Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Inspiratory Flow Parameters Through Dry Powder Inhalers in Healthy Volunteers and Patients with Chronic Obstructive Pulmonary Disease (COPD): Device Resistance Does Not Limit Use in COPD
Authors Jõgi R, Mattila L, Vahteristo M ![]() , Takala A, Lähelmä S
, Takala A, Lähelmä S ![]() , Vartiainen VA, Lindqvist A
, Vartiainen VA, Lindqvist A
Received 8 January 2021
Accepted for publication 1 April 2021
Published 30 April 2021 Volume 2021:16 Pages 1193—1201
DOI https://doi.org/10.2147/COPD.S298514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Rain Jõgi,1 Leena Mattila,2 Mikko Vahteristo,3 Aino Takala,2 Satu Lähelmä,4 Ville A Vartiainen,2 Ari Lindqvist5
1Tartu University Hospital, Lung Clinic, Tartu, Estonia; 2Medical Affairs, Orion Corporation, Espoo, Finland; 3Research Unit of Pulmonary Diseases, Helsinki University Hospital and Helsinki University, Helsinki, Finland; 4Inhalation Platform, Orion Corporation, Espoo, Finland; 5Biostatistics and Data Analytics, Orion Corporation, Espoo, Finland
Correspondence: Rain Jõgi
Tartu University Hospital, Lung Clinic, Riia 167, Tartu, 50104, Estonia
Tel +372 5331 8918
Email [email protected]
Introduction: Achieving correct inhalation technique through an inhaler to ensure effective drug delivery is key to managing symptoms in patients with chronic obstructive pulmonary disease (COPD). However, many patients struggle to use their inhalers correctly, with the resultant reduction in therapeutic benefit. Consequently, appropriate inhaler choice is important to maximize clinical benefit. The primary objective of this study was to characterize inspiratory flow parameters across two Easyhaler® inhalers and the HandiHaler® inhaler in patients with COPD and healthy volunteers.
Methods: In this randomized, open-label, crossover study, subjects (100 patients with COPD; 100 healthy volunteers) were trained to perform inhalations of placebo powder via two variants of Easyhaler and placebo capsules via the HandiHaler inhalers. Subjects then performed three placebo inhalations through each inhaler in a random sequence. Inspiratory flow parameters were assessed, including peak inspiratory flow (PIF), for each inhaler. A parallel sub-study was conducted in patients with COPD from the main study to assess correct use of the inhalers, patient’s preference, ability to learn to use the inhalers, and the feasibility of the In-Check Dial device to measure PIF values.
Results: Mean PIF rates and inspiratory volumes through the three inhalers were similar between patients with COPD and healthy volunteers, and all subjects achieved the 30 L/min PIF required for effective use of Easyhaler. Almost 70% of the 88 patients enrolled in the sub-study used the Easyhaler and HandiHaler inhalers without errors. The Easyhaler was preferred by 51% of patients, while 25% favored the HandiHaler. Teaching the use of both inhalers to almost 70% of patients was very easy. The In-Check Dial PIF values and those obtained via spirometry were strongly correlated (p< 0.0001) for all three inhalers.
Conclusion: The respiratory performance of patients with COPD does not appear to be a limiting factor in the use of Easyhaler.
Keywords: COPD, crossover study, Easyhaler, HandiHaler, dry powder inhaler, peak inspiratory flow
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive disorder characterized by severe airflow limitation and persistent respiratory symptoms, including dyspnea, cough, and sputum production.1 Although no cure is available currently for COPD, pharmacotherapy can be used to ease the symptoms, frequency and severity of exacerbations, as well as improving health and exercise tolerance.1,2 Maintenance bronchodilator therapy is pivotal to symptom management, with anticholinergics recommended as the first-line therapeutic option.1,2 The anticholinergic agent tiotropium is a long-acting, potent, and specific muscarinic antagonist that improves lung function in patients with COPD.3 Tiotropium also reduces exacerbations and related hospitalizations, improves symptoms and health status and improves the effectiveness of pulmonary rehabilitation.1
Oral inhalation is the preferred administration route in patients with chronic respiratory diseases; it enables direct exposure to the airways coupled with effective use of lower doses compared with other administration routes.4 The choice of inhaler is important, as failure to achieve the correct inhalation technique may result in a lower drug dose and failure to manage symptoms. Consequently, the inhaler should be easy to use to ensure adequate drug delivery.5 For home use, inhaled COPD medications are typically delivered via a dry powder inhaler (DPI) or a pressurized metered-dose inhaler (pMDI).5,6 The pMDI uses a pressurized propellant to deliver the dose; however, despite being widely used, pMDIs require considerable coordination between inhalation and drug delivery and a precise breathing pattern, making them difficult to use.5–7 A spacer can be used to ensure adequate delivery of the drug in patients who have difficulty coordinating activation of the pMDI with inhalation, but their use introduces additional complications, including reduced portability and higher costs.8
DPIs have advantages over most pMDIs in that they are breath-actuated, easy to use, and more environmentally friendly as they do not rely on propellants.4 However, to ensure drug delivery to the lungs, the patient must generate sufficient inspiratory flow to de-aggregate the powder formulation into breathable-sized particles.9 For most DPIs, a peak inspiratory flow (PIF) rate of ≥30L/min ensures delivery and deposition of aerosolized drugs into the lungs.10
The Easyhaler® (Orion Corporation, Orion Pharma, Espoo, Finland) device-metered DPI, which contains tiotropium bromide monohydrate (Tiotropium Easyhaler), is being developed to treat COPD, and is designed for ease of use. Tiotropium Easyhaler is compared to the originator product (Spiriva® 18μg capsule) administered via the HandiHaler® inhaler (Boehringer Ingelheim International GmbH, Germany), which is approved for use in the European Union (EU) as a maintenance bronchodilator treatment to relieve symptoms in patients with COPD.11
This clinical trial was designed to compare PIF rates generated using two different Easyhaler inhaler variants with those generated using the HandiHaler inhaler. A sub-study in patients recruited to the main study examined ease of use, patient preference, and the feasibility of using the In-Check Dial device to measure PIF values.
Methods
Study Design
This randomized, open-label, crossover study was conducted in Finland and Estonia. The primary objective of the study was to characterize the inspiratory flow parameters across Easyhaler and HandiHaler inhalers in patients with COPD and healthy volunteers. Easyhaler with placebo powder was used in two configurations, namely, standard (currently used for Easyhaler with salbutamol, formoterol, budesonide and beclomethasone) and center slot (currently used for Easyhaler with budesonide-formoterol and salmeterol-fluticasone) Easyhaler. The resistances for the standard and center slot Easyhaler were 0.044 √kPa min/L and 0.036 √kPa min/L.12 The comparator was the placebo powder in hard capsule form inhaled via a HandiHaler inhaler (resistance 0.047 √kPa min/L).12 These resistance levels correspond to medium-high for center slot Easyhaler and high for standard Easyhaler and Handihaler as classified by Laube et al.10 Study subjects were trained to perform the inhalations with placebo Easyhaler inhalers and placebo capsules inhaled via HandiHaler according to the manufacturers’ instructions including eg inhalation instructions for each inhaler. Subsequently, subjects were assigned to perform three single inhalations from each of the three inhalers in a randomly assigned sequence. Inspiratory flow parameters were assessed, and each subject was then crossed over to the next inhaler.
Study Subjects
Healthy volunteers and patients with COPD of differing severity were enrolled in the study. Eligible healthy volunteers were aged ≥18 years, with good general health ascertained by medical history and forced expiratory volume in 1 second (FEV1) ≥80% of the predicted value at screening. Eligible patients with COPD were aged ≥18 years with a documented diagnosis of COPD. Healthy volunteers were excluded if they had any evidence of a clinically significant cardiovascular, renal, hepatic, hematological, gastrointestinal, pulmonary, metabolic, endocrine, neurological, or psychiatric disease within the previous 2 years. Healthy volunteers and patients with COPD were excluded if they had any other chronic respiratory disease, acute respiratory infection or medical condition that in the opinion of the investigator might affect either the interpretation of the study results or the subject’s health, were participating in a clinical drug study, or if they had a severe milk allergy. All participants provided written informed consent. The study was conducted in accordance with the principles of the Declaration of Helsinki. The following local ethics committees approved the study: Ethics Committee IV of the HUS Hospital District for the sites in Finland, and the Research Ethics Committee of the University of Tartu (UT REC) for the site in Estonia.
Outcomes
The primary outcome variable was PIF rate through the Easyhaler and HandiHaler inhalers, measured as previously described.13 For each inhaler, three inspiratory flow profiles were recorded and the inhalation with the highest PIF rate was analyzed. The inspiratory flow parameters were measured using the SpiroMaster MX Spirometer (Medikro, Kuopio, Finland). The secondary outcome variable was inspiratory volume through the Easyhaler and HandiHaler, which was recorded and analyzed from the same inhalation used to derive the highest PIF rate. Additional assessments included: FEV1, FEV1% predicted, forced vital capacity (FVC) and peak expiratory flow (PEF) derived from spirometry, patient age, sex, height and weight, smoking history, concomitant treatments, and current medical health. For patients with COPD, the following were also assessed as part of the screening process: COPD assessment test (CAT), modified Medical Research Council (mMRC) dyspnea scale, and exacerbation history/symptom burden and exacerbation risk (GOLD-ABCD classification).14
Sub-Study
A randomized, open-label, crossover sub-study was conducted in patients with COPD who were enrolled in the main study. All patients with COPD enrolled in the main study were invited to participate. The objective of the study was fourfold: to assess (1) the correct use of the Easyhaler and HandiHaler inhalers according to the instructions for use; (2) subject’s acceptability and preference of the inhalers; (3) subject’s ability to learn to use the inhalers; and (4) to compare PIF rates measured with the In-Check Dial device (using inhaler-specific inhalation instructions) to PIF values obtained via spirometry (ie inhalation through the inhaler) in the main study. The study was conducted during the main study visit after measurement of the inspiratory flow parameters. Subjects were excluded if they had been using the Easyhaler or HandiHaler within one year prior to the main study.
Statistical Methods
The nature of the study was not suitable for determining the sample size based on formal power calculations. The per-protocol group, comprising all patients who completed the study without any major deviations, was used for the statistical analysis. The primary and secondary variables, as well as other inspiratory and exploratory variables, were analyzed using descriptive statistics. The correlation of PIF rate with age, anthropometric, and lung function parameters was calculated using the Pearson’s correlation coefficient.
Results
Patient Baseline Characteristics
In total, 100 patients with COPD and 100 healthy volunteers were recruited and randomized (102 healthy volunteers were screened). The baseline characteristics of the two groups are shown in Table 1. All study subjects were Caucasian, while the majority (79%) of patients with COPD were male, compared with 40% of healthy volunteers. The mean age (range) in the COPD patient group was 70 (51‒82) years and in the healthy volunteers 31 (18‒62) years. Airflow limitation in patients with COPD ranged from mild to very severe, with FEV1 values that were between 16% and 96% of that predicted. Prior use of nicotine products was reported in 53% of patients with COPD, while 43% were current users; 74% of healthy volunteers had never used nicotine products. Of the 100 patients with COPD enrolled in the main study who were invited to participate in the sub-study, 88 were randomized and completed the assessments.
 |
Table 1 Patient Baseline Characteristics |
Disease characteristics for patients with COPD are shown in Table 2. The mean CAT score (range) was 16.4 (2‒35) points. The mean mMRC dyspnea grade (range) was 1.5 (0‒3). The ABCD classification, derived from symptom burden and exacerbation risk, was used as part of the screening procedure; over half of patients with COPD (58%) were in Group B (low risk of exacerbations with greater symptom burden). For 5 patients FEV1/FVC was between 0.70 and 0.74 while for 95 patients it was <0.70.
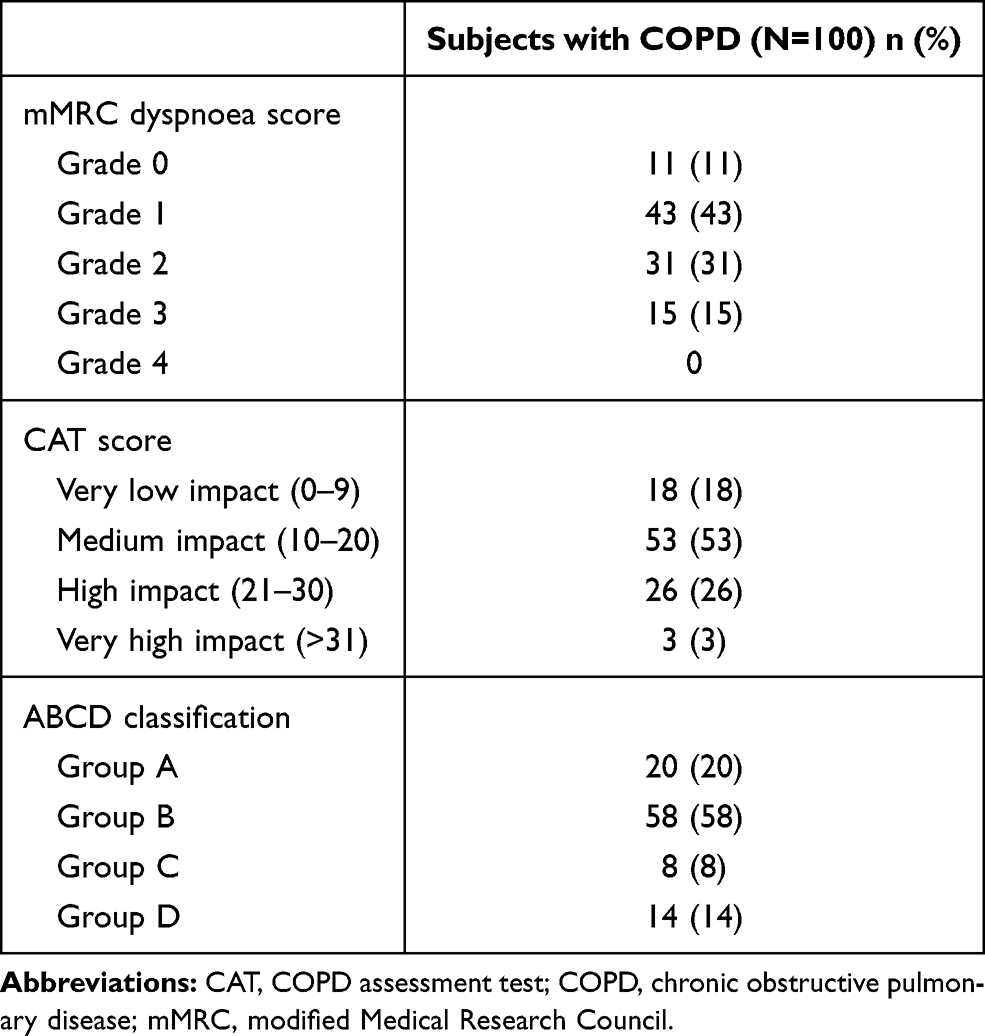 |
Table 2 Disease Characteristics for Patients with COPD |
All patients in the COPD group reported at least one current medical condition. The most common current medical condition reported by preferred term was hypertension (N=42), followed by hypercholesterolemia (N=21), and benign prostatic hyperplasia (N=15). Six healthy volunteers reported a current medical condition (two reported metabolism and nutrition disorders). A total of 104 subjects (96 COPD patients and 8 healthy volunteers) were taking 411 concomitant medications during the trial. The most common class of concomitant medications in COPD patients was adrenergics (N=80), followed by drugs for obstructive airway diseases (N=47), beta blocking agents (N=31), and lipid modifying agents (N=25).
PIF Rate
Healthy volunteers achieved a slightly higher (non-significant) mean PIF rate through the two Easyhaler inhalers than patients with COPD (center slot Easyhaler 72.2L/min and standard Easyhaler 62.0L/min versus 68.2L/min and 58.3L/min) (Figure 1; Table 3). No patients with COPD or healthy volunteers failed to achieve the recommended 30L/min with the Easyhaler devices.10 The mean PIF rate through the HandiHaler was slightly higher (non-significant) in COPD patients (49.5L/min versus 47.2L/min) (Figure 1). One patient in the COPD group failed to achieve the recommended 30L/min flow rate10 with the HandiHaler (29.9L/min) as did one subject in the healthy volunteer group (27.5L/min). No strong correlation between PIF rate and anthropometric measures or lung function parameters was observed in COPD patients or healthy volunteers.
 |
Figure 1 PIF rate for healthy volunteers and patients with COPD with each inhaler. Abbreviatios: COPD, chronic obstructive pulmonary disease; PIF, peak inspiratory flow. Note: Data presented for individual patients with mean value. |
 |
Table 3 Mean PIF, Mean Inspiratory Volume, Time to PIF and Duration of Inhalation for Healthy Volunteers and Patients with COPD |
Inspiratory Volume and Time
The mean inspiratory volumes for patients with COPD were slightly lower than those of healthy volunteers across the three inhalers, with the largest and only statistically significant (p < 0.01) difference between groups observed for the HandiHaler inhaler (Figure 2 and Table 3). Inspiratory volumes through the HandiHaler were higher for both healthy volunteers and patients with COPD versus the Easyhaler inhalers. Time to PIF and inhalation duration (Table 3) were similar between groups with Easyhaler while small difference was observed with Handihaler for both time to PIF and inhalation duration. In general, the acceleration of flow rate was faster and total duration shorter for Easyhaler when compared to Handihaler.
 |
Figure 2 Inspiratory volume for healthy volunteers and patients with COPD with each inhaler. Abbreviation: COPD, chronic obstructive pulmonary disease. Notes: Data presented for individual patients with mean. |
Sub-Study
Of the 88 patients with COPD enrolled in the sub-study, 24 (27%) made at least one error while using the Easyhaler inhaler, and 27 (31%) made at least one error using the HandiHaler. The two most common errors were not shaking the inhaler three times before actuation (6 patients) and not holding breath after inhalation (5 patients) for Easyhaler and not breathing out completely before inhalation (17 patients) and not breathing in slowly and deeply (6 patients) for HandiHaler. After training and demonstration of the use of the inhalers, patient’s acceptability and preference were assessed using a questionnaire. The proportion of patients choosing “no difference” was highest for 5 out of 9 inhaler characteristics included in the questionnaire. Those were instruction leaflet, inhalation through the inhaler, size, design, and mouthpiece. The proportion of patients choosing “Easyhaler” was highest for the following 4 characteristics: easier to learn how to use, easier to use, taking the drug is easier, handier to carry (Figure 3). The Easyhaler was preferred by 45 patients (51%), compared with 22 patients (25%) who preferred to use the HandiHaler. The study nurse assessed that it was very easy to teach the use of both inhalers to the majority of patients (Easyhaler 69% versus HandiHaler 66%), with most patients being taught how to use the inhalers in less than 5 minutes (Easyhaler 88% versus HandiHaler 78%). Mean PIF measured via In-Check Dial was lower than that measured by spirometry in the main study for all three devices; however, the In-Check Dial PIF values and those obtained via spirometry were strongly correlated (p<0.0001) for all three DPIs with R of 0.74, 0.68 and 0.68 for center-slot Easyhaler, standard Easyhaler and Handihaler, respectively (Table 4).
 |
Figure 3 Preference and acceptability of different inhaler characteristics for the Easyhaler and HandiHaler inhalers among patients with COPD. Patients were asked about preference and inhaler characteristics with the following questions and statements: which inhaler would you choose?; instruction leaflet of the inhaler is easier to understand; the inhaler is easier to learn how to use; taking the drug from the inhaler is easier; inhalation through the inhaler is easier; the inhaler has a more pleasant size; the design of the inhaler is more pleasant; the inhaler is handier to carry; mouthpiece of the inhaler is better. Abbreviation: COPD, chronic obstructive pulmonary disease. |
 |
Table 4 Mean PIF Measured Using In-Check Dial versus Spirometry |
Discussion
In this study, designed to compare inspiratory parameters between two Easyhaler variants and the HandiHaler inhaler, healthy volunteers and patients with COPD achieved the required PIF rate of 30L/min with the Easyhaler in both the standard and center slot configurations. Two subjects (one healthy volunteer and one patient with COPD) failed to achieve the required PIF rate when using the HandiHaler. Mean PIF rates through the three inhalers were very similar between healthy volunteers and patients with COPD.
The mean PIF rates achieved with the center slot and standard Easyhaler (68.2L/min and 58.3L/min) in patients with COPD observed in this study are consistent with those observed in previous studies.13,15,16 Similarly, the mean PIF rate of 49.5L/min achieved in patients with COPD using the HandiHaler is consistent with that from a previous observation in subjects with COPD,17 although it is higher than the 36L/min observed by Chapman et al in a small number of patients with moderate-to-severe COPD.18 The PIF rates achieved in this study were attained in a patient population that included patients with COPD with severe airflow limitation, where approximately 30% of the patients with COPD had a CAT score equating to high or very high disease impact. The mean PIF rates observed also reflect the relative inhaler airflow resistances: the highest mean PIF was achieved via the inhaler with the lowest resistance (the center slot Easyhaler [0.036 √kPa min/L]).19 The consistency observed between our findings and those from elsewhere adds additional strength to the findings of this study. When using the Easyhaler, no patient with COPD or healthy volunteer failed to achieve the 30L/min PIF rate considered to be the minimum required to achieve delivery and deposition of aerosolized drug deep into the lungs.10 Conversely, one patient with COPD and one healthy volunteer failed to achieve this threshold using HandiHaler, consistent with a previous observation, where some patients have failed to achieve 30L/min.18
Mean inspiratory volumes for center slot and standard Easyhaler were 2.16 and 2.02L in patients with COPD and 2.28 and 2.12L in healthy volunteers; however, mean inspiratory volumes with the HandiHaler were higher in both groups (COPD: 2.52L; healthy volunteers: 3.23L). This most likely reflects differences in the inhalation method used for each inhaler. For the Easyhaler, the inhalation starts at functional residual capacity (instructed as breathe out normally), while for the HandiHaler, inhalation starts at residual volume (breathe out completely). The difference, expiratory reserve volume, is in the magnitude of the difference we observed. In patients with COPD, the difference is smaller due to increased residual volume. In addition, the HandiHaler requires a slow and deep inhalation with a rate sufficient to hear or feel the capsule vibrate, making it easier to achieve a higher volume, while the Easyhaler inhalers require a strong and deep inhalation.
For clinical patient benefits as well as for the treating physician, patient satisfaction is an important property of any inhaler.20 In this study, Easyhaler was preferred over HandiHaler (51% vs 25%). The Easyhaler and HandiHaler inhalers were easy to use, with almost 70% of patients with COPD using each inhaler without errors. Furthermore, the healthcare practitioners involved in the study felt that it was easy to teach the use of the Easyhaler and HandiHaler inhalers, with most subjects learning to use them within 5 minutes, although this was somewhat more frequent among patients using the Easyhaler inhaler (88%). The correct use of an inhaler is key to drug delivery; however, user errors are common and may impact the effectiveness of the delivered drug.21 The most common errors with DPIs include exhaling into the inhaler before or after the actuation, and lack of breath holding after the inhalation.22 The importance of appropriate education, training, and use of checklists in the correct use of DPIs has been demonstrated.23,24 Sandler et al showed that patients who were unable to intuitively use an inhaler in the correct manner attained proficiency following careful guidance by the healthcare provider.25 Our results reinforce the concept that appropriate training combined with an easy-to-use inhaler increases the likelihood that patients will use the inhaler with minimal errors.
When inspiratory parameters were assessed using the In-Check Dial device, mean PIF values were between 4% (center slot Easyhaler) and 9% (HandiHaler) lower than those obtained via spirometry (through the inhaler); however, the relative results across the three inhalers showed a strong correlation with the results via spirometry, suggesting that In-Check Dial can correctly identify patients who are able to achieve the required inspiratory flow in order to use a particular DPI.
Limitations of our study include lack of blinding which is common to studies including several distinctive devices. This study consisted of a single visit and single training session. For the evaluation of correct use, the patients were allowed sufficient time to familiarize with the instructions and practice, but in real clinical use the training should be repeated. Even though the evaluation was standardized as far as possible, there is room for subjective interpretation with regard to steps like breathing out completely and taking a strong and deep breath in. Random allocation and crossover design was used to minimize any potential sequence bias. However, the most important variables for this study such as flow rates are objectively measured and therefore, relatively resistant to biasing. The diagnosis of COPD was not confirmed at the inclusion. However, 95 out of 100 patients had FEV1/FVC below 0.70 and for all of them it was below 0.75. FEV1/FVC results confirm that the study included a large population of subjects with spirometry verified airflow limitation and also that there was a wide range of disease severities in the study population.
Conclusions
Inspiratory flow parameters obtained with the two Easyhaler inhalers were similar to those obtained using the HandiHaler. These results were observed consistently across both healthy volunteers and patients with COPD. Using the Easyhaler, all study subjects were able to achieve a PIF rate greater than the required 30L/min threshold, even those with severe airflow limitations. Furthermore, patients with COPD appeared to prefer using the Easyhaler. Our data show that the respiratory performance of patients with COPD does not appear to be a limiting factor in the use of the Easyhaler.
Trial Identifier
NCT04147572.
Data Sharing Statement
Individual participant data will not be shared publicly.
Acknowledgments
Medical writing support, funded by Orion Corporation, Espoo, Finland, was provided by Paul Littlebury, PhD, from Bioscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The sponsor participated in study design, review, and approval, as well as manuscript review and approval for submission. The authors received no direct compensation related to the development of the manuscript. This trial was sponsored by Orion Corporation, Espoo, Finland.
Disclosure
Dr Jõgi reports personal fees from Boehringer, GSK, Novartis and Orion Pharma, outside the submitted work.
Dr Mattila, Mr Vahteristo, Dr Takala, Dr Lähelmä and Dr Vartiainen were employed by Orion Corporation.
Dr Lindqvist has been an investigator in studies sponsored by pharma companies in the field of obstructive lung diseases.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
2. Lopez-Campos JL, Soler-Cataluna JJ, Miravitlles M. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2019 report: future challenges. Arch Bronconeumol. 2020;56(2):65–67. doi:10.1016/j.arbres.2019.06.001
3. Keating GM. Tiotropium bromide inhalation powder: a review of its use in the management of chronic obstructive pulmonary disease. Drugs. 2012;72(2):273–300. doi:10.2165/11208620-000000000-00000
4. Lavorini F. Easyhaler((R)): an overview of an inhaler device for day-to-day use in patients with asthma and chronic obstructive pulmonary disease. Drugs Context. 2019;8:212596. doi:10.7573/dic.212596
5. Lavorini F. Inhaled drug delivery in the hands of the patient. J Aerosol Med Pulm Drug Deliv. 2014;27(6):414–418. doi:10.1089/jamp.2014.1132
6. Lavorini F, Fontana GA. Inhaler technique and patient’s preference for dry powder inhaler devices. Expert Opin Drug Deliv. 2014;11(1):1–3. doi:10.1517/17425247.2014.846907
7. Haughney J, Lee AJ, McKnight E, Pertsovskaya I, O’Driscoll M, Usmani OS. Peak inspiratory flow measured at different inhaler resistances in patients with Asthma. J Allergy Clin Immunol Pract. 2020.
8. Vincken W, Levy ML, Scullion J, Usmani OS, Dekhuijzen PNR, Corrigan CJ. Spacer devices for inhaled therapy: why use them, and how? ERJ Open Res. 2018;4(2):00065–2018. doi:10.1183/23120541.00065-2018
9. Lavorini F, Pistolesi M, Usmani OS. Recent advances in capsule-based dry powder inhaler technology. Multidiscip Respir Med. 2017;12:11. doi:10.1186/s40248-017-0092-5
10. Laube BL, Janssens HM, de Jongh FH, et al. What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37(6):1308–1331. doi:10.1183/09031936.00166410
11. Boehringer Ingelheim Limited. Spiriva 18 microgram inhalation powder, hard capsule; 2019. Available from: https://www.medicines.org.uk/emc/product/1693/smpc.
12. Delvadia R, Hindle M, Longest PW, Byron PR. In vitro tests for aerosol deposition II: IVIVCs for different dry powder inhalers in normal adults. J Aerosol Med Pulm Drug Deliv. 2013;26(3):138–144. doi:10.1089/jamp.2012.0975
13. Malmberg LP, Rytila P, Happonen P, Haahtela T. Inspiratory flows through dry powder inhaler in chronic obstructive pulmonary disease: age and gender rather than severity matters. Int J Chron Obstruct Pulmon Dis. 2010;5:257–262. doi:10.2147/COPD.S11474
14. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
15. Jogi R, Lahelma S, Vahteristo M, Happonen A, Haikarainen J. In vitro flow rate dependency of delivered dose and fine particle dose of salmeterol/fluticasone propionate easyhaler and seretide diskus with patient flow rates collected in a randomized controlled trial. J Aerosol Med Pulm Drug Deliv. 2019;32(2):88–98. doi:10.1089/jamp.2018.1463
16. Malmberg LP, Everard ML, Haikarainen J, Lahelma S. Evaluation of in vitro and in vivo flow rate dependency of budesonide/formoterol Easyhaler(R). J Aerosol Med Pulm Drug Deliv. 2014;27(5):329–340. doi:10.1089/jamp.2013.1099
17. Altman P, Wehbe L, Dederichs J, et al. Comparison of peak inspiratory flow rate via the Breezhaler(R), Ellipta(R) and HandiHaler(R) dry powder inhalers in patients with moderate to very severe COPD: a randomized cross-over trial. BMC Pulm Med. 2018;18(1):100. doi:10.1186/s12890-018-0662-0
18. Chapman KR, Fogarty CM, Peckitt C, et al. Delivery characteristics and patients’ handling of two single-dose dry-powder inhalers used in COPD. Int J Chron Obstruct Pulmon Dis. 2011;6:353–363. doi:10.2147/COPD.S18529
19. Levy ML, Carroll W, Izquierdo Alonso JL, Keller C, Lavorini F, Lehtimaki L. Understanding dry powder inhalers: key technical and patient preference attributes. Adv Ther. 2019;36(10):2547–2557. doi:10.1007/s12325-019-01066-6
20. Molimard M, Colthorpe P. Inhaler devices for chronic obstructive pulmonary disease: insights from patients and healthcare practitioners. J Aerosol Med Pulm Drug Deliv. 2015;28(3):219–228. doi:10.1089/jamp.2014.1142
21. Chrystyn H, van der Palen J, Sharma R, et al. Device errors in asthma and COPD: systematic literature review and meta-analysis. NPJ Prim Care Respir Med. 2017;27(1):22. doi:10.1038/s41533-017-0016-z
22. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105(6):930–938. doi:10.1016/j.rmed.2011.01.005
23. Pothirat C, Chaiwong W, Phetsuk N, Pisalthanapuna S, Chetsadaphan N, Choomuang W. Evaluating inhaler use technique in COPD patients. Int J Chron Obstruct Pulmon Dis. 2015;10:1291–1298. doi:10.2147/COPD.S85681
24. Sriram KB, Percival M. Suboptimal inhaler medication adherence and incorrect technique are common among chronic obstructive pulmonary disease patients. Chron Respir Dis. 2016;13(1):13–22. doi:10.1177/1479972315606313
25. Sandler N, Hollander J, Langstrom D, Santtila P, Saukkonen A, Torvinen S. Evaluation of inhaler handling-errors, inhaler perception and preference with Spiromax, Easyhaler and Turbuhaler devices among healthy Finnish volunteers: a single site, single visit crossover study (Finhaler). BMJ Open Respir Res. 2016;3(1):e000119. doi:10.1136/bmjresp-2015-000119
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.