Back to Journals » Clinical Ophthalmology » Volume 19
Intense Pulsed Light Combined with Low Level Blue and Red Light Therapy for Demodex-Associated Blepharitis
Authors Farrant S ![]() , Giannaccare G, Lim CHL, Coco G
, Giannaccare G, Lim CHL, Coco G
Received 1 March 2025
Accepted for publication 15 July 2025
Published 7 August 2025 Volume 2025:19 Pages 2575—2585
DOI https://doi.org/10.2147/OPTH.S521989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Sarah Farrant,1 Giuseppe Giannaccare,2 Chris Hong Long Lim,3– 5 Giulia Coco6
1Earlam and Christopher Optometrists Ltd, Taunton, UK; 2Department of Surgical Sciences, Eye Clinic, University of Cagliari, Cagliari, Italy; 3Department of Ophthalmology, National University Hospital, Singapore; 4Ocular Surface Research Group, Singapore Eye Research Institute, Singapore; 5Centre for Sustainable Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 6Ophthalmology Unit, Department of Clinical Sciences and Translational Medicine, University of Rome Tor Vergata, Rome, Italy
Correspondence: Giuseppe Giannaccare, Department of Surgical Sciences, Eye Clinic, University of Cagliari, Cagliari, Italy, Tel +39 3317186201, Email [email protected]
Purpose: Demodex-associated blepharitis is a chronic disease of the lid accounting for over 60% of all blepharitis. Although several therapies have been employed to address Demodex mites’ infestation, there is no universal consensus about the most effective strategy. Purpose of this study was to evaluate the efficacy of combined intense pulsed light (IPL) and low-level light therapy (LLLT) in the treatment of Demodex-associated blepharitis and associated ocular surface disease (OSD).
Patients and Methods: Medical records of patients with Demodex-associated blepharitis resistant to first-line therapy who underwent IPL and LLLT (12 minutes of blue light followed by 12 minutes of red light) were retrospectively examined. The following data collected before treatment (T0) and at last follow-up (T1) were reviewed: collarettes (0– 4 grade); saponification (presence/absence); lid margin telangiectasia (0– 3 grade); conjunctival hyperemia (0– 4 grade); corneal fluorescein staining (CFS) (0– 5 grade); noninvasive tear break-up time (NITBUT), tear meniscus height (TMH), inter-blink interval (IBI), meibomian gland dropout (0– 3 grade) and symptoms (5-item Dry Eye Questionnaire [DEQ-5]). Treatment-related adverse effects (TrAEs) were recorded.
Results: Data from 34 eyes of 17 patients (3 males, 14 females; mean age 64.6± 10.0 years) were included. A mean of 7.6 ± 3.6 treatment sessions of IPL and LLLT was performed. Mean score of collarettes decreases significantly from 1.44 ± 0.83 at T0 to 1.00 ± 0.97 at T1 (p = 0.007). The rate of eyes with saponification decreases significantly (from 41.18% to 11.76%; p = 0.002). Conjunctival hyperemia significantly decreased from 2.00 ± 0.78 to 1.47 ± 0.61 (p = 0.005). Mean CFS score decreased significantly from 0.56 ± 1.16 to 0.24 ± 0.96 (p = 0.031). Symptoms’ mean score improved significantly after treatment (from 12.00 ± 5.34 to 7.76 ± 4.92; p = 0.003). No patient reported TrAEs.
Conclusion: Combined light therapy with IPL and LLLT employing blue and red lights is an effective treatment strategy for patients with recalcitrant Demodex-associated blepharitis to reduce mites count and improve main ocular surface parameters along with patients’ symptoms.
Keywords: Demodex, dry eye, IPL, LLLT, meibomian gland dysfunction, MGD
Introduction
Demodex-associated blepharitis is a chronic disease of the lid margin determined by Demodex mites’ infestation, reported in approximately 58% of patients presenting to an outpatient clinic, and affecting around 25 million Americans.1 Demodex mites are the most common ectoparasites living on human skin and eyelids; they can reside in clusters around the lash root and lash follicle where they feed on sebum and follicular epithelial cells.2 Demodex-associated blepharitis may account for over 60% of all blepharitis.3,4 Prevalence of Demodex increases with age, and it is estimated to affect approximately 80% of people older than 60 years reaching 100% by the age of 70,5 with similar prevalence according to sex and ethnicity.1,3
Demodex mites may cause direct mechanical damage because of burrowing and laying eggs, together with irritation, inflammation and hypersensitivity reactions on the ocular surface due to the release of several chemicals, among which digestive enzymes, that break down epithelial cells used as food.2 Additionally, Demodex mites may favor bacterial overgrowth from harboring and being vectors for bacteria,2,6,7 and high numbers of mites have been associated with reactive conjunctivitis and keratitis.8 Nearly all patients with Demodex-associated blepharitis are symptomatic, and the vast majority (>95%) experience three or more symptoms among itching, more frequently at night and/or early morning, dry eyes, foreign body sensation, contact lenses intolerance, redness, burning, tearing, discharge, pain, and blurred vision.1,3,9–14
Demodex blepharitis is frequently intertwined with dry eye disease (DED) since 60–70% of DED patients also have Demodex blepharitis. In fact, alterations in the tear film may make the ocular surface environment more hospitable for Demodex mites thus facilitating infestations; simultaneously, the overgrowth of Demodex mites may exacerbate symptoms of ocular surface disease (OSD).1,14 Other common associations include meibomian gland dysfunction (MGD), ocular rosacea, chalaza, hordeola and pterygia.15,16
Over the years, several treatment strategies have been employed to address mites’ infestation and provide symptoms relief, but none proved to be clearly effective for Demodex blepharitis.9,17 The recent FDA approved lotilaner ophthalmic solution 0.25% has been reported to address Demodex mites’ infestation, but no data regarding other ocular surface signs or symptoms are available.18,19 However, given Demodex blepharitis is frequently associated with OSD, treatment strategies that address at the same time the overall ocular surface status and Demodex infestation may better and more comprehensively ameliorate patients’ signs and symptoms.
Combined light therapies using intense pulse light (IPL) and light modulation (LM) low level light therapy (LLLT) with blue/red lights may potentially conjugate the well-known advantages of IPL in killing mites and improving MGD function,20–23 with the advantages of blue light, which stimulates porphyrins and creates an anti-bacterial action,24,25 and red light, which stimulates adenosine triphosphate (ATP) production by increasing and improving cellular activity, reducing inflammation and oedema.24,25
The purpose of the present study was to evaluate the outcomes of combined IPL and LLLT with blue/red lights on signs and symptoms of patients with Demodex-associated blepharitis in a real-life setting.
Materials and Methods
The study followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Earlam and Christopher Optometrists Ltd, Taunton, United Kingdom, with a waiver of specific informed consent, as all patients had previously provided general written consent for the use of their clinical data in research. None of the authors participated in the approval process. All patient data were anonymized prior to analysis to ensure confidentiality, and no personally identifiable information was collected or stored. Data handling was conducted in full compliance with applicable data protection regulations.
Retrospective study in which medical records of patients who underwent combined light therapies with IPL and LM LLLT with blue and red lights for Demodex-associated blepharitis between June 2020 and October 2023 at Earlam and Christopher Optometrists Ltd (Taunton, UK) were examined to determine the efficacy of the treatment in reducing Demodex mites’ counts and signs and symptoms of OSD.
The inclusion criterion was the presence of Demodex-associated blepharitis refractory to first line therapy consisting of over-the-counter topical medicine with a low concentration of tea tree oil or hypochlorous-based acid in the form of scrub, spray or cleansing wipe. The diagnosis was reached clinically through the detection at the slit-lamp examination of the pathognomonic collarettes that were defined as the presence of cylindrical, waxy debris located at the base of the eyelashes, typically formed by undigested material, epithelial cells, keratin, digestive enzymes, dead or living mites, and eggs and/or egg casings.8,26–28 Patients were excluded in case of (1) systemic, facial or ocular acute inflammation, (2) systemic or ocular uncontrolled diseases, (3) ocular dermatosis within the previous month, (4) allergic diseases within the previous month, (5) eye surgery within the previous three months, (6) lid malposition or exophthalmos, (7) excessive sun exposure within the previous month, (8) Fitzpatrick skin types V and VI for the risk of skin depigmentation,29,30 (9) pregnancy or breastfeeding, and (10) incomplete data from medical charts.
Treatment
The Eye-light® device (Espansione Marketing S.p.A., Bologna, Italy), which is CE marked for the treatment of MGD, was used in all patients while continuing their first-line tailored home regime.
Treatment protocols included both Optimal Power Energy OPE™ IPL and Light Modulation LM™ LLLT with blue and red light. Briefly, OPE™ IPL employed a polychromatic light (600–1200 nm) with energy range of 4.5–8.2 J/cm2 and was performed without the use of a protective gel since the software-enabled technology and the thermal filter guaranteed the light impulse emission to be always at the right frequency, making the procedure safe and effective. Protective eye goggles were placed over the eyes and 5 flashes of light were applied for each eye without overlap (3 along the inferior orbital rim, 1 at the lateral canthus, and 1 applied horizontally along the inferior orbital rim). An automated software adjusted the therapeutic energy level based on the degree of skin pigmentation chosen by the practitioner according to Fitzpatrick Scale. The LM™ LLLT treatment was performed applying first the blue light (465 ± 40 nm) delivered through the blue mask for 12 minutes, and then the red light (625 ± 40 nm) delivered through the red mask for additional 12 minutes. No eye shields were used for this treatment, and patients were instructed to keep their eye closed to ensure a complete treatment of the upper and lower eyelids. Treatment was repeated at variable frequencies according to patients’ response.
Data Collection
Demographical and clinical data collected at baseline before treatment (T0) and at last follow-up (T1) were reviewed. Collarettes were graded clinically, and a 0–4 scale was used according to Gao et al and Hosseini et al27,31 Specifically, eyes were given grade 0 if only 0–2 lashes per eyelid had collarettes, grade 1 if 3–10 lashes per eyelid had collarettes, grade 2 if >10 but < 1/3 of the lashes per eyelid had collarettes, grade 3 if ≥ 1/3 but < 2/3 of the lashes per eyelid had collarettes and grade 4 if ≥ 2/3 of the lashes per eyelid had collarettes. Demodex eradication was defined as collarettes grade 0 after treatment. Presence of saponification was recorded. It was defined as the presence of a foamy, soapy material at the eyelid margin and was considered a sign of poor quality meibum resulting from Demodex enzymes reacting with tear lipids.32 Lid margin telangiectasia was graded on a 4-point scale. Specifically, grade 0 was used for no or mild redness in the lid margin conjunctiva and no telangiectasia crossing the meibomian gland orifices, 1 for redness in the lid margin conjunctiva and no telangiectasia crossing the meibomian gland orifices, 2 for redness in the lid margin conjunctiva and telangiectasia crossing the meibomian gland orifices involving less than ½ of the lid length, 3 for redness in the lid margin conjunctiva and telangiectasia crossing the meibomian gland orifices involving half or more of the lid length.33
The all-in-one MYAH device (Topcon, Visia Imaging, Japan) was used to collect data on: (1) noninvasive tear break-up time (NITBUT); (2) tear meniscus height (TMH); (3) inter-blink interval (IBI), defined as the mean time between two blinks; (4) inferior eyelid infrared meibography for scoring the extent of meibomian glands (MG) dropout a 0-3-point scale: 0 = no dropout; 1 = less than 1/3; 2 = 1/3–2/3; and 3 = more than >2/3.34 Conjunctival hyperemia was graded clinically according to Efron scale (0–4 point).35 Corneal fluorescein staining (CFS) was measured after instilling one drop of fluorescein into the lower conjunctival sac using a moist fluorescein strip according to the Oxford grading scheme.36 The severity of ocular surface symptoms was measured using the 5-item Dry Eye Questionnaire (DEQ-5). It consists of 5 questions on frequency and severity of DED symptoms of ocular discomfort, dryness, and tearing over a one-month recall period. The total score ranges from 0 to 22 and a DEQ-5 score of ≥6 indicates pathological symptoms.37 Treatment-related adverse effects (TrAEs) were recorded in patients’ charts.
Statistical Analysis
Data are presented as the mean ± standard deviation (SD) with 95% confidence intervals [95% CI], median and interquartile (IQR) range or as percentages for categorical variables. Clinical data were compared before and after treatment. Shapiro–Wilk test was used to test for data distribution. Since not all data followed a normal distribution, matched-paired Wilcoxon signed rank test was used for continuous variables and McNemar test was used for dichotomous variables. All statistical analyses were performed using STATA 18.0 (StataCorp, College Station, TX) and a p-value of less than 0.05 was considered statistically significant.
Results
Seventeen patients (34 eyes) with a mean age of 64.6 ± 10.0 years [range 48–83 years; median (IQR): 63 (14.5)] and of whom 77.8% females (n =14) were included. Patients received a mean of 7.6 ± 3.6 IPL and LLLT treatment sessions performed 4.3 ± 3 months apart, and last follow-up visit (T1) was performed at 25.5 ±12.2 weeks from the last treatment session. Changes of clinical parameters from T0 to T1 are shown in Table 1. Mean score of collarettes decreases significantly from 1.44 ± 0.83, 95% CI [1.15;1.73] at T0 to 1.00 ± 0.97, 95% CI [0.66;1.34] at T1 (p = 0.007). At T0, all eyes showed Demodex collarettes, which were above grade 1 in 10 eyes (29.4%). At T1, Demodex mites’ reduction of at least 1-point-scale was noted in 64.7% (n = 22) of eyes, while Demodex eradication was observed in 17.6% of cases. At T0, 41.18% (n = 14) 95% CI [23.7%;58.6%] of eyelid margins showed saponification; this rate significantly decreased to 11.76% [0.3%;23.2%] at T1 (p = 0.002). Although telangiectasia did not show significant changes from T0 to T1, its score improved in 17.6% of eyes (n = 6), while worsened in 5.9% (n = 2) and remained unchanged in all the other cases (76.5%). Conjunctival hyperemia significantly decreased from 2.00 ± 0.78 [1.73;2.27] at T0 to 1.47 ± 0.61 [1.26;1.69] after treatment (p = 0.005), improving in 35.3% of eyes (n = 12), while worsening in 5.9% (n = 2).
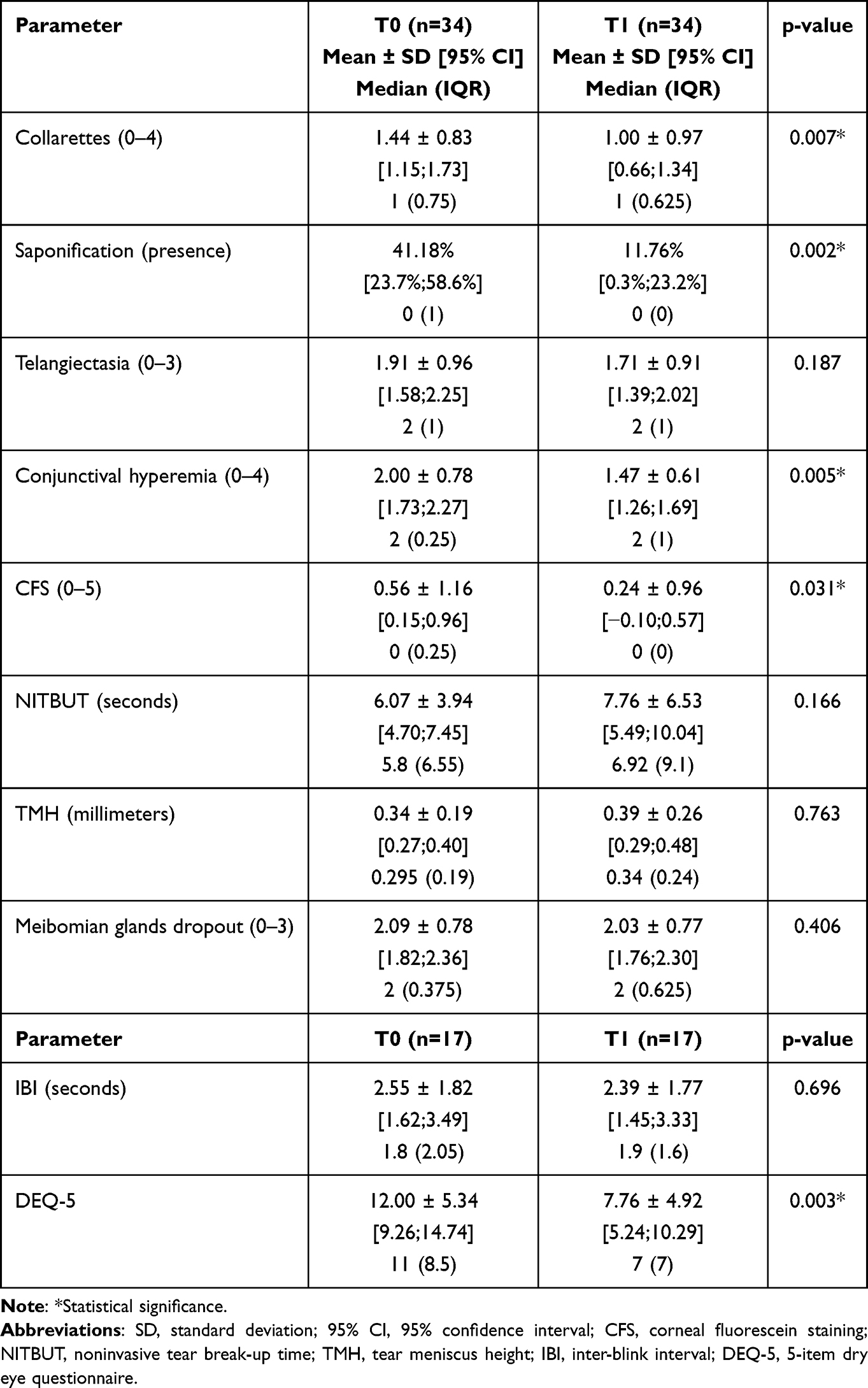 |
Table 1 Means, Standard Deviations and 95% Confidence Intervals of Data Collected at Baseline (T0) and After Treatment at the Last Follow-Up Visit (T1) |
At T0, 23.5% of eyes had positive CFS with an overall mean CFS score of 0.56 ± 1.16 [0.15;0.96] that decreased to 0.24 ± 0.96 [−0.10;0.57]at T1 (p = 0.031), remaining positive in 5.9% (n = 2).
Although NIBUT did not show significant changes from T0 to T1, its value improved in 65% of eyes (n = 22) by an average of 1.7 ± 7.5 sec [−4.32; +0.94]. No significant changes were recorded for TMH, infrared meibography or inter-blink interval (always p > 0.406).
Mean score of symptoms measured by the DEQ-5 showed significant changes after treatment (from 12.00 ± 5.34 [9.26;14.74] at T0 to 7.76 ± 4.92 [5.24;10.29] at T1; p = 0.003), and overall symptoms’ improvement was experienced by 82.4% (n = 14) of patients. No patient reported TrAEs during or after each session. Slit-lamp photographs taken in patients #5 and #12 before and after study treatment showing improvements in collarettes and saponification, respectively, are shown in Figure 1. Detailed demographical and clinical characteristics of each patient, number and frequency of treatments, length of observation and trend of changes for all parameters are shown in Table 2.
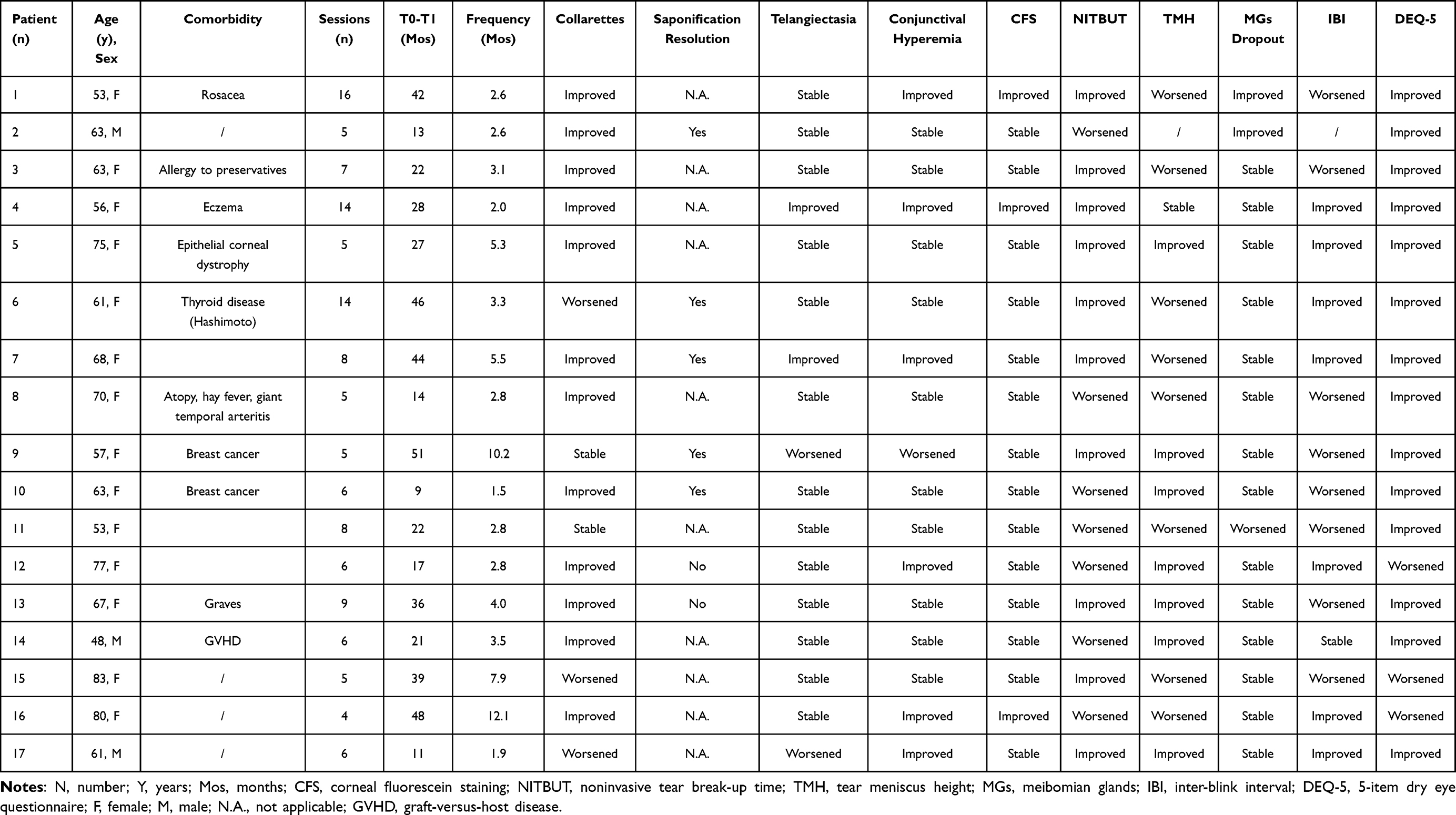 |
Table 2 Demographical and Clinical Characteristics of Each Patient, Number and Frequency of Treatments, Length of Observation and Trend of Changes for All Parameters |
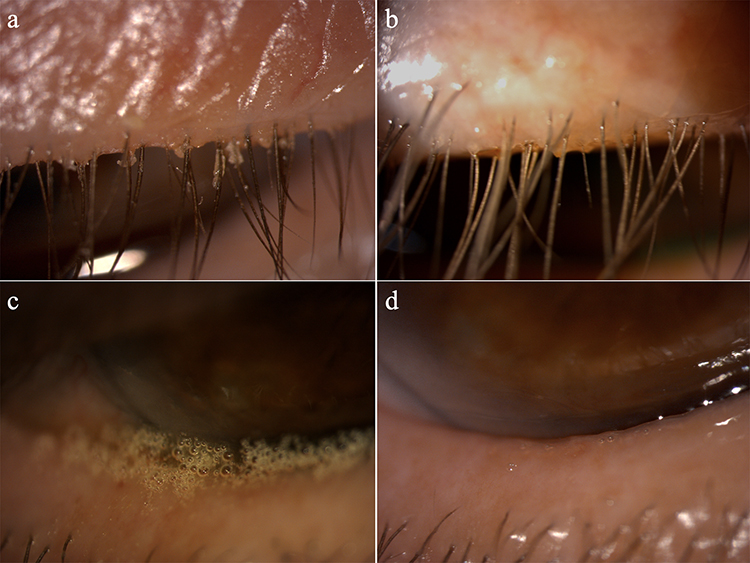 |
Figure 1 Slit lamp photographs of representative patients before and after treatment. (a) Collarettes of patient n.5 at T0 (grade 3). (b) Collarettes of patients n.5 at T1 (grade 1) after five sessions of intense pulsed light (IPL) and low level light therapy (LLLT). (c) Saponification of patient n.12 at T0. (d) Marked reduction in saponification in patient n.12 at T1 after six sessions of IPL and LLLT. Original magnification: ×16. |
Discussion
Demodex blepharitis is a common clinical finding and more than 77% of patients reports a negative impact of this condition on their daily lives.1,9,38 It is frequently intertwined with other OSDs, with 60–70% of DED patients and 85% of MGD patients suffering from Demodex blepharitis.14,39
The present study showed that the combined use of IPL and LLLT was able to significantly decrease Demodex mites’ infestation, with a reduction of collarettes grade in 58.8% of cases. Saponification on the eyelid margin resolved in 71% of cases; in parallel, significant improvements were detected in other ocular surface parameters, as demonstrated by the significant improvement in CFS, conjunctival hyperemia and, most importantly, patients’ symptoms.
IPL has previously been shown to be effective in reducing Demodex counts and improving MG function.20–23 This technique was initially developed as in-office procedure to treat skin conditions, and it seemed to coagulate Demodex mites one week after treatment while preserving the hair follicle structure.40,41 After the anecdotal finding that patients with rosacea receiving IPL showed improvements in ocular discomfort symptoms,42 its use was then applied to the ophthalmic field, determining the reduction of mites counts and the improvement of MG function, among others.20–23 The mechanism of action on MG function has not been fully elucidated; presumably, IPL provides thermal action by increasing the temperature in the vessels within the lid, thus heating meibum and facilitating its expression; simultaneously, it may also coagulate telangiectatic vessels thereby decreasing inflammatory mediators.43
The efficacy of IPL in the treatment of Demodex blepharitis was compared by Zhang et al to 5% tea tree oil (TTO) and, although no significant differences were noted between treatments, Demodex eradication rate was higher in the IPL group, being 55% one month after treatment and reaching 100% at 3 months.23 Interestingly, ocular discomfort symptoms, break-up time and meibum quality showed better results after IPL, highlighting its preferably therapeutic potential for ocular Demodicosis. A few studies also employed a combination of IPL and MG expression (MGX) to improve MG function.44–46 However, MGX may cause pain and can be scarcely tolerated by patients. Craig et al showed IPL alone to be effective in ameliorating signs and symptoms in patients with DED.21
More recently, LLLT demonstrated its potential as a treatment for ocular surface diseases, by acting through tissue photobiomodulation47 and resulting in overall improvements in cellular function with impact on wound healing,48 pain modulation49 and normalization of cell function.50,51 LLLT initial applications were studied in combination with IPL on recalcitrant MGD cases. Combined IPL/LLLT showed to improve patients’ symptoms, break-up time, MG grading and MG expressibility score.47,52 Additionally, combined IPL/LLLT showed to reduce tear fluid inflammatory markers such as interleukin-1β, interleukin-17F, MMP9 together with the MMP9/TIMP1 ratio and ocular surface B-cell proportions.52 The comparison between IPL and LLLT in DED owing to MGD showed that LLLT determined significantly greater improvements in symptoms scores, being also the only treatment able to increase TMH.53
The above-mentioned studies employed LLLT protocols with the sole use of the red light, taking advantages of its ability to improve cellular metabolism by increasing ATP production within mitochondria, reduce inflammation by regulating antioxidant defenses, mitigate oxidative stress and activate transcription factors and signaling pathways.54–56 Current LLLT protocols also employ the blue light to exploit its targeted action on Demodex-associated blepharitis due to its efficacy in bacteria elimination and microbiome stabilization.57,58 In fact, the blue light energy is absorbed by porphyrins within bacteria, generating singlet oxygen radicals that cause damage to the cell wall of gram-positive bacteria leading to cell death.24,25 In this context, the relatively weak bacterial defense mechanism against singlet oxygen-induced damage contributes to the high efficiency of the photodynamic inactivation.59
Several other treatment options may be considered in patients with Demodex-associated blepharitis; however, they may be uncomfortable, may come with side effects or may require daily use for 1–3 months to achieve both mites’ death and mating prevention, thus making patients’ compliance potentially suboptimal.60 Daily scrubs with TTO and its derivatives, especially with terpinen-4-ol (T40), besides showing uncertain efficacy in mites’ eradication, may be inconvenient for patients and contact dermatitis, ocular irritation, allergic reactions, epithelial cell toxicity, MG toxicity, strong odor and long treatment duration have all being reported with their use.26,61–68 Ivermectin and metronidazole use may be limited due to hypersensitivity reactions, drug interactions and severe side effects reported with oral use.63,69,70 Microblepharoexfoliation (MBE) alone do not reach mites’ eradication, and its use should be combined with daily home-based lid hygiene procedures.61,71,72 Additionally, the recently FDA-approved lotilaner ophthalmic solution 0.25% demonstrated high efficacy in Demodex mites and collarettes eradication as well as erythema reduction, with most reported side effect being instillation site pain; however, no additional benefit on ocular surface signs and symptoms has been reported and it is not yet available worldwide.18,19
Considering the challenges of compliance and side effects across this vast armamentarium of therapies, the significant reduction in Demodex collarettes score, coupled with overall improvements in OSD signs and symptoms and the absence of reported side effects, makes combined light therapy with IPL and LLLT a promising option for patients with symptomatic Demodex blepharitis who are refractory to first-line treatments such as over-the-counter topical tea tree oil or hypochlorous acid, which still retain the advantage of wide availability. Additionally, although the mite eradication rate was low, the significant reduction in collarettes score following treatment appears clinically meaningful. Higher Demodex infestation levels have been positively correlated with more severe structural damage to the meibomian glands,39 and it is hypothesized that Demodex must reach a certain threshold before causing a decrease in meibomian gland acinar density, thereby initiating glandular damage.39 Furthermore, symptoms of ocular irritation have been shown to correlate with higher mean Demodex densities, whereas asymptomatic patients tend to exhibit lower mean densities.73
The main limitation of the present study lies in its retrospective, real-world design. Patients followed individualized home regimens without a standardized treatment schedule, and no sham treatment was included, an omission known to potentially account for minor observed improvements, especially when subjective assessments exceed objective clinical findings.74,75 Both numbers and time-lapse in-between sessions varied on an individual basis based on clinical response. Without a fixed follow-up schedule, it is difficult to determine the precise duration of treatment efficacy; therefore, we can only estimate an approximate efficacy period of 4.3 ± 3 months per patient. Furthermore, last follow-up visit was not performed after a fixed interval from the last treatment session, and it is conceivable that the low eradication rate reached in our cohort may depend either on a too early or late assessment. On the one hand previous studies showed a Demodex eradication rate around 27% at 1 week after the last IPL treatment that increased further from 1 to 3 months post-treatment.22,46 On the other hand, Demodex blepharitis is a chronic and recurrent disease, in which although mites may be eradicated, re-infestations can occur again.10 The small number of eyes treated and analyzed represents another limitation and might have avoided reaching statistical significance for some parameters, such as NITBUT and TMH that showed non-significant increases. Furthermore, identification of Demodex mites and collarettes grading was performed through clinical examination only. Previous studies identified Demodex mites by eyelashes epilation followed by their exam under a light microscope or by in-vivo confocal microscopy.22,46 However, these techniques are often impractical in routine clinical practice, and the detection of collarettes at the slit-lamp examination can be considered pathognomonic.26
Conclusion
Based on the results of the present study, combined light therapy with IPL and LLLT employing both blue and red lights seems an effective treatment strategy for patients with recalcitrant Demodex-associated blepharitis to reduce collarettes score and saponification while also improving main ocular surface parameters and patients’ symptoms. Further well-designed prospective studies are required to better investigate and confirm these preliminary results.
Abbreviations
IPL, intense pulsed light; LLLT, low-level light therapy; DEQ-5, 5-item Dry Eye Questionnaire; CFS, corneal fluorescein staining; NITBUT, noninvasive tear break-up time; TMH, tear meniscus height; IBI, inter-blink interval; TaAEs, Treatment-related adverse effects; DED, dry eye disease; OSD, ocular surface disease; MGD, meibomian gland dysfunction; LM, light modulation; ATP, adenosine triphosphate; OPE, Optimal Power Energy; SD, standard deviation; TTO, tea tree oil; MGX, meibomian glands expression; MBE, microblepharoexfoliation.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was approved by the Institutional Review Board of Earlam and Christopher Optometrists Ltd, Taunton, United Kingdom, with a waiver of specific informed consent, as all patients had previously provided general written consent for the use of their clinical data in research. None of the authors participated in the approval process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Sarah Farrant, Giuseppe Giannaccare, Chris Hong Long Lim and Giulia Coco received speaker honorarium from Espansione Marketing S.p.A. Ms Sarah Farrant is also a key opinion leader for Topcon, Espansione; consultant for Scope Ophthalmics, Thea pharmaceuticals; and a company director for SOS Ophthalmics. The authors report no other conflicts of interest in this work.
References
1. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153–1164. doi:10.2147/OPTH.S354692
2. Fromstein SR, Harthan JS, Patel J, Opitz DL. Demodex blepharitis: clinical perspectives. Clin Optom (Auckl). 2018;10:57–63. doi:10.2147/OPTO.S142708
3. Biernat MM, Rusiecka-Ziółkowska J, Piątkowska E, Helemejko I, Biernat P, Gościniak G. Occurrence of Demodex species in patients with blepharitis and in healthy individuals: a 10-year observational study. Jpn J Ophthalmol. 2018;62(6):628–633. doi:10.1007/S10384-018-0624-3
4. Kabataş N, Doǧan AŞ, Kabataş EU, Acar M, Biçer T, Gürdal C. The effect of demodex infestation on blepharitis and the ocular symptoms. Eye Contact Lens. 2017;43(1):64–67. doi:10.1097/ICL.0000000000000234
5. Cheng AMS, Sheha H, Tseng SCG. Recent advances on ocular Demodex infestation. Curr Opin Ophthalmol. 2015;26(4):295–300. doi:10.1097/ICU.0000000000000168
6. Liu J, Sheha H, Tseng SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10(5):505–510. doi:10.1097/ACI.0B013E32833DF9F4
7. Luo X, Li J, Chen C, Tseng S, Liang L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;36(Suppl 1):S9–S14. doi:10.1097/ICO.0000000000001361
8. Rabensteiner DF, Aminfar H, Boldin I, et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am J Ophthalmol. 2019;204:7–12. doi:10.1016/J.AJO.2019.03.007
9. Barnett M, Simmons B, Vollmer P, et al. The impact of Demodex blepharitis on patient symptoms and daily life. Optom Vis Sci. 2024;101(3):151–156. doi:10.1097/OPX.0000000000002111
10. Ayres BD, Donnenfeld E, Farid M, et al. Clinical diagnosis and management of Demodex blepharitis: the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). Eye. 2023;37(15):3249–3255. doi:10.1038/S41433-023-02500-4
11. O’dell L, Dierker DS, Devries DK, et al. Psychosocial impact of Demodex blepharitis. Clin Ophthalmol. 2022;16:2979–2987. doi:10.2147/OPTH.S374530
12. Jalbert I, Rejab S. Increased numbers of Demodex in contact lens wearers. Optom Vis Sci. 2015;92(6):671–678. doi:10.1097/OPX.0000000000000605
13. Siddireddy JS, Vijay AK, Tan J, Willcox M. The eyelids and tear film in contact lens discomfort. Cont Lens Anterior Eye. 2018;41(2):144–153. doi:10.1016/J.CLAE.2017.10.004
14. Cheng AM, Hwang J, Dermer H, Galor A. Prevalence of ocular demodicosis in an older population and its association with symptoms and signs of dry eye. Cornea. 2021;40(8):995–1001. doi:10.1097/ICO.0000000000002542
15. Schear MJ, Milman T, Steiner T, Shih C, Udell IJ, Steiner A. The association of Demodex with chalazia: a histopathologic study of the eyelid. Ophthalmic Plast Reconstr Surg. 2016;32(4):275–278. doi:10.1097/IOP.0000000000000500
16. Tarkowski W, Moneta-Wielgoś J, Młocicki D. Do Demodex mites play a role in pterygium development? Med Hypotheses. 2017;98:6–10. doi:10.1016/J.MEHY.2016.09.003
17. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49(8):311–318. doi:10.1097/ICL.0000000000001003
18. Yeu E, Wirta DL, Karpecki P, Baba SN, Holdbrook M. Lotilaner ophthalmic solution, 0.25%, for the treatment of Demodex blepharitis: results of a prospective, randomized, vehicle-controlled, double-masked, pivotal trial (Saturn-1). Cornea. 2023;42(4):435–443. doi:10.1097/ICO.0000000000003097
19. Gaddie IB, Donnenfeld ED, Karpecki P, et al. Lotilaner ophthalmic solution 0.25% for Demodex blepharitis: randomized, vehicle-controlled, multicenter, phase 3 trial (Saturn-2). Ophthalmology. 2023;130(10):1015–1023. doi:10.1016/J.OPHTHA.2023.05.030
20. Huang X, Qin Q, Wang L, Zheng J, Lin L, Jin X. Clinical results of intraductal meibomian gland probing combined with intense pulsed light in treating patients with refractory obstructive meibomian gland dysfunction: a randomized controlled trial. BMC Ophthalmol. 2019;19(1):211. doi:10.1186/S12886-019-1219-6
21. Craig JP, Chen YH, Turnbull PRK. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2015;56(3):1965–1970. doi:10.1167/IOVS.14-15764
22. Cheng SN, Jiang FG, Chen H, Gao H, Huang YK. Intense pulsed light therapy for patients with meibomian gland dysfunction and ocular Demodex infestation. Curr Med Sci. 2019;39(5):800–809. doi:10.1007/S11596-019-2108-1
23. Zhang XZ, Song N, Gong L. Therapeutic effect of intense pulsed light on ocular demodicosis. Curr Eye Res. 2019;44(3):250–256. doi:10.1080/02713683.2018.1536217
24. Sułek A, Pucelik B, Kobielusz M, Barzowska A, Dąbrowski JM. Photodynamic inactivation of bacteria with porphyrin derivatives: effect of charge, lipophilicity, ROS generation, and cellular uptake on their biological activity in vitro. Int J Mol Sci. 2020;21(22):1–34. doi:10.3390/IJMS21228716
25. Malik Z, Hanania J, Nitzan Y. Bactericidal effects of photoactivated porphyrins--an alternative approach to antimicrobial drugs. J Photochem Photobiol B. 1990;5(3–4):281–293. doi:10.1016/1011-1344(90)85044-W
26. Savla K, Le JT, Pucker AD. Tea tree oil for Demodex blepharitis. Cochrane Database Syst Rev. 2020;6(6):CD013333. doi:10.1002/14651858.CD013333.PUB2
27. Gao YY, Di Pascuale MA, Li W, et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci. 2005;46(9):3089–3094. doi:10.1167/IOVS.05-0275
28. Aumond S, Bitton E. Palpebral and facial skin infestation by Demodex folliculorum. Cont Lens Anterior Eye. 2020;43(2):115–122. doi:10.1016/J.CLAE.2019.09.001
29. Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124(6):869–871. doi:10.1001/ARCHDERM.124.6.869
30. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41–46. doi:10.1089/PHO.2014.3819
31. Hosseini K, Bourque LB, Hays RD. Development and evaluation of a measure of patient-reported symptoms of Blepharitis. Health Qual Life Outcomes. 2018;16(1):11. doi:10.1186/S12955-018-0839-5
32. Epstein A, Pang L, Najafi-Tagol K, Najafi R, Stroman D, Debabov D. Comparison of bacterial lipase activity in the presence of eye lid cleansers. Invest Ophthalmol Vis Sci. 2015;7(56):4446.
33. Arita R, Minoura I, Morishige N, et al. Development of definitive and reliable grading scales for meibomian gland dysfunction. Am J Ophthalmol. 2016;169:125–137. doi:10.1016/J.AJO.2016.06.025
34. Srinivasan S, Menzies K, Sorbara L, Jones L. Infrared imaging of meibomian gland structure using a novel keratograph. Optom Vis Sci. 2012;89(5):788–794. doi:10.1097/OPX.0B013E318253DE93
35. Efron N, Morgan PB, Katsara SS. Validation of grading scales for contact lens complications. Ophthalmic Physiol Optics. 2001;21(1):17–29. doi:10.1046/J.1475-1313.2001.00575.X
36. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
37. Chalmers RL, Begley CG, Caffery B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont Lens Anterior Eye. 2010;33(2):55–60. doi:10.1016/J.CLAE.2009.12.010
38. Zhang AC, Muntz A, Wang MTM, Craig JP, Downie LE. Ocular Demodex: a systematic review of the clinical literature. Ophthalmic Physiol Opt. 2020;40(4):389–432. doi:10.1111/OPO.12691
39. Cheng S, Zhang M, Chen H, Fan W, Huang Y. The correlation between the microstructure of meibomian glands and ocular Demodex infestation: a retrospective case-control study in a Chinese population. Medicine. 2019;98(19):e15595. doi:10.1097/MD.0000000000015595
40. Raulin C, Goldman MP, Weiss MA, Weiss RA. Treatment of adult port-wine stains using intense pulsed light therapy (PhotoDerm VL): brief initial clinical report. Dermatol Surg. 1997;23(7):594–597. doi:10.1111/J.1524-4725.1997.TB00698.X
41. Prieto VG, Sadick NS, Lloreta J, Nicholson J, Shea CR. Effects of intense pulsed light on sun-damaged human skin, routine, and ultrastructural analysis. Lasers Surg Med. 2002;30(2):82–85. doi:10.1002/LSM.10042
42. Papageorgiou P, Clayton W, Norwood S, Chopra S, Rustin M. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol. 2008;159(3):628–632. doi:10.1111/J.1365-2133.2008.08702.X
43. Dell SJ. Intense pulsed light for evaporative dry eye disease. Clin Ophthalmol. 2017;11:1167–1173. doi:10.2147/OPTH.S139894
44. Gupta PK, Vora GK, Matossian C, Kim M, Stinnett S. Outcomes of intense pulsed light therapy for treatment of evaporative dry eye disease. Can J Ophthalmol. 2016;51(4):249–253. doi:10.1016/J.JCJO.2016.01.005
45. Yan X, Hong J, Jin X, et al. The efficacy of intense pulsed light combined with meibomian gland expression for the treatment of dry eye disease due to meibomian gland dysfunction: a multicenter, randomized controlled trial. Eye Contact Lens. 2021;47(1):45–53. doi:10.1097/ICL.0000000000000711
46. Huo Y, Mo Y, Wu Y, Fang F, Jin X. Therapeutic effect of intense pulsed light with optimal pulse technology on meibomian gland dysfunction with and without ocular Demodex infestation. Ann Transl Med. 2021;9(3):238. doi:10.21037/ATM-20-1745
47. Stonecipher K, Abell TG, Chotiner B, Chotiner E, Potvin R. Combined low level light therapy and intense pulsed light therapy for the treatment of meibomian gland dysfunction. Clin Ophthalmol. 2019;13:993–999. doi:10.2147/OPTH.S213664
48. Kuffler DP. Photobiomodulation in promoting wound healing: a review. Regenerative Med. 2016;11(1):107–122. doi:10.2217/RME.15.82
49. Merigo E, Vescovi P, Margalit M, et al. Efficacy of LLLT in swelling and pain control after the extraction of lower impacted third molars. Laser Ther. 2015;24(1):39–46. doi:10.5978/ISLSM.15-OR-05
50. Kim WS, Glen Calderhead R. Is light-emitting diode phototherapy (LED-LLLT) really effective? Laser Ther. 2011;20(3):205–215. doi:10.5978/ISLSM.20.205
51. Avci P, Gupta A, Sadasivam M, et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring - PubMed. Semin Cutan Med Surg. 2013;32(1):41–52.
52. D’Souza S, Padmanabhan Nair A, Iyappan G, et al. Clinical and molecular outcomes after combined intense pulsed light therapy with low-level light therapy in recalcitrant evaporative dry eye disease with meibomian gland dysfunction. Cornea. 2022;41(9):1080–1087. doi:10.1097/ICO.0000000000002954
53. Giannaccare G, Pellegrini M, Scalzo GC, Borselli M, Ceravolo D, Scorcia V. Low-level light therapy versus intense pulsed light for the treatment of meibomian gland dysfunction: preliminary results from a prospective randomized comparative study. Cornea. 2023;42(2):141–144. doi:10.1097/ICO.0000000000002997
54. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017;4(3):337–361. doi:10.3934/BIOPHY.2017.3.337
55. Poyton RO, Ball KA. Therapeutic photobiomodulation: nitric oxide and a novel function of mitochondrial cytochrome c oxidase. Discov Med. 2011;11(57):154–159.
56. Valter K, Tedford SE, Eells JT, Tedford CE. Photobiomodulation use in ophthalmology - an overview of translational research from bench to bedside. Frontiers in Ophthalmology. 2024;4:1388602. doi:10.3389/FOPHT.2024.1388602
57. Rupel K, Zupin L, Ottaviani G, et al. Blue laser light inhibits biofilm formation in vitro and in vivo by inducing oxidative stress. NPJ Biofilms Microbiomes. 2019;5(1):29. doi:10.1038/S41522-019-0102-9
58. Gwynne PJ, Gallagher MP. Light as a broad-spectrum antimicrobial. Front Microbiol. 2018;9(FEB):119. doi:10.3389/FMICB.2018.00119
59. Maisch T, Baier J, Franz B, et al. The role of singlet oxygen and oxygen concentration in photodynamic inactivation of bacteria. Proc Natl Acad Sci U S A. 2007;104(17):7223–7228. doi:10.1073/PNAS.0611328104
60. Zhao YE, Wu LP, Hu L, Xu JR. Association of blepharitis with Demodex: a meta-analysis. Ophthalmic Epidemiol. 2012;19(2):95–102. doi:10.3109/09286586.2011.642052
61. Amescua G, Akpek EK, Farid M, et al. Blepharitis preferred practice pattern®. Ophthalmology. 2019;126(1):P56–P93. doi:10.1016/J.OPHTHA.2018.10.019
62. Lam NSK, Long XX, Li X, Yang L, Griffin RC, Doery JCG. Comparison of the efficacy of tea tree (Melaleuca alternifolia) oil with other current pharmacological management in human demodicosis: a systematic review. Parasitology. 2020;147(14):1587–1613. doi:10.1017/S003118202000150X
63. Martínez-Pulgarín DF, Ávila MY, Rodríguez-Morales AJ. Interventions for Demodex blepharitis and their effectiveness: a systematic review and meta-analysis. Cont Lens Anterior Eye. 2021;44(6):101453. doi:10.1016/J.CLAE.2021.101453
64. Karakurt Y, Zeytun E. Evaluation of the efficacy of tea tree oil on the density of Demodex mites (Acari: demodicidae) and ocular symptoms in patients with demodectic blepharitis. J Parasitol. 2018;104(5):473–478. doi:10.1645/18-46
65. Chen D, Wang J, Sullivan DA, Kam WR, Liu Y. Effects of terpinen-4-ol on meibomian gland epithelial cells in vitro. Cornea. 2020;39(12):1541–1546. doi:10.1097/ICO.0000000000002506
66. Fulk GW, Murphy B, Robins MD. Pilocarpine gel for the treatment of demodicosis--a case series. Optom Vis Sci. 1996;73(12):742–745. doi:10.1097/00006324-199612000-00004
67. Gao YY, Di Pascuale MA, Li W, et al. In vitro and in vivo killing of ocular Demodex by tea tree oil. Br J Ophthalmol. 2005;89(11):1468–1473. doi:10.1136/BJO.2005.072363
68. Gao YY, Xu DL, Huang LJ, Wang R, Tseng SCG. Treatment of ocular itching associated with ocular demodicosis by 5% tea tree oil ointment. Cornea. 2012;31(1):14–17. doi:10.1097/ICO.0B013E31820CE56C
69. Ávila MY, Martínez-Pulgarín DF, Rizo Madrid C. Topical ivermectin-metronidazole gel therapy in the treatment of blepharitis caused by Demodex spp.: a randomized clinical trial. Cont Lens Anterior Eye. 2021;44(3):101326. doi:10.1016/J.CLAE.2020.04.011
70. Navel V, Mulliez A, Benoist d’Azy C, et al. Efficacy of treatments for Demodex blepharitis: a systematic review and meta-analysis. Ocul Surf. 2019;17(4):655–669. doi:10.1016/J.JTOS.2019.06.004
71. Epstein IJ, Rosenberg E, Stuber R, Choi MB, Donnenfeld ED, Perry HD. Double-masked and unmasked prospective study of terpinen-4-ol lid scrubs with microblepharoexfoliation for the treatment of Demodex blepharitis. Cornea. 2020;39(4):408–416. doi:10.1097/ICO.0000000000002243
72. Murphy O, O’Dwyer V, Lloyd-McKernan A. The efficacy of tea tree face wash, 1, 2-octanediol and microblepharoexfoliation in treating Demodex folliculorum blepharitis. Cont Lens Anterior Eye. 2018;41(1):77–82. doi:10.1016/J.CLAE.2017.10.012
73. Braulio de Venecia III A, Siong RLB. Demodex sp. infestation in anterior blepharitis, meibomian-gland dysfunction, and mixed blepharitis. Philipp J Ophthalmol. 2011;36(1):15–22.
74. Siegel H, Merz A, Gross N, et al. BlephEx-treatment for blepharitis: a prospective randomized placebo-controlled trial. BMC Ophthalmol. 2024;24(1):503. doi:10.1186/S12886-024-03765-3
75. Mohammad-Rabei H, Arabi A, Shahraki T, Rezaee-Alam Z, Baradaran-Rafii A. Role of blepharoexfoliation in Demodex blepharitis: a randomized comparative study. Cornea. 2023;42(1):44–51. doi:10.1097/ICO.0000000000003046
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Eyelid Warming Devices: Safety, Efficacy, and Place in Therapy
Bzovey B, Ngo W
Clinical Optometry 2022, 14:133-147
Published Date: 5 August 2022
Pulsed Light Therapy in the Management of Dry Eye Disease: Current Perspectives
Barbosa Ribeiro B, Marta A, Ponces Ramalhão J, Marques JH, Barbosa I
Clinical Ophthalmology 2022, 16:3883-3893
Published Date: 24 November 2022
Review of Literature on Intraductal Meibomian Gland Probing with Insights from the Inventor and Developer: Fundamental Concepts and Misconceptions
Warren NA, Maskin SL
Clinical Ophthalmology 2023, 17:497-514
Published Date: 8 February 2023
Multi-Frequency RF Combined with Intense Pulsed Light Improves Signs and Symptoms of Dry Eye Disease Due to Meibomian Gland Dysfunction
Chelnis J, Garcia CN, Hamza H
Clinical Ophthalmology 2023, 17:3089-3102
Published Date: 20 October 2023
Meibomian Gland Probing Stimulates a Proliferative Epithelial Response Resulting in Duct Regeneration
Maskin SL, Toland C
Clinical Ophthalmology 2024, 18:631-645
Published Date: 1 March 2024