Back to Journals » Clinical Ophthalmology » Volume 17
Multi-Frequency RF Combined with Intense Pulsed Light Improves Signs and Symptoms of Dry Eye Disease Due to Meibomian Gland Dysfunction
Authors Chelnis J, Garcia CN, Hamza H
Received 12 July 2023
Accepted for publication 27 September 2023
Published 20 October 2023 Volume 2023:17 Pages 3089—3102
DOI https://doi.org/10.2147/OPTH.S426564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
James Chelnis,1,2,* Chantel N Garcia,3,* Haya Hamza4
1New York Eye & Ear Infirmary of Mount Sinai, New York, NY, USA; 2Manhattan Face and Eye, New York, NY, USA; 3Carolina Eye Doctors, Harrisburg, NC, USA; 4Lumenis Be, Yokneam, Israel
*These authors contributed equally to this work
Correspondence: James Chelnis, Manhattan Face and Eye, 150 W 58th St #1C, New York, NY, 10019, USA, Tel +1 212-484-9707, Email [email protected]
Purpose: To evaluate the efficacy of multi-frequency RF and IPL + MGX combination for treatment of Meibomian Gland Dysfunction (MGD).
Patients and Methods: Eligible subjects had signs and moderate-to-severe symptoms of DED (Dry Eye Disease) due to MGD. Subjects underwent 4 treatments at 2-week intervals. Each treatment consisted of intense pulsed light (IPL) followed by radiofrequency (RF) on the periocular skin, followed by meibomian gland expression (MGX). The main outcome measure was the quality of meibum in 15 meibomian glands along the lower eyelid, using the modified Meibomian Gland Score (mMGS). The main hypothesis was a reduction of mMGS between the baseline (BL) and the follow-up (FU). Other outcome measures, such as symptoms measured with the OSDI (Ocular Surface Disease Index) questionnaire, meibography, non-invasive tear break-up time (NIBUT), and matrix metallopeptidase 9 (MMP-9) levels in tear samples were evaluated as well.
Results: 31 subjects completed the FU. Between BL and FU, mMGS decreased from 30.4 (8.5) to 9.3 (9.5) (− 69.3%, 95% CI: − 55.6% to − 82.9%, p< 0.0001); OSDI decreased from 63.6 (17.2) to 25.0 (20.6) (− 60.7%, 95% CI: − 47.8% to − 73.5%, p< 0.0001); NIBUT did not change (p=0.92). An adjusted model with a historical control was constructed to allow the comparison of these subjects with those treated similarly with IPL+MGX (but without RF) in a different study. This analysis identified that the change in mMGS was larger when RF was included (− 20.9 vs − 18.3, adjusted p-value (p_adjusted) < 0.05). The difference in OSDI change was not significant (− 38.1 vs − 25.5, p_adjusted = 0.196).
Conclusion: Combination of multi-frequency RF and IPL+MGX improves signs and symptoms of MGD. In comparison to a historical control, improvements were generally larger. A randomized controlled study comparing the combination of RF and IPL+MGX with IPL+MGX alone is required to further elaborate the relative contribution of RF.
Keywords: IPL, RF, MGD, DED
Introduction
Dry eye disease (DED) is a multifactorial disease of the ocular surface.1,2 A major cause of DED is meibomian gland dysfunction (MGD), where the secretion of meibomian glands (MGs) is abnormal, allowing for premature tear evaporation.3 Thus, in MGD the ocular surface may be exposed between blinks, resulting in dryness, inflammation, and symptoms.4
Various modalities are offered for managing MGD, including lid hygiene, warm compresses, heating apparatuses, tear substitutes, pharmacology, debridement, intraductal probing and meibomian gland expression.4–11 Additional approaches are Intense Pulsed Light (IPL) and Radiofrequency (RF).
IPL has numerous applications in dermatology, including the treatment of rosacea.12 Since rosacea is highly correlated with MGD,13 it was proposed that IPL could be beneficial for MGD as well.14 Indeed, recent studies have demonstrated the improvement of MGD following periocular IPL.15–18 The main mechanism of action is the triggering of anti-inflammatory processes that break the vicious cycle of ocular surface inflammation. These include thrombosis of disease-driven telangiectasia, photobiomodulation, controlling the population of Demodex parasites and reduction of the bacterial load in eyelids.19–21 This approach has recently gained FDA-approval and was recommended by DEWS II.11
Radiofrequency (RF) is a type of electromagnetic wave, transferred from an oscillatory electric field to charged particles or dipoles (eg, water molecules) in the target tissue. This generates vibrations of the tissue particles, which produce friction between tissue particles and, consequently, heat is generated. Controlled heat generated by RF is useful for a variety of medical applications, including surgery, ablation of tumors, tightening of skin tissue, production of heat-shock proteins, and pain control.22–24 In dermatology, RF is standard treatment for skin tightening, skin rejuvenation and improving skin laxity.23–25 In recent years, RF was proposed as a therapeutic alternative for the management of MGD.26,27 It was suggested that the heat generated with RF could be useful for liquefying waxy secretions, unclogging MGs, triggering neocollagenesis, expressing of heat-shock proteins, or attenuating inflammatory processes. Nevertheless, except for a limited number of studies that demonstrated potential for this approach, this has not been thoroughly investigated thus far.
Due to the multifactorial nature of DED, it is sensible to expect that combination treatments would be more effective than monotherapies. To the best of our knowledge, the combination of IPL, multi-frequency RF and MGX was not previously examined for treatment of subjects with MGD.
Materials and Methods
Participants
Participants were enrolled from July 2022 to October 2022. Eligible participants were men and women aged 22 to 85 years of age, with signs and symptoms of dry eye disease (DED) due to meibomian gland dysfunction (MGD). The main inclusion criteria comprised subjects with moderate to severe DED symptoms (OSDI ≥ 23), signs of MGD, and a modified Meibomian Gland Score (mMGS) > 12 in at least one eye. The main exclusion criteria included patients with Fitzpatrick skin type V–VI, severe active allergies or other severe uncontrolled eye disorders affecting the ocular surface or lid function (not including DED due to MGD), photosensitive medications, use of any eye drops for dry eye (excluding artificial lubricants) within 1 month prior to the study, and subjects with more than 75% loss of lower lid MGs. During the study, participants were allowed to use artificial lubricants, but no other medications. An informed consent was obtained from all participants.
Study Design
This was a prospective, interventional, single arm study, approved by an Institutional Review Board (Sterling IRB, # 10124). The study complied with the Declaration of Helsinki. The trial was registered in ClinicalTrials.gov (NCT05487547) and conducted at 2 sites in the USA.
Outcome Measures
Outcome measures were based on well-accepted diagnostic tests of DED and MGD.28,29 The primary outcome measure was the modified Meibomian Gland Score (mMGS), based on the Meibomian Gland Score defined by Lane et al.30 Briefly, mMGS was calculated as the sum of grades in 15 meibomian glands along the lower eyelid (5 nasal + 5 central + 5 temporal), each gland graded for meibum quality using a 4-point severity scale (0=clear liquid, 1 = cloudy liquid, 2 = inspissated, 3 =blocked). Secondary outcome measures included the Ocular Surface Disease Index (OSDI), non-invasive tear break up time (NIBUT), the percentage of Meibomian Gland Loss (%MGL) and the number of expressible meibomian glands (Nexpressible). Exploratory outcome measures comprised the Predominant Quality of the meibum (PQmeibum), matrix-metalloproteinase-9 (MMP-9) presence in tear samples, and features of eyelid appearance including lid margin thickness (LMT), lid margin vascularity (LMV), conjunctival injection (CJI), and plugged meibomian glands (PMG).
All outcome measures were tested at the baseline (BL) and at a single follow-up (FU) that occurred 4 weeks after the 4th treatment. mMGS, PQmeibum, and eyelid appearance features were also tested after every treatment session except the first session as they were already evaluated at the immediately preceding BL. Nexpress was tested after every treatment session including the first, as it was reasoned that MGX would affect this outcome measure.
mMGS
Fifteen MGs along the lower eyelid margin (5 nasal + 5 central + 5 temporal) were expressed, and secretion of each gland was graded 0 (clear liquid), 1 (cloudy liquid), 2 (inspissated) or 3 (no expression). mMGS was then calculated as the sum of these 15 grades. Range: 0 to 15.
OSDI
Symptoms were self-evaluated with the OSDI questionnaire.31 Range: 0 to 100.
NIBUT
Non-invasive tear breakup time (in seconds) measures the time between full opening of eyelids after a blink and first appearance of a break in the tear film. This was implemented with the analysis software of the Antares system (CSO, Florence, Italy).
% MGL
Each eyelid was everted, and an infra-red image was captured with the Antares system. % MGL (area occupied by MGs in this subject, divided by the area of MGs occupied in a healthy individual) was evaluated by meibography, using the Phoenix software of the Antares system.
Nexpressible
All MGs were squeezed, and the number of glands producing any secretion was counted per eyelid.
MMP-9
Tear samples were collected from the inferior fornix. Presence of MMP-9 was tested with the InflammaDry assay (Pathogen Screening, Sarasota FL, USA).
PQmeibum
The predominant quality of the meibum was judged by the study investigator, based on global estimation of meibum quality. Values: clear liquid, cloudy liquid, inspissated and blocked.
Eyelid Appearance
LMV, LMT, CJI and PMG were estimated by biomicroscopy at the slit lamp. Values: normal, mild, moderate, and severe.
Intervention
Subjects were treated at BL and at 3 additional visits, with 2 weeks intervals. Duration of each treatment session was about 20 minutes (10 minutes of IPL, immediately followed by 10 minutes of RF, immediately followed by MGX). A single FU visit was conducted 4 weeks after the 4th treatment.
Intense Pulsed Light (IPL)
Before IPL administration, both eyes of the subject were occluded with disposable eye patches. A thin layer of transparent coupling gel was spread over the treatment area, which consisted of the malar region (from tragus to tragus, including the nose), up to the lower edge of the eye patches (a few mm below the lower lid margins). IPL was administered with an OptiLight system (Lumenis Be, Yokneam, Israel) using a 590 nm high-pass filter. Two handpieces were used, each in 2 passes along the same treatment area: one handpiece was the universal IPL handpiece with a rectangular 35×15 mm lightguide, using fluences of 12 to 19 J/cm2 (depending on Fitzpatrick skin type); the second handpiece was the OPT handpiece with a circular (6 mm in diameter) lightguide. The OPT handpiece is unique to the OptiLight system, which was specifically designed for use in small areas such as below the lower eyelids and around the nostrils. In this study, the OPT handpiece was used with fluences of 11 to 14 J/cm2 (depending on Fitzpatrick skin type).
Radiofrequency (RF)
Monopolar RF was administered with a NueraTight device (Bios Srl, Vimodrone, Italy) using a 20 mm capacitive handpiece. Prior to treatment, a uniform layer of coupling cream was applied to the skin to separate it from the RF probe. Target skin temperature was set to 41°C. RF was applied in a continuous C-shape motion along the orbital rim, from supraorbital foramen to anterior lacrimal crest. After the skin temperature reached its target per side, RF was applied for 2.5 min at 1MHz and for 2.5 min at 4MHz.
Meibomian Gland Expression (MGX)
RF was followed with forced MGX, using a dedicated forceps (Sight Science, Menlo Park, CA, USA).
Statistical Analysis
Statistical analyses were done with excel and JMP (SAS, Cary NC, USA).
Analysis Sets
For variables in which FU was compared to BL (paired tests), analysis considered 31 subjects who completed the study (Per Protocol set, PP). For variables tested longitudinally, the analysis was applied on 33 subjects who started the study (Intention to Treat set, ITT). For longitudinal analyses, missing values were imputed with sample averages.
Descriptive Statistics
For continuous variables, normal distribution was tested with the Shapiro–Wilk test, and descriptive statistics were expressed with means, standard deviation (SD) and 95% confidence intervals. For ordinal variables, descriptive statistics included counts (N) and percentages (%).
Statistical Tests
Statistical significance (α) was set to 0.05. For continuous variables, intra-subject correlation was removed by analyzing the “average eye” (average of variable in the right and left eyes). For comparison between BL and FU, the probability (p) to reject H0 (no difference between BL and FU) was tested with a double-sided paired t-test for continuous variables, or with a chi-square / Fisher’s exact test for ordinal variables. For repeated measures over time, the probability (P) to reject H0 (no longitudinal change within subjects) was tested with a multiple analysis of variance (F-test) for normal distribution at BL, or with the non-parametric Dunn’s test if otherwise.
Comparison of the Current Study with a Historical Control (HC)
To estimate the contribution of RF, results of the current study were compared to data from 45 MGD subjects collected in a previously published study, where subjects were treated with IPL + MGX alone.15 Of these 45 subjects (ITT set of HC), 39 completed the FU (PP set of HC). Noteworthy, the two studies were similar in treatment parameters, regimen, and schedule. There was also an overlap in some of the tested outcome measures. In addition, in HC the treatment was performed with the M22 system (Lumenis), a predecessor of the OptiLight system, with identical core technology. IPL settings used in the two studies were the same. The only significant difference between the M22 and OptiLight system is the addition of the OPT handpiece in the latter, which is more convenient for the treating physician when administering IPL pulses in small areas such as below the lower eyelids. In both studies, mMGS, Nexpress and OSDI were measured using similar methods. Consequently, mMGS, Nexpress, and OSDI could be directly compared. Comparison of the tear breakup time was less straightforward as an inclusion criterion was applied in HC (tear breakup time ≤ 7sec). Hence, for the sake of comparison, in the current study we analyzed only subjects with NIBUT ≤ 7sec. Per each outcome measure tested, comparison of the current study and HC was done only at time points that were identical in both studies.
For a fair comparison between the current study and HC, per each examined variable the differences in baseline values were taken into account by fitting a Least Squares Mean (LSM) model with the identity of the data set (current study or HC) as the independent variable, and the value at BL pre-Tx1 (or post-Tx1 if a pre-Tx1 measurement was not available) as a covariate. Probabilities testing the difference between the current study and the HC are denoted padjusted for paired comparisons of BL and FU, or Padjusted for comparison of longitudinal changes within subjects.
Participant Flow
Thirty-four subjects were screened between July and October 2022. One subject was excluded due to ocular surgery within 3 months prior to screening. Two subjects were lost to follow-up (One was treated once but was too nervous to continue; One was treated twice but could not continue due to distance from home).
Results
Demographics
No subject with a systemic disease that could affect the ocular surface was included in this study. In the PP set (N=31), age was 52.1±16.0 years (95% CI: 46.5, 57.7); 27 (87.1%) were women; 2 (6.4%), 17 (54.8%), 11 (35.4%) and 1 (3.2%) had Fitzpatrick skin type I, II, III, and IV, respectively. In the ITT set (N=33), age was 51.8±15.6 years (95% CI: 46.5, 57.2); 29 (87.9%) were women; 2 (6.1%), 18 (54.5%), 12 (36.4%) and 1 (3.0%) had Fitzpatrick skin type I, II, III, and IV, respectively. Participants were Caucasian (N=30), Asian/Pacific (N=1), American Indian (N=1), or Hispanic/Latino (N=1). Before the study, no patient was treated with RF, and 3 patients were treated with IPL.
Baseline Values
Baseline values of all outcome measures are summarized in Table 1. For variables compared at BL and FU, the analysis set was PP (N=31 average eyes for continuous variables or N=62 eyes for ordinal variables): mMGS, OSDI, NIBUT, %MGL were normally distributed; BL means were 30.4±8.5 (mMGS), 63.6±17.2 (OSDI), 9.6±4.9 sec (NIBUT), 37.5±9.4% (%MGL in LL) and 32.3±9.6% (%MGL in UL). For the InflammaDry test, 60 eyes of 30 subjects had a positive result.
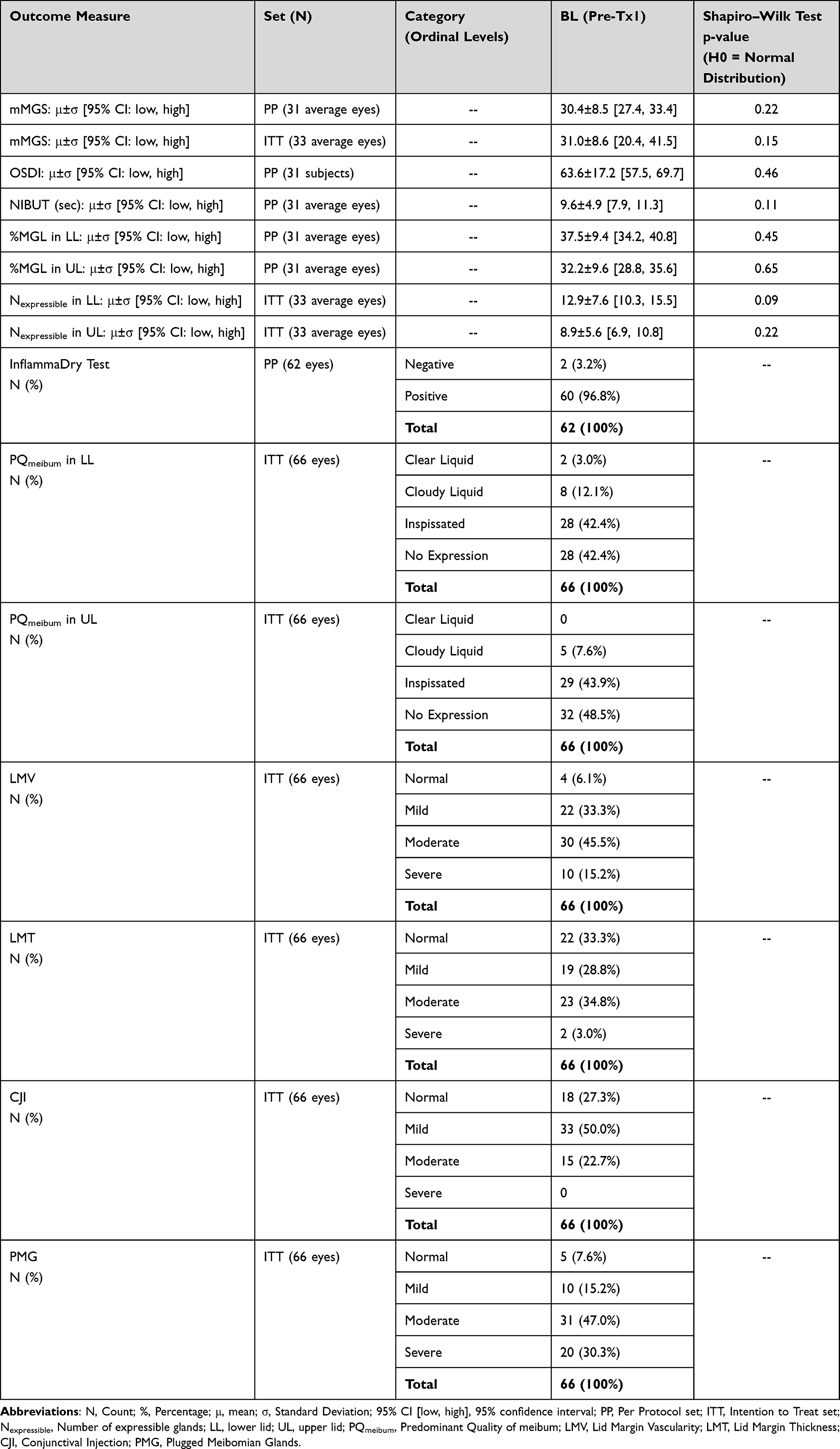 |
Table 1 Baseline Values of Outcome Measures |
For variables repeatedly measured over time, the analysis set was ITT (N=33 average eyes for continuous variables or 66 eyes for ordinal variables). mMGS, Nexpressible in LL and Nexpressible in UL were normally distributed; BL means were 31.0±8.6 (mMGS), 12.9±7.7 (Nexpress in LL) and 8.9±5.6 (Nexpress in UL). For PQmeibum, the number of eyes with clear liquid meibum, cloudy liquid meibum, inspissated meibum and no expression were 2 (3.0%), 8 (12.1%), 28 (42.4%) and 28 (42.4%) respectively in LL; and 0, 5 (7.6%), 29 (43.9%) and 32 (48.5%) respectively in UL. For features of eyelid appearance, the number of eyes with normal, mild, moderate and severe levels were 4 (6.1%), 22 (33.3%), 30 (45.5%) and 10 (15.2%) respectively for LMV; 22 (33.3%), 19 (28.8%), 23 (34.8%) and 2 (3.0%) respectively for LMT; 18 (27.3%), 33 (50%), 15 (22.7%) and 0 respectively for CJI; and 5 (7.6%), 10 (15.2%), 31 (47%) and 20 (30.3%) respectively for PMG.
Change of Outcome Measures Tested at BL and FU
Table 2 (8th column) summarizes the values of all variables measured at FU. Figure 1 illustrates the value of variables measured at BL and FU. mMGS (Figure 1A), OSDI (Figure 1B) and %MGL in both eyelids improved (Figure 1D and E). Relative to BL, mMGS decreased by −21.0±11.8 (95% CI: −25.2,-16.9; %Δ: −69.3%; p<0.0001), OSDI decreased by −38.6±23.3 (95% CI: −46.8,-30.4; %Δ: −60.7%; p<0.0001), %MGL decreased by −15.3±10.7% (95% CI: −19.1%,-11.5%; %Δ: −40.8%; p<0.0001) in LL, and by −9.0±9.8% (95% CI: −12.5%,-5.6%; %Δ: −28.0%; p<0.0001) in UL.
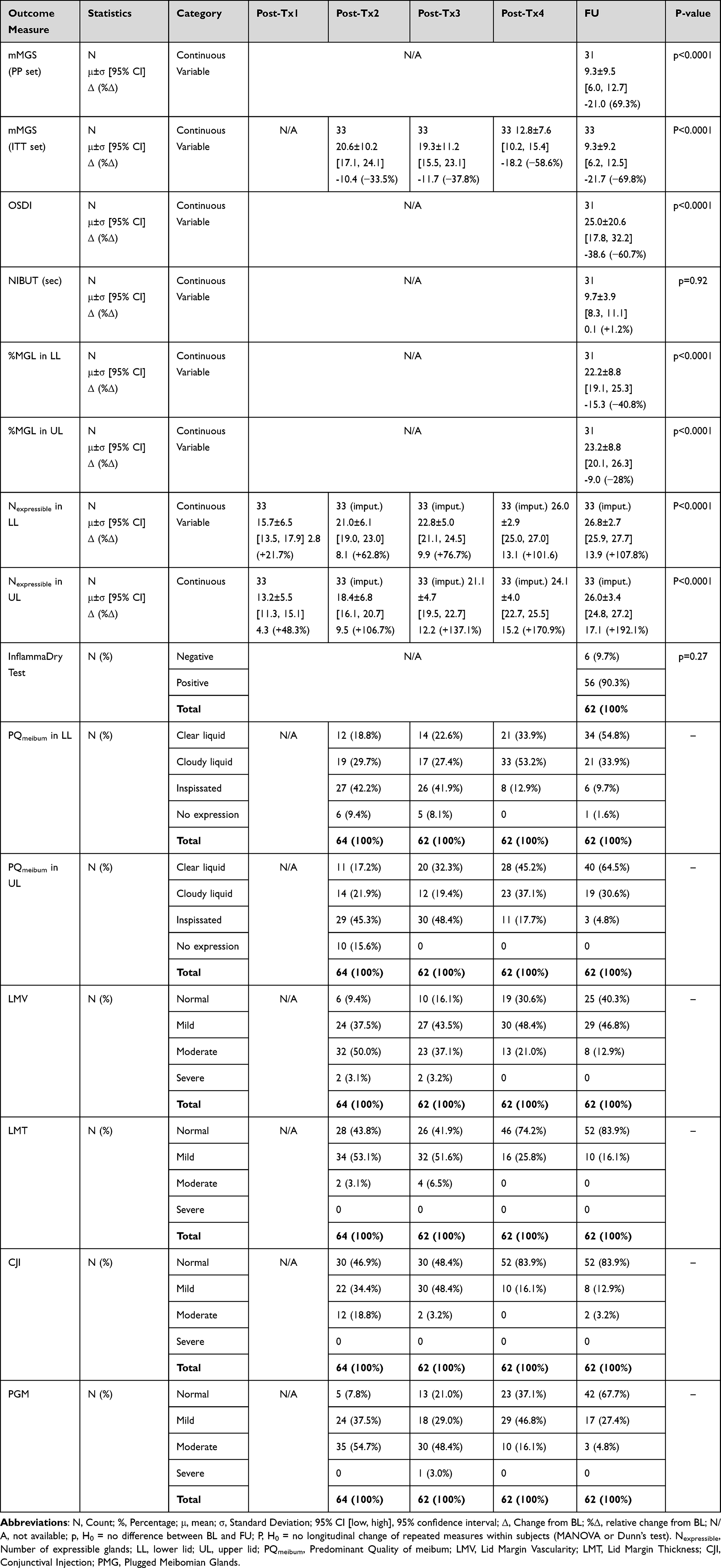 |
Table 2 Outcome Measures Tested Throughout the Study |
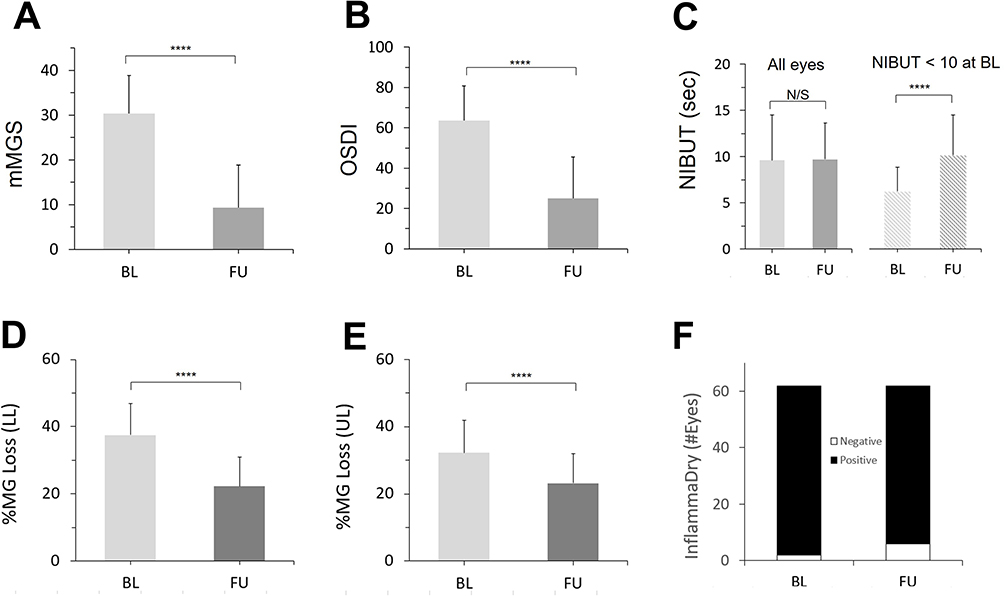 |
Figure 1 Change of outcome measures between BL and FU (paired comparison). PP set (N=31); Error bars: standard deviations; ****p <0.0001; N/S: Not significant. Except for OSDI, means and proportions were calculated for the average eye (see Methods). (A) Means of mMGS (the primary outcome). (B) Means of OSDI. (C) Means of NIBUT for all eyes (leftmost 2 bars) and for eyes with NIBUT<10 sec at BL (rightmost 2 bars). (D) Means of %meibomian gland loss (Meibography) in the lower lids. (E) Means of %meibomian gland loss (Meibography) in the upper lids. (F) Number of eyes with Negative and Positive results of the InflammaDry test. |
With respect to NIBUT (Figure 1C), there was no change between BL and FU (95% CI: −2.0, 2.2; %Δ: +1.2%; p = 0.92). However, when 13 subjects with normal NIBUT (>10 sec) at BL were excluded from the analysis, NIBUT increased by 3.8 sec (95% CI: 1.7, 6.0; %Δ: +61.8%; p<0.0001).
For MMP-9 presence (Figure 1F), the number of positive InflammaDry tests decreased from 60 (96.8%) to 56 (90.3%), but the change was not significant (p=0.61).
Outcome Measures Tested Longitudinally
Variables measured longitudinally are summarized in Table 2 (4th to 8th columns). Figure 2 illustrates the value of variables measured at BL and longitudinally. For all continuous variables, in comparison to BL the means gradually improved with time: mMGS (Figure 2A) decreased by −33.5%, −37.8%, −58.6% and −69.8% at Tx2, Tx3, Tx4 and FU, respectively (P<0.0001); Nexpressible in LL (Figure 2C, solid curve) increased by +22.1%, +63.3%, +77.5%, +102% and +108.5% immediately after Tx1, Tx2, Tx3, Tx4 and FU, respectively (P<0.0001); and Nexpressible in UL (Figure 2C, dotted curve) increased by +49.1%, +107.7%, +138%, +172.2% and +193.9% immediately after Tx1, Tx2, Tx3, Tx4 and FU, respectively (P<0.0001).
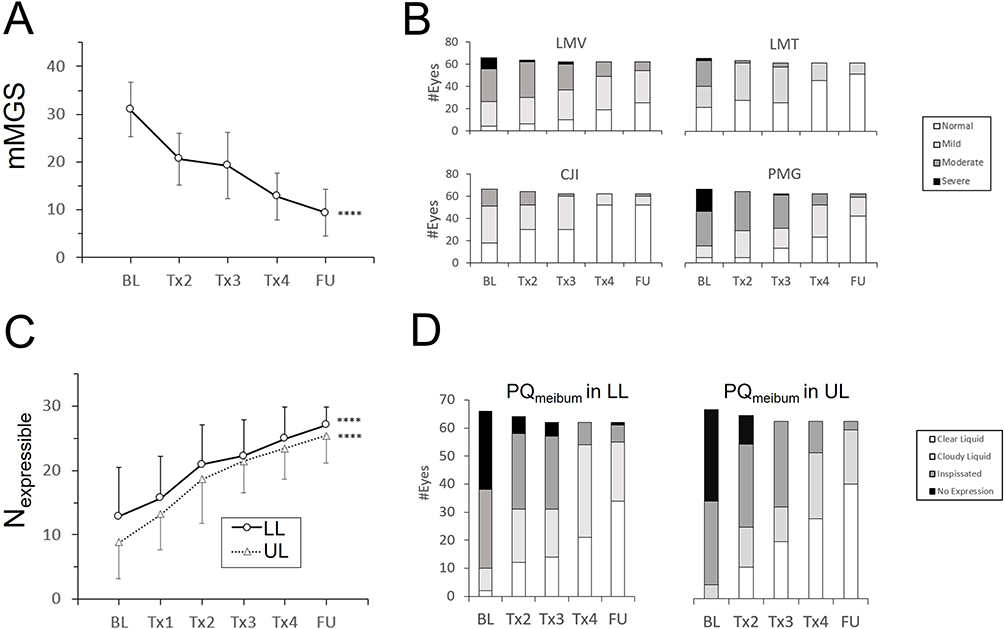 |
Figure 2 Longitudinal changes of outcome measures from BL to FU. ITT set. All means for continuous variables and proportions for ordinal variables were calculated for the average eye (Methods). For longitudinal analysis of means, missing values for two subjects who were lost to follow-up were imputed (Methods); Error bars: standard deviations; ****p<0.0001; BL: Immediately before the 1st treatment (D0); Tx1, Tx2, Tx3, and Tx4: Immediately after the 1st treatment (D0), 2nd treatment (D14), 3rd treatment (D28) and 4th treatment (D42), respectively; FU: Follow-up 4 weeks after the 4th treatment (D70). (A) Longitudinal change in the means of mMGS. (B) Longitudinal change in number of eyes with normal, mild, moderate or severe condition of lid margin vascularity (LMV), lid margin thickness (LMT), conjunctival injection (CJI) and plugged meibomian glands (PMG). (C) Longitudinal change in the means of Nexpressible in LL and UL (dotted line). For graphical clarity, per each curve half of the standard deviation is displayed (in opposite directions to prevent overlap). (D) Longitudinal change in the number of eyes where the Predominant Quality of the meibum (PQmeibum) is clear liquid, cloudy liquid, inspissated or no expression in LL and UL. |
With respect to ordinal variables, usually and unless noted otherwise the number of eyes with normal or mild condition gradually increased with time, and the number of eyes with moderate or severe condition gradually decreased with time.
For PQmeibum in LL (Figure 2D, Left), from BL to FU the number of eyes with clear liquid or cloudy meibum increased from 2 (3%) to 34 (54.8%) and from 8 (12.1%) to 21 (33.9%), respectively; and the number of eyes with inspissated meibum or blocked MGs decreased from 28 (42.4%) to 6 (9.7%) and from 28 (42.4%) to 1 (1.6%), respectively. For PQmeibum in UL (Figure 2D, Right), from BL to FU the number of eyes with clear liquid meibum or cloudy liquid meibum increased from 0 to 40 (64.5%) and from 5 (7.6%) to 19 (30.6%), respectively; and the number of eyes with inspissated meibum and blocked glands decreased from 29 (43.9%) to 3 (4.8%) and from 32 (48.5%) to 0, respectively.
Similar trends were observed in eyelid appearance. For LMV (Figure 2B, Top left), from BL to FU the number of eyes with normal or mild condition increased from 4 (6.1%) to 25 (40.3%) and from 22 (33.3%) to 29 (46.8%), respectively; and the number of eyes with moderate or severe condition decreased from 30 (45.5%) to 8 (12.9%) and from 10 (15.2%) to 0, respectively. For LMT (Figure 2B, Top right), from BL to FU the number of eyes with normal condition increased from 22 (33.3%) to 52 (83.9%); and the number of eyes with mild, moderate or severe condition decreased from 19 (28.8%) to 10 (16.1%), from 23 (34.8%) to 0, and from 2 (3%) to 0, respectively. For CJI (Figure 2B, Bottom left), from BL to FU the number of eyes with normal condition increased from 18 (27.3%) to 52 (83.9%); and the number of eyes with mild or moderate condition decreased from 33 (50%) to 8 (12.9%), and from 15 (22.7%) to 2 (3.2%), respectively. For PMG (Figure 2B, Bottom right), from BL to FU the number of eyes with normal and mild condition increased from 5 (7.6%) to 42 (67.7%) and from 10 (15.2%) to 17 (27.4%), respectively; and the number of eyes with moderate and severe condition decreased from 31 (47.0%) to 3 (4.8%) and from 20 (30.3%) to 0, respectively.
Post-Hoc Analyses (BL vs FU)
To estimate the contribution of RF, results of the current study were compared to data from subjects previously treated with IPL+MGX alone, referred to as the Historical Control (HC) (Figure 3). For change of BL versus FU, the PP sets of both studies were compared.
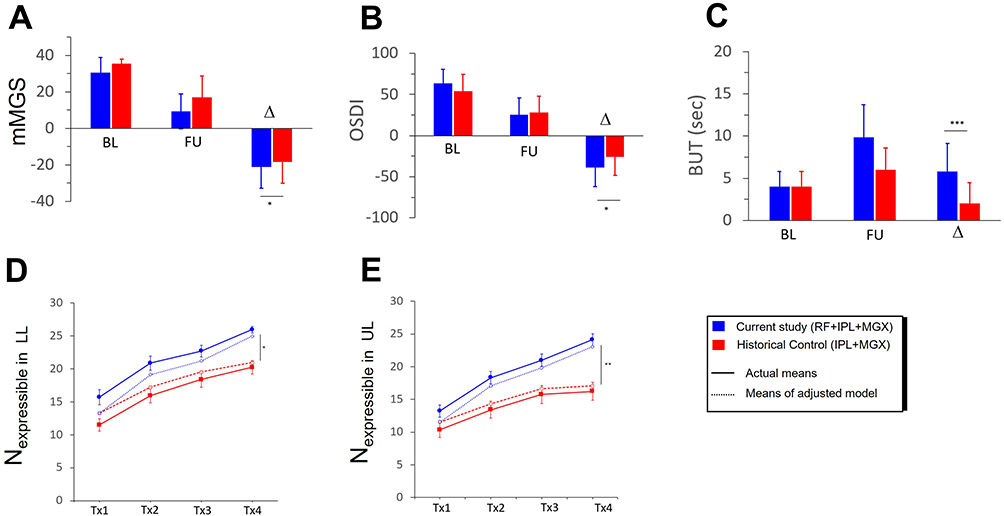 |
Figure 3 Comparison between the current study and an historical control (HC). Blue Bars: Current study. Red Bars: HC; Δ: Difference between FU and BL; ***: p<0.001, **: p<0.01, *: p<0.05, N/S: Not significant. (A) Comparison of mMGS in Current Study and HC. (B) Comparison of OSDI in Current Study and HC. (C). Comparison of NIBUT in Current Study and TBUT in HC. For the sake of fair comparison, in the current study subjects with NIBUT > 7 sec at BL were excluded. (D) Longitudinal comparison of Nexpressible in LL of the current study (blue curves) and HC (red curves). Solid curves represent the actual means. Dotted curves represent results of a model in which baseline differences were eliminated. (E) Same as D, for Nexpressible in UL. |
mMGS (Figure 3A) improved in both studies, with a larger decrease in the current study (Current study: −21.0±11.8 [95% CI: −16.9,-25.2]; HC: −18.5±11.5 [95% CI: −14.9,-22.1]; padjusted <0.05). OSDI (Figure 3B) improved in both studies, with no statistically significant difference (Current study: −38.6±23.3 [95% CI: −30.4,-46.8]; HC: −25.9±22.5 [95% CI: −18.8,-32.9]; padjusted = 0.196). With respect to NIBUT, comparison was not straightforward as an inclusion criterion in HC was a tear breakup time ≤ 7 sec, whereas there was no such restriction in the current study. To account for this difference, for this post-hoc analysis we compared results of HC with a sub-group of 9 subjects from the current study in whom NIBUT was ≤7sec at BL (Figure 3C). Under these conditions, the tear breakup time increased in both studies, with a larger increase in the current study (Current study: 5.8±3.3 sec [95% CI: 3.7, 8.0]; HC: 2.0±2.5 sec [95% CI: 1.2, 2.8]; padjusted<0.001).
Post-Hoc Analyses (Longitudinal)
A similar analysis was done to compare Nexpressible in LL and UL (Figure 3D and E). The ITT sets of both studies were compared, with missing values imputed in both studies. In HC these outcome measures were tested after each treatment session (after Tx1, Tx2, Tx3, and Tx4), but not at FU. Hence, comparison between the current study and HC was restricted to these time points.
In LL, for the non-adjusted data Nexpressible increased from 15.7±6.5 [95% CI: 13.5, 17.9] to 25.9±2.9 [95% CI: 25.0, 26.9] in the current study (%Δ: +65.1%; P<0.0001), and from 11.5±6.2 [95% CI: 9.7, 13.3] to 20.2±6.9 [95% CI: 18.2, 22.2] in HC (%Δ: +75.8%; P<0.0001); in an adjusted model that took account of BL differences (Methods), Nexpressible increased from 13.2 to 25.0 in the current study (%Δ: +89.4.0%; P<0.0001), and from 13.2 to 20.9 in HC (%Δ: +58.3%; P<0.0001). The difference was statistically significant (padjusted <0.05).
In UL, for the non-adjusted data Nexpressible increased from 13.2±5.5 [95% CI: 11.3, 15.1] to 24.1±4.0 [95% CI: 22.7, 25.5] in the current study (%Δ: 82.5%), and from 10.3±7.8 [95% CI: 8.1, 12.6] to 16.2±9.1 [95% CI: 13.6, 18.9] in HC (%Δ: +57.3%; P<0.0001); in the adjusted model, Nexpressible increased from 11.6 to 23.0 in the current study (%Δ: +98.3%; P<0.0001), and from 11.6 to 17.0 in HC (%Δ: +46.6%; P<0.0001). Here as well, the difference was statistically significant (padjusted <0.01).
Adverse Events
The safety population included 33 subjects. One subject experienced moderate bilateral conjunctivitis after the 4th treatment. The study investigator determined that this event was not related to the study devices or procedures. No other adverse event was reported.
Discussion
This study examined the effects of IPL combined with multi-frequency RF and followed by MGX in a population of subjects with moderate to severe MGD. The rationale to employ multiple frequencies of RF was to target various levels in the target tissue, in an effort to improve treatment efficacy.
The study population included patients with Fitzpatrick skin types I to IV, in line with FDA-approval. Significant improvements were observed in numerous parameters of meibomian gland function: the meibum quality of 15 glands along the lower eyelids (the primary outcome measure), the predominant quality of the meibum, the number of expressible glands, and the percentage of meibomian gland loss. Significant improvements were also observed in the appearance of eyelids, and in self-evaluation of symptoms with the OSDI questionnaire. One outcome measure that did not show improvement was the non-invasive tear breakup time (NIBUT), however this was due to the inclusion of subjects with a normal NIBUT at baseline. In a sub-group of subjects with abnormal (≤ 10 sec) NIBUT values at the baseline, NIBUT significantly improved as well. Another outcome measure that did not show significant change was the proportion of negative InflammaDry tests.
In feasibility studies or in the development stage of a novel treatment modality, historical controls (HCs) are often used as a supplementation or replacement of a control arm.32,33 In a post-hoc comparison of the current study with an HC in which MGD subjects were treated with IPL+MGX alone, improvements were more pronounced in the current study. Based on these preliminary results, it is tempting to propose that IPL and RF exhibit a synergic effect. Two independent mechanisms of action could explain such an interaction: (1) In subjects suffering from MGD, meibum quality is often low, with an elevated viscosity that impedes MGX. In principle, reducing the viscosity of the meibum back to normal levels could be achieved by a sustained increase of gland temperature by several degrees.21 Due to the pulsed nature of IPL, any increase in skin temperature following IPL treatment is likely modest and short-lived. Craig et al, for instance, measured an increase in skin temperature of less than 1 °C immediately after IPL.34 In this setting, immediately subsequent MGX would likely encounter meibum that has remained or returned to pre-treatment viscosity. In contrast, with RF, the signal is continuous, allowing the temperature to rise quickly and substantially, for example to 40–41 °C, as in this study. Such an effect may allow for subsequent MGX to be more efficient. (2) Another possible interaction between IPL and RF is the remodeling of collagen fibers within and around the eyelids. One of the causes of DED is inefficient blinking due to skin laxity of the eyelids and age-dependent loss of collagen elasticity.35 At controlled temperatures, RF causes a thermal injury in the dermis that stimulates a wound-healing response leading to new skin formation and the production of new collagen fibers.36,37 IPL, on the other hand, boosts neocollagenesis by photobiomodulation. Several studies have found that light in the red and near-infra red spectrum activates fibroblasts and enhances their collagen-production output.38,39 Thus, IPL and RF may have complementary roles in collagen remodeling, resulting in faster rejuvenation of collagen fibers, more rapid improvement in blinking efficacy, leading to increased relief of signs and symptoms of DED.
Comparison of the current study, where subjects were treated with IPL+RF+MGX, with an HC, where subjects were treated with IPL+MGX, should be interpreted with caution. Indeed, when using historical controls many potential biases need to be accounted for.32 The better results in our study may be due to statistical chance, variations in study populations, different ways of performing the same tests, or small technical differences between the IPL devices used. To support the hypothesis that multi-frequency RF has a contribution on top of IPL and MGX, a powered randomized control study is needed. This said, comparison of our study with an HC is still valuable as it provides a rough estimate for the expected effect size. Such information could be useful for designing powered randomized control studies in the future. Other limitations of the current study include a small sample size and a modest follow-up duration. Further studies with better patient selection, control groups, larger sample size, longer follow-ups and more sites are needed to better elaborate the merits of this approach.
Conclusion
In subjects with moderate to severe DED due to MGD, a series of four treatments consisting of a combination of IPL, multi-frequency RF and MGX decreased symptoms, improved meibum quality and the appearance of eyelids, increased the number of expressible glands, and decreased meibomian gland loss. In comparison to a historical control where subjects were treated with IPL and MGX only, improvements in the current study were generally larger. This suggests that multi-frequency RF may have an added value on top of IPL and MGX. Further studies, with larger sample size and control groups, are needed to examine this possibility.
Data Sharing Statement
De-identified data used to prepare tables and figures in this manuscript will be provided in response to reasonable requests from the corresponding author for 2 years following publication.
Disclosure
JC and CNG are consultants of Lumenis Be. In addition, JC reports non-financial support for RF generator from Soniquence and consulting fees from Horizon Therapeutics, outside the submitted work. HH is an employee of Lumenis Be. The authors report no other conflicts of interest in this work.
References
1. Shimazaki J. Definitions and diagnostic criteria of dry eye disease: historical overview and future directions. Invest Ophthalmol Vis Sci. 2018;59(14):DES7–DES12. doi:10.1167/iovs.17-23475
2. Nelson JD, Craig JP, Akpek EK, et al. TFOS DEWS II Introduction. Ocul Surf. 2017;15(3):269–275. doi:10.1016/j.jtos.2017.05.005
3. Sheppard JD, Nichols KK. Dry eye disease associated with meibomian gland dysfunction: focus on tear film characteristics and the therapeutic landscape. Ophthalmol Ther. 2023;12(3):1397–1418. doi:10.1007/s40123-023-00669-1
4. Baudouin C, de la Maza MS, Amrane M, et al. One-year efficacy and safety of 0.1% cyclosporine a cationic emulsion in the treatment of severe dry eye disease. Eur J Ophthalmol. 2017;27(6):678–685. doi:10.5301/ejo.5001002
5. Cui D, Li G, Akpek EK. Autologous serum eye drops for ocular surface disorders. Curr Opin Allergy Clin Immunol. 2021;21(5):493–499. doi:10.1097/ACI.0000000000000770
6. Kaiserman I, Rabina G, Mimouni M, et al. The effect of therapeutic meibomian glands expression on evaporative dry eye: a prospective randomized controlled trial. Curr Eye Res. 2021;46(2):195–201. doi:10.1080/02713683.2020.1789663
7. Tauber J. A 6-week, prospective, randomized, single-masked study of lifitegrast ophthalmic solution 5% versus thermal pulsation procedure for treatment of inflammatory meibomian gland dysfunction. Cornea. 2020;39(4):403–407. doi:10.1097/ICO.0000000000002235
8. Chan TYC, Chow SSW, Wan KHN, Yuen HKL. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med J. 2019;25(1):38–47. doi:10.12809/hkmj187331
9. Wang D, Liu X, Hao X, et al. Effect of the meibomian gland squeezer for treatment of meibomian gland dysfunction. Cornea. 2018;37:1270–1278. doi:10.1097/ICO.0000000000001682
10. Geerling G, Baudouin C, Aragona P, et al. Emerging strategies for the diagnosis and treatment of meibomian gland dysfunction: proceedings of the OCEAN group meeting. Ocul Surf. 2017;15(2):179–192. doi:10.1016/j.jtos.2017.01.006
11. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
12. Sharma A, Kroumpouzos G, Kassir M, et al. Rosacea management: a comprehensive review. J Cosmet Dermatol. 2022;21(5):1895–1904.
13. Viso S, Millán A, Rodríguez-Ares M. Rosacea-associated meibomian gland dysfunction- an epidemiological perspective. Eur Ophthalmic Rev. 2014;8:13–16. doi:10.17925/EOR.2014.08.01.13
14. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41–46. doi:10.1089/pho.2014.3819
15. Toyos R, Desai NR, Toyos M, Dell SJ. Intense pulsed light improves signs and symptoms of dry eye disease due to meibomian gland dysfunction: a randomized controlled study. PLoS One. 2022;17(6):e0270268. doi:10.1371/journal.pone.0270268
16. Yan X, Hong J, Jin X, et al. The efficacy of intense pulsed light combined with meibomian gland expression for the treatment of dry eye disease due to meibomian gland dysfunction: a multicenter, randomized controlled trial. Eye Contact Lens. 2021;47(1):45–53. doi:10.1097/ICL.0000000000000711
17. Arita R, Fukuoka S, Morishige N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul Surf. 2019;17(1):104–110. doi:10.1016/j.jtos.2018.11.004
18. Seo KY, Kang SM, Ha DY, Chin HS, Jung JW. Long-term effects of intense pulsed light treatment on the ocular surface in patients with rosacea-associated meibomian gland dysfunction. Cont Lens Anterior Eye. 2018;41(5):430–435. doi:10.1016/j.clae.2018.06.002
19. Suwal A, Hao JL, Zhou DD, Liu XF, Suwal R, Lu CW. Use of intense pulsed light to mitigate meibomian gland dysfunction for dry eye disease. Int J Med Sci. 2020;17(10):1385–1392. doi:10.7150/ijms.44288
20. Fishman HA, Periman LA, Shah AA. Real-time video microscopy of in vitro demodex death by intense pulsed light. Photobiomodul Photomed Laser Surg. 2020;38(8):472–476. doi:10.1089/photob.2019.4737
21. Dell SJ. Intense pulsed light for evaporative dry eye disease. Clin Ophthalmol. 2017;11:1167–1173. doi:10.2147/OPTH.S139894
22. Guo L, Kubat NJ, Isenberg RA. Pulsed radio frequency energy (PRFE) use in human medical applications. Electromagn Biol Med. 2011;30(1):21–45. doi:10.3109/15368378.2011.566775
23. Sadick NS, Malerich SA, Nassar AH, Dorizas AS. Radiofrequency: an update on latest innovations. J Drugs Dermatol. 2014;13(11):1331–1335.
24. Louis F, Fujii N, Katsuyama M, Okumoto S, Matsusaki M. Effects of radiofrequency and ultrasound on the turnover rate of skin aging components (skin extracellular matrix and epidermis) via HSP47-induced stimulation. Biochem Biophys Res Commun. 2020;:S0006-291X(20)30286–2. doi:10.1016/j.bbrc.2020.02.020
25. Araújo AR, Soares VP, Silva FS, Moreira Tda S. Radiofrequency for the treatment of skin laxity: mith or truth. An Bras Dermatol. 2015;90(5):707–721. doi:10.1590/abd1806-4841.20153605
26. Han JY, Park SY, Sunwoo JH, Kim JY, Tchah H, Lee H. Safety and efficacy of a low-level radiofrequency thermal treatment in an animal model of obstructive meibomian gland dysfunction. Lasers Med Sci. 2022;37(7):2907–2915. doi:10.1007/s10103-022-03559-3
27. Jaccoma EH, Litherland C, Jaccoma A, Ahmed A. Pellevé™ vs Lipiflow™ MGD-related dry eye treatment study: the ThermaLid™ procedure. Journal of Dry Eye and Ocular Surface Disease. 2018;1(1):e11–e21. doi:10.22374/jded.v1i1.2
28. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
29. Chester T, Garg SS, Johnston J, Ayers B, Gupta P. How can we best diagnose severity levels of dry eye disease: current perspectives. Clin Ophthalmol. 2023;17:1587–1604. doi:10.2147/OPTH.S388289
30. Lane SS, DuBiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396–404. doi:10.1097/ICO.0b013e318239aaea
31. Miller KL, Walt JG, Mink DR, et al. Minimal clinically important difference for the ocular surface disease index. Arch Ophthalmol. 2010;128(1):94–101. doi:10.1001/archophthalmol.2009.356
32. Ghadessi M, Tang R, Zhou J, et al. A roadmap to using historical controls in clinical trials - by drug information association adaptive design scientific working group (DIA-ADSWG). Orphanet J Rare Dis. 2020;15(1):69. doi:10.1186/s13023-020-1332-x
33. Viele K, Berry S, Neuenschwander B, et al. Use of historical control data for assessing treatment effects in clinical trials. Pharm Stat. 2014;13(1):41–54. doi:10.1002/pst.1589
34. Craig JP, Chen YH, Turnbull PRK. Prospective trial of intense pulsed Light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2015;56(3):1965–1970. doi:10.1167/iovs.14-15764
35. Wilson MW, Dailey RA. Eyelid malposition. In: Cioffi GA, editor. The Devers Manual: Ophthalmology for the Health Care Professional. Baltimore: Williams & Wilkins; 1997:27–35.
36. Zelickson BD, Kist D, Bernstein E, et al. Histological and ultrastructural evaluation of the effects of a radiofrequency-based nonablative dermal remodeling device: a pilot study. Arch Dermatol. 2004;140(2):204–209. doi:10.1001/archderm.140.2.204
37. Javate RM, Cruz RT Jr, Khan J, Trakos N, Gordon RE. Nonablative 4-MHz dual radiofrequency wand rejuvenation treatment for periorbital rhytides and midface laxity. Ophthalmic Plast Reconstr Surg. 2011;27(3):180–185. doi:10.1097/IOP.0b013e3181fe8e5a
38. Cuerda-Galindo E, Díaz-Gil G, Palomar-Gallego MA, Linares-GarcíaValdecasas R. Increased fibroblast proliferation and activity after applying intense pulsed light 800-1200 nm. Ann Anat. 2015;198:66–72. doi:10.1016/j.aanat.2014.11.005
39. Huang J, Luo X, Lu J, et al. IPL irradiation rejuvenates skin collagen via the bidirectional regulation of MMP-1 and TGF-β1 mediated by MAPKs in fibroblasts. Lasers Med Sci. 2011;26(3):381–387. doi:10.1007/s10103-010-0870-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intense Pulsed Light Combined with Low Level Blue and Red Light Therapy for Demodex-Associated Blepharitis
Farrant S, Giannaccare G, Lim CHL, Coco G
Clinical Ophthalmology 2025, 19:2575-2585
Published Date: 7 August 2025