Back to Journals » Journal of Inflammation Research » Volume 19
Integrating Preoperative Preserved Ratio Impaired Spirometry and Inflammatory Markers to Predict Postoperative Complications and Survival in Esophageal Squamous Cell Carcinoma After Neoadjuvant Therapy
Authors Xie Q, Lin Q, Zhan J, Chen C, Zheng B ![]() , Xu G, Zhu Y, Yang Z
, Xu G, Zhu Y, Yang Z
Received 30 September 2025
Accepted for publication 28 November 2025
Published 14 January 2026 Volume 2026:19 568960
DOI https://doi.org/10.2147/JIR.S568960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Junhao Wang
Qichang Xie,1– 3,* Qiong Lin,4,* Junpeng Zhan,1– 3,* Chun Chen,1– 3 Bin Zheng,1– 3 Guobing Xu,1– 3 Yong Zhu,1– 3 Zhang Yang1– 3
1Department of Thoracic Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 2Key Laboratory of Cardio-Thoracic Surgery (Fujian Medical University), Fuzhou, Fujian, People’s Republic of China; 3Clinical Research Center for Thoracic Tumors of Fujian Province, Fuzhou, Fujian, People’s Republic of China; 4Department of Pulmonary and Critical Care Medicine, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Zhu; Zhang Yang, Department of Thoracic Surgery, Fujian Medical University Union Hospital, No. 29 Xinquan Road, Fuzhou, 350000, People’s Republic of China, Email [email protected]; [email protected]
Background: Severe postoperative complications (SPCs) adversely affect outcomes in esophageal squamous cell carcinoma (ESCC) following neoadjuvant therapy. The prognostic significance of preserved ratio impaired spirometry (PRISm) and inflammation-based biomarkers such as the systemic inflammation response index (SIRI) and lymphocyte-to-monocyte ratio (LMR) remains unclear.
Methods: We retrospectively analyzed 224 ESCC patients who underwent esophagectomy after neoadjuvant therapy. PRISm was defined by FEV1 < 80% predicted and FEV1/FVC ≥ 0.7. Preoperative inflammatory indices, including SIRI, NLR, and LMR, were collected. The primary endpoint was the incidence of SPCs (Clavien–Dindo grade ≥ III); secondary endpoints included overall survival (OS) and recurrence-free survival (RFS). Multivariate regression was used to identify independent predictors. Nomograms were developed and validated using ROC curves, calibration plots, and decision curve analysis (DCA).
Results: PRISm and decreased SIRI independently predicted higher SPC risk (p < 0.05). The SPC nomogram demonstrated good discrimination (AUC = 0.726). PRISm was also associated with significantly worse OS and RFS (p < 0.001). Elevated SIRI and low LMR correlated with poor long-term outcomes. OS and RFS nomograms showed good calibration and outperformed TNM staging in clinical utility.
Conclusion: PRISm and systemic inflammatory markers are independent predictors of complications and prognosis in ESCC after neoadjuvant therapy. The proposed nomograms offer practical tools for individualized preoperative risk stratification and may support tailored perioperative management, especially in older or high-risk patients.
Keywords: esophageal squamous cell carcinoma, ESCC, preserved ratio impaired spirometry (PRISm), postoperative complications, nomogram
Introduction
Esophageal cancer remains a major global health burden, ranking as the 11th most common malignancy and the 7th leading cause of cancer-related death worldwide. Esophageal squamous cell carcinoma (ESCC) is the predominant histological subtype in East Asia, particularly in China.1,2 For patients with locally advanced ESCC, the standard of care includes neoadjuvant therapy—such as chemotherapy (nCT), chemoradiotherapy (nCRT), or chemoimmunotherapy (nCIT)—followed by curative esophagectomy.
Despite advances in surgical techniques and perioperative management, the incidence of severe postoperative complications (SPCs), especially those classified as Clavien–Dindo grade III or higher, remains substantial. These complications are associated with longer hospital stays, increased healthcare costs, and worse long-term survival.3,4 Therefore, identifying reliable preoperative predictors of SPCs and oncologic outcomes is essential for guiding perioperative management and individualized treatment strategies.
Preserved ratio impaired spirometry (PRISm), defined as a forced expiratory volume in one second (FEV1) of less than 80% predicted with a preserved FEV1/FVC ratio (≥ 0.7), is a distinct spirometric pattern not classified as obstructive or restrictive. Although often underrecognized, PRISm affects 7–13% of the general population and has been linked to systemic inflammation, cardiometabolic comorbidities, and increased mortality.5,6 However, its prognostic value in thoracic malignancies, including ESCC, remains poorly characterized.
At the same time, systemic inflammation plays a pivotal role in influencing both surgical recovery and cancer progression. Several inflammation-based hematologic indices—such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI)—have emerged as cost-effective markers of immune imbalance and tumor-promoting inflammation. These indices have demonstrated prognostic utility across various solid tumors, including ESCC.7–9
Despite their individual significance, limited data exist regarding the combined predictive value of preoperative PRISm and systemic inflammatory markers in patients with ESCC undergoing neoadjuvant therapy and surgery. To our knowledge, no integrated prognostic model has yet incorporated both respiratory function and immunoinflammatory status to guide comprehensive risk stratification in this population.
This study aimed to evaluate the impact of preoperative PRISm and inflammatory biomarkers on both short-term outcomes (SPC incidence) and long-term outcomes (overall survival [OS] and recurrence-free survival [RFS]) in ESCC patients undergoing neoadjuvant therapy followed by curative esophagectomy. We also sought to develop and validate predictive nomograms to guide personalized clinical decision-making and improve perioperative risk stratification.
Method
Patient Selection
This retrospective study included patients with histologically confirmed esophageal squamous cell carcinoma (ESCC) who underwent neoadjuvant therapy followed by curative-intent esophagectomy at Fujian Medical University Union Hospital between January 2016 and December 2021. Inclusion criteria: (1) Age between 18 and 75 years; (2) Histologically confirmed ESCC; (3) Clinical stage II–IVA according to the American Joint Committee on Cancer (AJCC) 8th edition TNM staging system; (4) Eastern Cooperative Oncology Group (ECOG) performance status 0–2. Exclusion criteria: (1) Concurrent other malignancies or anticancer treatments for other cancers; (2) Mixed histological tumor types on postoperative pathology; (3) The presence of other known respiratory diseases that significantly affect lung function was an exclusion criterion. These encompassed conditions manifested primarily as isolated small airway dysfunction (eg, early-stage bronchiolitis obliterans), interstitial lung disease, and severe emphysema; (4) Preoperative spirometry showing FEV1/FVC < 0.7. A total of 224 patients met all eligibility criteria and were included in the final analysis. The study was approved by the Ethics Committee of Fujian Medical University Union Hospital (Approval No. 2025KY081) and conducted in accordance with the Declaration of Helsinki and its amendments. Due to the retrospective nature of the study, informed consent was waived.
Preoperative Examination
Pulmonary function tests were performed within 7 days prior to surgery for all patients. The following parameters were recorded: forced expiratory volume in one second (FEV1; actual and predicted), forced vital capacity (FVC; actual and predicted), FEV1/FVC ratio, maximal expiratory flow at 25%, 50%, and 75% of FVC (FEF25, FEF50, FEF75), and maximal voluntary ventilation (MMV). Hematological analyses were completed within 1 week preoperatively for all patients, including retrospective assessment of neutrophil (NEU), monocyte (MO), lymphocyte (LY), and platelet (PLT) counts. Inflammatory indices were calculated as follows: NLR (NEU/LY), PLR (PLT/LY), LMR (LY/MO), SII, [(PLT × NEU)/LY], and SIRI, [(NEU × MO)/LY].
Treatment Plan
Patients received one of three neoadjuvant regimens: chemotherapy (nCT), chemoimmunotherapy (nCIT), or chemoradiotherapy (nCRT). The nCT group received 2–4 cycles of paclitaxel (or nab-paclitaxel) plus a platinum-based agent every three weeks. In the nCIT group, the same chemotherapy regimen was combined with intravenous PD-1 inhibitors (pembrolizumab, camrelizumab, or sintilimab, 200 mg). Patients in the nCRT group received the same chemotherapy with concurrent radiotherapy, totaling 50.4 Gy in 23 fractions. Curative esophagectomy was performed 4–6 weeks after therapy completion, using minimally invasive (laparoscopic/thoracoscopic) or robotic-assisted techniques (da Vinci), with either McKeown or Ivor Lewis approaches. A standardized two-field lymphadenectomy was performed in all cases, with intraoperative transition to three-field dissection if metastasis of the right recurrent laryngeal nerve nodes was confirmed by frozen section.
Follow-Up
Short-term outcomes were defined as SPC according to Clavien–Dindo grade ≥III. For long-term outcomes, follow-up assessments were conducted every 3 months during the first two years, every 6 months between years 3 to 5, and annually thereafter beyond 5 years. Follow-up investigations included hematological tests, contrast-enhanced CT of the neck/chest/abdomen, color Doppler ultrasound of the neck and abdomen, upper gastrointestinal endoscopy, and PET/CT when necessary. OS and RFS were documented based on follow-up results.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range) and compared using the Student’s t-test or Mann–Whitney U-test, as appropriate. Categorical variables were presented as frequencies and percentages and analyzed using the chi-square test or Fisher’s exact test. Univariate and multivariate logistic regression analyses were used to identify independent predictors of severe postoperative complications (SPCs). Survival outcomes, including overall survival (OS) and recurrence-free survival (RFS), were assessed using Kaplan–Meier curves with Log rank tests and Cox proportional hazards models. Variables with statistical significance in multivariate analysis were incorporated into nomograms constructed using the “rms” package in R (version 4.2.1). Model performance was evaluated by area under the ROC curve (AUC), calibration plots, and decision curve analysis (DCA). A two-sided p-value < 0.05 was considered statistically significant.10,11
Result
Patient Characteristics
A total of 224 patients with histologically confirmed ESCC who underwent neoadjuvant therapy followed by radical esophagectomy were included in the analysis (Figure 1A). Of these, 58 patients (25.9%) were classified as having PRISm, while 166 (74.1%) had normal pulmonary function. Baseline clinical characteristics are summarized in Table 1. The cohort comprised 169 men (75.4%) and 55 women (24.6%), with a median age of 62 years (range: 38–75) and a mean body mass index (BMI) of 22.01 ± 2.93 kg/m2. Tumors were most frequently located in the middle thoracic esophagus (61.6%), followed by the lower (28.1%) and upper (10.3%) segments. Neoadjuvant regimens included nCT in 148 patients (66.1%), nCRT in 45 (20.1%), and nCIT in 31 (13.8%). Baseline demographics, tumor location, clinical stage, and treatment regimens did not differ significantly between the PRISm and normal groups (all P > 0.05). However, the PRISm group showed significantly lower mean FEV1 (2.24 ± 0.53 vs 2.72 ± 0.60 L), FVC (2.73 ± 0.64 vs 3.28 ± 0.70 L), FEF50 (2.99 ± 1.21 vs 3.65 ± 1.22 L/s), and FEF75 (0.98 ± 0.58 vs 1.20 ± 0.51 L/s) (all P < 0.01), while predicted FEV1 and FVC percentages were similar. Inflammatory markers (NLR, PLR, LMR, SII, SIRI) did not differ significantly between groups. Notably, the incidence of severe postoperative complications was significantly higher in the PRISm group (31.0% vs 7.8%, P < 0.001).
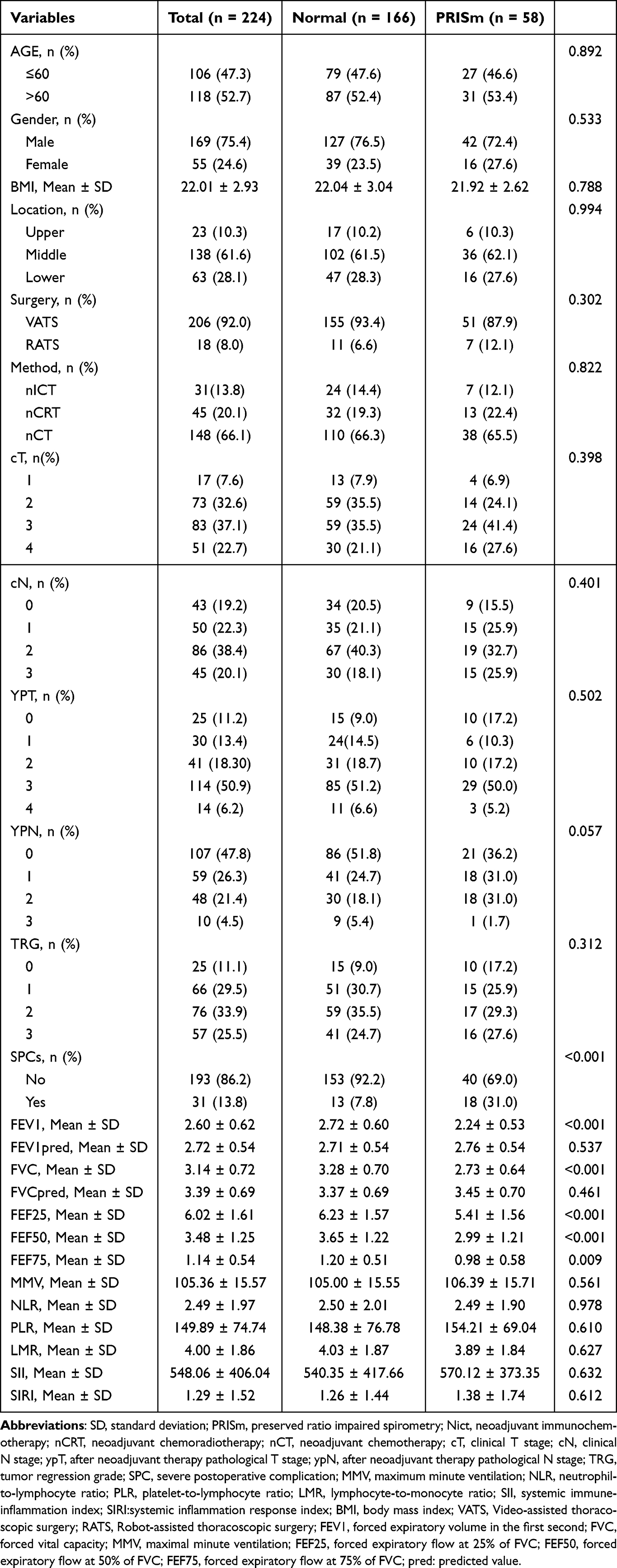 |
Table 1 Baseline Characteristics (Stratification by PRISm) |
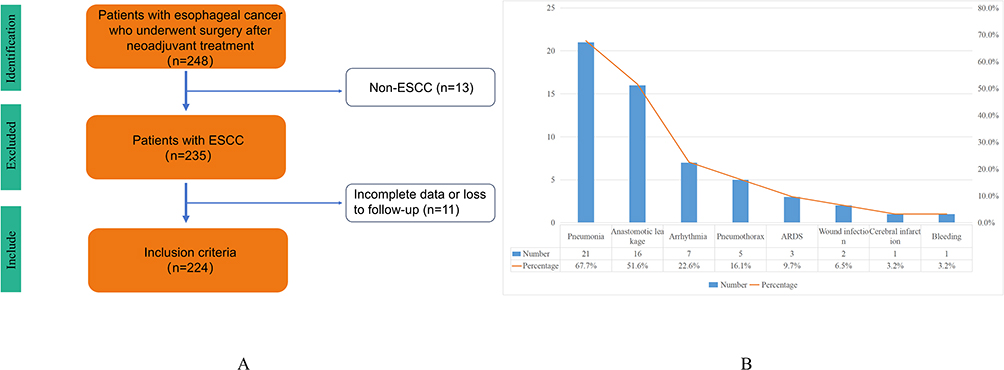 |
Figure 1 Analysis overview (A). Summary of severe postoperative complications (B). Abbreviations: ESCC, esophageal squamous cell carcinoma; ARDS, acute respiratory distress syndrome. |
Hematological Indices: ROC Curve Analysis
ROC curve analysis was conducted to assess the prognostic value of preoperative hematological inflammatory markers for overall survival (OS). The AUC values were as follows: NLR, 0.512 (95% CI: 0.431–0.592); PLR, 0.568 (95% CI: 0.488–0.647); LMR, 0.524 (95% CI: 0.444–0.604); SII, 0.519 (95% CI: 0.437–0.600); and SIRI, 0.472 (95% CI: 0.392–0.553) (Figure 1). All five markers showed limited discriminative ability for OS, with AUCs below 0.6, indicating weak prognostic performance when used as continuous variables. Therefore, optimal cut-off values were determined using the Youden index: NLR, 3.302; PLR, 141.373; LMR, 2.278; SII, 477.111; and SIRI, 0.751. Patients were subsequently categorized into high and low groups for each marker: NLR (n = 43 high, n = 181 low), PLR (n = 94 high, n = 130 low), LMR (n = 183 high, n = 41 low), SII (n = 98 high, n = 126 low), and SIRI (n = 51 high, n = 173 low). These dichotomized variables were used in univariate and multivariate analyses to evaluate associations with SPCs, OS, and RFS.
PRISm Predicts the Occurrence of SPCs
In this cohort, the overall incidence of SPC was 13.84% (31/224). Patients with preoperative PRISm had a significantly higher SPC rate compared to those with normal spirometry (31.0% vs 7.8%, P < 0.001). The most common SPCs included pneumonia (67.7%), anastomotic leakage (51.6%), atrial fibrillation, and surgical site infections (Figure 1B). Univariate logistic regression identified PRISm (OR: 5.296; 95% CI: 2.395–11.713; P < 0.001) and elevated SIRI (OR: 0.324; 95% CI: 0.094–1.112; P = 0.073) as potential predictors. In multivariate analysis, both PRISm (OR: 6.158; 95% CI: 2.715–13.966; P < 0.001) and SIRI (OR: 0.237; 95% CI: 0.066–0.856; P = 0.028) remained independent predictors of SPCs (Table 2). Other pulmonary function variables (eg, FEF25, FEF50, FEF75, MMV) and neoadjuvant regimens (nCT, nCIT, nCRT) were not significantly associated with SPC incidence (Table 2). A nomogram incorporating PRISm and SIRI was developed and showed good discriminative performance (AUC = 0.726; 95% CI: 0.633–0.818; Figure 2A and B). Calibration plots demonstrated close agreement between predicted and observed SPC probabilities (Hosmer–Lemeshow test: χ2 = 0.022, df = 1, P = 0.882; Figure 2C). Decision curve analysis (DCA) confirmed the model’s clinical utility, with greater net benefit than “treat-all” or “treat-none” strategies across a 10%–50% risk threshold range (Figure 2D).
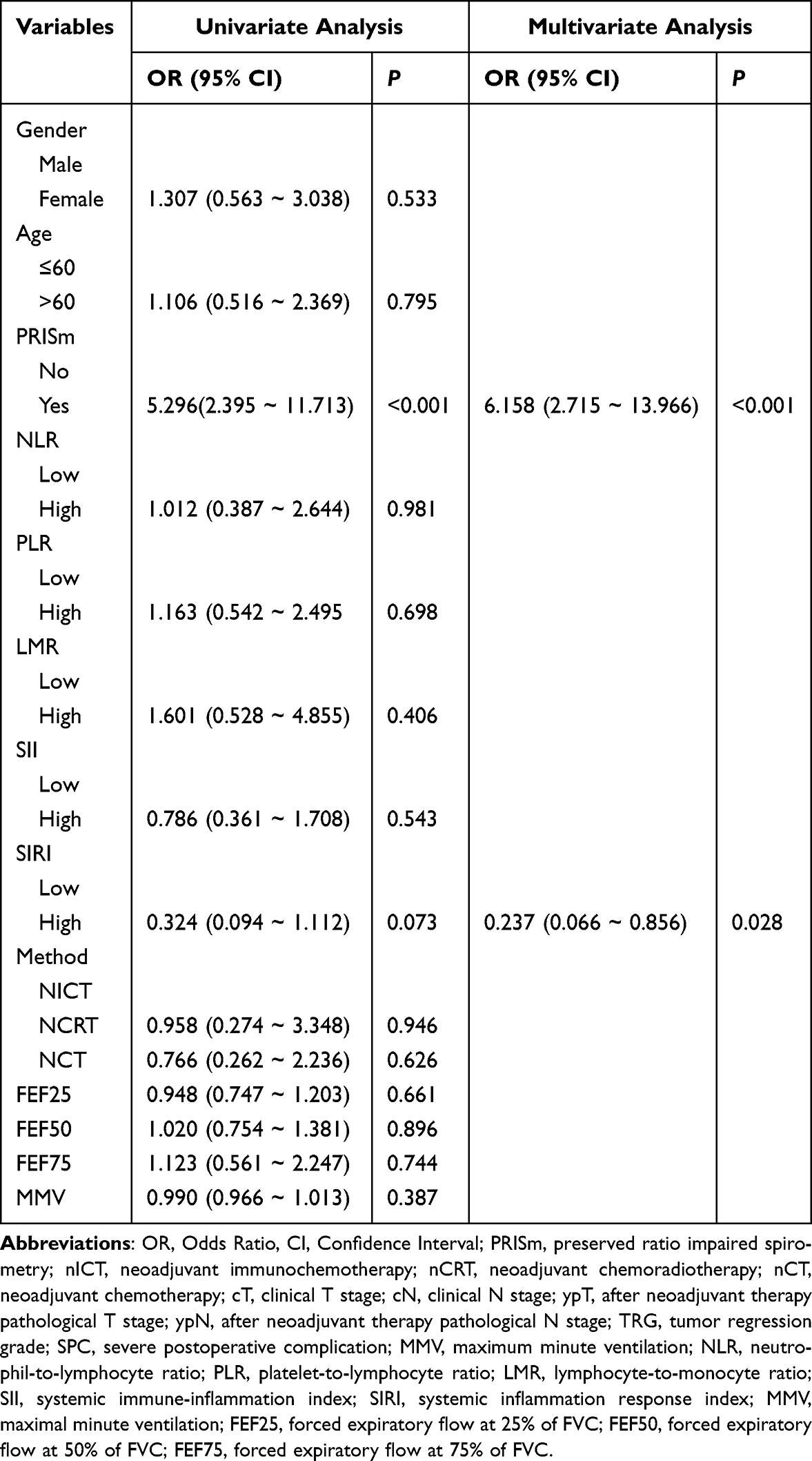 |
Table 2 Logistic Regression for Predicting SPCs |
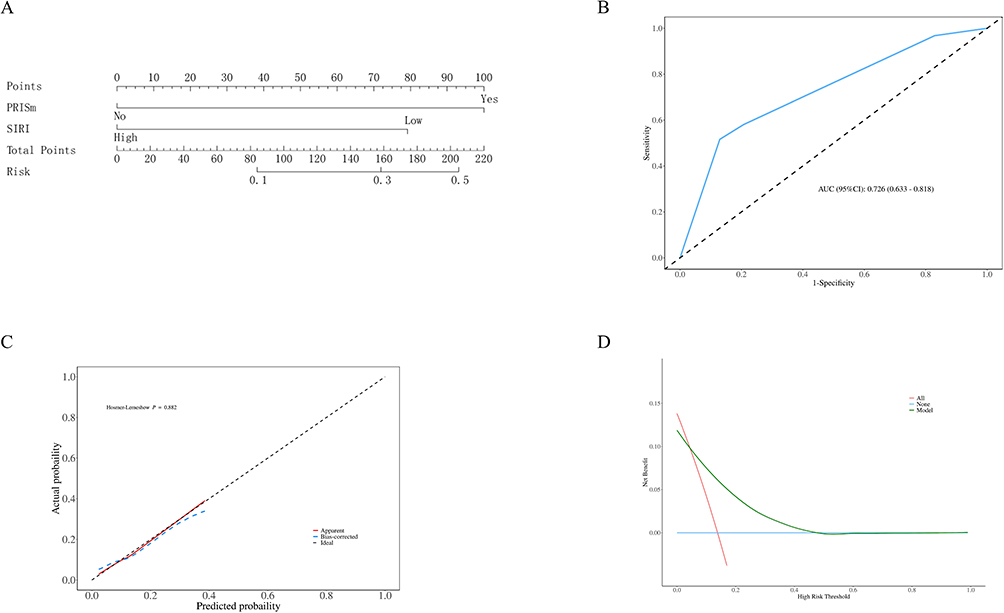 |
Figure 2 Nomogram for predicting SPCs (A). ROC curve of nomogram-SPCs (B). The model’s calibration curve demonstrates well-fitted results (C). DCA curve of nomogram-SPCs (D). Abbreviations: PRISm, preoperative preserved ratio impaired spirometry; SIRI, systemic inflammation response index. |
The Impact of PRISm on Long-Term Survival
Kaplan–Meier survival analysis revealed a significant difference in long-term outcomes between the PRISm and normal spirometry groups. Patients in the normal group had a markedly higher 3-year overall survival (OS) rate of 78.0%, with the median OS not reached during follow-up. In contrast, the PRISm group exhibited a 3-year OS rate of 53.1%, with a median survival time of 44 months (95% CI: 31.0–65.0) (p < 0.001, Figure 3A). Similarly, recurrence-free survival (RFS) outcomes were significantly worse in the PRISm group. The normal group achieved a 3-year RFS rate of 81.1% with no median RFS reached, whereas the PRISm group had a 3-year RFS rate of 50.1% and a median RFS of 39 months (95% CI: 23.0–59.0) (p < 0.001). These disparities persisted over longer follow-up, with 5-year OS and RFS rates of 78.8% and 63.8%, respectively, in the normal group, compared to 31.3% and 28.6% in the PRISm group (Figure 3B).
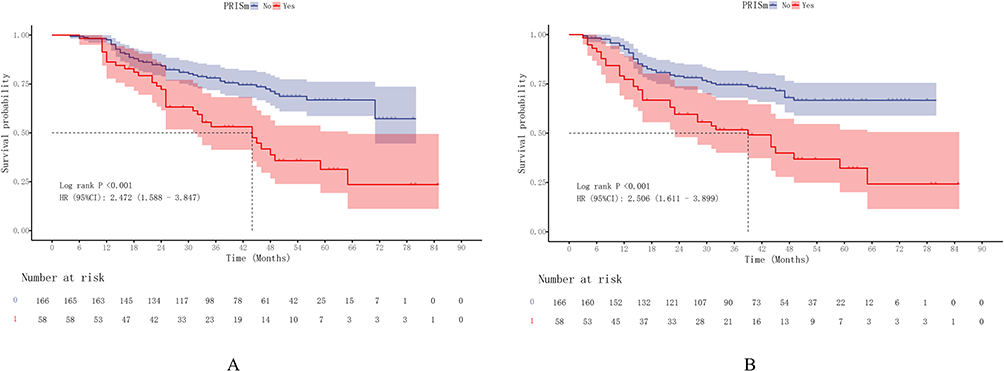 |
Figure 3 Survival curves of patients after neoadjuvant therapy. This figure demonstrates the relationship between PRISm and OS (A)/RFS (B). |
Univariate Cox regression identified several significant prognostic factors for OS, including PRISm (HR: 2.472; 95% CI: 1.588–3.847; P < 0.001), low LMR (HR: 0.578; 95% CI: 0.353–0.944; P = 0.028), advanced pathological nodal stage (ypN1–3), partial or no pathological response (HR: 2.074; 95% CI: 1.270–3.387; P = 0.004), and reduced FEF50 (HR: 0.817; 95% CI: 0.679–0.983; P = 0.032) (Table 3). For RFS significant univariate predictors included PRISm (HR: 2.444; P < 0.001), high NLR (HR: 1.625; P = 0.049), low LMR (HR: 0.535; P = 0.009), SPC occurrence (HR: 1.752; P = 0.039), pathological nodal stage, nCRT (HR: 3.124; P = 0.022), and decreased FEF50 (HR: 0.803; P = 0.017). In multivariate analysis, PRISm (HR: 1.975; P = 0.006), ypN stage (ypN1–3, all P < 0.01), nCRT (HR: 3.094; P = 0.034), and FEF50 (HR: 0.769; P = 0.011) remained independent predictors of RFS. SPC and NLR lost significance after adjustment (Supplementary Table 1). These findings underscore the prognostic impact of impaired lung function, inflammation, and nodal burden on both OS and RFS. Interestingly, nCRT was associated with recurrence but not OS, suggesting treatment-related recurrence risk may be influenced by host factors and tumor biology.
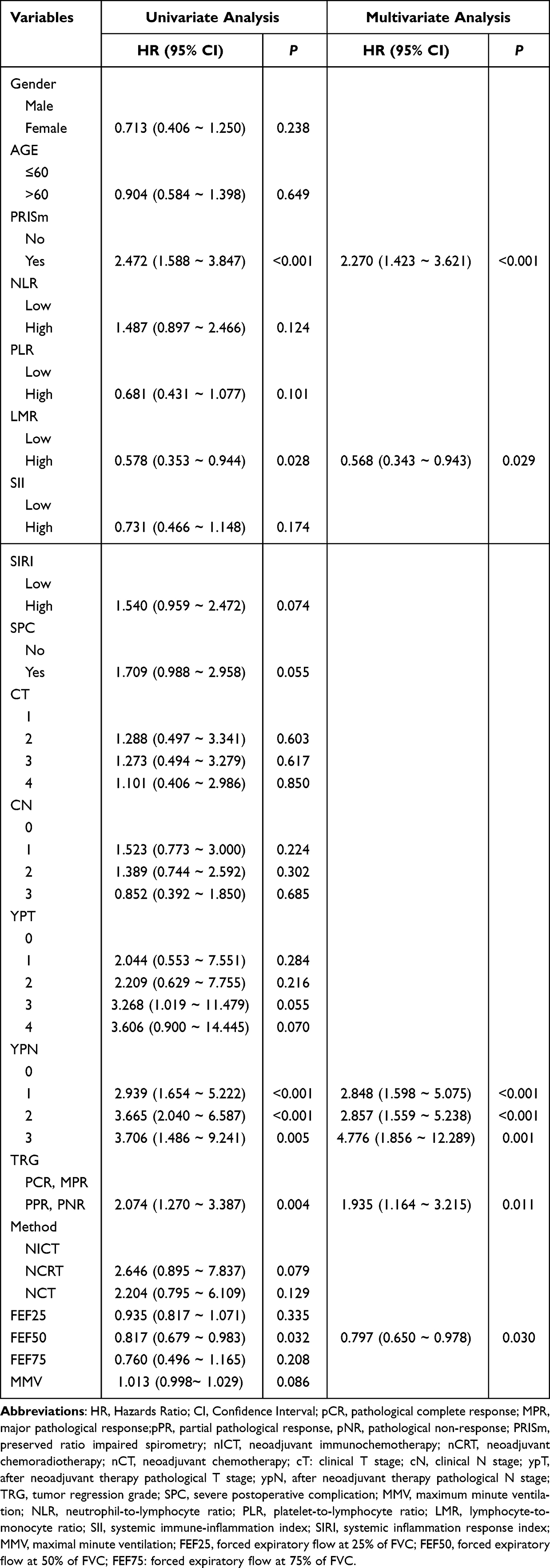 |
Table 3 Univariate and Multivariate Cox Regression Analysis for Predicting OS |
Nomograms for OS and RFS were constructed using coefficients from multivariate Cox models. For OS, a score below 80 corresponded to >90% 3-year survival, and a score under 40 predicted >90% 5-year survival (Figure 4A). The nomogram showed strong performance, with AUCs of 0.742 and 0.833 for 3- and 5-year OS, respectively (Figures 4B), and excellent calibration (Figures 4D and E). Time-dependent AUCs confirmed superiority over TNM staging (Figure 4C), and DCA showed greater net benefit across 20%–80% risk thresholds (Figures 4F and G).
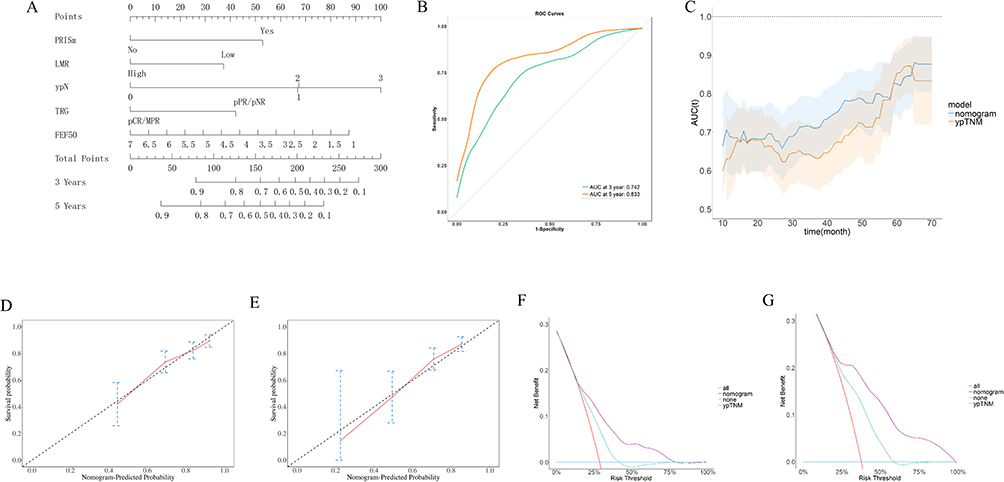 |
Figure 4 Nomogram for predicting OS (A). This figure demonstrates the model’s good performance in predicting 3-year and 5-year OS (B). The time-dependent AUCs demonstrate superior overall predictive performance compared to TNM staging (C). The calibration curves (D and E) and DCA curves (F and G) both indicate favorable model performance. |
The RFS nomogram similarly demonstrated strong discrimination (3-year AUC: 0.700; 5-year AUC: 0.802) and calibration (Supplementary Figure 1A and B). It outperformed TNM staging in time-dependent analysis and provided superior clinical utility in DCA (Supplementary Figure 1C–G). These models offer practical tools for individualized survival prediction and treatment planning in neoadjuvant-treated ESCC.
Discussion
To date, few studies have comprehensively evaluated the clinical significance of preserved ratio impaired spirometry (PRISm) in patients with esophageal squamous cell carcinoma (ESCC), particularly those undergoing neoadjuvant therapy followed by surgery.
In this study, we demonstrate for the first time that preoperative PRISm is significantly associated with a higher incidence of severe postoperative complications (SPCs) and poorer long-term outcomes—including both overall survival (OS) and recurrence-free survival (RFS)—in patients with ESCC treated with curative surgery following neoadjuvant therapy. Mechanistically, PRISm is characterized by small airway dysfunction, which may predispose patients to hypoventilation, impaired mucociliary clearance, and reduced oxygen diffusion capacity. These respiratory limitations likely contribute to postoperative pulmonary complications such as pneumonia, anastomotic leakage, and atrial fibrillation. Multivariable logistic regression identified PRISm (OR: 6.158) and decreased systemic inflammation response index (SIRI) (OR: 0.237) as independent predictors of SPCs. These findings align with the COPDGene study, which reported that PRISm patients commonly show reduced resting oxygen saturation and heightened systemic inflammation.12 The hypoxic state characteristic of PRISm may induce endothelial dysfunction and promote the release of inflammatory cytokines such as IL-6 and TNF-α, thereby exacerbating the risk of infectious and ischemic complications.13 In the specific population of esophageal cancer patients who have undergone neoadjuvant therapy, preoperative SIRI may not indicate a healthy immune state, but rather reflect a certain degree of treatment-related immunosuppression or immune paralysis.14–16 While chemotherapy and/or radiotherapy can kill tumor cells, they may also exert profound effects on the immune system—particularly causing significant and sustained lymphocyte depletion. In such cases, an excessively suppressed immune system may fail to mount an effective and appropriate inflammatory response to surgical trauma, yet this moderate inflammatory response is crucial for initiating tissue repair and defending against postoperative infections.
In survival analyses, PRISm was independently associated with worse OS and RFS, consistent with prior studies in other malignancies linking PRISm to both all-cause and cancer-specific mortality.17,18 Potential mechanisms include reduced cardiopulmonary reserve, comorbid metabolic and cardiovascular conditions, and a persistent pro-inflammatory state. Additionally, impaired ventilatory function may limit patients’ tolerance to neoadjuvant therapy and hinder postoperative recovery, ultimately impacting oncologic outcomes. These findings highlight the importance of routine pulmonary function testing, particularly for older or high-risk surgical candidates. A decrease in FEF50 usually indicates early lesions or dysfunction of peripheral small airways.19,20 In patients undergoing neoadjuvant therapy and radical esophageal cancer surgery, the fragile small airways may be more susceptible to treatment-related toxicity or surgical trauma. This could potentially affect the susceptibility to postoperative pulmonary complications and also indirectly reflects a systemic fragile state, ultimately impacting patients’ long-term survival outcomes.
Our study also validates the prognostic significance of systemic inflammatory biomarkers. Decreased SIRI was independently associated with SPCs, while low lymphocyte-to-monocyte ratio (LMR) predicted worse OS. These indices reflect the dynamic interplay between tumor-promoting inflammation and host immune surveillance. In ESCC, neoadjuvant therapy may intensify systemic inflammation, which in turn contributes to impaired healing, recurrence, and metastasis. Prior studies in gastric and pancreatic cancers have reported similar associations, reinforcing the translational relevance of these markers.21–24
Notably, pathological nodal status (ypN1–3) and suboptimal tumor regression (TRG) also significantly predicted poorer survival outcomes, in line with previous evidence linking nodal downstaging and histopathological response to improved outcomes after neoadjuvant treatment.25–29 Interestingly, patients who received neoadjuvant chemoradiotherapy (nCRT) had shorter RFS compared to those treated with chemotherapy or chemoimmunotherapy, suggesting that treatment modality may influence recurrence dynamics and should be tailored based on individual risk profiles.
Based on PRISm, this study provides several robust predictive tools. On one hand, the nomogram established by combining PRISm status and SIRI levels for SPC helps clinicians identify high-risk populations, thereby formulating individualized surgical approaches and perioperative management models to improve patient survival. On the other hand, the nomogram for OS based on PRISm, pulmonary function, LMR levels, and postoperative pathological findings not only reflects the oncological characteristics of patients but also their inflammatory status and potential cardiopulmonary dysfunction. This enables a more comprehensive capture of the core factors contributing to all-cause mortality that affect OS. The models were internally validated using the Bootstrap method. Their favorable C-index and calibration curves indicate reliable predictive accuracy and a low risk of overfitting. Particularly importantly, decision curve analysis (DCA) confirmed the practical utility of the models from the perspective of clinical decision-making. These tools are expected to serve as powerful decision-support aids for clinicians.
This study has several limitations. First, its retrospective, single-center design may introduce selection and information bias. Second, heterogeneity in neoadjuvant regimens and treatment cycles could confound outcome comparisons. Third, spirometric classification of PRISm lacks universally accepted thresholds and cut-off values for all inflammatory markers were determined based on the overall dataset of this study through ROC curve analysis and the method of maximizing the Youden index, potentially limiting external reproducibility. Finally, the sample size may reduce statistical power, particularly in subgroup analyses. Prospective multicenter validation is essential to confirm the predictive value of PRISm and systemic inflammatory markers across diverse populations. Further studies should also explore the biological mechanisms underlying PRISm-associated inflammation and its role in tumor progression and treatment resistance. The nomogram proposed in this study demonstrates good performance; however, its practical application still requires further validation in external centers.
Conclusion
Preoperative PRISm independently predicted severe postoperative complications and worse survival in ESCC patients undergoing neoadjuvant therapy and surgery. Systemic inflammatory markers, especially SIRI and LMR, also held prognostic value. We developed nomograms integrating PRISm, inflammation, and pathology, which outperformed TNM staging in predicting complications and survival. These tools may support personalized risk stratification and guide perioperative decision-making. Further prospective validation is warranted. We believe these tools are expected to become powerful aids for clinicians to assess the perioperative risks and prognosis of ESCC patients who undergo neoadjuvant therapy and surgery, and hold significant potential for clinical translation.
Data Sharing Statement
In this study, data such as patients’ pulmonary function data and blood test results involve patients’ privacy, so the data of this study will not be made public.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Fujian Medical University Union Hospital (Approval No. 2025KY081) and conducted in accordance with the Declaration of Helsinki and its amendments. Due to the retrospective nature of the study, informed consent was waived.
Acknowledgments
We thank all patients, their families and all investigators involved in the present study.
Author Contributions
Zhang Yang and Yong Zhu: Conceptualization, Funding acquisition, Supervision, Writing – review and editing.
Qichang Xie: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Software.
Qiong Lin: Software, Resources, Validation, Writing – original draft.
Junpeng Zhan: Visualization, Validation, Formal analysis, Writing – original draft.
Chun Chen; Bin Zheng; Guobing Xu: Data curation, Formal analysis, Methodology, Validation, Writing – original draft.
Qichang Xie, Qiong Lin, and Junpeng Zhan are joint first authors of this work. All authors have agreed on the final version submitted for publication; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82203307); Talent Fund Project of Fujian Medical University Union Hospital (2021XH029) and Joint Fund for the innovation of science and Technology, Fujian province (Grant number: 2023Y9204).
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Zhu H, Ma X, Ye T, et al. Esophageal cancer in China: practice and research in the new era. Nt. J. Cancer. 2023;152(9):1741–1751. doi:10.1002/ijc.34301
3. Lerut T, Moons J, Coosemans W, et al. Postoperative complications after transthoracic esophagectomy for cancer of the esophagus and gastroesophageal junction are correlated with early cancer recurrence: role of systematic grading of complications using the modified Clavien classification. Ann Surg. 2009;250(5):798–807. doi:10.1097/SLA.0b013e3181bdd5a8
4. Kauppila JH, Johar A, Lagergren P. Postoperative complications and health-related quality of life 10 years after esophageal cancer surgery. Ann Surg. 2020;271(2):311–316. doi:10.1097/SLA.0000000000002972
5. He D, Yan M, Zhou Y, et al. Preserved ratio impaired spirometry and COPD accelerate frailty progression: evidence from a prospective cohort study. Chest. 2024;165(3):573–582. doi:10.1016/j.chest.2023.07.020
6. Cadham CJ, Oh H, Han MK, et al. The prevalence and mortality risks of PRISm and COPD in the United States from NHANES 2007-2012. Respir Res. 2024;25(1):208. doi:10.1186/s12931-024-02841-y
7. Zhang X, Gari A, Li M, et al. Combining serum inflammation indexes at baseline and post treatment could predict pathological efficacy to anti‑PD‑1 combined with neoadjuvant chemotherapy in esophageal squamous cell carcinoma. J Transl Med. 2022;20(1):61. doi:10.1186/s12967-022-03252-7
8. Xu X, Jing J. Inflammation-related parameter serve as prognostic biomarker in esophageal squamous cell carcinoma. Front Oncol. 2022;12:900305. doi:10.3389/fonc.2022.900305
9. Kim JY, Yun JK, Kim YH, et al. Prognostic impact of inflammation-based factors in patients with esophageal squamous cell carcinoma achieving pathological complete response after neoadjuvant chemoradiotherapy followed by surgery. Ann Surg Oncol. 2024;31(10):6662–6672. doi:10.1245/s10434-024-15678-y
10. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J clin oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
11. Xu S, Liu Y, Ma H, et al. A novel signature integrated of immunoglobulin, glycosylation and anti-viral genes to predict prognosis for breast cancer. Front Genetics. 2022;13:834731. doi:10.3389/fgene.2022.834731
12. Wan ES, Hokanson JE, Murphy JR, et al. Clinical and radiographic predictors of GOLD-unclassified smokers in the COPDGene study. Am J Respir Crit Care Med. 2011;184(1):57–63. doi:10.1164/rccm.201101-0021OC
13. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
14. Leliefeld PH, Wessels CM, Leenen LP, Koenderman L, Pillay J. The role of neutrophils in immune dysfunction during severe inflammation. Critical Care. 2016;20:73. doi:10.1186/s13054-016-1250-4
15. Sriskandan S, Altmann DM. The immunology of sepsis. J Pathol. 2008;214(2):211–223. doi:10.1002/path.2274
16. Leliefeld PH, Koenderman L, Pillay J. How neutrophils shape adaptive immune responses. Front Immunol. 2015;6:471. doi:10.3389/fimmu.2015.00471
17. Im Y, Kim T, Hwang JH, et al. Association of Preserved-Ratio Impaired Spirometry (PRISm) with all-cause mortality: a longitudinal cohort study. Ann Am Thoracic Soc. 2025;22(4):486–493. doi:10.1513/AnnalsATS.202403-250OC
18. Wan ES, Balte P, Schwartz JE, et al. Association between preserved ratio impaired spirometry and clinical outcomes in us adults. JAMA. 2021;326(22):2287–2298. doi:10.1001/jama.2021.20939
19. Wang Z, Lin J, Liang L, et al. Combining small airway parameters with conventional parameters obtained during spirometry to diagnose airflow obstruction: a cross-sectional study. Respirology. 2024;29(7):605–613. doi:10.1111/resp.14725
20. Ren WY, Li L, Zhao RY, Zhu L. Age-associated changes in pulmonary function: a comparison of pulmonary function parameters in healthy young adults and the elderly living in Shanghai. Chinese Med J. 2012;125(17):3064–3068.
21. Hu G, Liu G, Ma JY, Hu RJ. Lymphocyte-to-monocyte ratio in esophageal squamous cell carcinoma prognosis. Int J clin Chem. 2018;486:44–48. doi:10.1016/j.cca.2018.07.029
22. Menyhart O, Fekete JT, Győrffy B. Inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the systemic immune-inflammation index (SII) and the systemic inflammation response index (SIRI). Int J Mol Sci. 2024;25(15):8441. doi:10.3390/ijms25158441
23. Pacheco-Barcia V, Mondéjar Solís R, France T, et al. A systemic inflammation response index (SIRI) correlates with survival and predicts oncological outcome for mFOLFIRINOX therapy in metastatic pancreatic cancer. Pancreatology. 2020;20(2):254–264. doi:10.1016/j.pan.2019.12.010
24. Wu Q, Zhao H. Prognostic and clinicopathological role of pretreatment systemic inflammation response index (SIRI) in gastric cancer: a systematic review and meta-analysis. World J. Surg. Oncol. 2024;22(1):333. doi:10.1186/s12957-024-03602-3
25. Hatogai K, Fujii S, Kojima T, et al. Prognostic significance of tumor regression grade for patients with esophageal squamous cell carcinoma after neoadjuvant chemotherapy followed by surgery. J. Surg. Oncol. 2016;113(4):390–396. doi:10.1002/jso.24151
26. Leng X, He W, Yang H, et al. Prognostic impact of postoperative lymph node metastases after neoadjuvant chemoradiotherapy for locally advanced squamous cell carcinoma of esophagus: from the results of NEOCRTEC5010, a randomized multicenter study. Ann Surg. 2021;274(6):e1022–e1029. doi:10.1097/SLA.0000000000003727
27. Tang H, Tan L, Wang H, Shen Y, Yin J. Nodal downstaging of esophageal squamous cell carcinoma after neoadjuvant chemoradiotherapy: survival analysis if ypN0 Is achieved. J Gastrointest Sur. 2020;24(7):1469–1476. doi:10.1007/s11605-019-04317-7
28. Yun JK, Kim Y, Lee GD, et al. Tumor regression grade combined with lymph node status in esophageal squamous cell carcinoma after neoadjuvant chemoradiotherapy. Cancer Med. 2022;11(19):3623–3632. doi:10.1002/cam4.4748
29. Zhang C, Xu F, Qiang Y, et al. Prognostic significance of tumor regression grade in esophageal squamous cell carcinoma after neoadjuvant chemoradiation. Front Surg. 2022;9:1029575. doi:10.3389/fsurg.2022.1029575
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.