")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Integrated Chinese and Western Medicine for Coronary Heart Disease Prevention in Polycystic Ovary Syndrome: A 19-Year Nationwide Cohort Study
Authors Liao CC , Chien CH, Yu TS, Li JM
Received 2 October 2023
Accepted for publication 4 December 2023
Published 8 December 2023 Volume 2023:16 Pages 3959—3973
DOI https://doi.org/10.2147/JMDH.S442816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chung-Chih Liao,1,2 Chi-Hsien Chien,1 Teng-Shun Yu,3 Jung-Miao Li4,5
1Department of Post-Baccalaureate Veterinary Medicine, College of Medical and Health Science, Asia University, Taichung, 41354, Taiwan; 2Chuyuan Chinese Medicine Clinic, Taichung, 40455, Taiwan; 3Management Office for Health Data, China Medical University Hospital, Taichung, 40459, Taiwan; 4School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, 40402, Taiwan; 5Department of Chinese Medicine, China Medical University Hospital, Taichung, 40447, Taiwan
Correspondence: Jung-Miao Li, School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan, Tel +886– 4-22053366 ext.3139, Email [email protected]
Background: Polycystic ovarian syndrome (PCOS) is a common endocrine disorder in women of reproductive age. Chinese herbal medicine (CHM), a major branch of traditional Chinese medicine, has been reported to exert beneficial effects on PCOS symptoms. However, the relationship between CHM use and the risk of coronary heart disease (CHD) in patients with PCOS remains unclear. The study aimed to investigate the potential protective role of CHM on CHD incidence in patients with PCOS and to understand CHM prescription patterns for PCOS treatment.
Methods: This retrospective cohort study was performed using data from Taiwan’s Longitudinal Health Insurance Database 2000 (LHID2000). Patients with PCOS were identified, and data on their demographic characteristics, comorbidities, and medication use were extracted. The patients were then divided into CHM and non-CHM users.
Results: Propensity score matching yielded two balanced cohorts of 2913 individuals each. CHM users demonstrated a 94% reduced risk of CHD compared to non-CHM users (adjusted hazard ratio, 0.06; 95% confidence interval, 0.04– 0.1) during the 19-year follow-up period. Stratified analysis confirmed the benefits of CHM treatment on the incidence of CHD across various subgroups. The key elements identified in the CHM prescription patterns associated with reduced CHD risk were Xiang Fu, Yi Mu Cao, Jia Wei Xiao Yao San, and Gui Zhi Fu Ling Wan.
Conclusion: This study provides evidence that CHM may protect against CHD development in patients with PCOS. It is also highlight the most frequently prescribed CHM for mitigating CHD risk among patients with PCOS. These findings lay the groundwork for future studies to confirm and elucidate CHM’s therapeutic mechanisms in PCOS-related CHD prevention, offering a significant contribution to the field.
Keywords: polycystic ovary syndrome, coronary heart disease, Chinese herbal medicine, retrospective cohort study, prescription pattern
Introduction
Polycystic ovary syndrome (PCOS) is a prevalent endocrine disorder affecting an estimated 5–18% of women of reproductive age worldwide.1 It is a multifaceted disorder characterized by a constellation of symptoms, including ovulatory dysfunction, hyperandrogenism, and polycystic ovaries.2 However, PCOS transcends the boundaries of a reproductive disorder and has profound implications for metabolic and cardiovascular health.3
Numerous studies have established a substantial link between PCOS and a heightened risk of metabolic syndrome, including insulin resistance, obesity, dyslipidemia, and type 2 diabetes mellitus.4,5 The combination of these factors places women with PCOS at a significantly increased risk of cardiovascular diseases, and coronary heart disease (CHD) is a critical concern.6,7 CHD results from the buildup of plaque in the coronary arteries of the heart, leading to a reduction in blood flow to the heart muscle.8 The symptoms of CHD include chest pain and shortness of breath and, in more severe cases, can lead to heart attacks, heart failure, and even death, is the leading cause of death globally, accounting for millions of deaths annually.9
The association between PCOS and elevated CHD risk has been corroborated by various epidemiological studies.10–12 Women diagnosed with PCOS are more likely to possess conventional cardiovascular risk factors, such as obesity, hypertension, dyslipidemia, and insulin resistance, leading to an increased risk of CHD development.13,14 Furthermore, inflammation, a key player in the pathophysiology of atherosclerosis, has been observed to be chronically elevated in patients with PCOS, which could provide an additional link to their elevated CHD risk.15–17 Despite our growing understanding of the PCOS–CHD connection, the gap in developing effective strategies for the prevention and management of CHD in patients with PCOS remains substantial. The current therapeutic options, such as lifestyle modifications and pharmacological interventions targeting insulin resistance and dyslipidemia, have yielded some benefits but are often hampered by limited adherence, side effects, and inadequate risk reduction.18–20
Traditional Chinese medicine (TCM), with a rich history spanning several thousand years, offers a wide range of Chinese herbal medicine (CHM) treatments that have been increasingly integrated into modern healthcare. Several integrated CHM products have demonstrated cardiovascular protective effects.21–23 For example, a study demonstrated that Bushen Jieyu Tiaochong Formula (BJTF) effectively treats PCOS in a rat model. This is achieved by reducing cystic follicle dilation, normalizing hormone levels, and lessening stress-induced behavioral changes. It involves modulating the PERK-ATF4-CHOP signaling pathway and cerebral monoamine neurotransmitters, offering a novel approach for treating PCOS associated with psychological stress.24 Another study revealed that Bu-Shen-Tian-Jing Formula (BSTJF) significantly improved the outcomes of in vitro fertilization (IVF) in Chinese patients with PCOS. This included a higher number of retrieved and fertilized oocytes, increased pregnancy rates, and decreased anti-Müllerian hormone (AMH) levels in follicular fluids, without affecting fertilization rates or increasing complications.25 However, their long-term benefits in reducing CHD risk in patients with PCOS remain largely unexplored.
To investigate the effect of CHM treatment on the long-term risk of CHD in women diagnosed with PCOS, we conducted a retrospective cohort study using data extracted from a comprehensive population-based database in Taiwan. Moreover, we examined the prescription patterns of CHM used in the treatment of PCOS, which may be beneficial for preventing CHD.
Materials and Methods
Data Source
Since 1995, the National Health Insurance (NHI) program has been instrumental in providing healthcare coverage to both Taiwanese and foreign residents. It ensures access to medical services, medications, and treatments. The National Health Insurance Research Database (NHIRD) was established to support this program. It serves as an extensive repository of anonymized health data gathered from the NHI system, which encompasses the entire Taiwanese population. This retrospective cohort study utilized data from the Longitudinal Generation Tracking Database (LGTD) of the NHIRD for the year 2000. The LGTD 2000 contains claims data from a random sample of two million beneficiaries within the NHIRD, spanning from 2000 to 2018. Within the LGTD 2000, diseases were diagnosed using the International Classification of Diseases, 9th Revision, and 10th Revision, Clinical Modification (ICD-9-CM and ICD-10-CM, respectively) codes. Before 2016, diseases were identified using ICD-9-CM codes. However, since 2016, the ICD-10-CM has been used for this purpose. Medications were classified using anatomical therapeutic chemical codes, and CHMs were defined using the database’s unique codes for CHM. Due to privacy concerns for insured individuals, events reported in counts of one or two are not disclosed. This study received approval from the Institutional Review Board of China Medical University (CMUH111-REC2-109(CR-1)). Informed consent was waived, as the study utilizes de-identified data.
Study Populations
We selected female participants who were diagnosed with PCOS (ICD-9-CM:256.4; ICD-10-CM: E28.2) and had a minimum of two ambulatory or inpatient claims from January 1, 2000, to December 31, 2017, in the LGTD 2000. The following exclusion criteria were applied: (1) age < 20 years (n=1875) and (2) a history of CHD (ICD-9-CM: 410–414; ICD-10-CM: I20-I25) before the index date (n=388). Patients were divided into two cohorts during 2000–2017: the CHM cohort (n = 17,285) and the non-CHM cohort (n = 2959). The CHM cohort included patients who received CHM after the initial diagnosis of PCOS. The index date for this cohort was defined as the date when the patients first began receiving CHM. The non-CHM cohort included patients who did not receive CHM after their initial diagnosis of PCOS. The index date for this cohort was selected randomly between 2000 and 2017. Lastly, we employed 1:1 propensity score matching to balance potential confounders between the groups, such as demographic characteristics, comorbidities, and medications.
Covariate Assessment
The demographic factors evaluated included age, urbanization level, and income. Female patients were further divided into three age subgroups as follows: 20–29, 30–39, and ≥40 years. Urbanization was classified into three levels based on the population density in residential areas, with level 1 being the most urbanized and level 3 being the least urbanized. Income was defined by an individual’s monthly earnings and divided into three categories as follows: ≤19,999; 20,000–38,999; and ≥39,000 NT$. Baseline comorbidities were considered if the patients had these conditions before the index date. These comorbidities included diabetes mellitus (ICD-9-CM: 250; ICD-10-CM: E08-E13), hypertension (ICD-9-CM: 401–405; ICD-10-CM: I10-I15), hyperlipidemia (ICD-9-CM: 272; ICD-10-CM: E71.30, E75.21, E75.22, E75.24, E75.3, E75.5, E75.6, E77, E78.0, E78.1, E78.2, E78.3, E78.4, E78.5, E78.6, E78.70, E78.79, E78.8, and E78.9), congestive heart failure (ICD-9-CM: 428; ICD-10-CM: I50), stroke (ICD-9-CM: 430–438; ICD-10-CM: I60-I69), chronic kidney disease (ICD-9-CM: 585, 586, 587, 588, 589; ICD-10-CM: N18, N19, N25, N26, and N27), female infertility (ICD-9-CM: 628; ICD-10-CM: N97), mental disorders (ICD-9-CM: 290–319; ICD-10-CM: F01–F99), and obesity (ICD-9-CM: 278, 783.1; ICD-10-CM: E66.09, E66.1, E66.8, E66.9, E66.01, E66.2, E65, E67.0, E67.1, E67.3, E67.2, E67.8, E68, and R63.5). We also included covariates if the participants were prescribed common medications associated with PCOS during the study period. These medications include metformin, oral contraceptive pills (OCPs), clomiphene, and spironolactone.
Outcome Measures
The follow-up period was extended from the index date to December 31, 2018, the date of the patient’s death, withdrawal from the NHI system, or occurrence of CHD, whichever occurred first. We compared the incidence of CHD between the two groups of patients with PCOS during the follow-up period. In the CHM user group, we further examined the prescribed treatments, including calculating the frequency of single Chinese herbs and Chinese herbal formulas used for PCOS. Additionally, to ascertain the individual effects of specific CHM on CHD risk, we analyzed the association between CHD incidence and the most commonly used single herbs and herbal formulas. To understand the relationships between different single herbs and herbal formulas used for PCOS and to identify a core prescription pattern, we conducted a social network analysis of commonly combined CHM.
Statistical Analyses
Categorical variables are presented as frequencies and percentages, whereas continuous variables are reported as means and standard errors. To test the difference between the means of the two groups, we used t-tests for continuous variables and chi-square tests for categorical variables. Person-years were calculated by adding the follow-up times (in years), and the incidence rates of CHD were computed for each study cohort. Univariate and multivariate Cox models were used to estimate the hazard ratios (HR) and 95% confidence intervals (CI) to investigate the risk of CHD among patients with PCOS. Kaplan–Meier curves were plotted to depict the cumulative incidence of CHD in the two cohorts. The Log rank test was used to compare the survival data of patients with PCOS according to the use of CHM and non-CHM users to determine a significant difference in the survival curves. To understand the prescription pattern of CHM in PCOS, the frequency distribution, pattern of single herbs/herbal formula, and HR associated with the risks of CHM among patients with PCOS were determined. Social network analysis is a methodological approach that examines the connections and interactions between variables within a network. In this study, the network focused on single herbs and herbal formulas of PCOS and aimed to illustrate their relationships. The significance level was set at 0.05 for a two-tailed test. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Kaplan–Meier curves and social network plots were generated using R studio (3.5.2).
Results
Baseline Characteristics of the Study Population
After applying the inclusion and exclusion criteria, we identified 17,285 CHM and 2959 non-CHM users with PCOS from the LGTD 2000 dataset. Using 1:1 propensity score matching, the final study population was reduced to 2913 individuals in each cohort. A flowchart illustrating this process is presented in Figure 1. Table 1 presents the baseline characteristics of the cohorts. After propensity score matching, a balanced distribution of demographic characteristics and comorbidities was observed between the CHM and non-CHM cohorts. The mean age of the study population was approximately 32 years, with the majority of participants in the 30–39-year age group. The most common baseline comorbidity in both groups was female infertility, followed by mental disorders. More than half of the patients with PCOS used OCPs and clomiphene, with similar usage rates observed between the cohorts.
 |
Table 1 Characteristics of Patients with Polycystic Ovary Syndrome According to Reception of Chinese Herbal Medicine |
 |
Figure 1 Flowchart illustrating participant selection and cohort formation process in the study. |
CHD Risk and Covariates in Patients with PCOS
Table 2 presents a comprehensive analysis of crude and adjusted HRs for CHD and its covariates in patients with PCOS. Among patients with PCOS, the adjusted Cox model demonstrated a significant overall benefit for CHM users compared with non-CHM users (adjusted HR, 0.06; 95% CI, 0.04–0.1) after adjusting for adjusted for age, insurance amount, urbanization level, all comorbidities, and medication used. This indicates that CHM users had a 94% reduced risk of developing CHM compared to non-CHM users, suggesting that CHM treatment may play a protective role against the development of CHD in patients with PCOS. The risk of CHD was significantly higher in patients aged ≧40 years (adjusted HR, 1.8; 95% CI, 1.25–2.59) than in those aged 20–29 years. Patients with PCOS and baseline comorbidities such as hypertension, hyperlipidemia, stroke, female infertility, and mental disorders experienced a significantly increased risk of CHD (aHR > 1 and p < 0.05). No increase or decrease in the CHD risk in patients with PCOS who used metformin, OCPs, clomiphene, or spironolactone was observed (p > 0.05).
 |
Table 2 Crude and Adjusted Hazard Ratios for Coronary Heart Disease with Chinese Herbal Medicine and Covariates Among Patients with Polycystic Ovary Syndrome by Multivariable Cox Proportional Hazards Regression Analysis |
Stratified Analyses of CHM Treatment and CHD Risk in Patients with PCOS
Table 3 compares the incidence rates and HRs of CHD between CHM users and non-CHM users, stratified by demographics and clinical factors. The beneficial impact of CHM treatment on CHD incidence was observed across various subgroups, encompassing all ages, income, and urbanization, as well as patients with or without baseline comorbidities and medication usage, compared with non-CHM users (all aHR < 1 and p < 0.01).
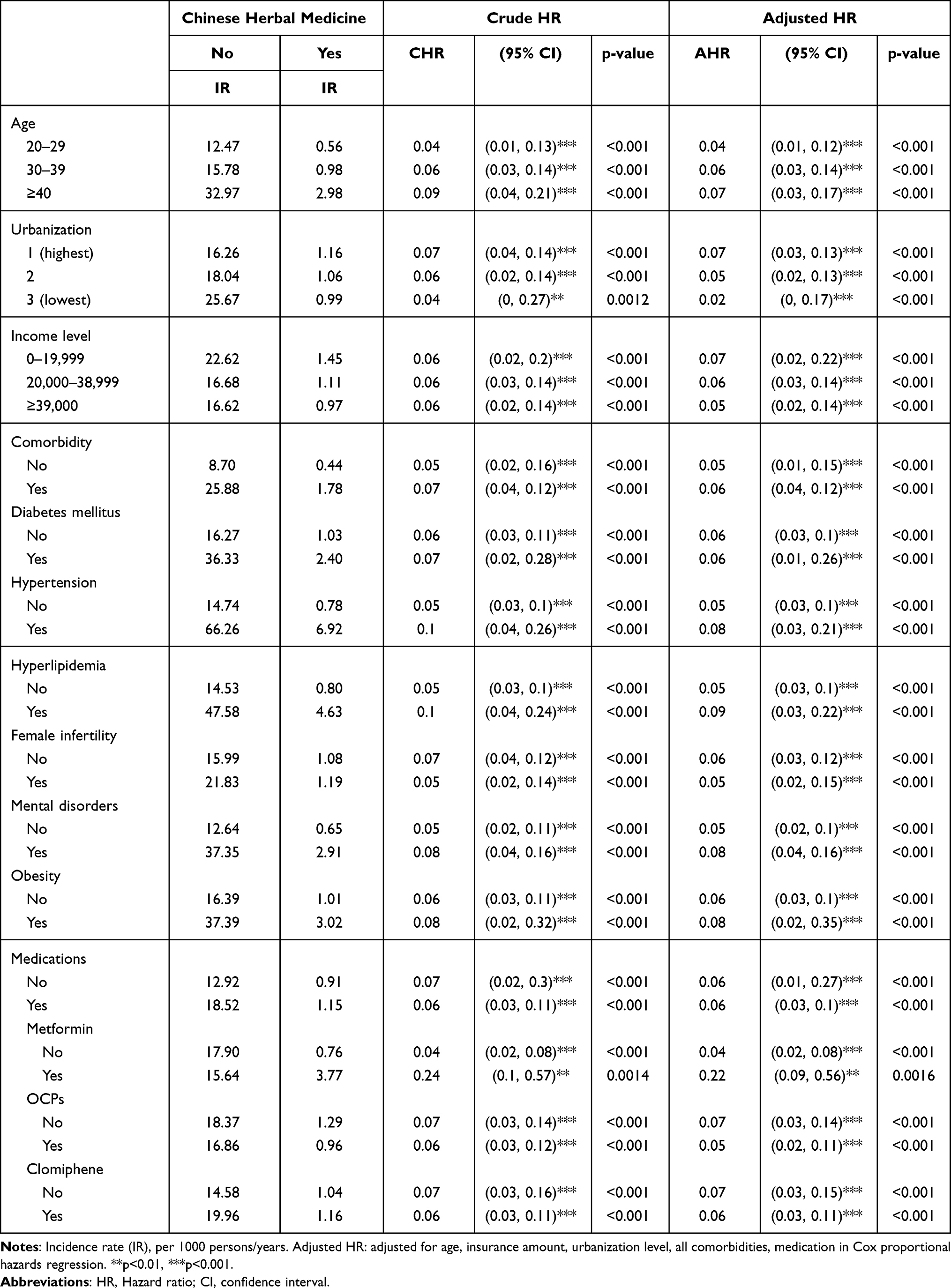 |
Table 3 Comparison of Incidence Rates and Hazard Ratios for Coronary Heart Disease Between Patients with Polycystic Ovary Syndrome Who Received Chinese Herbal Medicine Treatment and Those Who Did Not |
Association Between CHD Incidence and Cumulative Use Days of CHM in Patients with PCOS
We categorized the cumulative use days of CHM treatment into three subgroups:1–29 days, 30–59 days, and ≧60 days and compared them to those of the non-CHM treatment group in terms of the association of the risk of CHD with cumulative use days of CHM during the follow-up period among the patients PCOS. The patients with PCOS who received CHM treatments for cumulative 1–29 days exhibited a reduced risk of CHD (adjusted HR [aHR] = 0.13; 95% CI, 0.06–0.27) compared to the non-CHM users (Table 4). Similar benefits were observed in those who received CHM treatments for cumulative 30–59 days (aHR = 0.14; 95% CI, 0.06–0.35), while the risk of CHD was minimized in patients who underwent CHM treatments for cumulative ≧60 days (aHR = 0.02; 95% CI, 0.01–0.06) compared to the non-CHM users (Table 4).
 |
Table 4 Association Between Coronary Heart Disease Incidence and Cumulative Use Days of Chinese Herbal Medicine in Patients with Polycystic Ovary Syndrome |
Cumulative Incidence of CHD in Patients with PCOS
Figure 2 presents the results of the Kaplan–Meier analysis, which demonstrates the cumulative incidence of CHD in patients with PCOS. During the 19-year follow-up period, the CHM cohort demonstrated a significantly lower cumulative incidence of CHD than the non-CHM cohort (Log rank test, p < 0.001). This finding further supports the potential benefits of CHM treatment as a therapeutic intervention to reduce long-term CHD risk in patients with PCOS.
 |
Figure 2 Kaplan–Meier curve demonstrating the cumulative incidence of coronary heart disease in patients with polycystic ovary syndrome in the Chinese herbal medicine (CHM) and non-CHM cohorts. |
Prescription Patterns of Single Herbs and Herbal Formulas for PCOS and Their Association with CHD Risk
Table 5 presents the top 10 most frequently prescribed single Chinese herbs and herbal formulas for PCOS, along with information of the number of person-days, average daily dose (g), and average duration for prescription (days). The three most frequently prescribed single Chinese herbs were Xiang Fu (6396 prescriptions), Yi Mu Cao (5878 prescriptions), and Da Huang (5072 prescriptions). Jia Wei Xiao Yao San (8556 prescriptions), Gui Zhi Fu Ling Wan (5075 prescriptions), and Dang Gui Shao Yao San (5069 prescriptions) were the most commonly used Chinese herbal formulas. Moreover, compared to patients who did not receive CHM, patients with PCOS who received these single herbs and herbal formulas had a significantly lower risk of CHD.
 |
Table 5 Top 10 Most Frequently Prescribed Single Herbs and Herbal Formulas for Polycystic Ovary Syndrome, and Their Association with Coronary Heart Disease Risk |
Analysis of Common CHM Combinations and Social Correlation Network for PCOS
Table 6 lists the top 10 most frequently prescribed dual combinations of CHM for PCOS. The most common combination was “Xiang Fu plus Yi Mu Cao”, followed by “Nu Zhen Zi plus Han Lian Cao”, “Xiang Fu plus Jia Wei Xiao Yao San”, “Yi Mu Cao plus Jia Wei Xiao Yao San”, and “Yi Mu Cao plus Gui Zhi Fu Ling Wan”. Figure 3 illustrates a social correlation network graph representing the relationships between various Chinese herbs and herbal formulas used to treat PCOS. This graph was created by analyzing the 100 most commonly prescribed CHM combinations using RStudio. In the graph, each node represents a herb or herbal formula, and the edges (connecting lines) denote their co-prescription for treating PCOS. The thickness of each edge reflects the correlation strength or co-prescription frequency between two nodes. Combining this social correlation network with previous results from the most frequently prescribed single Chinese herbs and herbal formulas for reduced CHD risk in patients with PCOS, we identified Xiang Fu, Yi Mu Cao, Jia Wei Xiao Yao San, and Gui Zhi Fu Ling Wan as key elements in CHM prescription patterns (nodes marked in red in Figure 3).
 |
Table 6 Top 10 Most Frequently Prescribed Dual Combinations of Chinese Herbal Medicines for Polycystic Ovary Syndrome |
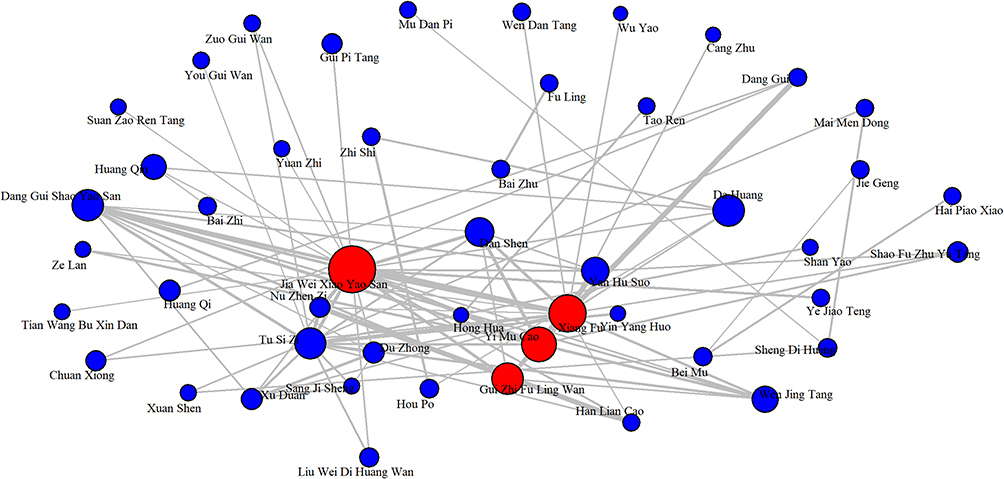 |
Figure 3 Social correlation network depicting relationships between various single herbs and herbal formulas used in Chinese herbal medicine for polycystic ovary syndrome treatment. |
Discussion
This population-based cohort study presents a significant association between CHM use and a long-term 94% reduction in the risk of CHD in patients with PCOS. This is a key finding, as the high prevalence of cardiovascular disease in women with PCOS is a well-documented phenomenon,26,27 and therapeutic strategies to mitigate this risk are continually being investigated. Using the comprehensive LGTD 2000 dataset, we identified specific patterns of CHM prescription and usage that were associated with significantly reduced CHD risk in patients with PCOS. These insights could not have been achieved through clinical trials owing to their inherent limitations, such as shorter duration, smaller sample size, and the challenge of isolating variables in complex conditions, such as PCOS. Moreover, our longitudinal approach provided a more robust and realistic picture of the effects of CHM over time, particularly in relation to CHD, a disease that typically develops over many years. This further enhances the validity of our findings and their applicability in real-world clinical settings. Furthermore, through the application of big data analytics, we uncovered correlations and generated hypotheses on a scale that is not feasible in traditional clinical trials. For example, our analyses of the most common CHM combinations and their efficacy in reducing CHD risk could pave the way for future investigations into the mechanisms of action of these herbal formulations.
The remarkable number of CHM users identified in this study (>85%) reflects the high prevalence of CHM use among patients with PCOS. This is consistent with previous studies demonstrating the popularity of complementary and alternative medicines, including CHM, in women with gynecological conditions.28–30 PCOS, a chronic and complex disorder, often requires long-term management, which may explain why many patients seek complementary treatment options such as CHM that emphasize holistic care and fewer side effects. The high usage rate of CHM in our study population could also be considered a reflection of its perceived effectiveness by patients and doctors, which is in line with previous research suggesting positive patient outcomes and satisfaction with CHM treatment for gynecological conditions.31,32 Moreover, the high utilization of CHM may be bolstered by the integration of TCM into Taiwan’s healthcare system, facilitating easy access to these treatments. Interestingly, the high prevalence of CHM use did not diminish the use of conventional treatments such as OCPs and clomiphene, as more than half of the patients in our study reported using these medications. This suggests that patients seek a complementary approach to managing PCOS by combining the benefits of traditional and modern medicine.
Our results echo the outcomes of numerous clinical trials and observational studies,33–35 providing additional real-world evidence on CHM therapy as an effective intervention for patients with PCOS. CHM, with its rich repository of bioactive components and multi-targeted action, is often lauded for its potential therapeutic benefits against various diseases, including PCOS and its associated complications.36–38 The most common single herbs and herbal formulas identified in our study, namely, Xiang Fu (Cyperi Rhizoma), Yi Mu Cao (Leonuri Herba), Jia Wei Xiao Yao San (Augmented Rambling Powder), and Gui Zhi Fu Ling Wan (Cinnamon and Poria Pill), were frequently prescribed to patients with PCOS and correlated with a lower CHD risk. Xiang Fu plays a crucial role as an important herb in Cangfu-Daotan decoction (CFDTT). A previous study has demonstrated that CFDTT treatment in obese PCOS rats led to dose-dependent improvements in lipid profiles, hormone levels, and inflammation markers. Furthermore, CFDTT enhances the expression of OATP2B1 and OATP3A1 in the ovarian and uterine tissues, which may have a positive impact on pregnancy outcomes.39 Another study identified Yi Cao’s potential for treating PCOS by harnessing active substances, such as quercetin and kaempferol, to regulate endocrine disorders and reduce inflammation. Therapeutic effects are achieved by targeting key pathways, including lipid metabolism, atherosclerosis, endocrine resistance, and AGE–RAGE signaling in diabetic complications, as validated by successful molecular docking experiments.40 In a pharmacoepidemiological study conducted in Taiwan, Jia Wei Xiao Yao San was identified as the most frequently prescribed Chinese herbal formula among the population.41 Jia Wei Xiao Yao San is also frequently used in women’s health. For example, one study compared the efficacy of Jia Wei Xiao Yao San with that of hormone replacement therapy, Premelle, for managing menopausal symptoms. Findings revealed that Jia Wei Xiao Yao San had fewer side effects and was as effective as Premelle in alleviating most menopausal symptoms, with its benefits not being mediated by hormone-like effects, thus demonstrating good compliance and safety.42 A systematic review and meta-analysis of clinical trials revealed that Xiao Yao San, when combined with conventional medicines, significantly improved ovulation and pregnancy rates and decreased fasting insulin levels and insulin resistance in women with PCOS.43 A previous study has revealed that Gui Zhi Fu Ling Wan alleviates inflammation and improves insulin resistance in rats with PCOS and insulin resistance (PCOS-IR). The underlying mechanism was demonstrated to be through regulating intestinal flora, which in turn controls inflammation, thus supporting the therapeutic use of Gui Zhi Fu Ling Wan for PCOS-IR.44 Another study has demonstrated that Gui Zhi Fu Ling Wan inhibits autophagy in granulosa cells, which is a key component of PCOS. This process is mediated by the upregulation of miR-29b-3p and the downregulation of H19, consequently reducing the expression of autophagy-related proteins and the formation of autophagosomes and autophagic polymers.45 Furthermore, one study has reported that the Fuling–Guizhi herb pair, a traditional Chinese herbal formula, has the potential to treat CHD. This potential is realized through the regulation of inflammatory responses and the reduction of TNF-α and IL-6 expressions, as identified by a combined approach of network pharmacology prediction and experimental verification.46
The significant reduction in CHD risk associated with CHM use in our study suggests that CHM could be considered as a complementary therapeutic option in the clinical management of PCOS, particularly for patients at elevated risk of cardiovascular diseases. However, this study has several limitations. First, we utilized administrative health data from the LGTD 2000 dataset, which may lack information on crucial clinical and lifestyle variables such as body mass index, dietary patterns, and physical activity levels. These factors significantly influence both PCOS and CHD; hence, their absence may have led to residual confounding factors. Second, our study did not consider instances in which patients may have purchased CHM out-of-pocket outside of health insurance coverage. This scenario may have led to significant variations in the dosage, quality, and consistency of treatment among patients, introducing variability that our study was unable to capture. Third, although we applied propensity score matching to address potential confounding factors, there may still be unmeasured confounders that could not be adjusted for in our analysis. Finally, the generalizability of our findings may be limited because of the nature of our study population, which comprised Taiwanese women only. Our findings may not apply to populations with different ethnic backgrounds, healthcare systems, or cultural attitudes toward CHM. Future prospective randomized studies should be conducted to address these limitations and further explore the potential benefits and mechanisms of CHM in reducing CHD risk in patients with PCOS.
Conclusion
This study highlights TCM’s effectiveness in lowering long-term CHD risk in PCOS patients. Key herbs and formulas, notably Xiang Fu, Yi Mu Cao, Jia Wei Xiao Yao San, and Gui Zhi Fu Ling Wan, emerge as beneficial. These results encourage integrating TCM in PCOS treatment, warranting further research to confirm these findings and understand underlying mechanisms.
Abbreviations
CHD, coronary heart disease; CHM, Chinese herbal medicine; PCOS, polycystic ovary syndrome; TCM, traditional Chinese medicine.
Data Sharing Statement
The data in this study are available to other researchers upon request from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the China Medical University in central Taiwan (CMUH111-REC2-109(CR-1)).
Acknowledgments
We are grateful to Health Data Science Center, China Medical University Hospital for providing administrative, technical and funding support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW112-TDU-B-212-144004), China Medical University Hospital (DMR-112-087). The funders had no role in the study design, data collection and analysis, the decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Disclosure
The authors declare no conflicts of interest.
References
1. The Lancet Regional H-E. Polycystic ovary syndrome: what more can be done for patients? Lancet Reg Health Eur. 2022;21:100524. doi:10.1016/j.lanepe.2022.100524
2. Harada M. Pathophysiology of polycystic ovary syndrome revisited: current understanding and perspectives regarding future research. Reprod Med Biol. 2022;21(1):e12487. doi:10.1002/rmb2.12487
3. Sangaraju SL, Yepez D, Grandes XA, et al. Cardio-metabolic disease and Polycystic Ovarian Syndrome (PCOS): a narrative review. Cureus. 2022;14(5):e25076. doi:10.7759/cureus.25076
4. Rojas J, Chávez M, Olivar L, et al. Polycystic ovary syndrome, insulin resistance, and obesity: navigating the pathophysiologic labyrinth. Int J Reprod Med. 2014;2014:719050. doi:10.1155/2014/719050
5. Kim JJ, Choi YM. Dyslipidemia in women with polycystic ovary syndrome. Obstet Gynecol Sci. 2013;56(3):137–142. doi:10.5468/ogs.2013.56.3.137
6. Kim C, Schreiner PJ, Siscovick D, et al. Factors associated with self-report of polycystic ovary syndrome in the Coronary Artery Risk Development in Young Adults study (CARDIA). BMC Womens Health. 2023;23(1):248. doi:10.1186/s12905-023-02394-0
7. Talbott E, Guzick D, Clerici A, et al. Coronary heart disease risk factors in women with polycystic ovary syndrome. Arterioscler Thromb Vasc Biol. 1995;15(7):821–826. doi:10.1161/01.atv.15.7.821
8. Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481–3488. doi:10.1161/circulationaha.105.537878
9. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;11(2):169–177. doi:10.2991/jegh.k.201217.001
10. Ollila MM, Arffman RK, Korhonen E, et al. Women with PCOS have an increased risk for cardiovascular disease regardless of diagnostic criteria-a prospective population-based cohort study. Eur J Endocrinol. 2023;189(1):96–105. doi:10.1093/ejendo/lvad077
11. Osibogun O, Ogunmoroti O, Michos ED. Polycystic ovary syndrome and cardiometabolic risk: opportunities for cardiovascular disease prevention. Trends Cardiovasc Med. 2020;30(7):399–404. doi:10.1016/j.tcm.2019.08.010
12. Wekker V, van Dammen L, Koning A, et al. Long-term cardiometabolic disease risk in women with PCOS: a systematic review and meta-analysis. Hum Reprod Update. 2020;26(6):942–960. doi:10.1093/humupd/dmaa029
13. Teede HJ, Hutchison S, Zoungas S, Meyer C. Insulin resistance, the metabolic syndrome, diabetes, and cardiovascular disease risk in women with PCOS. Endocrine. 2006;30(1):45–53. doi:10.1385/ENDO:30:1:
14. Lo JC, Feigenbaum SL, Yang J, et al. Epidemiology and adverse cardiovascular risk profile of diagnosed polycystic ovary syndrome. J Clin Endocrinol Metab. 2006;91(4):1357–1363. doi:10.1210/jc.2005-2430
15. Fenkci V, Fenkci S, Yilmazer M, Serteser M. Decreased total antioxidant status and increased oxidative stress in women with polycystic ovary syndrome may contribute to the risk of cardiovascular disease. Fertil Steril. 2003;80(1):123–127. doi:10.1016/s0015-0282(03)00571-5
16. Aboeldalyl S, James C, Seyam E, et al. The role of chronic inflammation in polycystic ovarian syndrome-a systematic review and meta-analysis. Int J Mol Sci. 2021;22(5):2734. doi:10.3390/ijms22052734
17. Rudnicka E, Suchta K, Grymowicz M, et al. Chronic low grade inflammation in pathogenesis of PCOS. Int J Mol Sci. 2021;22(7):3789. doi:10.3390/ijms22073789
18. Bełtowski J, Wójcicka G, Jamroz-Wiśniewska A. Adverse effects of statins - mechanisms and consequences. Curr Drug Saf. 2009;4(3):209–228. doi:10.2174/157488609789006949
19. Wake M, Oh A, Onishi Y, et al. Adherence and persistence to hyperlipidemia medications in patients with atherosclerotic cardiovascular disease and those with diabetes mellitus based on administrative claims data in Japan. Atherosclerosis. 2019;282:19–28. doi:10.1016/j.atherosclerosis.2018.12.026
20. Razavi-Nematollahi L, Ismail-Beigi F. Adverse effects of glycemia-lowering medications in type 2 diabetes. Curr Diab Rep. 2019;19(11):132. doi:10.1007/s11892-019-1266-7
21. Shaito A, Thuan DTB, Phu HT, et al. Herbal medicine for cardiovascular diseases: efficacy, mechanisms, and safety. Front Pharmacol. 2020;11:422. doi:10.3389/fphar.2020.00422
22. Kumar G, Dey SK, Kundu S. Herbs and their bioactive ingredients in cardio-protection: underlying molecular mechanisms and evidences from clinical studies. Phytomedicine. 2021;92:153753. doi:10.1016/j.phymed.2021.153753
23. Fugh-Berman A. Herbs and dietary supplements in the prevention and treatment of cardiovascular disease. Prev Cardiol. 2000;3(1):24–32. doi:10.1111/j.1520-037x.2000.80355.x
24. Pan X, Liu Y, Liu L, et al. Bushen Jieyu Tiaochong Formula reduces apoptosis of granulosa cells via the PERK-ATF4-CHOP signaling pathway in a rat model of polycystic ovary syndrome with chronic stress. J Ethnopharmacol. 2022;292:114923. doi:10.1016/j.jep.2021.114923
25. Pan X, Gu Y, Zhang X, et al. Chinese herbal medicine (Bu-Shen-Tian-Jing Formula) for outcomes of IVF in Chinese patients with polycystic ovary syndrome: a retrospective cohort study. Integr Med Res. 2022;11(1):100775. doi:10.1016/j.imr.2021.100775
26. Dwivedi AK, Vishwakarma D, Dubey P, Reddy S. Association of polycystic ovary syndrome with cardiovascular disease among female hospitalizations in the United States. Eur J Endocrinol. 2023;188(6):555–563. doi:10.1093/ejendo/lvad067
27. Wild S, Pierpoint T, McKeigue P, Jacobs H. Cardiovascular disease in women with polycystic ovary syndrome at long-term follow-up: a retrospective cohort study. Clin Endocrinol. 2000;52(5):595–600. doi:10.1046/j.1365-2265.2000.01000.x
28. Posadzki P, Lee MS, Moon TW, et al. Prevalence of complementary and alternative medicine (CAM) use by menopausal women: a systematic review of surveys. Maturitas. 2013;75(1):34–43. doi:10.1016/j.maturitas.2013.02.005
29. Nazik E, Nazik H, Api M, et al. Complementary and alternative medicine use by gynecologic oncology patients in Turkey. Asian Pac J Cancer Prev. 2012;13(1):21–25. doi:10.7314/apjcp.2012.13.1.021
30. Lin YR, Wu MY, Chiang JH, et al. The utilization of traditional Chinese medicine in patients with dysfunctional uterine bleeding in Taiwan: a nationwide population-based study. BMC Complement Altern Med. 2017;17(1):427. doi:10.1186/s12906-017-1939-1
31. Yang XC, Liu Y, Sun WW, et al. Efficacy of Chinese herbal medicines on pregnancy outcomes in patients with endometriosis in long-term management: a Multicenter Retrospective Cohort Study. Chin J Integr Med. 2023;29(11):971–979. doi:10.1007/s11655-023-3736-z
32. Zhao RH, Liu Y, Tan Y, et al. Chinese medicine improves postoperative quality of life in endometriosis patients: a randomized controlled trial. Chin J Integr Med. 2013;19(1):15–21. doi:10.1007/s11655-012-1196-6
33. Liao WT, Chiang JH, Li CJ, et al. Investigation on the use of traditional Chinese medicine for polycystic ovary syndrome in a nationwide prescription database in Taiwan. J Clin Med. 2018;7(7):179. doi:10.3390/jcm7070179
34. Zhu P, Guan JZ, Hai QC, et al. The clinical effectiveness and safety of traditional Chinese medicine Jinfeng pill in adjuvant treatment of infertility with polycystic ovary syndrome: a protocol for systematic review and meta-analysis. Medicine. 2022;101(4):e28676. doi:10.1097/md.0000000000028676
35. Wang L, Liang R, Tang Q, Zhu L. An overview of systematic reviews of using Chinese medicine to treat polycystic ovary syndrome. Evid Based Complement Alternat Med. 2021;2021:9935536. doi:10.1155/2021/9935536
36. Chen H, Deng C, Meng Z, Meng S. Effects of TCM on polycystic ovary syndrome and its cellular endocrine mechanism. Front Endocrinol. 2023;14:956772. doi:10.3389/fendo.2023.956772
37. Luo L, Shen Y, Ning D, et al. Chao Nang Qing prescription promotes granulosa cell apoptosis and autophagy by targeting GATA3. Gynecol Endocrinol. 2023;39(1):2223724. doi:10.1080/09513590.2023.2223724
38. Liao WT, Su CC, Lee MT, et al. Integrative Chinese herbal medicine therapy reduced the risk of type 2 diabetes mellitus in patients with polycystic ovary syndrome: a nationwide matched cohort study. J Ethnopharmacol. 2019;243:112091. doi:10.1016/j.jep.2019.112091
39. Yi W, Li X, Chen K, et al. Effects of Cangfu Daotan Decoction on obese polycystic ovary syndrome and its mechanism. Steroids. 2021;165:108740. doi:10.1016/j.steroids.2020.108740
40. Wu M, Liu H, Zhang J, et al. The mechanism of Leonuri Herba in improving polycystic ovary syndrome was analyzed based on network pharmacology and molecular docking. J Pharm Pharm Sci. 2023;26:11234. doi:10.3389/jpps.2023.11234
41. Hsieh SC, Lai JN, Lee CF, et al. The prescribing of Chinese herbal products in Taiwan: a cross-sectional analysis of the national health insurance reimbursement database. Pharmacoepidemiol Drug Saf. 2008;17(6):609–619. doi:10.1002/pds.1611
42. Chen LC, Tsao YT, Yen KY, et al. A pilot study comparing the clinical effects of Jia-Wey Shiau-Yau San, a traditional Chinese herbal prescription, and a continuous combined hormone replacement therapy in postmenopausal women with climacteric symptoms. Maturitas. 2003;44(1):55–62. doi:10.1016/s0378-5122(02)00314-6
43. Zhou X, Ma Q, Yan Z, et al. Efficacy and safety of Chinese patent medicine Xiao Yao San in polycystic ovary syndrome: a systematic review and meta-analysis. J Ethnopharmacol. 2023;313:116517. doi:10.1016/j.jep.2023.116517
44. Zhu Y, Li Y, Liu M, et al. Guizhi Fuling Wan, Chinese herbal medicine, ameliorates insulin sensitivity in PCOS model rats with insulin resistance via remodeling intestinal homeostasis. Front Endocrinol (Lausanne). 2020;11:575. doi:10.3389/fendo.2020.00575
45. Wu P, Zhu Y, Li J, et al. Guizhi Fuling Wan inhibits autophagy of granulosa cells in polycystic ovary syndrome mice via H19/miR-29b-3p. Gynecol Endocrinol. 2023;39(1):2210232. doi:10.1080/09513590.2023.2210232
46. Duan B, Han L, Ming S, et al. Fuling-Guizhi herb pair in coronary heart disease: integrating network pharmacology and in vivo pharmacological evaluation. Evid Based Complement Alternat Med. 2020;2020:1489036. doi:10.1155/2020/1489036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.