrocytes, which in turn secrete more IL-1β and TNF-α.60 Animal experiments have demonstrated that SP expression in DRG tissues increases by 2.1-fold following nerve injury. Through binding to the neurokinin 1 (NK1) receptor, SP promotes IL-6 secretion by macrophages, thus forming a closed loop. SP release after nerve injury activates inflammation, leading to elevated pro-inflammatory interleukins that further exacerbate nerve injury.65 Meanwhile, nerve injury-induced disruption of the blood-nerve barrier facilitates the infiltration of peripheral inflammatory cells into the periradicular region, aggravating local inflammation.66 Meanwhile, nerve injury-induced disruption of the blood-nerve barrier facilitates the infiltration of peripheral inflammatory cells into the periradicular region, aggravating local inflammation.63,69
This vicious cycle is particularly pronounced in patients with postoperative residual pain: in patients who still suffer from chronic pain 3 months after surgery, the levels of IL-1β and TNF-α in DRG tissues are 1.9-fold higher than those in pain-free patients, while BDNF expression is reduced by 52%.63,70 This indicates that residual inflammation sustains the pain state by inhibiting nerve repair. Furthermore, fat infiltration of the multifidus muscle and inflammatory imbalance mutually reinforce each other. Elevated IL-1β levels in subcutaneous fat can inhibit muscle regeneration, and muscle dysfunction further exacerbates spinal mechanical imbalance, accelerating intervertebral disc degeneration and inflammatory activation.63,71 The interaction between the inflammatory network, interleukin imbalance, and nerve root injury in lumbar disc herniation is shown in Figure 1.
 |
Figure 1 The Crosstalk Between Inflammatory Network, Interleukin Imbalance and Nerve Root Injury in LDH. The Source of Inflammation (Left): As the disc degenerates, these cells break down and release DNA and other cellular debris, labeled here as DAMPs (Damage-Associated Molecular Patterns), which trigger an immune response. Th17 Cells (Purple cells): A type of immune cell that responds to the DAMPs. They primarily release the cytokine IL-17 (represented by purple dots). M1 Macrophages (Red cells): Pro-inflammatory immune cells that also respond to the DAMPs. They release the cytokines IL-1β and IL-6 (represented by red dots). Cytokine Storm: The massive, combined release of these inflammatory signaling molecules (IL-17, IL-1β, IL-6) into the surrounding tissue. MMP-9 (represented as scissors) cutting up the ECM (Extracellular Matrix, the green structural web), which further contributes to tissue breakdown. Downstream Effects on the Nervous System (Right): The cytokine storm impacts three main types of cells in the nervous system, leading to distinct negative outcomes. Microglia: These are the primary immune cells of the central nervous system. IL-1β binds to their receptors, activating the NLRP3 inflammasome and Caspase-1, which eventually leads to Pyroptosis (a highly inflammatory form of programmed cell death). Astrocyte: These are supporting cells in the nervous system. IL-6 binds to their receptors (gp130), activating the JAK/STAT3 pathway, which causes them to form a fibrous Glial Scar. DRG Neuron (Dorsal Root Ganglion): This is the primary sensory nerve cell responsible for transmitting pain. IL-17 binds to its receptor, triggering the NF-κB pathway, which can lead to Apoptosis (programmed cell death). The inflammatory environment sensitizes and activates specific ion channels on the neuron—TRPV1 (allowing Calcium/Ca2⁺ in) and Nav1.7 (allowing Sodium/Na⁺ in). This ion influx triggers the electrical impulses (red lightning bolts) that the brain interprets as pain. |
Mechanisms of Interleukins Regulating Inflammatory Network to Alleviate Nerve Root Injury in LDH
Targeting Pro-Inflammatory Interleukins for Blocking the Inflammation and Nerve Injury Cascade
As a key inflammatory initiating factor, blocking IL-1β signaling can suppress the inflammatory cascade at its source. The NF-κB inhibitor Bay11-7082 blocks NF-κB nuclear translocation by inhibiting IκBα phosphorylation, which significantly reduces the expression of IL-1β and IL-18 in the DRG tissues of LDH rats. Meanwhile, it suppresses NLRP3 inflammasome activation, resulting in a 40% increase in the mechanical allodynia threshold.70 Phellodendrine improves motor dysfunction in rats by downregulating the mRNA expression of NF-κB p65 and reducing IL-1β release.34 Preclinical studies have demonstrated that anti-IL-1β monoclonal antibodies can reduce the demyelination area of nerve roots by 38%, while upregulating BDNF expression to promote axonal regeneration.50,70
The IL-6/JAK-STAT pathway is a key node in inflammatory amplification and nerve injury, and its targeted inhibition can simultaneously alleviate inflammation and nerve damage. The PDE2A inhibitor Bay 60–7550 inhibits JAK2/STAT3 phosphorylation by increasing cAMP/cGMP levels, downregulates IL-6 expression, and elevates the pain threshold by 35% in rats with non-contained lumbar disc herniation (NCLDH).72 Clinical studies have confirmed that the Isobar dynamic stabilization system combined with discectomy can significantly reduce postoperative IL-6 levels while improving lumbar spine function, with the improvement rate of JOA scores being 1.3-fold higher than that of the discectomy-only group.70 In addition, propofol total intravenous anesthesia inhibits the NF-κB pathway, reduces postoperative IL-6 and C-reactive protein (CRP) levels, and mitigates secondary nerve injury induced by surgery-related inflammation.73
IL-17 exacerbates nerve injury by promoting the release of MMPs, and its targeted inhibition can protect the intervertebral disc matrix and nerve tissue. Animal experiments have demonstrated that Shinbaro 2 restores the morphology and function of the spinal cord by inhibiting IL-17 expression and reducing the levels of MMP-1 and MMP-9.74 Anti-IL-17 antibodies can reduce the degree of axonal degeneration by 45% in rats with ruptured LDH.66 Clinical studies have found that the magnitude of the postoperative decrease in IL-17 levels is positively correlated with the degree of pain relief in patients with non-contained disc herniation, suggesting that IL-17 inhibition is an effective therapeutic target.57 The mechanism by which interleukin regulates the inflammatory network to alleviate LDH nerve root damage is shown in Figure 2.
 |
Figure 2 Mechanisms of Interleukins Regulating Inflammatory Network to Alleviate Nerve Root Injury. Acupuncture/TCM: Represents external therapy triggering a cascade of healing signaling molecules. M1 Macrophage/M2 Macrophage: Represents the two functional states of immune cells. The shift from M1 (pro-inflammatory) to M2 (anti-inflammatory) is labeled as a Phenotypic Switch. Tocilizumab & Canakinumab: Biological drugs (monoclonal antibodies) that target specific cytokines to halt inflammation. Glial Cell (e.g., Astrocyte/Microglia): Supporting brain/spinal cells that are being “de-activated” from their inflammatory state. Neuron: The target of the regenerative process, specifically showing the Axonal Growth Cone (rebuilding the nerve tip) and Myelin Sheath (insulating the nerve). Neuroprotection & Regeneration: The ultimate positive outcome of the illustrated pathways. Red Elements (IL-6, IL-1β): These represent Pro-inflammatory Cytokines. They are shown being blocked or neutralized. Blue Elements (IL-4, IL-10): These represent Anti-inflammatory Cytokines. They promote healing and suppress the “bad” pathways. Purple Elements (Arg-1): Arginase-1, a specific marker and tool of the “healing” M2 macrophage. Green Elements (BDNF, TrkB): BDNF is a “growth factor” (star-shaped). It binds to the TrkB receptor to signal the neuron to grow. JAK-STAT3 & NLRP3 Pathways: These are the “inflammatory engines” inside cells. In this diagram, they are struck through with a Red X, meaning they are being inhibited by the treatments. Blue Block Arrow: Represents the initiation of therapy (Acupuncture). Green Block Arrows: Represent “Progress” or “Transition” (moving from a bad state to a good state). T-Bar Line (T): A standard biological symbol for Inhibition. It shows where a drug (like Tocilizumab) stops a molecule (IL-6) from working. Curved Black Arrows: Indicate the secretion of molecules out of a cell or the movement of transcription factors (like STAT6 or NF-κB) into the nucleus. DNA Helix (inside nucleus): Indicates that genes are being “turned on” to produce new proteins for repair. |
Enhancing Anti-Inflammatory Interleukins for Activating the Nerve Repair and Inflammation Balance Pathway
In a cell experiment, IL-10 promotes nerve repair by inhibiting the excessive activation of immune cells. Glycoprotein non-metastatic melanoma protein B (GPNMB) binds to CD44 to inhibit the NF-κB pathway, increase IL-10 secretion, while reducing IL-6 expression and extracellular matrix (ECM) degradation, thereby protecting the perineural microenvironment.69 Animal experiments have demonstrated that IL-10 overexpression reduces the apoptotic rate of dorsal root ganglion (DRG) neurons by 32% and promotes myelin basic protein (MBP) expression to repair myelin sheath injury.54 Clinical studies have confirmed that serum IL-10 levels in lumbar disc herniation (LDH) patients who respond positively to conservative treatment are 2.1-fold higher, and this elevation is positively correlated with improvements in visual analog scale (VAS) pain scores, suggesting that IL-10 is a potential biomarker for therapeutic efficacy evaluation.54,75
IL-4 creates a neuroprotective microenvironment by inducing the polarization of macrophages toward the M2 phenotype. It activates the STAT6 pathway to promote macrophages to express anti-inflammatory markers including Arginase-1 (Arg-1) and CD163, while reducing the secretion of TNF-α and IL-1β.49,55 In patients with Modic changes, the proportion of CD206+ M2 macrophages is significantly increased, accompanied by elevated IL-4 expression, which is associated with pain relief.49 The active components of Yaobishu Formula, namely PA and THMC, indirectly upregulate IL-4 levels by reshaping the gut microbiota and activating autophagy as well as the Wnt/β-catenin pathway. This process reduces TRPV1 expression and alleviates neuropathic pain.64
Downstream Dual Therapeutic Effects
Interleukin modulation significantly reduces local inflammatory cytokine levels: following warm acupuncture and moxibustion treatment, serum IL-6 and TNF-α levels in LDH rats were reduced by 42% and 38%, respectively, while the protein expression of phosphorylated p38MAPK (P-p38MAPK) and NF-κB p65 in dorsal root ganglion (DRG) tissues was downregulated.60 Compared with traditional posterior lumbar interbody fusion (PLIF) surgery, unilateral biportal endoscopic surgery (ULIF) resulted in lower IL-6 and TNF-α levels on postoperative day 5, accompanied by a milder inflammatory response.76 Concurrent with inflammatory alleviation is reduced inflammatory cell infiltration. Acupuncture inhibits the CXCL12/CXCR4-ERK/NF-κB pathway to diminish the infiltration of macrophages and neutrophils, thereby creating a favorable microenvironment for nerve repair.77
Interleukin modulation can protect myelin sheath integrity and promote axonal regeneration. UPAL gel implantation inhibits IL-6 and TNF-α, downregulates tropomyosin receptor kinase A (TrkA) expression to reduce neural ingrowth into intervertebral disc tissues, and simultaneously promotes MBP expression to repair the myelin sheath.78 IL-10 overexpression increases brain-derived neurotrophic factor (BDNF) levels in DRG tissues by 2.3-fold and promotes axonal regeneration.69 At the functional level, interleukin modulation improves nerve conduction function: after phellodendrine treatment, motor function scores of LDH rats are significantly elevated, and nerve conduction velocity is accelerated by 30%.34 Clinical studies have shown that acupuncture combined with nerve block therapy achieves a 78% improvement rate in lower limb paresthesia among LDH patients.79
The ultimate effect of interleukin modulation is reflected in pain relief and functional recovery: inflammation-preserving therapy (acupuncture combined with gabapentin) enabled complete intervertebral disc resorption in 100% of patients with acute LDH, with the VAS pain score decreasing from 6.12 to 1.8.80 After 4 weeks of warm acupuncture and moxibustion treatment, the paw withdrawal threshold of LDH rats increased by 50%, and the pathological damage of (DRG) tissues was alleviated.60 In surgical treatment, the Isobar dynamic stabilization system combined with discectomy reduced the Oswestry Disability Index (ODI) score by 48% and increased the Japanese Orthopaedic Association (JOA) score by 55% at 6 months postoperatively. Meanwhile, it reduced the recurrence rate, and its therapeutic effect was closely associated with the significant decrease in IL-6 and C-reactive protein (CRP) levels.70
Current Domestic and International Research Progress
International Research Progress
International research has focused on highly specific biologics to achieve precision anti-inflammation plus neurorepair. Tocilizumab (an anti-IL-6 receptor monoclonal antibody) reduced the VAS score for neuropathic pain by 32% and increased nerve conduction velocity by 25% in patients with LDH in a phase II clinical trial. The underlying mechanism involves blocking the IL-6/JAK2/STAT3 pathway to reduce MMP-9-mediated myelin degradation.61,81 Canakinumab (an anti-IL-1β monoclonal antibody) inhibited microglial activation, upregulated brain-derived neurotrophic factor (BDNF) expression, and reduced the apoptotic rate of dorsal root ganglion (DRG) neurons by 36% in LDH rats in preclinical studies.50 An interleukin-10 fusion protein (IL-10-Fc), which has an extended half-life, achieved sustained anti-inflammatory effects and promoted neurotrophic factor secretion without systemic immunosuppressive side effects in animal experiments.54
International research has identified the key molecular targets through which interleukins regulate nerve injury. IL-6 directly upregulates MMP-9 promoter activity by activating the STAT3 pathway, thereby promoting myelin degradation.61 In an animal experiment, IL-1β triggers a cascade consisting of IL-1β, caspase-1, and IL-18 via NLRP3 inflammasome activation, which exacerbates central sensitization.20 IL-21 regulates the expression of TNF-αand a disintegrin and metalloproteinase with thrombospondin motifs-7 (ADAMTS-7) through STAT3, accelerating intervertebral disc degeneration and nerve compression.82,83 In addition, progress has been made in dissecting the mechanism underlying the dual roles of IL-6. Studies have revealed that IL-6 exerts pro-inflammatory effects via the classical signaling pathway (membrane-bound receptors) in the acute phase, while it participates in tissue repair through the trans-signaling pathway mediated by soluble receptors in the chronic phase.81
To enhance local therapeutic efficacy and minimize systemic side effects, international researchers have developed nerve root-targeted delivery vectors. Ganglioside-modified liposomes can specifically bind to the GM1 receptors on the surface of DRG neurons, enabling local enrichment of IL-1β inhibitors at the nerve roots, with the local drug concentration being 5.8-fold higher than that of free drugs.78 In addition, phosphodiesterase 2A (PDE2A) inhibitors, delivered via intrathecal injection, act directly on the dorsal horn of the spinal cord, dose-dependently downregulating pro-inflammatory cytokines and alleviating mechanical allodynia.72 Research has found that the potential of using the Histologic Degradation Score for Histologic assessment can provide valuable insights into disease progression and outcomes in LDH patients.84 In addition, host factors such as BMI also have a significant impact on intervertebral disc degeneration.85
Domestic Research Progress
Domestic research has demonstrated distinctive strengths in the studies of natural products and TCM formulas. Tanshinone IIA downregulates the expression of IL-1β and IL-17 by inhibiting the NF-κB pathway, while simultaneously promoting the secretion of BDNF, resulting in a 39% reduction in the area of myelin sheath injury in LDH rats.34 Astragalus polysaccharides reduce the apoptotic rate of DRG neurons by upregulating IL-10 levels and inhibiting caspase-3 activation.54 Curcumin improves nerve root inflammation and demyelination by regulating the gut microbiota, activating the autophagic pathway, and downregulating IL-6 and TNF-α expression. For TCM formulas, the active components of Yaobishu Formula (PA and THMC) reshape the gut microbiota, activate the Wnt/β-catenin pathway, and downregulate the expression of TRPV1 and IL-1β.64 Duhuo Jisheng Decoction promotes M2 macrophage polarization by balancing the IL-6/IL-10 ratio. A small-sample clinical study has shown that it can increase the Japanese Orthopaedic Association (JOA) score by 23%.86
Acupuncture and Tuina regulate the interleukin network through multiple pathways: warm acupuncture and moxibustion (40°C with 2Hz electrical stimulation) at acupoints GB30 and BL54 inhibits the p38MAPK/NF-κB pathway, downregulates the protein expression of IL-1β and IL-6 in DRG tissues, and simultaneously upregulates IL-10 levels, increasing the pain threshold of rats by 50%.60 “Root-Branch Acupoint” acupuncture improves pain and lumbar spine function by regulating the CXCL12/CXCR4 pathway and reducing IL-6 and TNF-α levels.86 Tuina inhibits peripheral inflammation by modulating the TLR4 pathway and miRNAs, and simultaneously regulates P2X3 and Piezo ion channels to suppress glial cell activation, achieving a 76% effective rate in treating LDH-related neuropathic pain.87 Korean traditional medicine (acupuncture combined with Tuina) can alleviate postoperative complications and reduce Numerical Rating Scale (NRS) and Oswestry Disability Index (ODI) scores.
In China, cohort studies focusing on the interleukin expression profile of LDH in the Chinese population have been conducted. These studies revealed that the serum levels of IL-17 and IL-33 in patients with severe nerve injury were 2.1-fold and 1.8-fold higher than those in patients with mild nerve injury, respectively, indicating that these two interleukins can serve as predictive biomarkers for the severity of nerve injury.57,88 A multicenter randomized controlled trial demonstrated that 6 weeks of treatment with Bosinji Granules combined with acupuncture reduced the VAS score by 41%, and its safety was verified through liver and kidney function tests.89 In the field of targeted delivery, domestic researchers have developed chitosan microspheres loaded with active traditional Chinese medicine components (eg., phellodendrine). Administered via percutaneous intervertebral disc injection, this delivery system achieves local sustained release of the drug at the nerve roots, with the anti-inflammatory effect lasting for 21 days.34 In addition, cutaneous acupuncture therapy alleviates inflammatory infiltration at gluteal tender points, reduces the inflammatory response width observed under B-ultrasound, and decreases the VAS score by 38%.86
Domestic studies have explored the combined regulatory mechanism of “acupuncture plus TCM”, confirming that acupuncture downregulates pro-inflammatory interleukins by inhibiting the p38MAPK pathway, while TCM activates autophagy by regulating the gut microbiota. Their synergistic effect results in significantly higher downregulation magnitudes of IL-1β and IL-6 compared with monotherapy.64 TCM minimally invasive techniques (cutaneous acupuncture and filiform-knife acupuncture) alleviate fascia tension, reduce the release of inflammatory factors, and simultaneously promote IL-10 expression, which is suitable for the tension-type pain of nerve endings secondary to tissue texture changes.90 In addition, domestic research has focused on the impacts of risk factors such as smoking and obesity on the expression of IL-6 and IL-1β, revealing that the levels of IL-1β and IL-6 in the ligamentum flavum are significantly elevated in smokers, thus providing evidence for risk factor intervention.91,92
Discussion
There are significant interindividual differences in the type (demyelination-predominant, axonal injury-predominant, or mixed injury) and severity of nerve injury among patients with LDH) Patients with non-contained disc herniation mainly present with demyelination, accompanied by significantly elevated levels of IL-17 and IL-8.47 In contrast, patients with chronic nerve compression are characterized by axonal degeneration, with much higher levels of IL-6 and TNF-α.58 This heterogeneity leads to substantial variability in the efficacy of single interleukin-targeted drugs. The effective rate of anti-IL-1βmonoclonal antibodies reaches 67% in patients with demyelination-predominant injury, but only 32% in those with axonal injury-predominant injury.50 The lack of precision stratification criteria has become a major barrier to clinical translation.
Existing delivery methods are difficult to achieve efficient local enrichment of drugs at the nerve roots. For systemic administration (eg., oral anti-inflammatory agents), the local drug concentration at the nerve roots is only 12–18% of the serum concentration, which is prone to inducing gastrointestinal and hepatorenal adverse effects.34,72 Although intrathecal injection can act directly on the spinal cord, it is associated with considerable invasiveness and fails to precisely target the affected nerve roots.72 Drugs delivered via intervertebral disc injection are easily adsorbed by the intervertebral disc matrix, resulting in low release efficiency.49 In addition, the blood–nerve barrier hinders drug penetration, which further impairs local therapeutic efficacy.
Current clinical efficacy evaluation relies heavily on subjective symptom scales (Visual Analog Scale [VAS] and Oswestry Disability Index [ODI]), with a notable absence of objective biomarkers. Detection of myelin repair markers (myelin basic protein [MBP]) and axonal regeneration markers (neurofilament heavy chain [NF-H]) requires invasive biopsy, which cannot be routinely applied in clinical practice.69 Serum inflammatory cytokines (IL-6 and IL-10) show weak correlation with nerve repair processes.93 Imaging examinations, such as magnetic resonance imaging (MRI), are unable to quantify the severity of myelin and axonal injuries.50 This deficiency makes it impossible to evaluate the effect of nerve repair at an early stage, leading to delays in the adjustment of therapeutic regimens.
The mechanisms of action of TCM and natural products remain unclear. For instance, the specific targets (eg., specific bacterial genera) through which the active components of Yaobishu Formula (PA and THMC) regulate the gut microbiota have not been clarified.64 The upstream signaling pathways (eg., neural conduction pathways of acupoint stimulation) underlying acupuncture-mediated regulation of the p38MAPK/NF-κB pathway are still poorly understood.60 In addition, there is a lack of sufficient standardization for the components of natural products. Variations in production regions and extraction processes result in 30–50% differences in the content of active components, which affects the stability of clinical therapeutic efficacy.86
Developing combination therapies targeting both inflammation and nerve injury is a key focus, with regimens incorporating pro-inflammatory interleukin inhibitors (eg., anti-IL-1β monoclonal antibodies), anti-inflammatory interleukin mimetics (eg., IL-10-Fc fusion protein), and neurotrophic factors (eg., brain-derived neurotrophic factor [BDNF]). Animal experiments have shown that this combination can increase the nerve repair rate to 68%, which is significantly higher than that of monotherapy.78 In addition, individualized combination regimens can be formulated clinically based on different injury types. For patients with demyelination-predominant injury, a therapeutic regimen combining IL-17 inhibitors and myelin basic protein (MBP) repair agents is recommended; for those with axonal injury-predominant injury, the regimen can consist of IL-6 inhibitors and BDNF.50
Developing nerve root-specific targeted vectors is another critical direction. Tropomyosin receptor kinase A (TrkA)-modified nanoparticles can specifically bind to DRG neurons, enabling targeted delivery of IL-1β inhibitors, with the local drug concentration increased to 8.3-fold higher than that of free drugs.78 Degradable chitosan-alginate composite gel, administered via intervertebral disc injection, enables sustained drug release for up to 4 weeks while promoting intervertebral disc repair.78 In addition, combining with minimally invasive interventional technology (percutaneous endoscopic guidance) allows for precise injection at the affected nerve roots, minimizing invasiveness.76
Another key research direction focuses on leveraging multi-omics technologies, mechanism exploration, and standardization to address the limitations of TCM and natural products. Specifically, multi-omics approaches (transcriptomics and metabolomics) will be used to screen the core targets of TCM, clarifying the interaction between active components (eg., PA and THMC) and the gut microbiota—such as regulating the abundance of Ruminococcaceae.64
Meanwhile, the association between neural signal transduction and immune cell activation following acupoint stimulation will be deciphered.94 A standardized production process for natural products will be established, utilizing fingerprinting to control the content of active components with the error controlled within 10%.86 Additionally, derivatives of active TCM components will be developed to improve bioavailability and target specificity.34
Phase I/II clinical trials will be conducted, with patients who have different types of nerve injury enrolled. A comprehensive evaluation approach that combines objective indicators and subjective scales will be adopted, where objective indicators encompass nerve conduction velocity, magnetization transfer ratio (MTR) MRI for myelin assessment and serum neurofilament heavy chain (NF-H)/MBP levels.63 Subjective scales cover the VAS, ODI and JOA score.70,76 Meanwhile, an individualized treatment algorithm based on interleukin expression profiles and nerve injury types will be established, with machine learning technology leveraged to predict patients’ treatment response rates.55 In addition, clinical trials of integrated traditional Chinese and Western medicine (TCM-WM) therapies will be carried out to verify the synergistic therapeutic effects of acupuncture, TCM and biologics.95
Further in-depth exploration of fundamental mechanisms and animal model refinement is crucial to advance LDH research. Specifically, the molecular switches underlying the dual roles of interleukins will be deciphered, clarifying the switching mechanism between the classical and trans-signaling pathways of IL-6.81 Additionally, the crosstalk pathways between inflammation and nerve repair (eg., the interaction between NF-κB and Wnt/β-catenin pathways) will be investigated.64 LDH animal models more closely mimicking human pathology (eg., non-human primate models) will be constructed to enhance the translational value of preclinical research.51 Furthermore, the impact of epigenetic regulation (eg., miRNAs and DNA methylation) on interleukin expression will be explored, providing a theoretical basis for the development of novel therapeutic targets.77,96
Conclusion
Interleukins act as core regulators in LDH-associated nerve injury. Human clinical evidence confirms that circulating IL-6, IL-1β and IL-17 levels are associated with radicular pain severity and neurological deficits in LDH patients. Mechanistic inferences from preclinical studies suggest pro-inflammatory ILs drive myelin degradation and axonal injury via NF-κB, JAK-STAT3 and p38MAPK pathways, while anti-inflammatory IL-4/IL-10 may promote neuroprotection. Cautiously interpreted, targeting IL signaling may hold translational potential for LDH, but clinical application requires further large-scale human trials to validate efficacy and safety.
Critical barriers currently stand in the way of clinical translation. Validated non-invasive objective biomarkers for early nerve injury assessment are lacking. Targeted delivery across the blood nerve barrier remains inefficient which limits local drug concentration and weakens therapeutic efficacy.
Interleukin-targeted strategies are expected to benefit three groups of patients to the greatest extent. These patients include those with acute lumbar disc herniation accompanied by severe radicular pain, those with persistent chronic residual pain after lumbar discectomy, and those with non-contained disc herniation and obvious nerve root inflammation who fail to respond to conservative treatment. Overcoming the above translational barriers will allow interleukin-based precision therapy to realize integrated anti-inflammation and nerve repair. This will ultimately improve functional recovery and quality of life for patients with lumbar disc herniation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Key Discipline of Acupuncture of the National Administration of Traditional Chinese Medicine (No.14061230010).
Disclosure
The authors declare that this research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Kocaman H, Yldrm H, Gken A, Arman GM. An investigation of machine learning algorithms for prediction of lumbar disc herniation. Med Biol Eng Comput. 2023;61:11. doi:10.1007/s11517-023-02888-x
2. Jordan J, Konstantinou K, O’Dowd J. Herniated lumbar disc. BMJ Clin Evid. 2011;2011.
3. Friberg S, Hirsch C. Anatomical and clinical studies on lumbar disc degeneration. Acta Orthop Scand. 1949;19:222–16. doi:10.3109/17453674908991095
4. Schultz A, Andersson G, Ortengren R, Haderspeck K, Nachemson A. Loads on the lumbar spine. Validation of a biomechanical analysis by measurements of intradiscal pressures and myoelectric signals. J Bone Joint Surg Am. 1982;64:713–720. doi:10.2106/00004623-198264050-00008
5. Gao C, Jiang J, Tan Y, Chen S. Microglia in neurodegenerative diseases: mechanism and potential therapeutic targets. Signal Transduct Target Ther. 2023;8:359. doi:10.1038/s41392-023-01588-0
6. Harrell CR, Volarevic A, Djonov V, Volarevic V. Mesenchymal stem cell-derived exosomes as new remedy for the treatment of neurocognitive disorders. Int J Mol Sci. 2021;23(1):22. doi:10.3390/ijms23010022
7. Zhang L, Yao Q, Hu J, et al. Hotspots and trends of microglia in Alzheimer’s disease: a bibliometric analysis during 2000-2022. Eur J Med Res. 2024;29:75. doi:10.1186/s40001-023-01602-9
8. Mysiris DS, Vavougios GD, Karamichali E, et al. Post-COVID-19 parkinsonism and parkinson’s disease pathogenesis: the exosomal cargo hypothesis. Int J Mol Sci. 2022;23(17). doi:10.3390/ijms23179739
9. Dhapola R, Sharma P, Kumari S, Vellingiri B, Medhi B, HariKrishnaReddy D. Exploring retinal neurodegeneration in Alzheimer’s disease: a molecular and cellular perspective. Neurotox Res. 2025;43:22. doi:10.1007/s12640-025-00744-4
10. Zhang Y, Zhang X, Zhou J, Li Y, Kai T, Zhang L. Lycium ruthenicum murray exosome-like nanovesicles alleviated Alzheimer’s disease-like symptoms induced by Aβ protein in transgenic caenorhabditis elegans through the DAF-16 pathway. Int J Biol Macromol. 2025;304:140758. doi:10.1016/j.ijbiomac.2025.140758
11. Counil H, Krantic S. Synaptic activity and (Neuro)Inflammation in Alzheimer’s disease: could exosomes be an additional link? J Alzheimers Dis. 2020;74:1029–1043. doi:10.3233/JAD-191237
12. Hamlett ED, Ledreux A, Potter H, et al. Exosomal biomarkers in down syndrome and Alzheimer’s disease. Free Radic Biol Med. 2018;114:110–121. doi:10.1016/j.freeradbiomed.2017.08.028
13. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13:e12404.
14. Kaur S, Verma H, Dhiman M, et al. Brain exosomes: friend or foe in alzheimer’s disease? Mol Neurobiol. 2021;58:6610–6624. doi:10.1007/s12035-021-02547-y
15. Couch Y, Buzàs EI, Di Vizio D, et al. A brief history of nearly EV-erything - The rise and rise of extracellular vesicles. J Extracell Vesicles. 2021;10:e12144.
16. Wang L, Shui X, Diao Y, Chen D, Zhou Y, Lee TH. Potential implications of miRNAs in the pathogenesis, diagnosis, and therapeutics of Alzheimer’s disease. Int J Mol Sci. 2023;25(1):24. doi:10.3390/ijms25010024
17. Boccardi V, Poli G, Cecchetti R, et al. miRNAs and Alzheimer’s disease: exploring the role of inflammation and vitamin E in an old-age population. Nutrients. 2023:15.
18. Lei LM, Lin X, Xu F, et al. Exosomes and obesity-related insulin resistance. Front Cell Dev Biol. 2021;9:651996. doi:10.3389/fcell.2021.651996
19. Paolicelli RC, Bergamini G, Rajendran L. Cell-to-cell communication by extracellular vesicles: focus on microglia. Neuroscience. 2019;405:148–157. doi:10.1016/j.neuroscience.2018.04.003
20. Alvarez-Erviti L, Seow Y, Yin H, Betts C, Lakhal S, Wood MJ. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat Biotechnol. 2011;29:341–345. doi:10.1038/nbt.1807
21. Cui CX, Shao XN, Li YY, Qiao L, Lin JT, Guan LH. Therapeutic potential of mesenchymal stem cells in neurodegenerative diseases. World J Stem Cells. 2025;17:107717. doi:10.4252/wjsc.v17.i8.107717
22. Kuzu A, Jawad SR, Canli, Züdoru A M, Özüdoğru A. Investigation of efficacy of high and low intensity laser therapy in patients with lumbar disc herniation: a randomized controlled trial. J Med Biol Eng. 2025;45(5):738–744. doi:10.1007/s40846-025-00989-6
23. Cao Z, Kong F, Ding J, Chen C, He F, Deng W. Promoting Alzheimer’s disease research and therapy with stem cell technology. Stem Cell Res Ther. 2024;15:136. doi:10.1186/s13287-024-03737-w
24. Li Y, Zhang J, Wan J, Liu A, Sun J. Melatonin regulates Aβ production/clearance balance and Aβ neurotoxicity: a potential therapeutic molecule for Alzheimer’s disease. Biomed Pharmacother. 2020;132:110887. doi:10.1016/j.biopha.2020.110887
25. Pang C, Zhang J, Gu Y, Zhang Q, Zhao Y. The biological roles of exosome-encapsulated traditional Chinese medicine monomers in neuronal disorders. J Pharm Anal. 2025;15:101131. doi:10.1016/j.jpha.2024.101131
26. Ozansoy M, Mikati H, Velioglu HA, Yulug B. Exosomes: a missing link between chronic systemic inflammation and Alzheimer’s disease? Biomed Pharmacother. 2023;159:114161. doi:10.1016/j.biopha.2022.114161
27. Chunhui G, Yanqiu Y, Jibing C, Ning L, Fujun L. Exosomes and non-coding RNAs: bridging the gap in Alzheimer’s pathogenesis and therapeutics. Metab Brain Dis. 2025;40:84. doi:10.1007/s11011-024-01520-7
28. Zhou Y, Rong Y. Hypoxic natural killer cells-derived HIF-1α-Containing exosomes inhibit cellular senescence and apoptosis in neurocytes to ameliorate alzheimer’s disease by eliminating oxidative damages. Mol Neurobiol. 2025;62:13089–13102. doi:10.1007/s12035-025-05111-0
29. Kim E, Otgontenger U, Jamsranjav A, Kim SS. Deleterious alteration of glia in the brain of alzheimer’s disease. Int J Mol Sci. 2020;22(1):21. doi:10.3390/ijms22010021
30. Elia CA, Losurdo M, Malosio ML, Coco S. Extracellular vesicles from mesenchymal stem cells exert pleiotropic effects on amyloid-β, inflammation, and regeneration: a spark of hope for alzheimer’s disease from tiny structures? Bioessays. 2019;41:e1800199.
31. Canseco-Rodriguez A, Masola V, Aliperti V, Meseguer-Beltran M, Donizetti A, Sanchez-Perez AM. Long non-coding RNAs, extracellular vesicles and inflammation in Alzheimer’s disease. Int J Mol Sci. 2022;23(21):13171. doi:10.3390/ijms232113171
32. Engin A. Dark-side of exosomes. Adv Exp Med Biol. 2021;1275:101–131.
33. Pascual M, Calvo-Rodriguez M, Núñez L, Villalobos C, Ureña J, Guerri C. Toll-like receptors in neuroinflammation, neurodegeneration, and alcohol-induced brain damage. IUBMB Life. 2021;73:900–915. doi:10.1002/iub.2510
34. Tan P, Mei J, Wang D. Evaluation of the effect of phellodendrin application on rats creating an experimental model of non-compression lumbar disc herniation on the NF-κB-related inflammatory signaling pathway. J Orthop Surg Res. 2024;19:816. doi:10.1186/s13018-024-05313-7
35. Vandendriessche C, Bruggeman A, Van Cauwenberghe C, Vandenbroucke RE, Hölscher C. Extracellular vesicles in Alzheimer’s and Parkinson’s disease: small entities with large consequences. Cells. 2020;10(1):9. doi:10.3390/cells10010009
36. Bir A, Ghosh A, Chauhan A, et al. Exosomal dynamics and brain redox imbalance: implications in Alzheimer’s disease pathology and diagnosis. Antioxidants. 2024;14(1):13. doi:10.3390/antiox14010013
37. Bashirrohelleh MA, Bavarsad K, Khodadadi A, Shohan M, Asadirad A. Curcumin-enhanced stem cell exosomes: a novel approach to modulating neuroinflammation and improving cognitive function in a rat model of Alzheimer’s disease. Eur J Pharmacol. 2025;999:177695. doi:10.1016/j.ejphar.2025.177695
38. Pluta R, Ułamek-Kozioł M. Lymphocytes, platelets, erythrocytes, and exosomes as possible biomarkers for alzheimer’s disease clinical diagnosis. Adv Exp Med Biol. 2019;1118:71–82.
39. D’Egidio F, Castelli V, d’Angelo M, Ammannito F, Quintiliani M, Cimini A. Brain incoming call from glia during neuroinflammation: roles of extracellular vesicles. Neurobiol Dis. 2024;201:106663. doi:10.1016/j.nbd.2024.106663
40. Garcia G, Pinto S, Ferreira S, et al. Emerging role of miR-21-5p in neuron-glia dysregulation and exosome transfer using multiple models of Alzheimer’s disease. Cells. 2022;12(1):11. doi:10.3390/cells12010011
41. Verduzco Espinoza AP, Na N, Campanati L, Ngo P, Baldwin KK, Cline HT. Microglia-to-neuron signaling links APOE4 and inflammation to enhanced neuronal lipid metabolism and network activity. Proc Natl Acad Sci U S A. 2025;122:e2516103122.
42. Shamseddine AA, Airola MV, Hannun YA. Roles and regulation of neutral sphingomyelinase-2 in cellular and pathological processes. Adv Biol Regul. 2015;57:24–41. doi:10.1016/j.jbior.2014.10.002
43. Odfalk KF, Bieniek KF, Hopp SC. Microglia: friend and foe in tauopathy. Prog Neurobiol. 2022;216:102306. doi:10.1016/j.pneurobio.2022.102306
44. Kumari M, Anji A, Khan LU. Small but mighty-exosomes, novel intercellular messengers in neurodegeneration. Biology. 2022;12(1):11. doi:10.3390/biology12010011
45. Doita M, Kanatani T, Harada T, Mizuno K. Immunohistologic study of the ruptured intervertebral disc of the lumbar spine. Spine. 1996;21:235–241. doi:10.1097/00007632-199601150-00015
46. Cosamalón-Gan I, Cosamalón-Gan T, Mattos-Piaggio G, Villar-Suárez V, García-Cosamalón J, Vega-álvarez JA. Inflammation in the intervertebral disc herniation. Neurocirugia. 2021;32:21–35. doi:10.1016/j.neucie.2020.04.001
47. Nygaard OP, Mellgren SI, Osterud B. The inflammatory properties of contained and noncontained lumbar disc herniation. Spine. 1997;22:2484–2488. doi:10.1097/00007632-199711010-00004
48. Tian P, Li ZJ, Fu X, Ma XL. Role of interleukin-17 in chondrocytes of herniated intervertebral lumbar discs. Exp Ther Med. 2015;10:81–87. doi:10.3892/etm.2015.2449
49. Li XC, Luo SJ, Wu F, et al. Investigation of macrophage polarization in herniated nucleus pulposus of patients with lumbar intervertebral disc herniation. J Orthop Res. 2023;41:1335–1347. doi:10.1002/jor.25480
50. Feng ZY, Hu XJ, Zheng QQ, Battié MC, Chen Z, Wang Y. Cartilaginous endplate avulsion is associated with modic changes and endplate defects, and residual back and leg pain following lumbar discectomy. Osteoarthritis Cartilage. 2021;29:707–717. doi:10.1016/j.joca.2021.01.010
51. Kim H, Hong JY, Lee J, Jeon WJ, Ha IH. IL-1β promotes disc degeneration and inflammation through direct injection of intervertebral disc in a rat lumbar disc herniation model. Spine J. 2021;21:1031–1041. doi:10.1016/j.spinee.2021.01.014
52. Zhang A, Wang K, Ding L, et al. Bay11-7082 attenuates neuropathic pain via inhibition of nuclear factor-kappa B and nucleotide-binding domain-like receptor protein 3 inflammasome activation in dorsal root ganglions in a rat model of lumbar disc herniation. J Pain Res. 2017;10:375–382. doi:10.2147/JPR.S119820
53. Tan JH, Li ZP, Liu LL, Liu H, Xue JB. IL-17 in intervertebral disc degeneration: mechanistic insights and therapeutic implications. Cell Biol Int. 2022;46:535–547. doi:10.1002/cbin.11767
54. Wang K, Bao JP, Yang S, et al. A cohort study comparing the serum levels of pro- or anti-inflammatory cytokines in patients with lumbar radicular pain and healthy subjects. Eur Spine J. 2016;25:1428–1434. doi:10.1007/s00586-015-4349-4
55. Morkoç B, Aktan O, Solak HS, et al. Inflammatory and analgesic profiles in intervertebral disc herniation: variability with respect to neurological deficit. Niger J Clin Pract. 2025;28:393–400. doi:10.4103/njcp.njcp_814_24
56. Pedersen LM, Schistad E, Jacobsen LM, Røe C, Gjerstad J. Serum levels of the pro-inflammatory interleukins 6 (IL-6) and −8 (IL-8) in patients with lumbar radicular pain due to disc herniation: a 12-month prospective study. Brain Behav Immun. 2015;46:132–136. doi:10.1016/j.bbi.2015.01.008
57. Cheng L, Fan W, Liu B, Wang X, Nie L. Th17 lymphocyte levels are higher in patients with ruptured than non-ruptured lumbar discs, and are correlated with pain intensity. Injury. 2013;44:1805–1810. doi:10.1016/j.injury.2013.04.010
58. Chen X, Wang W, Cui P, Li Y, Lu S. Evidence of MRI image features and inflammatory biomarkers association with low back pain in patients with lumbar disc herniation. Spine J. 2024;24:1192–1201. doi:10.1016/j.spinee.2024.02.006
59. Huang Y, Li Y, Zhong X, et al. Src-family kinases activation in spinal microglia contributes to central sensitization and chronic pain after lumbar disc herniation. Mol Pain. 2017;13:1744806917733637. doi:10.1177/1744806917733637
60. Pan F, Zeng F, Chen Y, et al. Warm acupuncture reduces pain and inflammation in rats with lumbar disc herniation induced by autologous nucleus pulposus transplantation via regulating p38MAPK/NF-κB pathway. J Acupunct Meridian Stud. 2024;17:28–37. doi:10.51507/j.jams.2024.17.1.28
61. Sun C, Tian J, Liu X, Guan G. MiR-21 promotes fibrosis and hypertrophy of ligamentum flavum in lumbar spinal canal stenosis by activating IL-6 expression. Biochem Biophys Res Commun. 2017;490:1106–1111. doi:10.1016/j.bbrc.2017.06.182
62. Jimbo K, Park JS, Yokosuka K, Sato K, Nagata K. Positive feedback loop of interleukin-1beta upregulating production of inflammatory mediators in human intervertebral disc cells in vitro. J Neurosurg Spine. 2005;2:589–595. doi:10.3171/spi.2005.2.5.0589
63. Chen X, Hodges PW, James G, Diwan AD. Do markers of inflammation and/or muscle regeneration in lumbar multifidus muscle and fat differ between individuals with good or poor outcome following microdiscectomy for lumbar disc herniation? Spine. 2021;46:678–686. doi:10.1097/BRS.0000000000003863
64. Li S, Chen T, Zhou Y, Li X. Palmitic acid and trans-4-hydroxy-3-methoxycinnamate, the active ingredients of Yaobishu formula, reduce inflammation and pain by regulating gut microbiota and metabolic changes after lumbar disc herniation to activate autophagy and the Wnt/β-catenin pathway. Biochim Biophys Acta Mol Basis Dis. 2024;1870:166972. doi:10.1016/j.bbadis.2023.166972
65. Liu J, Ye YJ, Liu SM, Liu S. Analysis of the effect of midazolam on pain in a rat model of lumbar disc herniation based on the p38 MAPK signaling pathway. Zhongguo Gu Shang. 2023;36:55–60. doi:10.12200/j.issn.1003-0034.2023.01.010
66. De Souza Grava AL, Ferrari LF, Defino HLA, De Souza Grava HL. Cytokine inhibition and time-related influence of inflammatory stimuli on the hyperalgesia induced by the nucleus pulposus. Eur Spine J. 2012;21(3):537–545. doi:10.1007/s00586-011-2027-8
67. Ahn SH, Cho YW, Ahn MW, Jang SH, Sohn YK, Kim H-S. mRNA expression of cytokines and chemokines in herniated lumbar intervertebral discs. Spine. 2002;27(9):911–917. doi:10.1097/00007632-200205010-00005
68. Burke JG, Watson RW, McCormack D, Dowling FE, Walsh MG, Fitzpatrick JM. Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators. J Bone Joint Surg Br. 2002;84:196–201. doi:10.1302/0301-620X.84B2.0840196
69. Zheng J, Song Y, Yu B. GPNMB suppresses inflammation and extracellular matrix degradation in nucleus pulposus cells by inhibiting pro-inflammatory cytokine production and activation of the NF-κB signaling pathway. J Interferon Cytokine Res. 2025;45:238–246. doi:10.1089/jir.2025.0022
70. Liu YL, Yang H, Zhang M, et al. Short-term effect of Isobar dynamic stabilization system fixation combined with lumbar discectomy in patients with lumbar disc herniation. Zhonghua Yi Xue Za Zhi. 2019;99:188–192. doi:10.3760/cma.j.issn.0376-2491.2019.03.007
71. Hur JW, Bae T, Ye S, et al. Myofibroblast in the ligamentum flavum hypertrophic activity. Eur Spine J. 2017;26:2021–2030. doi:10.1007/s00586-017-4981-2
72. Wang JN, Zhao XJ, Liu ZH, Zhao XL, Sun T, Fu ZJ. Selective phosphodiesterase-2A inhibitor alleviates radicular inflammation and mechanical allodynia in non-compressive lumbar disc herniation rats. Eur Spine J. 2017;26:1961–1968. doi:10.1007/s00586-017-5023-9
73. Yediyıldız MB, Durmuş İ, Ak HY, et al. Comparison of inhalation and total intravenous anesthesia on inflammatory markers in microdiscectomy: a double-blind study. BMC Anesthesiol. 2025;25:238. doi:10.1186/s12871-025-03119-6
74. Kim WK, Shin JS, Lee J, et al. Effects of the administration of Shinbaro 2 in a rat lumbar disk herniation model. Front Neurol. 2023;14:1044724. doi:10.3389/fneur.2023.1044724
75. Rožac K, Matić A, Budrovac D, et al. Biological mechanisms of pain management in lumbar disk herniation: focus on cytokine correlations and therapeutic approaches. Int J Mol Sci. 2025;27(1):26. doi:10.3390/ijms27010026
76. Liu G, Liu W, Jin D, Yan P, Yang Z, Liu R. Clinical outcomes of unilateral biportal endoscopic lumbar interbody fusion (ULIF) compared with conventional posterior lumbar interbody fusion (PLIF). Spine J. 2023;23:271–280. doi:10.1016/j.spinee.2022.10.001
77. Shi F, Wu Z, Yin J, Liu Y, Li Z, Zhang S. Acupuncture mitigates sciatic neuropathic pain in lumbar disc herniation via inhibiting spinal CXCL12/CXCR4-driven glial activation and neuroinflammation. J Neuroimmunol. 2026;410:578797. doi:10.1016/j.jneuroim.2025.578797
78. Ura K, Yamada K, Tsujimoto T, Ukeba D, Iwasaki N, Sudo H. Ultra-purified alginate gel implantation decreases inflammatory cytokine levels, prevents intervertebral disc degeneration, and reduces acute pain after discectomy. Sci Rep. 2021;11:638. doi:10.1038/s41598-020-79958-9
79. Qu M, Ding XN, Liu HB, Liu YQ. Clinical observation on acupuncture combined with nerve block for treatment of lumbar disc herniation. Zhongguo Zhen Jiu. 2010;30:633–636.
80. Albert HB, Sayari AJ, Barajas JN, et al. The impact of novel inflammation-preserving treatment towards lumbar disc herniation resorption in symptomatic patients: a prospective, multi-imaging and clinical outcomes study. Eur Spine J. 2024;33:964–973. doi:10.1007/s00586-023-08064-x
81. Weber KT, Alipui DO, Sison CP, et al. Serum levels of the proinflammatory cytokine interleukin-6 vary based on diagnoses in individuals with lumbar intervertebral disc diseases. Arthritis Res Ther. 2016;18:3. doi:10.1186/s13075-015-0887-8
82. Xue H, Yao Y, Wang X, et al. Interleukin-21 is associated with the pathogenesis of lumbar disc herniation. Iran J Allergy Asthma Immunol. 2015;14:509–518.
83. Chen B, Liu Y, Zhang Y, Li J, Cheng K, Cheng L. IL-21 Is Positively Associated with Intervertebral Disc Degeneration by Interaction with TNF-α Through the JAK-STAT Signaling Pathway. Inflammation. 2017;40:612–622. doi:10.1007/s10753-017-0508-6
84. Bečulić H, Begagić E, Šegalo S, et al. Histopathologic degenerative score as a predictor of minimal clinically important difference in pain and functionality following surgical treatment for disc herniation. Biomol Biomed. 2025;25:623–631. doi:10.17305/bb.2024.10877
85. Juković-Bihorac F, Bečulić H, Begagić E, et al. Histopathological spectrum of lumbar disc changes in obesity: analysis of intervertebral discs in lumbar hernia patients in Zenica-Doboj Canton, Bosnia and Herzegovina. Med Glas. 2024;21:140–146. doi:10.17392/1698-23
86. Di XS, Chen J, Wang XR, et al. Progress of researches on mechanisms of acupuncture therapy in the treatment of lumbar disc herniation. Zhen Ci Yan Jiu. 2024;49:526–533. doi:10.13702/j.1000-0607.20230129
87. Liu ZF, Wang HR, Yu TY, Zhang YQ, Jiao Y, Wang XY. Tuina for peripherally-induced neuropathic pain: a review of analgesic mechanism. Front Neurosci. 2022;16:1096734. doi:10.3389/fnins.2022.1096734
88. Huang SJ, Yan JQ, Luo H, Zhou LY, Luo JG. IL-33/ST2 signaling contributes to radicular pain by modulating MAPK and NF-κB activation and inflammatory mediator expression in the spinal cord in rat models of noncompressive lumber disk herniation. J Neuroinflammation. 2018;15:12. doi:10.1186/s12974-017-1021-4
89. Goo B, Kim SJ, Kim EJ, et al. Clinical research on the efficacy and safety of Bosinji for low back pain with radiculopathy caused by herniated intervertebral disc of the lumbar spine: a protocol for a multicenter, randomized, controlled equivalence trial. Medicine. 2018;97:e13684.
90. Dong FH. Precise application of Traditional Chinese Medicine in minimally-invasive techniques]. Zhongguo Gu Shang. 2018;31:493–496.
91. Çetin E, Başgül Sagiri D, Kahraman Özlü EB, et al. Inflammatory biomarkers in smokers: implications for ligamentum flavum hypertrophy. Med Sci Monit. 2025;31:e947508.
92. Kocaoğlu S, Sagiri DB, Kahraman Özlü EB, et al. The impact of smoking on inflammatory biomarkers in intervertebral disc degeneration: a biochemical and diagnostic evaluation. Clin Spine Surg. 2025. doi:10.1097/BSD.0000000000001942
93. Andrade P, Hoogland G, Garcia MA, Steinbusch HW, Daemen MA, Visser-Vandewalle V. Elevated IL-1β and IL-6 levels in lumbar herniated discs in patients with sciatic pain. Eur Spine J. 2013;22:714–720. doi:10.1007/s00586-012-2502-x
94. Shi F, Wu Z, Li Z, et al. Exploring potential mechanistic aspects of “Biaoben acupoint” acupuncture for lumbar disc herniation using 4D proteomics. Front Neurol. 2025;16:1630736. doi:10.3389/fneur.2025.1630736
95. Koh AR, Kim HW, Lee YJ, et al. Integrative Korean medicine for recurrent lumbar disc herniation after coronavirus disease vaccination: a case report and literature review. Medicine. 2025;104:e41079. doi:10.1097/MD.0000000000041079
96. Lin X, Lin Q. MiRNA-495-3p attenuates TNF-α induced apoptosis and inflammation in human nucleus pulposus cells by targeting IL5RA. Inflammation. 2020;43:1797–1805. doi:10.1007/s10753-020-01254-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Innovative Insights into Interleukin-Mediated Macrophage Polarization: Metabolic Reprogramming and Inflammatory Pathway Crosstalk in Chronic Kidney Disease and Therapeutic Implications—A Narrative Review
Jiang Z, Zhang X, Jin L, Han M, Zhang Y, Jiang Y, Zhang J, Jin L
International Journal of General Medicine 2026, 19:610534
Published Date: 15 June 2026