Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
“Intensive-Home-Rehabilitation” Intervention for Older Persons: A Follow-Up Study of Team Members’ Perceptions
Authors Söderman M ![]() , Bondesson A, Pettersson T, Gustafsson LK
, Bondesson A, Pettersson T, Gustafsson LK ![]()
Received 23 February 2023
Accepted for publication 2 June 2023
Published 2 August 2023 Volume 2023:16 Pages 2207—2216
DOI https://doi.org/10.2147/JMDH.S409879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mirkka Söderman, Anna Bondesson, Tina Pettersson, Lena-Karin Gustafsson
Division of Caring Science, School of Health, Care and Social Welfare, Mälardalen University, Eskilstuna, Sweden
Correspondence: Mirkka Söderman, School of Health, Care and Social Welfare, Box 325, Eskilstuna, 631 05, Sweden, Tel +46 16153433, Email [email protected]
Background: Reablement as a concept includes a health-promoting perspective with the goal of strengthening health and the ability to perform and participate in daily activities, a broader perspective than in general home care and rehabilitation. Reablement interventions have shown to be both more effective and to a greater extent improve the function and health-related quality of life of older persons when compared to traditional home-based care. Success factors for intensive-home-rehabilitation (IHR), an intervention based on the reablement concept, have been described earlier; however, there is a lack of knowledge about why some persons do not recover despite receiving IHR.
Aim: The aim was to shed light on the older persons’ conditions during IHR from the perspective of the rehabilitation team members and to describe obstacles to recovery.
Methods: Qualitative analysis of health and care records of persons (65+) who received IHR (n=19) performed by an interprofessional team.
Results: The analysis revealed various problematic situations, dilemmas, that occurred in the older persons’ lives during IHR, as well as their consequences and the strategies employed by the older persons as a result. IHR aspects perceived as successful by the older persons also emerged, as well as differences in experiences of the physical and mental aspects of the IHR. Analysis also revealed reasons why the IHR might be experienced as broadly successful.
Conclusion: The older persons seemed to be satisfied with IHR and achieved their goals; however, some seemed to need more time to reach their goals. Background factors such as having additional diagnoses and living alone might affect the rehabilitation process.
Implication for Practice: The study provides knowledge regarding the importance of IHR for the recovery process for the increasing numbers of older persons, which might also be useful in other patient groups requiring otherwise long-term rehabilitation and recovery such as after covid-19 infection.
Keywords: home-based care, intensive-home-rehabilitation, interprofessional team, older persons, reablement, recovery, rehabilitation process
Introduction
Older persons need good conditions to be able to live as long as possible in their homes and have the opportunity to have an active life with preserved independence and influence over their own everyday lives.1 This includes independent living with safe conditions and having an active and meaningful existence with others.2 Furthermore, the right to life with dignity and well-being,3 which is in line with the WHO’s definition of healthy aging.4 To this purpose the development of appropriate care interventions that consider individual- and contextual obstacles to rehabilitation is important for qualitative, municipal and home-based care.5
A team-based model for home-based care seems to be the best way to meet complex biomedical- and psychosocial needs in the home.6 This is in line with the fact that the rehabilitation of older persons requires an overall interprofessional strategy,7 and collaboration between all professionals involved in the care of the home-dwelling older persons.8 Reablement is then a term used in international research9–11 for the rehabilitation that is performed in ordinary housing or assisted living, aimed at regaining independence, and defined by Social Care Institute for Excellence12 as: “services for seniors with physical or mental disabilities that help them adapt to their condition by learning or re-learning the skills needed to function in everyday life”. The term can also be related to the Danish term “hverdagsrehabilitering” or the Swedish concept of everyday rehabilitation, referring to support and help for older persons to recover the ability to perform and participate in daily activities. This type of rehabilitation is interprofessional, intensive and time limited, and the possibility of receiving this short-term targeted rehabilitation has increased. Evaluations of short-term targeted rehabilitation have shown improved health related quality of life10 and positive effects on the physical functions of older persons,13 as well as lower costs for the municipality in the form of a reduction in granted home care hours10,13 and increased job satisfaction among employees.10 There are also studies showing that mortality is reduced in older persons receiving reablement interventions,14 that those at risk of functional decline can be identified at an earlier stage,15 and that reablement seems to be more effective than traditional home-based care for older persons with disabilities.16 Although there is good evidence supporting the effectiveness of reablement for older persons living in their own homes, it can be seen as a doubt that the patient groups in previous studies regarding reablement have been heterogeneous and therefore these results are difficult to apply to specific interventions.17
The current study is a follow-up study on the project “intensive-home-rehabilitation” (IHR) carried out in 2015–2019, an intervention based on the term reablement12 and performed as a randomized controlled trial (RCT) including qualitative studies based on samples from participants in the RCT.18–22 The project aimed at developing the work of an integrated interprofessional team and designing new working methods offering a cohesive care and nursing system for older persons (65+) in need of rehabilitation in ordinary housing. The intention of the project was to reduce care efforts, promote self-care and safe situations for home-dwelling older persons. This may in turn delay the need for additional care efforts such as expanded home care, nursing home, or hospital care. A more detailed description of the project can be found in previous publications from the project. Success factors for IHR found in the project were the caregiver being motivating, creating a positive atmosphere, feeling the common rhythm, and doing something beyond what is expected in the effort to support the person.21 Moreover, the older person’s reablement process was strengthened through the cooperation between- and efforts from different professional groups,20 the professionals experienced that the goal-oriented teamwork gave the older persons a sense of calm and of not being abandoned, resulting in less need of care. It even appeared that older persons could achieve autonomy through the IHR, although not always to the same extent as before.19
In summary, the older persons appreciated IHR, which included rehabilitation goals related to their relationships with relatives and their lives in a larger context. However, knowledge is still limited concerning the impact of IHR and reablement, and especially scarce regarding obstacles to recovery. Such knowledge is needed as a foundation when developing relevant support for home-dwelling older persons in need of rehabilitation, and to inform how such programmes can be structured and optimized to meet the needs of older persons. Therefore, this study aimed to shed light on the older persons’ conditions during IHR from the perspective of the rehabilitation team members, and to describe obstacles for recovery.
Materials and Methods
A qualitative retrospective descriptive approach was chosen as the method in this study, and the study was conducted via health and care records. The request for participation in the follow-up study and consent from older persons who received IHR to collection of their health and care records occurred from June 2021 until October 2021. The selection process was performed with support from Eskilstuna Municipality’s care- and welfare administration.
Participants in the Intervention Study
In the start phase of the RCT, a new interprofessional IHR-team supposed to work with a short-term goal-directed reablement of older persons were trained, and the training consisted of four weeks full-time studies regarding a new way to rehabilitate older persons who after a time in hospital need home care. The IHR-team consisted of social workers, assistant nurses, physiotherapists, occupational therapists, and registered nurses, specially trained and focused on rehabilitation. Members of the team could visit the older persons several times a day to work on the rehabilitation together with them. The older persons met the same team members as far as possible throughout the project. Each older person had twice as much time with a contact person compared to the usual home care service.
The sample for the current study, health and care records, was chosen to offer a reasonable basis to describe the situation of older persons (65+) receiving IHR performed by an interprofessional team in a middle-size municipality’s care- and welfare administration in Sweden. The initial exclusion criteria for receiving the IHR during the RCT based intervention study were severe cognitive dysfunction, life-threatening illness, severe mental illness, or other illness / disability that made the older persons unable to express their will. The IHR-team supported the researchers in giving oral information about the study and distributing information letters and consent forms. After exclusion of persons who died after the IHR implementation project, and persons who were no longer able to express their consent, a total of 19 older persons gave consent to participate in the current study, collection of their health and care records, and publication of their anonymized responses. Data were collected by the IHR-team, by extracting the health and care records from the Cambio VIVA documentation program. Cambio VIVA is an operating system for handling, documentation, and decision support to coordinate activities within social services, care, and social care.23 The records were deidentified and coded by the IHR-team and transferred to an Excel file by the research team.
Data Analysis
Data regarding older persons who received IHR, such as age, marital status, diagnosis, granted IHR, were extracted from health and care records and compiled. The other data material in the current study was suitable for more in-depth qualitative analysis methods because of the richness of text data. A qualitative approach to the problem may also provide the details and depth required to fully understand the consequences. This study’s new data in the form of the collection of health and care records was processed via deductive content analysis inspired by Elo and Kyngäs’ method description.24 The health and care records were read several times for a better overall understanding and to allow immersion in the text. Subsequently, a structured categorization matrix was prepared based on previous studies in the field and which constituted a deductive framework for the analysis (Box 1).
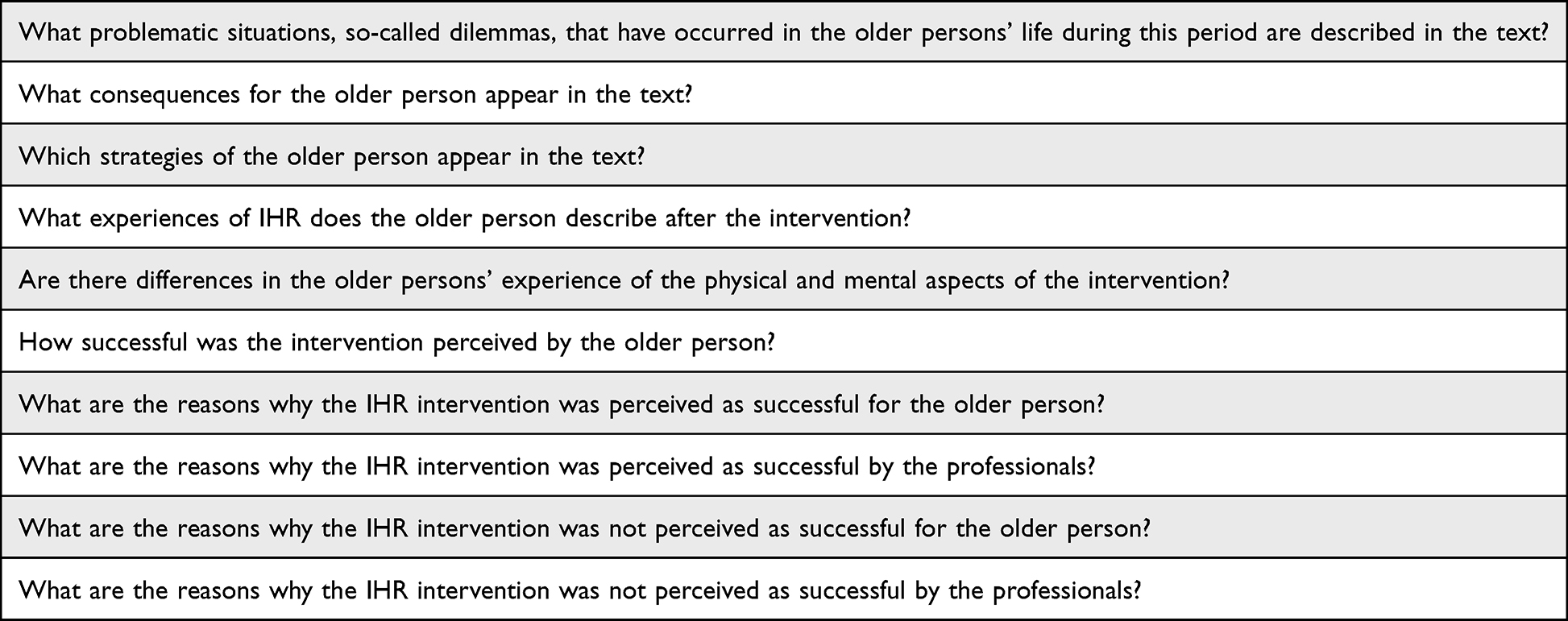 |
Box 1 Deductive Framework for the Analysis Used in Data Extraction from Care Records |
Next, the contents of the text were examined, and the data were coded by extracting the data corresponding to the categorization matrix from the text. Thereafter, data were analysed both horizontally and vertically in accordance with Vehko et al,25 ie, question by question for everyone included and each patient / case separately. The codes were transferred to a code sheet and coded into categories according to each aspect with different headings (Table 1). Furthermore, the analytical framework was validated through discussions between the authors, and credibility was achieved through discussions between all authors throughout the analysis process via research team meetings.
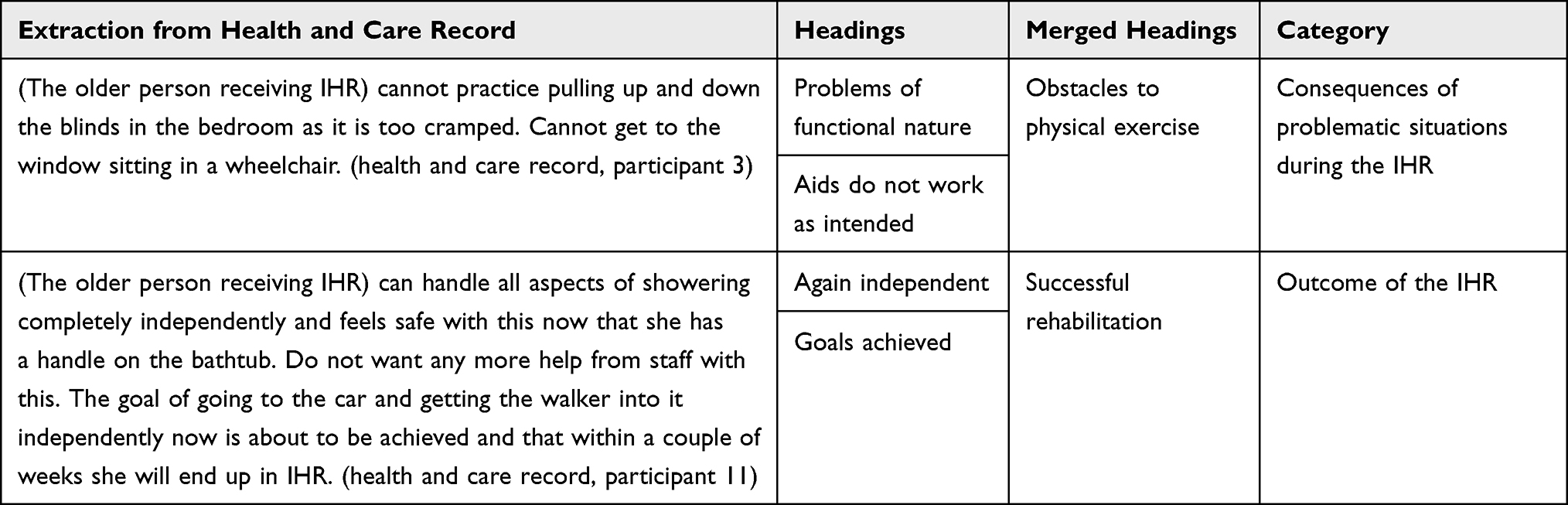 |
Table 1 An Example of the Implementation of the Content Analysis |
Ethics
The project was approved by the Regional Ethics Committee in Uppsala, Sweden (D. nr 2021–01500). Furthermore, the study was carried out in accordance with the World Medical Association Declaration of Helsinki26 and informed consent was obtained from all subjects along with The Swedish Data Protection Authority (DPA) GDPR (2016/ 679). The invited participants were informed that participation was voluntary, and that the information collected would be handled in such a way as to ensure that only authorized persons have access to it.
Results
Demographics of the Older Persons Who Received IHR
A majority of the older persons included in this follow-up study were women (n=15 women v. n=4 men), the average age was 84.8 years, and the majority were living alone without a partner (n=15/19). It turned out that a majority of the older persons were included in the IHR due to an orthopaedic diagnosis (n=12/19) and had at least one additional medical diagnosis (n=15/19) in addition to the diagnosis for which they received the IHR. However, only two of the diagnoses (osteoarthritis n=3, rheumatism n=3) affected the older persons’ spatial ability in a larger sense. The number of hours granted for IHR differed both between women (148 hours) and men (97 hours), and within those groups. On average, women had more IHR granted hours. However, almost all of them, except for one woman, lived alone (n = 14) and could not receive help from a close relative concerning daily life activities. It also appeared that, both divided between the sexes and with all in common based on the number of IHR granted hours, some of the older persons needed much support and others apparently needed less (24 hours vs 405 hours, n = 19) (Table 2).
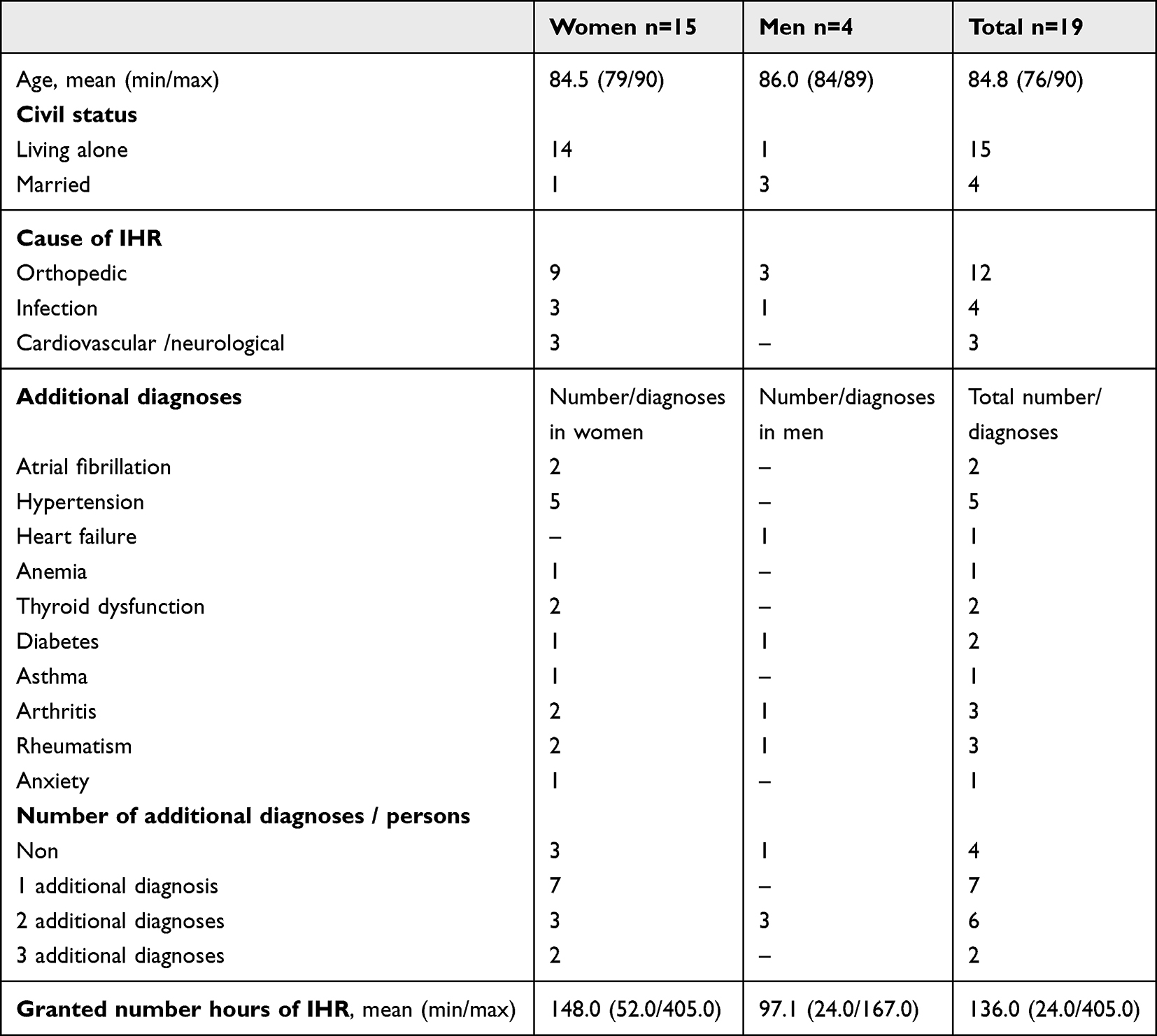 |
Table 2 Description of Background Conditions of the Persons Who Received Intensive Home Rehabilitation (IHR) n=19 |
Results of the Content Analysis
The presentation of the results is based on the four categories identified in the analysis, and in relation to the purpose of the study; “IHR as an answer to their needs”, “Consequences of problematic situations during the IHR”, “Strategies used during the IHR”, and “Outcome of the IHR”.
IHR as an Answer to Their Needs
The IHR-team members expressed, according to the health and care records, that the older persons goals for IHR were achieved. The older persons in turn expressed, according to the health and care records, that they were satisfied with IHR, and that the team gave them an experience of security and support to regain autonomy. Rehabilitation with IHR was appreciated, older persons expressed both joy and satisfaction, and individual conversations were appreciated. The older persons expressed that there was a need for social interaction and the thought that the IHR period would end gave rise to feelings of sadness and emptiness. They were also concerned about missing support and the opportunity of having someone who came to have regular conversations.
…it can be sad not to meet the team in the future, she is very happy with her rehabilitation together with IHR (health and care record, participant 1), … she is very happy with her time in IHR, that she has received support to become independent again and that she felt very safe with the team. She also expresses that it has been good for her to have individual conversations… feels stressed because the end of IHR is approaching (health and care record, participant 6).
The physical and mental experiences of IHR seemed to reinforce each other. This was shown when the need for social interaction increased, when they became stronger or when they felt safe in the activity and mastered the exercises, they experienced less anxiety. When they experienced the training as successful, they dared to take on more and asked for less help or refrained some help and managed the situation on their own with success.
…no longer experiences stair climbing as a problem and dares to go up the stairs herself, he ends up doing the stair training (health and care record, participant 2), …felt that she could manage on her own and did not need any help at night (health and care record, participant 9).
Consequences of Problematic Situations During the IHR
The identified problematic situations in the older persons’ lives during the IHR period, according to the health and care records, were both of a functional nature such as dressing on their own or that aids did not work as intended, and of a physical nature such as pain, loss of appetite and unsteadiness during movement. Consequences could then be having difficulty with movement both with and without aids or that aids limited mobility, and that IHR was experienced as too energy-intensive, or the pain limited both mobility and independence in the use of aids.
… cannot practice pulling up and down the blind in the bedroom as it is too crowded. Cannot get to the window sitting in a wheelchair (health and care record, participant 3), … states that she has a lot of pain in her arms / shoulders when she drives the current wheelchair and that it takes all her energy (health and care record, participant 10).
The problematic situations in older persons’ lives, seen in the health and care records, could also be of an emotional nature such as anxiety about the future, fear of falling, depressive symptoms, and experiencing loneliness. Consequences of this could be that the older persons due to fear of falling did not get out of bed at night or needed to sleep during the day due to medication. Activities were not performed since the older persons did not have the required ability to concentrate.
… states that she is still tired after everything she has been through and that she is taking diuretics. Needs to get up and pee at night (health and care record, participant 14), …states that she has not started using her left hand yet for this purpose as it requires great concentration to cope with this (health and care record, participant 12).
Strategies Used During the IHR
The older persons seemed, according to the health and care records, to use several strategies to manage their lives during the IHR, such as performing decided activities and training, as well as using the prescribed aids. They also took the initiative for self-care, for outdoor activities to improve physical fitness and sleep, or for both housing adaptation and aids. The older persons also prioritized activities to save their energy, to be able to handle anxiety attacks without medication, and to establish social contacts to reduce loneliness.
…states that she walks with the walker several times a day to the guest house to keep going on (health and care record, participant 9), …refused to take a shower in the morning to save energy for the walk, which she was motivated to perform (health and care record, participant 2), …got sad for a moment when she looked out and saw the nice weather. She longs to go out, she said. Feeling trapped. She would call and talk to a friend (health and care record, participant 3).
Outcome of the IHR
The health and care records revealed that the older persons expressed the IHR as successful when they managed to achieve their goals and could be more independent again in their everyday lives. Records also revealed that the IHR team conveyed a sense of security while the older persons performed their training. The possibility to talk with the IHR team seemed to be appreciated, and the team visits were experienced as stress reducing and increased joy in older persons’ everyday lives. From the professionals’ perspective, the IHR was successful when the older persons seemed satisfied with it, trained towards their goals, made some progress in the training, and performed the training and everyday activities independently. They also judged it successful when the older persons were perceived as being safe with the aids that had been introduced to them and their physical ailments seemed to have been alleviated.
…expresses no concern at the (training) moment and says that she probably just needs to try with someone to feel that she can do it (health and care record, participant 1), …moves between the bed and wheelchair independently according to the care and nursing plan. Follows up and completes goals and measures in the care and nursing plan (health and care record, participant 8), …has got two handles on the wall inside the shower, via the home adaptation…is very pleased that the adaptation has been completed (health and care record, participant 13).
The IHR seemed to be, according to the health and care records, experienced as less successful by older persons when information about changes in visit frequency was lacking or when visiting hours were not to their satisfaction. The IHR was also less successful when they felt they needed more time to reach their goals or when the goals could not be achieved due to physical problems, such as pain and unsteadiness when moving, which made it difficult for them to practice. The professionals experienced the IHR as less successful when the older persons did not understand how the IHR-team worked or when they were not receptive to information about IHR. This made the rehabilitation troublesome since the older persons did not perform the training either with IHR or on their own, nor did they use aids. The professionals also experienced that physical ailment limited the older persons training during the IHR.
…did not understand how and why the IHR-team works the way we do, she says that she never had IHR work explained when she chose us at the hospital, only that she was given the opportunity to be part of a project… During the visit, she refuses to try moving in / out of the bathtub via a bathing board (health and care record, participant 4), …according to the training programme…states that she did not exercise due to back pain (health and care record, participant 15), …states that she, when visiting the toilet, managed the hygiene independently, but that her strength is affected by the amount of pain she is in (health and care record, participant 16).
Synthesis of the Qualitative Analysis
In the overall understanding, based on health and care records, differences were seen in the experience of the physical and mental aspects of the IHR among the older persons who received IHR. During the IHR, there were various problematic situations, dilemmas, that had consequences for the lives of the older persons. Based on these experiences, the older persons used certain strategies in specific situations. These strategies affected the older persons’ experiences of IHR, ie, whether the outcome of the IHR was perceived as more or less successful. These core categories of the meaning of IHR for older persons and how the categories are interrelated are illustrated in Figure 1.
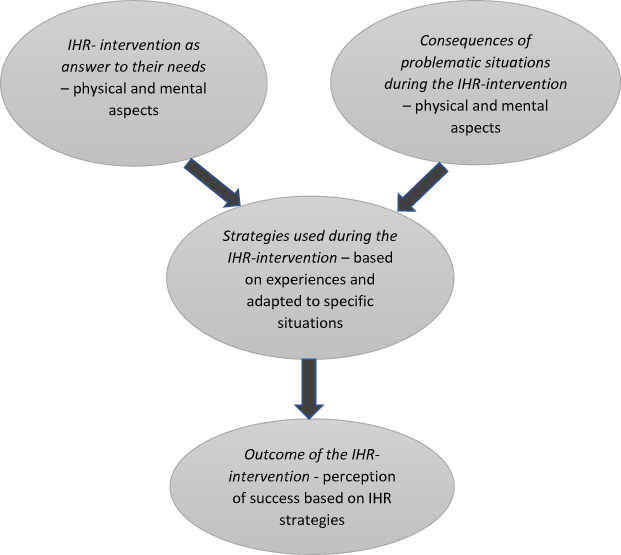 |
Figure 1 Illustration of the core categories concerning the IHR for older persons and how the categories are interrelated. |
Discussion
In this qualitative study of IHR-team members’ perceptions of the IHR for older persons’ obstacles for recovery, it appeared that the older persons seemed to be satisfied with IHR and that they achieved their goals to perform and participate in daily activities. However, some of the older persons seemed to need more time to reach their goals due to background factors such as additional diagnoses, mental- and physical ailments, and living alone.
Even if a majority of the older persons, based on the health and care records, achieved the set goals during the IHR, some of them faced various dilemmas during the rehabilitation period. The findings showed a dilemma in terms of priority for older persons between IHR activities or saving energy to focus on such things as establishing social contacts that gave them a sense of well-being. Both choices are intended to support health in a long-term perspective, but the proposed IHR activities may not have provided a sense of well-being in the short term and thus often disappeared as a choice. Some of the older persons seemed to need more time to be able to achieve their goals. Others could not achieve their goals as there seemed to be communicative aspects that hindered, sometimes caused by the older person’s cognitive ability to perceive information. In those cases, the older persons did not perform exercises either with the IHR-team or on their own, nor did they use the prescribed aids. However, not following providers’ instructions (for exercise, use of equipment) could also be a cue that interventions need to be adjusted since non-compliance with exercise regimes is universal and not all equipment works well in every context, regardless of whether the person has cognitive impairments or not. The results from the current study showed that older persons’ physical ailments, such as pain and unsteadiness, led to fear of falling, which might also have complicated the training in the IHR.
A majority of the older persons were included in the IHR due to an orthopaedic diagnosis. It seems to be a correct assessment regarding potential success in the rehabilitation process as even previous research shows that this diagnosis group benefits most from this type of intervention.10 That might be because the recovery processes for orthopaedic diagnosis are more linear causal compared to other diagnoses such as cardiovascular diagnosis. Most older persons had at least one additional diagnosis, which is also consistent with previous research.13,16 Since the disease-related obstacles to IHR have such a large place in the health and care records, one may ask whether a medical assessment of, for example, a nurse alongside an assistance officer would be preferable before deciding on inclusion in IHR under the auspices of the municipality. This might determine that those who are assessed to have the most potential benefits and opportunities from the IHR can be offered this type of effort, and those in the need of an adjusted versions of the IHR, eg, persons with cognitive dysfunction, can be offered such intervention. Although we know that many people who receive home care have dementia, cognitive impairments, they do not receive this type of intervention as also seen in previous research, where people with cognitive disorders and dementia were ineligible for reablement interventions and not included.10,13 Researchers are, however, beginning to evaluate reablement programs that include consideration of cognitive issues including dementia27 but still a major knowledge gap exists in this specific area.
Most of the older persons lived alone, which might have affected their strength and energy since they couldn´t get help from a cohabitant in their everyday life, thus complicating and extending the time for implementation of the training programme. Moreover, these older persons might have had an increased need for support from IHR. The degree of assistance was not considered upon inclusion in the present study, which can be related to, for example, the fact that older persons who needed more than 15 hours / week of home care were not included in previous research.28 It is therefore necessary to consider whether this type of intervention is suitable for everyone or intended for a specific group of older persons.
The older persons in our study were on average older than participants in previous studies,10,13,16 except for one study conducted in Norway.15 One can hypothesize that a higher age might affect the ability to achieve IHR goals due to age-related factors affecting stamina and strength, although the results of this study do not indicate this. Therefore, the IHR should also be offered to older persons of higher age, given that most of the older persons in the current study were satisfied and achieved their goals.
Strengths and Limitations
All older persons participating in the IHR-project with RCT, were invited to participate in this study as well. Of those who accepted the invitation and gave consent to collection of their health and care records, 4 persons of 19 were men, which is also consistent with the proportion of the IHR project in total. Although the intention was to even out the imbalance in the distribution between the sexes, the same gender distribution can also be seen in previous research in this area with the same age range as the current study. In addition, at the population level, there are more women than men aged 65+ who live in ordinary housing in Sweden. Men also rarely live alone without someone taking care of them, which could also be seen in this study.
The qualitative, deductive content analysis was found to be a suitable method to use because it provided an opportunity to operationalize the analysis structure based on knowledge from the RCT. Moreover, it enabled finding out about variations in descriptions of the situations during IHR and acted to reduce preconceptions, influences, and interpretations. Since the results were based on the IHR-team documentation of their observations and discussions with older persons, it is not possible to say with certainty whether the health and social care professionals' interpretation may have influenced the description of the different situations, which is a weakness in this study. What, however, strengthens the data is that the professionals’ documentation in the health and care records is consistent between the different professionals who cared for older persons. In addition, the results are strengthened by the fact that the data were analysed both horizontally and vertically, which confirmed that the results were consistent.
Conclusions and Relevance to Clinical Practice
This study focuses on the dilemmas older persons might have in the context of short-term goal-directed home reablement, the IHR. According to the health and care records, some of the older persons seemed to experience different types of dilemmas during the IHR and needed more time to achieve their goals. The dilemmas were related to additional diagnoses, living alone without the support of a partner in daily activities, and having communicative impairments. These dilemmas might affect the rehabilitation process and make the prognosis more uncertain. The present study gives an indication that there are specific needs for adaptation in intensive home-based rehabilitation depending on diagnosis and life situation, even if further research is needed to draw conclusions. These results are relevant to policy makers and the municipal health and social care administration when designing and improving strategies for preventive care and rehabilitation in home care for older persons. The study also provides important knowledge regarding the importance of IHR for older persons regarding reablement and might be useful in other groups otherwise requiring long-term rehabilitation and recovery such as after covid-19 infection.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Walker A, Maltby T. Active ageing: a strategic policy solution to demographic ageing in the European Union. Int J Soc Welf. 2012;21:S117–S30. doi:10.1111/j.1468-2397.2012.00871.x
2. Goverment office of Sweden. SFS 2001:453, 5 kap § 4. Social Services Act (In Swedish: socialtjänstlag). Available from: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453.
3. Goverment office of Sweden. SOU 2008:51 Dignified life in elderly care (In Swedish: SOU 2008:51 Värdigt liv i äldreomsorg). Available from: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2008/05/sou-200851/.
4. WHO. WHO’s work on the UN Decade of Healthy Ageing (2021–2030). WHO; 2020. Available from: https://www.who.int/initiatives/decade-of-healthy-ageing.
5. Gustafsson LK, Mattsson K, Dubbelman K, Snöljung Å. Aspects of nursing with evidence‐base when nursing frail older adults: a phenomenographic analysis of interviews with nurses in municipal care. Scand J Caring Sci. 2014;28(4):793–801. doi:10.1111/scs.12112
6. Reckrey JM, Soriano TA, Hernandez CR, et al. The team approach to home‐based primary care: restructuring care to meet individual, program, and system needs. J Am Geriatr Soc. 2015;63(2):358–364. doi:10.1111/jgs.13196
7. Hjelle KM, Alvsvåg H, Førland O. The relatives’ voice: how do relatives experience participation in reablement? A qualitative study. J Multidiscip Healthc. 2017;10:1. doi:10.2147/JMDH.S122385
8. Janssen BM, Snoeren MW, Van Regenmortel T, Abma TA. Working towards integrated community care for older people: empowering organisational features from a professional perspective. Health Policy (New York). 2015;119(1):1–8. doi:10.1016/j.healthpol.2014.09.016
9. Kjerstad E, Tuntland HK. Reablement in community-dwelling older adults: a cost-effectiveness analysis alongside a randomized controlled trial. Health Econ Rev. 2016;6(1):1–10. doi:10.1186/s13561-016-0092-8
10. Tessier A, Beaulieu M-D, McGinn CA, Latulippe R. Effectiveness of Reablement: a Systematic Review. Healthc Policy. 2016;11(4):49–59.
11. Wilde A, Glendinning C. ‘If they’re helping me then how can I be independent?’The perceptions and experience of users of home‐care re‐ablement services. Health Soc Care Community. 2012;20(6):583–590. doi:10.1111/j.1365-2524.2012.01072.x
12. Social Care Institute for Excellence (SCIE). SCIE Guide 49: Maximizing the Potential of Reablement. London: SCIE; 2013.
13. Sims-Gould J, Tong CE, Wallis-Mayer L, Ashe MC. Reablement, Reactivation, Rehabilitation and Restorative Interventions With Older Adults in Receipt of Home Care: a Systematic Review. J Am Med Dir Assoc. 2017;18(8):653–663. doi:10.1016/j.jamda.2016.12.070
14. Anthun KS, Lillefjell M, Anthun KS. Reablement in a small municipality, a survival analysis. BMC Health Serv Res. 2021;21(1):877. doi:10.1186/s12913-021-06910-6
15. Meisingset I, Bjerke J, Taraldsen K, et al. Patient characteristics and outcome in three different working models of home-based rehabilitation: a longitudinal observational study in primary health care in Norway. BMC Health Serv Res. 2021;21(1):887. doi:10.1186/s12913-021-06914-2
16. Langeland E, Tuntland H, Folkestad B, Førland O, Jacobsen FF, Kjeken I. A multicenter investigation of reablement in Norway: a clinical controlled trial. BMC Geriatr. 2019;19(1):29. doi:10.1186/s12877-019-1038-x
17. Legg L, Gladman J, Drummond A, Davidson A. A systematic review of the evidence on home care reablement services. Clin Rehabil. 2016;30(8):741–749. doi:10.1177/0269215515603220
18. Gustafsson L, Östlund G, Elfström M, Anbacken E-M, Zander V. IHR PROJECT RESEARCH REPORT (In Swedish: IHR- PROJEKTET 330 AQ8 FORSKNINGSRAPPORT); 2020. Available from: https://www.samhallskontraktet.se/download/18.74aa99c17471d6226f7472/1600012114179/Rapport%20IHR%20200826.pdf.
19. Östlund G, Zander V, Elfström ML, Gustavsson L-K, Anbäcken E-M. Older adults’ experiences of a reablement process. “To be treated like an adult, and ask for what I want and how I want it”. Educ Gerontol. 2019;45(8):519–529. doi:10.1080/03601277.2019.1666525
20. Gustafsson LK, Anbäcken EM, Elfström ML, Zander V, Östlund G. Working with short-term goal-directed reablement with older adults: strengthened by a collaborative approach. Nordic j Nursing Res. 2019;39(4):178–185. doi:10.1177/2057158519850974
21. Gustafsson LK, Östlund G, Zander V, Elfström ML, Anbäcken EM. ‘Best fit’ caring skills of an interprofessional team in short‐term goal‐directed reablement: older adults’ perceptions. Scand J Caring Sci. 2019;33(2):498–506. doi:10.1111/scs.12650
22. Hochwälder J, Gustafsson L-K, Östlund G, Zander V, Elfström ML. Psychometric evaluation of the subjective well-being measure GP-CORE in a group of older adults in Sweden. BMC Geriatr. 2022;22(1):913. doi:10.1186/s12877-022-03625-z
23. Cambio. Cambio VIVA. Available from: https://www.cambiogroup.com/our-solutions/cambio-viva/.
24. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
25. Vehko T, Jolanki O, Aalto A-M, Sinervo T. How do health care workers manage a patient with multiple care needs from both health and social care services?–A vignette study. Int j Care Coordination. 2018;21(1–2):5–14. doi:10.1177/2053434517744070
26. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects 2014. Available from: http://www.wma.net/en/30publications/10policies/b3/.
27. Jeon Y-H, Clemson L, Naismith SL, et al. Improving the social health of community-dwelling older people living with dementia through a reablement program. Int Psychogeriatr. 2018;30(6):915–920. doi:10.1017/S1041610217001533
28. Lewin G, Allan J, Patterson C, Knuiman M, Boldy D, Hendrie D. A comparison of the home-care and healthcare service use and costs of older Australians randomised to receive a restorative or a conventional home-care service. Health Soc Care Community. 2014;22(3):328–336. doi:10.1111/hsc.12092
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.