Back to Journals » Infection and Drug Resistance » Volume 16
Intensive Care Unit Sluice Room Sinks as Reservoirs and Sources of Potential Transmission of Carbapenem-Resistant Bacteria in a South African Tertiary Care Hospital
Authors Dheda KR, Centner CM, Wilson L, Pooran A, Grimwood S, Ghebrekristos YT, Oelofse S, Joubert IA, Esmail A, Tomasicchio M ![]()
Received 24 April 2023
Accepted for publication 25 July 2023
Published 21 August 2023 Volume 2023:16 Pages 5427—5432
DOI https://doi.org/10.2147/IDR.S418620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Khelan R Dheda,1 Chad M Centner,2 Lindsay Wilson,3,4 Anil Pooran,3,4 Shireen Grimwood,2 Yonas T Ghebrekristos,2 Suzette Oelofse,3,4 Ivan A Joubert,5 Aliasgar Esmail,3,4 Michele Tomasicchio3,4
1Department of Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa; 2Division of Medical Microbiology, National Health Laboratory Services (NHLS)/Groote Schuur Hospital, Microbiology, University of Cape Town, Cape Town, South Africa; 3Division of Pulmonology, Department of Medicine, Centre for Lung Infection and Immunity, University of Cape Town and UCT Lung Institute, Cape Town, South Africa; 4South African MRC/UCT Centre for the Study of Antimicrobial Resistance, University of Cape Town, Cape Town, South Africa; 5Division of Critical Care, Department of Anaesthesia and Perioperative Medicine, University of Cape Town, Cape Town, South Africa
Correspondence: Michele Tomasicchio, Division of Pulmonology, Department of Medicine, Centre for Lung Infection and Immunity, University of Cape Town and UCT Lung Institute, Cape Town, South Africa, Tel +27 21 650 4331, Fax +27 21 650 3824, Email [email protected]
Purpose: Carbapenem-resistant bacteria (CRB) pose a major health risk to patients in intensive care units (ICU) across African hospitals. There are hardly any data about the role of hospital sinks as reservoirs of CRB in resource-poor African settings. Furthermore, the specific within-sink location of the highest concentration of pathogens and the role of splash back as a transmission mechanism remains poorly clarified.
Methods: We swabbed ICU sluice room sinks in a tertiary hospital in Cape Town, South Africa. Swabs were taken from four different parts of the sluice room sinks (tap-opening, trap, below the trap, and u-bend). Dilutions were prepared and plated on carbapenem-infused agar. Colonies were identified and drug resistance profiles were determined using a biochemical analyser. To evaluate the potential transmission from the sink, similar plates were placed at fixed distances from the sink when the tap was turned on and off.
Results: CRB were isolated from the trap, water interface below the trap, and the u-bend (the latter harboured the highest density of CRB species). Five CRB, resistant to at least 7 antibiotic classes, were isolated including Pseudomonas, Klebsiella, Citrobacter, Serratia, and Providencia. CRB could be cultured from droplets that fell on agar-containing plates placed at a varying distance from the trap.
Conclusion: There is a higher density of CRB in the u-bend of ICU sluice room sinks which can act as a potential source of transmission. The data inform targeted CRB transmission-interruption strategies in resource-poor settings.
Keywords: carbapenem-resistant bacteria, multi drug resistant bacteria, sluice room sink, intensive care units, antimicrobial resistance
Introduction
Antimicrobial resistance is considered by the WHO as one of the top ten public health challenges facing humankind in the 21st century.1 Nosocomial infections involving highly drug-resistant or pan drug-resistant bacteria are now common globally.2–8 Outbreaks occur frequently, mortality is higher in affected persons, and the outcomes are worse in immunocompromised patients.2 Interrupting transmission of drug-resistant pathogens is a priority.
However, the reservoirs and transmission linkages involving hospital-based drug-resistant bacteria are only partially understood. Several mechanisms and processes have been implicated; in particular, hospital sinks have been singled out as harbouring drug-resistant bacteria via a biofilm mechanism (reviewed in9). Indeed, several global reports have documented sinks being reservoirs of pan-resistant organisms.10–12 However, there is a paucity of data regarding the role of hospital sinks as reservoirs for drug-resistant bacteria in resource-poor African settings. There are hardly any data about the specific location within sinks where drug-resistant bacteria reside. This information is critical for implementing transmission interrupting interventions. Finally, whether sink-based reservoirs of drug-resistant pathogens can serve as sentinels for onward transmission remains largely unclarified.
To address these knowledge gaps, swabs were taken from different locations or areas of two surgical intensive care unit (ICU) sluice room sinks in a South African tertiary hospital and the samples plated on carbapenem-infused agar plates. Unique colonies were isolated, identified and their drug resistance profile determined. Finally, carbapenem-infused agar plates were placed at varying distances away from the sink, whilst the tap was turned on, and subsequently cultured.
Methods
Sample Collection
Two sluice room sinks in the surgical ICU unit at Groote Schuur Hospital in Cape Town, South Africa, were swabbed on different days at the opening of the tap, the trap (drain grate), 10 cm below the trap, and at the u-bend (overview-figure Figure 1). Nurses on duty at the ICU were also interviewed to determine sink cleaning protocols, which revealed that the sinks were being surface scrubbed with 0.06% (w/v; 250 ppm) sodium dichloroisocyanurate (Hygenie Capricide Extra, Caprichem, South Africa) 3 times a day, and in addition when biological material was discarded. There was no specific cleaning of the sink pipe below the trap and leading to the u-bend. The study was approved by the University of Cape Town Research Ethics Committee (HREC approval number 153/2019) and the Groote Schuur Hospital research approvals board.
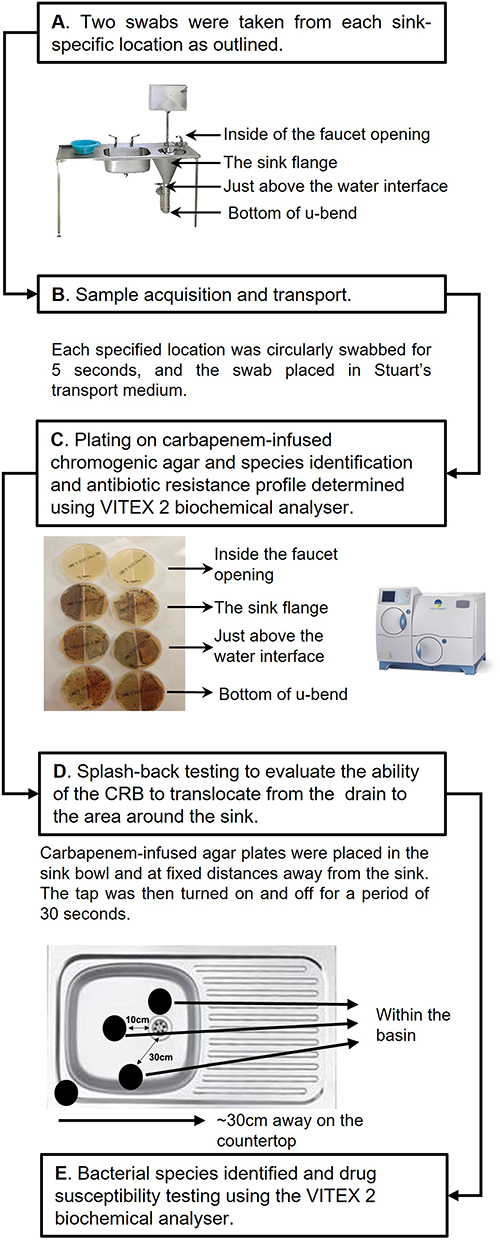 |
Figure 1 Schematic showing the study overview and the sampling methods used. (A) The sluice drain was swabbed inside the tap opening, the area around the trap, at the water interface below the trap, and at the bottom of the u-bend. (B) The swabs were transported to the laboratory and dilutions were plated on to carbapenem-impregnated agar plates as detailed in the materials and methods. (C) After incubating the plates for 5 days at 30°C individual colonies were selected for phenotypic identification and antibiotic susceptibility testing (VITEX 2). (D) To study the transmission dynamics of the CRB, carbapenem-infused agar plates were placed around various areas of the sluice sink as outlined. The tap was turned on and off for 30 seconds, and the agar plates were incubated at 30°C for 5 days. (E) The bacteria were identified, and antimicrobial susceptibility testing performed as above. |
Swabs were placed in Stuart’s transport medium. In the laboratory (intervening transport time of ~15 minutes) the swabs were cut and placed in 1mL Dulbecco’s phosphate-buffered saline (DPBS; Lonza, Germany) and vortexed for 1 minute. Five serial 1 in 10 dilutions were prepared, and 100µL of each dilution was spread on to carbapenem-infused agar plates (ChromID Carba Smart Agar Plates; BioMérieux; Marcy-l’Étoile, France; Figure 1C). The plates were incubated aerobically at 30°C for 5 days, after which individual colonies were streaked onto MacConkey agar plates (Sigma, South Africa) and incubated for an additional 5 days.
Splashback Experiments
Four carbapenem-infused agar plates were placed at different locations (varying distances of 1cm to 30cm from the trap) inside one of the sinks in the ICU unit (Figure 1D). The last remaining plate was placed on the countertop on the edge of the basin. The tap was turned on for 30 seconds. The plates were incubated as outlined above.
Identification and Susceptibility Testing
The bacterial species cultured on the MacConkey agar plate were identified and antibiotic resistance profile determined using the automated biochemical analyser, VITEK® 2 (BioMérieux, South Africa), using the GN identification and AST-255 susceptibility testing cards. Clinical Laboratory Standards Institute clinical breakpoints (M100) were applied.13
Results
A total of 4 swabs were taken from the various areas of the sink depicted in Figure 1, of which 3 yielded growth on the carbapenem-infused agar. Eight unique carbapenem-resistant bacterial species (resistant to 7 antibiotic classes; Table 1), with potential to cause outbreaks in the ICU, were identified from 8 chromogenically and morphologically distinct colonies (Table 1). The greatest concentration of carbapenem-resistant bacteria (CRB; plate growth density and number of species) were found at the bottom of the u-bend though CRB could also be cultured from the trap and the water interface below the trap (but not from the tap opening). One K. pneumonia isolate was resistant to almost all 18 antibiotics tested. Splash back experiments isolated colonies of P. fluorescens from the plate within the sink and closest to the drain trap but not from plates placed outside the basin (Figure 1).
 |
Table 1 Carbapenem-Resistant Bacteria Isolated from the Sluice Drain of an ICU at a Tertiary Hospital in Cape Town, South Africa. The Drug Susceptibility Profile of Each Organism is Shown, and the Organisms are Ordered by Isolation Location from the Trap to the u-bend |
The greatest concentration of CRB (by plate growth density and number of species) were found in the u-bend: these included S. marcescens, K. pneumoniae, and P. rettgeri. While no CRB were isolated from the tap-opening, C. freundii and P. aeruginosa were cultured from the water-level and S. marcescens and P. aeruginosa were cultured from the trap.
Discussion
The key findings of this preliminary study were that (i) CRB could be cultured from ICU sluice room sinks in a resource-poor African setting, (ii) the sample location within the sink that cultured the highest taxonomic density of CRB was the u-bend, and (iii) CRB could be cultured from agar plates placed at the sink trap when the tap was turned on suggesting cross-contamination and potential transmission via this route may occur. It is often assumed that multi-drug antibiotic resistance is uncommon in Africa.14 However, we have demonstrated that this assumption is untrue. Clearly, further epidemiological studies are required from resource-poor settings to add to the limited existing data.14
Overall, there are hardly any data about CRB density from different parts of the sink. In most studies samples were only taken from the sink trap (reviewed in15) though several studies documented CRB growth from the u-bend of the sink.15 Our data, incorporating sampling of the tap opening, trap, at water level below the trap, and the u-bend suggest that simply sampling from the sink trap is insufficient in determining the extent of CRB colonisation, and that better decontamination strategies are required to remove bacterial biofilms deeper within the draining pipe. Such strategies may include pressured steam in conjunction with chemical disinfectants though there are no comprehensive comparative studies.15 Another method to prevent CRB colonisation may involve installing sinks without a u-bend and only a trap, where the contents are discarded into biohazardous drums. We did not ascertain the quantitative microbiological load at each of the drain locations because of funding constraints, the preliminary nature of the study, and the high cost of the carbapenem-infused agar plates (US$ 125/plate). Another limitation was that confirmation of the mechanism of carbapenem resistance and detection of carbapenemases, either phenotypic, antigenic, or genotypic, was not performed, nor was molecular typing of isolates (for the same reasons as outlined above).
Our droplet-related spread data are in keeping with that of other studies using fluorescent-labelled fluid or whole-genome sequencing16,17 showing the potential of CRB to be transmitted to patients and healthcare workers. A limitation of all these methods and studies is lack of data about the clinical impact of these findings. Thus, there is a need for further studies of improved splash-resistant sink design and transmission-minimising protocols for health care workers and those who clean in health care facilities.18
In conclusion, we isolated a variety of CRB from sluice room sinks in an African ICU. The u-bend of ICU sluice room sinks are reservoirs for CRB with transmission potential. These data have implications for infection control interventions and limiting antimicrobial resistance in resource-poor settings. Such interventions may include implementation of regular approved and effective sink cleaning protocols, regularly swab monitoring of hospital sinks, and using sink designs that minimise splashback or do not have conventional trap systems that perpetuate microbiological reservoirs.
Acknowledgments
The authors would like to thank the ICU Head Nurse, Sr Jennifer Abrahams, who generously helped to facilitate the sampling and interviews, and Dr Jason Limberis, who provided valuable intellectual input.
Funding
This work was supported by Antrum Biotech, a University of Cape Town spin off company, through an unrestricted student support grant. The research and development company does not work in the field of antibiotics, antimicrobial resistance, or decontamination products, and its employees played no role in the study design, collection, analysis and interpretation of data, writing of the report, or the decision to submit the article for publication. AE was supported by funding received from the European and developing Countries Clinical Trials Partnership (EDCTP TMA-2015CDF-1052). Some of work was supported by the South African MRC (RFA-EMU-02-2017). AP was supported by funding received from the European and developing Countries Clinical Trials Partnership (EDCTP TMA-2019CDF-2780).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Antimicrobial resistance; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance#:~:text=Antimicrobial%20resistance%20(AMR)%20is%20a,public%20health%20threats%20facing%20humanity.
2. Alanis AJ. Resistance to antibiotics: are we in the post-antibiotic era? Arch Med Res. 2005;36(6):697–705. doi:10.1016/j.arcmed.2005.06.009
3. De Geyter D, Blommaert L, Verbraeken N, et al. The sink as a potential source of transmission of carbapenemase-producing Enterobacteriaceae in the intensive care unit. Antimicrob Resist Infect Control. 2017;6:24. doi:10.1186/s13756-017-0182-3
4. Feng Y, Wei L, Zhu S, et al. Handwashing sinks as the source of transmission of ST16 carbapenem-resistant Klebsiella pneumoniae, an international high-risk clone, in an intensive care unit. J Hosp Infect. 2020;104(4):492–496. doi:10.1016/j.jhin.2019.10.006
5. Low YM, Yap PS, Abdul Jabar K, et al. The emergence of carbapenem resistant Klebsiella pneumoniae in Malaysia: correlation between microbiological trends with host characteristics and clinical factors. Antimicrob Resist Infect Control. 2017;6:5. doi:10.1186/s13756-016-0164-x
6. Nordmann P, Naas T, Poirel L. Global spread of Carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis. 2011;17(10):1791–1798. doi:10.3201/eid1710.110655
7. Sukhum KV, Newcomer EP, Cass C, et al. Antibiotic-resistant organisms establish reservoirs in new hospital built environments and are related to patient blood infection isolates. Commun Med. 2022;2:62. doi:10.1038/s43856-022-00124-5
8. Yoon EJ, Kim JO, Kim D, et al. Klebsiella pneumoniae carbapenemase producers in South Korea between 2013 and 2015. Front Microbiol. 2018;9:56. doi:10.3389/fmicb.2018.00056
9. Sharma D, Misba L, Khan AU. Antibiotics versus biofilm: an emerging battleground in microbial communities. Antimicrob Resist Infect Control. 2019;8:76. doi:10.1186/s13756-019-0533-3
10. Potter RF, D’Souza AW, Dantas G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist Updat. 2016;29:30–46. doi:10.1016/j.drup.2016.09.002
11. Weingarten RA, Johnson RC, Conlan S, et al. Genomic analysis of hospital plumbing reveals diverse reservoir of bacterial plasmids conferring carbapenem resistance. mBio. 2018;9(1). doi:10.1128/mBio.02011-17
12. Wendel AF, Ressina S, Kolbe-Busch S, Pfeffer K, MacKenzie CR. Species diversity of environmental GIM-1-producing bacteria collected during a long-term outbreak. Appl Environ Microbiol. 2016;82(12):3605–3610. doi:10.1128/AEM.00424-16
13. Clinical and laboratory standards institute. Performance standards for antimicrobial susceptibility testing. CLSI supplement M100; 2020. Available from: https://www.nih.org.pk/wp-content/uploads/2021/02/CLSI-2020.pdf.
14. Tadesse BT, Ashley EA, Ongarello S, et al. Antimicrobial resistance in Africa: a systematic review. BMC Infect Dis. 2017;17(1):616. doi:10.1186/s12879-017-2713-1
15. Parkes LO, Hota SS. Sink-related outbreaks and mitigation strategies in healthcare facilities. Curr Infect Dis Rep. 2018;20(10):42. doi:10.1007/s11908-018-0648-3
16. Guo X, Tang N, Lei H, et al. Metagenomic analysis of antibiotic resistance genes in untreated wastewater from three different hospitals. Front Microbiol. 2021;12:709051. doi:10.3389/fmicb.2021.709051
17. Hendriksen RS, Munk P, Njage P, et al. Global monitoring of antimicrobial resistance based on metagenomics analyses of urban sewage. Nat Commun. 2019;10(1):1124. doi:10.1038/s41467-019-08853-3
18. World Health Organization. Environmental cleaning and infection prevention and control in health care facilities in low- and middle-income countries: trainer’s guide; 2022. Available from: https://apps.who.int/iris/handle/10665/366379.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Distribution and Antimicrobial Resistance Trends of Bloodstream Bacterial Isolates: A 10-year Single-Center Study in China
He X, Liu M, Wang X, Li S, Zhang Y, Jiang S, Liu Z, Waqas M, Wang X
Infection and Drug Resistance 2026, 19:588264
Published Date: 17 March 2026