Back to Journals » Cancer Management and Research » Volume 18

Integrating Ultrasound and Clinicopathologic Characteristics to Predict the Invasive Papillary Thyroid Carcinoma Among Indeterminate Thyroid Nodules
Authors Yao M, Zhang Z, Hua Z, Chen Y, Zhao S, Sun Y, Shen J, Zhang X
Received 29 October 2025
Accepted for publication 24 March 2026
Published 28 March 2026 Volume 2026:18 577043
DOI https://doi.org/10.2147/CMAR.S577043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Harikrishna Nakshatri
Minfang Yao,1,2 Zheng Zhang,1 Zheng Hua,1 Yanwei Chen,1 Shuangshuang Zhao,1 Yajun Sun,3 Jun Shen,1,2 Xin Zhang1
1Department of Medical Ultrasound, Affiliated Hospital of Jiangsu University, Zhenjiang, 212000, People’s Republic of China; 2Department of Medical Ultrasound, Kunshan second People’s Hospital, Suzhou, 215300, People’s Republic of China; 3Department of Pathology, Affiliated Hospital of Jiangsu University, Zhenjiang, 212000, People’s Republic of China
Correspondence: Xin Zhang, Department of Medical Ultrasound, Affiliated Hospital of Jiangsu University, Zhenjiang, 212000, People’s Republic of China, Tel +86-13775554185, Email [email protected]
Purpose: The management of indeterminate thyroid nodules (ITNs; Bethesda III–V) poses significant clinical challenges. This study sought to identify preoperative ultrasound and clinicopathologic predictors of invasive papillary thyroid carcinoma (PTC) among ITNs and to develop a corresponding risk prediction model.
Patients and Methods: In this retrospective study, 494 patients with FNA-confirmed ITNs and postoperative PTC diagnosis were included. Based on pathology confirming extrathyroidal extension and/or lymph node metastasis, patients were classified as invasive PTC (n=141) or non-invasive PTC (n=353). Univariate and multivariate logistic regression analyses identified independent risk factors, and a predictive nomogram was developed and validated.
Results: Male (odds ratio [OR]=2.91, 95% confidence interval [CI]:1.78– 4.76), age ≤ 45 years (OR=1.93, 95% CI:1.23– 3.03), abundant nodule vascularity (OR=4.60, 95% CI:2.42– 8.75), and capsule proximity ≤ 2 mm (OR=3.63, 95% CI:2.15– 6.14) were independent risk factors for invasive PTC, while abnormal thyroglobulin antibody (TgAb) levels reduced risk (OR=0.38, 95% CI:0.18– 0.77). The prediction model achieved an AUC of 0.776 (95% CI:0.728– 0.825) in the training set and 0.759 (95% CI:0.643– 0.874) in validation, with decision curve analysis confirming clinical utility.
Conclusion: An integrated model incorporating sex, age, vascularity, capsule distance, and TgAb status effectively predicts invasive PTC risk in ITNs. The nomogram provides preoperative risk stratification to guide personalized treatment, potentially reducing unnecessary aggressive surgery in low-risk cases while ensuring optimal management of high-risk patients. An interactive online version is available for clinical implementation.
Keywords: ultrasound, indeterminate thyroid nodules, invasive papillary thyroid carcinoma
Introduction
Thyroid nodules are a common clinical finding, with detection rates having increased markedly over the past three decades.1 Ultrasonography is the primary modality for the initial assessment of thyroid nodules.2 Ultrasound-guided fine needle aspiration (FNA) cytology is a key method for further evaluating the benign or malignant nature of these nodules.3 FNA results are classified using The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC), which categorizes nodules into Bethesda classes I through VI. Specifically, Bethesda classes III, IV, and V are classified as indeterminate thyroid nodules (ITNs),4 with associated malignancy risks of 13–30%, 23–34%, and 67–83%, respectively.4,5 Management options for these categories include repeat FNA, molecular testing, diagnostic lobectomy, total thyroidectomy, or surveillance, posing significant challenges for clinical decision-making.
When clinical evidence suggests a high suspicion of malignancy in ITNs, further intervention is warranted. Over 80% of malignant thyroid nodules are papillary thyroid carcinoma (PTC).6 Within PTC, a subset of low-risk variants may be managed with alternatives to lobectomy, such as active surveillance or minimally invasive ablation techniques.7–10 These approaches aim to reduce surgical risks, avoid scarring, and mitigate overtreatment of indolent tumors.11 In addition, patients with low-risk papillary thyroid microcarcinoma (PTMC) may experience decision regret after thyroidectomy,12 which also provides important evidence for exploring more conservative management strategies. However, some PTCs exhibit aggressive features, including local or distant metastasis and extrathyroidal extension, which are associated with relatively poor prognoses.13 For such cases, lobectomy alone may constitute insufficient initial treatment, making more extensive total thyroidectomy the preferred option, often accompanied by central compartment lymph node dissection.8,14
Current research on ITNs primarily focuses on assessing malignancy risk,15–21 rather than stratifying surgical patients by risk. Existing risk stratification systems, such as the TI-RADS and ATA guidelines, are predominantly designed for preoperative malignancy risk assessment and have limited capacity to guide the extent of surgical intervention. Ultrasound remains the principal imaging modality for thyroid nodule diagnosis,22 and is a valuable examination tool,23 with high-resolution ultrasound being standard for evaluating thyroid cancer.2
This study retrospectively analyzes patients with ITNs who underwent surgical resection and received a postoperative diagnosis of PTC. We aim to identify risk factors for invasive PTC and construct a predictive model based on available ultrasonic and clinicopathological characteristics. In contrast to existing systems that focus on malignancy detection, our model is specifically designed for preoperative risk stratification of invasiveness, aiming to complement current guidelines by assisting clinicians in determining the appropriate extent of surgery (eg, lobectomy vs. total thyroidectomy). This model is expected to offer precise individualized treatment plans, improving treatment efficacy while avoiding unnecessary surgery.
Materials and Methods
Study Design and Population
This retrospective study was approved by the Ethics Committee of Affiliated Hospital of Jiangsu University (Approval Number: SWYXLL20190225-2).
We retrospectively collected data from patients who underwent ultrasound-guided FNA at the Affiliated Hospital of Jiangsu University between March 2016 and October 2024. Inclusion required cytological results classified as Bethesda III, IV, or V, and a postoperative pathological diagnosis of PTC. Clinical, pathological, and preoperative thyroid ultrasound data were collected. Based on postoperative pathology as the gold standard, patients were categorized into invasive PTC and non-invasive PTC groups.
Invasive PTC was defined as exhibiting extrathyroidal extension (ETE) and/or local lymph node metastasis. ETE was defined according to the 8th edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual as tumor invasion into surrounding structures, including strap muscles, larynx, trachea, esophagus, recurrent laryngeal nerve, prevertebral fascia, or encasement of the carotid artery or mediastinal vessels.24
Inclusion Criteria
(a) Age ≥18 years;
(b) Preoperative routine thyroid ultrasound examination performed;
(c) US-FNA cytology classified as Bethesda III, IV, or V followed by surgical resection and postoperative pathological confirmation of PTC;
(d) Availability of complete preoperative clinical records.
Exclusion Criteria
(a) Family history of thyroid cancer;
(b) History of any malignancy;
(c) History of head and neck radiotherapy;
(d) Postoperative pathology indicating a benign lesion or a thyroid malignancy other than PTC;
(e) Incomplete thyroid function laboratory data.
After applying these criteria, 494 patients were included in the final analysis (Figure 1).
 |
Figure 1 Patient Selection Flowchart. |
Ultrasound (US) Evaluation
All thyroid nodules underwent ultrasound assessment. Two senior radiologists, each with over 10 years of experience in thyroid imaging, independently evaluated the US features. Any discrepancies between their assessments were resolved by re-evaluation and consensus with a third experienced radiologist.
The US evaluation was performed according to the 2023 Korean Thyroid Radiology Society (K-TRADS) consensus25 and the 2017 American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) guidelines.26 The following features were assessed: (a) echogenicity; (b) aspect ratio; (c) calcification; (d) location; (e) vascularity; (f) distance to capsule; (g) maximum nodule diameter.
Clinicopathologic Evaluation
Thyroid function test results were interpreted based on the reference ranges applicable at the time of testing. Values within the reference range were considered normal, while those outside the range were considered abnormal. Histopathological evaluation followed a two-step review process. Initial diagnosis was performed by a pathologist with at least five years of experience. All cases were then reviewed and the final pathological diagnosis was confirmed by a second, senior pathologist with over ten years of experience. The final diagnosis of ITNs, serving as the gold standard, was established based on these postoperative pathological findings.
Statistical Analysis
Potential risk factors for invasive PTC were first identified using univariate logistic regression analysis. Variables showing a significant association (P < 0.05) in univariate analysis were then included in a multivariate logistic regression model to identify independent predictors.
A predictive model for invasive PTC was developed based on the results of the multivariate analysis. The discriminative ability of the model was evaluated using receiver operating characteristic (ROC) curve analysis, with the area under the curve (AUC) calculated. The clinical utility of the model was assessed using decision curve analysis (DCA). A nomogram was constructed to visualize the final predictive model.
All statistical analyses were performed using SPSS software (version 25.0, IBM Corp., Armonk, NY, USA) and R software (version 4.4.2, R Foundation for Statistical Computing, Vienna, Austria). A p-value < 0.05 was considered statistically significant.
Results
Clinical and Pathological Data and Statistical Analysis
A total of 494 patients were included in the final analysis. The cohort comprised 366 females (74.1%) and 128 males (25.9%), with a mean age of 46.40 ± 11.96 years. Overall, 262 patients (53.0%) were >45 years old and 232 (47.0%) were ≤45 years old (Table 1).
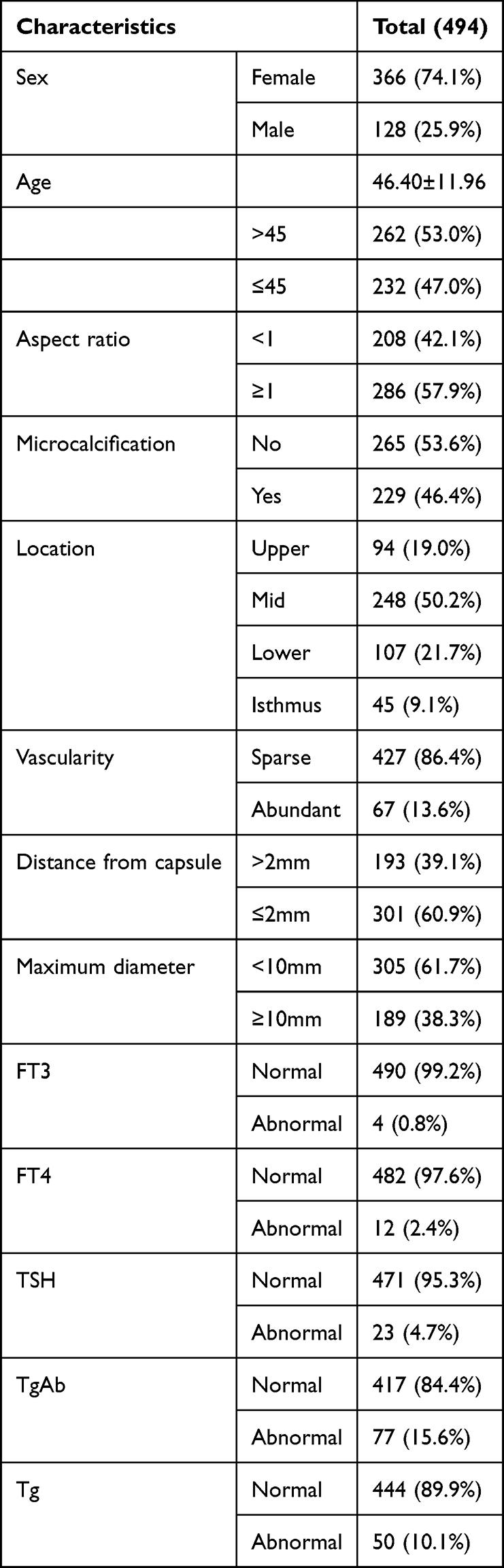 |
Table 1 Clinical and Pathological Characteristics |
Based on postoperative pathology, 353 patients (71.5%) were diagnosed with non-invasive PTC and 141 patients (28.5%) with invasive PTC.
Univariate analysis revealed that male, age ≤45 years, presence of microcalcifications, abundant vascularity, distance from the thyroid capsule ≤2 mm, larger maximum nodule diameter, FT4 levels, and TgAb levels were significantly associated with invasive PTC (all p<0.05). In contrast, nodule location, FT3 levels, TSH levels, and Tg levels showed no significant association (all p>0.05) (Table 2).
 |
Table 2 Results of Univariate and Multivariate Analysis |
Multivariate logistic regression analysis identified the following independent predictive risk factors for invasive PTC: male (OR = 2.91, 95% CI: 1.78–4.76, P < 0.001), age ≤45 years (OR = 1.93, 95% CI: 1.23–3.03, P = 0.04), abundant vascularity (OR = 4.60, 95% CI: 2.42–8.75, P < 0.001), distance from the capsule ≤2 mm (OR = 3.63, 95% CI: 2.15–6.14, P < 0.001), and abnormal TgAb levels (OR = 0.38, 95% CI: 0.18–0.77, P = 0.008) (Table 2).
Development and Validation of the Clinical Prediction Model
The 494 patients were randomly divided into a training set (80%) and a validation set (20%) using a computer-generated random sequence. The clinical prediction model for invasive PTC was developed in the training set based on the independent predictors identified by multivariate logistic regression analysis. The model’s performance was then evaluated in the validation set.
Receiver operating characteristic (ROC) curve analysis demonstrated moderate discriminative ability of the model. The area under the curve (AUC) was 0.776 (95% CI: 0.728–0.825) for the training set and 0.759 (95% CI: 0.643–0.874) for the validation set (Figure 2).
 |
Figure 2 (a) The receiver operating characteristics (ROC) curve and area under the curve (AUC) in the training set; (b) The ROC curve and AUC in the test set. |
Decision curve analysis (DCA) further assessed the clinical utility of the model across a range of threshold probabilities. The DCA curves for both the training and validation sets indicated that the model provides a good net benefit compared to treating all or no patients, supporting its potential clinical usefulness (Figure 3).
 |
Figure 3 (a) Decision curve analysis in the training set; (b) Decision curve analysis in the test set. |
Construction of the Nomogram for Invasive PTC
Multivariate logistic regression analysis confirmed that male, age ≤45 years, abundant vascularity, distance from the thyroid capsule ≤2 mm, and abnormal TgAb levels were independent predictors of invasive PTC in patients with ITNs. Based on these significant predictors, a static nomogram was constructed to provide a visual representation of the predictive model, facilitating the estimation of individual risk (Figure 4).
 |
Figure 4 The nomogram for predicting invasive PTC in ITNs. |
Additionally, to enhance accessibility and ease of use, an interactive online dynamic nomogram has been developed and is publicly accessible at: https://indeterminate-345.shinyapps.io/nomogram/.
Figure 5 illustrates a representative example of using the nomogram for risk prediction in a patient with indeterminate thyroid nodules, alongside the corresponding postoperative pathological findings confirming invasive PTC.
 |
Figure 5 Dynamic nomogram prediction example for an indeterminate thyroid nodule. (a) Ultrasound image showing the thyroid nodule (0.70 cm × 0.62 cm) located≤ 2mm from the capsule. (b) Ultrasound image indicating abundant vascularity in the thyroid nodule. (c) The web-based dynamic nomogram predicts a risk score of 0.838 for invasive PTC in this patient. (d) Pathological findings confirm the nodule as PTC, with cancerous tissue invading vascular walls and surrounding thyroid soft tissue. |
Discussion
The indeterminate cytological diagnosis of thyroid nodules by FNA presents a significant clinical dilemma in therapeutic decision-making. While conservative management may be appropriate for non-invasive papillary thyroid carcinoma (PTC) in indeterminate thyroid nodules (ITNs),27,28 invasive PTC necessitates more extensive surgical resection. This study demonstrates that readily accessible ultrasonographic features combined with clinicopathological characteristics can effectively predict invasive PTC risk in ITNs, enabling clinicians to formulate individualized treatment strategies.
Consistent with extensive evidence,29–33 our study confirms younger age (≤45 years) and male as independent predictors of invasive PTC, demonstrating 1.93-fold and 2.91-fold elevated risks respectively. This aligns with a meta-analysis of 27,741 patients across 41 studies.34 Notably, while females exhibit higher overall PTC incidence, males face disproportionate invasive disease risks.35–37 Potential mechanisms for this sex disparity include: androgenic promotion of tumor invasiveness,37 increased environmental carcinogen exposure (eg, radiation/occupational hazards), higher prevalence of smoking/alcohol consumption, and potential diagnostic delays due to reduced healthcare engagement. For younger patients (≤45 years), accelerated tumor progression may stem from heightened metabolic activity promoting cancer cell proliferation, coupled with less effective immune surveillance against microscopic invasion.
Our analysis further establishes abundant vascularity and capsule proximity (≤2 mm) as novel independent predictors of invasive PTC in indeterminate thyroid nodules. This finding corroborates existing evidence of an inverse relationship between capsular distance and invasion risk.38 Mechanistically, the thyroid capsule serves as a critical anatomical barrier against tumor spread. Nodules within ≤2 mm proximity promote extracapsular extension through both direct breaching of the capsular boundary and compression-induced invasive growth in confined microenvironments.
Concurrently, tumor neovascularization indicated by abundant vascularity promotes invasiveness via dual mechanisms: enhanced oxygen/nutrient delivery accelerating local proliferation, and providing hematogenous dissemination routes to cervical lymph nodes and distant sites (eg, lungs/bones). These vascular features signify biologically aggressive phenotypes.
The observed protective association of abnormal thyroglobulin antibody (TgAb) levels against invasive PTC in ITNs presents a novel finding. While elevated TgAb typically correlates with autoimmune thyroid disorders and has been linked to increased invasion risk in conventional PTC,39,40 our data paradoxically demonstrate reduced aggressiveness in ITN contexts. This may reflect enhanced immune surveillance wherein TgAb activates antitumor responses that eliminate early malignant cells before invasion develops. Additionally, patients with TgAb abnormalities typically undergo more intensive thyroid monitoring, potentially enabling earlier intervention during pre-invasive stages. The differential expression patterns and immunological mechanisms of TgAb in ITNs warrant prospective investigation.
Regarding nodule size, while prior studies associate larger nodules (≥1 cm) and microcalcifications with invasiveness,41–44 our multivariate analysis failed to establish these as independent predictors. The persistent association in univariate analysis suggests these features may serve as secondary indicators meriting consideration in comprehensive risk assessment.
This study has several limitations. First, its single-center retrospective design may introduce selection bias, and the moderate sample size warrants validation in larger prospective cohorts. Second, while internal validation demonstrated model efficacy, external validation across diverse populations is needed to confirm generalizability. Future multi-center studies should address this gap. Third, molecular testing was not systematically incorporated; while this reflects real-world scenarios where such testing may be cost-prohibitive or clinically unnecessary prior to surgery,45 integrating molecular markers could enhance future models. Fourth, we acknowledge that the extended study period (2016–2024) may introduce potential temporal biases, and we recommend that future prospective studies with standardized protocols be conducted to validate our findings. Finally, the ultrasound protocol utilized conventional B-mode and Doppler imaging without advanced techniques like contrast-enhanced or elastographic ultrasound, which may provide additional predictive information.
Conclusion
We established and validated an integrated clinical-ultrasonic model incorporating five key predictors of invasive PTC in indeterminate thyroid nodules: male, age ≤45 years, abundant vascularity, capsule proximity (≤2 mm), and elevated thyroglobulin antibodies. This readily accessible tool provides individualized risk stratification to guide clinical decision-making, and is intended for preoperative risk assessment to assist in determining the extent of surgery, rather than as a substitute for pathological diagnosis. This model has the potential to reduce unnecessary aggressive surgery in low-risk cases while ensuring appropriate management of high-risk patients. The online nomogram implementation facilitates point-of-care application (https://indeterminate-345.shinyapps.io/nomogram/).
Ethics Approval and Consent to Participate
This study design followed the international regulations in accordance with The Declaration of Helsinki. Our research was approved by the Ethical Committee of the Affiliated Hospital of Jiangsu University (SWYXLL20190225-2) and written informed consent was obtained from participants.
Acknowledgments
We are indebted to all the teams and patients who participated in this trail and made it possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Basic Research Special Fund Project of Zhenjiang (No. JC2004028); Medical Education Collaborative Innovation Fund of Jiangsu University (No. JDY2023005); National Science Foundation for Young Scientists of China (No. 82302208); Medical research project of Jiangsu Provincial Health Commission (No. H2023141).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Erik KA, Gerard MD, Justine AB. Management of thyroid nodules. Lancet Diabetes Endocrinol. 2022;10(7):540–12.
2. Alexander EK, Cibas ES. Diagnosis of thyroid nodules. Lancet Diabetes Endocrinol. 2022;10(7):533–539. doi:10.1016/S2213-8587(22)00101-2
3. Mulan LDJ. Expert consensus on the cytopathological diagnosis of thyroid fine needle aspiration (version 2023). Zhonghua Bing Li Xue Za Zhi. 2023;52(5):441–446.
4. David LS, Carty SE, Sippel RS, et al. Performance of a multigene genomic classifier in thyroid nodules with indeterminate cytology. JAMA Oncol. 2019;5(2):204–212.
5. Syed ZA, Baloch ZW, Cochand-Priollet B, Schmitt FC, Vielh P, VanderLaan PA. The 2023 Bethesda system for reporting thyroid cytopathology. J Am Soc Cytopathol. 2023;33(9):1039–1044.
6. Laura B, Mark Z, Maria EC. Thyroid cancer. JAMA. 2024;331(21):1863–1864.
7. Administration, N.H.C.o.t.P.s.R.o.C.M.A.a.H. Guidelines for the diagnosis and treatment of thyroid carcinoma (2022). Chinese J Pract Sur. 2022;42(12):1343–1357+1363.
8. Grani G, Sponziello M, Filetti S, et al. Thyroid nodules: diagnosis and management. Nat Rev Endocrinol. 2024;20(12):715–728. doi:10.1038/s41574-024-01025-4
9. Lisa AO, Noel JE, Stack BC, et al. Radiofrequency ablation and related ultrasound‐guided ablation technologies for treatment of benign and malignant thyroid disease: an international multidisciplinary consensus statement of the American head and neck society endocrine surgery section with the Asia Pacific society of thyroid surgery, associazione medici endocrinologi, British association of endocrine and thyroid surgeons, European thyroid association, italian society of endocrine surgery units, Korean society of …. Head Neck. 2021;44(3):633–660.
10. Giovanni M, Hegedüs L, Bandula S, et al. European thyroid association and cardiovascular and interventional radiological society of Europe 2021 clinical practice guideline for the use of minimally invasive treatments in malignant thyroid lesions. European Thyroid J. 2021;10(3):185–197.
11. Debbie C, Lang BH, McLeod DS, Newbold K, Haymart MR. Thyroid cancer. Lancet. 2023;401(10387):1531–1544.
12. Li G, Li R, Zhong J, et al. A multicenter cohort study of thyroidectomy-related decision regret in patients with low-risk papillary thyroid microcarcinoma. Nat Commun. 2025;16(1):2317. doi:10.1038/s41467-025-57627-7
13. Ashok RS. Implications of prognostic factors and risk groups in the management of differentiated thyroid cancer. Laryngoscope. 2004;114(3):393–402.
14. Bryan RH. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016.
15. Ahn HS, Na DG, Kim JH. Risk stratification of thyroid nodules diagnosed as bethesda category III by ultrasound, size, and cytology. Korean J Radiol. 2024;25(10):924–933. doi:10.3348/kjr.2024.0292
16. Yunong W, Xu T, Cao X, et al. BRAFV600E vs. TIRADS in predicting papillary thyroid cancers in Bethesda system I, III, and V nodules. Cancer Biol Med. 2019;16(1):131–138.
17. Bekir K, Atmaca A, Tarim IA, et al. Risk factors associated with malignancy and with triage to surgery in thyroid nodules classified as Bethesda category III (AUS/FLUS). Eur J Surg Oncol. 2016;42(1):87–93.
18. Ebtihal YA, Alhmayin L, Albasri E, et al. Ultrasonographic predictors of thyroid cancer in Bethesda III and IV thyroid nodules. Front Endocrinol. 2024;15:1326134.
19. Grégoire DA, Gal J, Mandine L, et al. Application of machine learning methods to guide patient management by predicting the risk of malignancy of Bethesda III-V thyroid nodules. European J Endocrinol. 2023;188(3):249–257.
20. Aline Machado Larcher de A, Delfim RL, Vidal AP, et al. Combining the American thyroid association’s ultrasound classification with cytological subcategorization improves the assessment of malignancy risk in indeterminate thyroid nodules. Thyroid. 2021;31(6):922–932.
21. Owen J, Blackabey V, Nisar Ahmad B. 1629 the risk of malignancy in cytologically indeterminate thyroid nodules. Br J Surg. 2021;108(Supplement_6):znab259–577.
22. Lee JY, Baek JH, Ha EJ, et al. 2020 imaging guidelines for thyroid nodules and differentiated thyroid cancer: korean society of thyroid radiology. Korean J Radiol. 2021;22(5):840–860. doi:10.3348/kjr.2020.0578
23. Patel KN, Yip L, Lubitz CC, et al. Executive summary of the American association of endocrine surgeons guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. 2020;271(3):399–410. doi:10.1097/SLA.0000000000003735
24. Tuttle RM, Bryan RH, Nancy DP. Updated American joint committee on cancer/tumor-node-metastasis staging system for differentiated and anaplastic thyroid cancer (Eighth Edition): what changed and why? Thyroid. 2017;27(6):751–756. doi:10.1089/thy.2017.0102
25. Min Kyoung L, Na DG, Joo L, et al. Standardized imaging and reporting for thyroid ultrasound: korean society of thyroid radiology consensus statement and recommendation. Korean J Radiol. 2023;24(1):22.
26. Franklin NT, Middleton WD, Grant EG, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am College Radiol. 2017;14(5):587–595.
27. Roger C, Dana T, Haymart M, et al. Active surveillance versus thyroid surgery for differentiated thyroid cancer: a systematic review. Thyroid. 2022;32(4):351–367.
28. Iwao S, Ito Y, Takeuchi D, et al. Indications and strategy for active surveillance of adult low-risk papillary thyroid microcarcinoma: consensus statements from the japan association of endocrine surgery task force on management for papillary thyroid microcarcinoma. Thyroid. 2021;31(2):183–192.
29. Wei M, Wang R, Zhang W, et al. Landscape of gene mutation in Chinese thyroid cancer patients: construction and validation of lymph node metastasis prediction model based on clinical features and gene mutation marker. Cancer Med. 2023;12(11):12929–12942. doi:10.1002/cam4.5945
30. Feng Y, Min Y, Chen H, et al. Construction and validation of a nomogram for predicting cervical lymph node metastasis in classic papillary thyroid carcinoma. J Endocrinol Invest. 2021;44(10):2203–2211. doi:10.1007/s40618-021-01524-5
31. Huang Y, Huang Z, Cai H, et al. Evaluation of serum B7-H3 expression, ultrasound and clinical characteristics to predict the risk of cervical lymph node metastases in papillary thyroid carcinoma by nomogram. J Clin Lab Anal. 2023;37(1):e24811. doi:10.1002/jcla.24811
32. Chang Q, Zhang J, Wang Y, et al. Nomogram model based on preoperative serum thyroglobulin and clinical characteristics of papillary thyroid carcinoma to predict cervical lymph node metastasis. Front Endocrinol. 2022;13:937049. doi:10.3389/fendo.2022.937049
33. Wang W, Ding Y, Meng C, et al. Patient’s age with papillary thyroid cancer: is it a key factor for cervical lymph node metastasis? Eur J Surg Oncol. 2023;49(7):1147–1153. doi:10.1016/j.ejso.2023.02.011
34. Hafez LG, Elkomos BE, El-Shafaei MAM, et al. The risk of central nodal metastasis based on prognostic factors of the differentiated thyroid carcinoma: a systematic review and meta-analysis study. Eur Arch Otorhinolaryngol. 2023;280(6):2675–2686. doi:10.1007/s00405-023-07863-8
35. Yan HX, Pang P, Wang F-L, et al. Dynamic profile of differentiated thyroid cancer in male and female patients with thyroidectomy during 2000-2013 in China: a retrospective study. Sci Rep. 2017;7(1):15832. doi:10.1038/s41598-017-14963-z
36. Shobab L, Burman KD, Wartofsky L. Sex differences in differentiated thyroid cancer. Thyroid. 2022;32(3):224–235. doi:10.1089/thy.2021.0361
37. Suteau V, Munier M, Briet C, et al. Sex bias in differentiated thyroid cancer. Int J Mol Sci. 2021;22(23):12992. doi:10.3390/ijms222312992
38. Qiu-Cheng W, Cheng W, Wen X, Li JB, Jing H, Nie CL. Shorter distance between the nodule and capsule has greater risk of cervical lymph node metastasis in papillary thyroid carcinoma. Asian Pac J Cancer Prev. 2014;15(2):855–860.
39. Julia EN, Thatipamala P, Hung KS, Chen J, Shi RZ, Orloff LA. Pre-operative antithyroid antibodies in differentiated thyroid cancer. Endocr Pract. 2021;27(11):1114–1118.
40. Yeqian L, Gu Y, Yu M, Deng J. Thyroglobulin antibody (TgAb) positive is an independent risk factor for lymph node metastasis in patients with differentiated thyroid carcinoma. Int J Gene Med. 2023:5979–5988.
41. Xiaojuan Z, Miao Z, Huang X, et al. The risk stratification of papillary thyroid cancer with Bethesda Category III (Atypia of undetermined significance/follicular lesion of undetermined significance) by thyroid fine‐needle aspiration could be assisted by tumor size for precision treatment. Front Endocrinol. 2022;13:822423.
42. Xian NE, Zhang GZ, Jia JZ, Hu HX, Fang QX, Wang XW. Correlation between contrast-enhanced ultrasound quantitative parameters and papillary thyroid carcinoma with extrathyroidal invasion. J Clin Ultrasound Med. 2020;22(11):812–815.
43. Wenhao L, Mao L, Li J, et al. Three-dimensional ultrasound-based radiomics nomogram for the prediction of extrathyroidal extension features in papillary thyroid cancer. Front Oncol. 2023;13:1046951.
44. Juan L, Jia X, Gu Y, et al. Thyroid parenchyma microcalcifications on ultrasound for predicting lymph node metastasis in papillary thyroid carcinoma: a prospective multicenter study in China. Front Oncol. 2021;11:609075.
45. Kepal NP, Yip L, Lubitz CC, et al. The American association of endocrine surgeons guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. 2020;271(3):e21–93.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.