")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Interactive Nutrition Education Is More Effective in Terms of Improved Levels of Glycated Hemoglobin in Adolescent Patients with Poorly Controlled Type 1 Diabetes – A Randomized Study
Authors Dłużniak-Gołaska K , Panczyk M , Szypowska A , Sińska B , Szostak-Węgierek D
Received 30 August 2019
Accepted for publication 5 November 2019
Published 10 December 2019 Volume 2019:12 Pages 2619—2631
DOI https://doi.org/10.2147/DMSO.S229246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Karolina Dłużniak-Gołaska,1 Mariusz Panczyk,2 Agnieszka Szypowska,3 Beata Sińska,4 Dorota Szostak-Węgierek1
1Department of Clinical Dietetics, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland; 2Department of Education and Research in Health Sciences, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland; 3Department of Pediatrics, The First Faculty of Medicine, Medical University of Warsaw, Warsaw, Poland; 4Department of Human Nutrition, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland
Correspondence: Mariusz Panczyk
Department of Education and Research in Health Sciences, Faculty of Health Sciences, Medical University of Warsaw, Zwirki i Wigury 61, Warsaw 02-091, Poland
Tel +48 22 572 0490
Fax +48 22 572 0491
Email [email protected]
Introduction: Effectively conducted nutrition education is one of the key elements of the therapy of type 1 diabetes. The aim of the study was to compare the effectiveness of two methods of nutrition education.
Material and methods: A noninvasive interventional randomized single-blind study included 151 patients (13.7±2.2 years old) with poorly controlled type 1 diabetes, treated with the use of insulin pumps. The participants were randomly divided into two groups: a control group (C) in which informative education methods were used (a lecture) and an experimental group (E) in which interactive methods (quiz and multimedia application) were additionally applied. The concentration of glycated hemoglobin (HbA1c) was the primary outcome. The secondary outcomes were: standard deviation score-body mass index (SDS-BMI), standard deviation score-systolic blood pressure (SDS-SBP), standard deviation score-diastolic blood pressure (SDS-DBP), scores of Nutrition Knowledge Survey (NKS) and indices of healthy and unhealthy diet.
Results: A marked reduction in HbA1c concentrations was observed after 3 months in group E [−0.47% (−0.77; −0.17), P<0.01; P=0.038 for the intergroup difference]. The positive effect was no longer present after 6 months. No significant changes regarding HbA1c were noted in group C at any stage of the study. After 6 months, both groups obtained better results in one part of NKS (“Blood glucose response to food”): group C [0.41 (0.15; 0.66), P<0.01], group E [0.80 (0.52; 1.08), P<0.001; P=0.042 for the intergroup difference]. No statistically significant differences between groups were noted as regards the remaining parameters.
Conclusion: Interactive nutrition education is more effective in terms of improved levels of HbA1c in children and adolescents with poorly controlled diabetes. However, an intensification of training frequency is recommended due to the transient effect of education.
Keywords: nutrition education, type 1 diabetes, glycated hemoglobin
Introduction
Type 1 diabetes mellitus is an autoimmune disease characterized by an injury to β cells of the pancreas which are responsible for insulin production. Currently, it is one of the most common chronic diseases occurring in children and adolescents.1 The process of the treatment of type 1 diabetes involves daily administration of insulin, monitoring glycemia and caring for appropriate quality of the diet.2 Numerous patients suffering from type 1 diabetes find it difficult to achieve proper control of glycemia.2,3 Therefore, education, also nutrition education, is an essential element of the treatment of the disease.4,5 It needs to be emphasized that effectively conducted nutrition education combined with other components of the treatment may contribute to an improvement in clinical and metabolic parameters.5 Moreover, apart from parents and caregivers, children should also be involved in the educational process, so as to be able to control the disease independently in the future.6 However, educating children and adolescents requires particular attention.7 Methods employed during training should be trainee oriented, interactive, motivating and practical. The topics tackled should be interesting, useful and understandable. Education should focus on solving specific problems.8 It is also recommended to employ modern tools (such as mobile applications) during training in order to improve diabetes control.4 Seemingly, the implementation of informative methods of education only, based on one-way lecture, has low effectiveness.
The aim of the present study was to verify the effectiveness of two different methods of nutrition education and a comparison of their influence on selected clinical parameters, knowledge about nutrition and the quality of the diet in adolescent patients with type 1 diabetes.
Materials and Methods
Material
The study group included children and adolescents aged 8–17 years with at least 1-year history of type 1 diabetes, treated with the use of insulin pumps, with no concomitant chronic diseases (especially whose which require dietary modifications). The exclusion criteria were as follows: a diagnosis of a different type of diabetes, the presence of concomitant chronic diseases (eg, celiac disease), a history of the disease shorter than a year and treatment with multiple injections with insulin pens.
Ethics Statement
A noninvasive interventional randomized single-blind study was conducted. The study was performed between October 2017 and April 2019 at the Children’s Teaching Hospital in Warsaw. The study design was accepted by the Bioethics Committee of the Medical University of Warsaw (approval no AKBE/188/17 issued on the 10th of October 2017). All the procedures were consistent with ethical standards and the Declaration of Helsinki as of 1964, as amended. Prior to the study, all the participants and their parents or legal guardians expressed oral consent to participate in the study. This form of consent was acceptable and approved by the Bioethics Committee of the Medical University of Warsaw.
Methods
All the data were collected throughout patient hospitalizations at the Department of Pediatric Diabetology or during follow-up visits at the hospital Diabetology Clinic. Sociodemographic data and key information about the disease, treatment methods, control of glycemia and the frequency of hypo- and hyperglycemia episodes were collected during individual history taking. The remaining essential clinical data, including the results of anthropometric measurements (body weight and height, waist circumference), blood pressure and the concentration of glycated hemoglobin (HbA1c), were completed basing on the history of the present illness records of the patients. According to the recommendations of the International Society for Pediatric and Adolescent Diabetes (ISPAD), normal reference values for glycemia should be: 70–130 mg/dL before meals, 90–180 mg/dL postprandially and 80–140 mg/dL at bedtime. The target level of HbA1c for children, adolescents and adults younger than 25 for whom comprehensive care is available should be <7.0%.9
Basing on the obtained data, each patient had the body mass index (BMI) value calculated according to the formula: BMI = body weight [kg]/body height [m]2. The obtained values were interpreted with growth charts for BMI for girls and boys in the Polish population according to ranges specified by the authors. The results were standardized by determining the standard deviation score-body mass index (SDS-BMI) using the following formula: (raw score of the patient – average BMI for the specific age and gender)/standard deviation.10
The values of blood pressure were also interpreted with growth charts for girls and boys in the Polish population.11 Systolic and/or diastolic pressure ≥95th centile for the age, gender and height was assumed to be abnormal.12 Moreover, the results were standardized by determining standard deviation score-systolic blood pressure (SDS-SBP) and standard deviation score-diastolic blood pressure (SDS-DBP) with the following formulae: (raw score of the patient – average SBP or DBP for the specific age and gender)/standard deviation.11
The value of waist to height ratio (WHtR) was calculated basing on the formula: waist circumference [cm]/body height [cm]. WHtR index has a universal cutoff point of 0.5 regardless of gender, age and ethnicity. Values ≥0.5 indicate an increased metabolic risk.13
Two questionnaires were used in the study. They were completed by the patients during individual history taking sessions. A modified version of the KomPAN questionnaire was used to verify dietary habits and the quality of the diet.14 Two indices (“index of healthy diet” and “index of unhealthy diet”) comprising products (or groups of products) which were potentially recommended or nonrecommended for patients with type 1 diabetes were developed on the basis of the present authors’ version of the questionnaire. Index values were presented on the scale from 0 to 100, with higher results indicating a more marked consumption of a specific category of products.15
The assessment of knowledge concerning the rules of proper nutrition in type 1 diabetes was performed with the use of a modified version of Nutrition Knowledge Survey (NKS).16 The introduction of necessary changes resulted from the differences present in education (eg, using the system of carbohydrate exchanges and not grams of carbohydrates) and different dietary habits of children in the Polish population. The present authors’ questionnaire included 33 closed-ended single-answer questions. We assessed the scores obtained in the whole questionnaire and in its individual subscales. The scoring was as follows: the whole questionnaire (from 0 to 37), including “Healthful eating” section (from 0 to 22), “Blood glucose response to food” section (from 0 to 4), “Carbohydrate counting” section (from 0 to 4) and “Nutrition label reading” section (from 0 to 7). Higher results should be interpreted as better knowledge about issues regarding nutrition.
Study Design
The patients were randomly assigned to two groups using 1:1 technique. Simple randomization was used with a list of random numbers generated by computer software. In this way, two groups were distinguished: a control group (C) in which the patients were educated with the use of informative methods (lecture) and an experimental group (E) in which interactive methods were additionally applied (quiz + multimedia application). The patients were assigned to the groups by the trainer. However, they were not informed which group they joined. A detailed course of the individual stages of the study is presented in Table 1.
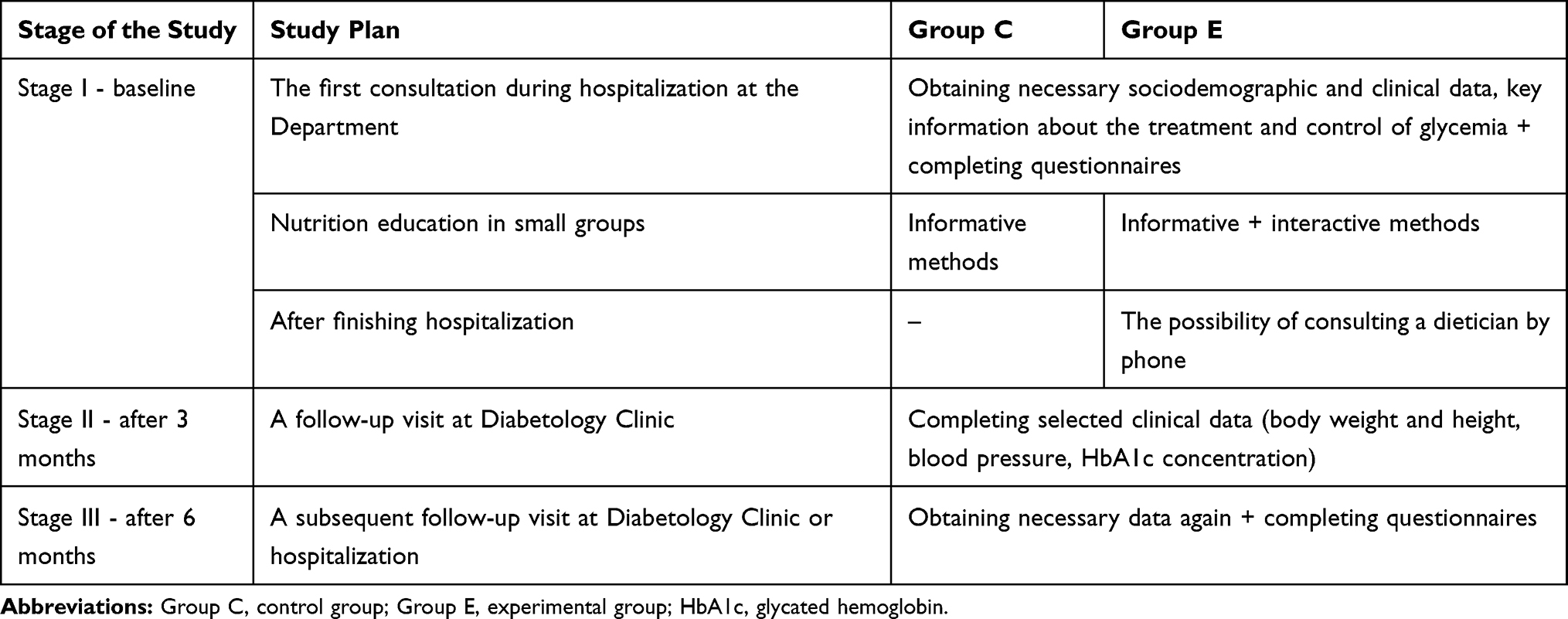 |
Table 1 Description of Individual Stages of the Study |
During the study, each patient participated in a training conducted during the hospitalization by a properly prepared dietician. Educating patients in the control group was conducted in the form of a 30-min lecture concerning the rules of proper nutrition in diabetes and counting carbohydrate exchanges (CE) and protein-fat exchanges (PFE). The lecture was also presented to the experimental group. Subsequently, practical issues became the focus. The present authors’ “true-false” quiz was used during the training. It included such elements as examples of correctly or incorrectly balanced meals, labels of healthy and unhealthy foods and photos of products and dishes in which the exchanges were to be calculated. Moreover, we used food packaging and VitaScale multimedia application which helps to calculate exchanges basing on data provided on food labels and includes an embedded database of products and dishes.17 After completing the training, each patient could download the application free of charge for personal use. The duration of the interactive part was about 60 mins. A detailed scenario of conducted nutrition education is presented in the “Supplementary data“ section (Figure S1 and Table S1).
Primary and Secondary Outcomes
The concentration of HbA1c was the primary outcome. The secondary outcomes were: the values of SDS-BMI, SDS-SBP, SDS-DBP and the scores obtained in NKS and the indices of healthy and unhealthy diet.
Sample size was estimated based on the primary outcome. The study was designed with 85% power to detect medium (0.50) effect size for the difference in HbA1c between the experimental and control groups at 6 months. Power calculations were based on a sample size of 146 participants completing the study with a 2-sided significance level of 0.05. Sample size was calculated using G*Power version 3.1.9.2 (Universität Kiel, Germany).18
Statistical Analyses
Differences between baseline characteristics of patients from group C and E were examined using a t-test, Fisher’s or Fisher-Freeman-Halton exact test, as appropriate. Descriptive statistics for all intergroup outcome measures are presented as mean (M) and standard deviation (SD). For nonmetric variables, data were shown using number (N) and frequency (%).
Treatment effects were examined using matched-pairs t-test and mixed-design analysis of variance and presented together with their 95% confidence intervals. For nonmetric variables, the treatment effect was estimated using the McNemar’s test and Cochran–Mantel–Haenszel test and presented together with their 95% confidence intervals for odds ratio (OR).
Data were analyzed using STATISTICA version 13.3 (Tibco Software Inc., Palo Alto, CA, USA). P-value lower than 0.05 was considered to indicate statistical significance.
Results
Patient Characteristics
The study included 196 patients who were randomly assigned to two groups: C (informative methods of education) and E (informative and interactive methods of education). However, only 189 of them received allocated intervention. A total of 38 persons were excluded during the subsequent stages of the study. There was no significant difference in the number of “lost to follow up” after 3 and 6 months between groups C and E. Finally, data of 151 patients were analyzed (Figure 1).
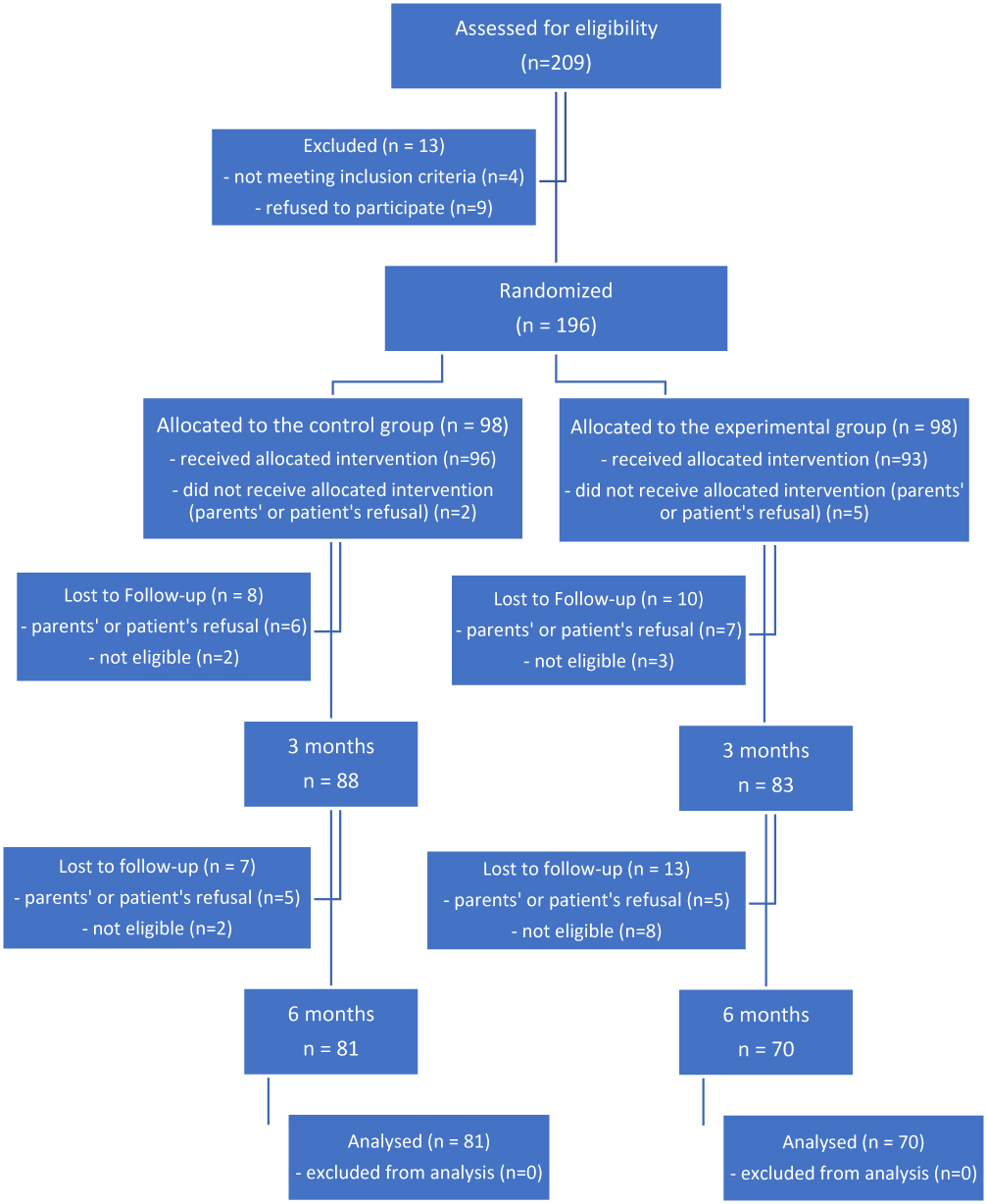 |
Figure 1 Study flow diagram. |
Initially, no statistically significant intergroup differences were noted as regards the majority of variables. However, it was noted that patients from group E were characterized by a significantly higher concentration of HbA1c and a higher mean score in one section of NKS – “Healthful eating” (Table 2). Moreover, a significant difference was observed as regards the structure of sex in both groups. There was a majority of girls in group E, while in group C the number of girls and boys was similar (Table 3).
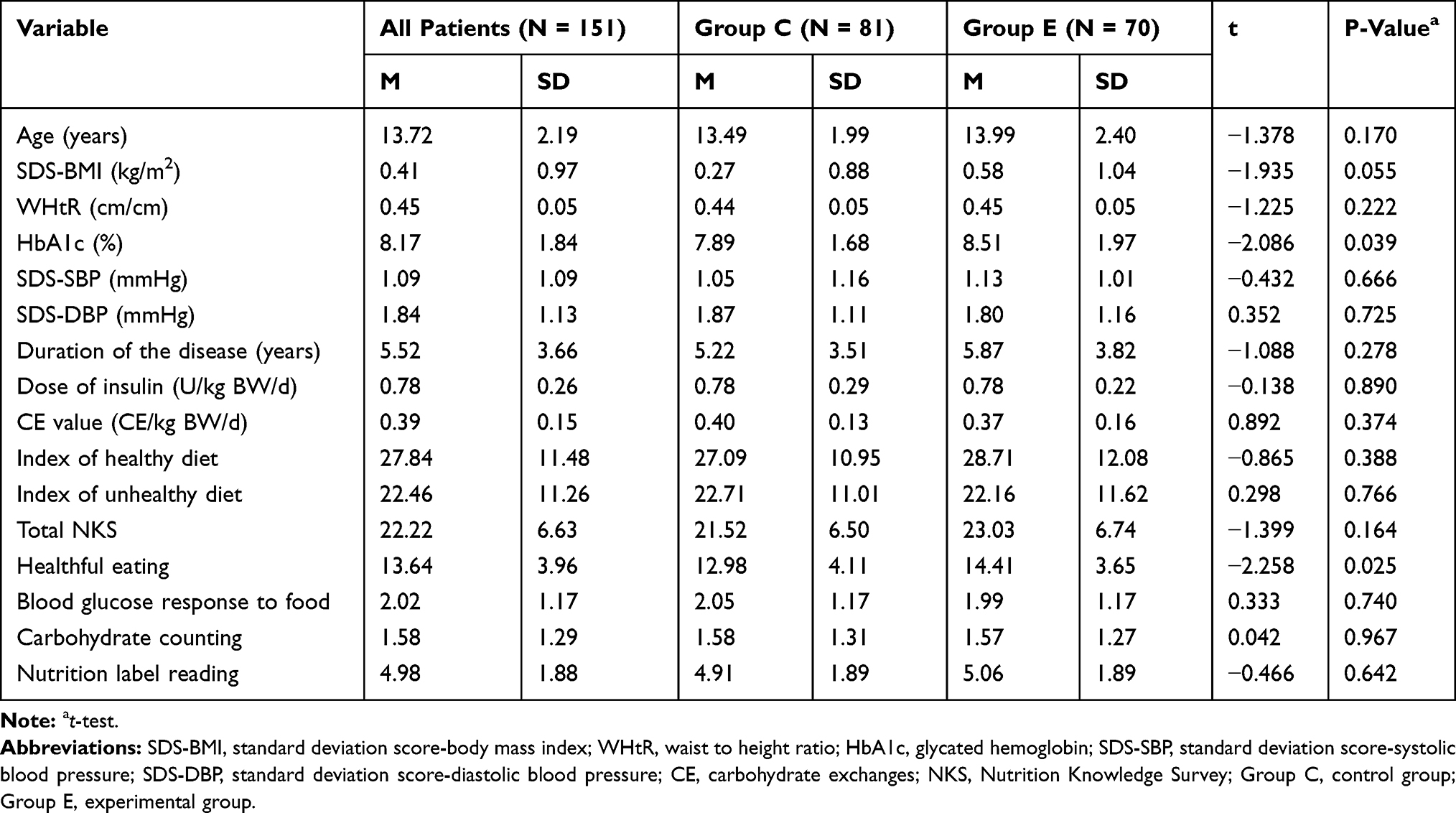 |
Table 2 Baseline Characteristics of Patients |
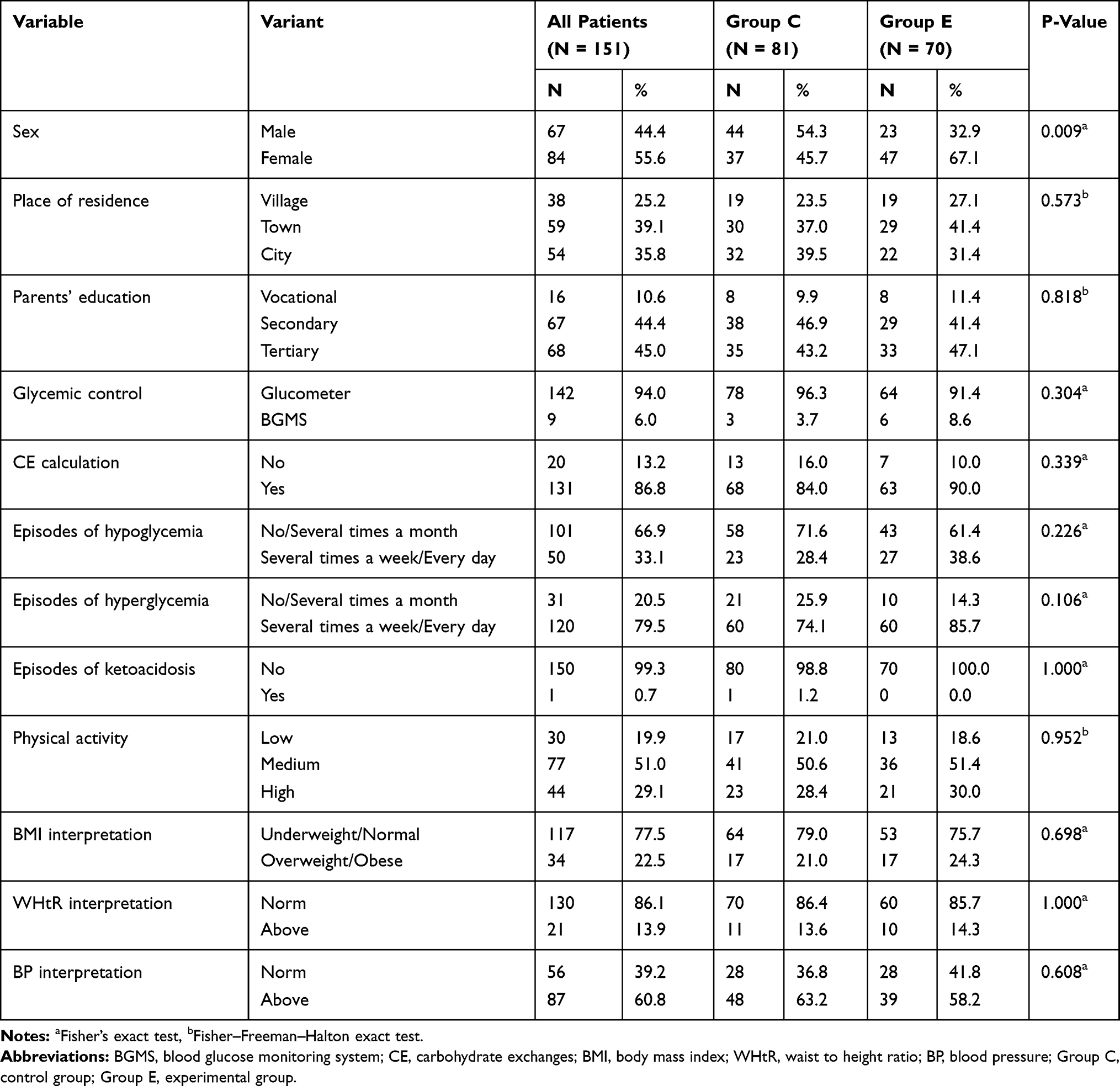 |
Table 3 Baseline Characteristics of Patients |
Changes from Baseline to 3 Months
During the second stage of the study, we assessed changes compared to baseline values and differences between groups as regards HbA1c concentrations, values of BMI and blood pressure.
No statistically significant changes were noted for HbA1c concentrations in group C. However, a significant reduction in its mean concentration was observed in group E. Moreover, the intergroup difference was statistically significant. In both groups, a significant increase in the mean value of SDS-BMI was noted, with a slightly higher value in group E. However, the intergroup difference was not statistically significant (Table 4). No changes were reported as regards the frequency of excessive body weight and respective intergroup differences (Table 5).
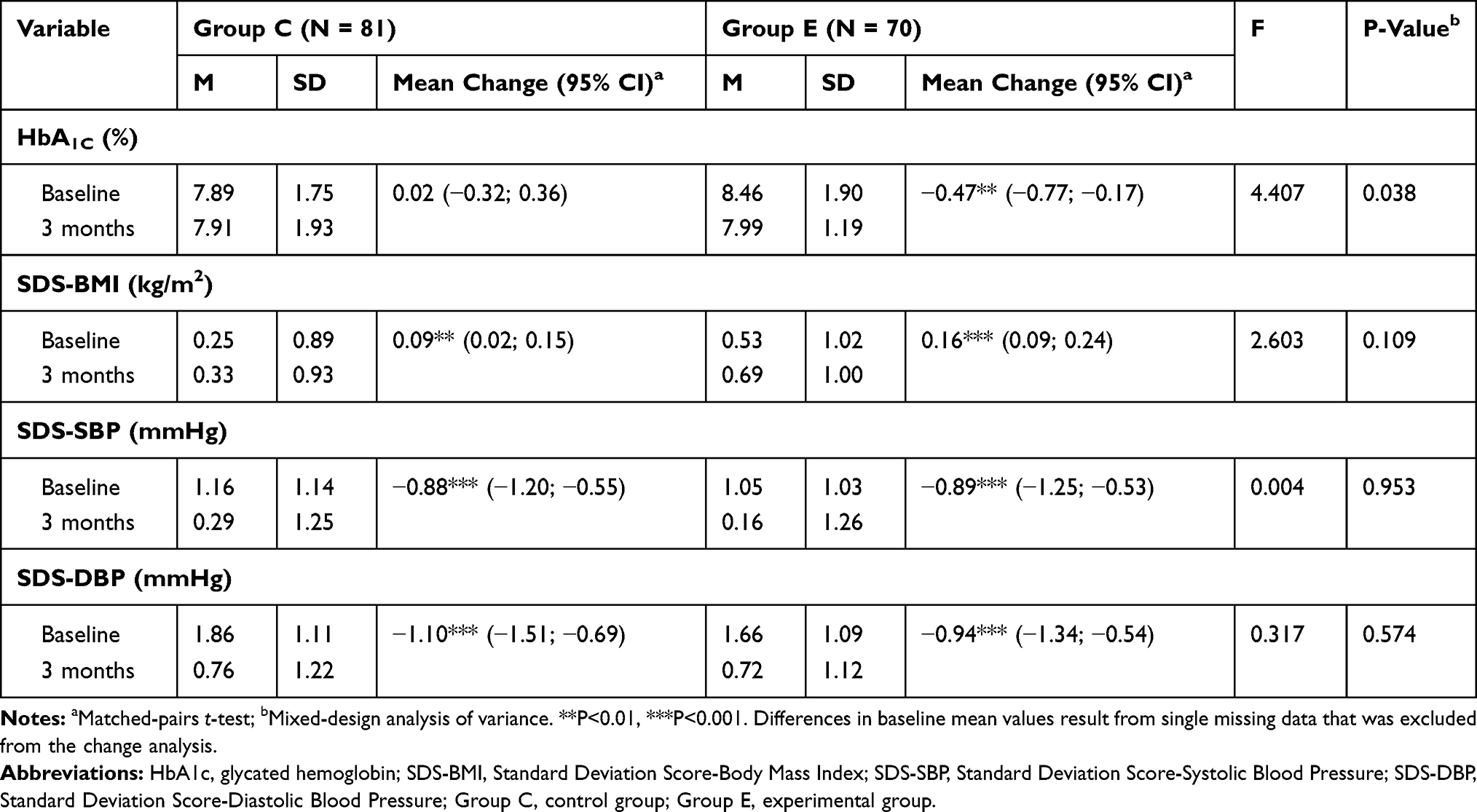 |
Table 4 Changes in Selected Clinical Parameters After 3 Months |
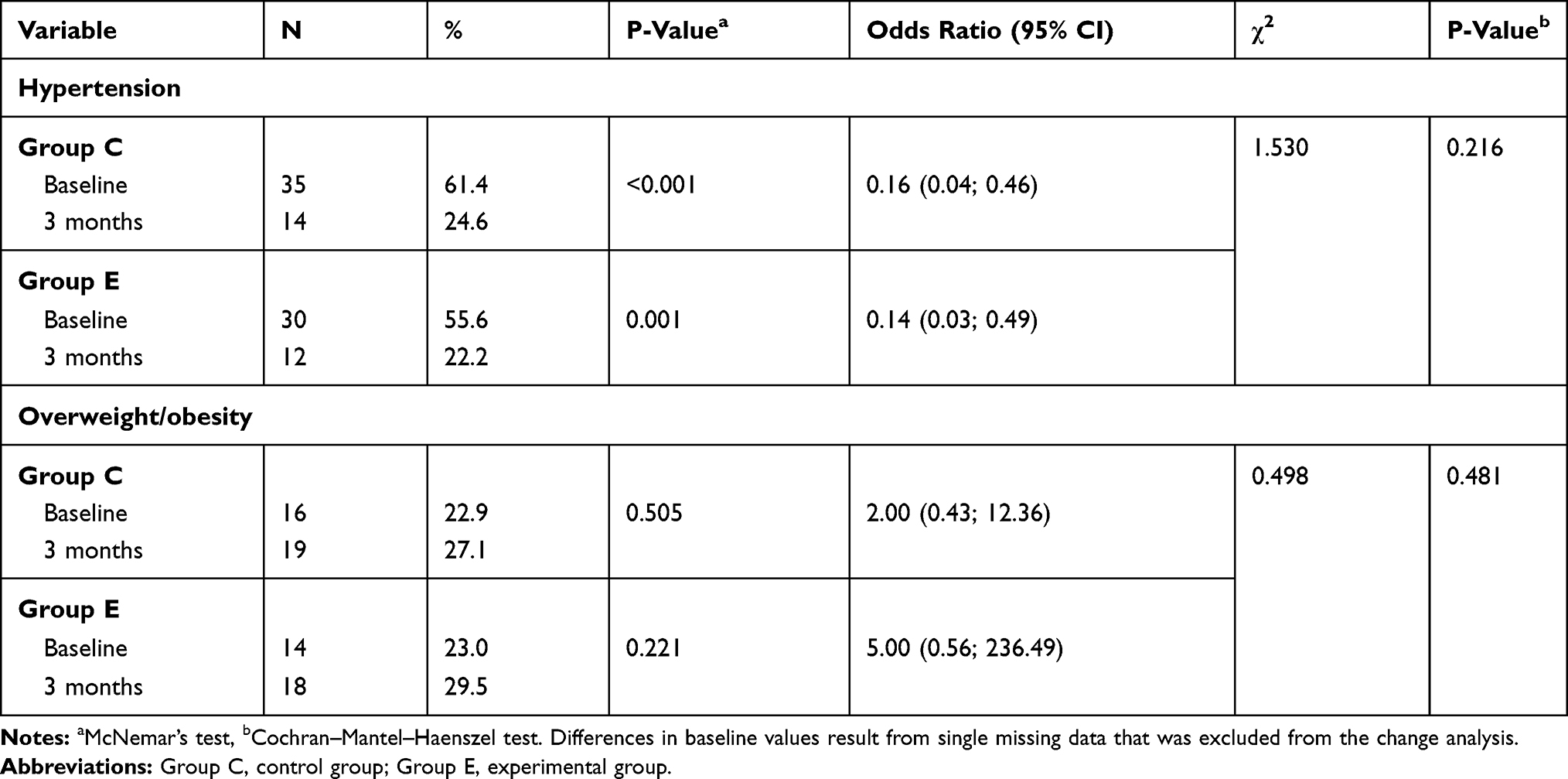 |
Table 5 Changes Regarding the Occurrence of Hypertension and Overweight/Obesity After 3 Months |
A significant reduction in the mean values of SDS-SBP and SDS-DBP was reported for both groups. However, the intergroup differences were not significant (Table 4). Furthermore, a significant improvement was noted for the occurrence of hypertension in both groups. However, the intergroup difference was not statistically significant (Table 5).
Changes from Baseline to 6 Months
During the third stage of the study, we assessed changes compared to baseline values and differences between groups as regards HbA1c concentrations, values of BMI, WHtR and blood pressure, daily CE value and insulin dose, scores referring to knowledge about nutrition and indices of diet quality.
Changes Regarding Clinical Parameters
No significant changes or differences were reported for HbA1c concentrations in both groups.
A significant increase in the mean value of SDS-BMI and reduction in the mean values of SDS-SBP and SDS-DBP were noted in group C. In group E, we found a significant increase in the mean values of SDS-BMI, WHtR and insulin dose (U/kg BW/d). A significant reduction in the mean values of SDS-SBP, SDS-DBP and CE value (CE/kg BW/d) was also noted. However, changes concerning the discussed variables did not significantly differ between study groups (Table 6).
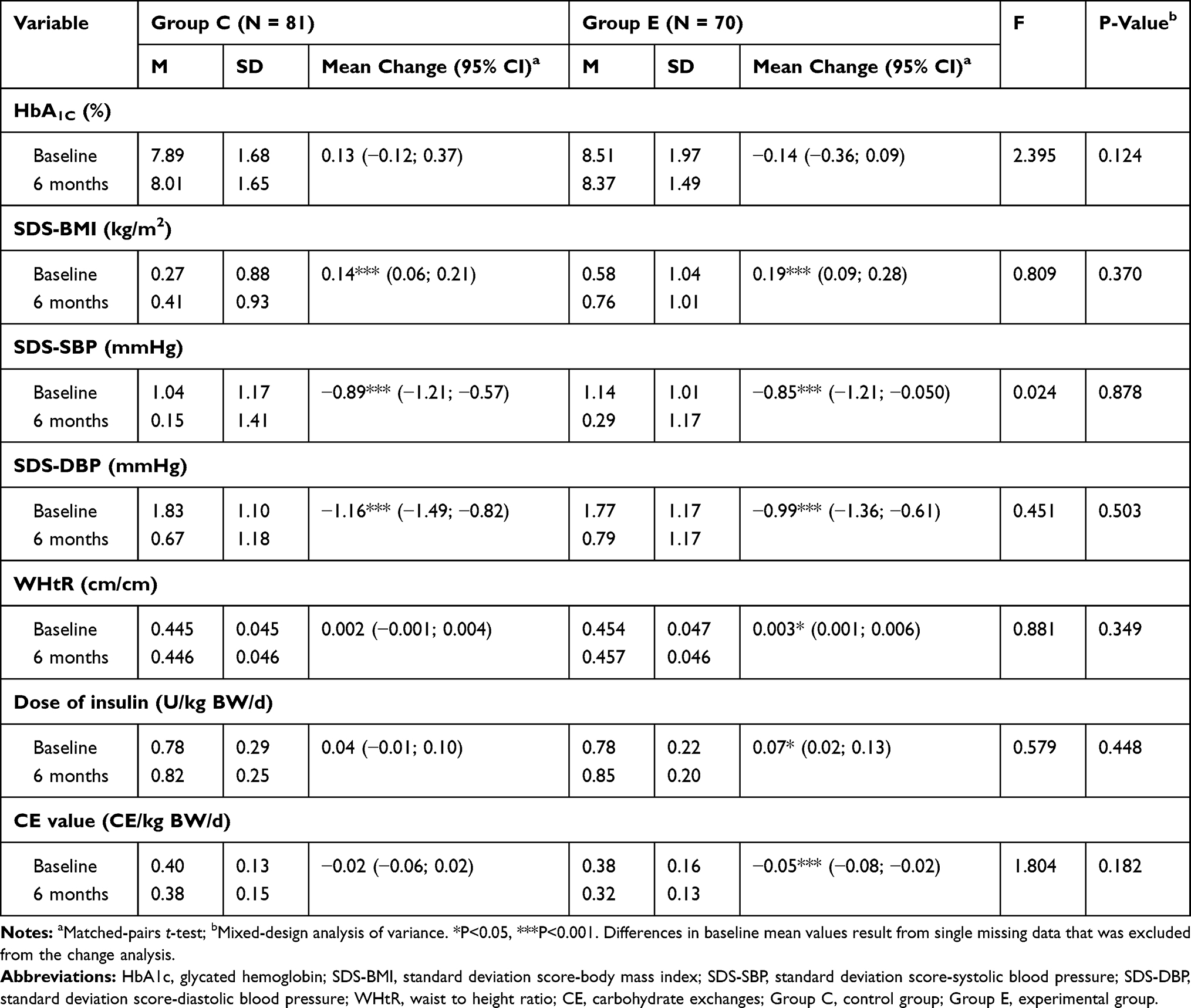 |
Table 6 Changes in Selected Clinical Parameters After 6 Months |
Both in group C and in group E, a significant improvement was observed as regards the occurrence of hypertension, but the intergroup difference was not statistically significant. Moreover, the percentage of overweight or obese patients significantly increased in group C, which was not observed in group E. However, the intergroup difference was not statistically significant in this matter (Table 7).
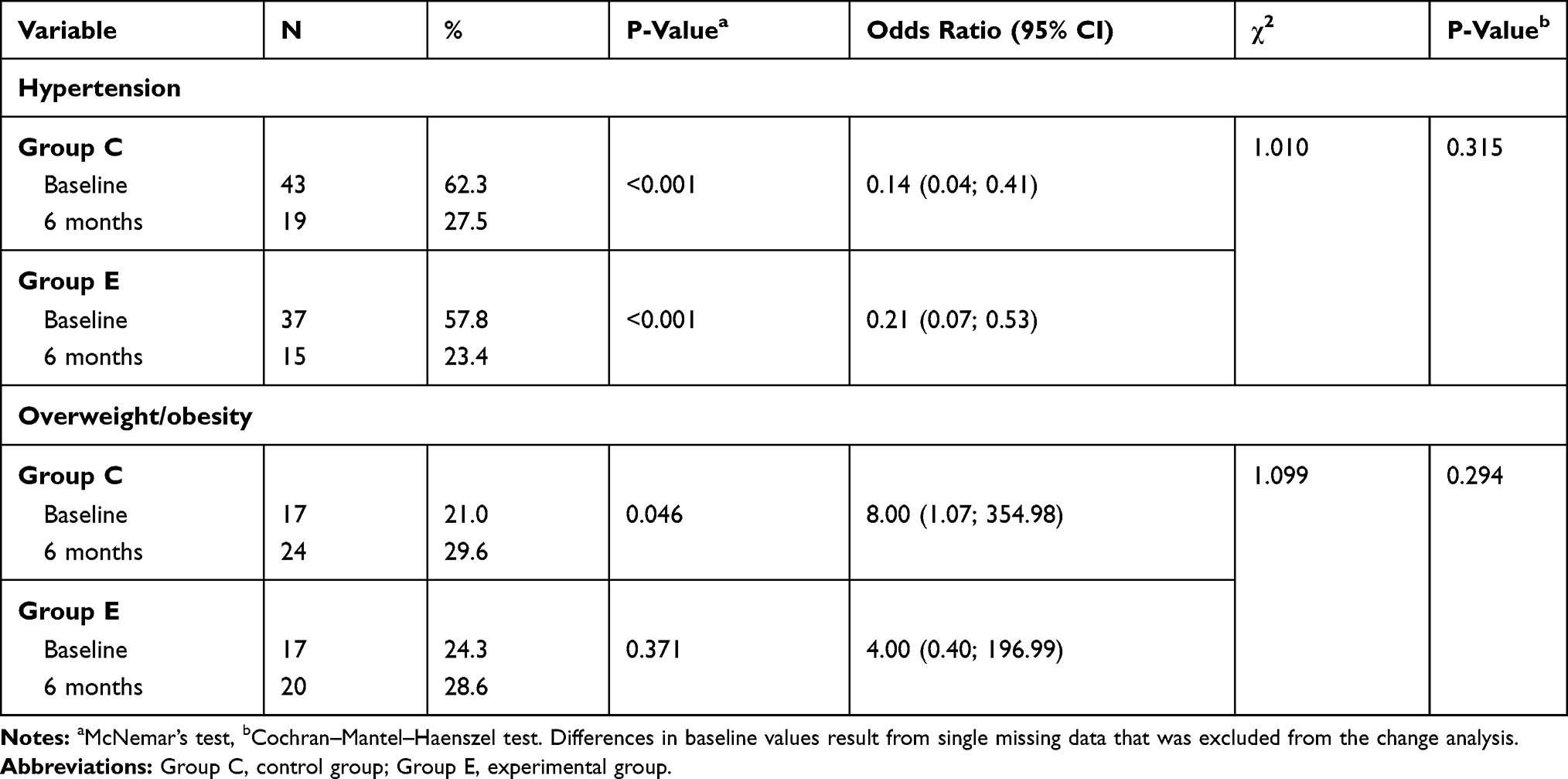 |
Table 7 Changes Regarding the Occurrence of Hypertension and Overweight/Obesity After 6 Months |
It needs to be emphasized that despite a significant disproportion in the structure of sex in both groups, additional multivariate analysis of variance (MANOVA) showed no correlation between the sex and the group which would significantly influence the differences described above.
Changes Regarding Knowledge About Nutrition and the Quality of Diet
Both groups were characterized by a significant improvement of the total NKS score and the sections: “Healthful eating” and “Carbohydrate counting”. Furthermore, a significant improvement of results in the “Nutrition label reading” section was observed in group E. However, the described changes did not significantly differ between groups.
A significant difference between groups was only noted in the scoring for the “Blood glucose response to food” section. In both groups, a significant improvement was obtained as regards the obtained number of points with better results noted in group E.
The analysis of results concerning the quality of the diet showed no significant changes except a marked reduction in the index of healthy diet in group C. However, the intergroup difference was not statistically significant in this matter (Table 8).
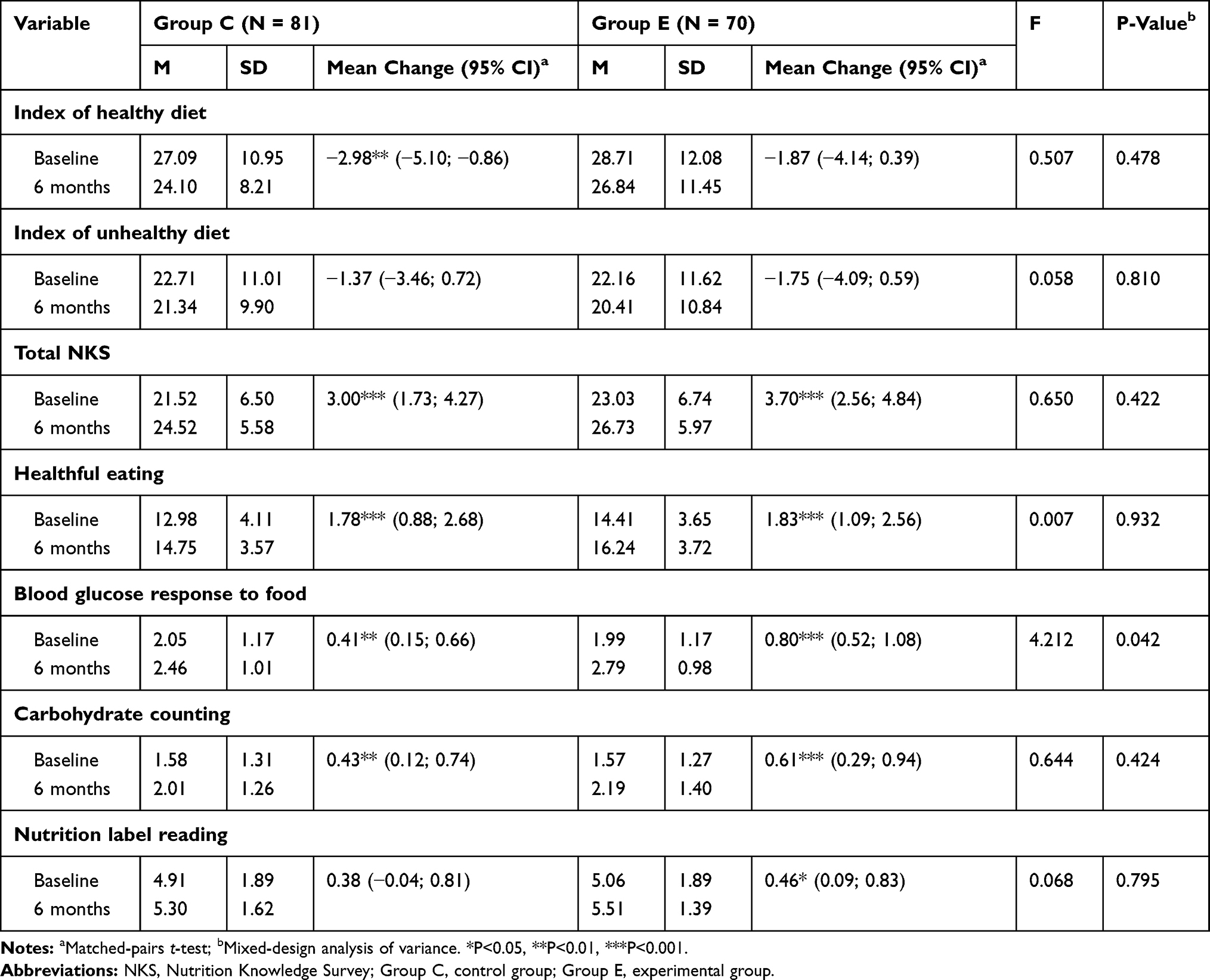 |
Table 8 Changes in the Scores Concerning Knowledge About Nutrition and Indices of the Quality of Diet After 6 Months |
Discussion
The authors of the present study attempted to verify the effectiveness of two different methods of nutrition education and compare their influence on selected clinical parameters, knowledge about nutrition and the quality of the diet in patients with type 1 diabetes. To the best of our knowledge, it is the first study aiming to compare the effectiveness of various educational interventions in a group of children and adolescents suffering from type 1 diabetes and treated with the use of insulin pumps. Study participants were randomly assigned to two groups: the control group (C) in which informative education methods (a lecture) were used and the experimental group (E) in which interactive methods (quiz and multimedia application) were additionally applied. It needs to be emphasized that both groups were characterized by poor diabetes control, as baseline mean HbA1c concentrations exceeded 7.0% both in groups C and E.9
The analysis of changes concerning clinical parameters after 3 months since the intervention revealed a significant improvement regarding HbA1c concentration in group E. After 6 months, the change of HbA1c was no longer significant. However, an improvement compared to baseline values was still observed. The reason for the regress of the positive effect may be associated with the increasing trouble with daily self-control concerning insulin administration, glycemia monitoring and carbohydrate consumption. Notably, the average duration of the disease did not exceed 5 years in study participants. No improvement was noted as regards the concentration of HbA1c in the control group during any stage of the study. However, it is worth noting that prior to initiating the education, group E had been characterized by significantly higher HbA1c concentrations than group C, which might contribute to easier control of the disease. Conversely, it may have caused more problems with establishing cooperation with the patient.
Different results were reported by Bowen et al who conducted a study in 150 adults suffering from type 2 diabetes and compared the effectiveness of two methods of nutrition education against the control group of generally healthy individuals. A significant reduction in HbA1c was observed in all groups of patients 3 months after the intervention. However, after 6 months, the positive effect did not continue only in the case of the control group.19 As a comparison, in Kids in Control of Food (KICk–OFF) study conducted in a group of 396 children and adolescents with type 1 diabetes, the researchers assessed the effectiveness of a 5-day educational course compared to a customary training. Interestingly, no significant changes regarding HbA1c were noted in study participants after 6, 12 and 24 months following the intervention.20
A significant increase in the mean SDS-BMI was observed in both groups after 3 months. Moreover, this unfavorable change also sustained after 6 months. Intergroup differences were not statistically significant. Notably, a significant increase in the average insulin dose (U/kg BW/d) was noted after 6 months in both groups. However, only in group E, this change was statistically significant. The occurrence of overweight and obesity has substantially increased over the past 30 years in children, also in those suffering from type 1 diabetes. Seemingly, the age, being a female, disease duration and the onset of the disease after puberty constitute independent risk factors of body weight increase in this group of patients.21 It was corroborated by the results obtained by Marigliano et al who conducted a study in a group of 25 children and adolescents with type 1 diabetes treated with the use of insulin pumps in whom a special method of nutrition education was implemented. After 18 months, despite a significant improvement in HbA1c concentrations, a significant increase in mean body weight, height and z-score BMI was observed.22 It is also worth noting that a strong correlation was present between introducing insulin treatment and an increase in body weight in individuals suffering from type 1 diabetes.23
After 3 months, in spite of increased SDS-BMI, a significant reduction in the mean SDS-SBP and SDS-DBP was reported in both groups. A positive effect was also present after 6 months. Moreover, the development of hypertension was significantly less common in both groups after 3 and 6 months. However, differences in the improvement of those intergroup parameters were not statistically significant. Seemingly, such a situation may be due to more extensive knowledge about nutrition, especially as regards the rules of proper nutrition comprising the limitation of the consumption of table salt and highly processed products. Nevertheless, despite the lack of statistical significance, a reduction in the index of unhealthy diet, which reflected the consumption of such products as salty snacks, fast-foods and meat products, was noted in both groups after 6 months.
Slightly different results were reported by Velázquez–López et al who conducted a study in 351 adults suffering from type 2 diabetes. They compared the effectiveness of traditional nutrition therapy and a special educational program which implemented multimedia tools (interventional group). Seven months later, a significant improvement was observed for mean DBP, while SBP-related changes were not statistically significant in both groups. Interestingly, after 21 months, the researchers still observed a positive effect concerning DBP values. Additionally, they reported a marked reduction in mean SBP only in the interventional group.24
The analysis of changes concerning nutritional knowledge after 6 months following the intervention showed a significant improvement in both groups regarding the following scores: total NKS, “Healthful eating” section, “Blood glucose response to food” and “Carbohydrate counting” sections. Intergroup differences regarding the obtained results were statistically significant only in the “Blood glucose response to food” section. Additionally, an improvement was noted in group E as regards “Nutrition label reading” which seems to be particularly important in the context of appropriate CE calculations. It is worth emphasizing that a marked reduction in the consumed CE value (CE/kg BW/d) was also observed in group E after 6 months. However, expanding the knowledge about nutrition did not contribute to improving the quality of the diet in both groups. Moreover, a significant decrease in the index of healthy diet was reported in group C. As a comparison, Breen et al conducted a study in a group of 118 adults diagnosed with type 2 diabetes. They observed that patients with more extensive knowledge about nutrition were characterized by a significantly higher consumption of fruit and vegetables and a lower glycemic index of the diet. However, simultaneously, the same group of subjects consumed significantly higher amounts of simple carbohydrates (also those which were not found in milk).25 It confirms our observations that the level of knowledge about nutrition does not always translate into the quality of diet.
The present results are not free from limitations. Primarily, the randomization method used in the study did not allow for proper selection of the control group. As a result, significant differences in the baseline characteristics between the groups may have a potential impact on the results obtained and the reliability of inference. Second, a relatively large number of patients “lost to follow-up” also constitutes a certain limitation in the interpretation of our results. It is worth emphasizing that longitudinal studies conducted among children are very demanding and it is extremely difficult to avoid “lost to follow-up”. It should also be noted that the loss of 20% of participants, with an equal loss of both groups, should not have a significant impact on the reliability of inference. In addition, we used the present authors’ tools (questionnaires, “true-false” quiz) and methods of nutrition education which were adjusted to the needs of a specific group of patients. Therefore, the results should not be generalized in patients at a different age or treated with a different method. Furthermore, the duration of the study, which was limited to 6 months, might be too short to assess long-term changes resulting from the intervention. Finally, we may not exclude the influence of additional factors, such as parents' education, duration of the disease, intelligence quotient, the level of motivation or individual predisposition for learning in the patients.
Conclusions
To conclude, the obtained results indicate a comparable effect of informative and interactive methods of nutrition education on the occurrence of overweight and obesity, hypertension and the level of knowledge about nutrition and the quality of diet in patients with poorly controlled diabetes. However, based on the obtained results, it may also be stated that informative methods were considerably less effective as regards the improvement in HbA1c concentrations. Therefore, it seems that the implementation of interactive nutrition education is more beneficial provided that the frequency of training is intensified in order to sustain long-term effects.
As a recommendation to improve the efficiency of nutritional education of children and adolescents with type 1 diabetes, it should be emphasized that training must be regularly repeated so that education is a continuous process. In addition, education methods should be individually tailored to the patient’s needs. Factors such as age, motivation, existing knowledge and cognitive skills should also be considered.
Data Sharing Statement
The data that support the findings of this study are openly available in “Zenodo” at http://doi.org/10.5281/zenodo.3519773.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82. doi:10.1016/S0140-6736(13)60591-7
2. Smythe K, Saw M, Mak M, Wong VW. Carbohydrate knowledge, lifestyle and insulin: an observational study of their association with glycaemic control in adults with type 1 diabetes. J Hum Nutr Diet. 2018;31(5):597–602. doi:10.1111/jhn.2018.31.issue-5
3. Lawton J, Rankin D. How do structured education programmes work? An ethnographic investigation of the dose adjustment for normal eating (DAFNE) programme for type 1 diabetes patients in the UK. Soc Sci Med. 2010;71(3):486–493. doi:10.1016/j.socscimed.2010.04.030
4. Phelan H, Lange K, Cengiz E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: diabetes education in children and adolescents. Pediatr Diabetes. 2018;19(Suppl 27):75–83. doi:10.1111/pedi.2018.19.issue-S27
5. Smart CE, Annan F, Higgins LA, Jelleryd E, Lopez M, Acerini CL. ISPAD Clinical Practice Consensus Guidelines 2018: nutritional management in children and adolescents with diabetes. Pediatr Diabetes. 2018;19(Suppl 27):136–154. doi:10.1111/pedi.2018.19.issue-S27
6. Blanson Henkemans OA, Bierman BP, Janssen J, et al. Using a robot to personalise health education for children with diabetes type 1: a pilot study. Patient Educ Couns. 2013;92(2):174–181. doi:10.1016/j.pec.2013.04.012
7. Chaney D. Structured diabetes education for children and adolescents. Nurs Stand. 2012;27(6):41–47. doi:10.7748/ns.27.6.41.s55
8. Calle-Bustos AM, Juan MC, García-García I, Abad F. An augmented reality game to support therapeutic education for children with diabetes. PLoS One. 2017;12(9):e0184645. doi:10.1371/journal.pone.0184645
9. DiMeglio LA, Acerini CL, Codner E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes. Pediatr Diabetes. 2018;19(Suppl 27):105–114. doi:10.1111/pedi.2018.19.issue-S27
10. Kułaga Z, Różdżyńska-Świątkowska A, Grajda A, et al. Siatki centylowe dla oceny wzrastania i stanu odżywienia polskich dzieci i młodzieży od urodzenia do 18 roku życia [Percentile charts for growth and nutritional status assessment in Polish children and adolescents from birth to 18 year of age]. Standardy Medyczne/Pediatria. 2015;12:119–135.
11. Kułaga Z, Litwin M, Grajda A, et al. Rozkłady wartości ciśnienia krwi w populacji referencyjnej dzieci i młodzieży w wieku szkolnym [Distribution of blood pressure in school-aged children and adolescents reference population]. Standardy Medyczne/Pediatria. 2010;7:100–111.
12. Donaghue KC, Marcovecchio ML, Wadwa RP, et al. ISPAD Clinical Practice Consensus Guidelines 2018: microvascular and macrovascular complications in children and adolescents. Pediatr Diabetes. 2018;19(Suppl 27):262–274. doi:10.1111/pedi.2018.19.issue-S27
13. Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 2005;56(5):303–307. doi:10.1080/09637480500195066
14. Jeżewska‐Zychowicz M, Gawęcki J, Wądołowska L, et al. Kwestionariusz do badania poglądów i zwyczajów żywieniowych dla osób w wieku od 16 do 65 lat, wersja 1.2 –kwestionariusz do samodzielnego wypełnienia przez Respondenta [Questionnaire for the study of views and dietary habits for people in age from 16 to 65 years, version 1.2 - questionnaire for unassisted completion by the Respondent]. In: Gawęcki J, editor. Kwestionariusz Do Badania Poglądów i Zwyczajów Żywieniowych oraz Procedura Opracowania Danych. Warszawa: Wydawnictwo Komitetu Nauki o Żywieniu Człowieka Polskiej Akademii Nauk; 2014:
15. Dłużniak-Gołaska K, Panczyk M, Szostak-Węgierek D, Szypowska A, Sińska B. Analysis of the diet quality and dietary habits of children and adolescents with type 1 diabetes. Diabetes Metab Syndr Obes. 2019;12:167–170. doi:10.2147/DMSO.S186237
16. Rovner AJ, Nansel TR, Mehta SN, Higgins LA, Haynie DL, Laffel LM. Development and validation of the type 1 diabetes nutrition knowledge survey. Diabetes Care. 2012;35(8):1643–1647. doi:10.2337/dc11-2371
17. Application: VitaScale Kalkulator kalorii i wymienników [homepage on the Internet]. Available from: https://vitascale.pl/.
18. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
19. Bowen ME, Cavanaugh KL, Wolff K, et al. The diabetes nutrition education study randomized controlled trial: a comparative effectiveness study of approaches to nutrition in diabetes self-management education. Patient Educ Couns. 2016;99(8):1368–1376. doi:10.1016/j.pec.2016.03.017
20. Price KJ, Knowles JA, Fox M, et al. Effectiveness of the Kids in Control of Food (KICk–OFF) structured education course for 11–16 year olds with Type 1 diabetes. Diabet Med. 2016;33(2):192–203. doi:10.1111/dme.12881
21. De Keukelaere M, Fieuws S, Reynaert N, et al. Evolution of body mass index in children with type 1 diabetes mellitus. Eur J Pediatr. 2018;177(11):1661–1666. doi:10.1007/s00431-018-3224-9
22. Marigliano M, Morandi A, Maschio M, et al. Nutritional education and carbohydrate counting in children with type 1 diabetes treated with continuous subcutaneous insulin infusion: the effects on dietary habits, body composition and glycometabolic control. Acta Diabetol. 2013;50(6):959–964. doi:10.1007/s00592-013-0491-9
23. Łuczyński W, Szypowska A, Głowińska-Olszewska B, Bossowski A. Overweight, obesity and features of metabolic syndrome in children with diabetes treated with insulin pump therapy. Eur J Pediatr. 2011;170(7):891–898. doi:10.1007/s00431-010-1372-7
24. Velázquez–López L, Muñoz-Torres AV, Medina-Bravo P, Vilchis-Gil J, Klünder-Klünder M. Escobedo–de la Peña J. Multimedia education program and nutrition therapy improves HbA1c, weight, and lipid profile of patients with type 2 diabetes: a randomized clinical trial. Endocrine. 2017;58(2):236–245. doi:10.1007/s12020-017-1416-0
25. Breen C, Ryan M, Gibney MJ, O’Shea D. Diabetes-related nutrition knowledge and dietary intake among adults with type 2 diabetes. Br J Nutr. 2015;114(3):439–447. doi:10.1017/S0007114515002068
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.