Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Intensity-Modulated Proton Therapy for Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis
Authors Liu CM ![]() , Lai CH, Wang YM, Huang EY, Chen YH
, Lai CH, Wang YM, Huang EY, Chen YH ![]() , Ou HY
, Ou HY ![]() , Hu TH, Hung CH, Lu SN
, Hu TH, Hung CH, Lu SN ![]() , Chen WY, Huang BS, Cheng JY
, Chen WY, Huang BS, Cheng JY ![]()
Received 2 July 2025
Accepted for publication 22 November 2025
Published 1 December 2025 Volume 2025:12 Pages 2655—2670
DOI https://doi.org/10.2147/JHC.S551113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Mohamed Shaker
Chieh-Min Liu,1 Chia-Hsuan Lai,2 Yu-Ming Wang,1,3,4 Eng-Yen Huang,1,3,4 Yen-Hao Chen,5– 7 Hsin-You Ou,8 Tsung-Hui Hu,9 Chao-Hung Hung,9 Sheng-Nan Lu,9 Wan-Yu Chen,10,11 Bing-Shen Huang,1,6,12,* Jen-Yu Cheng1,13,*
1Department of Radiation Oncology & Proton and Radiation Therapy Center, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan; 2Department of Radiation Therapy, Chang Gung Memorial Hospital, Chiayi, Taiwan; 3School of Traditional Chinese Medicine, Chang Gung University, Taoyuan, Taiwan; 4Department of Radiation Oncology, Kaohsiung Chang Gung Memorial Hospital, School of Medicine, College of Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan; 5Division of Hematology-Oncology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 6School of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan; 7Department of Nursing, School of Nursing, Fooyin University, Kaohsiung, Taiwan; 8Department of Diagnostic Radiology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 9Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan; 10Division of Radiation Oncology, Department of Oncology, National Taiwan University Hospital, Taipei City, Taiwan; 11Cancer Research Center, National Taiwan University College of Medicine, Taipei City, Taiwan; 12Department of Radiation Oncology, Linkou Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Taoyuan, Taiwan; 13Center for General Education, Cheng Shiu University, Kaohsiung, Taiwan
*These authors contributed equally to this work
Correspondence: Bing-Shen Huang, Email [email protected] Jen-Yu Cheng, Email [email protected]
Background: Patients with hepatocellular carcinoma (HCC) with portal vein tumor thrombosis (PVTT) have poor outcomes and limited treatment options. Clinical data specifically evaluating the effects of intensity-modulated proton therapy (IMPT) for this population remain scarce. We reported the outcomes of patients with HCC with PVTT treated with IMPT.
Material and Methods: We retrospectively reviewed the data of 83 patients with nonmetastatic HCC with PVTT treated with IMPT between March 2019 and June 2023. Survival outcomes were analyzed with Kaplan–Meier analysis, and prognostic factors were identified via multivariable Cox regression. Treatment responses were assessed with the modified Response Evaluation Criteria in Solid Tumors. Toxicities, including liver dysfunction and gastrointestinal events, were documented.
Results: The median overall survival (OS) was 32.4 months, with 1- and 2-year OS rates of 82.6% and 61.0%, respectively. The 2-year local control rate was 88.8%, and the objective response rate was 91.5%. Complete response after IMPT was independently associated with improved OS and liver control, whereas an albumin-bilirubin (ALBI) grade of 2 predicted a greater risk of liver dysfunction. Grade 3 gastrointestinal toxicities occurred in 4.8% of patients, and radiation-induced liver disease occurred in 9.3%. IMPT facilitated curative-intent surgery in 8.4% of patients after treatment.
Conclusion: IMPT offers excellent local control and a favorable safety profile in patients with HCC and PVTT, with the potential to downstage tumors for curative interventions. These findings, though limited by the retrospective design and heterogeneity of systemic therapies, support the integration of IMPT into multidisciplinary treatment strategies and highlight the need for prospective studies to clarify its role alongside systemic therapy.
Keywords: HCC, IMPT, PVTT, retrospective
Introduction
Hepatocellular carcinoma (HCC) is the third leading cause of cancer-related mortality globally. Up to 44% of patients with advanced HCC will develop portal vein tumor thrombosis (PVTT), which significantly worsens their outcomes.1,2 Although systemic therapies remain the standard first-line approach for advanced HCC, the median overall survival (OS) remains disappointing, ranging from only 9.7 to 14.2 months. Furthermore, patients with advanced PVTT, particularly those with Vp4 (thrombosis in the main trunk of the portal vein) involvement, are frequently excluded from pivotal clinical trials.3–5 Effective management of patients with HCC with PVTT thus requires a multidisciplinary approach that carefully balances the liver reserve, tumor extent, and performance status of the patient.
Radiation therapy (RT) has emerged as an effective locoregional treatment modality for HCC patients with PVTT, particularly when high doses are delivered.6–8 However, gastrointestinal (GI) toxicity and radiation-induced liver disease (RILD) remain significant barriers, restricting the ability to increase the radiation dose and thus often limiting RT to a palliative role. Compared with conventional photon-based RT, proton therapy, which utilizes the Bragg peak phenomenon, provides improved dose conformality, potentially improving therapeutic outcomes while reducing the effects to the normal tissue.9,10 Previous research has focused primarily on passive scattering proton therapy (PSPT) in the treatment of HCC, whereas intensity-modulated proton therapy (IMPT), which represents a more advanced approach, allows precise optimization of the dose delivered to the tumor and increased sparing of adjacent normal liver parenchyma.11 This advanced dose distribution capability may allow dose escalation, thereby improving local tumor control while significantly reducing the risk of RILD, a critical advantage for managing intrahepatic malignancies such as HCC with PVTT.12,13 Theoretically, this dosimetric superiority suggests that IMPT could be an ideal modality to safely deliver ablative radiation doses, which may translate into improved clinical outcomes for this high-risk population. Despite these potential advantages, the optimal management strategy for HCC complicated by PVTT remains controversial, particularly in patients with Vp3 or Vp4 involvement, who are consistently underrepresented in pivotal systemic therapy trials. In this context, radiotherapy—particularly advanced proton-based techniques—may offer a promising approach by achieving high local tumor control with limited hepatic toxicity.14 However, prospective or large-scale retrospective evidence specifically evaluating the efficacy of IMPT in this patient population, particularly for those with advanced PVTT, remains lacking and is urgently needed.
In this study, we describe the largest single-institution experience in evaluating the outcomes of patients with nonmetastatic HCC and concurrent PVTT treated with IMPT, representing the complete and updated analysis of a cohort whose preliminary findings were previously reported.15 We hypothesized that IMPT provides superior disease control with minimal toxicity over other treatment modalities, potentially facilitating subsequent curative treatments. Our findings aim to challenge the current systemic therapy-only approach recommended for patients classified with Barcelona Clinic Liver Cancer (BCLC) stage C disease by evaluating the potential of IMPT as a curative-enabling modality.
Materials and Methods
Patients
We conducted a retrospective review of the data of 104 patients diagnosed with HCC complicated by PVTT who underwent proton therapy at the Proton Therapy Center of our medical center between March 2019 and June 2023. Patients with nodal metastases (n=10), distant metastases (n=9), incomplete radiotherapy (n=1), or a history of prior liver irradiation (n=1) were excluded, resulting in a final cohort of 83 patients. As all patients were required to have a good performance status to be eligible for proton therapy, all included patients had an Eastern Cooperative Oncology Group (ECOG) score of 0 or 1. Both treatment-naïve patients and patients with recurrent tumors were included. The Japanese classification system was used to denote the extent of PVTT.16 The diagnosis of tumoral PVTT was based on a combination of clear radiological features on dynamic contrast-enhanced magnetic resonance imaging (MRI). These features included: (1) direct continuity with the primary tumor (ie, no skip lesions), (2) the presence of arterial phase hyper-enhancement and/or venous phase washout within the portal vein thrombus, and (3) findings consistent with tumor on diffusion-weighted imaging and apparent diffusion coefficient mapping. Furthermore, all diagnoses were confirmed by an experienced radiologist, and any ambiguous cases were resolved through multidisciplinary team discussion. The study was approved and exempted from written informed consent by the Institutional Review Boards of the Chang Gung Medical Foundation at Taipei, Taiwan (permit number: 202400637B0). All patient data were fully anonymized and handled with strict confidentiality before analysis. The study was conducted in compliance with the Declaration of Helsinki and other ethical guidelines.
Radiation Planning and Treatment
All patients underwent respiratory evaluation and received respiratory training before simulation. Treatment planning involved both four-dimensional computed tomography (4D-CT) and Primovist-enhanced MRI to accurately delineate the tumor and PVTT volumes. All the MRI images were reviewed by an experienced radiologist to ensure precise target delineation. Before October 2021, abdominal belt compression was used to restrict diaphragmatic and tumor motion to within 1 cm. Subsequently, gated IMPT was implemented with an Anzai Gating System (Anzai Medical Co., Ltd., Tokyo, Japan). Patients exhibiting stable respiratory patterns were instructed to use breath holding or were managed with respiratory gating techniques at the end-expiratory phase to limit tumor motion to 0.5–1 cm. Abdominal compression was performed for patients unable to maintain a stable breathing pattern. The gross tumor volume encompassed the primary liver tumor(s) and the associated PVTT. Crucially, only the portions of the portal vein thrombus demonstrating tumoral signals on MRI were included in the GTV. The clinical target volume was defined as the gross tumor volume with an additional margin of 0–0.5 cm, and the internal target volume (ITV) was determined on the basis of 4D-CT analysis.
The IMPT treatments included a total dose of either 72.6 Gy (relative biological effectiveness [RBE]) delivered in 22 fractions or 66 Gy (RBE) delivered in 10 fractions. The choice of fractionation was based on institutional guidelines and guided by the proximity of the tumor to critical structures such as the gastrointestinal (GI) tract or porta hepatis (the 22-fraction regimen was favored for tumors within 2 cm of these structures).17 Dose constraints restricted the maximum bowel dose to less than 65% (47.19 Gy) of the prescribed dose for the 22-fraction regimen and less than 50% (33Gy) for the 10-fraction regimen. The heart doses were constrained to below 90% and 65%, respectively, of these prescribed doses. Additionally, the unirradiated liver volumes receiving less than 1 Gy were maintained above 300 cc for patients with Child‒Pugh class A disease and at 450 cc for those with Child‒Pugh class B disease. The IMPT plans were generated with RayStation (RaySearch Laboratories, Stockholm, Sweden) software using robust optimization accounting for a 3–5 mm setup uncertainty and 3.5% range uncertainty, as validated via Monte Carlo simulation. Proton therapy was delivered using pencil beam scanning technology (Sumitomo Heavy Industries). Key dosimetric and volume parameters from the achieved treatment plans were retrospectively collected and analyzed, including dose-volume histogram (DVH) parameters for the target volumes (CTV, ITV) and organs at risk (OARs) such as the liver and gastrointestinal tract. The detailed dosimetric data, stratified by fractionation regimen, are presented in Supplementary Table 1. Daily imaging guidance via orthogonal X-rays, fluoroscopy, or cone-beam CT and adaptive replanning every 2–4 weeks were conducted to ensure precise treatment delivery.
Systemic Agents
Systemic therapy remains the standard-of-care for patients with BCLC stage C patients, especially for newly diagnosed patients. Following the landmark IMbrave150 trial, immune-based combination therapies were recommended starting in 2020.18 However, at the time of patient enrollment in this study, these immune-based therapies were not reimbursed by Taiwan’s National Health Insurance system. Consequently, the choice and order of targeted therapies or immunotherapies in combination with IMPT were individualized. While concurrent therapy was generally encouraged by the multidisciplinary team, there was no standardized protocol; the final decision and timing were determined collaboratively by medical oncologists or gastroenterologists, following a detailed discussion with the patient regarding the potential pros and cons of each option, including the financial implications of self-funded therapies. This individualized decision-making method considers factors such as patient performance status, treatment-related adverse effects, previous treatment exposure, and patients’ financial considerations.
Endpoints and Follow-up
Patients were evaluated weekly by radiation oncologists throughout the IMPT treatment period. Following treatment completion, patients underwent regular follow-up visits. The first follow-up for response assessment, including clinical examination, laboratory tests, and liver MRI, was scheduled 3 months post-IMPT, and every 3 months thereafter. Chest CT scans or additional imaging studies were conducted on the basis of clinical indications determined by the attending physician.
Treatment responses were evaluated according to the Modified Response Evaluation Criteria in Solid Tumors (mRECIST).19 The objective response rate (ORR) was defined as the proportion of patients who achieved either a complete response (CR) or partial response (PR). Gastrointestinal (GI) toxicities were graded using the Common Terminology Criteria for Adverse Events, version 5.0. Posttreatment liver dysfunction was defined as an increase in the Child‒Pugh score by ≥2 points within three months following the completion of treatment. RILD was diagnosed if liver dysfunction occurred in the absence of intrahepatic disease progression outside the irradiated area.20
Statistical Analysis
Survival outcomes were analyzed with the Kaplan–Meier method, and differences between survival curves were assessed with the Log rank test. Multivariable analysis was conducted with the Cox proportional hazards model to identify independent prognostic factors of survival. All the statistical tests were two-sided, and statistical significance was identified if the p value was less than 0.05. Data analyses were performed using SPSS statistical software (version 25.0; IBM Corp., Armonk, NY, USA).
Results
The data of 83 patients with nonmetastatic HCC complicated by PVTT were analyzed. The median follow-up duration for the surviving patients was 17 months (range, 4.0–52.2 months). Details of the demographic and clinical characteristics are summarized in Table 1. The median age was 62 years (range, 34–93 years), and most patients were male (84.3%) and classified as having Child‒Pugh class A disease (89.2%). A substantial proportion of patients (42.2%) presented with an albumin‒bilirubin (ALBI) grade of 2. Approximately one-third (32.5%) of the patients had multiple liver tumors, and 41% had tumors measuring ≥10 cm in size (median, 8 cm). The thrombosis involved the main trunk or first-order branches of the portal vein (Vp3/4) in 75.9% of patients. Additionally, nearly half (51.8%) of the patients had recurrent HCC, and 32.5% received IMPT as monotherapy without concurrent systemic therapy. At baseline, 28 patients (33.7%) were known to have gastroesophageal varices, five of whom had already received endoscopic ligation prior to IMPT. No patient had portal vein cavernous malformation (PVCM) at baseline.
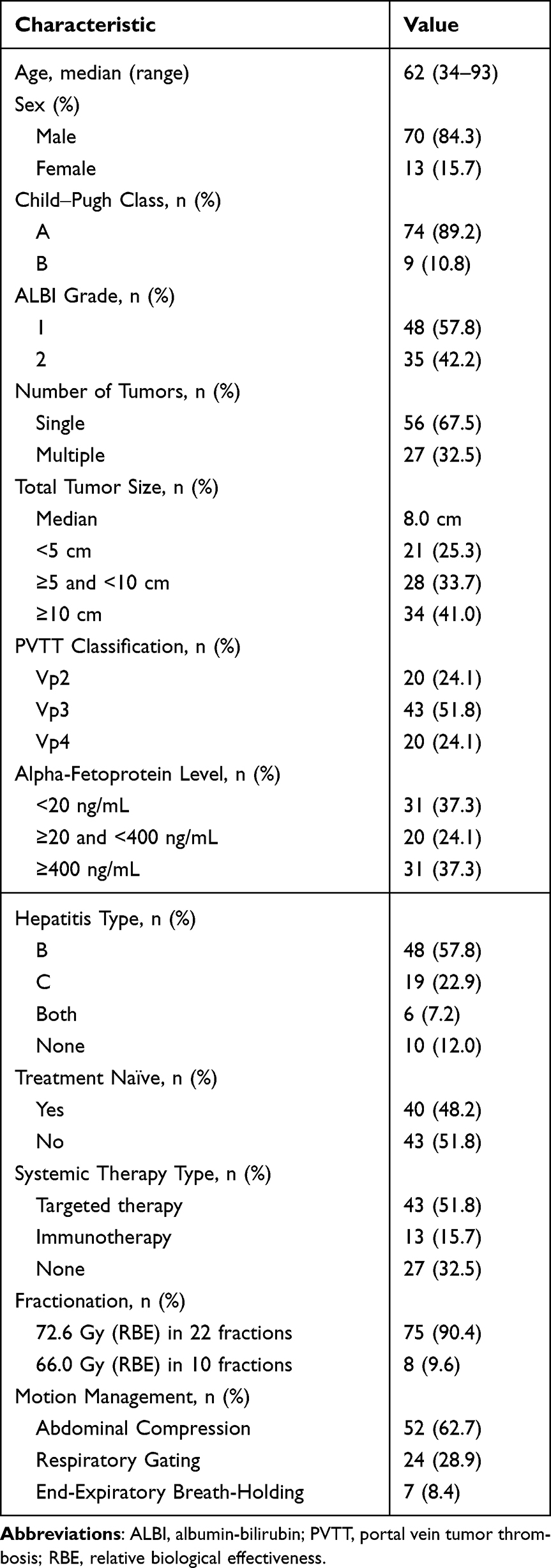 |
Table 1 Patient Demographics and Clinical Characteristics |
Systemic therapy was administered either concurrently with radiotherapy or in the adjuvant setting. Patients in the targeted therapy group (n=43) received lenvatinib or sorafenib; among them, 21 patients (48.8%) received concurrent treatment and 22 (51.2%) received adjuvant treatment. The immunotherapy group (n=13) included patients treated with atezolizumab plus bevacizumab or monotherapy with immune checkpoint inhibitors (one patient received nivolumab and another pembrolizumab); in this group, 7 patients (53.8%) received concurrent treatment and 6 (46.2%) received adjuvant treatment. A total of 27 patients (32.5%) received proton therapy alone without concurrent or adjuvant systemic treatment. The remaining patients did not receive systemic therapy due to factors such as poor performance status, financial constraints, or personal refusal.
Dosimetric details of the delivered IMPT plans are summarized in Supplementary Table 1. In brief, for the 75 patients (90.4%) in the 72.6 Gy/22 fractions group, the median CTV D95 was 5406 cGy (RBE) and the median maximum dose to the gastrointestinal tract was 4617 cGy (RBE). For the 8 patients (9.6%) in the 66.0 Gy/10 fractions group, the median CTV D95 was 4782 cGy (RBE) and the median maximum dose to the gastrointestinal tract was 3385 cGy (RBE). The median unirradiated liver volumes (receiving < 1 Gy) were 432 mL and 677 mL in the respective fractionation groups.
The median OS of the entire cohort was 32.4 months, and the 1- and 2-year OS rates were 82.6% and 61.0%, respectively. The local control (LC) rates remained consistently high, reaching 88.8% at both one and two years. The intrahepatic 1- and 2-year recurrence-free survival rates were 49.2% and 30.7%, respectively, whereas the corresponding distant metastasis-free survival rates were 63.6% and 51.1%, respectively (Figure 1).
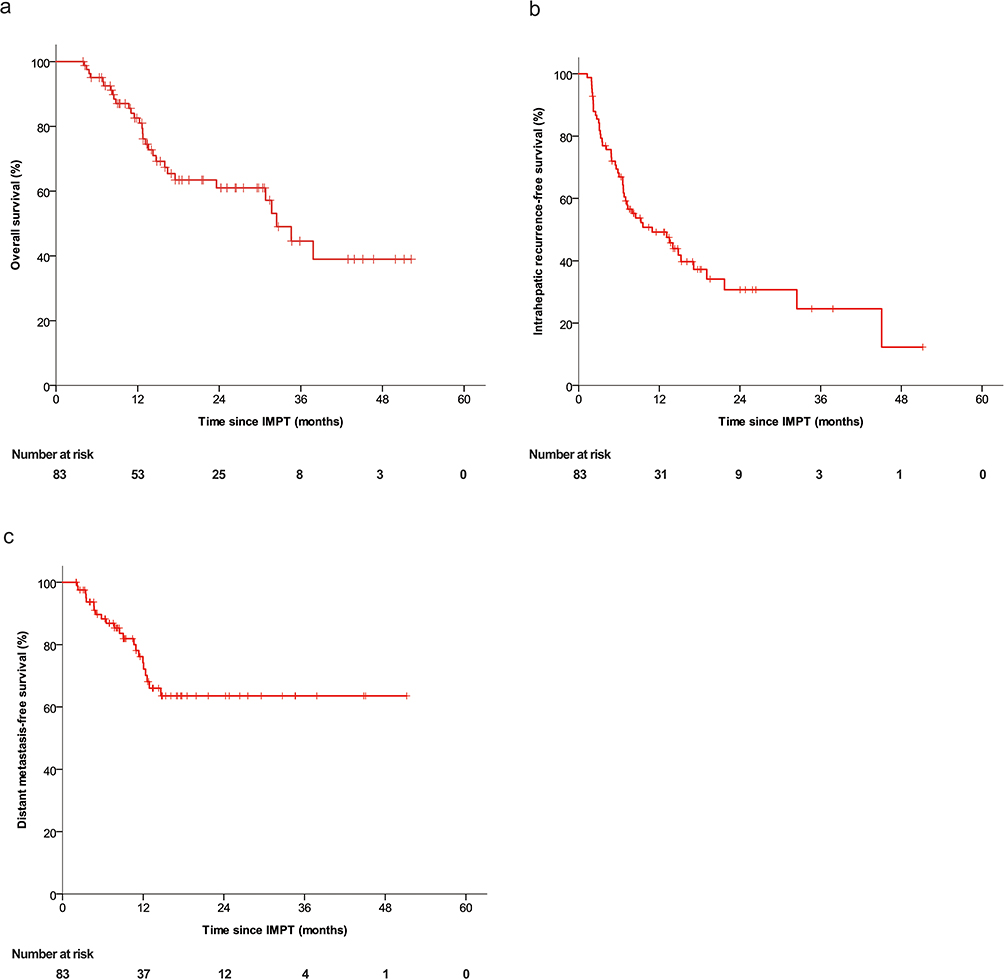 |
Figure 1 Kaplan–Meier analysis of survival outcomes in all patients treated with IMPT. (a) Overall survival; (b) intrahepatic recurrence-free survival; (c) distant metastasis-free survival. Abbreviation: LIMPT, intensity-modulated proton therapy. |
Both univariable and multivariable analyses revealed that ALBI grade of 2 and advanced PVTT (Vp3/4) were independently associated with worse survival outcomes (Table 2). Notably, concurrent systemic therapy in addition to IMPT did not yield a significant survival advantage over IMPT alone (median OS: 34.6 vs 32.4 months; p = 0.795). Subgroup analyses in terms of PVTT classification and the use of systemic therapies were performed, but no significant differences in OS or progression-free survival (PFS) were observed (Table 3 and Figure 2).
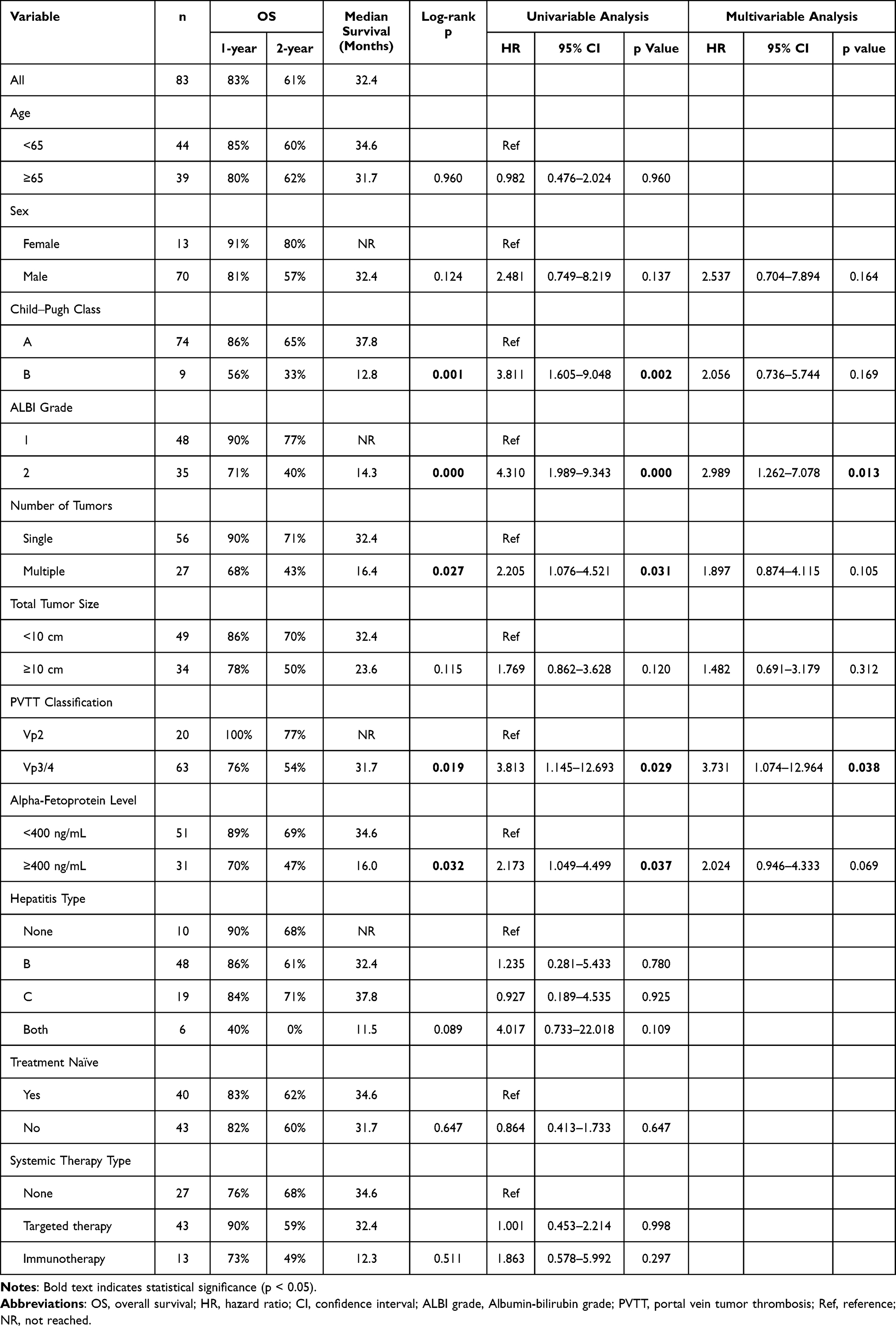 |
Table 2 Survival Outcomes and Prognostic Factors for Overall Survival |
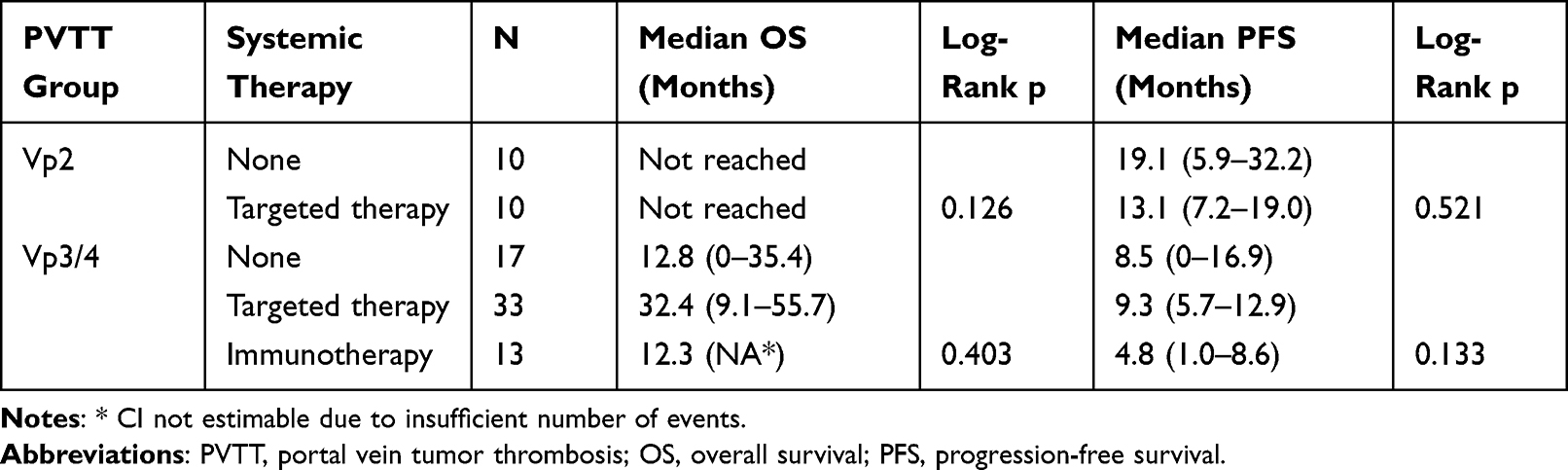 |
Table 3 Stratified Kaplan-Meier Analysis of Overall Survival and Progression-Free Survival According to Systemic Therapy Status in Vp2 and Vp3/4 Subgroups |
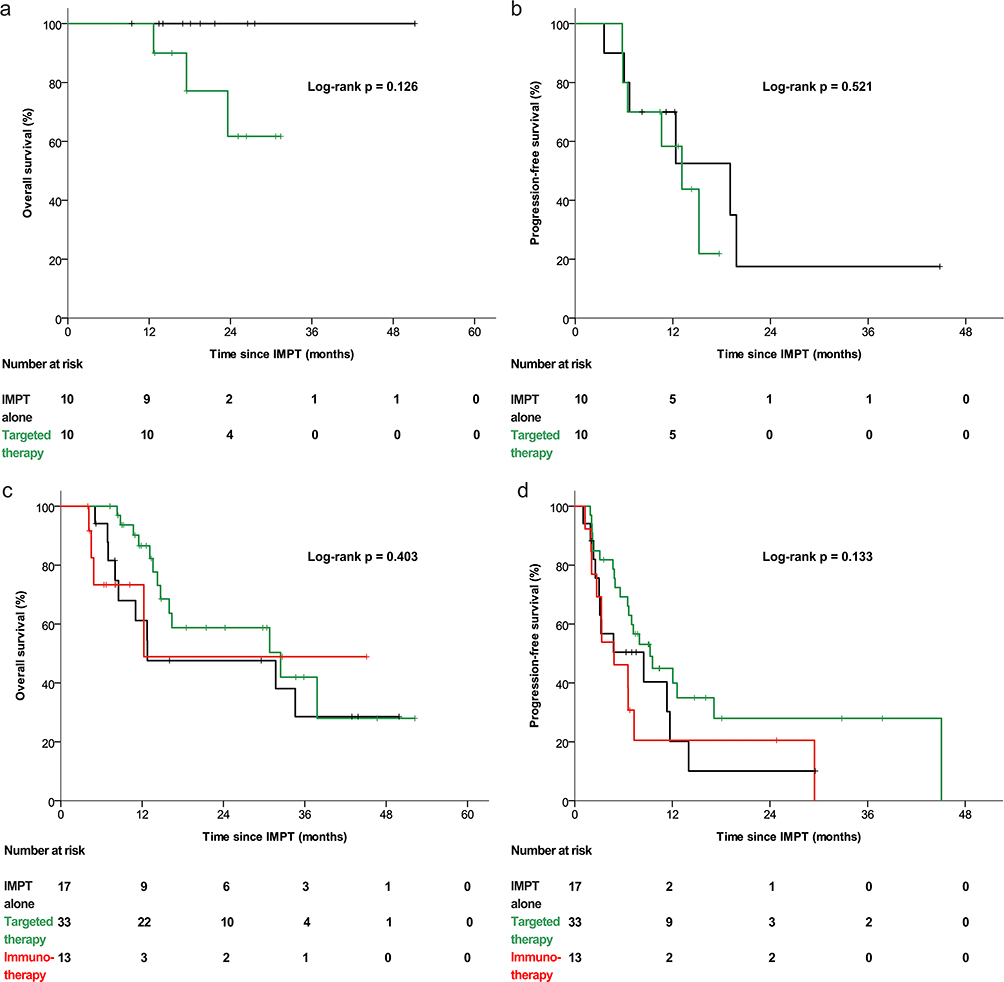 |
Figure 2 Subgroup analysis of overall survival and progression-free survival stratified by systemic therapy in patients with different PVTT classifications. Kaplan–Meier survival curves are shown for: (a) overall survival and (b) progression-free survival of patients with Vp2 PVTT, comparing IMPT alone (black line) versus IMPT with targeted therapy (green line), and (c) overall survival and (d) progression-free survival of patients with Vp3/4 PVTT, comparing IMPT alone (black line), IMPT plus targeted therapy (green line), and IMPT plus immunotherapy (red line). Abbreviations: PVTT, portal vein tumor thrombosis; IMPT, intensity-modulated proton therapy. |
Further subgroup analyses comparing patients with Vp3 and Vp4 PVTT revealed no statistically significant differences in median OS (31.7 vs 37.8 months, p = 0.461), median PFS (8.5 vs 5.6 months, p = 0.147), median intrahepatic PFS (9.7 vs 4.8 months, p = 0.133), or median local PFS (45.1 vs 32 months, p = 0.332).
One patient was excluded from the disease response analysis because they died early from esophageal variceal rupture. The rates of mRECIST-defined CR and PR were 37.8% and 53.7%, respectively, resulting in an ORR of 91.5%. Specifically, when assessing response of with primary liver tumors, the CR and PR rates were 48.8% and 43.8%, respectively, whereas for the portal venous tumor thrombi, the CR and PR rates were 45.1% and 40.2%, respectively. Consequently, the ORRs were 92.5% for the liver tumors and 85.4% for the tumor thrombi (Table 4).
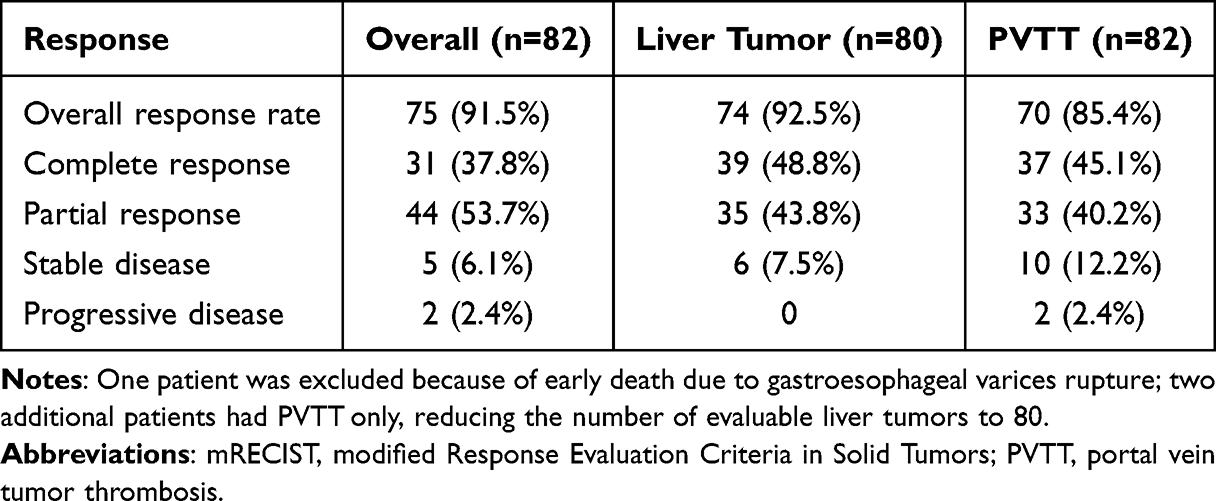 |
Table 4 Treatment Efficacy as Evaluated by the mRECIST |
Figure 3 displays the Kaplan–Meier survival curves for patients with different treatment responses (CR vs non-CR groups). Compared with those who did not achieve CR, patients who achieved CR had a significantly improved OS, and the corresponding hazard ratio (HR) was 2.57 (95% CI, 1.13–5.85; p = 0.020). Additionally, the liver control outcomes were significantly better in the CR group than in the non-CR group (HR, 1.95; 95% CI, 1.03–3.68; p = 0.037). Although distant metastasis-free survival tended to be better in the CR group (HR, 1.84; 95% CI, 0.75–4.54), the difference was not statistically significant (p = 0.177).
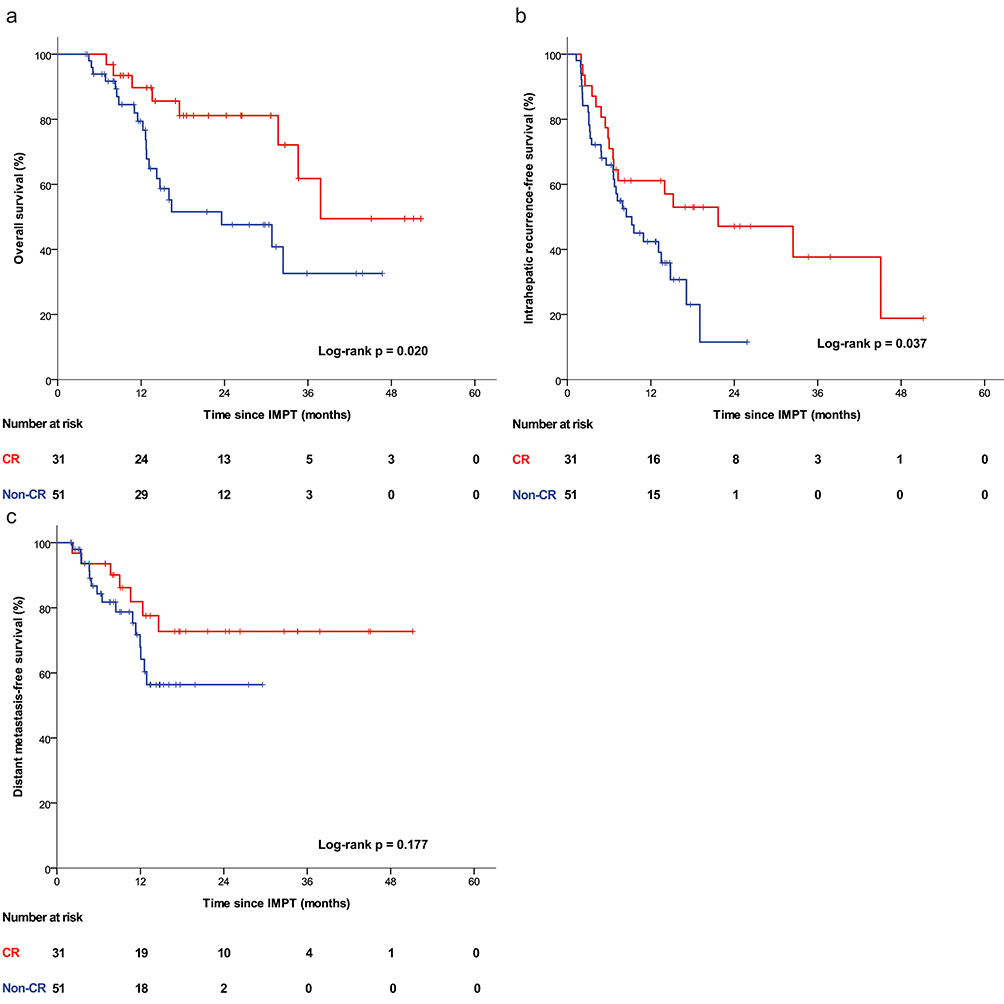 |
Figure 3 Kaplan–Meier survival curves according to treatment response (CR vs non-CR). (a) Overall survival, (b) intrahepatic recurrence-free survival, and (c) distant metastasis-free survival for patients who achieved a complete response (CR, red line) versus those who did not achieve a complete response (non-CR, blue line) after IMPT. Abbreviations: CR, complete response; IMPT, intensity-modulated proton therapy. |
Treatment-related toxicities included posttreatment liver dysfunction in 15 patients (18.1%). Among these patients, 8 experienced intrahepatic tumor recurrence, while the other 7 (9.3%) were classified as having RILD. Three patients (3.6%) eventually died due to liver decompensation in the absence of disease recurrence. Multivariable logistic regression analysis was performed to identify predictors of liver dysfunction. We identified ALBI grade of 2 as a significant predictor of post-IMPT liver dysfunction (Table 5). The discriminative performance of ALBI grade 2 was further supported by receiver operating characteristic (ROC) curve analysis, which yielded an area under the curve (AUC) of 0.842 (95% CI, 0.734–0.950; p < 0.001; Figure 4). Grade 3 GI toxicities occurred in four patients (4.8%). One patient developed an antrum ulcer four months post-IMPT and was treated with endoscopic Argon Plasma Coagulation. A 92-year-old patient presented with bloody and tarry stool (suspected lower GI bleeding) at six months; this patient refused invasive procedures and was subsequently stabilized with conservative medication and blood transfusion. A third patient was diagnosed with a duodenal bulb ulcer at 11 months, with concurrent suspicion of tumor recurrence invading the site, and underwent transarterial embolization for hemostasis. The fourth patient developed a duodenal bulb ulcer at 12 months and was managed with endoscopic treatment, including bosmin injection and hemoclipping. No Grade 4 or 5 GI toxicities were observed, and none of these Grade 3 events were fatal. Regarding portal hypertension complications, one patient (1.2%) experienced a fatal esophageal variceal rupture early after treatment (as noted previously). During follow-up, an additional three patients (3.6%) received prophylactic endoscopic ligation for high-risk varices, but no other variceal bleeding events were recorded in the cohort.
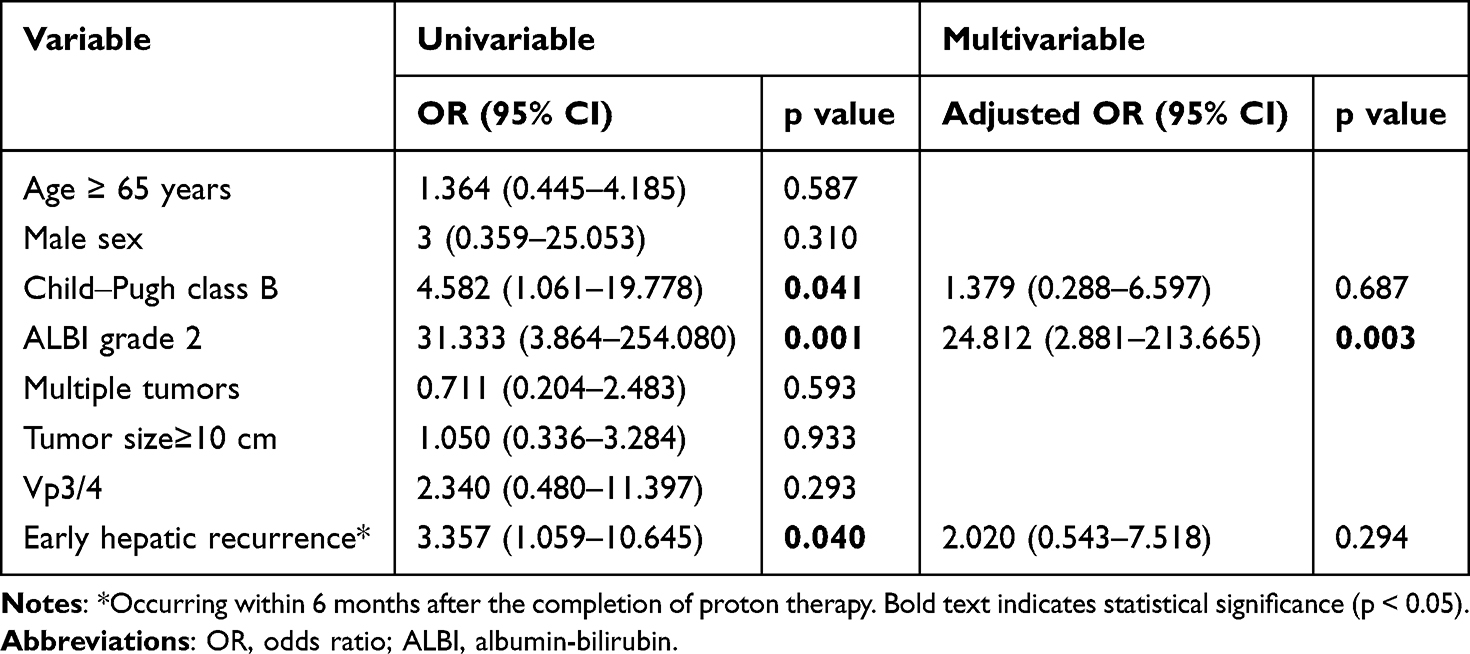 |
Table 5 Multivariable Logistic Regression Analysis of Predictors of Liver Dysfunction |
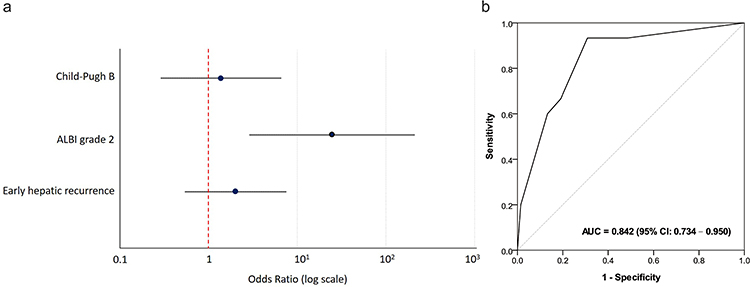 |
Figure 4 Multivariable logistic regression and ROC curve analysis for predictors of post-IMPT liver dysfunction. (a) Forest plot showing the adjusted odds ratios from multivariable logistic regression for liver dysfunction after IMPT. (b) ROC curve for ALBI grade 2 as a predictor demonstrated strong discriminative ability, with an AUC of 0.842 (95% CI: 0.734–0.950). Abbreviations: ALBI, albumin-bilirubin; ROC, receiver operating characteristic; AUC, area under the curve; IMPT, intensity-modulated proton therapy. |
Seven patients (8.4%) underwent curative-intent surgery following IMPT, including five living donor liver transplantations (LDLTs) and two hepatectomies. Two patients developed recurrent disease after undergoing LDLT and subsequently died, while another patient died from pancreatic cancer following LDLT. The remaining four patients were disease free at the time of the study analyses.
Discussion
In this retrospective study, IMPT resulted in excellent locoregional control and favorable survival outcomes in patients with nonmetastatic HCC with PVTT. The median OS was 32.4 months, and the 2-year LC rate reached 88.8%. A CR after IMPT was independently associated with better OS and liver control, while ALBI grade of 2 predicted post-treatment liver dysfunction. Importantly, IMPT enabled curative-intent surgery in a subset of patients, highlighting its potential as a downstaging modality. These findings demonstrate that IMPT can be an effective and well-tolerated therapeutic option for this difficult-to-treat population.
HCC with PVTT is associated with poor prognosis and limited treatment options. Systemic therapy remains the standard first-line approach, yet outcomes are disappointing, particularly for patients with advanced PVTT, who are often excluded from pivotal clinical trials. For example, only 38% of patients in the IMbrave150 trial had macrovascular invasion, and the HIMALAYA trial excluded patients with Vp4 PVTT altogether. In our cohort, 24.1% of patients had Vp4 involvement, and despite this, we observed favorable outcomes that compare favorably with prior reports of RT in similar populations. Previous photon-based RT series reported LC rates of 50–88% and median survival durations of 10–24 months, whereas our study demonstrated superior control and extended survival (Table 6).
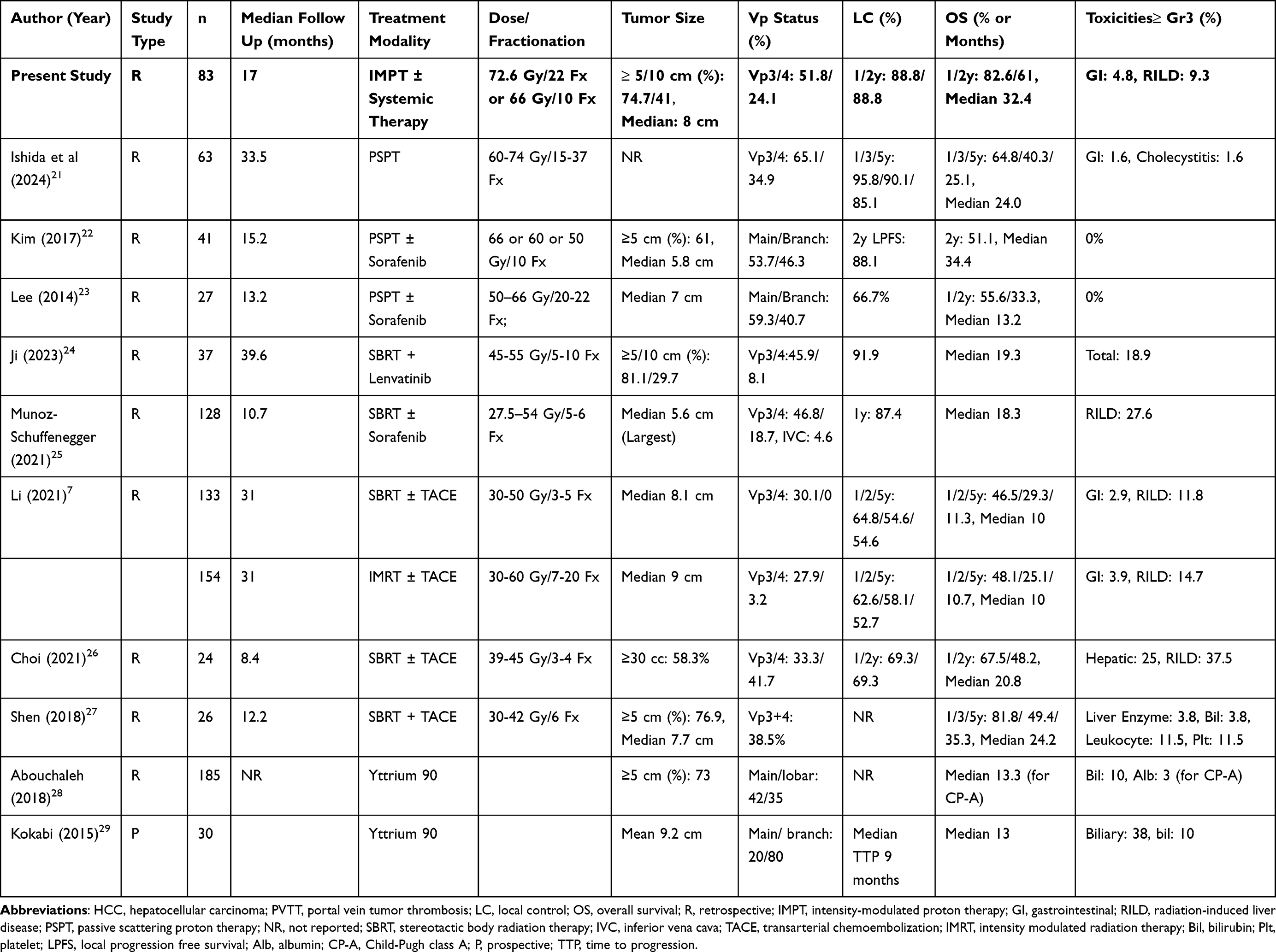 |
Table 6 Clinical Outcomes of Radiotherapy for HCC with PVTT (Publications From the Past 10 years [Post-2014]) |
RT has shown promise in improving outcomes for patients with advanced HCC. Randomized trials such as the Korean study comparing RT plus TACE to sorafenib, and the RTOG1112 trial evaluating SBRT plus sorafenib, demonstrated the superiority of combined approaches over systemic therapy alone.6,30 Meta-analyses further support the integration of local therapy with systemic agents.31 However, patients with Vp4 PVTT remain underrepresented in these studies, and their outcomes with standard systemic therapy alone remain poor. For instance, in the IMbrave150 trial, patients with Vp4 involvement had a median OS of only 7.6 months, compared with 21.1 months in those without.32 In contrast, our study showed a median OS of 37.8 months for Vp4 patients treated with IMPT, suggesting that achieving effective local control can translate into improved survival, even in this high-risk subgroup. Furthermore, our subgroup analysis revealed no significant difference in OS between Vp3 and Vp4 patients (31.7 vs 37.8 months, p=0.461), reinforcing the potential of IMPT to overcome the traditionally poor prognosis associated with main trunk involvement.
IMPT offers dosimetric advantages over photon-based RT by sparing normal liver tissue while delivering ablative doses to tumors. This is particularly important for HCC patients with limited hepatic reserve, in whom the risk of RILD is high. Our findings confirm previous studies showing lower rates of RILD with proton therapy.9,10 Furthermore, our results strongly corroborate the findings of Sanford et al.9 Despite our cohort comprising 100% PVTT patients (compared to 27% with tumor thrombus in their study), we achieved a comparable median overall survival (32.4 months vs 31 months) and a similar 2-year local control rate (88.8% vs 93%). Critically, both studies independently validated the baseline ALBI score as a significant prognostic factor for OS, underlining the robustness of our findings. The incidence of RILD in our cohort was 9.3%, which is substantially lower than the ~30% reported with photon RT in similar populations.25 The use of IMPT, with its enhanced dose conformality and motion management strategies, likely contributed to this favorable toxicity profile.
Another noteworthy finding is the association between CR and survival. Patients achieving CR had significantly improved OS and liver control, emphasizing the importance of achieving a robust radiographic response. This aligns with prior studies demonstrating that early tumor response to RT is a prognostic marker in HCC.33 However, this finding requires prospective validation to confirm the long-term benefit of achieving CR with IMPT and to identify which patients are most likely to achieve this optimal response. Future studies identifying tumor- or patient-specific predictors of CR could help optimize patient selection and personalize treatment.
In our cohort, baseline liver function was a critical determinant of both survival and toxicity. ALBI grade 2 was not only an independent negative prognostic factor for overall survival (HR 2.989, p=0.013), as shown in Table 2, but it was also the only significant predictor of post-treatment liver dysfunction (Adjusted OR 24.812, p=0.003), as detailed in Table 5. Three patients with ALBI grade 2 died from liver decompensation despite no evidence of recurrence. These findings highlight the critical need for pre-treatment risk stratification using ALBI grade. This result provides potential clinical decision-making guidance, suggesting that patients with ALBI grade 2 may require modified treatment strategies, such as more conservative dosing, enhanced liver-sparing techniques, or more intensive post-treatment follow-up to mitigate the risk of severe liver dysfunction.
Importantly, IMPT facilitated tumor downstaging in a subset of patients, enabling curative-intent interventions such as liver transplantation or resection. Seven patients (8.4%) underwent curative-intent surgery after IMPT, four of whom remained disease-free at the time of analysis. This supports the concept that proton therapy, like other liver-directed treatments, can be used in a bridging or downstaging strategy to expand curative opportunities for initially unresectable patients.34–36 Although data are limited, our results add to growing evidence supporting this approach.
In our study, the addition of systemic therapy did not demonstrate a statistically significant OS or PFS benefit. However, this finding must be interpreted with caution and should not be taken as evidence against combination therapy. This lack of statistical significance is likely attributable to small subgroup sizes, heterogeneity in systemic regimens, and limited access to reimbursed immunotherapy during the study period. These factors introduce significant selection bias and severely limit our power to detect a true synergistic effect. Theoretically, the dose-sparing advantages of IMPT may reduce toxicity and permit safer concurrent administration of systemic agents. Furthermore, emerging data suggest proton therapy may reduce radiation-associated lymphopenia, potentially enhancing the efficacy of immune checkpoint inhibitors.37 Therefore, the lack of observed benefit in our cohort should not discourage the integration of IMPT and modern systemic therapies; rather, it highlights the urgent need for multicenter randomized prospective trials to define the optimal combination and sequencing.
To our knowledge, this study includes the largest single-center cohort to date for specifically evaluating the efficacy of IMPT in patients with HCC complicated by PVTT. However, several limitations inherent to its retrospective design must be acknowledged. Firstly, the relatively short follow-up duration for some patients may underestimate late recurrences or toxicities. Secondly, there was no standardization of systemic therapy regimens, and the limited use of contemporary immunotherapy combinations due to reimbursement restrictions hinders our ability to assess synergistic effects with IMPT. Thirdly, while our diagnostic criteria for tumoral PVTT were stringent, relying on definitive MRI features, the lack of pathological confirmation remains a limitation. Although current international guidelines primarily depend on such imaging findings for diagnosis, the theoretical possibility of misclassifying rare cases of bland thrombus cannot be entirely excluded without histology.38 Relatedly, serum D-dimer was not routinely collected, as it is not a primary diagnostic criterion in guidelines and its utility is questionable, as elevated levels may correlate with tumor thrombosis itself.39 In this context, our finding of zero baseline PVCM cases is noteworthy. While PVCM is associated with chronic obstruction, recent evidence suggests it is less common in HCC.40 The absence of PVCM in our cohort is likely attributable to our stringent MRI criteria excluding chronic bland thrombus and relatively early treatment initiation, limiting time for its development. This zero finding of PVCM, along with the fact that no patients were suspected of having concurrent non-tumoral thrombosis or received anticoagulation therapy, strongly supports that our cohort represents active, tumoral PVTT. Finally, selection bias related to the self-funded nature of IMPT and the homogeneous good performance status of our cohort may limit the generalizability of our findings to the broader BCLC C population. These limitations underscore the need for prospective randomized control trials.
The integration of advanced radiotherapy techniques with emerging systemic therapies, including immunotherapy and targeted agents, holds significant promise for improving outcomes in this challenging population. Prospective studies are urgently needed to optimize patient selection and treatment sequencing and develop multidisciplinary strategies to further increase the proportion of HCC patients eligible for potentially curative approaches. Ongoing studies, such as NRG-GI003, are expected to provide high-level evidence regarding the comparative effectiveness of proton versus photon therapy for HCC and may shape future treatment paradigms.
Conclusion
In summary, IMPT demonstrated excellent local control, a favorable safety profile, and potential to enable curative-intent treatments in patients with nonmetastatic HCC with PVTT. A complete response was associated with improved survival, while ALBI grade 2 identified patients at higher risk of liver toxicity. While these findings are based on a retrospective analysis and must be interpreted with caution given the limitations of selection bias and systemic therapy heterogeneity, they support the integration of IMPT into multidisciplinary care for selected patients with advanced HCC. Future prospective studies are warranted to validate these observations and further explore optimal treatment strategies, such as the combined strategy of IMPT with immunotherapy and patient stratification based on predictive biomarkers, to refine patient selection and maximize therapeutic gains.
Abbreviations
ALBI, Albumin-bilirubin; AUC, Area under the curve; BCLC, Barcelona Clinic Liver Cancer; CR, Complete response; CT, Computed tomography; 4D-CT, Four-dimensional computed tomography; GI, Gastrointestinal; HCC, Hepatocellular carcinoma; HR, Hazard ratio; IMPT, Intensity-modulated proton therapy; LC, Local control; LDLT, Living donor liver transplantation; MRI, Magnetic resonance imaging; ORR, Objective response rate; OS, Overall survival; PFS, Progression-free survival; PSPT, Passive scattering proton therapy; PVCM, Portal vein cavernous malformation; PVTT, Portal vein tumor thrombosis; RBE, Relative biological effectiveness; RILD, Radiation-induced liver disease; ROC, Receiver operating characteristic; RT, Radiation therapy.
Acknowledgments
The interim findings of this study were presented orally at the 62nd Annual Conference of the Particle Therapy Cooperative Group in 2024.
The study is partly supported by grants from the Chang Gung Medical Research Fund (CMRPG8N0661 & CMRPG3M1501)
Funding
The study is partly supported by grants from the Chang Gung Medical Research Fund (CMRPG8N0661 & CMRPG3M1501).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca A Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Z-m Z, Lai EC, Zhang C, et al. The strategies for treating primary hepatocellular carcinoma with portal vein tumor thrombus. Int J Surg. 2015;20:8–16. doi:10.1016/j.ijsu.2015.05.009
3. Cheng A-L, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
4. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evidence. 2022;1(8):EVIDoa2100070. doi:10.1056/EVIDoa2100070
5. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
6. Yoon SM, Ryoo BY, Lee SJ, et al. Efficacy and safety of transarterial chemoembolization plus external beam radiotherapy vs sorafenib in hepatocellular carcinoma with macroscopic vascular invasion: a randomized clinical trial. JAMA Oncol. 2018;4(5):661–669. doi:10.1001/jamaoncol.2017.5847
7. Li L-Q, Zhou Y, Huang Y, Liang P, Liang S-X, Su T-S. Stereotactic body radiotherapy versus intensity-modulated radiotherapy for hepatocellular carcinoma with portal vein tumor thrombosis. Hepatol Internat. 2021;15:630–641. doi:10.1007/s12072-021-10173-y
8. Holliday EB, Tao R, Brownlee Z, et al. Definitive radiation therapy for hepatocellular carcinoma with portal vein tumor thrombus. Clin Transl Radiat Oncol. 2017;4:39–45. doi:10.1016/j.ctro.2017.04.003
9. Sanford NN, Pursley J, Noe B, et al. Protons versus photons for unresectable hepatocellular carcinoma: liver decompensation and overall survival. Int J Radiat Oncol Biol Phys. 2019;105(1):64–72. doi:10.1016/j.ijrobp.2019.01.076
10. Cheng J-Y, Liu C-M, Wang Y-M, et al. Proton versus photon radiotherapy for primary hepatocellular carcinoma: a propensity-matched analysis. Radiat Oncol. 2020;15:1–10. doi:10.1186/s13014-020-01605-4
11. Mohan R, Das IJ, Ling CC. Empowering intensity modulated proton therapy through physics and technology: an overview. Int J Radiat Oncol Biol Phys. 2017;99(2):304–316. doi:10.1016/j.ijrobp.2017.05.005
12. Hong TS, Wo JY, Yeap BY, et al. Multi-institutional Phase II study of high-dose hypofractionated proton beam therapy in patients with localized, unresectable hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J Clin Oncol. 2016;34(5):460. doi:10.1200/JCO.2015.64.2710
13. Hilal L, Reyngold M, Wu AJ, et al. Ablative radiation therapy for hepatocellular carcinoma is associated with reduced treatment-and tumor-related liver failure and improved survival. J Gastrointestinal Oncol. 2021;12(4):1743. doi:10.21037/jgo-21-116
14. Yu JI, Park HC. Radiotherapy as valid modality for hepatocellular carcinoma with portal vein tumor thrombosis. World J Gastroenterol. 2016;22(30):6851. doi:10.3748/wjg.v22.i30.6851
15. Liu C-M, Huang B-S, Huang -T-T, Huang E-Y, Wang Y-M, Cheng J-Y. effectiveness of intensity modulated proton therapy for portal vein tumor thrombosis in patients with hepatocellular carcinoma, a single-institutional experience. Int J Part Ther. 2024;12:100135. doi:10.1016/j.ijpt.2024.100135
16. Ikai I, Yamamoto Y, Yamamoto N, et al. Results of hepatic resection for hepatocellular carcinoma invading major portal and/or hepatic veins. Surg Oncol Clin. 2003;12(1):65–75. doi:10.1016/s1055-3207(02)00082-0
17. Mizumoto M, Okumura T, Hashimoto T, et al. Proton beam therapy for hepatocellular carcinoma: a comparison of three treatment protocols. Int J Radiat Oncol Biol Phys. 2011;81(4):1039–1045. doi:10.1016/j.ijrobp.2010.07.015
18. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
19. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Paper presented at: Seminars in liver disease 2010.
20. Pan CC, Kavanagh BD, Dawson LA, et al. Radiation-associated liver injury. Int J Radiat Oncol Biol Phys. 2010;76(3):S94–S100. doi:10.1016/j.ijrobp.2009.06.092
21. Ishida T, Mizumoto M, Saito T, et al. Proton beam therapy for treating patients with hepatocellular carcinoma with major portal vein tumor invasion: a single center retrospective study. Cancers. 2024;16(11):2050. doi:10.3390/cancers16112050
22. Kim DY, Park J-W, Kim TH, et al. Risk-adapted simultaneous integrated boost-proton beam therapy (SIB-PBT) for advanced hepatocellular carcinoma with tumour vascular thrombosis. Radiother Oncol. 2017;122(1):122–129. doi:10.1016/j.radonc.2016.12.014
23. Lee SU, Park J-W, Kim TH, et al. Effectiveness and safety of proton beam therapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Strahlentherapie Onkol. 2014;190(9):806. doi:10.1007/s00066-014-0604-6
24. Ji X, Xu Z, Sun J, Li W, Duan X, Wang Q. Lenvatinib with or without stereotactic body radiotherapy for hepatocellular carcinoma with portal vein tumor thrombosis: a retrospective study. Radiat Oncol. 2023;18(1):1–12. doi:10.1186/s13014-023-02270-z
25. Munoz-Schuffenegger P, Barry A, Atenafu EG, et al. Stereotactic body radiation therapy for hepatocellular carcinoma with macrovascular invasion. Radiother Oncol. 2021;156:120–126. doi:10.1016/j.radonc.2020.11.033
26. Choi HS, Kang KM, Jeong BK, et al. Effectiveness of stereotactic body radiotherapy for portal vein tumor thrombosis in patients with hepatocellular carcinoma and underlying chronic liver disease. Asia-Pacific J Clin Oncol. 2021;17(3):209–215. doi:10.1111/ajco.13361
27. Shen L, Xi M, Zhao L, et al. Combination therapy after TACE for hepatocellular carcinoma with macroscopic vascular invasion: stereotactic body radiotherapy versus sorafenib. Cancers. 2018;10(12):516. doi:10.3390/cancers10120516
28. Abouchaleh N, Gabr A, Ali R, et al. 90Y radioembolization for locally advanced hepatocellular carcinoma with portal vein thrombosis: long-term outcomes in a 185-patient cohort. J Nucl Med. 2018;59(7):1042–1048. doi:10.2967/jnumed.117.199752
29. Kokabi N, Camacho JC, Xing M, et al. Open‐label prospective study of the safety and efficacy of glass‐based yttrium 90 radioembolization for infiltrative hepatocellular carcinoma with portal vein thrombosis. Cancer. 2015;121(13):2164–2174. doi:10.1002/cncr.29275
30. Dawson LA, Winter KA, Knox JJ, et al. Stereotactic body radiotherapy vs sorafenib alone in hepatocellular carcinoma: the NRG oncology/RTOG 1112 phase 3 randomized clinical trial. JAMA Oncol. 2024;11 :136–44.
31. Chen J, He K, Han Y, Guo L, Su K, Wu Z. Clinical efficacy and safety of external radiotherapy combined with sorafenib in the treatment of hepatocellular carcinoma: a systematic review and meta-analysis. Ann Hepatol. 2022;27(4):100710. doi:10.1016/j.aohep.2022.100710
32. Finn RS, Galle PR, Ducreux M, et al. Efficacy and safety of atezolizumab plus bevacizumab versus sorafenib in hepatocellular carcinoma with main trunk and/or contralateral portal vein invasion in IMbrave150. Liver Cancer. 2024;13(6):655–668. doi:10.1159/000539897
33. Wu -Q-Q, Chen Y-X, Du -S-S, Hu Y, Yang P, Zeng Z-C. Early complete tumor response as a survival predictor in hepatocellular carcinoma patients receiving stereotactic body radiation therapy. Clin Transl Radiation Oncol. 2023;39:100465. doi:10.1016/j.ctro.2022.03.010
34. Chen C-L, Ong AD, Cheng J-Y, et al. Proton beam therapy to bridge or downstage locally advanced hepatocellular carcinoma to living donor liver transplantation. Hepatobiliary Surg Nutr. 2022;11(1):103. doi:10.21037/hbsn-21-379
35. Chen C-L, Dungca LBP, Yong -C-C, et al. Proton beam therapy for downstaging hepatocellular carcinoma with lobar portal vein tumor thrombosis to living donor liver transplantation. Hepatobiliary Surg Nutr. 2023;12(6):966. doi:10.21037/hbsn-23-410
36. Kim J, Kim YT, Lee JG, Joo DJ, Seong J. Liver-directed combined radiation therapy for downstaging beyond-milan hepatocellular carcinoma to liver transplantation. Int J Radiat Oncol Biol Phys. 2024;119(4):1171–1178. doi:10.1016/j.ijrobp.2024.01.221
37. De B, Ng SP, Liu AY, et al. Radiation-associated lymphopenia and outcomes of patients with unresectable hepatocellular carcinoma treated with radiotherapy. J Hepatocell Carcinoma. 2021;8:57–69. doi:10.2147/JHC.S282062
38. Lu J, Zhang X-P, Zhong B-Y, et al. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: comparing east and west. Lancet Gastroenterol Hepatol. 2019;4(9):721–730. doi:10.1016/S2468-1253(19)30178-5
39. Kim HK, Lee KR, Yang JH, et al. Plasma levels of D-dimer and soluble fibrin polymer in patients with hepatocellular carcinoma: a possible predictor of tumor thrombosis. Thrombosis Res. 2003;109(2–3):125–129. doi:10.1016/S0049-3848(03)00183-X
40. Attanasi ML, Bou Daher H, Rockey DC. Natural history and outcomes of cavernous transformation of the portal vein in cirrhosis. Dig Dis Sci. 2023;68(8):3458–3466. doi:10.1007/s10620-023-07993-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combining Hepatic Arterial Interventional Therapies with Lenvatinib and Programmed Cell Death-1 Inhibitors for Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis: A Single-Center, Real-World Study
Shen X, Shao T, Yu J, Zhang Z
Journal of Hepatocellular Carcinoma 2025, 12:1267-1278
Published Date: 2 July 2025
Liver Transplantation After Radiotherapy-Antiangiogenesis-Immune Checkpoint Blockade Combination Therapy in Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: A Propensity Score Matching Analysis
Zhao Y, Song J, Li K, Li T, Li W, Yang Y, Tong X, Xiao Y, Xu G, Lu Q, Li G, Li G, Dong J
Journal of Hepatocellular Carcinoma 2026, 13:570163
Published Date: 8 May 2026