Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Integration of Artificial Intelligence in Nursing Clinical Education: Enhancing the Mini-CEX Model
Authors Wang XJ, Song LJ, Jiao XP, Chen SQ
Received 27 June 2025
Accepted for publication 23 October 2025
Published 7 November 2025 Volume 2025:18 Pages 7327—7337
DOI https://doi.org/10.2147/JMDH.S550145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Xiao-Jun Wang,1,* Li-Juan Song,2,* Xue-Ping Jiao,2 Su-Qing Chen3
1The Second People’s Hospital of Yangquan City, Yangquan, People’s Republic of China; 2Department of Colorectal and Anal Surgery, Shanxi Province Cancer Hospital, Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences, Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, People’s Republic of China; 3Department of Gastrointestinal Center, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su-Qing Chen, Department of Gastrointestinal Center, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, No. 99 of Longcheng Road, Xiaodian District, Taiyuan, 030032, People’s Republic of China, Tel +86 13834698844, Email [email protected]
Objective: This study aimed to examine the integration of artificial intelligence (AI) into nursing clinical education, with particular emphasis on enhancing the Mini-Clinical Evaluation Exercise (Mini-CEX). The study focused on the role of AI in improving the objectivity of clinical performance assessment and the quality of feedback provided.
Methods: A mixed-methods approach was used, involving 140 undergraduate nursing students randomly assigned to a control or intervention group. The intervention group received conventional clinical instruction supplemented by an AI-assisted Mini-CEX. The AI was integrated during the assessment process to provide automated performance analysis of video-recorded clinical skills and transcripts of patient interactions. This analysis generated structured, individualized feedback reports for learners, which were then used by instructors to guide the dissemination of results in post-assessment debriefing sessions.
Results: The AI-supported Mini-CEX demonstrated a significant enhancement in the consistency and objectivity of clinical evaluations. In this study, artificial intelligence was specifically applied through automated performance analysis, real-time feedback delivery, and its integration into Mini-CEX assessments, thereby clarifying the role of AI within the instructional process. Learners in the intervention group achieved more rapid acquisition of technical skills and exhibited increased engagement, which was attributed to the provision of immediate and personalized feedback.
Conclusion: The incorporation of AI into the Mini-CEX framework, specifically for automating aspects of performance analysis and feedback generation, contributed to real-time, standardized, and learner-centered assessments. This approach improved the objectivity of evaluations while maintaining the integral role of human mentorship for interpretive guidance.
Keywords: artificial intelligence, clinical competence, educational technology, mini-clinical evaluation exercise, Mini-CEX, nursing education, performance assessment, real-time feedback
Introduction
The incorporation of artificial intelligence (AI) into healthcare education marks a significant advancement in the training of future nursing professionals to address the demands of increasingly complex clinical settings.1 Although traditional nursing education provides essential foundational knowledge, it often faces limitations in adapting to the expanding breadth of medical information, the necessity for personalized learning trajectories, and the expectation of consistently high-quality patient care delivery.2 The emergence of AI-driven educational tools has offered potential solutions to these challenges by improving the objectivity, efficiency, and scalability of instructional methods in nursing education.
Among the various assessment strategies, the Mini-Clinical Evaluation Exercise (Mini-CEX) has gained recognition as a structured, real-time, and formative tool for evaluating clinical competencies within authentic healthcare environments. However, its conventional application is frequently constrained by the intensive time requirements for educators and susceptibility to evaluator subjectivity and inconsistency;3 The integration of AI into the Mini-CEX framework introduces a novel approach characterized by continuous personalization of learning, immediate and data-informed feedback, and performance measurement aligned with standardized criteria.4
Although traditional nursing education provides essential foundational knowledge, it often faces limitations in adapting to the expanding breadth of medical information, the necessity for personalized learning trajectories, and the expectation of consistently high-quality patient care delivery. Recent studies have highlighted similar challenges, noting that conventional approaches lack sufficient scalability and personalization.3,5 However, its conventional application is frequently constrained by the intensive time requirements for educators and susceptibility to evaluator subjectivity and inconsistency. The novelty of this study lies in combining AI-based automated feedback mechanisms with the Mini-CEX framework, thereby addressing existing gaps in objectivity, timeliness, and learner-centered assessment. Furthermore, AI platforms are capable of aggregating and synthesizing extensive datasets from multiple learners, which supports performance benchmarking and informs curricular enhancements at the institutional level. Empirical findings also suggest that AI can improve student engagement and accelerate skill acquisition in nursing education by providing real-time individualized feedback and reducing variability in evaluations.2,6–8
The potential of AI to transform clinical assessment is a rapidly advancing field of inquiry. Recent studies have begun to explore the integration of AI with established assessment tools. For instance, research has demonstrated the feasibility of using AI and natural language processing (NLP) to evaluate medical students’ communication skills during clinical encounters, providing objective metrics that complement faculty evaluations.1,2 Similarly, computer vision algorithms have been deployed to assess procedural skills in surgery and emergency medicine, offering real-time feedback on technical proficiency.3,4
Specific to nursing education, Buchanan et al2 highlighted in their scoping review that AI is predicted to significantly impact nursing education through personalized learning and automated assessment, though they noted a scarcity of empirical studies at the time. More recently, Hwang et al3 profiled the applications of AI in nursing education research, identifying a trend towards intelligent tutoring systems and student performance prediction. However, their analysis also revealed that the direct application of AI to formative clinical assessment tools remains underexplored.
While these studies establish a foundational promise, a significant gap exists in the rigorous, empirical integration of AI with the Mini-CEX for nursing students. Many existing works are conceptual, focus on predictive analytics, or are situated in medical rather than nursing education. The novelty of this study lies in its specific focus on augmenting the Mini-CEX framework with a multimodal AI system (utilizing both computer vision and NLP) to provide automated, objective performance analysis and structured feedback. This approach directly addresses the identified gaps in objectivity, timeliness, and scalability of clinical assessments in nursing education, moving beyond conceptual prediction to empirical validation of an AI-augmented assessment model.
Accordingly, the effective integration of AI into nursing education requires deliberate design that upholds the core principles of nursing practice—compassion, safety, and individualized patient care. This study examines the potential of AI to enhance the. The Mini-CEX is a structured and real-time clinical evaluation tool that assesses core competencies of nursing students during authentic patient encounters. This study employs a mixed-methods design to compare a traditional Mini-CEX model against an AI-augmented version. The AI augmentation is based on discriminative machine learning models, specifically leveraging computer vision for automated analysis of procedural technique and natural language processing (NLP) for evaluating communication skills. The comparison focuses on quantitative and qualitative outcomes, including skill acquisition, learner satisfaction, and instructional efficiency.
Materials and Methods
Study Participants
A convenience sampling method was used to recruit 140 undergraduate nursing students who commenced their clinical internship at a tertiary Class-A hospital in April 2023. The participants were randomly assigned to either a control group or an intervention group, with 70 students in each group.
The inclusion criteria consisted of the following: inclusion criteria required nursing educators with at least five years of clinical teaching experience. This threshold was chosen to ensure that evaluators possessed sufficient pedagogical expertise and clinical judgment to deliver reliable Mini-CEX assessments. The exclusion criteria were: (1) participants who were not undergraduate nursing students from the April 2023 cohort; and (2) those who declined to participate. Questionnaires were excluded if the proportion of missing items exceeded 10%.
Ethical approval for the study was granted by the hospital’s Medical Ethics Committee (Approval No.: SYDELL-2023-005). Informed consent was obtained from all participants, who voluntarily agreed to participate in the research. The participants did not receive renumeration or reward.
Teaching Methods
Faculty Team
The teaching staff assigned to both groups consisted of qualified nurse instructors who held the title of “supervising nurse” or above and had a minimum of five years of clinical teaching experience. All instructors had completed standardized training and assessments and were certified as “dual-qualified” teachers in accordance with hospital requirements, thereby demonstrating proficiency in both theoretical knowledge and clinical practice.
Control Group Teaching
The control group was provided with standardized training based on the clinical internship teaching syllabus established by the hospital. This training included one-on-one clinical mentorship, and specialty-specific knowledge instruction was delivered at the beginning of each rotation. Upon completion of each specialty rotation, theoretical knowledge and clinical skill assessments were administered to both groups. The control group was evaluated using the standard Mini-CEX without AI augmentation, while the intervention group was assessed using the AI-assisted Mini-CEX as described. The AI component was implemented via a dedicated digital platform that incorporated automated video-based performance analysis, real-time scoring support, and structured feedback generation.
Intervention Group Teaching
The intervention group received the same clinical internship training as the control group, supplemented by a hybrid teaching model that integrated the Nursing Mini-CEX with case-based teaching. The implementation process was conducted as outlined below:
Formation of the Teaching Team
A teaching team was established, comprising of the head of the nursing research office, the deputy head of the nursing department, and six clinical teaching faculty members. The team consisted of eight members, including two with master’s degrees and six with bachelor’s degrees. All members underwent standardized training and assessment.
Development of the Teaching Plan
Relevant domestic and international literature was reviewed by the teaching team to develop a teaching plan aligned with the clinical and educational needs of undergraduate nursing students. The primary objective was to enhance both clinical competence and empathetic capacity. An initial version of the plan was formulated following internal discussions within the teaching team. The intervention plan was subsequently assessed by an expert panel, resulting in a 100% positive response rate, a judgment coefficient of 0.96, and an authority coefficient of 0.98.3 These results indicated that the teaching intervention was both scientifically sound and feasible.
Implementation of the Teaching Plan
Training Content
Training encompassed five essential nursing procedures along with the corresponding theoretical knowledge: two-person cardiopulmonary resuscitation (CPR), electrocardiogram (ECG) monitoring, oxygen administration, peripheral venous catheter insertion, and basic wound care (including techniques for hemostasis, bandaging, and fixation). Each procedure was taught through the use of real-life clinical case studies. The Mini-CEX framework was incorporated to assess nursing evaluation, physical examination, clinical diagnosis, intervention implementation, provision of health education, delivery of humanistic care, organizational efficiency, and overall performance.
Training Methodology
Training was conducted using a blended approach that included both offline and online methods. Offline instruction consisted of scheduled in-person training sessions, whereas online learning involved access to instructional videos demonstrating the required procedures. These videos were made available for self-paced review, with student progress monitored by the teaching faculty.
Training Timeline (7 Months)
Prior to the commencement of clinical practice, both groups were provided with standardized demonstrations and initial evaluations. Procedural demonstrations were conducted using case-based teaching integrated with the Mini-CEX framework. Additionally, instructional videos were developed under the supervision of the nursing research office to offer students standardized learning resources.
Practice exercises were carried out by the students using clinical cases prepared by the teaching team, with Mini-CEX assessments conducted at each stage of the training. A total of 10 assessments were completed during this phase, and feedback was provided by the teaching team to address identified performance issues.
Four experienced nurses, each with a minimum of three years of clinical practice, were selected to serve as standardized patients. These individuals demonstrated familiarity with disease diagnosis and nursing procedures. The simulation-based assessment was conducted using the Mini-CEX framework, with an emphasis on communication skills and patient observation abilities.
Formative assessments were conducted by the teaching team throughout the process to monitor student progress and provide instructional guidance, thereby facilitating the gradual improvement of theoretical knowledge and nursing skills.
Evaluation Indicators and Methods
Skill Operations and Theoretical Knowledge
Both the intervention and control groups underwent pre- and post-intervention assessments using a standardized 50-item nursing operation scoring rubric. The assessment included practical evaluations of the following procedures: two-person CPR, ECG monitoring, oxygen administration, peripheral venous catheter insertion, and basic wound care (including hemostasis, bandaging, and fixation). In addition, theoretical knowledge related to each procedure was assessed. Both theoretical and practical components were scored on a 100-point scale, and the theoretical portion was assessed through oral questioning.
Clinical Comprehensive Ability
Clinical competency was assessed using the Nursing Mini-CEX scale developed by Motefakker S et al.9 The scale demonstrated good reliability, with a reported Cronbach’s α coefficient of 0.78. The evaluations measured performance across key domains, including history-taking, physical examination, clinical reasoning, communication, humanistic care, and professionalism. Each component was rated on a 9-point scale, with scores of 1–3 indicating poor performance, 4–6 indicating satisfactory performance, and 7–9 indicating excellent performance. Evaluations were carried out during practical assessments.
Statistical Analysis
Data were analyzed using SPSS version 26.0 statistical software. For variables that conformed to a normal distribution, results were expressed as mean ± standard deviation (x ± s), and intergroup comparisons were conducted using independent t-tests. For non-normally distributed data, the median and interquartile range [M (IQR)] were reported, with group differences analyzed using the Mann–Whitney U-test. Categorical variables were presented as frequencies and percentages, and intergroup comparisons were performed using the chi-squared (χ2) test. A p-value of < 0.05 was considered indicative of statistical significance. Descriptive analyses of pre- and post-intervention scores were presented as x ± s to facilitate visualization of score changes.
Results
General Data
A total of 140 nursing students were included in the study and evenly assigned to an intervention group (n = 70) and a control group (n = 70). No participants withdrew from the study, resulting in full completion by all enrolled students. Baseline characteristics, including age and gender distribution, were comparable between the two groups. The mean age of the intervention group was 21.51 years (± 0.94), while that of the control group was 21.58 years (± 0.11), with no statistically significant difference observed (p = 0.743). The proportion of female students was 85.7% in the intervention group and 84.3% in the control group, with no significant difference identified in gender distribution (p = 0.813) based on the chi-square test. These findings indicated that the two groups were demographically well matched, supporting the attribution of any differences in outcomes to the effects of the training interventions rather than baseline variables (Table 1). We conducted semi-structured interviews with a subset of participants, which were transcribed and analyzed using inductive thematic analysis by two independent researchers to identify key themes.
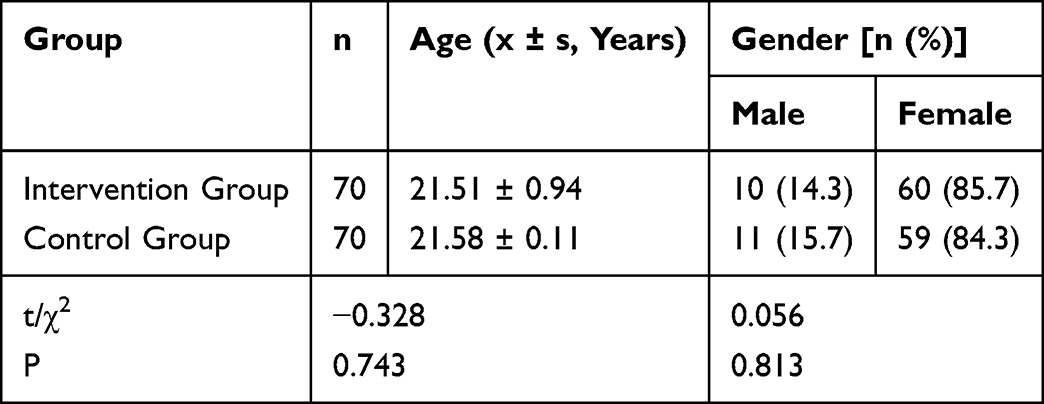 |
Table 1 General Information of Nursing Undergraduates |
Comparison of Nursing Skill Operation and Theoretical Scores Prior to and After Training
Prior to the training intervention, no statistically significant differences were identified between the intervention and control groups in terms of nursing skills and theoretical knowledge (p > 0.05). Following the intervention, both groups exhibited significant improvements in nursing procedural performance and theoretical examination scores compared to their respective pre-training values. Notably, the intervention group demonstrated superior post-training performance in specific nursing skills, including hemostasis, bandaging, fixation, and superficial vein indwelling needle infusion. For instance, in the skill set involving hemostasis, bandaging, and fixation, scores in the intervention group increased from 91.50 (± 3.43) to 96.28 (± 2.22), whereas the control group improved from 91.51 (± 3.40) to 94.98 (± 2.15). The post-training scores of the intervention group were significantly higher than those of the control group (p < 0.05), indicating that the applied intervention exerted a greater effect on enhancing clinical nursing skills and theoretical comprehension (Table 2).
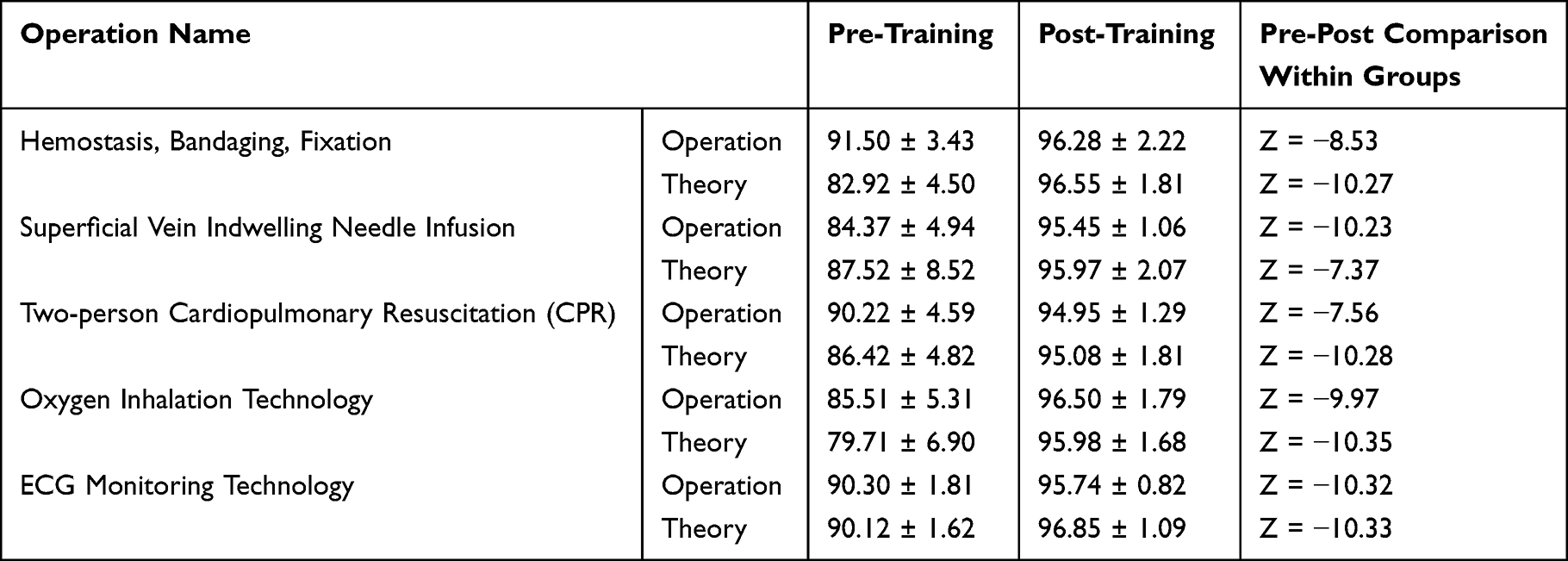 |
Table 2 Comparison of Nursing Technique Operation and Theoretical Scores Before and After Training (x ± s, Score) |
Comparison of Mini-CEX Scores Prior to and After Training
Improvements in Mini-CEX scores, which assess competency across a range of clinical tasks, were observed in both groups following the training intervention (Table 3). However, the intervention group demonstrated significantly higher performance in several key domains, including nursing inquiry, physical examination, and health consultation (Table 4). For example, in general wound care procedures like hemostasis, bandaging, and fixation, the intervention group achieved a post-training score of 6.92 (± 0.90) in the humanistic care domain, compared to 6.41 (± 0.83) in the control group, with the difference reaching statistical significance (p < 0.05) (Table 5).
 |
Table 3 Comparison of Mini-CEX Scores Before and After Training in General Wound Treatment (Hemostasis, Bandaging, Fixation Techniques) |
 |
Table 4 Comparison of Mini-CEX Scores in Superficial Vein Indwelling Needle Infusion Technology |
 |
Table 5 Comparison of Mini-CEX Scores in Dual Cardiopulmonary Resuscitation (CPR) |
Similarly, in procedures involving CPR and oxygen administration, the intervention group obtained higher scores across all Mini-CEX domains, including organizational effectiveness, overall evaluation, and humanistic care (Table 6). Although large effect sizes were noted in both groups in pre- and post-intervention comparisons, consistently superior performance was demonstrated by the intervention group. These findings indicate that the structured training intervention contributed not only to the development of technical skills but also to the enhancement of a holistic approach to patient care, encompassing interpersonal communication and humanistic competencies.
 |
Table 6 Comparison of Mini-CEX Scores in Oxygen Inhalation Technology |
The Mini-CEX results support the conclusion that the intervention group experienced a more comprehensive improvement in clinical capabilities, which may be attributed to the focused and intensive nature of the training. These outcomes highlight the value of integrating practical, scenario-based learning into nursing education to enhance clinical competency in real-world settings.
Discussion
Impact of the Training Intervention on Clinical Competence: A Focus on Nursing Skill Development
The findings of this study highlight the substantial impact of the AI-augmented Mini-CEX training intervention on nursing students’ clinical competence, with a particular focus on skill development across multiple dimensions of practice. Clinical competence in nursing education encompasses technical proficiency, critical thinking, communication skills, and the ability to provide safe, patient-centered care. Traditional methods of training, while valuable, often fall short in providing individualized feedback at scale or ensuring consistency across evaluators. In this regard, the intervention addressed key limitations by supplementing conventional clinical instruction with structured, AI-supported assessments that provided real-time guidance. Students in the intervention group demonstrated accelerated acquisition of procedural and cognitive skills, suggesting that AI integration is not merely additive but transformative in reshaping the way competence is cultivated.
A central strength of the intervention lies in its capacity to standardize the evaluation process while tailoring feedback to the unique needs of each learner. Unlike traditional Mini-CEX assessments, which rely heavily on the subjective judgment of faculty members, the AI component employed automated performance analysis tools to detect specific errors in execution and to benchmark learner performance against established standards. This not only mitigated the variability introduced by human evaluators but also empowered students with actionable insights that were immediately relevant to their clinical practice. For instance, learners reported that the AI-generated feedback provided clarity regarding both technical errors, such as incomplete aseptic technique, and non-technical issues, such as hesitations in patient communication. The integration of these insights into subsequent training sessions fostered iterative improvement and reinforced the development of both technical and interpersonal competencies.
The observed outcomes are consistent with previous research demonstrating that technology-enhanced assessment tools can contribute to skill mastery in healthcare education. Several studies in medical and nursing education have suggested that digital platforms support repetitive practice, facilitate individualized feedback, and promote learner autonomy.10–18 However, this study advances the field by providing empirical evidence that AI-supported assessments can yield measurable improvements in performance indicators such as procedural accuracy, communication clarity, and overall competency ratings. Importantly, the results also indicate that improvements were not limited to technical procedures but extended to broader aspects of professional behavior, including empathy, situational awareness, and adherence to ethical standards.
Another critical aspect of the intervention was its influence on learners’ engagement with the training process. Nursing students frequently face challenges in maintaining sustained motivation during clinical rotations, especially when feedback is delayed or inconsistent. The immediacy of AI-supported feedback in this study appears to have enhanced engagement, as students reported feeling more accountable for their performance and more empowered to take ownership of their learning. This heightened engagement likely contributed to the observed acceleration in skill acquisition, underscoring the importance of timely and specific feedback in competency-based education.
From a pedagogical standpoint, the intervention underscores the evolving role of AI in bridging the gap between formative and summative assessments. By embedding AI into the Mini-CEX framework, the evaluation process was transformed into a dynamic learning opportunity rather than a static judgment of performance. This aligns with contemporary shifts in nursing education toward competency-based frameworks that emphasize continuous improvement and learner-centered approaches. Furthermore, the intervention demonstrated that AI can be integrated without replacing the role of human educators; rather, it complemented their expertise by providing objective metrics that enriched the feedback process.
Role of Mini-CEX in Assessing Clinical Performance and Enhancing Feedback Loops: Empowering Teaching with AI
The Mini-Clinical Evaluation Exercise (Mini-CEX) has long been recognized as an effective tool for assessing clinical performance in authentic healthcare settings, yet its implementation in nursing education has been hindered by several practical challenges. Chief among these are the subjective variability of evaluator judgments, the considerable time burden for faculty, and the difficulty in providing timely and actionable feedback to students. The findings of this study indicate that augmenting the Mini-CEX with artificial intelligence can meaningfully address these limitations, thereby empowering teaching practices and enriching the learning experience. The integration of AI within the Mini-CEX did not replace the established framework but enhanced its utility by embedding data-driven insights and facilitating a more consistent, transparent, and learner-centered feedback process.
One of the most significant contributions of AI to the Mini-CEX framework is the standardization of evaluation criteria.19 Traditional Mini-CEX assessments rely heavily on faculty members’ interpretations of performance, which can vary widely depending on personal experience, expectations, or unconscious bias. In this study, the AI component analyzed student performance using objective markers such as procedural precision, communication efficiency, and adherence to established clinical protocols. This helped reduce evaluator subjectivity and improved inter-rater reliability, thereby ensuring that assessment outcomes were not unduly influenced by individual variation. Students benefited from knowing that their evaluations reflected standardized benchmarks rather than fluctuating criteria.
The AI-supported Mini-CEX also enhanced the feedback loop between learners and educators. Feedback in clinical education is most effective when it is specific, timely, and directly actionable. However, faculty constraints often delay feedback or limit its depth. The AI system employed in this study generated immediate, structured feedback reports that highlighted strengths, identified specific areas for improvement, and suggested targeted practice strategies. These reports were accessible to both students and instructors, enabling follow-up discussions that were grounded in objective evidence. By combining the immediacy of AI-generated insights with the interpretive expertise of faculty, the intervention fostered richer dialogues and strengthened the feedback loop.
Furthermore, the AI-enhanced Mini-CEX contributed to the scalability of clinical assessments in resource-limited educational contexts. Nursing schools often face faculty shortages, which make it difficult to provide individualized feedback to all students. The AI system alleviated some of this burden by automating aspects of performance analysis and documentation, thereby freeing faculty to focus on higher-order mentoring and professional development. In this way, the intervention demonstrated how AI can serve as a pedagogical partner rather than a replacement for human educators. Faculty members were able to devote more time to nuanced discussions of professionalism, empathy, and ethical reasoning, while the AI platform managed routine analysis and documentation tasks.
Beyond efficiency and consistency, the integration of AI into the Mini-CEX also promoted greater learner autonomy. By providing students with accessible feedback dashboards, the system empowered them to self-monitor progress and take ownership of their development. Learners reported using these dashboards to track improvements over time and to identify recurring challenges, which allowed them to engage in self-directed practice outside of formal clinical encounters. This aligns with modern educational theories that emphasize active, learner-driven approaches to professional development.
Importantly, the study findings highlight that AI-enhanced Mini-CEX can strengthen the educational value of formative assessments by transforming them into iterative learning experiences. Rather than perceiving the Mini-CEX as a summative judgment at discrete time points, students engaged with it as an ongoing process of self-improvement, reinforced by both human and AI feedback.
Significance of Patient-Centered Care in Nursing Education and Its Long-Term Impact
Patient-centered care remains a foundational principle of nursing education and practice, emphasizing the holistic consideration of patients’ needs, preferences, and values in the delivery of healthcare. Although the primary focus of this study was the integration of AI into the Mini-CEX framework, it is essential to contextualize these innovations within the broader goal of preparing nurses to deliver patient-centered care. The findings suggest that while AI-enhanced assessments primarily targeted improvements in skill acquisition and feedback mechanisms, they also indirectly contributed to strengthening patient-centered competencies among nursing students. This is because clinical competence in nursing is inseparable from the capacity to communicate empathetically, respect patient autonomy, and integrate ethical considerations into practice.
The incorporation of AI into clinical training raised important opportunities for reinforcing patient-centered care principles. For instance, the AI system not only evaluated technical procedures but also identified communication patterns, such as clarity of explanations and responsiveness to patient concerns. By drawing attention to these dimensions, the intervention underscored that effective clinical performance extends beyond procedural accuracy to include relational and humanistic aspects of care. Learners who received AI-generated feedback on communication and interpersonal interactions reported greater awareness of their role in fostering trust and understanding with patients. This finding is significant, as it demonstrates that digital tools can be leveraged to highlight the humanistic aspects of nursing practice, rather than reducing training to a purely technical exercise.
Another long-term implication of embedding patient-centered care within AI-supported training is the potential to instill reflective practice among students. Nursing education increasingly emphasizes the importance of reflection as a means of integrating theory with practice and developing professional identity. The structured feedback reports generated by the AI system provided students with opportunities to reflect on both strengths and areas for improvement, particularly in domains related to empathy, compassion, and patient advocacy. Reflection on these qualities is critical for developing a patient-centered orientation that persists throughout one’s career. By embedding reflection into the assessment process, the intervention encouraged learners to internalize patient-centered values alongside technical skills.
The significance of patient-centered care also extends to broader health system outcomes. Nurses who are trained to consistently prioritize patients’ needs contribute to improved satisfaction, adherence to treatment, and clinical outcomes. In this sense, the indirect impact of AI-enhanced training on patient-centered care may translate into tangible improvements in healthcare delivery over time. Although the present study did not conduct longitudinal follow-up of patient outcomes, the observed improvements in communication and empathy suggest that learners are being better prepared to deliver care that aligns with these principles. Future studies should consider investigating whether graduates of AI-supported programs demonstrate measurable differences in patient-reported outcomes compared to those trained with conventional methods.
It is also important to acknowledge potential risks and challenges associated with integrating AI into nursing education from a patient-centered perspective. Overreliance on technology may inadvertently shift focus away from the relational aspects of care if not carefully designed. To mitigate this risk, AI systems should be explicitly programmed to evaluate and provide feedback on interpersonal skills, cultural competence, and ethical decision-making, in addition to technical performance. Educators must remain vigilant to ensure that technology complements rather than displaces the humanistic dimensions of nursing.
Limitations
This study evaluated the integration of AI into the Mini-CEX model, showing improved learner satisfaction, enhanced skill acquisition, and increased consistency of evaluation. However, several limitations should be considered. Limitations include reliance on structured video analysis, sample size, and short-term outcomes. Future studies should employ longer follow-up periods and include multi-center samples to enhance generalizability.
Conclusion
This study demonstrated that the integration of a machine learning-based AI tool—which provided automated performance analysis of clinical skills and communication—significantly enhanced the Mini-CEX framework within nursing education. The objective, data-driven feedback generated by the AI led to more consistent evaluations and was associated with accelerated skill acquisition and higher learner engagement compared to traditional methods.
These findings affirm that AI can be a powerful tool for augmenting clinical assessment by making it more objective, efficient, and learner-centered. For the broader field, this signifies a pivotal step toward data-informed nursing education. Future implementation must carefully balance technological advancement with the indispensable role of human mentorship, ensuring that AI serves to uphold, rather than undermine, the foundational humanistic values of the nursing profession.
Abbreviations
AI, Artificial Intelligence; Mini-CEX, Mini-Clinical Evaluation Exercise; NLP, natural language processing.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The investigation was sanctioned by the the Ethics Committee of the Second People’s Hospital of Yangquan City, Shanxi Province (Approval No.: SYDELL-2023-005). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all patients.
Consent for Publication
All participants signed a document of informed consent.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Irwin P, Jones D, Fealy S. What is ChatGPT and what do we do with it? Implications of the age of AI for nursing and midwifery practice and education: an editorial. Nurse Educ Today. 2023;127:105835. PMID: 37267643. doi:10.1016/j.nedt.2023.105835
2. Buchanan C, Howitt ML, Wilson R, Booth RG, Risling T, Bamford M. Predicted influences of artificial intelligence on nursing education: scoping review. JMIR Nurs. 2021;4(1):e23933. PMID: 34345794; PMCID: PMC8328269. doi:10.2196/23933
3. Hwang GJ, Tang KY, Tu YF. How artificial intelligence (AI) supports nursing education: profiling the roles, applications, and trends of AI in nursing education research (1993–2020). Interactive Learning Environ. 2022;1–20. doi:10.1080/10494820.2022.2147959
4. Robert N. How artificial intelligence is changing nursing. Nurs Manage. 2019;50(9):30–39. PMID: 31425440; PMCID: PMC7597764. doi:10.1097/01.NUMA.0000578988.56622.21
5. Russell RG, Lovett Novak L, Patel M, et al. Competencies for the use of artificial intelligence-based tools by health care professionals. Acad Med. 2023;98(3):348–356. PMID: 36731054. doi:10.1097/ACM.0000000000004963
6. Gabrielli S, Piras EM, Mayora Ibarra O. Digital twins in the future design of digital therapeutics. In
7. Norcini JJ, Blank LL, Duffy FD, Fortna GS. The mini-CEX: a method for assessing clinical skills. Ann Intern Med. 2003;138(6):476–481. PMID: 12639081. doi:10.7326/0003-4819-138-6-200303180-00012
8. Liu YP, Jensen D, Chan CY, et al. Development of a nursing-specific Mini-CEX and evaluation of the core competencies of new nurses in postgraduate year training programs in Taiwan. BMC Med Educ. 2019;19(1):270. PMID: 31319845; PMCID: PMC6639917. doi:10.1186/s12909-019-1705-9
9. Motefakker S, Shirinabadi Farahani A, Nourian M, et al. The impact of the evaluations made by Mini-CEX on the clinical competency of nursing students. BMC Med Educ. 2022;22(1):634. PMID: 35987659; PMCID: PMC9392056. doi:10.1186/s12909-022-03667-2
10. Nisheva-Pavlova M. AI courses for secondary and high school-comparative analysis and conclusions. ERIS. 2021;9:16.
11. Ouyang F, Zheng L, Jiao P. Artificial intelligence in online higher education: a systematic review of empirical research from 2011 to 2020. Educat Inform Technol. 2022;27(6):7893–7925. doi:10.1007/s10639-022-10925-9
12. El Arab RA, Al Moosa OA, Sagbakken M, et al. Integrative review of artificial intelligence applications in nursing: education, clinical practice, workload management, and professional perceptions. Front Public Health. 2025;13:1619378. PMID: 40823249; PMCID: PMC12354398. doi:10.3389/fpubh.2025.1619378
13. Schreier AM, Peery AI, McLean CB. An integrative curriculum for accelerated nursing education programs. J Nurs Educ. 2009;48(5):282–285. PMID: 19476034. doi:10.3928/01484834-20090416-08
14. Adhikari R, Tocher J, Smith P, Corcoran J, MacArthur J. A multi-disciplinary approach to medication safety and the implication for nursing education and practice. Nurse Educ Today. 2014;34(2):185–190. PMID: 24219921. doi:10.1016/j.nedt.2013.10.008
15. Montejo L, Fenton A, Davis G. Artificial intelligence (AI) applications in healthcare and considerations for nursing education. Nurse Educ Pract. 2024;80:104158. PMID: 39388757. doi:10.1016/j.nepr.2024.104158
16. Hu MY, Yi TX, Liu QR, et al. Artificial intelligence and network pharmacology reveal the medication rules of Professor Wang Yu-Ying in the treatment of climacteric syndrome. World J Tradit Chin Med. 2024;10:180–190. doi:10.4103/2311-8571.382287
17. Sapci AH, Sapci HA. Teaching Hands-On Informatics Skills to Future Health Informaticians: a Competency Framework Proposal and Analysis of Health Care Informatics Curricula. JMIR Med Inform. 2020;8(1):e15748. PMID: 31961328; PMCID: PMC7001041. doi:10.2196/15748
18. Prideaux D. ABC of learning and teaching in medicine. Curriculum design. BMJ. 2003;326(7383):268–270. PMID: 12560283; PMCID: PMC1125124. doi:10.1136/bmj.326.7383.268
19. Negrete D, Lopes SLPC, Barretto MDA, et al. Artificial intelligence and dentomaxillofacial radiology education: innovations and perspectives. Dent J. 2025;13(6):245. PMID: 40559148; PMCID: PMC12192462. doi:10.3390/dj13060245
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Revolutionizing Nursing Education in Somalia: Recommendations for Integrating AI and Deep Learning in Outcome Based Assessments to Enhance Knowledge, Practice, and Graduate Competence
Yusuf FY, Hussein AM
Journal of Multidisciplinary Healthcare 2026, 19:611974
Published Date: 22 May 2026
Integrating Artificial Intelligence with Gamification in Medical Education: A Pedagogically Grounded Framework and Critical Review
Bharatha A, Ojeh N, Campbell MH, Krishnamurthy K, Sangishetti VP, Bhuvanagiri L, Gupta S, Rahman S, Reddy S, Majumder MAA
Advances in Medical Education and Practice 2026, 17:612934
Published Date: 14 July 2026