Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Integrated Digital Decision-Making Systems in Maternal Nursing and Maternity Care: A Scoping Review
Authors Darmayanti D, Widiasih R ![]() , Hadi S
, Hadi S ![]() , Solehati T
, Solehati T ![]()
Received 29 April 2026
Accepted for publication 6 June 2026
Published 19 June 2026 Volume 2026:19 620994
DOI https://doi.org/10.2147/JMDH.S620994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Darmayanti Darmayanti,1 Restuning Widiasih,2 Setiawan Hadi,3 Tetti Solehati2
1Faculty of Nursing, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia; 2Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia; 3Department of Computer Science, Faculty of Mathematics and Natural Sciences, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia
Correspondence: Darmayanti Darmayanti, Faculty of Nursing, Universitas Padjadjaran, Bandung, Jawa Barat, 45363, Indonesia, Tel +6281221765312, Email [email protected]
Background: Effective decision-making systems are essential in maternal nursing and maternity care, particularly in situations requiring timely risk assessment, early complication detection, referral, and coordinated clinical action. Integrated digital systems, including electronic records, clinical decision support systems, mHealth applications, digital triage tools, and risk calculators, may support evidence-informed decision-making and improve care processes.
Objective: To map evidence on the implementation, outcomes, and barriers of integrated digital decision-making systems in maternal nursing and broader maternity care services.
Methods: A scoping review was conducted following the Arksey and O’Malley framework, enhanced by Levac et al, and reported according to PRISMA-ScR. Searches were conducted in PubMed, Scopus, and CINAHL for original research articles published in English or Indonesian between 2011 and 2025. Eligible studies focused on digital or integrated decision-making systems used in maternal nursing or maternity care. Data were extracted using a standardized charting form and synthesized using descriptive qualitative thematic analysis.
Results: Twelve studies met the inclusion criteria. Four themes were identified: impact on protocol adherence and workflow, clinical outcomes and predictive accuracy, patient-centered and psychosocial outcomes, and implementation barriers and sustainability. Several systems were associated with improved protocol adherence, history-taking completeness, triage timeliness, staff confidence, complication detection, patient knowledge, and satisfaction. However, clinical outcomes were mixed. Some tools showed high predictive accuracy or improved detection of complications, but effects on neonatal mortality, unnecessary admissions, transfers, and clinical management were inconsistent. Implementation barriers included limited infrastructure, poor connectivity, software inflexibility, dual documentation, workload burden, low digital literacy, and sustainability challenges.
Conclusion: Integrated digital decision-making systems may support maternal nursing and maternity care by improving care processes and patient-centered outcomes. However, their effects on hard clinical outcomes remain uncertain and depend on infrastructure, workforce readiness, workflow integration, interoperability, and sustained implementation support.
Keywords: clinical decision support system, digital health, electronic health records, maternity care, maternal nursing
Introduction
Maternal nursing has a central role in ensuring the safety of mothers and babies during pregnancy, childbirth, and postpartum.1 Nurses have primary responsibility for monitoring patient conditions, detecting complications early, and coordinating with other healthcare professionals to ensure timely interventions and adherence to standards of care.2 The complexity of maternal health conditions, shaped by physiological, psychological, and environmental factors, creates demanding decision-making situations with significant consequences for maternal and neonatal outcomes.3
Decision-making in maternal nursing is a complex process because it involves various clinical, managerial, and ethical aspects that must be considered simultaneously.4 Physiological factors of the mother and fetus, such as health status, pregnancy history, and potential obstetric complications, are key elements in the decision-making process. Furthermore, nurses’ decisions are influenced by hospital policies, evidence-based practice guidelines, and the availability of resources, including healthcare personnel and medical facilities.5 The dynamic and often stressful work environment in maternal care units adds to the challenges of decision-making, particularly in emergency situations such as eclampsia, postpartum hemorrhage, or fetal distress. Nurses are required to act quickly in situations that do not always allow sufficient time for in-depth analysis, increasing the risk of clinical errors. Furthermore, the need to coordinate with physicians, midwives, and other healthcare professionals to provide comprehensive care further complicates the decision-making process.6
Technological advances in healthcare have brought significant changes to clinical decision-making processes, including in maternal and maternity care. Various digital innovations, such as electronic medical records, electronic health records, clinical decision support systems, mobile health applications, and artificial intelligence-based tools, have increasingly been adopted to improve the efficiency, accuracy, and continuity of service delivery.7 In this context, an Electronic Medical Record (EMR) refers to a digital record of patient information used within a single healthcare institution, whereas an Electronic Health Record (EHR) generally refers to a broader electronic health information system that may support data sharing across healthcare providers or services. EHR allows nurses to access patient data in real time, including medical history, laboratory results, and obstetric records, making it easier to identify risks and plan interventions.8 A Clinical Decision Support System (CDSS) refers to a system that provides guideline-based recommendations, reminders, alerts, or risk assessments to support clinical decisions. CDSS can assist maternal nurses and maternity care teams by providing early warnings for maternal complications, such as gestational hypertension or fetal growth restriction.9 Meanwhile, mobile health (mHealth) refers to mobile applications or phone-based services that support health assessment, communication, monitoring, education, or decision-making. These technologies have increasingly been used to standardize practice and reduce variation in clinical decisions.
In this review, an integrated decision-making system refers to a technology-enabled system that combines patient data, clinical guidelines, alerts, risk assessment, and communication support to assist nurses and maternity care teams in making timely and evidence-informed decisions. This concept differs from general digital health tools because it emphasizes the integration of data, decision support, and clinical workflow rather than the use of a single standalone application.10 Therefore, the focus of this review is maternal nursing within broader maternity care systems. This clarification is important because decision-making in maternal care often involves not only nurses, but also midwives, physicians, community health workers, and other members of maternity care teams.11 Integrated systems may therefore support maternal nursing roles while also strengthening interprofessional coordination, documentation, referral, and team-based clinical decision-making.12
The lack of uniformity in standards and protocols in maternal nursing care presents a serious challenge to improving quality and patient safety. Variations in clinical policies and operational procedures between hospitals, or even within the same institution, often lead to inconsistencies in nursing practice.13 These differences can be seen in various aspects, such as maternal and fetal monitoring procedures, management of obstetric complications, and the use of clinical decision-making tools. Such inconsistencies can result in delayed intervention, inappropriate case management, and an increased risk of maternal and neonatal morbidity and mortality.14 In addition, the lack of uniform standards also makes coordination between health professionals difficult, especially when nurses must collaborate with doctors, midwives, and other medical personnel in emergency situations.15
An integrated decision-making system in maternal nursing services is a technology-based innovation designed to support efficiency, accuracy, communication, and safety in clinical decision-making. This system enables real-time access to patient data, allowing nurses and other healthcare professionals to obtain comprehensive information to determine appropriate interventions.16 Its key components may include EMR or EHR, CDSS, mHealth applications, risk calculators, digital triage systems, automated reminders, and, in some contexts, artificial intelligence-based analytic functions. The integration of these components may support early detection of maternal complications, such as preeclampsia or postpartum infections, and assist in risk management by providing automated alerts regarding patient conditions.17 In addition, this system can support communication and coordination between health professionals, including doctors, midwives, nurses, and other medical personnel, so that decision-making may be carried out more quickly and accurately.18 Such integrated systems may help reduce practice variation and strengthen interprofessional collaboration when they are effectively embedded into clinical workflows.
Previous reviews have examined digital maternal health, electronic records, telehealth, mobile health, or decision-support tools in broader obstetric, public health, and health informatics contexts. However, limited synthesis has specifically mapped how integrated decision-making systems support maternal nursing roles, interprofessional coordination, workflow, patient-centered outcomes, and implementation barriers in maternal nursing and broader maternity care settings. This gap is important because the effectiveness of digital systems in maternal care is not determined only by the availability of technology, but also by how these systems are integrated into nursing documentation, clinical reasoning, communication, team-based decision-making, and existing hospital infrastructure.
Although technology-based decision-making systems have been widely implemented in various health fields, research specifically exploring their application in maternal nursing remains limited. Several studies have shown that these technologies may improve the efficiency and accuracy of decision-making, but there has been no comprehensive review summarizing scientific evidence regarding their implementation, characteristics, impacts, and barriers in maternal nursing and maternity care contexts. A preliminary search indicates that very few reviews focus specifically on maternal nursing compared with broader obstetric or health informatics decision-making studies, highlighting a clear gap in the literature. Therefore, this study used a scoping review method to address the following question: What is known about integrated digital decision-making systems within maternal nursing and broader maternity care services? The objective of this review was to map the existing evidence, identify system characteristics, and analyze the challenges and impacts related to the integration of decision-making systems in maternal nursing and maternity care.
Method
Study Design
This study used a scoping review design to map the available evidence on integrated digital decision-making systems in maternal nursing and broader maternity care services. A scoping review was considered appropriate because the purpose of this study was not to estimate pooled intervention effectiveness, but to identify the types of systems used, their key characteristics, reported outcomes, implementation barriers, and gaps in the existing literature. The review was guided by the methodological framework proposed by Arksey and O’Malley and further developed by Levac et al19,20 The reporting of this review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). No formal review protocol was registered (Supplementary File 1).
Search Strategy
A comprehensive literature search was conducted in three electronic databases: PubMed, Scopus, and CINAHL. These databases were selected because they provide broad coverage of nursing, maternity care, health informatics, digital health, and clinical decision-support literature. The search included original research articles published between 2011 and 2025, representing the last 15 years of evidence relevant to digital and integrated decision-making systems in maternal nursing and maternity care.
The search strategy combined controlled vocabulary, database-specific subject headings, and free-text keywords related to decision-support systems, digital health technologies, maternal nursing, and maternity care. Boolean operators were used to combine the search terms. The main search terms included: “clinical decision support,” “decision support system,” “integrated decision-making system,” “electronic medical record,” “electronic health record,” “mHealth,” “digital health,” “maternal nursing,” “maternity care,” “obstetric care,” “antenatal care,” “perinatal care,” “hospital,” and “health facility.”
An example of the search string used was:
(“clinical decision support” OR “decision support system” OR “integrated decision-making system” OR “electronic medical record” OR “electronic health record” OR “mHealth” OR “digital health”) AND (“maternal nursing” OR “maternity care” OR “obstetric care” OR “antenatal care” OR “perinatal care”) AND (“hospital” OR “health facility”).
The search strategy was adapted according to the syntax and indexing system of each database. All retrieved records were exported to reference management software for organization and duplicate removal.
Eligibility Criteria
The eligibility criteria were guided by the Population/Participants, Concept, and Context (PCC) framework, which is appropriate for scoping reviews because it allows broader mapping of evidence without requiring a comparator group.
The Population/Participants included nurses, midwives, maternal healthcare workers, community health workers, or multidisciplinary maternity care teams involved in maternal decision-making. The Concept was integrated digital decision-making systems, including clinical decision support systems, electronic medical records, electronic health records, mHealth decision aids, digital triage systems, risk calculators, automated reminders, or other technology-enabled tools designed to support clinical decisions. The Context included maternal nursing and maternity care services, including antenatal, intrapartum, postpartum, obstetric emergency, hospital-based, and health-facility-based maternal care settings.
Studies were included if they met the following criteria: original research articles; published in English or Indonesian; published between 2011 and 2025; available in full text; and focused on technology-based or integrated decision-making systems used in maternal nursing or maternity care. Studies were excluded if they were review articles, editorials, opinion papers, conference abstracts without full text, grey literature, or studies that did not explicitly address digital or integrated decision-making systems in maternal nursing or maternity care.
Although the main focus of this review was maternal nursing in hospital-based or health-facility-based care, studies conducted in primary-level maternal health facilities or community-linked maternity care were included when the intervention directly supported maternal decision-making, referral, risk assessment, clinical workflow, or coordination with maternity care teams. This decision was made because maternal nursing decision-making often occurs within broader maternity care systems that involve multiple professionals and levels of care.
Study Selection
The study selection process was conducted in several stages. First, all retrieved records were imported into reference management software, and duplicates were removed. Second, two reviewers independently screened titles and abstracts based on the eligibility criteria. Before formal screening, the reviewers piloted the eligibility criteria on a sample of retrieved records to ensure consistent interpretation. Disagreements were discussed, and the criteria were refined before full screening.
Third, potentially eligible articles were retrieved and assessed in full text by two reviewers independently. Any disagreements during title-abstract screening or full-text assessment were resolved through discussion. If consensus could not be reached, a third reviewer was consulted. The study selection process was documented using a PRISMA flow diagram.21
Data Extraction
Data extraction was conducted using a standardized data-charting form developed in Microsoft Excel. The form was piloted on several included studies before full extraction to ensure that all relevant information could be captured consistently. Two reviewers independently extracted the data, and the extracted information was compared for accuracy and completeness. Any discrepancies were resolved through discussion, and unresolved disagreements were reviewed by a third reviewer.
The extracted data included author and year of publication, country, study setting, study design, sample size, population or participants, type of digital decision-making system, system components, intervention characteristics, outcome category, key findings, and reported barriers or facilitators to implementation. Outcome categories included process-related outcomes, clinical outcomes, patient-centered outcomes, workforce-related outcomes, and implementation outcomes.
Critical Appraisal
Consistent with the purpose of a scoping review, no formal methodological quality appraisal or risk-of-bias assessment was conducted. The aim of this review was to map the extent, characteristics, and nature of the available evidence rather than to determine intervention effectiveness or exclude studies based on methodological quality. However, the methodological characteristics of the included studies, including study design, setting, sample, intervention type, and reported outcomes, were charted and described to support interpretation of the findings.
Data Analysis and Synthesis
Data were analyzed using a descriptive qualitative thematic synthesis. Thematic synthesis was conducted using an inductive approach. Two reviewers independently read the extracted data several times to become familiar with the content, generated initial codes, compared coding decisions, and grouped similar codes into descriptive themes. The themes were then refined through discussion among the review team to ensure that they were grounded in the extracted findings.
The synthesis focused on identifying patterns across studies regarding the types of decision-making systems used, their reported effects, implementation barriers, and implications for maternal nursing and maternity care. Quantitative findings, such as statistical significance, effect estimates, or reported changes in outcomes, were summarized descriptively because the included studies were heterogeneous in design, intervention type, population, and outcome measurement. No meta-analysis was conducted.
Four main themes were developed from the synthesis: (1) impact of digital tools on protocol adherence and workflow, (2) clinical outcomes versus predictive accuracy, (3) patient-centered and psychosocial outcomes, and (4) barriers to sustainable implementation. These themes were used to organize the results and align the synthesis with the objectives of the review.
Results
Selection of Sources of Evidence
The database search yielded 684 records. After removing 80 duplicates, 604 records were screened by title and abstract. Of these, 542 records were excluded because they did not meet the eligibility criteria. Sixty-two reports were sought for retrieval. After further screening, 45 reports were excluded based on title and abstract relevance, leaving 17 reports for full-text assessment. Five full-text reports were excluded, and 12 studies were included in the final synthesis (Figure 1).
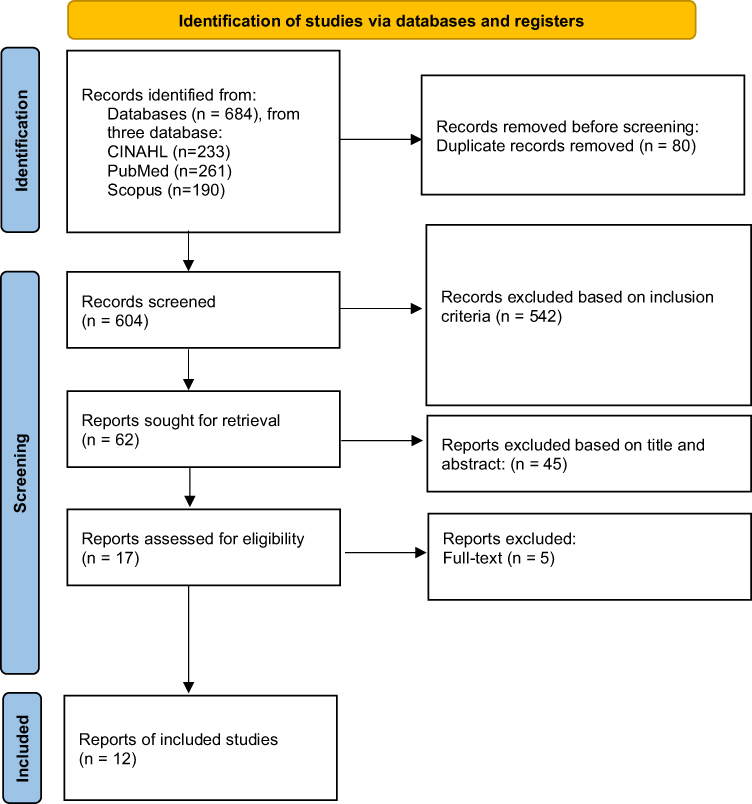 |
Figure 1 PRISMA Flow Diagram.21 |
Characteristics of Included Studies
The 12 included studies originated from diverse geographical settings: Ghana (n = 5),22–26 the United Kingdom (n = 2),27,28 Australia (n = 1),29 India (n = 1),30 Burkina Faso (n = 1),17 South Africa (n = 1),31 and a multi-country study involving Ghana and Tanzania (n = 1).7 A significant proportion of the evidence (6 out of 12 studies) involved health systems in Ghana, which provides a strong regional focus but may limit the direct transferability of some findings to significantly different healthcare infrastructures (Table 1).
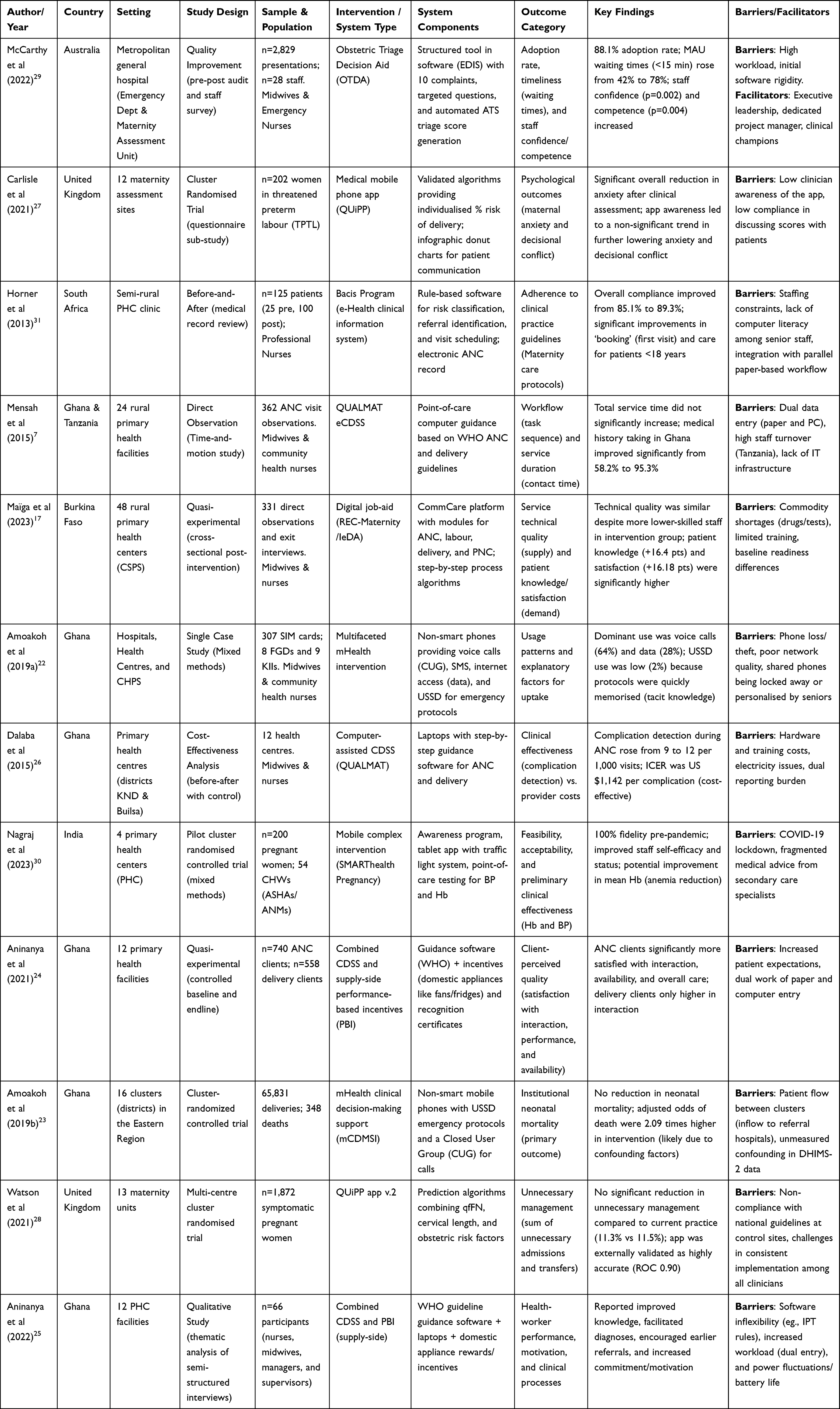 |
Table 1 Extraction Data |
Study Designs and Settings
The study designs were standardized into five categories for consistency:
Cluster Randomized Controlled Trials (cRCT) (n = 4): These evaluated system-wide impacts on neonatal mortality,23 prediction of preterm birth,27,28 and high-risk pregnancy screening.30
Pre-post Intervention Studies (n = 3): These assessed compliance with protocols,31 workflow efficiency,7 and the cost-effectiveness of complication detection.26
Quasi-experimental Studies (n = 2): These compared intervention and control groups regarding service quality17 and client satisfaction.24
Qualitative Studies (n = 2): These explored patterns of use and professional perspectives on performance.22,25
Quality Improvement Studies (n = 1): This audited the implementation and adoption of triage tools in clinical practice.29
The study settings varied across primary health facilities, rural health centers, antenatal care clinics, Community-based Health Planning and Services (CHPS) compounds, hospital maternity units, maternity assessment units, emergency departments, and community-linked maternal care services. This diversity of settings reflects the broad range of maternal care environments in which digital decision-support systems have been implemented.
Target Populations and Decision-Making Scope
While the focus of this review is on maternal nursing, the included evidence reflects a broader maternal care decision-making context. While several studies focused specifically on the performance and compliance of nurses and midwives,25,26,29,31 others involved community health workers (CHWs)—such as ASHAs in India—and auxiliary staff who play critical roles in frontline maternal care.7,30 Additionally, some studies evaluated impacts from the perspective of pregnant and postpartum women17,27 or utilized large-scale institutional data from entire maternity teams.23,28 Thus, the evidence represents a multi-disciplinary effort in maternal health decision-making rather than being exclusively nursing-specific.
Synthesis of Results
The synthesis of results from the 12 included studies is organized into four main themes: impact on protocol adherence and workflow, clinical outcomes and predictive accuracy, patient-centered and psychosocial outcomes, and implementation barriers and sustainability.
Impact on Protocol Adherence and Workflow
The implementation of computerized clinical decision support systems (CDSS) consistently demonstrated improvements in health-worker adherence to clinical protocols, although the impact on service duration and workload was varied. In South Africa, the Bacis Program improved overall compliance with maternity care protocols from 85.1% to 89.3%, with notable improvement in the “booking” or first-visit category (p = 0.016) and care for patients under 18 years of age (p = 0.0023).31 Similarly, in Ghana, the use of the QUALMAT eCDSS led to a substantial increase in medical history taking, rising from 58.2% to 95.3% (p < 0.001).7 Digital tools also supported standardized care; in Burkina Faso, the use of a digital job aid reduced variation in health history assessment scores across different health cadres.17
Regarding workflow, the Obstetric Triage Decision Aid (OTDA) in Australia improved timeliness, with the proportion of women seen within 15 minutes of arrival in the Maternity Assessment Unit (MAU) increasing from 42.0% to 78.0%.29 While there were initial concerns that technology might lengthen consultation times, studies in Ghana and Tanzania found no significant increase in total contact time for antenatal care (ANC) visits attributable to the eCDSS: 0.51 minutes in Ghana (p = 0.06) and 0.54 minutes in Tanzania (p = 0.26).7 However, a quasi-experimental study in Burkina Faso reported significantly longer median visit times in the intervention group, at 24 minutes, compared with 12 minutes in the comparison group.17 A recurring workflow challenge across multiple settings was the “dual entry” burden, where providers had to complete both the electronic system and mandatory paper registers, thereby increasing perceived workload.25,26
Clinical Outcomes and Predictive Accuracy
Digital interventions demonstrated high levels of accuracy in risk assessment and improved the detection of clinical complications. The QUiPP app v.2 was externally validated as a highly accurate tool for predicting preterm birth within seven days, achieving an area under the curve (AUC) of 0.90 (95% CI: 0.85–0.95).28 In rural India, the SMARThealth Pregnancy intervention showed preliminary effectiveness in improving maternal health markers, with a significant increase in mean hemoglobin levels in the intervention group compared with the control group (p = 0.01).30
In terms of clinical detection, the QUALMAT CDSS in Ghana significantly increased the identification of pregnancy complications during ANC from 9 to 12 per 1,000 visits (p = 0.010).26 Despite these improvements in detection and accuracy, the impact on broader clinical outcomes was limited. A large trial in Ghana found no significant reduction in neonatal mortality; the adjusted odds of death were 2.09 times higher in the intervention arm, with borderline statistical significance (p = 0.051), likely influenced by data confounding and patient flow issues.23 Similarly, the use of the QUiPP app in the UK did not significantly reduce unnecessary clinical management, defined as the sum of unnecessary admissions and transfers, compared with standard practice: 11.3% versus 11.5% (p = 0.883).28
Patient-Centered and Psychosocial Outcomes
Digital health interventions positively influenced patient knowledge, satisfaction, and the professional confidence of health workers. In Burkina Faso, women in the intervention group achieved significantly higher scores in knowledge of counseling, with an increase of 16.4 points, and overall satisfaction, with an increase of 16.18 points (p < 0.001).17 In Ghana, the combination of CDSS and performance-based incentives (PBI) significantly improved antenatal client satisfaction regarding provider interaction (p = 0.001) and provider availability (p = 0.001).24
Psychosocially, the process of clinical assessment, with or without the app, was found to significantly reduce maternal anxiety (p < 0.05).27 From the provider perspective, the implementation of the OTDA in Australia led to a significant increase in staff confidence (p = 0.002) and competence (p = 0.004) to conduct obstetric triage.29 Community health workers in India also reported improved self-efficacy and enhanced professional recognition within their villages through the use of the mHealth platform.30
Implementation Barriers and Sustainability
Barriers to successful implementation included technical, infrastructural, and human factors. Infrastructural issues, such as power fluctuations and limited battery life, were major constraints in rural Ghana.25,26 Technical barriers included software inflexibility, such as rigid algorithms for malaria treatment and faulty electronic partographs that triggered unnecessary referrals.25 Furthermore, poor mobile network quality forced health workers in some areas to travel to specific locations to access USSD protocols.22
Human factors included low computer literacy among senior staff31 and a pattern in which USSD usage declined because providers quickly converted the digital protocols into tacit knowledge or “mindlines”.22 From a sustainability standpoint, the QUALMAT CDSS was found to be a cost-effective option in Ghana, with an incremental cost-effectiveness ratio (ICER) of US$1,142 per complication detected, which was below the national GDP per capita.26 Successful sustainability was linked to executive leadership support, the presence of clinical champions, and a dedicated project management team.29
Discussion
This scoping review mapped the evidence regarding integrated decision-making systems in maternal nursing services across diverse global settings. The review identified 12 studies employing various digital or technology-enabled interventions, including clinical decision support systems, mHealth applications, digital job aids, obstetric triage decision aids, risk prediction tools, and electronic clinical information systems. The findings indicate a complex landscape in which several digital tools were associated with improvements in process measures, such as adherence to clinical protocols, history taking, and patient satisfaction, but yield mixed results regarding hard clinical outcomes like mortality reduction. Furthermore, the effectiveness of these systems is heavily contingent upon infrastructural readiness and workforce adaptability.
The findings suggest that integrated digital decision-making systems were more consistently associated with improvements in process-related and patient-centered outcomes than with hard clinical outcomes. Improvements were reported in protocol adherence, history-taking completeness, timeliness of triage, staff confidence, patient satisfaction, and maternal knowledge.32 However, evidence regarding neonatal mortality, unnecessary admissions, transfers, and other clinical endpoints remained inconsistent.33 This distinction is important because it indicates that digital decision-support systems may strengthen how care is delivered, but they do not automatically improve clinical outcomes without adequate infrastructure, workforce readiness, and downstream clinical resources.
Within the Donabedian framework, structural deficiencies are identified as the primary drivers of intervention failure in low-resource settings. While recent studies demonstrated the feasibility of digital tools in specific contexts, other evidence reported declining usage of mHealth interventions over time due to logistical barriers such as shared phone ownership and network instability.34 This aligns with broader health informatics literature suggesting that technocentrism, or focusing on the tool rather than the socio-technical environment, often leads to implementation failure.35 Unlike in high-income settings where infrastructure is robust, the success of decision-making systems in developing regions is less determined by the accuracy of the algorithms and more by basic structural factors such as power stability and hardware availability.36
Beyond physical infrastructure, the economic sustainability of these interventions remains a critical structural consideration. While some evidence suggested that computer-based decision support systems could reduce the average cost per detected complication, this finding was an outlier in the broader review.6,37 Most included studies did not explicitly analyze the long-term maintenance costs of digital systems, such as software updates, server maintenance, and continuous staff training. In low-resource settings, the initial funding for pilot projects often covers these costs, but sustainability becomes fragile once external funding ceases.8,38 Therefore, the long-term viability of integrated decision-making systems may be strengthened when digital health initiatives are supported by sustainable financing mechanisms, including maintenance costs, software updates, staff training, and infrastructure support.16,39
Furthermore, the integration of digital decision-making systems fundamentally alters the dynamics of interprofessional collaboration within maternity wards. Traditionally, decision-making relies on verbal communication between midwives, nurses, and obstetricians.16 The shift to screen-based systems creates a centralized repository of information that can enhance coordination by ensuring all team members view the same real-time data. However, reliance on these systems can also inadvertently create communication silos, where clinicians prioritize data entry and screen interaction over face-to-face clinical discussions.38 Effective implementation therefore requires protocols that ensure digital tools support, rather than replace, the critical verbal handover and collaborative problem-solving required in complex obstetric emergencies.40
Regarding process indicators, several included studies reported improvements in adherence to evidence-based guidelines, completeness of assessment, and documentation following the introduction of decision-support systems or electronic records. Prompts and mandatory fields in digital systems forced more comprehensive history taking and protocol compliance. However, this thoroughness often came at the cost of workflow efficiency.41 The effects on workflow efficiency were mixed. Some tools improved timeliness, whereas other interventions were associated with longer visit duration or additional documentation burden. This mirrors findings in emergency nursing literature, where computerized provider order entry systems are often associated with increased time-on-task despite reducing error rates.42 This creates a tension for maternal nurses who must balance the need for comprehensive, algorithm-driven assessment with the urgency required in obstetric emergencies like postpartum hemorrhage.43
From a nursing informatics perspective, these systems have implications beyond the introduction of digital technology itself. They may influence nursing documentation, clinical reasoning, risk recognition, prioritization of care, communication with other professionals, and continuity of maternal care.44 However, these benefits depend on whether digital systems are designed around nursing workflows and whether nurses are adequately supported to interpret system-generated alerts and recommendations.45 Therefore, integrated decision-making systems should be understood as socio-technical interventions that combine digital infrastructure, clinical knowledge, professional judgment, and interprofessional communication.
The findings also suggest that digital decision-support systems may influence nurses’ clinical reasoning and confidence. For example, structured triage tools were associated with increased staff confidence and competence, while some predictive tools showed high accuracy without clearly changing clinical management. Although automation bias and algorithm aversion were not directly examined in the included studies, they may be relevant conceptual considerations when implementing decision-support systems in high-stakes maternal care. Digital tools should therefore be designed to support, rather than replace, nurses’ clinical judgment and interprofessional discussion.46
Another critical dimension often overlooked is the disparity in digital literacy among the nursing workforces. The successful adoption of integrated decision-making systems presupposes that the end-users possess adequate technological skills.47 However, a generational divide often exists where younger nurses may be digitally native but lack clinical experience, while senior nurses possess deep clinical intuition but may struggle with complex user interfaces. This gap can lead to resistance or misuse of the system, reducing the validity of the data entered. Consequently, implementation strategies must move beyond generic training sessions to provide targeted mentorship that bridges the gap between clinical expertise and digital competency, ensuring that the technology empowers rather than alienates the workforce.26
A critical finding of this review is the disconnect between the predictive accuracy of tools and actual clinical improvements. Some studies found that although predictive apps were highly accurate in forecasting preterm birth, they did not reduce unnecessary hospitalizations or medical interventions compared to standard care.12,48 Similarly, large-scale trials in Ghana found no reduction in neonatal mortality despite the availability of decision support. This suggests that decision aids alone are insufficient to change outcomes if the downstream resources, such as medicines and surgical capacity, or the clinical judgment to act on the advice are lacking.
The predominance of studies from Ghana suggests that the current evidence base is strongly shaped by low-resource maternal health system contexts. While this provides valuable insight into infrastructure and workforce barriers, caution is needed when transferring the findings to high-income settings or to hospital systems with different staffing models, digital infrastructure, and clinical governance structures.49 Conversely, the findings may be particularly relevant for other low- and middle-income settings where maternal health services face similar challenges related to power supply, internet connectivity, workforce shortages, and parallel paper-based documentation.50
Interoperability and integration with existing health information systems also emerged as important considerations. Integrated decision-making systems are unlikely to function optimally when EMR, EHR, CDSS, mHealth applications, and paper-based registers operate as separate or poorly connected systems.51 Fragmented data systems may increase documentation burden, contribute to double data entry, and reduce the usability of decision-support tools in time-sensitive maternity care.52 Future implementation should therefore consider platform compatibility, data standards, alert governance, user-centered interface design, and integration with existing clinical workflows to prevent digital tools from becoming an additional workload for nurses and maternity care teams.
In contrast, patient-centered outcomes were more consistently favorable, particularly in relation to satisfaction, knowledge, anxiety reduction, and perceived quality of communication. These findings suggest that digital tools may have value in supporting communication and counseling, even when effects on clinical endpoints remain uncertain. The findings also have relevance for maternal health systems in low- and middle-income countries, including Indonesia, where rapid and coordinated responses are essential in obstetric emergencies. In Indonesia, the Comprehensive Emergency Obstetric and Neonatal Care or Pelayanan Obstetri Neonatal Emergensi Komprehensif (PONEK) system illustrates the importance of multidisciplinary coordination in emergency maternal and neonatal care. However, this context should be viewed as one example of transferability rather than the primary focus of the review. Across settings, integrated digital decision-support systems may support timely access to patient data, referral decisions, documentation, and team communication when they are appropriately embedded into existing maternity care workflows.53,54
Although AI was discussed in the broader background as part of the evolving landscape of decision-support systems, the included studies primarily evaluated EMR/EHR, CDSS, mHealth interventions, digital triage tools, job aids, and risk calculators rather than fully AI-driven systems. Therefore, the findings of this review should not be interpreted as direct evidence of the effectiveness of artificial intelligence in maternal nursing decision-making.
Integrated decision-making systems in maternal nursing may offer a promising approach for supporting adherence to clinical protocols and improving patient-centered outcomes. However, their impact on hard clinical outcomes remains inconsistent and is heavily mediated by the socio-technical environment. For health service managers and policymakers, the findings suggest that investing in digital tools alone may be insufficient without attention to infrastructure, workflow, and workforce readiness. The findings suggest that implementation may be strengthened by simultaneous attention to structural elements, such as reliable power and internet connectivity, and workflow redesign to reduce the documentation and time burden on nurses. Future research should focus on implementation science to understand how to sustain these interventions in resource-limited settings beyond the pilot phase.
Limitations
This review has several limitations. First, no formal methodological quality appraisal or risk-of-bias assessment was conducted. This approach is consistent with the purpose of a scoping review, which aims to map the extent and nature of available evidence rather than determine pooled intervention effectiveness. However, the absence of formal critical appraisal limits the ability to judge the methodological robustness of individual studies and should be considered when interpreting the strength of the evidence. Second, the included studies were heterogeneous in terms of design, setting, population, intervention type, system components, and outcome measures. The inclusion of cluster randomized trials, quasi-experimental studies, pre-post studies, qualitative studies, and quality improvement studies limited the ability to perform meta-analysis or draw causal conclusions regarding effectiveness.
Third, the included studies were not evenly distributed across countries. Several studies were conducted in Ghana, and one additional multi-country study also involved Ghana. This concentration may limit the transferability of the findings to health systems with different digital infrastructure, clinical governance, workforce composition, and maternal care delivery models. Fourth, although this review focused on maternal nursing, not all included studies were exclusively nursing-specific. Some studies involved midwives, community health workers, physicians, managers, supervisors, pregnant women, postpartum women, or broader maternity care teams. Therefore, the findings should be interpreted as evidence related to maternal nursing within broader maternity care systems rather than maternal nursing practice alone.
Fifth, not all interventions represented fully integrated hospital decision-making systems. Some were mHealth interventions, digital job aids, risk calculators, triage tools, or systems implemented in primary health facilities and community-linked maternal care settings. This may limit the specificity of conclusions regarding hospital-based integrated decision-making systems. Sixth, only a small number of studies reported long-term outcomes, sustainability indicators, implementation costs, or cost-effectiveness. As a result, this review provides limited evidence on whether these systems remain effective, acceptable, and financially sustainable beyond the initial implementation or pilot phase. Finally, the search was limited to three electronic databases and to articles published in English or Indonesian. Relevant studies published in other languages, indexed in other databases, or available as grey literature may therefore have been missed.
Conclusion
This scoping review mapped evidence from 12 studies on integrated digital decision-making systems in maternal nursing and broader maternity care services. The findings suggest that electronic medical records, electronic health records, clinical decision support systems, mHealth interventions, digital triage tools, and risk calculators may improve process-related outcomes, including protocol adherence, completeness of history-taking, timeliness of triage, staff confidence, complication detection, and patient satisfaction. However, the effects on clinical outcomes, such as neonatal mortality, unnecessary hospitalization, transfer, and intervention rates, remain inconsistent.
The implementation of these systems appears to be influenced by infrastructure, workflow integration, workforce readiness, digital literacy, interoperability, and sustainability. Patient-centered outcomes, including satisfaction, maternal knowledge, anxiety reduction, and perceived quality of care, were generally more favorable than hard clinical outcomes. Future research should further examine long-term effectiveness, cost-effectiveness, nursing-specific outcomes, and implementation strategies across diverse maternal healthcare settings.
Acknowledgments
Authors would like to express their deepest gratitude to Universitas Padjadjaran that supported this research work.
Funding
This research has no external funding.
Disclosure
The authors have declared no conflict of interest regarding this work.
References
1. Ameme DK, Akweongo P, Afari EA, Noora CL, Anthony R, Kenu E. Effectiveness of adjunct telephone-based postnatal care on maternal and infant illness in the Greater Accra Region, Ghana: a randomized controlled trial. BMC Pregnancy Childbirth. 2022;22(1):800. doi:10.1186/s12884-022-05138-4
2. Hailemariam S, Agegnehu W, Derese M. Exploring COVID-19 related factors influencing antenatal care services uptake: a qualitative study among women in a rural community in Southwest Ethiopia. J Prim Care Community Health. 2021;12:2150132721996892. doi:10.1177/2150132721996892
3. Jean-Francois B, Bailey Lash T, Dagher RK, Green Parker MC, Han SB, Lewis Johnson T. The potential for health information technology tools to reduce racial disparities in maternal morbidity and mortality. J Womens Health. 2021;30(2):274–16. doi:10.1089/jwh.2020.8889
4. Kuppermann M, Kaimal AJ, Blat C, et al. Effect of a patient-centered decision support tool on rates of trial of labor after previous cesarean delivery: the proceed randomized clinical trial. JAMA. 2020;323(21):2151–2159. doi:10.1001/jama.2020.5952
5. Jongsma KR, van den Heuvel JFM, Rake J, Bredenoord AL, Bekker MN. User experiences with and recommendations for mobile health technology for hypertensive disorders of pregnancy: mixed methods study. JMIR mHealth uHealth. 2020;8(8):e17271–e17271. doi:10.2196/17271
6. Comrie-Thomson L, Webb K, Patel D, et al. Engaging women and men in the gender-synchronised, community-based Mbereko+Men intervention to improve maternal mental health and perinatal care-seeking in Manicaland, Zimbabwe: a cluster-randomised controlled pragmatic trial. J Glob Health. 2022;12:4042. doi:10.7189/jogh.12.04042
7. Mensah N, Sukums F, Awine T, et al. Impact of an electronic clinical decision support system on workflow in antenatal care: the QUALMAT eCDSS in rural health care facilities in Ghana and Tanzania. Glob Health Action. 2015;8(1):25756. doi:10.3402/gha.v8.25756
8. Kuo DZ, Houtrow AJ, Arango P, Kuhlthau KA, Simmons JM, Neff JM. Family-centered care: current applications and future directions in pediatric health care. Matern Child Health J. 2012;16(2):297–305. doi:10.1007/s10995-011-0751-7
9. Adepoju AA, Vidler M, Akadri AA, et al. The ability and safety of community-based health workers to safely initiate lifesaving therapies for pre-eclampsia in Ogun State, Nigeria: an analysis of 260 community treatments with MgSO4 and/or methyldopa. Pregnancy Hypertens. 2021;25:179–184. doi:10.1016/j.preghy.2021.05.005
10. Buur LE, Finderup J, Søndergaard H, Kannegaard M, Madsen JK, Bekker HL. Shared decision-making and planning end-of-life care for patients with end-stage kidney disease: a protocol for developing and testing a complex intervention. Pilot Feasibility Stud. 2022;8(1). doi:10.1186/s40814-022-01184-z
11. Tesha J, Fabian A, Mkuwa S, Misungwi G, Ngalesoni F. The role of gender inequities in women’s access to reproductive health services: a population-level study of Simiyu Region Tanzania. BMC Public Health. 2023;23(1):1111. doi:10.1186/s12889-023-15839-w
12. Has EM, Krisnana I, Efendi F, et al. Enhancing maternal caregiving capabilities model to prevent childhood stunting: a UNICEF-inspired model. SAGE Open Nurs. 2024;10;23779608231226060. doi:10.1177/23779608231226061
13. Ashebir F, Medhanyie AA, Mulugeta A, Persson LÅ, Berhanu D. Exploring women’s development group leaders’ support to maternal, neonatal and child health care: a qualitative study in Tigray region. Ethiop PLOS ONE. 2021;16. doi:10.1371/journal.pone.0257602.
14. Choudhary TS, Mazumder S, Haaland ØA, et al. Health equity impact of community-initiated kangaroo mother care: a randomized controlled trial. Int J Equity Health. 2021;20(1):263. doi:10.1186/s12939-021-01605-0
15. Townsend R, Chmielewska B, Barratt I, et al. Global changes in maternity care provision during the COVID-19 pandemic: a systematic review and meta-analysis. EClinicalMedicine. 2021;37:100947. doi:10.1016/j.eclinm.2021.100947
16. Oduro-Mensah E, Agyepong IA, Frimpong E, Zweekhorst M, Vanotoo LA. Implementation of a referral and expert advice call center for maternal and newborn care in the resource constrained health system context of the greater accra region of ghana. BMC Pregnancy Childbirth. 2021;21(1):56. doi:10.1186/s12884-020-03534-2
17. Maïga A, Ogyu A, Millogo RM, et al. Use of a digital job-aid in improving antenatal clinical protocols and quality of care in rural primary-level health facilities in Burkina Faso: a quasi-experimental evaluation. BMJ Open. 2023;13(9):e074770. doi:10.1136/bmjopen-2023-074770
18. Meißner A, Schnepp W. Staff experiences within the implementation of computer-based nursing records in residential aged care facilities: a systematic review and synthesis of qualitative research. BMC Med Inform Decis Mak. 2014;14:54. doi:10.1186/1472-6947-14-54
19. Arksey H, O’Malley L. Scoping studies: toward a methodological framework. Int J Soc Res Methodol. 2005;8:19–32. doi:10.1080/1364557032000119616
20. Levac D, Coquhoun H, O’Brien K. Scoping studies: advancing the methodology. Implement Sci. 2010;5. doi:10.1186/1748-5908-5-69.
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
22. Amoakoh HB, Klipstein-Grobusch K, Ansah EK, Grobbee DE, Yveoo L, Agyepong I. How and why front-line health workers (did not) use a multifaceted mHealth intervention to support maternal and neonatal healthcare decision-making in Ghana. BMJ Glob Heal. 2019;4(2):1–14.
23. Amoakoh HB, Klipstein-Grobusch K, Agyepong IA, et al. The effect of an mHealth clinical decision-making support system on neonatal mortality in a low resource setting: a cluster-randomized controlled trial. EClinicalMedicine. 2019;12:31–42. doi:10.1016/j.eclinm.2019.05.010
24. Aninanya GA, Otupiri E, Howard N. Effects of combined decision-support and performance-based incentives on reported client satisfaction with maternal health services in primary facilities: a quasi-experimental study in the Upper East Region of Ghana. PLoS One. 2021;16(4):e0249778. doi:10.1371/journal.pone.0249778
25. Aninanya GA, Williams JE, Williams A, Otupiri E, Howard N. Effects of computerized decision support on maternal and neonatal health-worker performance in the context of combined implementation with performance-based incentivisation in Upper East Region, Ghana: a qualitative study of professional perspectives. BMC Health Serv Res. 2022;22(1):1–9. doi:10.1186/s12913-022-08940-0
26. Dalaba MA, Akweongo P, Aborigo RA, et al. Cost-effectiveness of clinical decision support system in improving maternal health care in Ghana. PLoS One. 2015;10(5):1–12. doi:10.1371/journal.pone.0125920
27. Carlisle N, Watson HA, Seed PT, et al. Impact of a medical mobile phone app (QUiPP) for predicting preterm birth on the anxiety and decisional conflicts faced by women in threatened preterm labour. Midwifery. 2021;92:102864. doi:10.1016/j.midw.2020.102864
28. Watson HA, Carlisle N, Seed PT, et al. Evaluating the use of the QUiPP app and its impact on the management of threatened preterm labour: a cluster randomised trial. PLoS Med. 2021;18(7):1–15. doi:10.1371/journal.pmed.1003689
29. McCarthy MF, Pollock WE, McDonald SJ. Implementation of an obstetric triage decision aid into a maternity assessment unit and emergency department. Women Birth. 2022;35(3):e275–85. doi:10.1016/j.wombi.2021.06.001
30. Nagraj S, Kennedy S, Jha V, et al. A mobile clinical decision support system for high-risk pregnant women in rural india (smarthealth pregnancy): pilot cluster randomized controlled trial. JMIR Form Res. 2023;7:1–14. doi:10.2196/44362
31. Horner V, Rautenbach P, Mbananga N, Mashamba T, Kwinda H. An e-health decision support system for improving compliance of health workers to the maternity care protocols in South Africa. Appl Clin Inform. 2013;4(1):25–36. doi:10.4338/ACI-2012-10-RA-0044
32. Racine N, Madigan S, Plamondon A, Hetherington E, McDonald S, Tough S. Maternal psychosocial risk profiles in pregnancy: associations with postpartum maternal health and child outcomes. Clin Psychol Sci. 2018;6(6):783–796. doi:10.1177/2167702618788863
33. Shukla VV, Carlo WA. Review of the evidence for interventions to reduce perinatal mortality in low- and middle-income countries. Int J Pediatr Adolesc Med. 2020;7(1):4–10. doi:10.1016/j.ijpam.2020.02.004
34. Tomizawa R, Shigeta M, Reeves S. Framework development for the assessment of interprofessional teamwork in mental health settings. J Interprof Care. 2017;31(1):43–50. doi:10.1080/13561820.2016.1233098
35. Jedwab RM, Chalmers C, Dobroff N, Redley B. Measuring nursing benefits of an electronic medical record system: a scoping review. Collegian. 2019;26(5):562–582. doi:10.1016/j.colegn.2019.01.003
36. Mackintosh N, Agarwal S, Adcock K, et al. Online resources and apps to aid self-diagnosis and help seeking in the perinatal period: a descriptive survey of women’s experiences. Midwifery. 2020;90:102803. doi:10.1016/j.midw.2020.102803
37. Aliakbari F, Ghaedamini M, Deris F, Masoudi R. Relationship between nurses’ decision-making style and their disaster response competencies. Disaster Med Public Health Prep. 2022;16(1):19–24. doi:10.1017/dmp.2020.225
38. Venkateswaran M, Ghanem B, Abbas E, et al. A digital health registry with clinical decision support for improving quality of antenatal care in Palestine (eRegQual): a pragmatic, cluster-randomised, controlled, superiority trial. Lancet Digit Heal. 2022;4(2):e126–36. doi:10.1016/S2589-7500(21)00269-7
39. Rodriguez-Arrastia M, Martinez-Ortigosa A, Ruiz-Gonzalez C, Ropero-Padilla C, Roman P, Sanchez-Labraca N. Experiences and perceptions of final-year nursing students of using a chatbot in a simulated emergency situation: a qualitative study. J Nurs Manag. 2022;30:3874–3884. doi:10.1111/jonm.13630
40. van den Heuvel JFM, van Lieshout C, Franx A, Frederix G, Bekker MN, van Lieshout C. SAFE@HOME: cost analysis of a new care pathway including a digital health platform for women at increased risk of preeclampsia. Pregnancy Hypertens. 2021;24:118–123. doi:10.1016/j.preghy.2021.03.004
41. Ram S, Goldin D. Primary care clinician’s knowledge of trafficking in persons: a systematic review. J Transcult Nurs. 2022;33(3):388–397. doi:10.1177/10436596211070285
42. Ancker JS, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inf Decis Mak. 2017;17. doi:10.1186/s12911-017-0430-8.
43. Santos LGS, Rodrigues V, Rocha JR, de Assunção MRL, Borges MVC, Fontoura Nogueira da Cruz MC. Nationwide Spatial Patterns and Maternal and Birth-Related Factors Associated with Orofacial Clefts in Brazil. Int J Environ Res Public Health. 2025;22(7):995. doi:10.3390/ijerph22070995
44. Reeder B, Lee K. Evaluating and Incorporating Generative AI in Nursing Informatics and Data Science Graduate Courses. In: Strudwick G, Hardiker NR, Rees G, Lee YJ, editors. Studies in Health Technology and Informatics [Internet]. Columbia, United States: IOS Press BV: University of Missouri; 2024:205–209. https://www.scopus.com/inward/record.uri?eid=2-s2.0-85199654184&doi=10.3233%2FSHTI240135&partnerID=40&md5=832c4a0e8e2c509009be6d15723e7f1f.
45. Arcia A. Incorporation of Generative AI in an Introductory Nursing Informatics Course. In: Strudwick G, Hardiker NR, Rees G, Lee YJ, editors. Studies in Health Technology and Informatics [Internet]. San Diego, United States: IOS Press BV: University of San Diego; 2024:505–510. https://www.scopus.com/inward/record.uri?eid=2-s2.0-85199606414&doi=10.3233%2FSHTI240200&partnerID=40&md5=7c5b39eb5b909f217f88f45593a0abe0.
46. Kalmbach DA, Cheng P, Roth T, et al. Examining patient feedback and the role of cognitive arousal in treatment non-response to digital cognitive-behavioral therapy for insomnia during pregnancy. Behav Sleep Med. 2022;20(2):143–163.
47. Brown Amoakoh H, Klipstein-Grobusch K, Amoakoh-Coleman M, et al. The effect of a clinical decision-making mHealth support system on maternal and neonatal mortality and morbidity in Ghana: study protocol for a cluster randomized controlled trial. Trials. 2017;18:1–11. doi:10.1186/s13063-016-1752-z
48. Aliakbari F, Ghaedamini M, Deris F, Masoudi R. Relationship between nurses’ decision-making style and their disaster response competencies. Disaster Med Public Health Prep. 2022;16(1):19–24.
49. van den Heuvel JFM, Lely AT, Huisman JJ, Trappenburg JCA, Franx A, Bekker MN. SAFE@HOME: digital health platform facilitating a new care path for women at increased risk of preeclampsia – a case-control study. Pregnancy Hypertens. 2020;22:30–36. doi:10.1016/j.preghy.2020.07.006
50. Perrenoud P, Chautems C, Kaech C. “Whatsapping” the continuity of postpartum care in Switzerland: a socio-anthropological study. Women Birth. 2021;35:e263–e274. doi:10.1016/j.wombi.2021.06.009
51. Kataoka K, Nishizaki Y, Shimizu T, et al. Hospital Use of a Web-Based Clinical Knowledge Support System and In-Training Examination Performance Among Postgraduate Resident Physicians in Japan: nationwide Observational Study. JMIR Med Educ. 2024;10:e52207–e52207. doi:10.2196/52207
52. Donelle L, Hiebert B, Hall J. An investigation of mHealth and digital health literacy among new parents during COVID-19. Front Digit Heal. 2023;5.
53. Yusrawati Y, Respati T, Sekarwana N. Factors to improve the quality of comprehensive emergency obstetric and newborn care. Int J Public Heal Sci. 2023;12(3):1030–1039. doi:10.11591/ijphs.v12i3.22915
54. von Dadelszen P, Bhutta ZA, Sharma S, et al. The Community-Level Interventions for Pre-eclampsia (CLIP) cluster randomised trials in Mozambique, Pakistan, and India: an individual participant-level meta-analysis. Lancet. 2020;396(10250):553–563.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.