Back to Journals » International Journal of General Medicine » Volume 16
Intention to Donate Kidney and Associated Factors Among Students in Bahir Dar University: Application of Theory of Planned Behavior
Authors Tesema B, Bogale EK ![]() , Wasihun Y
, Wasihun Y ![]() , Anagaw TF
, Anagaw TF ![]()
Received 10 October 2023
Accepted for publication 13 November 2023
Published 20 November 2023 Volume 2023:16 Pages 5363—5376
DOI https://doi.org/10.2147/IJGM.S441636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Belete Tesema,1 Eyob Ketema Bogale,2 Yosef Wasihun,2 Tadele Fentabil Anagaw2
1Department Public Health, College of Medicine and Health Science, Wolaita Sodo University, Wolaita, Ethiopia; 2Department of Health Promotion and Behavioral Science, School of Public Health, College of Medicine and Health Science, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Tadele Fentabil Anagaw, Department of Health Promotion and Behavioral Science, School of Public Health, College of Medicine and Health Science, Bahir Dar University, Pobox O79, Bahir Dar, Ethiopia, Tel +251-927692916, Email [email protected]
Background: Kidney donation is the donation of a kidney from a living or dead person to another living person who requires transplantation. The scarcity of kidneys is a great public health concern worldwide, owing to an increase in end-stage renal failure. There is no sufficient evidence regarding the intention to donate kidneys in Ethiopia.
Objective: To assess the intention to donate kidneys and its associated factors among Bahir Dar University students in Ethiopia in 2023 by the application of theory of planned behavior.
Method and Materials: This institution-based cross-sectional study was conducted from March 7 to April 5, 2023. A multistage sampling technique was used to select 630 participants. Self-administered structured questionnaires were used to collect data. Data were entered into Epi-data version 4.6, and exported to the Statistical Package for the Social Sciences (SPSS) version 25 for analysis. Bivariate and multivariate linear regression analyses were performed. Findings with a p-value < 0.05 at the 95% confidence interval were considered statistically significant and interpreted by the unstandardized beta (ß) coefficient.
Results: The mean score of intention to donate the kidney was 12.9 ± 4.1 standard deviation. Direct attitude (B = 0.341, 95% CI = 0.265, 0.416), direct subjective norm (B = 0.088, 95% CI = 0.010, 0.167), direct perceived behavioral control (B = 0.353, 95% CI 0.251, 0.455), knowledge (B = 0.417, 95% CI 0.251, 0.583), and previous experience of blood donation (B = 0.915, 95% CI 0.321, 1.510) were factors associated with intention to kidney donation.
Conclusion: The mean score of intention to donate kidneys was 12.9 ± 4.1 SD. Direct attitude, direct subjective norm, direct perceived behavioral control, experience with blood donation, and knowledge of participants were significant factors for the intention to donate kidneys. Therefore, social and behavioral change communication strategies should address these factors in order to increase kidney donation.
Keywords: intention, kidney donation, theory of planned behavior, organ donation
Introduction
Organ donation is the removal and legal transfer of biological tissue or an organ of the human body from a living person through consent or from a dead person to a living recipient who requires transplantation.1
There are two types of organ donation: deceased organ donation is the donation of parts of cells, tissues, or organs after death, whereas living organ donation is the donation of organs from one living person to another who requires a transplant.2,3 The kidney is the most commonly donated and transplanted solid organ worldwide.4
Kidney transplant (KT) is one of the major developments in modern medicine and the best choice for failed kidneys.5 The first successful KT was performed in 1959 in Louisiana.6 The transplant practice first reached South Africa in 1967. The first living-related KT program was initiated in Ethiopia in 2015.7 In 2014, the Ethiopian government enacted an organ transplantation law accepting KT program candidates over the age of 14.7
Chronic kidney disease (CKD) is a common global health problem affecting 10–15% of the world’s population.8,9 The global burden of CKD is rapidly increasing, and is expected to become the fifth leading causes of death (4–10 million people) worldwide by 2040.10 According to the Global Burden of Disease (GBD) study, disability-adjusted life years (DALYs) for CKD increased from 0.8% to 1.6%, with the largest absolute increase in the number of DALYs between 1990 and 2019.11
Renal dialysis is the most common treatment for renal failure, worldwide. However, KT is now a better treatment than dialysis, offering better quality of life, better survival, and greater economic productivity.12 According to the International Society of Nephrology (ISN), the framework for integrated kidney care prioritizes KT over all other modalities of KRT.13
However, the applicability of KT is limited by a shortage of organs for transplant; this remains an unsolved problem for human resources, and many patients wait for extended periods of time for kidneys from donors.14
According to the International Report on Organ Donation and Transplantation (IRODT) 2020, approximately 80,926 KTs were performed, 32% of which were from living donors, this showed a 21% decrease from 2019 and only covered less than 10% of the global need for kidney supply, so the donation rates remain insufficient to meet the minimum need.15
In the USA, 17 people die every day, waiting for a life-saving organ transplant. More than 100,000 patients are waiting for a transplant, and the majority of those (89,735) are waiting for a kidney.16 In India approximately 150,000 people wait for a KT every year, but only 5000 are transplanted, and more of them die while waiting for transplantation due to a shortage of the organ.17 In Singapore, living kidney donors contribute to 54% of all transplants at a rate of 24.8 PMP but this cannot meet the demand for transplantation.18
Only 21% of low-income and middle-income countries (LLMIC) were performing KTs.19 In Africa, the living donor KT rate is the lowest at 2 PMP, which is eight times lower than in North America, and reports on the deceased organ donation rate are limited.12 In South Africa, the national KT rate of 6.4 PMP is on a downward trend owing to the constraints of kidney donation.20
The prevalence and incidence of End stage kidney disease(ESKD) requiring dialysis are increasing, and 59% of people in sub-Sahara Africa (SSA) stop dialysis because of economic crises.21 This has become a significant challenge for achieving the health-related sustainable development goals by 2030 and Universal Health Coverage.22
Kidney donation is greatly influenced by multiple factors, such as lack of knowledge, pre-existing relations, religious beliefs, family influences, body integrity, and previous interactions with the health care system, negative attitudes, and socio-demographic factors.23–25 Renal disease has become a significant public health problem in Ethiopia, and the number of patients requiring maintenance dialysis and transplantation is steadily rising.26 In 2022, 1132 patients were undergoing hemodialysis (HD).27
Kidney transplantation is the ideal choice for KRT because it offers a lower risk of mortality and better quality of life than dialysis care.19 Evidence suggests that an increasing number of Ethiopians travel abroad to seek tertiary health care services. Some patients travel to other countries for transplantation; such travel involves an estimated average cost of about US$20,000 per trip and this resulted in the cost of annual outflow for medical tourism in Ethiopia exceeding US$100 million per year. To avoid this, the Ethiopian Ministry of Health launched a national specialty and sub-specialty service road map, planned to expand transplant centers, and planned to perform 10,000 and 50,000 organ transplantation in the fifth and tenth year of the road map, respectively.28 However, only 300 transplant recipients received organs from living donors at the Saint Paul’s Hospital, Millennium Medical College.7
Theory of Planned Behavior (TPB) focus on theoretical constructs concerned with individual motivational factors as determinants of the likelihood of performing specific behaviors. TPB is an extension of the theory of reasoned action and is important for an individual’s decision-making behavior.29 TPB rest on an underlying assumption that the best predictor of a behavior is intention, which is determined by attitudes toward behavior, social normative perceptions and perceived control over the performance behavior.30 The Theory of Planned Behavior (TPB) is a behavioral theory that can be used to discover the factors that influence organ donation behavior and design successful interventions.31 Therefore, applying this theoretical model is important for predicting students’ intention to donate a kidney.
An imbalance in the demand and supply of organs exists in almost every country owing to numerous causes; thus, students are a younger and healthier part of the population, and they have the potential to donate a kidney in future life.32 Although KT is accepted as the best treatment modality for End stage renal failure (ESRF), there is no evidence of the intention and factors associated with kidney donation. Therefore, this study aimed to assess the intention to donate kidneys and the associated factors among students at Bahir Dar University by the application of theory of planned behavior to fill this gap.
Methods and Materials
Study Area and Period
Bahir Dar University is located in Bahir Dar City, 565 km from Addis Ababa, the capital of Ethiopia. It was established in 1954 as a polytechnic, and in 2001 as a university. It is one of Ethiopia’s largest universities, accepting over 21,000 students and offering a different undergraduate and postgraduate program divided into 69 bachelors, 118 masters, and 32 doctoral programs. By 2023, it had eight campuses and 15 academic units.33 The study participants are under graduate students attending at Bahir Dar university. The total number of students at Bahir Dar university attending undergraduate program was 21,577 by 2022/2023. The study was conducted from March 7 to April 5, 2023.
Study Design
An institution-based cross-sectional study design was used to recruited undergraduate students in Bahir Dar University.
Population
Source population
All undergraduate students who attend at Bahir Dar University at regular program.
Study Population
Randomly selected regular undergraduate students from selected departments of Bahir Dar University.
Inclusion Criteria
All undergraduate regular students who were present during data collection at Bahir Dar University.
Exclusion Criteria
Those extension and distance undergraduate students that means students who cannot be accessed during data collection period due to their educational program schedule. First year students are excluded due to the fact that they are not assigned specific department, all they take common course.
Sample Size Determination
The sample size was determined using a single population proportion formula with proportion of (45.9%) previous studies on willingness to donate kidneys in Nigeria34 by considering 95% confidence interval and 5% margin of error (d).
The sample size was determined using the following formula: -

Design effect 1.5 = 572 and 10% nonresponse rate final sample size was 630 participants.
Sampling Procedure and Technique
A multi-stage sampling technique was used to select 630 students. From the 15 academic units at Bahir Dar University, five were randomly selected by lottery methods as a primary sampling unit with 30% consideration. Each unit was proportionally and randomly chosen from the selected academic unit departments. Three departments from the College of Medicine and Health Science, four departments from the College of Science, four departments from the College of Social Science, three departments from the College of Business and Economics, and two departments from the College of Education and Behavioral Science were selected as secondary sampling units. Then, proportional allocation was performed for each selected department and year of study. Finally, the participants were selected using a simple lottery method from each year of study from second year to sixth year of study.
Study Variables
Dependent Variable
Intention to donate a kidney.
Independent Variables
Socio-demographic variables: Age, sex, religion, year of study, department, resident, personal related factors (history of blood donation, having family living with CKD, having family who donated kidney, family with CKD), knowledge and TPB constructs (attitude, subjective norm, perceived behavioral control).
Operational Definition
Knowledge: Study participants were asked 10 knowledge questions that required a yes or no response regarding kidney donation, and the total score obtained for each respondent was summed, with a higher score indicating good knowledge.35
Intention: The participant’s report of the readiness to donate a kidney and the summed score of five items of 5-point Likert scale approaching the maximum sum score considered high intention to donate a kidney.36
Attitude: The belief of the participants on the usefulness of donating a kidney.36
Subjective norm: Social pressure from others that participants feel to donate kidney.36
Perceived behavioral control: The participant’s perception of the degree to which the kidney is easy or difficult to donate.36
Data Collection Procedure
Data were collected using self-administered, structured, and pretested questionnaires. The questionnaire were adapted from different literatures,37–40 and theory of planned behavior constructs attitude, subjective norm and perceived control items were developed from elicitation studies. An open-ended elicitation interview was conducted with 20 participants to identify relevant behavioral outcomes, referents, facilitators, and barriers to the target population. Elicitation study content was analyzed by coding related items into similar constructs and a frequency table for the participant’s response. The items of theory of planned behavior were validating using explanatory factor analysis. The questionnaires included questions on sociodemographic variables, attitudes, subjective norms, perceived behavioral control, and knowledge (Supplementary File 1).
Measurement
Knowledge was assessed using ten items, and each item was measured as a yes or no response. All items’ scores were summed up to get over all knowledge scores, when individuals correctly answered the item was recoded and given a value of “1”, and those answered incorrectly were valued at “0”, which ranges from 0 to 10 and used as continuous variable for further analysis.
Intention to kidney donation was measured using five items with 5-point Likert scale responses ranging from “strongly disagree” (1) to “strongly agree” (5). All items were summed up as a composite score with a minimum of 5 to a maximum score of 25 points and approaching the maximum sum score considered high intention to donate a kidney.
Direct attitude was measured using five items on the SDS with a minimum of 5- and a maximum of 25-point scores. A composite score of direct attitudes was obtained by summing all five items and approaching the maximum sum score considered favorable. Indirect attitude was measured by using four items of behavioral belief, responses ranged from “strongly disagree agree” (1) to “strongly agree” (5), and the respective four items of outcome evaluation with a 5-point Likert scale with responses ranging from “very bad = (1) to very good = (5)”. A composite score of indirect attitudes was obtained by summing up all four products of behavioral belief and outcome evaluation and then used for further analysis as a continuous variable.
Direct subjective norm was measured by using five items of 5-point Likert scale with a minimum of 5- and maximum 25-point score with response ranged from “strongly disagree agree = (1) to strongly agree = (5)” and the composite score was obtained summing up of all items and used for further analysis as continuous variable.
Indirect subjective norm was measured using four items of normative belief 5-point Likert scale responses ranging from “strongly disagree = (1) to strongly agree = (5)” and respective motivation to comply of four items of 5-point Likert scale responses from “not very much = (1) to very much = (5)”. A composite score of indirect subjective norm was obtained by summing up all the products of normative belief with the respective motivation to comply with items, and was used for further analysis as continuous variables.
Direct perceived behavioral control was measured using four items of a 5-point Likert scale. The composite score of direct perceived behavioral control was obtained by summing all items with a minimum of 4- to a maximum 20-point score, and was used for further analysis as continuous variables. Indirect perceived behavioral control was measured by four items of control belief response ranged from “very unlikely = (1) to very likely = (5)” and respective four items of perceived power with 5-point Likert scale response ranging from “strongly disagree = (1) to strongly agree = (5)”. The indirect perceived behavioral control score was obtained by summing all the products of control beliefs and perceived power and was used for further analysis as a continuous variable.
Data Processing and Analysis
Data were cleaned, edited, checked for consistency and completeness, recoded, entered into Epi-data version 4.6 then exported to SPSS version 25 for analysis. Descriptive statistics were used to summarize the frequency and percentage for categorical variables and the mean and standard deviation for continuous variables. Correlation analysis was performed between each construct and intention using the Pearson’s correlation coefficient(r). Bi-variable and multivariable linear regression analyses were performed to test the strength and association between the dependent and independent variables. Variables with a p-value <0.25 in simple linear regression were entered into multiple linear regression analysis to identify the significant variables that affected behavioral intention, and variables with p-value <0.05, with 95% confidence intervals considered as significant for the final model of analysis. The unstandardized ß coefficient was used to explain the strength of the association between direct and indirect constructs and intention.
The assumption of normality was checked graphically by using a histogram with a normal bell shape and a P-P plot that resulted in residuals that were normally distributed and lay around the diagonal line. Homoscedasticity was checked using a scatter plot, and no pattern was observed in the graph, indicating that the residuals had a constant variance. Linearity was assessed by using a scatter plot of the dependent variable and each independent variable. Multicollinearity was also checked by the variance inflation factor (VIF) and tolerance. The independent variables had a VIF value of less than 1.3 and were checked by conducting a correlation matrix of independent variables, and there was no correlation coefficient greater than 0.7, which was suspected of multi-collinearity. The assumption of an outlier was tested using Cook’s distance. The box plot showed that there was no outlier less than 0.01 Cook’s distance, and there were no observations (asterisk) in the box plot.
Data Quality Control
Data quality was assured through a pretest, which was conducted at Injibara University on 5% of study participants one week before the actual data collection period, and necessary corrections and clarities were made on the questionnaire. One-day training was provided to two BSc nurse data collectors and one BSc public health supervisor on the objective of the study, data collection procedures, content of the questionnaire, close supervision of the data collectors, and proper handling of the data. All negatively worded items were reverse-coded for analysis. The reliability of the constructs was measured using Cronbach’s alpha to check the internal consistency of each item, with a minimum Cronbach alpha (α = 0.74). The validity of the construct was checked using exploratory factor analysis with a principal component analysis (PCA) as the extraction method and the Prom ax rotation.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of the College of Medicine and Health Science of Bahir Dar University (approval number: CMHS/ IRB /726/2023). Detailed information was provided to the participants, and written consent was obtained from each study participant before the beginning of data collection. The study received ethical clearance in accordance with the Declaration of Helsinki.
Result
Socio-Demographic Characteristics of Study Participants
Of the total sample size (630), 601 participants completed the study, making a response rate of 95.4%. The mean age of the respondents was 23.12 years with ±1.96 SD. Three hundred forty-three (57.1%) participants were Orthodox religious followers. Approximately 213 (35.4%) participants were fourth year students. Among the total study participants, 312 (51.9%) were from urban areas (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Bahir Dar University Students, North West Ethiopia, 2023 (n = 601) |
Knowledge of Students Towards Kidney Donation
The mean score for knowledge of kidney donation was 6.56 ± 1.76 SD. Among the study participants, 520 (86.5%) and 321 (53.4%) know a kidney could be donated during life and after death, respectively, and 410 (68.2) participants reported that selling the kidney is an illegal practice (Table 2).
 |
Table 2 Knowledge Towards Kidney Donation Among Students in Bahir Dar University, Bahir Dar Ethiopia, 2023 (n = 601) |
Personal Related Factors
Two hundred forty-one (40.1%) participants had donated blood previously. Thirty-nine (6.5%) participants had family members/relatives living with CKD and 35 (5.8%) had discussed kidney donation with their family. Two and three participants reported having family members/relatives who had undergone KT and donation, respectively.
Reliability and Validity of TPB Construct
A reliability analysis was performed to check the internal consistency of the TPB constructs using Cronbach’s alpha (α). The reliability score of behavioral intention (α = 0.91) was the highest, and attitude (α = 0.86), subjective norm (α = 0.83), and perceived behavioral control (α = 0.72) were the lowest.
An exploratory factor analysis was conducted using PCA as the extraction method and prom ax rotation. For direct construct, there were four components with a total variation of 60.3%: KMO = 0.88, Bartlett’s test of sphericity chi-squared = 4608.54, def. = 171, sig. = 0.000, factor loading >0.4 retained until the cross-loading removed one cross-loaded item was dropped at one component. From intention, five out of six items, all items of attitude, subjective norm, and perceived behavioral control were loaded with their respective constructs. For indirect constructs of TPB, all items were validated, with total variance explaining 66.70% of items with five components: KMO value = 0.86, Bartlett’s test of sphericity chi-square = 6530.26, DF = 276, sig = 0.000, factor loading >0.4 was retained. Two items from indirect attitude, one from indirect subjective norm, and two from indirect perceived behavioral control, were excluded. Finally, eight items for each of indirect attitude, indirect subjective norm, and indirect perceived behavioral control were validated.
Descriptive Statistics of TPB Construct
The mean score of behavioral intention towards kidney donation was Mean = 12.9 ± 4.1SD with the minimum of 5- to the maximum of 25-point score. The mean score of direct attitudes, and indirect attitude towards kidney donation were (Mean = 17.70 ± 4.0, SD) and Mean = 58.0 ± 21.5 SD) respectively (Table 3).
 |
Table 3 Descriptive Statistics of the Components of the TPB Among Students in Bahir Dar University, North West Ethiopia, 2023 (n = 601) |
Mean Difference Between Predictor Variable and Intention to Donate Kidney
An independent-samples t-test was run to determine whether there was a mean difference between male and female participants regarding the intention to donate a kidney.
The results showed that there was no significant mean difference between males and females in terms of gender to donate kidneys, but there was a mean difference between rural and urban inhabitants on the intention to donate a kidney. Overall, the score for rural inhabitants (M = 2.4 SD = 0.87) was significantly lower than that for urban inhabitants (M = 3.0, SD = 0.90, t (599) –2.375, p = 0.018). Based on the previous exercise of participant, those participants who donated blood had a slightly higher mean than those had not donated blood previously (M = 3.01, SD = 0.89, higher than those had not donated blood: M = 2.4, SD 0.85, t (599) = 2.903, p = 0.004). Sociodemographic variables (religion, years of study, and department) showed no significant mean differences in the one-way ANOVA.
Descriptive Results of Direct Constructs of TPB
Two hundred thirty-three (38.8%) and 46 (7.5%) of participants reported that kidney donation was good and bad, respectively. More than one-third (34.3%) of respondents reported that kidney donation was useful. Approximately a quarter of the respondents (26.6%) agreed that most people would agree to donate a kidney. One hundred eighty-five (30.8%) participants reported that donating a kidney was difficult for them. Moreover, approximately 158 (26.3%) participants agreed that they intended to donate a kidney in the future.
Descriptive Frequency of Indirect Components of TPB
Frequency of Indirect Attitude
Nearly half of the study participants, 49.4 and 49.9 respectively agreed that donating a kidney could save lives, and saving lives through kidney donation was good for them.
Indirect Subjective Norm
The study showed that 10.6% of respondents agreed that friends think that participants should donate a kidney. Approximately 258 (42.9%) respondents disagreed that their mothers believed participants should donate a kidney. However, 177 (29.5%) respondents reported that their mother’s approval was very important when deciding whether to donate a kidney.
Indirect Perceived Behavioral Control
The results showed that 220 (36.6%) of the respondents reported that they were likely to free to donate a kidney. One hundred sixty-two (27%) participants reported that they were likely to donate a kidney if the service was available. More than one-third (36.4%) of participants agreed that lack of knowledge makes it difficult to donate a kidney.
Correlation Analysis of Direct and Indirect Construct of TPB
Correlation was performed between the direct and indirect constructs of TPB using the Pearson correlation coefficient, which showed a positive relationship between the constructs. Direct and indirect subjective norms had the strongest correlation (r = 0.537, p < 0.01) (Table 4).
 |
Table 4 Correlation Between Direct and Indirect Constructs of TPB |
Intention of Students Towards Kidney Donation
This study showed that the mean score of intention to donate kidney among the students was 12.9 ± 4.1 with a maximum and minimum score of 5- to-25-point scores.
The average weighted mean score of the participant was 2.56 ± 1.00, which was below the neutral score.
Factors Associated with Intention to Donate a Kidney Among Bahir Dar University Students
A bi-variable analysis was conducted to assess the association between the intention to donate a kidney and other independent variables. Variables with a P-value ≤0.25 from bi-variable analysis, were department (Marketing, Nursing, Biology, Medicine, Midwifery, Civics and Geography), year of study, residence, direct attitude, direct subjective norm, direct perceived behavioral control, previous history of blood donation, having a family with kidney disease, and transplantation were candidates for multiple linear regression analysis.
From multiple linear regression analysis, direct attitude (B = 0.341, 95% CI [0.265, 0.416], p < 0.001), direct subjective norms (B = 0.088, 95% CI [0.010, 0.167], p = 0.027), direct perceived behavioral control (B = 0.353, 95% CI [0.251, 0.455], p < 0.001), knowledge (B = 0.417, 95% CI [0.251, 0.583], p < 0.001), and previous experience of blood donation (B = 0.915, 95% CI [0.321, 1.510], P = 0.003) were statistically significant predictor of intention to donate kidneys.
The TPB variables were explained 38.3% of the variance in intention to donate a kidney. All variables in the model were accounted 44.2% (Adjusted R2 = 0.442) of the variance in intention to donate kidney. For a unit increase in positive attitude towards kidney donation, the intention to donate the kidney will increase by 0.341, and for a unit increase in direct perceived behavioral control sum of score, the intention to donate a kidney will increase by 0.353, keeping other variables constant. As participants’ knowledge increased by one unit, their intention to donate a kidney increased by 0.417, with other variables constant. Participants who had previous experience of blood donation were 0.915 times more likely than those who had not donated blood previously (Table 5).
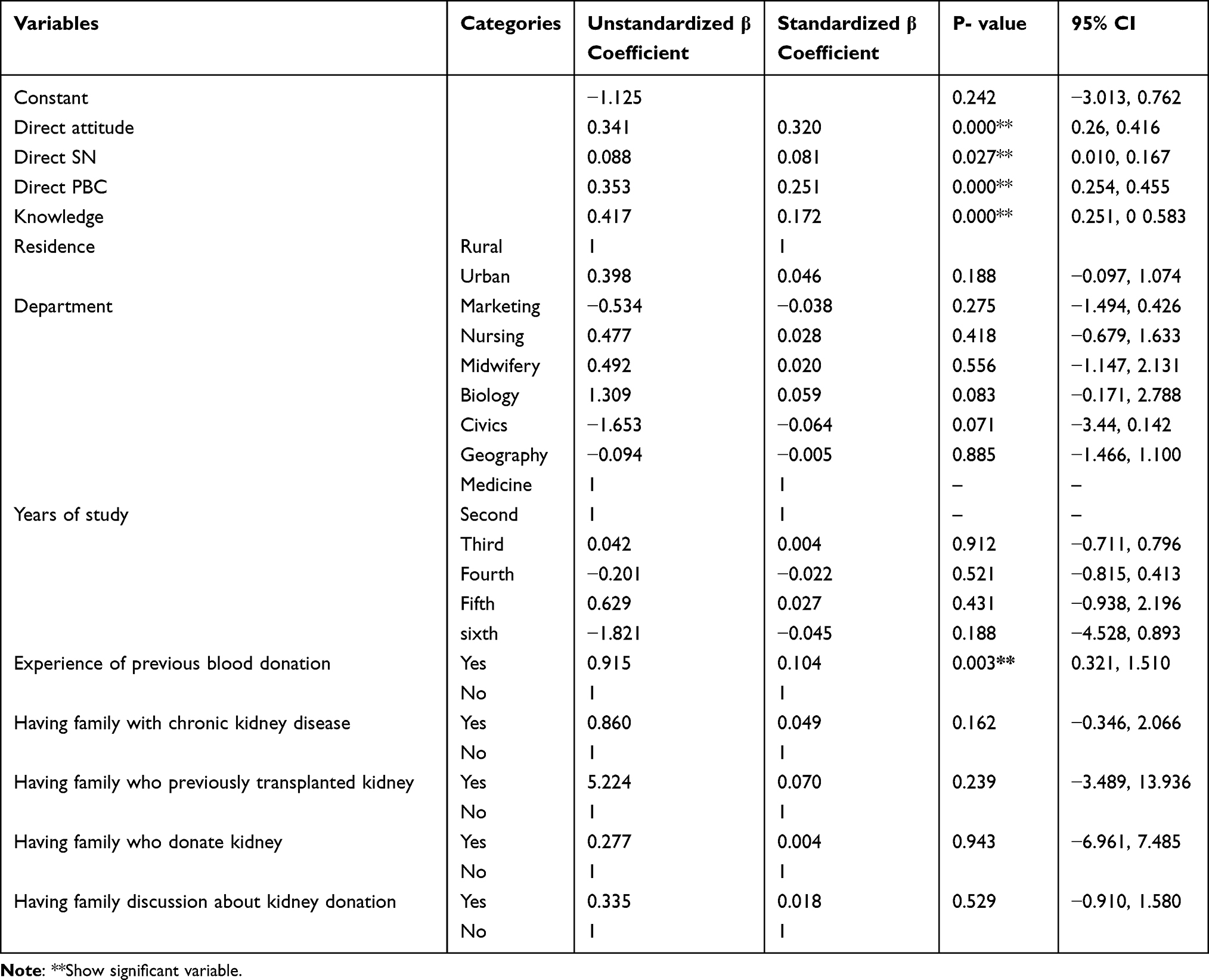 |
Table 5 Factors Associated with Intention to Donate a Kidney Among Bahir Dar University Students, North West Ethiopia, 2023 (N = 601) |
Discussion
This study aimed to determine the intention to donate a kidney and its predictors among students. Direct attitude, subjective norms, perceived behavioral control, knowledge, and previous experience with blood donation were predictors of the intention to donate the kidney.
The TPB variables explained 38.3% of the variance of intention to donate a kidney, this finding was lower than the results indicated in a review of health-related behaviors, an average of 41% explanation of intention.41 This result was also lower than a study conducted in the UK, the variance accounted by the model was 72% variation in organ donation intention.42 This discrepancy might be due to the relative difference in the predictive ability of theory on the different behavioral intentions and settings and might be due to the socioeconomic and sociocultural variation of the participants. The results showed that the mean score for kidney donation kidney was 12.9. This finding is lower than that of a study conducted in China that reported a mean willingness toward organ donation of 56.9.43 This discrepancy may be due to methodological variations, population differences, or measurement scales. The current study revealed that the average weighted mean was 2.56 ± 1.00, indicating that the weighted mean of respondents was slightly lower than the neutral score.
This study showed that perceived behavioral control is a strong predictor of the intention to donate a kidney. This finding is similar to those of studies conducted in Iran and Saudi Arabia on organ donation, indicating that perceived behavioral control is significantly and positively associated with behavioral intention.31,44 This implies that, considering that these control factors are crucial in supporting students to donate the kidney and removing the barriers through the possible assurance mechanisms and promoting the facilitators could improve the intention of the students to donate a kidney, the findings indicate that considerable effort should be undertaken to control the barriers. This result is supported by Ajzen’s theoretical assumptions, which mean that the more an individual has a high degree of control over factors that facilitate or prevent them from donating a kidney, the greater is their intention to donate a kidney.45
In this study, positive attitude was another important predictor of intention to donate the kidney. This study is similar to a study conducted in Nigeria in that positive attitude was an important predictor of students’ willingness to donate kidneys,34 and that attitude has a statistically significant association with willingness among students to donate kidneys.44,46 However, another study in Iran indicated that attitude was not a significant predictor of intention to donate organs.47 This difference may be due to the difference in the study setting or conditions in which the behavior occurred and where the study was carried out, and may be due to variation in personal beliefs and evaluation of behavior among participants. This result implies that undertaking targeted behavior change intervention on negative behavioral beliefs and promoting positive beliefs regarding kidney donation is important to increase positive attitudes toward kidney donation and may influence behavioral intentions to donate a kidney.
The current study revealed that subjective norms were a predictor of the intention to donate a kidney among participants. This finding is supported by studies conducted in Iran and Korea, with two studies conducted in Saudi Arabia and America; subjective norm was an important significant predictor of intention to donate organs.31,48–50 This implies that significant others have the power to influence a participant’s decision to donate kidneys. Thus, considering strategies that address the influence of these referents on the participant’s decision, focusing on both the targeted population and significant others, those who have the power to influence others’ decisions, such as family members and friends, should be considered as a whole to improve kidney donation. This suggests that decisions made in this context not only depend on the respondents, but other important influences could also be the target for promoting participants’ decisions on kidney donations.51
The current results revealed that knowledge is another important and significant factor associated with kidney donation intentions. This result is also consistent with a study conducted in Nigeria and Saudi Arabia, which indicated that knowledge had a significant association with the intention to donate a kidney, indicating that having knowledge regarding kidney donation may have a profound importance in removing and/or decreasing the barriers to participants’ decisions about kidney donation.34,46 This implies the need for considerable strategies, such as developing campaigns and expanding educational activity campaigns by skilled professionals and media involvement, as important strategies to raise knowledge about kidney donation and increase kidney donation intention.52
The current study showed that previous experience with blood donation was another significant predictor of the intention to donate a kidney. This finding is similar to that of a study conducted in Australia, the UK, and China.53–55
This indicates that a participant’s belief that they may be the type of person who would donate organs may be informed by other donation behaviors, such as blood donation, and reinforced by behaviors such as communicating about donation desires with others. Therefore, blood donors are an important target population for potential kidney donors, and it is possible to recruit potential organ donors from blood donors. Hence, interventions on kidney donation should be considered, programs and campaigns on blood donation, which may increase kidney donation awareness through frequent information exposure, and decrease barriers and negative beliefs.
Strengths and Limitations of the Study
The strength of this study may be unique in that it is the first in this area to assess the intention to donate the kidney among students and the application of a theoretical model, which is a good theoretical model for predicting a student’s intention to donate a kidney and identifying the factors. This study is not out of limitation because the self-administered questionnaire and self-reports might lead to a social desirability bias, even if maintained by anonymizing the participants by code rather than name and assuring confidentiality. Another limitation of this study is that the results may not be generalizable to the community level.
Conclusion
This study established that the mean score of the intention to donate a kidney was 12.9 ±4.1 SD, which was far to the maximum score. From the theory of planned behavior constructs direct attitude, subjective norm, and perceived behavioral control were significant predictors of intention to donate kidney. Past experience of blood donation, and knowledge of participants toward kidney donation were positively and significantly associated with intention to donate kidney. Therefore, these factors need to be considered when designing interventions to increase students’ intentions to donate a kidney.
Abbreviations
CKD, chronic kidney disease; ESRF, end-stage renal failure; HD, hemodialysis; ISN, International Society of Nephrology; KRT, kidney replacement therapy; KT, kidney transplantation; PMP, per million population; TPB, theory of planned behavior.
Data Sharing Statement
Data is available with the manuscript.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of the College of Medicine and Health Science of Bahir Dar University (approval number: CMHS/ IRB /726/2023). Detailed information was provided to the participants, and written consent was obtained from each study participant before the beginning of data collection. The study received ethical clearance in accordance with the Declaration of Helsinki.
Consent for Publication
All authors have agreed upon publication of this original article.
Acknowledgment
First, I would like to thank Bahir Dar University College of Medicine and the Health Science Department of Health Promotion and Behavioral Science for providing me with this opportunity. In addition, I would like to express special thanks to all study participants, data collectors, and supervisors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. World Health Organization. Global Glossary of Terms and Definitions on Donation and Transplantation. Genebra: World Health Organization; 2009.
2. Rudow DL, Ohler L, Shafer T. A Clinician’s Guide to Donation and Transplantation. Natco; 2006.
3. World Health Organizatin. Global Glossary of Terms and Definitions on Donation and Transplantation. World Health Organizatin; 2009.
4. Maldonado RA, Bisigniano L. Global perspective on kidney transplantation: Argentina. Kidney. 2022;3(2):368. doi:10.34067/KID.0002632021
5. Barker CF, Markmann JF. Historical overview of transplantation. Cold Spring Harb Perspect Med. 2013;3(4):a014977. doi:10.1101/cshperspect.a014977
6. Nordham KD, Ninokawa S. The history of organ transplantation. In: Baylor University Medical Center Proceedings. Taylor & Francis; 2022.
7. Ahmed MM, Tedla FM, Leichtman AB, Punch JD. Organ transplantation in Ethiopia. Transplantation. 2019;103(3):449–451. doi:10.1097/TP.0000000000002551
8. Alemu H, Hailu W, Adane A. Prevalence of chronic kidney disease and associated factors among patients with diabetes in northwest Ethiopia: a hospital-based cross-sectional study. Curr Ther Res. 2020;92:100578. doi:10.1016/j.curtheres.2020.100578
9. Ke C, Liang J, Liu M, Liu S, Wang C. Burden of chronic kidney disease and its risk-attributable burden in 137 low-and middle-income countries, 1990–2019: results from the global burden of disease study 2019. BMC Nephrol. 2022;23(1):1–12. doi:10.1186/s12882-021-02628-z
10. Li P, Garcia-Garcia G, Lui S-F, et al. Kidney health for everyone everywhere–from prevention to detection and equitable access to care. Braz J Med Biol. 2020;2020:53.
11. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
12. Mudiayi D, Shojai S, Okpechi I, et al. Global estimates of capacity for kidney transplantation in world countries and regions. Transplantation. 2022;106:6.
13. Tonelli M, Nkunu V, Varghese C, et al. Framework for establishing integrated kidney care programs in low-and middle-income countries. Kidney Int Suppl. 2020;10(1):e19–e23. doi:10.1016/j.kisu.2019.11.002
14. Nurrachma EA, Haryanto B, Sumarta NH. Intention to donate kidney in Indonesia: the role of financial incentive, perceived risk, and altruism. MIX. 2018;8(3):463–476. doi:10.22441/mix.2018.v8i3.002
15. World Health Organization. International Report on Organ Donation and Transplantation. World Health Organization; 2022.
16. Bennett D. Pig organs head for the clinic. Nature. 2022;2022:611.
17. Dhiman R, Harsvardhan R. Organ donation: a gift of life. J Indra Gandhi Inst Med. 2021;7(2):81. doi:10.4103/2394-9031.331757
18. Khan BA, Singh T, Ng ALC, Teo RZC. Health economics of kidney replacement therapy in Singapore: taking stock and looking ahead. Ann Acad Med Singapore. 2022;51(4):236–240. doi:10.47102/annals-acadmedsg.2021494
19. Iyengar A, McCulloch M. Paediatric kidney transplantation in under-resourced regions—a panoramic view. Pediat Nephrol. 2022;37(4):745–755. doi:10.1007/s00467-021-05070-3
20. Dayal C, Davies M, Diana NE, Meyers A. Living kidney donation in a developing country. PLoS One. 2022;17(5):e0268183. doi:10.1371/journal.pone.0268183
21. Lai T-S, Hsu -C-C, Lin M-H, V-C W, Chen Y-M. Trends in the incidence and prevalence of end-stage kidney disease requiring dialysis in Taiwan: 2010–2018. J Formos Med Assoc. 2022;121:S5–S11.
22. Ashu JT, Mwangi J, Subramani S, Kaseje D, Ashuntantang G, Luyckx VA. Challenges to the right to health in sub-Saharan Africa: reflections on inequities in access to dialysis for patients with end-stage kidney failure. Int J Equity Health. 2022;21(1):1–14. doi:10.1186/s12939-022-01715-3
23. Ali A, Ahmed T, Ayub A, et al. Organ donation and transplant: the Islamic perspective. Clin Transplant. 2020;34(4):e13832. doi:10.1111/ctr.13832
24. Bekele M, Jote W, Workneh T, Worku B. Knowledge and attitudes about organ donation among patient companion at a tertiary hospital in Ethiopia. Ethiop J Health Sci. 2021;31(1):119–128. doi:10.4314/ejhs.v31i1.14
25. Huang J, Millis JM, Mao Y, Millis MA, Sang X, Zhong S. Voluntary organ donation system adapted to C hinese cultural values and social reality. Liver Transpl. 2015;21(4):419–422. doi:10.1002/lt.24069
26. Derseh BT, Dadi AF. Mortality and predictors of chronic kidney diseases (CKD) in selected dialysis centers in Addis Ababa. Ethiopia medRxiv. 2022;2022:1.
27. Mengistu YT, Ejigu AM. Global dialysis perspective: Ethiopia. Kidney360. 2022;3:1431–1434. doi:10.34067/KID.0006902021
28. Ethiopian Federal Ministry of Health. National Specialty and Sub-Specialty Service Road Map: 2020–2029 Ministry of Health. Ethiopia Addis Ababa: Ministry of Health; 2020.
29. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
30. Bauer JE. Health Behavior and Health Education: Theory, Research, and Practice. Medknow; 2004.
31. Latifi M, Pauli J, Dehghani S, Nejad MS. Application of theory of planned behavior on organ donation behavior: a systematic review. Saudi J Kidney Dis Transpl. 2021;32(5):1201. doi:10.4103/1319-2442.344739
32. Lei L, Deng J, Zhang H, Dong H, Luo Y. Level of organ donation–related knowledge and attitude and willingness toward organ donation among a group of university students in Western China. In: Transplantation Proceedings. Elsevier; 2018.
33. Bahir Dar University human resources management system. Background information of Bahir Dar University; 2022. Available from: https://hrm.bdu.edu.et/.
34. Egbi OG. Knowledge and attitude about kidney donation and transplantation among undergraduate medical students of Niger Delta University, Bayelsa, Nigeria. Nig Del Med J. 2019;3(4):11–21.
35. Uwingabiye ML, Baziga V, Chironda G, Rajeswaran L. Assessment of knowledge, attitude and perceptions regarding kidney donation among nursing students at the University of Rwanda. Int J Afr Nurs Sci. 2021;15:100317. doi:10.1016/j.ijans.2021.100317
36. Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice. John Wiley & Sons; 2015.
37. Muoneke VU, Obu DC, Uwaezuoke SN, Asiegbu UV, Anya AA, Una AF. Perspectives of clinical students toward organ donation and transplantation: a cross-sectional descriptive study in a Nigerian tertiary hospital. Int J Med Sci Public Health. 2020;25(2):112. doi:10.4103/ijmh.IJMH_14_20
38. Bekele M. Assessment of knowledge, attitude and associated factors about organ donation among medical students of SPHMMC. Ethiop Med J. 2020;2020:1.
39. Dibaba FK, Goro KK, Wolide AD, et al. Knowledge, attitude and willingness to donate organ among medical students of Jimma University, Jimma Ethiopia: cross-sectional study. BMC Public Health. 2020;20:1–7. doi:10.1186/s12889-020-08931-y
40. Alghamdi A, Alsaleh AA, Alfozan OA, et al. Awareness, attitude, and beliefs regarding organ donation among the General Public in Saudi Arabia. Int J Gen Med. 2023;16:4973–4989. doi:10.2147/IJGM.S434589
41. Godin G, Kok G. The theory of planned behavior: a review of its applications to health-related behaviors. Am J Health Promot. 1996;11(2):87–98. doi:10.4278/0890-1171-11.2.87
42. Sault K. Understanding organ donation attitudes and behaviour from a theory of planned behaviour perspective; 2011.
43. Zeng M, Li H, Song X, Jiang J, Chen Y. Factors Associated with Willingness toward Organ Donation in China: a Nationwide Cross-Sectional Analysis Using a Social–Ecological Framework. In: Healthcare. MDPI; 2023.
44. Ghaffari M, Rakhshanderou S, Najafizadeh K, Ramezankhani A, Latifi M. Determinants of medical students for intention to organ donation: application of theory of planned behavior. Saudi J Kidney Dis Transpl. 2019;30(6):1375–1380. doi:10.4103/1319-2442.275481
45. Ajzen I, Joyce N, Sheikh S, Cote NG. Knowledge and the prediction of behavior: the role of information accuracy in the theory of planned behavior. Basic Appl Soc Psych. 2011;33(2):101–117. doi:10.1080/01973533.2011.568834
46. Sharaan R, Alsulami S, Arab R, et al. Knowledge, attitude, and willingness toward kidney donation among health sciences students at king Saud Bin Abdulaziz University. Front Public Health. 2021;9:667582. doi:10.3389/fpubh.2021.667582
47. Ghaffari M, Latifi M, Rocheleau C, Najafizadeh K, Rakhshanderou S, Ramezankhani A. Using the Theory of Planned Behavior Framework for Designing Interventions Related to Organ Donation. Springer; 2018.
48. Kim EA, Choi SE. Structural equation modeling on living and brain death organ donation intention in nursing students. J Korean Acad Nurs. 2015;45(6):802–811. doi:10.4040/jkan.2015.45.6.802
49. Rochelle TL, Ng JS. Examining behavioural intention towards organ donation in Hong Kong. J Health Psychol. 2022;2022:13591053221092857.
50. Yun D, Park HS. Culture and the theory of planned behaviour: organ donation intentions in Americans and Koreans. J Pac Rim Psychol. 2010;4(2):130–137. doi:10.1375/prp.4.2.130
51. Umair S, Ho JA, Basha NK, Ng SS-I, Waqas U. Understanding the attitudes and factors influencing organ donation decisions among university students in Pakistan: a qualitative study. Human Soc Sci Rev. 2020;8(1):52–59. doi:10.18510/hssr.2020.818
52. Wolide AD, Kabaye KG, Dibaba FK, et al. Do health sciences students have the appropriate knowledge and attitude to advance organ donation in Ethiopia? Cross-sectional study. Transpl Res Risk Manag. 2020;12:1. doi:10.2147/TRRM.S226492
53. Ferguson E, Murray C, O’Carroll RE. Blood and organ donation: health impact, prevalence, correlates, and interventions. Psychol Health. 2019;34(9):1073–1104. doi:10.1080/08870446.2019.1603385
54. Dong H, Xu X, Zhang J, et al. Survey of current status and influencing factors analysis of attitude and willingness of ICU nurses towards organ donation in Chongqing. Organ Transplant. 2019;2019:61.
55. Hyde MK, Knowles SR, White KM. Donating blood and organs: using an extended theory of planned behavior perspective to identify similarities and differences in individual motivations to donate. Health Educ Res. 2013;28(6):1092–1104. doi:10.1093/her/cyt078
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychosocial Determinants of Intention to Use Dual Contraception Among Thai Female Students: Integrating the Health Belief Model and Theory of Planned Behavior
Suntonpiyapan A, Sarnkhaowkhom C, Santre S
International Journal of Women's Health 2026, 18:605370
Published Date: 12 June 2026