")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Inter-Rater Reliability of a Pressure Injury Risk Assessment Scale for Home Care: A Multicenter Cross-Sectional Study
Authors Kohta M , Ohura T, Tsukada K, Nakamura Y, Sukegawa M, Kumagai E, Kameda Y, Kitte T
Received 9 November 2020
Accepted for publication 10 December 2020
Published 22 December 2020 Volume 2020:13 Pages 2031—2041
DOI https://doi.org/10.2147/JMDH.S291162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Masushi Kohta,1 Takehiko Ohura,2 Kunio Tsukada,3 Yoshinori Nakamura,4 Mishiho Sukegawa,5 Eiko Kumagai,6 Yuki Kameda,7 Toshihiro Kitte8
1Medical Engineering Laboratory, ALCARE Co. Ltd., Tokyo, Japan; 2Pressure Ulcers and Wound Healing Research Center, Sapporo, Japan; 3Takaoka Ekinan Clinic, Takaoka, Japan; 4Department of Medical Home Healthcare Center, Tenri Hospital Shirakawa Branch, Tenri, Japan; 5Miyama-Takinoi Comprehensive Community Support Center, Funabashi, Japan; 6Murata Day Surgery & WOC Clinic, Sendai, Japan; 7Wound Care Marketing Division, ALCARE Co Ltd., Tokyo, Japan; 8Department of Health Care Policy, Shiga Government Office, Otsu, Shiga, Japan
Correspondence: Masushi Kohta
Medical Engineering Laboratory, ALCARE Co., Ltd., Tokyo, Japan
Email [email protected]
Purpose: The aim of the current study was to assess the inter-rater reliability and agreement of the Pressure Injury Primary Risk Assessment Scale for Home Care (PPRA-Home), a risk assessment scale recently developed for Japan-specific social welfare professionals called care managers, to predict pressure injury risk in geriatric individuals who require long-term home care needs.
Methods: A multicenter cross-sectional study was conducted at 30 home-based geriatric support services facilities located at four local districts in Japan. Eligible participants were individuals who needed partial or full assistance for daily living under Japan’s long-term care insurance system (care levels 1– 5). The degree of agreement and kappa coefficient were calculated for each item and the total score, after which inter-rater reliability was determined. The effect of the participant’s care level on reliability was also evaluated as secondary analysis.
Results: A total of 96 participants were assessed by 83 care managers (two assessors scored each participant). The degree of agreement and calculated kappa coefficient of the PPRA-Home total score were 59% and 0.72, respectively, with the inter-rater reliability for the total score determined to be “Substantial”. Our subgroup analysis showed that the inter-rater reliability differed according to the participant’s care level. Accordingly, the kappa coefficient for the total score was lower in subgroup “care level 1– 3” than in subgroup “care level 4– 5” (0.51 and 0.76, respectively).
Conclusion: Our result showed that the PPRA-Home has substantial inter-rater reliability for evaluation of risks of pressure injury development at home care. However, some research focusing on intra-later reliability and validity of the PPRA-Home with adequate sample sizes are required to provide categorical conclusions on whether it can be used for the risk assessment scale in actual clinical settings.
Keywords: pressure ulcer, risk assessment, reproducibility, agreement, geriatrics
Introduction
The focus of healthcare, including nursing care and specialized medical services, is expected to shift from hospital-based to home- and community-based care as more individuals are expected to avail of home healthcare services in the aging society.1–3 In Japan, the number of individuals requiring long-term care benefits at home under Japan’s long-term care insurance (LTCI) system established by Japanese government has continued to increase annually, reaching 6 million in 2016.4 Considering that most individuals have single or multiple diseases that are associated with pressure injury development, risk of pressure injury development during home care appears to be increasing.5 Several studies have reported a 3.6–10% prevalence of pressure injury among the Japanese population.6–8 Moreover, elderly individuals at home or within communities suffered from more serious pressure injury problems than those admitted to acute care hospitals.
Prevention of pressure injuries is always better than its treatment. As such, preventive measures are need to be developed for the successful management of pressure injuries during home care. The use of risk assessment tools after classifying single or multiple risk factors of development of immobility-related injuries can be vital first step for evaluating individuals in pressure injury prevention.9 The Braden scale has been the most widely used risk assessment scale for predicting the risk of hospital- or facility-acquired pressure injuries.10 Several reports have shown that the Braden scale had moderate to high levels of reliability and validity.11,12 Thus, acute care and university hospitals have recommended the use of pressure redistribution mattresses based on risk assessment using Braden Scale.13 The Ohura-Hotta (OH) scale, which consists of four subscales (ie, spontaneous body turning, sacral bony prominence, edema, and articular contracture) has also been widely accepted as a risk assessment scale for predicting pressure injury risk among elderly individuals specifically within Japan.14 One study showed that the clinical application of a support surface selection algorithm based on the OH scale resulted in reduced incidence rates of pressure injuries within a Japanese general hospital.15
Despite the benefits offered by the Braden and OH scales, they have seen limited use in current home care settings wherein Japanese social welfare professionals work. Our previous questionnaire survey targeting care managers, one type of professional occupation under the social welfare services of the LTCI system, revealed that less than half of the participants found it difficult to use the Braden or OH scales in daily actual clinical practice.16 Reports have shown that the Braden scale did not have a strong enough impact for use in long-term care facilities.17,18 The Japanese government had originally introduced a medical-social welfare networking model into the LTCI system with care managers as gatekeepers.19,20 Accordingly, they are entirely responsible for providing home care management services, including assessing the physical conditions and living circumstances of individuals, planning all care, and assisting with procedures necessary to avail such services. In addition, the care service plan should be adjusted based on changes to each individual’s condition. To obtain a care manager license, 5 years or more of experience in geriatric care as a medical and/or social welfare professional is necessary, as well as passing a national examination. Care managers visit the house of each individual to interview them and/or their cohabitants at least once a month. Thus, risk assessment by care managers is imperative for a comprehensive understanding on the necessary support needed by individuals receiving long-term care under the LTCI system.
Recently, a risk assessment scale, called “Pressure Injury Primary Risk Assessment Scale for Home Care (PPRA-Home)”, has been developed for use by care managers under the LTCI system of Japan.21 Moreover, the application of the PPRA-Home could be one solution for achieving successful individual-centered multidisciplinary collaboration between medical professionals and social welfare professionals with care managers acting as a bridge. Notably, although one study has been conducted on the reliability and validity of the PPRA-Home in a Japanese geriatric health services facility, more research regarding its reliability is needed before being introduced into practical use.21
The current study therefore sought to evaluate inter-rater reliability of the PPRA-Home among care managers in facilities located across several local areas wherein the use of medical and nursing care resources tends to be limited.
Materials and Methods
Study Design
This multicenter cross-sectional study was conducted at 30 different home-based geriatric support services facilities in Takaoka city (Toyama prefecture), Funabashi city (Chiba prefecture), Nara city (Nara prefecture), and Sendai city (Miyagi prefecture), Japan from November 2019 to June 2020.
Samples and Setting
Eligible participants were individuals classified as requiring care levels 1–5 in the four aforementioned districts. Two types of Japanese public insurance programs allow elderly individuals access to medical and nursing care: 1) the medical insurance program and 2) the LTCI system. The former is available for all people (regardless of age) upon needing appropriate treatment or examination at a hospital, while the latter is available for individuals aged 40–64 years with specific diseases or those aged 65 years or over. Individuals that use the LTCI are categorized into seven care needs levels: support levels 1 and 2 and care levels 1 to 5.22 The definition of each care level is presented in the Data Collection section of this paper.
Individuals with existing pressure injuries at the start of the study were excluded. The present study needed 66 participants to obtain a power of 0.08, an alpha of 0.05, and a desired reliability coefficient of 0.8, as demonstrated in a previous research.21 After accounting for attrition, the target number of 75 participants was required.
Instruments
Since its creation in 2019, the PPRA-Home has yet to be translated into other languages from its original language of Japanese.21 Briefly, the concepts underlying the designing of PPRA-Home included: 1) identifying risk factors for pressure injury development among Japanese elderly individuals; 2) simple question and answer; and 3) utilizing descriptions that Japanese care managers can easily understand. The developer extracted risk factors in a home-based pressure injury development by reviewing the existing risk factors from well-established pressure injury risk assessment scales such as Braden and OH scales. Next, the words of the extracted risk factors were rephrased to become more understandable for Japanese care managers. Finally, the PPRA-Home was completed after receiving advice to be revised in regard with the words and their meaning of each item on the PPRA-Home by an associate professor specialized in home health care in a certain university. The scale includes the following eight items: spontaneous body turning, body type, mobility, decreased food intake, skin moisture, using diapers, edema, and using head-of-bed elevation. Responses to each item of the PPRA-Home can be indicated by two categories, “yes” or “no”, with a score of “1” being given when the answers were “yes” and “0” when “no”. Scores for each item were then summed up, resulting in a total score ranging from 0– 8. A total score of 8, the highest score possible, indicates the highest risk for developing pressure injuries. The definitions of each item on the PPRA-Home and their scoring rules are shown in Table 1. A fair agreement with Fleiss’s kappa statistics of 0.29 was obtained in a previous reliability study conducted by the developer.21 In the same literature, a cutoff score of 2 on the PPRA-Home had a sensitivity of 77% and specificity of 99% in a cutoff validity testing.
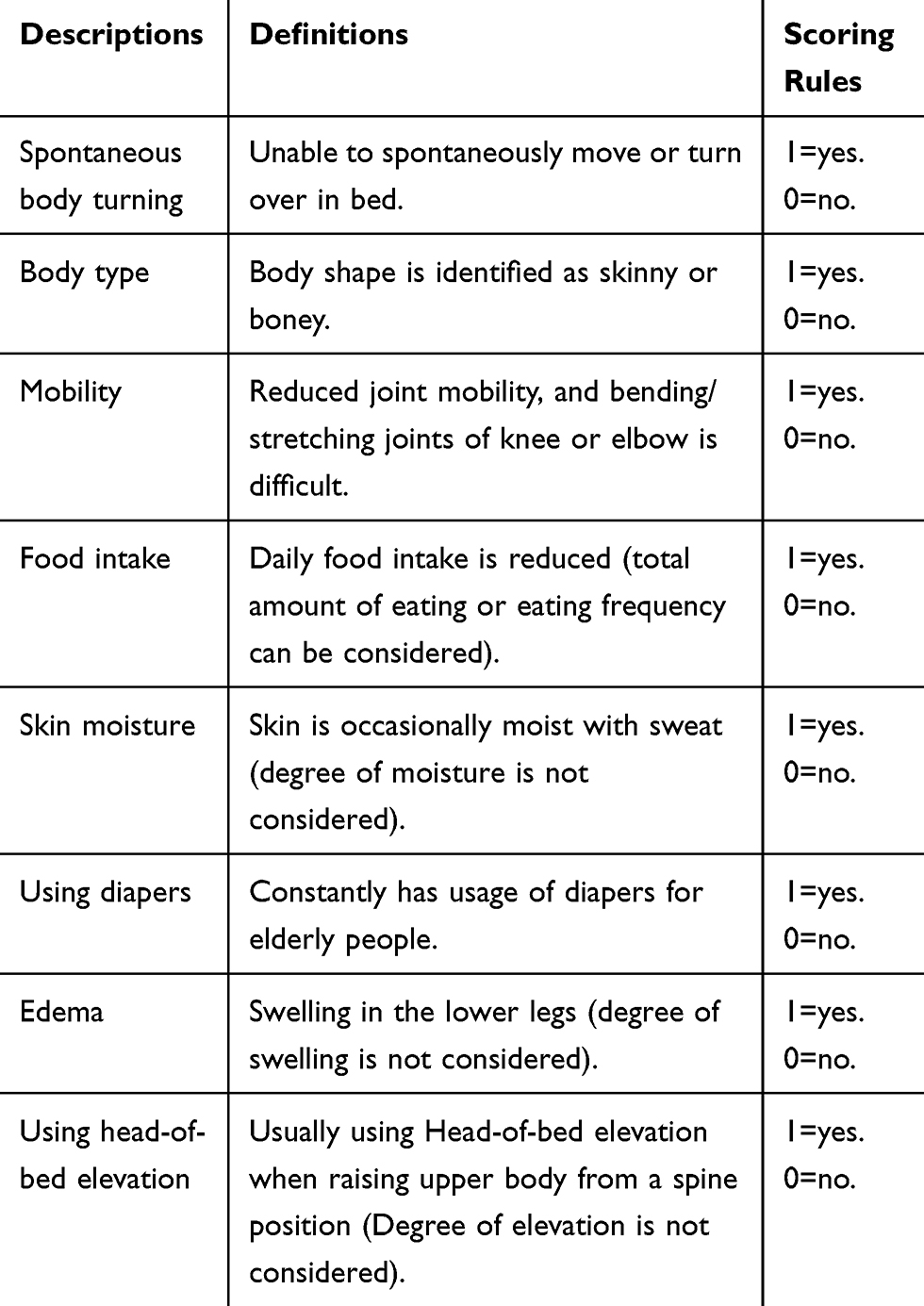 |
Table 1 Definition and Scoring Rule of Pressure Injury Primary Risk Assessment Scale for Home Care |
Study Procedure
All assessors had a care manager license and several years of experience in the field of home-based care. Moreover, they worked at the home-based geriatric support services facilities studied herein. The investigators orally explained the outline of this study to the candidates of the assessors who then received a written agreement for cooperation upon deciding to participate in this study.
Two assessors performed the data collection during regular visits to the participant’s home or day-care service center. A day-care service center where individuals could receive any care support services, such as meals and baths, without staying the night was also included during data collection. Among the two assessors for each participant, one supervised the participant in actual practice, while the other worked at the same facility where the first one worked. The PPRA-Home in this study was performed by a pair of assessors who visually assessed the physical condition of the participants. The assessors were also allowed to ask the participants, cohabitants, or their caregiver regarding anything related to the circumstances of the participant’s daily life. Two assessors visited the participants at their home or day-service center throughout the study period. However, both assessors performed observations independently, with no communication between them. Neither of the assessors received training regarding the PPRA-Home prior to start of this study considering the importance of clarifying the inter-rater reliability and agreement of the PPRA-Home under the care manager’s current level of knowledge and experience without any specific training. The assessment lasted for an average of 2 minutes per assessor.
Data Collection
All data were obtained from the study records and prepared using written data collection forms. The records were reviewed for the assessor’s demographic data (age, gender, and years of experience as a care manager) and professional background (previous role) and the participant’s demographic data (age, gender, living arrangement), care needs level, level of functional disability (bedridden level), and level of cognitive impairment (dementia rating). Each item and total score of the PPRA-Home were also recorded on the data collection forms. The forms were placed in an envelope and returned to the authors by assessor pairs.
Data on care level, bedridden level, and rating of dementia were obtained from official data of the Care Needs Level Certification Committee of the city’s administrative office. Individuals with care level 1 required any partial support for daily living, whereas those with care level 5 had difficulty living without excessive assistance by medical and/or social welfare professionals. The bedridden level was ranked from Rank J (independent but required partial support) to Rank C (completely bedridden). The rating of dementia was also ranked from Independent (very low cognitive disorder) to Rank M (severe cognitive disorder).
Statistical Analysis
Continuous variables are expressed as means and standard deviation, while categorical variables are expressed as frequencies and percentages.
Inter-rater reliability was addressed using both degree of agreement and kappa coefficient for assessor pairs considering that these were the most prevalent reliability measures in this context.21,23 Degree of agreement was defined as the number of agreed cases divided by the sum of the cases with agreements and disagreements. Unweighted kappa was performed to calculate the inter-rater reliability of each item, while kappa with quadratic weighting was employed to calculate sum scores. An unweighted and weighted kappa of <0.00 were identified as poor, 0.00–0.20 as slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect based on previous literature.21 Finally, kappa values above 0.70 were considered as adequate acceptance criteria in this inter-rater reliability study.11
Post-hoc subgroup analysis was also performed to explore possible differences in the inter-rater reliability of the PPRA-Home total score according to subgroups of participants.24 This analysis focused on care needs level, bedridden level, and rating of dementia given their importance for confirming the participant’s current physical/cognitive status.
All statistical analyses were conducted using the Statistical Package for the Social Sciences version 20.0 (IBM Corporation, Tokyo, Japan).
Results
Characteristics of Assessors and Participants
Data from a total of 83 assessors were collected in this study. The characteristics of the assessors are summarized in Table 2. Most of the assessors were 40–49 years old (41%) and female (82%). Approximately half of the assessors (50%) had a certificated care worker license, whereas only 6% had a nursing license (registered nurse and/or licensed practical nurse).
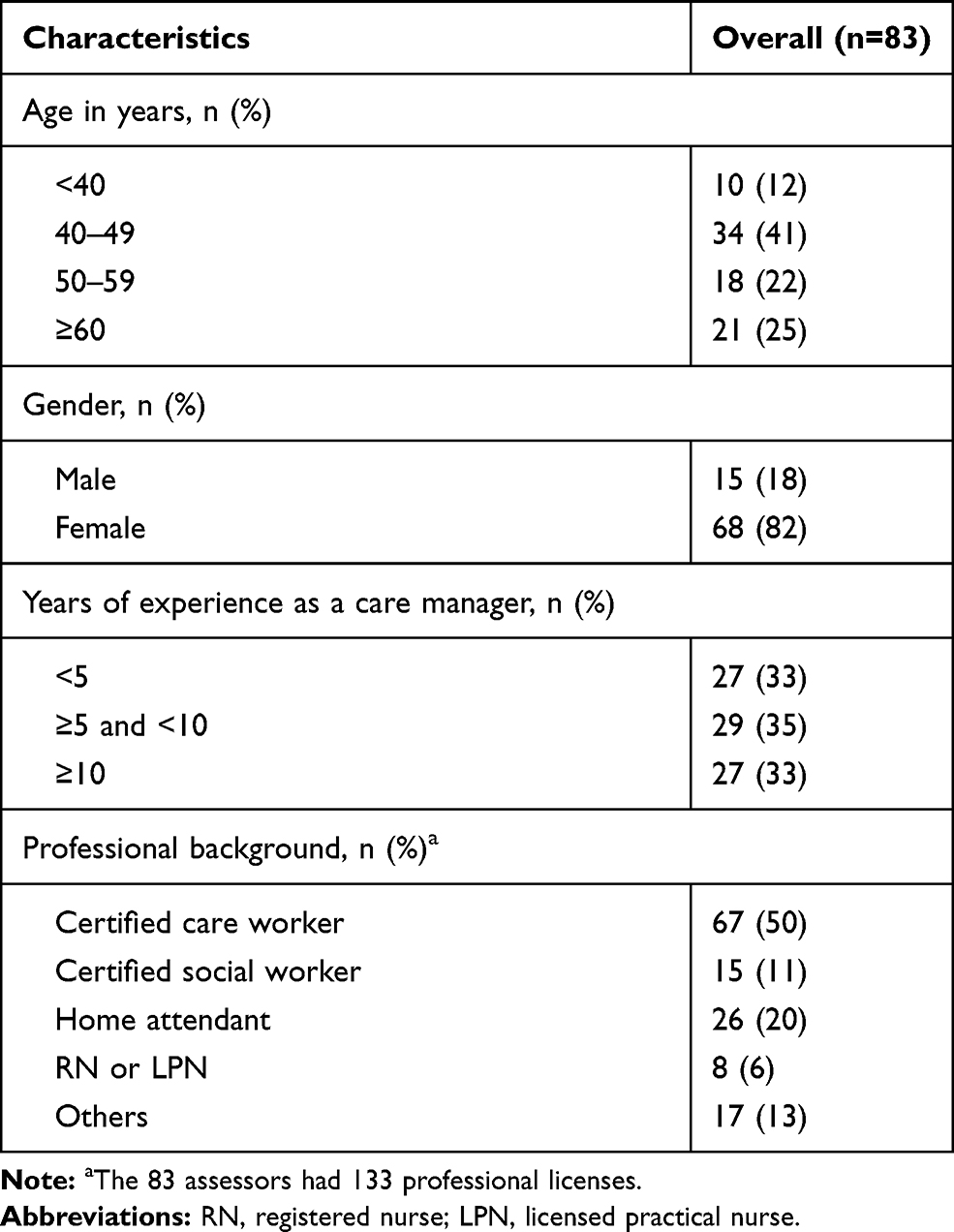 |
Table 2 Assessor Characteristics |
Data from a total of 96 participants with a mean age of 84 (9.7) located at Takaoka city (n=45), Funabashi city (n=30), Nara city (n=20), and Sendai city (n=1) were collected in this study (Table 3). Approximately 71% were female, and 80% were living in the same house as others (spouse and/or children). Care level was almost equally distributed (level 1, 20%; level 2, 22%; level 3, 19%; level 4, 25%; and level 5, 13%).
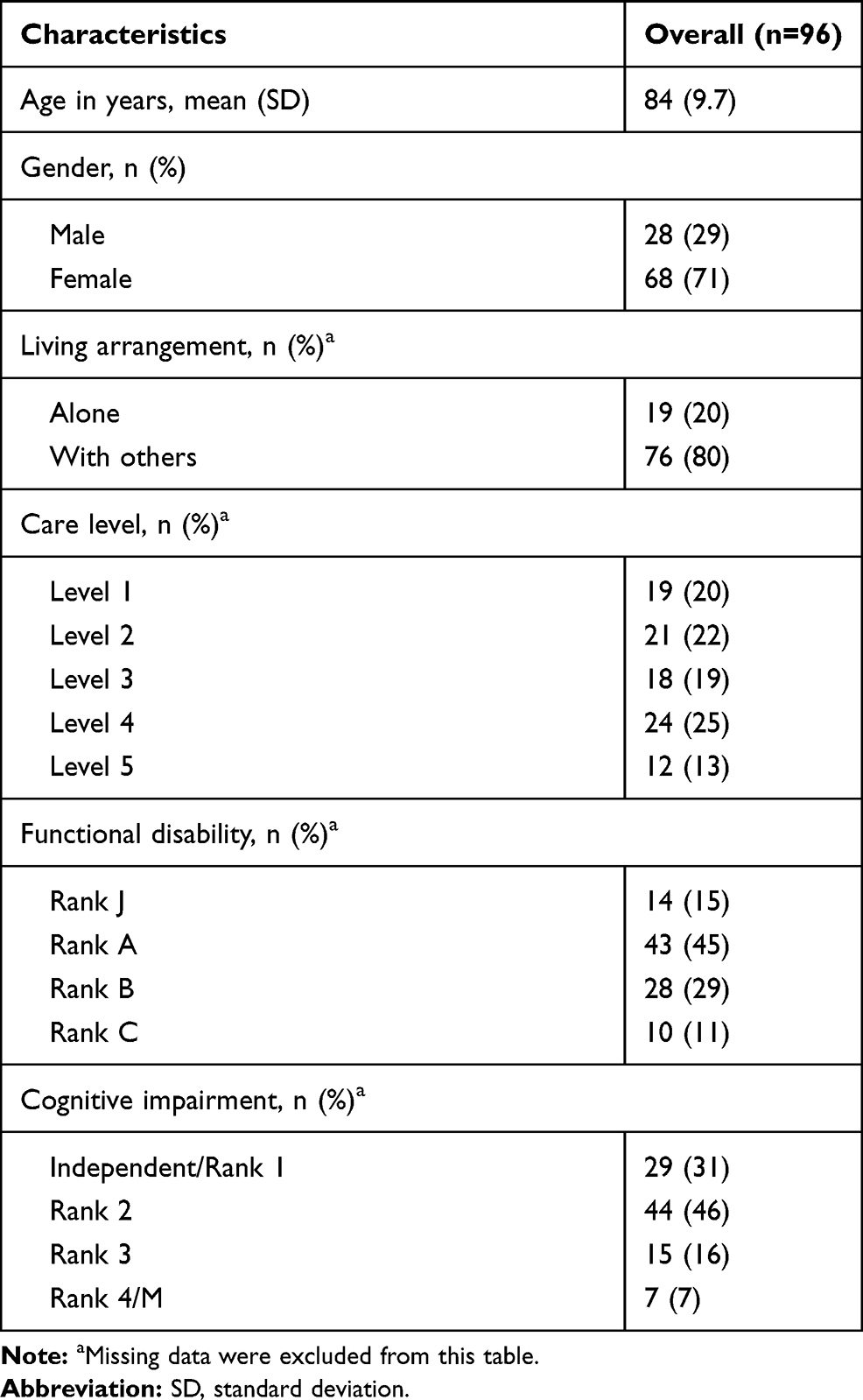 |
Table 3 Participant Characteristics |
Inter-Rater Reliability
The degree of agreement on each item and total score for the two assessors are presented in Table 4. The degree of agreement was considered good, ranging from 80–93% for each item and 59% for the total score. Kappa coefficients for each item and total score are also detailed in Table 3. The item “using head-of-bed elevation” yielded the highest kappa coefficient (unweighted kappa=0.82; 95% CI=0.69–0.95), whereas the item “skin moisture” yielded the lowest kappa coefficient (unweighted kappa=0.58; 95% CI=0.42–0.75). The calculated weighted kappa for total score was 0.72 (95% CI=0.44–0.98), while findings determined that the PPRA-Home score had “Substantial” inter-rater reliability.
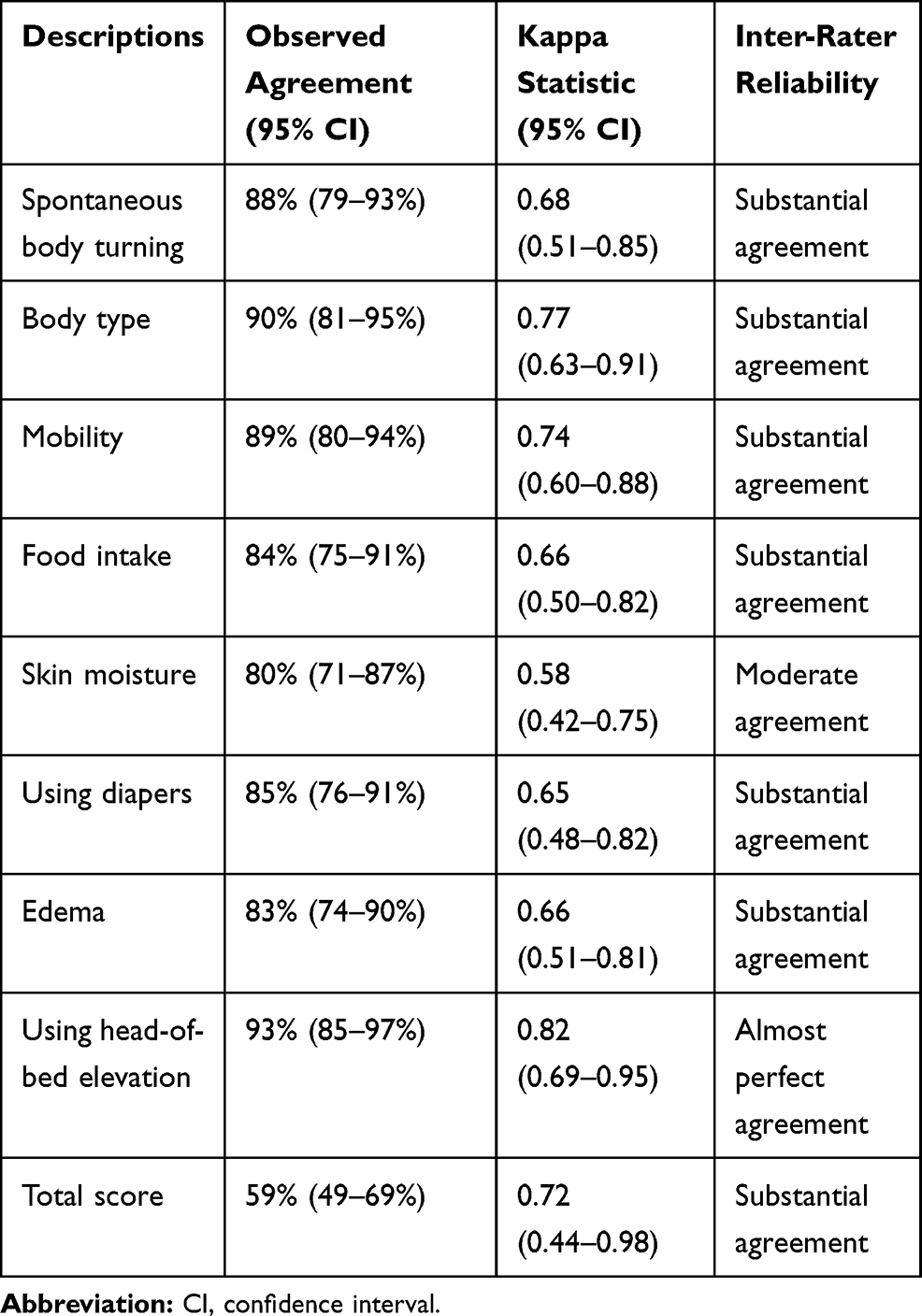 |
Table 4 Inter-Rater Reliability and Agreement of the Pressure Injury Primary Risk Assessment Scale for Home Care |
Subgroup Analysis
The degree of agreement, kappa statistics, and inter-rater reliability of each item and total score for each subgroup are outlined in Table 5. Notably, inter-rater reliability differed according to the participant’s physical characteristics. In particular, subgroup “care level 1–3” had a lower kappa statistic for the total score compared to subgroup “care level 4–5” (weighted kappa=0.51; 95% CI=0.03–0.98 and 0.76; 95% CI=0.38–1.00, respectively). Similar results are shown in the functional disability subgroup (bedridden level). In contrast, almost no difference was observed in the cognitive impairment subgroup (dementia rating).
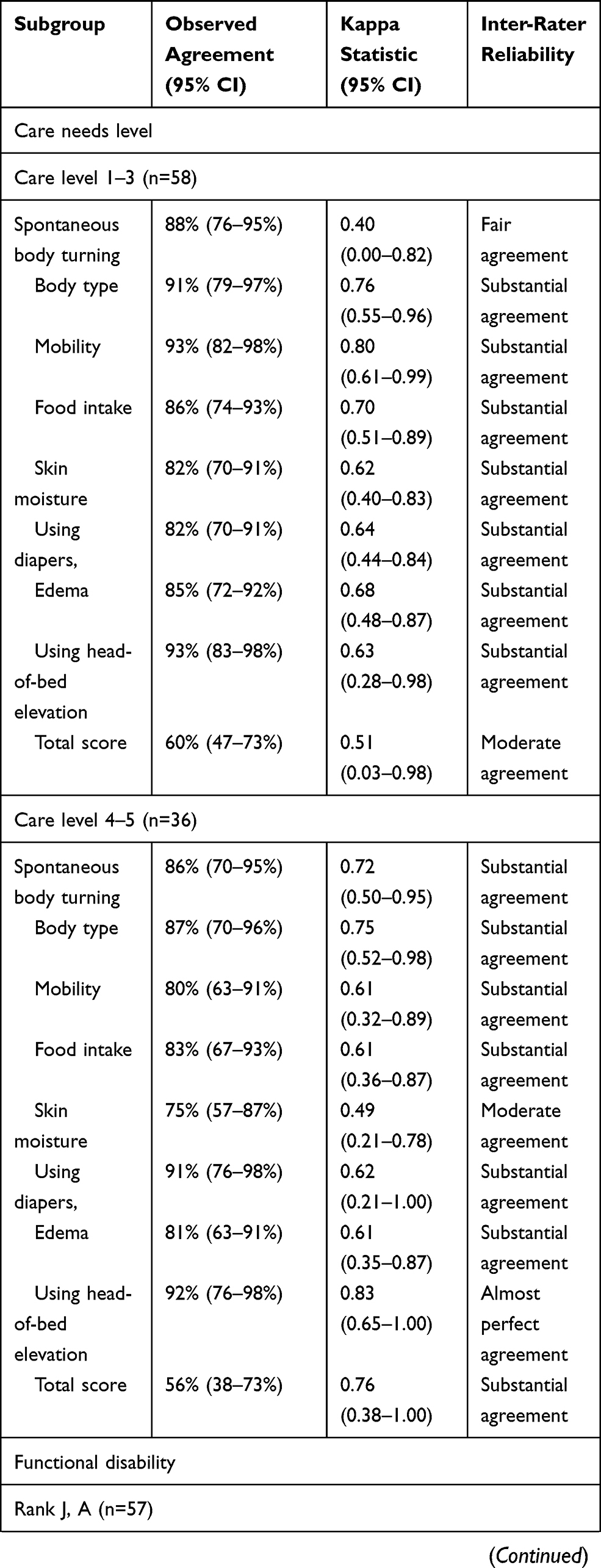 | 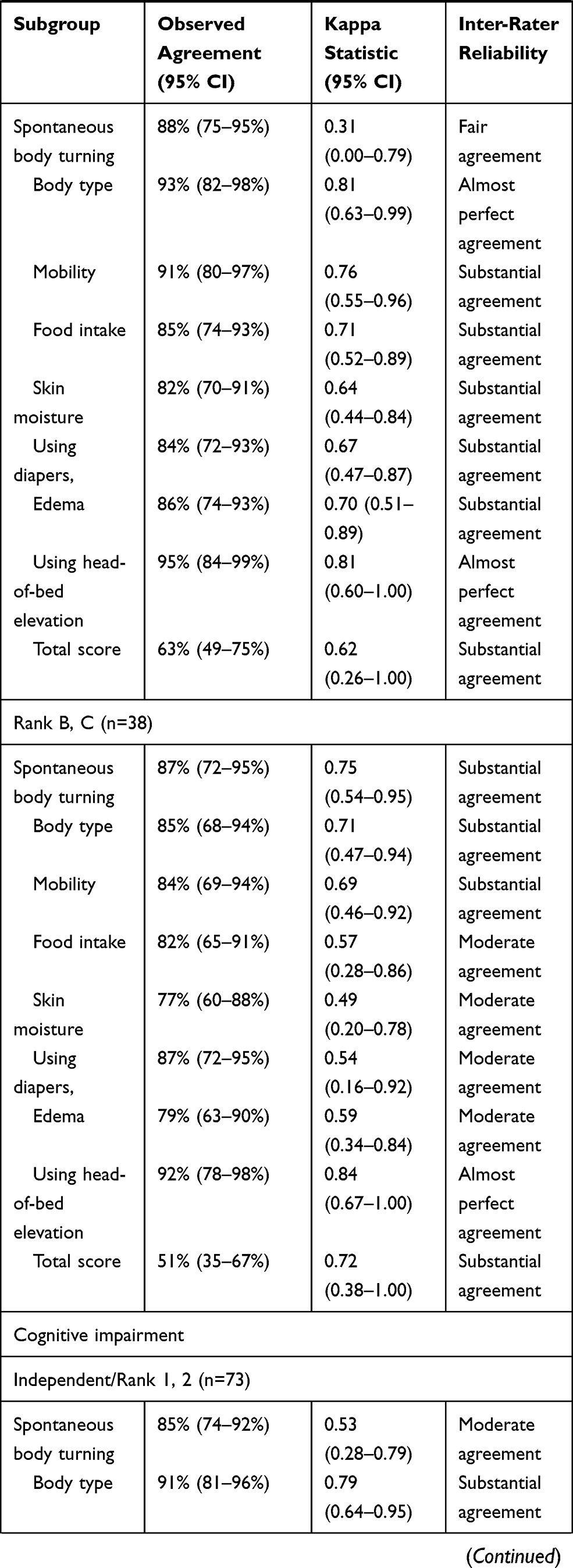 | 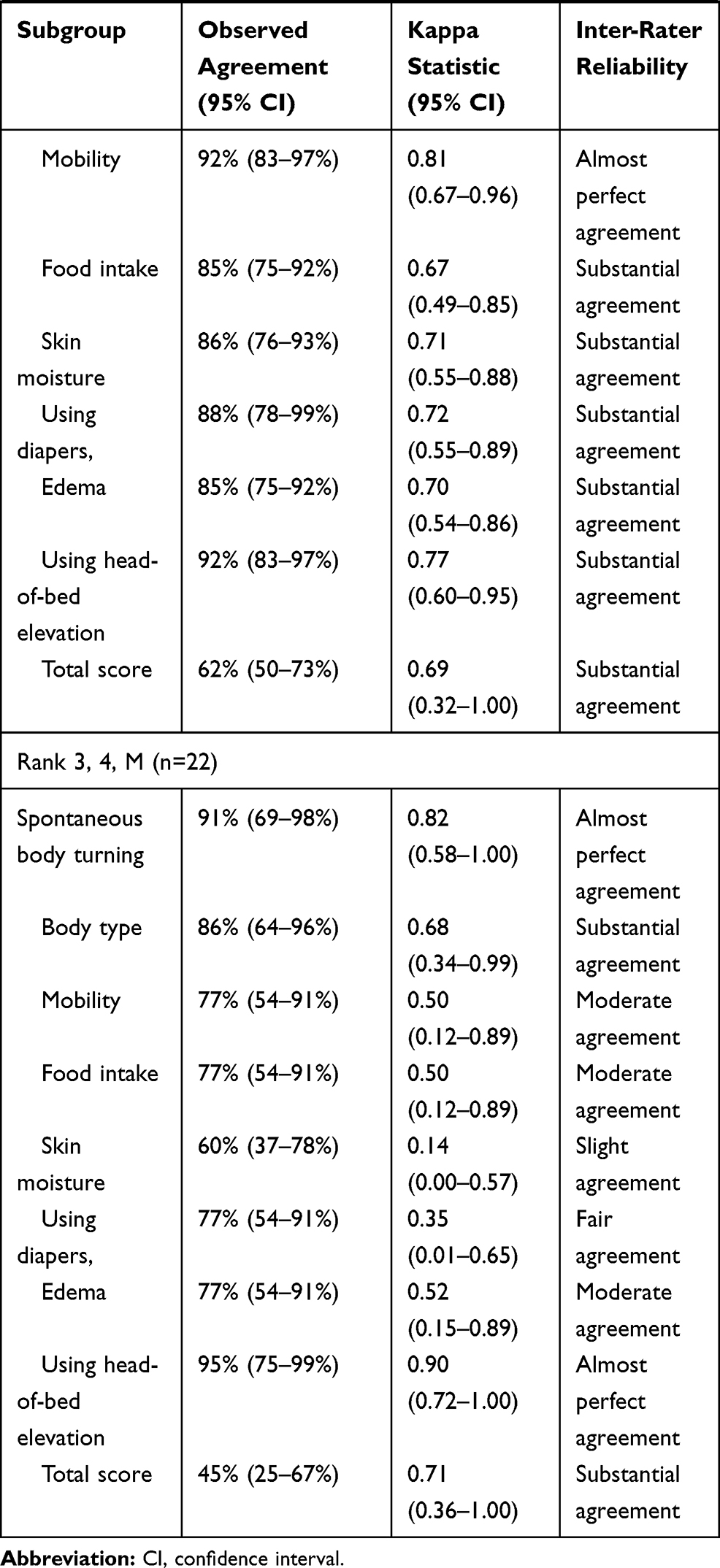 |
Table 5 Subgroup Analysis for Inter-Rater Reliability and Agreement of Each Item and Total Score of the Pressure Injury Primary Risk Assessment Scale for Home Care |
Discussion
Given the importance of reliability studies of risk assessment scales, several previous studies investigating the inter-rater reliability of well-established pressure injury risk assessment scales have helped establish clinical guidelines for the prevention and treatment of pressure injuries.25–27 Currently, the PPRA-Home is a unique risk assessment scale that targets Japanese care managers for pressure injury prevention. However, the inter-rater reliability of the PPRA-Home has not been adequately addressed in contemporary literature.21 Accordingly, our findings revealed the PPRA-Home had adequate reliability, suggesting that care managers should consider utilizing this scale when providing social welfare geriatric services in aging societies.
The current study had been based on a previous study by Kottner et al,28 which proposed a guideline for reporting reliability and agreement studies across a wide range of disciplines. Moreover, our multicenter approach can be even more advantageous given that it allowed for adequate sample size, which ensured that the current study achieved adequate participant enrolment and reached its target sample size. Furthermore, considering that 86 assessors were included herein, data obtained from this study should comprise important information for all specialists in the management of pressure injuries that would facilitate the use of the PPRA-Home.
The most important finding of the current study was that the PPRA-Home total score had substantial inter-rater reliability, with a weighted kappa of 0.72 (Table 4), indicating that the PPRA-Home meets the generally acceptable criteria for inter-rater reliability. A previous report showed that each item on Braden scale had a Cohen’s kappa ranging from 0.72–0.86,25 while another showed that the total Braden scale score measured by incentive care unit nurses had an intra-class correlation coefficient ranging from 0.72–0.84.26 A similar result was also reported by another study conducted in a home care setting.27 To the best of our knowledge, an official kappa value acceptance criterion with sufficient reliability has yet to be established in the field of medical research. Nonetheless, values above 0.70 have generally been considered adequate.29 Therefore, our findings indicate that the obtained kappa coefficient for the PPRA-Home total score is currently acceptable with sufficient reliability.
The inter-rater reliability for each item of the PPRA-Home ranged from moderate to almost perfect (Table 4). Moreover, items “body type (skinny or not)”, “mobility”, and “using head-of-bed elevation” complied with the acceptance criteria of this study (Kappa value>0.70), whereas the remaining items did not. The item “skin moisture” yielded the lowest kappa value (0.58; 95% CI=0.42–0.75), which may have been due to the different interpretations of the term among the assessors. The item was included in the PPRA-Home given that exposure to the excessive moisture from urine and/or sweat can increase the possibility for skin surface and superficial tissue damage due to external stimuli, such as friction.30 However, the PPRA-Home employs simple and concise words with no supplementary explanation for each item.21 Therefore, the assessors participating in this study were considered to have had varying interpretations of the term “skin moisture”.
Another possible reason for the low kappa (below 0.7) in some items was the lack of education regarding pressure injury prevention among care managers. Although all assessors included herein were licensed care managers, their background profession (previous occupation) varied considerably, ranging from nursing specialists to home attendants. The difference in their background may have had an effect on their knowledge and practice related to pressure injury prevention. All assessors need to understand not only the words themselves but also the background in which those words were employed in the risk assessment scale. The authors suggest that more education among care managers would increase inter-rater reliability and agreement among assessors.
PPRA-Home was originally developed for easy to use in home care without the need for specific training and/or education aimed at assessors (care managers) in the context of pressure injury prevention.21 Considering the effect of training and education is also important when investigating risk assessment scale for ulcer management. However, the authors did not consider the training and education for the assessors in this study, because it should be respected as a philosophy of the developer of PPRA-home. A problem of this study that the assessors did not receive any training was that their current level of knowledge in pressure injury prevention was not recognized. It would have been better if knowledge of the assessors was evaluated with some validated scales prior to the start of this study.
The inter-rater reliability and kappa values of PPRA-Home obtained herein were better that those reported in Morita et al,21 which were conducted in one Japanese geriatric health services facility (Kappa in total score=0.29). However, strictly comparing the kappa coefficients of both studies is difficult given the differences in statistical approach used for calculations. Notably, the current study utilized weighted kappa for the PPRA-Home total score, whereas the previous report employed unweighted Fleiss kappa.21
The present study hypothesized that the results of the PPRA-Home would be sufficient among all subgroups. However, participants in the “care level 4–5” subgroup had a higher kappa coefficient than those in the “care level 1–3” subgroup (Table 5). Although the reason for this is unclear, care managers may often check the physical condition to provide comprehensive care to individuals with higher care levels. Moreover, the possible influence of the assessors’ individual interests on kappa and agreement cannot be excluded and will require further study. As such, the competence of care managers with respect to preventing pressure injury may differ based on the care level of the individuals.
From a clinical point of view, the use of the PPRA-Home is a chance to promote a multidisciplinary approach for achieving pressure injury prevention. A previous study suggested that care managers rarely communicate with physicians and nurses regarding the physical condition of individuals needing care support for their daily living.31 Most care managers currently believe that physician and/or nurse interventions can be initiated after the development of pressure injury, which is not ideal in real-world settings.16 We therefore believe that pressure injury risk assessment scales, including the PPRA-Home, can serve as a bridge between medical and social welfare professionals to achieve a multidisciplinary approach in preventing pressure injuries during home care.
The current study has some limitations worth addressing. The subgroup analysis was underpowered given that this trial focused on determining the overall effects of assessment. Our subgroup analysis showed that the upper limit of the 95% CI in several subgroups reached 1.0, suggesting an excessively wide CI due to small numbers during each analysis.32,33 Considering that subgroup analysis may address practical concerns, such as identifying which type of individuals would benefit the most, more observational or prospective clinical studies with larger sample sizes, including participants with higher care levels, will be needed to determine the effectiveness of each subgroup. The second limitation is intra-observer variability was not evaluated, although the outcome of this study was to measure inter-rater reliability. The busy schedule made it difficult for assessors to conduct intra-observer variability testing in-parallel with this inter-rater reliability study. Separate study needs to be required to clarify whether the assessors themselves valued the same with a temporal distance.
Despite such limitations, the PPRA-Home is currently considered to be a useful pressure injury risk assessment scale among care managers in Japanese home care settings. Based on a previous validity research, this was performed on the premise that the PPRA-Home would be a valid scale for measuring pressure injury risk.21 However, the authors consider that the previous study was preliminary and scarce. Future research shall be conducted to investigate the validity of the PPRA-Home in order to investigate all aspects of the scale with regard to pressure injury prevention. An estimation of cutoff value with sensitivity and specificity will allow care managers to identify risk levels for pressure injury development. Also, an evaluation for clinicometric properties of PPRA-Home with assessors and individuals who have a risk of pressure injury development will be expected to include as a validity study.
Conclusions
The current multicenter cross-sectional study assessed the inter-rater reliability and agreement of the PPRA-Home for pressure injury prevention among individuals who needed partial or full assistance for daily living under the Japanese LTCI system. Our result showed that the PPRA-Home has substantial inter-rater reliability for evaluation of risks of pressure injury development at home care. It is expected that the use of the PPRA-Home potentially contribute to the improvement of the quality of nursing care by early detection of the individuals who have a risk of developing pressure injuries in home care. However, some research focusing on intra-later reliability and validity of the PPRA-Home with adequate sample sizes are required to provide categorical conclusions on whether it can be used for the risk assessment scale in actual clinical settings.
Abbreviations
PPRA-Home, Pressure Injury Primary Risk Assessment Scale for Home Care; LTCI, long-term care insurance.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Sapporo Dermatology Clinic (Number: PRJ Code 21S031). Written informed consent was obtained from all participants. All aspects of this research were in accordance with the principles set forth by the Declaration of Helsinki. There were no major changes in study methods after trial commencement.
Consent for Publication
All authors and their affiliations consented to publication of the study in this journal.
Acknowledgments
The authors thank all the staff, including the manager, nursing stuff, and administrative officer, of our facilities for their valuable cooperation. We also thank Enago (http://www.enago.jp) for their English language editing services.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by funding from ALCARE (Tokyo, Japan).
Disclosure
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MK and YK are employees of ALCARE (Tokyo, Japan) and report this research was supported by funding from ALCARE (Tokyo, Japan). The authors report no other potential conflicts of interest for this work.
References
1. Morikawa M. Towards community-based integrated care: trends and issues in Japan’s long-term care policy. Int J Integr Care. 2014;14:1.
2. Zhang X, Oyama T. Investigating the health care delivery system in Japan and reviewing the local public hospital reform. Risk Manag Health Policy. 2016;9:21–32. doi:10.2147/RMHP.S93285
3. Arai H, Ouchi Y, Toba K, et al. Japan as the front-runner of super-aged societies: perspectives from medicine and medical care in Japan. Geriatr Gerontol Int. 2015;15(6):673–687. doi:10.1111/ggi.12450
4. Masui H, Otaga M, Moriyama Y, Matsushige T. Current issues in long-term care policy and research: toward the promotion of evidence-based policy. J Natl Inst Public Health. 2019;68(1):34–44.
5. Sato A. Characteristics of elderly people with pressure ulcers, and provision of pressure redistribution by family caregivers in home care setting home care setting -analysis of elderly individuals with nursing care levels 4 and 5. Jpn J PU. 2018;20(1):16–25.
6. Sanada H, Miyachi Y, Ohura T, et al. The Japanese pressure ulcer surveillance study: a retrospective cohort study to determine prevalence of pressure ulcers in Japanese hospitals. Wounds. 2008;20(6):176–182.
7. Igarashi A, Yamamoto-Mitani N, Gushiken Y, Takai Y, Tanaka M, Okamoto Y. Prevalence and incidence of pressure ulcers in Japanese long-term-care hospitals. Arch Gerontol Geriatr. 2013;56(1):220–226. doi:10.1016/j.archger.2012.08.011
8. Nakashima S, Yamanashi H, Komiya S, Tanaka K, Maeda T, Jan Y-K. Prevalence of pressure injuries in Japanese older people: a population-based cross-sectional study. PLoS One. 2018;13(6):e0198073. doi:10.1371/journal.pone.0198073
9. García-Fernández FP, Agreda JJS, Verdú J, Pancorbo-Hidalgo PL. A new theoretical model for the development of pressure ulcers and other dependence-related lesions. J Nurs Scholarsh. 2014;46(1):28–38. doi:10.1111/jnu.12051
10. Bergstrom N, Braden B, Laguzza A, Holman V. The braden scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205–210. doi:10.1097/00006199-198707000-00002
11. Kring DL. Reliability and validity of the braden scale for predicting pressure ulcer risk. JWOCN. 2007;34(4):399–406.
12. Park SH, Choi YK, Kang CB. Predictive validity of the braden scale for pressure ulcer risk in hospitalized patients. J Tissue Viability. 2015;24:102–113. doi:10.1016/j.jtv.2015.05.001
13. Comfort EH. Reducing pressure ulcer incidence through braden scale risk assessment and support surface use. Adv Skin Wound Care. 2008;21(7):330–334. doi:10.1097/01.ASW.0000323519.08306.ea
14. Ohura T. Risk factors for pressure ulcers of elderly people. Jpn J PU. 2002;4(3):397–405.
15. Takagi Y, Toyohara T. Use of our criteria for the selection support surface and changes in the incidence of pressure ulcer. Jpn J PU. 2008;10(1):39–43.
16. Kohta M, Kameda Y, Morita S. Knowledge and practice for pressure injury prevention among care managers in a home care setting: a cross-sectional study. Chronic Wound Care Manag Res. 2017;4:99–105. doi:10.2147/CWCMR.S140673
17. Walsh JS, Plonczynski DJ. Evaluation of a protocol for prevention of facility-acquired heel pressure ulcers. JWOCN. 2007;34(2):178–183.
18. Webster J, Coleman K, Mudge A, et al. Pressure ulcers: effectiveness of risk-assessment scale. A randomized controlled trial (the ULCER trial). BMJ Qual Saf. 2011;20(4):297–306. doi:10.1136/bmjqs.2010.043109
19. Matsuda S. How has the Japanese health system implemented the care management system? Asian Pac J Dis Manage. 2009;3(2):33–38.
20. Tsutsui T, Muramatsu N. Care-needs certification in the long-term care insurance system of Japan. J Am Geriatr Soc. 2005;53(3):522–527. doi:10.1111/j.1532-5415.2005.53175.x
21. Morita S, Kohta M, Nakamura C, Kameda Y. Development of a risk assessment scale to predict pressure injury targeting Japanese care managers. Jpn J PU. 2019;21(1):34–40.
22. Fujii K, Komoda T, Maekawa A, Nishikawa M. Foot care knowledge and practices among Japanese nurses and care workers in home care and adult service center: a cross sectional study. BMC Nurs. 2020;19:75. doi:10.1186/s12912-020-00467-1
23. Landis JR, Koch CG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. doi:10.2307/2529310
24. Kohta M, Sakamoto K, Kawachi Y, Oh-I T. A single-center, prospective, randomized, open label, clinical trial of ceramide 2-containing hydrocolloid dressings versus polyurethane film dressings for pressure ulcer prevention in high risk surgical patients. Chronic Wound Care Manag Res. 2015;2:171–179. doi:10.2147/CWCMR.S93555
25. Halfens RJ, Achterberg TV, Bal RM. Validity and reliability of the braden scale and the influence of other risk factors: a multi-centre prospective study. Int J Nurs Stud. 2000;37(4):313–319. doi:10.1016/S0020-7489(00)00010-9
26. Kottner J, Dassen T. Pressure ulcer risk assessment in critical care: interrater reliability and validity studies of the braden and waterlow scales and subjective ratings in two intensive care units. Int J Nurs Stud. 2010;47(6):671–677. doi:10.1016/j.ijnurstu.2009.11.005
27. Kottner J, Halfens R, Dassen T. An interrater reliability study of the assessment of pressure ulcer risk using the braden scale and the classification of pressure ulcers in a home care setting. Int J Nurs Stud. 2009;46(10):1307–1312. doi:10.1016/j.ijnurstu.2009.03.014
28. Kottner J, Audigé L, Brorson S. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. J Clin Epidemiol. 2011;64(1):96–106. doi:10.1016/j.jclinepi.2010.03.002
29. Hripcsak G, Heitjan DF. Measuring agreement in medical informatics reliability studies. J Biomed Inform. 2002;35(2):99–110. doi:10.1016/S1532-0464(02)00500-2
30. Shaked E, Gefen A. Modeling the effects of moisture-related skin-support friction on the risk for superficial pressure ulcers during patient repositioning in bed. Front Bioeng Biotechnol. 2013;1:9. doi:10.3389/fbioe.2013.00009
31. Inoue T. The present situation and the problem of visiting nursing: team care management of pressure ulcer in the elderly. Japan Med Assoc J. 2015;58(1–2):19–22.
32. Cuzick J. Forest plots and the interpretation of subgroups. Lancet. 2005;365(9467):1308. doi:10.1016/S0140-6736(05)61026-4
33. Rothwell PM. Subgroup analysis in randomised controlled trials: importance, indications, and interpretation. Lancet. 2005;365(9454):176–186. doi:10.1016/S0140-6736(05)17709-5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.