Back to Journals » Nature and Science of Sleep » Volume 14
Insomnia Prevalence Varies with Symptom Criteria Used with Implications for Epidemiological Studies: Role of Anthropometrics, Sleep Habit, and Comorbidities
Authors Appleton SL ![]() , Reynolds AC, Gill TK
, Reynolds AC, Gill TK ![]() , Melaku YA
, Melaku YA ![]() , Adams RJ
, Adams RJ ![]()
Received 21 January 2022
Accepted for publication 6 April 2022
Published 21 April 2022 Volume 2022:14 Pages 775—790
DOI https://doi.org/10.2147/NSS.S359437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Sarah L Appleton,1,2 Amy C Reynolds,1 Tiffany K Gill,2 Yohannes Adama Melaku,1 Robert J Adams1
1Flinders Health and Medical Research Institute – Sleep Health (Adelaide Institute for Sleep Health), College of Medicine and Public Health, Flinders University, Adelaide, SA, Australia; 2The Adelaide Medical School, University of Adelaide, Adelaide, SA, Australia
Correspondence: Sarah L Appleton, Flinders Health and Medical Research Institute -Sleep Health (Adelaide Institute for Sleep Health), College of Medicine and Public Health, Flinders University, Mark Oliphant Building, L2, 5 Laffer Drive, Bedford Park, Adelaide, 5042, SA, Australia, Tel +61 8 74219755, Email [email protected]
Introduction: Estimating insomnia prevalence in epidemiological studies is hampered by variability in definitions and interpretation of criteria. We addressed the absence of a population-based estimate of insomnia in Australia using the widely accepted contemporary International Classification of Sleep Disorders (ICSD-3) criteria, which includes sleep opportunity, and has not been applied in studies to date. Consistent use of these criteria across epidemiological studies, however, requires evidence of the clinical utility of a sleep opportunity criterion for targeting strategies.
Methods: A cross-sectional national on-line survey (2019 Sleep Health Foundation Insomnia Survey) of Australian adults (18– 90 years, n = 2044) was conducted. Chronic insomnia was defined as sleep symptoms and daytime impairment experienced ≥ 3 times per week, and present for ≥ 3 months, with adequate sleep opportunity (time in bed (TIB) ≥ 7.5 hrs). Self-rated general health (SF-1) and ever diagnosed health conditions (including sleep disorders) were assessed.
Results: Chronic difficulties initiating and maintaining sleep and daytime symptoms (n = 788) were more common in females (41.5%) than males (35.3%), p = 0.004. Excluding participants reporting frequent pain causing sleep disruption and TIB < 7.5 hrs generated an insomnia disorder estimate of 25.2% (95% CI: 22.5– 28.2) in females and 21.1% (18.4– 23.9) in males [23.2% (21.2– 25.2) overall]. This compares with 8.6% (7.3– 10.0) with insomnia symptoms and TIB < 7.5 hrs and 7.5% (6.4– 8.7%) ever diagnosed with insomnia. Insomnia symptom groups with TIB < 7.5 and ≥ 7.5 hours demonstrated similar odds of reporting fair/poor health [odds ratio (OR): 3.2 (95% CI: 2.1– 4.8) and 2.9 (95% CI: 2.2– 3.9) respectively], ≥ 1 mental health condition, ≥ 1 airway disease, and multimorbidity.
Conclusion: Adults with significant sleep and daytime symptomatology and TIB < 7.5 hrs did not differ clinically from those with insomnia disorder. Consideration of criteria, particularly adequate sleep opportunity, is required to consistently identify insomnia, and establish health correlates in future epidemiological studies. Further evaluation of the clinical utility of the sleep opportunity criterion is also required.
Keywords: insomnia, sex, epidemiology, population
Introduction
Insomnia contributes to a considerable burden of physical and mental health problems,1 including cardiovascular disease,2,3 and chronic pain.4 Insomnia is highly co-morbid with a number of psychiatric diseases, and increases the risk of incident major depressive disorder.5 Insomnia also predicts earlier retirement6 and accidents.7 Some, but not all, studies identify an association with mortality.8 Increased investment in surveillance for insomnia is clearly warranted, given that 14% of good sleepers were shown to be at risk of developing insomnia over five years.9 A one-year incidence rate of acute insomnia of 27.0% was reported by Perlis et al, and while most recovered good sleep, 7% developed chronic insomnia and 19% developed persistent poor sleep, neither remitting to normal sleep nor progressing to chronic insomnia disorder.10
However, determining the prevalence of chronic insomnia in population studies for the development of targeted preventative strategies is challenging due to variations in definitions employed, ie night-time symptoms, with or without daytime impairment, dissatisfaction with sleep, adequate opportunity to sleep, and chronicity of symptoms. This contributes to the substantial variation in prevalence estimates in population studies. For example, large health surveys in the USA and Canada from 2011 to 2015 have reported the prevalence of “trouble going to sleep or staying asleep most/all of the time”, ranging from 17.1%11 to 25.3%12 with significant increases over earlier estimates. In the America Insomnia Survey, insomnia prevalence rates of 22.1% and 14.7% as defined by the DSM-IV and ICSD-2 criteria, respectively, were found,13 and similar findings have been reported from Hong Kong.14 The DSM- IV defined insomnia prevalence varies across European countries15 ranging from 6% in Spain16 to 19.0% in France,17 with evidence the insomnia prevalence has increased over time.18
Few epidemiological studies globally have defined insomnia by contemporary criteria. Chronic insomnia is defined in the ICSD-319 and endorsed by the European Sleep Research Society for diagnostic purposes15 as difficulties initiating or maintaining sleep (DIMS) causing impairment in social, occupational, educational, academic, behavioural, or other important areas of functioning. These symptoms should occur three or more times per week for more than three months with adequate opportunity and circumstances to sleep. In a recent Norwegian population study, 25% of females and 15% of males fulfilled the ICSD-3 criteria for chronic insomnia, when two possible daytime impairments (including tiredness or sleepiness affecting work or private life), and dissatisfaction with sleep were considered.20 Similarly, a French survey of adults estimated the prevalence according to ICSD-3/DSM-5 at 23% in females and 13% in males.21 In 22-year-old participants of The Western Australian Pregnancy (Raine) Study, DSM-5 chronic insomnia was estimated at 19.3% of females and 10.6% of males.22 Of note, none of these studies considered the adequacy of sleep opportunity criterion. A standardised approach to assessing insomnia disorder in epidemiological studies with contemporary criteria to potentially improve consistency across studies requires application of a sleep opportunity criterion to determine if it has clinical utility for targeting strategies.
The aim of this study was to address the limited Australian population-level data on insomnia symptoms and insomnia disorder according to current ICSD-3 diagnostic criteria, including perceived adequate sleep opportunity. Given the lack of evaluation of the sleep opportunity criterion in existing epidemiological studies, we also aimed to determine its clinical utility and whether application of a sleep opportunity criterion identifies a more severe insomnia phenotype. Specifically, we sought to determine if sleep opportunity, interpreted as time in bed of 7.5 hours, differentiated chronic insomnia symptom groups in terms of the level of sleep difficulties and underlying contributors to sleep initiation and maintenance difficulties, and chronic disease conditions and risk factors.
Methods
Survey Methodology
We undertook a cross-sectional web-based survey of adult Australians. The survey could be completed using a smartphone, tablet device or computer. The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) for the survey has been previously published.23 Participants aged ≥18 years (n = 2044) were recruited by Dynata from an online panel of over 500,000 registered survey takers, in March and April 2019. Sampling was performed to match Australian Bureau of Statistics estimates on key indicators including age, sex, state and regional representation.
As members of the survey panel, all participants have provided informed consent to participate in online surveys. Participants were informed on the survey welcome page that the survey concerned sleep and health issues, the completion time was approximately 20–25 minutes, that all responses will be confidential and anonymous, and all reporting occurs on an aggregate level only. Consent was indicated when respondents clicked the “Go to Survey” button on the welcome page. The study was conducted in accordance with the Declaration of Helsinki. The University of Adelaide Office of Research Ethics, Compliance and Integrity (H-2018-214) approved the survey methodology.
A three-stage randomization process during recruitment was used to minimize the risk of bias.24 Specific project details are not included in the invitation to “take a survey” to avoid self-selection bias. Invitations for participants include emails, banners, messaging and text alerts. Invitation text varies between respondents, reducing the potential for language to bias participation. A set of profiling questions are randomly selected for completion (these are not affirmation questions). Participants are then matched to suitable surveys. Details of the study were disclosed only when the survey had been selected within the system. The study sample matched the 2016 Australian Census data on key indicators including age, sex, location and socio-economic status as previously described.23 The survey was created by the authors to ascertain the frequency and chronicity of insomnia symptoms in line with the ICSD-3 definition. Further questions were derived from a number of sources including the United States National Sleep Foundation’s 2002 Sleep in Adults survey25 and previous Australian Sleep Health Foundation surveys.24,26 Survey respondents were included in the analysis irrespective of work status/shift schedule, and a more detailed consideration of insomnia symptoms in shift workers from this sample has been previously reported.27
Sociodemographic Variables
Standard items were assessed including financial stress (assessing a participant’s family money situation and ability to save), location of residence (metropolitan/regional), and main language spoken at home.
Health Status
Self-rated health was assessed with question 1 from the SF-36- “In general, would you say your health is?” Responses were categorised as excellent/very good/good, or fair/poor (SF-1).
Common doctor diagnosed medical conditions were determined including heart disease; diabetes; high blood pressure (or ≥1 cardiometabolic disorder); depression or bi-polar disease; anxiety or panic disorder; post-traumatic stress disorder (or ≥1 mental health disorder); asthma; nasal obstruction/hay fever/rhinitis; other lung disease, eg COPD, (or ≥1 airway disease); arthritis; gout; heartburn or reflux disease; prostate disease/bladder problems. Multi-morbidity was also defined as two or more medical conditions. Body mass index (BMI; kg/m2) was calculated from self-reported height and weight. Current smoking was assessed as never, some days, every day.
Sleep Opportunity
Subjective assessment of sleep opportunity (“Does your current work schedule or typical weekday routine, including your duties at home, allow you to get enough sleep?”) and sleep quantity/quality (“In the past month, felt you got adequate or satisfactory sleep”) was made. We also determined if pain caused sleep disturbance by asking how often pain 1) “stops you from going to sleep at night” or 2) “wakes you up at night”.
We assessed the time in bed (TIB) on weekdays (difference between “At what time do you usually go to bed on nights before workdays or weekdays?” and “At what time do you usually get up on days you work or on weekdays?”). Week/workday and weekend/non-workday sleep duration was assessed with “how many hours, not including naps, do you usually sleep during one night?”
Insomnia Symptoms and Disorder
Difficulties initiating or maintaining sleep (DIMS) were determined as the frequencies of “difficulty falling asleep”, “waking a lot during the night”, and “waking up too early and not able to get back to sleep” occurring at least three nights per week in the past month. Chronic DIMS were those reported for at least 3 months. Acute DIMS were DIMS that were present either “less than one month”, or “at least one month, but less than 3 months”.
Sleep disturbances causing clinically significant daytime distress or impairment occurring three or more times per week were identified by the following questions: “In the past month how often have you experienced these daytime feelings? - 1) Sleepiness that interfered with daily activities; 2) Felt sleepy sitting quietly day/early evening; 3) Fatigue/exhaustion; 4) Irritable/moody; 5) Reduced motivation/energy; 6) Reduced concentration, attention, memory; 7) Hyperactive, impulsive, aggressive; 8) Had little interest/pleasure in doing things; 9) Felt down, depressed, hopeless. Chronic daytime symptoms were those reported as being present for at least 3 months. Impairment in occupational function was determined if participants made errors at work on 1–2 days or more in the past 3 months “because you were too sleepy or you had a sleep problem?”
Insomnia disorder was classified using ICSD-3 criteria, requiring chronic DIMs and daytime impairments (described above), in those with adequate sleep opportunity defined in this study as a self-report of spending ≥7.5 hours TIB on nights before workdays/weekdays. This quantitative measure was chosen which allows for 30 minutes awake and 7 hours sleep, the minimum recommended by the National Sleep Foundation.28 TIB data were missing in 38 participants with chronic insomnia symptoms.
Diagnosed Sleep Disorders and Symptoms
We determined ever-diagnosed insomnia, obstructive sleep apnea and restless legs/periodic leg movements of sleep and symptoms by self-report.29 The frequency of daytime napping and the use of sleep medication prescribed by a doctor (eg temazepam, valium) over the past 12 months was also determined.
Statistical Analysis
All analyses were conducted using IBM SPSS version 25.0 (IBM Corporation, Armonk, NY, USA). The primary intent of this analysis was to establish differences in the prevalence of insomnia (95% CI) by sex and age. The sample was stratified based on age 55 as this was the average retirement age of all retirees in Australia (2018–19) according to the Australian Bureau of Statistics.30 Difference in prevalence estimates was determined as detected when there was no overlap of 95% CI. One-way ANOVA determined differences in BMI, and age across all sleeper categories.
The following analyses of insomnia symptoms, sleep disorders, and health conditions were conducted in the participants free of pain that caused frequent sleep disruption. Pearson χ2 statistics determined differences in distributions of 1) insomnia sleep and daytime symptoms, 2) sleep disorders (diagnosed and symptoms) and sleep factors, and 3) health status and ever diagnosed conditions, between those with chronic insomnia symptoms who did and did not meet TIB criterion. Additionally, χ2 statistics determined differences in distributions of 1) sleep disorders (diagnosed and symptoms) and sleep factors across all three chronic DIMS groups, and 2) health status and ever diagnosed conditions across all sleep categories.
Binary logistic regression analyses determined adjusted associations of insomnia status with outcomes (health status, chronic conditions, and sleep disorder symptoms) for age, sex, current smoking and BMI with the following exceptions: napping and restless leg symptoms (age, sex and BMI adjusted), obesity (age, sex, and smoking adjusted), and current smoking (age and sex adjusted).
Results
Sample Characteristics
The sample of 2044 adults were closely matched with the Australian population as per our previous estimates in 201624 with regard to age, sex, income, and geographic location across states and metropolitan and rural locations (Supplementary Table 1). The sample had a higher proportion with tertiary-level education than population estimates, and females were more common in younger age groups, while males were more common in older age groups.
Sleep Duration and Opportunity
Females overall, and particularly at age 25–44, reported that their routine allows enough sleep (all/most of the time) less frequently than males, however 78% of both males and females reported at least 7.5 hours TIB (Table 1). Mean self-reported sleep duration on work/weekdays was not significantly different by sex, but mean sleep duration on non-working days was 21 minutes higher on average in females. Mean sleep duration (weekdays and weekends) significantly decreased with increasing age up to age 55–64, after which it increased in adults aged ≥65 years (Supplementary Figure 1). Work/weekday TIB of ≥7.5 hr showed a similar pattern across age groups.
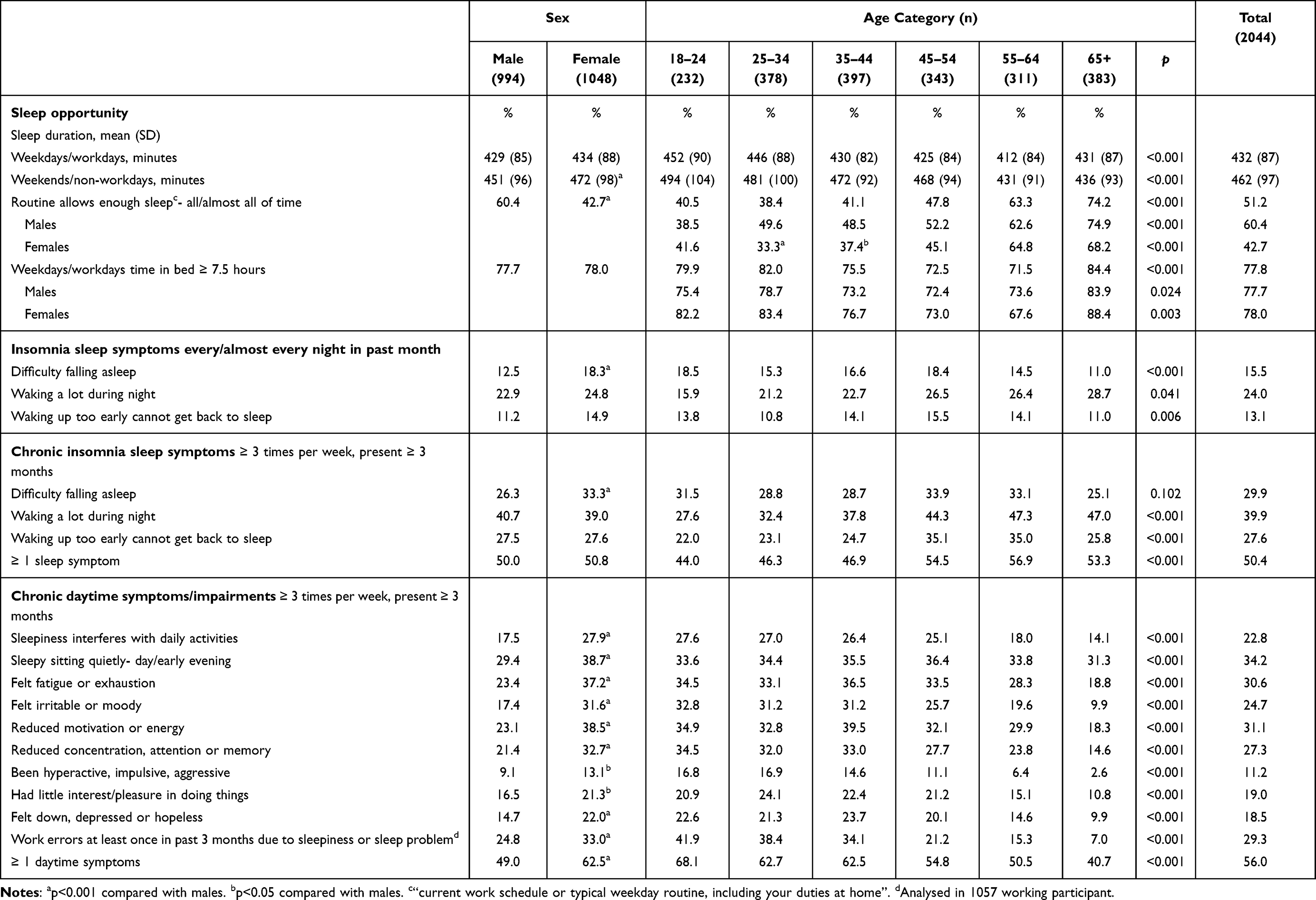 |
Table 1 Sleep Opportunity, Chronic Insomnia Sleep and Daytime Symptoms (%) by Sex and Age |
Insomnia Symptom Prevalence
At least one chronic DIMS was reported by 50.4% and significantly increased across age groups (Table 1). Waking at night was more common in participants aged ≥65 years than in those aged 18–24 y (47.0% versus 27.6%, p < 0.001). Difficulties falling asleep were significantly more common in females. Chronic symptoms of daytime dysfunction were significantly more frequent in females and decreased in prevalence with increasing age (Table 1). Chronic sleep and daytime symptoms (38.6%, n = 788) were more frequent in females than males (41.5% versus 35.3%, p = 0.004).
Insomnia Disorder Prevalence
Frequent pain that caused sleep disturbance was reported by 14.0% of participants (n = 286). Given the criterion that insomnia symptoms should not be caused by a pain condition, we excluded these participants from prevalence estimates, leaving 1758 participants to estimate insomnia prevalence. Chronic DIMS and daytime symptoms were reported in 575 (32.7%) of these participants, and TIB data were available in 551 participants, with 73% reporting TIB ≥ 7.5 hrs. This resulted in an insomnia disorder prevalence of 23.2% (21.2–25.2%), leaving 8.6% (95% CI: 7.3–10.0%) with chronic symptoms of insomnia with inadequate sleep opportunity (Table 2). Although not significantly so, insomnia disorder was more common in females than males overall (25.2% versus 21.1%), in those aged <55 years (26.4% versus 19.7%) and in younger compared to older females (26.4% versus 17.9%). In both males and females, acute DIMS (9.5% overall) were significantly more common in younger compared to older participants (Table 2).
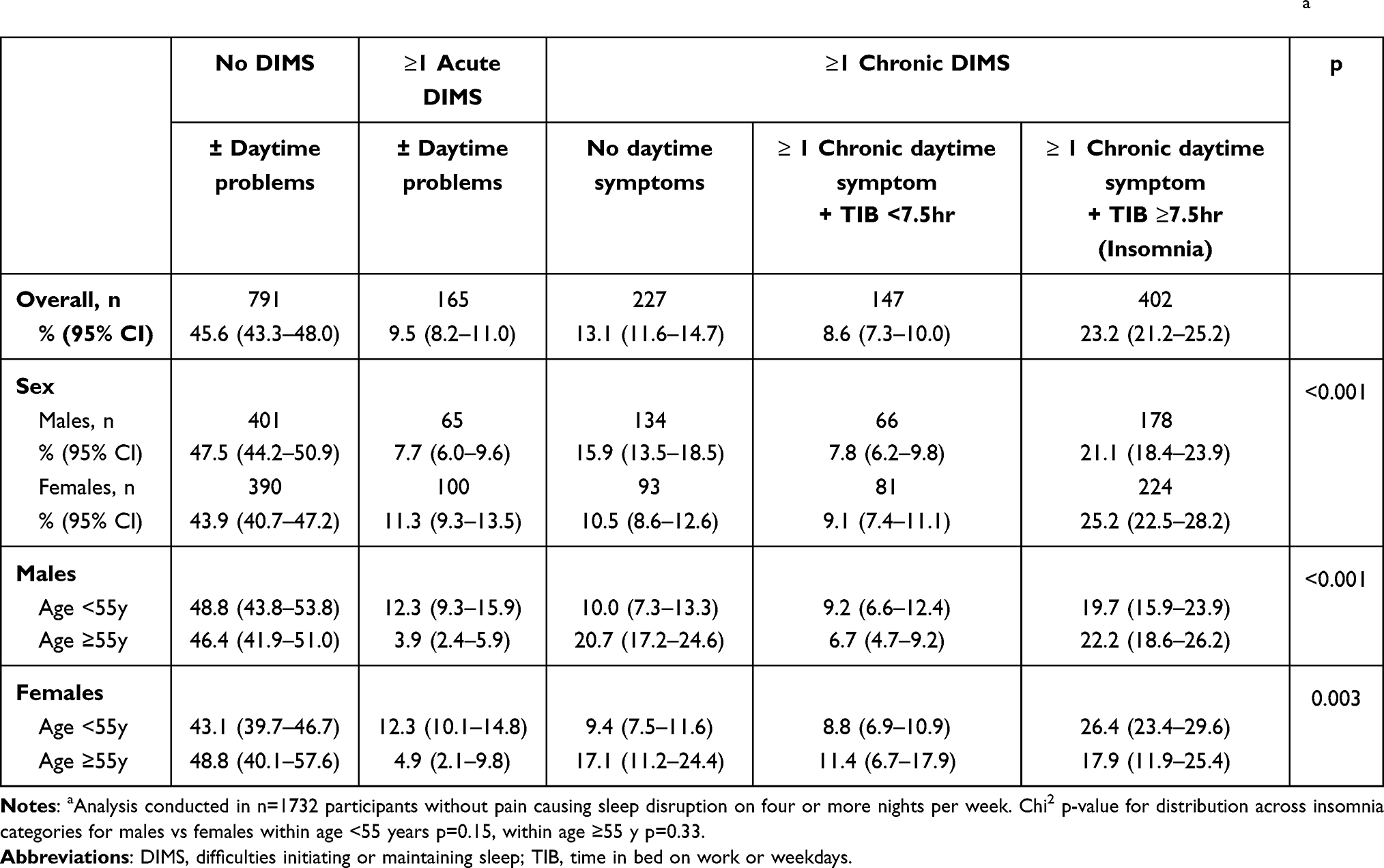 |
Table 2 Prevalence of Insomnia Symptoms [% (95% CI)] by Sex, Age in Participants Without Pain Causing Sleep Disruptiona |
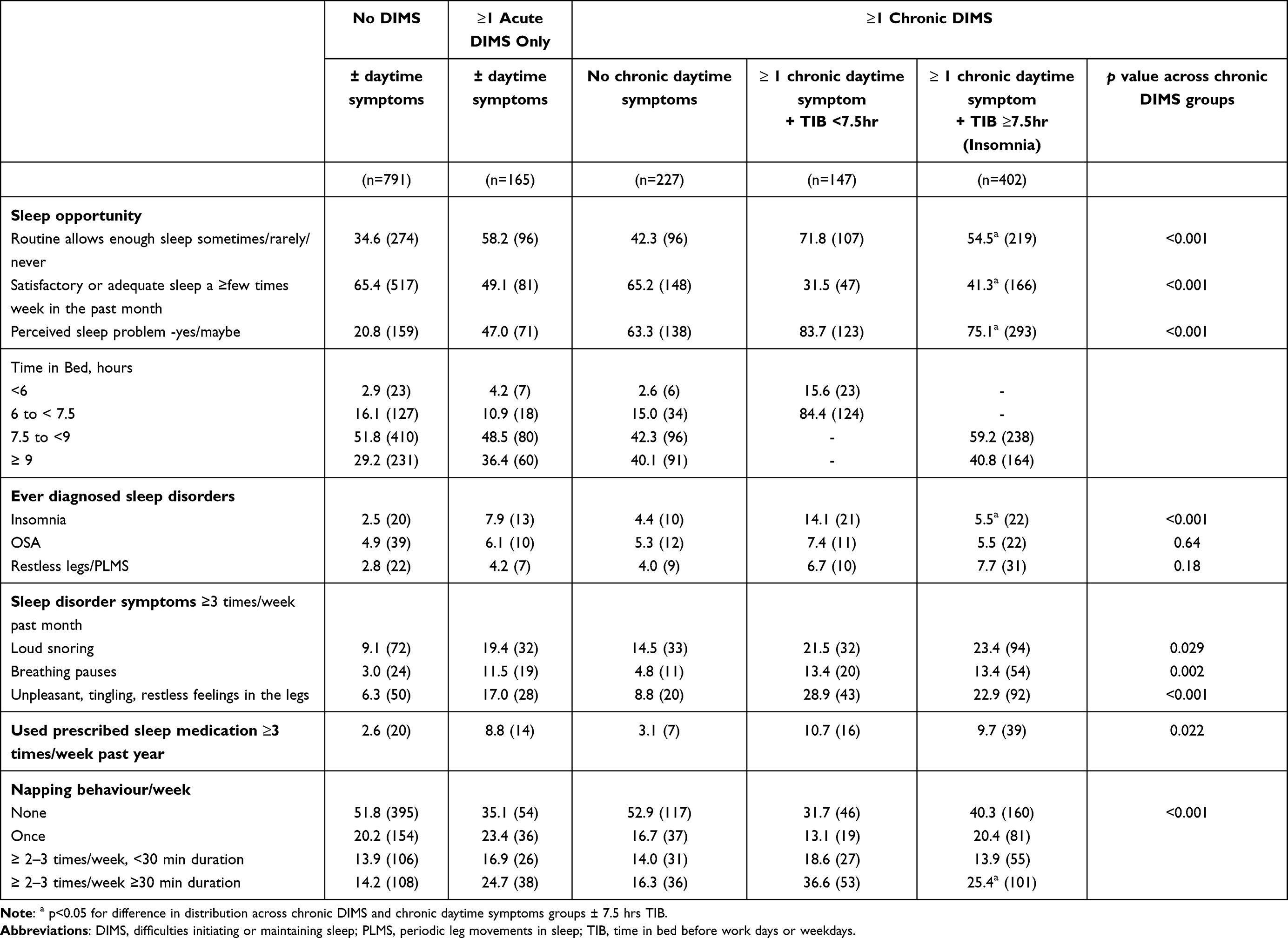 |
Table 3 Sleep Opportunity and Sleep Disorders/Symptoms [% (N)] with Possible Influence on Sleep Difficulties and Daytime Symptoms |
Participant perceptions of sleep adequacy further influenced the insomnia prevalence in our sample. When insomnia disorder was limited to those reporting they got adequate or satisfactory sleep less than a few nights/week, the prevalence of insomnia was reduced to 13.6% (95% CI:12.1–15.3) [n = 236; females: 15.7% (13.4–18.2); males: 11.5% (9.5–13.8)]. Surprisingly, of the participants reporting chronic insomnia symptoms and TIB <7.5 hours, 31.5% reported getting adequate or satisfactory sleep at least few times per week (Table 3), while 8.7% reported this “every or almost every night”.
As shown in Supplementary Table 2, insomnia disorder prevalence [27.3% (95% CI: 25.4–29.3%)] in the sample, when participants reporting pain causing sleep disruption were retained, was significantly more common in females than males overall (30.0% versus 24.5%) and in younger participants (30.6% versus 23.0%).
The remaining study results are reported from the sample free of pain frequently causing sleep disruption as described in the methods.
Influence of Sleep Opportunity (Time in Bed) on Insomnia Symptom, Sleep and Health Correlates in Those With Chronic Insomnia Symptoms
Insomnia Sleep and Daytime Symptom Characteristics
In participants free of pain causing sleep disruption, a median of 2 chronic DIMS and 4 chronic daytime symptoms were seen in those with chronic insomnia symptoms with or without TIB ≥7.5 hrs (Table 4). However, work errors were significantly more common in participants with insomnia disorder (47.8%). The most frequent sleep and daytime symptoms were, respectively, waking a lot during the night, and feeling sleepy while sitting quietly during the day or early evening.
 |
Table 4 Prevalence of Chronic Sleep Difficulties and Chronic Daytime Symptoms [% (n)] in Relation to Insomnia Status |
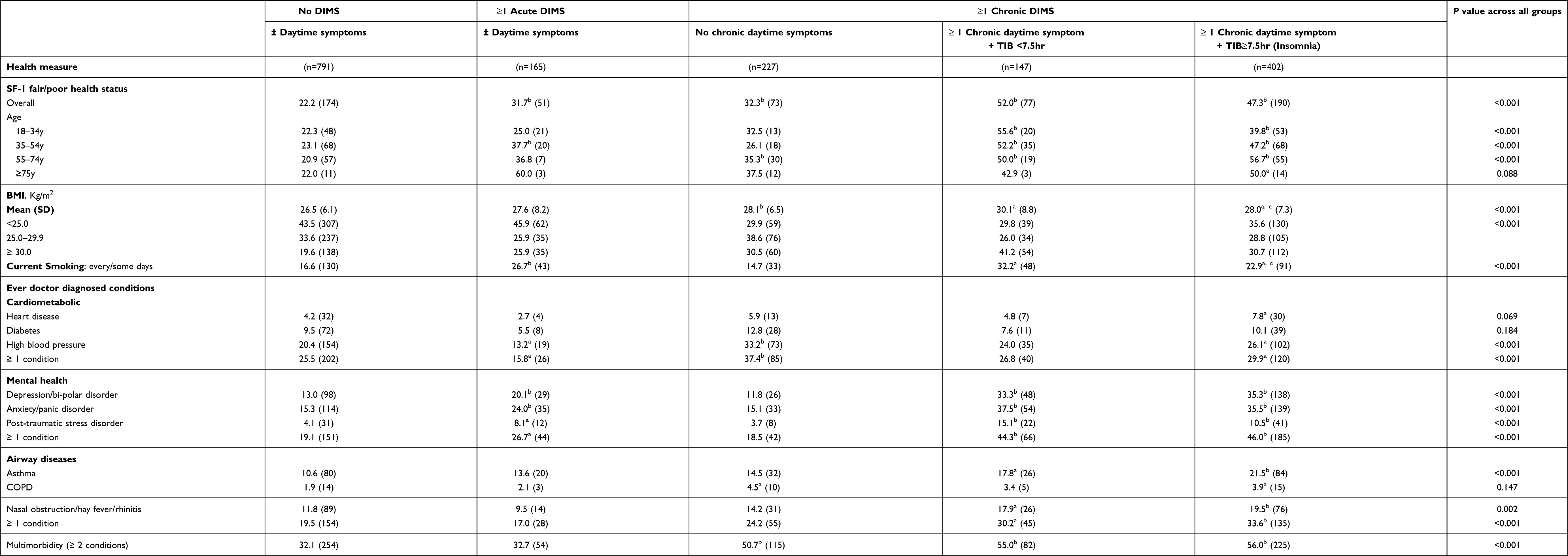 |
Table 5 Health Status [% (N)] and Ever Diagnosed Health Conditions [% (N)] in Relation to Insomnia Status |
Sleep Disorders and Sleep Factors That May Contribute to Difficulties Sleeping and Daytime Symptoms
Ever diagnosed insomnia was significantly more prevalent in participants with chronic insomnia symptoms not meeting the TIB criterion (14.1% versus 5.5%, Table 3). Ever-diagnosed OSA and restless legs showed little variation across chronic DIMS categories, however symptoms of these disorders were significantly more frequent in those with chronic daytime symptoms. Consistent with a restricted sleep opportunity, participants with insomnia symptoms spending <7.5 hrs TIB reported significantly higher prevalence rates of a routine infrequently permitting enough sleep (71.8% versus 54.5%) and napping at least 2–3 times per week (55.2% versus 39.3%), and were less likely to report getting satisfactory or adequate sleep a few times per week or more than those reporting TIB ≥7.5 hours. However, frequent prescribed sleep medication use (a few times/week or more in the past year) was uncommon but highest in the chronic insomnia symptom groups (~10%).
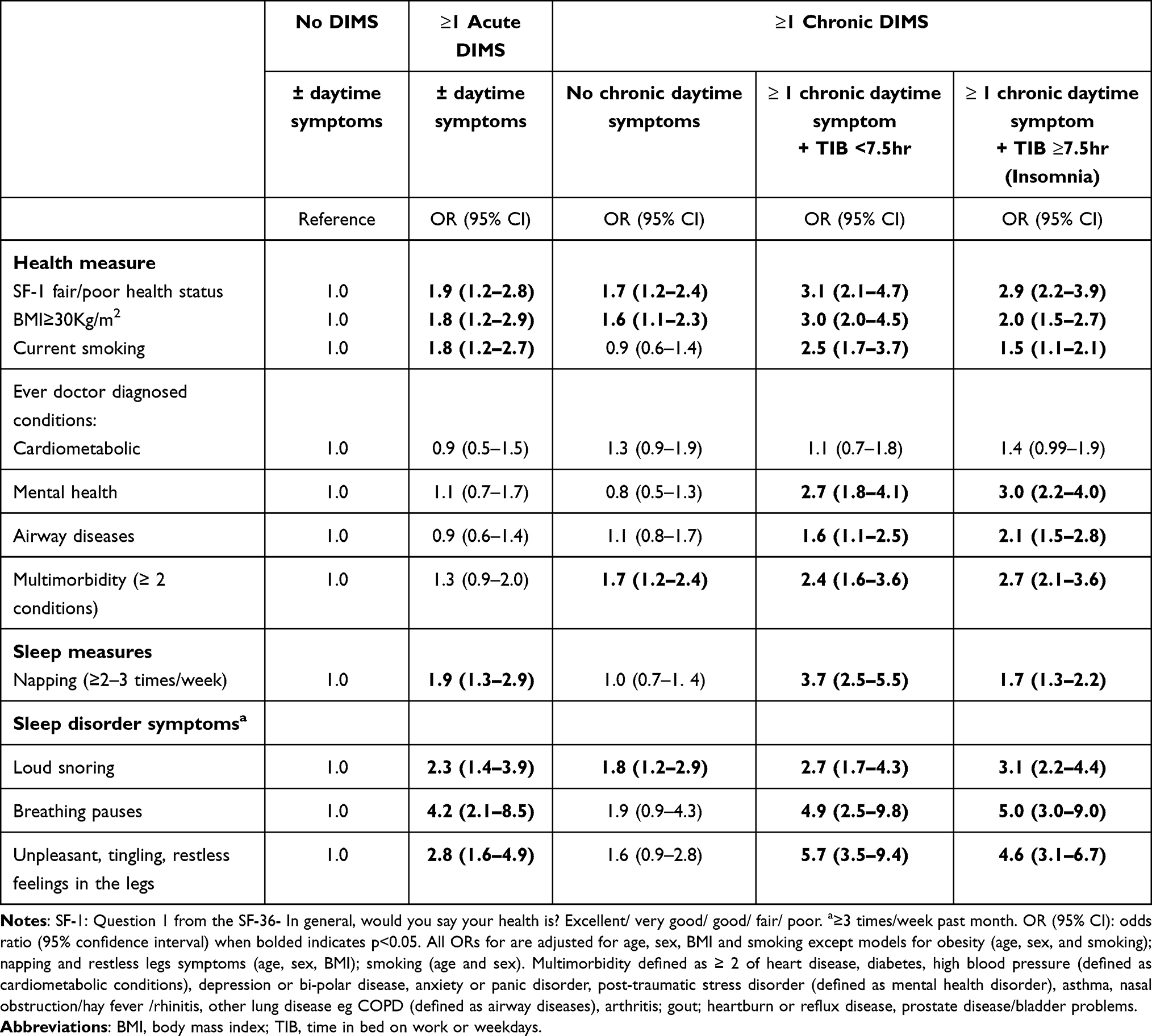 |
Table 6 Logistic Regression Analyses of Likelihood of Health Conditions, Chronic Disease Risk Factors and Sleep Disorder Symptoms [or (95% CI)] Associated with Insomnia Status |
Insomnia and Health Status
Compared to good sleepers (no DIMS), both chronic insomnia symptom groups (irrespective of TIB) significantly more frequently reported poor/fair health on the SF-1 and demonstrated higher rates of current smoking, obesity, and the presence of ≥1 diagnosed mental health condition, and ≥1 diagnosed airway disease, and multimorbidity (Table 5). In those with chronic insomnia symptoms, the prevalence of poor/fair health (~50%) did not significantly differ by TIB, overall, or across age groups. Similarly, ever-diagnosed chronic conditions were not different by TIB category; however, obesity and smoking were significantly more frequent in those with TIB <7.5 hrs (Table 5).
As shown in Table 6, compared to good sleepers (no DIMS), insomnia symptom groups (irrespective of TIB) showed significant adjusted associations with poor/fair health, obesity, smoking, diagnosed mental health conditions, and airway diseases. Participants with chronic DIMS only, in contrast, demonstrated significant adjusted associations limited to poor/fair health, obesity and multimorbidity, while those with acute DIMS showed adjusted associations with poor/fair health and chronic disease risk factors including obesity and current smoking. The univariate association of insomnia disorder with reporting one or more cardiometabolic conditions was attenuated after adjustment for confounders.
In age and sex adjusted analyses, napping at least 2–3 times per week, and frequent (at least a few times per week) restless leg symptoms and apneas were significantly associated with the presence of acute symptoms, chronic insomnia symptoms and TIB <7.5 hours, and insomnia disorder. Snoring, however, was significantly more likely in all symptom groups, including those with chronic DIMS but without daytime dysfunction (Table 6).
Socio-Demographics Correlates of Insomnia
Compared to good sleepers (reporting no DIMS), insomnia disorder was more frequent in participants from households speaking English as the primary language and experiencing financial stress, and in participants with intermediate levels of education, and less likely in participants born overseas and engaged in full-time work (Supplementary Table 3). Acute DIMS were significantly more common in females and younger adults. No significant differences in the distribution of demographic variables were observed between the chronic insomnia symptom groups stratified by TIB.
Discussion
In the first Australian study to use contemporary ICSD-3 criteria for its classification, chronic insomnia was common with overall estimates of 23.3% in those reporting adequate opportunity to sleep and without pain frequently causing sleep disturbance. Overall, and in participants aged <55y, insomnia prevalence was higher in females than males. Chronic insomnia symptoms in participants reporting time in bed less than 7.5 hours (inadequate sleep opportunity) were reported by an additional 8.6% of the sample, while chronic DIMS without daytime impairment occurred in 13%. This chronic insomnia symptom burden contrasts with the 7.5% of participants reporting a previous diagnosis of insomnia. Importantly, the chronic insomnia symptom groups demonstrated a significant burden of impaired health that did not vary with opportunity to sleep criterion (7.5 hrs TIB).
A chronic insomnia prevalence of 15% (19% in females and 11% in males) in 22-year-old Australians has been recently reported based on DSM-5 criteria, although notably without consideration of sleep opportunity.22 Not surprisingly, our findings vary significantly from an estimate of severe insomnia in another Australian study using sleep difficulties plus daytime impairment, which reported a prevalence of 8.7% in females and 5% in males.26 However, severe insomnia symptoms (“trouble going to sleep or staying asleep?” experienced most or all of the time) have been frequently reported (17–25%) in large North American studies.11,12 We observed similar rates of sleep initiation (15.5%) and maintenance difficulties (13.1–24%) experienced every/almost every night. However, we found that the frequency of at least one sleep symptoms increased with age, but older people were less likely to report daytime impairments (possibly reflecting more autonomy regarding sleep timing, with less social and occupational constraints than younger people or under-reporting of complaints) which is likely to have accounted for the relative decrease in insomnia prevalence with age. This is consistent with the mean age of participants reporting chronic DIMS only (comprising 8.6% of the sample) being the highest of all symptom groups (mean 53 years, and 52% were aged 55 or more). Similarly, Boyle et al recently demonstrated discordance of sleep insomnia severity (total time awake) and daytime dysfunction based on median splits of these variables, with a prevalence of 13% and this group was older than other concordant and discordant groups. The contribution of sleep need was proposed such that “those who need a little, may suffer only a little, in the face of a lot”.31
Other international studies have also reported high rates of insomnia that varied by use of criteria as evidenced by 22.1% (DSM-IV) and 14.7% (ICSD-2, including sleep opportunity) in the United States (n = 10,094).13 In Europe, the DSM-IV insomnia prevalence varies15 from 6%16 to 19.0%.17 Sivertsen et al also reported ICSD-3 prevalence rates of 25% in females and 15% in males, however daytime symptoms assessed were limited, and sleep opportunity was not included.20 Further consideration at a population level in both developing and developed countries is required to clarify whether these findings differ by country.
Our work extends these studies by assessing a range of other health and sleep conditions and considering the interpretation of insomnia criteria. Prior population-based studies have not done this, nor have studies attempted to address sleep opportunity in association with ICSD-3 criteria. In the context of epidemiological studies, insomnia criteria may be open to interpretation, difficult to precisely define and may be explained by other conditions and thus be subject to influence by contextual, cultural, and social factors.
Consistent with studies of insomnia variously defined,1,4,5,32 we found participants with chronic DIMS demonstrated associations with multi-morbidity in adjusted models. Around half of those reporting chronic insomnia symptoms irrespective of the TIB criterion demonstrated poor health status and ever diagnosed chronic conditions (mental health and airway disorders). The contribution of these chronic conditions, as well as sleep disorders (including restless legs syndrome and OSA) to sleep disturbance cannot be excluded, particularly nocturnal airway disease symptoms including dyspnea33 and allergic rhinitis34 and asthma35 Similarly, mental disorders have been shown to be highly comorbid with insomnia.5,36 The bidirectional associations of mental disorders and insomnia have implications for management.5,37 For this reason, we considered mental health conditions (and other sleep disorders38) comorbid with insomnia.
The distinction between insomnia with and without 7.5 h TIB (indicative of “adequate opportunity”) is interesting. Specifically, while “adequate opportunity” is a component of the diagnostic criteria, this did not necessarily present a different phenotype of insomnia disorder than those who have insomnia symptoms but inadequate sleep opportunity. Although only “insomnia disorder” was associated with work errors, the chronic symptom group with TIB <7.5 hours reported significantly higher rates of current smoking and BMI that may expose this group to additional health risk in the future. We considered adequate opportunity to sleep based upon self-reported time in bed of 7.5 hours or more. This is within the National Sleep Foundation recommended range of sleep,28 and is higher than the threshold used to ascertain non-restorative sleep, requiring a report of feeling at least moderately unrefreshed and there being at least 7 hours sleep (adequate opportunity) in the Brief Insomnia Questionnaire for DSM-IV-TR insomnia.39 Outside of a clinic setting, subjective assessment of adequate sleep opportunity is difficult, and in the broader population, perceptions, and beliefs regarding adequate sleep and sleep health literacy may be problematic. This is illustrated by the reduction in insomnia disorder prevalence to 13.6% when we made a complaint of infrequent satisfactory or adequate sleep, a criterion for classification of insomnia disorder, suggesting that the level of perceived bother from, or acceptance of, significant sleep and daytime impairments is lower than would be anticipated.
We also observed that 25% of those with insomnia disorder did not perceive that they had a sleep problem and in contrast, despite having by definition, at least 7.5 hours TIB on weekdays or before work days, only 45% believed their routine/schedule permits them to get enough sleep all/most of the time. However, given the poor health status in those with chronic insomnia symptoms not meeting our TIB in criterion, we speculate that from an epidemiological/surveillance perspective, the application of a sleep opportunity criterion (focussed on identifying insomnia disorder) may limit opportunities for important health promotion activities in this group, as by definition, DIMS in participants with a reduced sleep opportunity may lead to unhealthy levels of sleep and impart increased risks of future morbidity as supported by previous work.40 On the other hand, the highest rates of daytime napping occurred in participants with chronic insomnia symptoms and TIB <7.5hrs. While intuitive, and the direction of the relationship is unknown, frequent, long napping may reduce sleep drive leading to additional sleep disturbance, suggesting sleep hygiene or habit may be a problem requiring attention, rather than a behavioural approach using sleep restriction as would be recommended in cognitive behavioural therapy for insomnia (CBTi). Therefore, our findings suggest that a standardised sleep opportunity criterion, based on time in bed rather than a subjective measure based on perceptions or skewed beliefs, may enable the identification and targeting of those with significant sleep and daytime impairment but reduced sleep opportunity for health promotion and sleep health literacy strategies. Many of these measures already exist in standard sleep questionnaires, meaning additional detail does not have to equate to additional burdens or time demands in future studies of sleep for participants. However, further evaluation consideration of the time in bed-based criterion will be beneficial for the field, to be used consistently.
The strengths of the study included a sample that matched the Australian adult population on key indicators and the use of items that provided a close approximation of the inclusion criteria for insomnia disorder according to the ICSD‐3, including a detailed list of possible daytime impairments. Study limitations included reliance on self-reported data, and no clinician-verified information was available. The sample included a higher proportion with post-school qualifications than population census estimates, with more females and males in younger and older age groups, respectively, which should be considered when comparing our findings with other population studies. The on-line nature of the survey excludes people without access to the technology; however, internet access is almost universal with approximately 27.0 million mobile handset subscribers and an additional 14.7 million broadband internet subscribers (households) in the population of 25.7 million (2019).41
Conclusion
We have demonstrated that the prevalence of insomnia disorder in our population-based on-line survey varied when sleep opportunity, and pain causing sleep disturbance were considered. Considering time in bed to determine adequate opportunity did not differentiate between chronic insomnia symptom groups as both groups demonstrated significantly increased odds of reporting poor health status and multiple health conditions that require clinical attention. Future longitudinal epidemiological studies should aim for consistency in the definition of insomnia to adequately quantify changes in prevalence and predictors over time. The ICSD-3 criteria generally match the clinical issues and symptoms of insomnia, with consideration of a wide range of daytime impairments and chronicity. A measure of sleep opportunity based on time in bed rather than perceived sleep opportunity may facilitate the accurate identification of at-risk symptomatic subgroups in the population and the provision of applicable public health messages and recommendations relating to insomnia and sleep hygiene in the community.
Abbreviations
DIMS, difficulty initiating or maintaining sleep; DSM, Diagnostic and Statistical Manual of Mental Disorders; ICSD, International Classification of Sleep Disorders; TIB, time in bed.
Data Access
Data may be available upon reasonable request to the corresponding author.
Funding
The online survey was funded by the not-for-profit Australian Sleep Health Foundation, using an unrestricted grant from Merck, Sharp & Dohme (MSD Australia) Pty Limited, awarded to RJA, SLA, TKG and ACR. MSD Australia played no role in the study design, the collection, analysis and interpretation of data, the writing of the report, or the decision to submit the article for publication.
Disclosure
Dr Sarah Appleton reports grants from Sleep Health Foundation, during the conduct of the study. Dr Amy C Reynolds reports grants from Sleep Health Foundation/Merck Sharp and Dohme, during the conduct of the study; personal fees from Sealy Australia and Teva Pharmaceuticals; completing work for Compumedics, outside the submitted work. Dr Tiffany K Gill reports grants from Sleep Health Foundation, during the conduct of the study; grants from Arthritis Australia and The Hospital Research Foundation, outside the submitted work. Dr Yohannes Adama Melaku has nothing to disclose. Professor Robert J Adams reports grants from Sleep Health Foundation, during the conduct of the study; grants from Philips, The National Health and Medical Research Council, ResMed Foundation, and The Hospital Research Foundation, outside the submitted work.
References
1. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1(1):15026. doi:10.1038/nrdp.2015.26
2. Li Y, Zhang X, Winkelman JW, et al. Association between insomnia symptoms and mortality: a prospective study of us men. Circulation. 2014;129(7):737–746. doi:10.1161/CIRCULATIONAHA.113.004500
3. Zheng B, Yu C, Lv J, et al. Insomnia symptoms and risk of cardiovascular diseases among 0.5 million adults. A 10-year cohort. Neurology. 2019;93(23):e2110–e2120. doi:10.1212/WNL.0000000000008581
4. Skarpsno ES, Mork PJ, Hagen K, Nilsen TIL, Marcuzzi A. Number of Chronic nighttime insomnia symptoms and risk of chronic widespread pain and pain-related disability: the HUNT study. Nat Sci Sleep. 2020;12:1227–1236. doi:10.2147/NSS.S284498
5. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. doi:10.1016/j.smrv.2018.10.006
6. Hale L, Singer L, Barnet JH, Peppard PE, Hagen EW. associations between midlife insomnia symptoms and earlier retirement. Sleep Health. 2017;3(3):170–177. doi:10.1016/j.sleh.2017.03.003
7. Laugsand LE, Strand LB, Vatten LJ, Janszky I, Bjørngaard JH. Insomnia symptoms and risk for unintentional fatal injuries–the HUNT Study. Sleep. 2014;37(11):1777–1786. doi:10.5665/sleep.4170
8. Lovato N, Lack L. Insomnia and mortality: a meta-analysis. Sleep Med Rev. 2019;43:71–83. doi:10.1016/j.smrv.2018.10.004
9. Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, persistence, and remission rates of insomnia over 5 years. JAMA Netw Open. 2020;3(11):e2018782–e2018782. doi:10.1001/jamanetworkopen.2020.18782
10. Perlis ML, Vargas I, Ellis JG, et al. the natural history of insomnia: the incidence of acute insomnia and subsequent progression to chronic insomnia or recovery in good sleeper subjects. Sleep. 2019;43(6):zsz299
11. Garland SN, Rowe H, Repa LM, Fowler K, Zhou ES, Grandner MA. A decade’s difference: 10-year change in insomnia symptom prevalence in Canada depends on sociodemographics and health status. Sleep Health. 2018;4(2):160–165. doi:10.1016/j.sleh.2018.01.003
12. Chaput JP, Yau J, Rao DP, Morin CM. Prevalence of insomnia for Canadians aged 6 to 79. Health Rep. 2018;29(12):16–20.
13. Roth T, Coulouvrat C, Hajak G, et al. Prevalence and perceived health associated with insomnia based on DSM-IV-TR; international statistical classification of diseases and related health problems, tenth revision; and research diagnostic criteria/International Classification of Sleep Disorders, Second Edition Criteria: results from the America Insomnia Survey. Biol Psychiatry. 2011;69(6):592–600. doi:10.1016/j.biopsych.2010.10.023
14. Chung KF, Yeung WF, Ho FY, Yung KP, Yu YM, Kwok CW. Cross-cultural and comparative epidemiology of insomnia: the diagnostic and statistical manual (DSM), international classification of diseases (ICD) and international classification of sleep disorders (ICSD). Sleep Med. 2015;16(4):477–482. doi:10.1016/j.sleep.2014.10.018
15. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
16. Ohayon MM, Sagales T. Prevalence of insomnia and sleep characteristics in the general population of Spain. Sleep Med. 2010;11(10):1010–1018. doi:10.1016/j.sleep.2010.02.018
17. Leger D, Guilleminault C, Dreyfus JP, Delahaye C, Paillard M. Prevalence of insomnia in a survey of 12,778 adults in France. J Sleep Res. 2000;9(1):35–42. doi:10.1046/j.1365-2869.2000.00178.x
18. Pallesen S, Sivertsen B, Nordhus IH, Bjorvatn B. A 10-year trend of insomnia prevalence in the adult Norwegian population. Sleep Med. 2014;15(2):173–179. doi:10.1016/j.sleep.2013.10.009
19. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
20. Sivertsen B, Pallesen S, Friborg O, et al. Sleep patterns and insomnia in a large population-based study of middle-aged and older adults: the Tromso study 2015–2016. J Sleep Res. 2021;30(1):e13095. doi:10.1111/jsr.13095
21. Andreeva VA, Torres MJ, Druesne-Pecollo N, et al. Sex-specific associations of different anthropometric indices with acute and chronic insomnia. Eur J Public Health. 2017;27(6):1026–1031. doi:10.1093/eurpub/ckx123
22. McArdle N, Ward SV, Bucks RS, et al. The prevalence of common sleep disorders in young adults: a descriptive population-based study. Sleep. 2020;43(10). doi:10.1093/sleep/zsaa072.
23. Appleton SL, Reynolds AC, Gill TK, Melaku YA, Adams R. Waking to use technology at night, and associations with driving and work outcomes: a screenshot of Australian adults. Sleep. 2020;43(8):zsaa015. doi:10.1093/sleep/zsaa015
24. Adams R, Appleton S, Taylor A, et al. Sleep health of Australian adults in 2016: results of the 2016 sleep health foundation national survey. Sleep Health. 2017;3(1):35–42. doi:10.1016/j.sleh.2016.11.005
25. National Sleep Foundation. Adult sleep habits; 2002. Available from: https://sleepfoundationorg/sleep-polls-data/sleep-in-america-poll/2002-adult-sleep-habits.
26. Hillman DR, Lack LC. Public health implications of sleep loss: the community burden. Med J Aust. 2013;199(8):S7–10. doi:10.5694/mja13.10620
27. Reynolds AC, Ferguson SA, Appleton SL, et al. Prevalence of probable shift work disorder in non-standard work schedules and associations with sleep, health and safety outcomes: a cross-sectional analysis. Nat Sci Sleep. 2021;13:683–693. doi:10.2147/NSS.S301493
28. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–243. doi:10.1016/j.sleh.2015.10.004
29. Sweetman A, Melaku YA, Lack L, et al. Prevalence and associations of co-morbid insomnia and sleep apnoea in an Australian population-based sample. Sleep Med. 2021;82:9–17. doi:10.1016/j.sleep.2021.03.023
30. Australian Bureau of Statistics. Retirement and retirement intentions, Australia. retiree statistics and the retirement plans of people aged 45 years and over. Available from: https://wwwabsgovau/statistics/labour/employment-and-unemployment/retirement-and-retirement-intentions-australia/latest-release.
31. Boyle JT, Vargas I, Rosenfield B, Grandner MA, Perlis ML, Severity I. Degree of dysfunction: what is to be learned when these domains are discordant? Behav Sleep Med. 2022;20(2):164–172. doi:10.1080/15402002.2021.1895794
32. Laugsand LE, Vatten LJ, Platou C, Janszky I. Insomnia and the risk of acute myocardial infarction: a population study. Circulation. 2011;124(19):2073–2081. doi:10.1161/CIRCULATIONAHA.111.025858
33. Collop N. Sleep and Sleep disorders in chronic obstructive pulmonary disease. Respiration. 2010;80(1):78–86. doi:10.1159/000258676
34. Liu J, Zhang X, Zhao Y, Wang Y, Bhatt GC. The association between allergic rhinitis and sleep: a systematic review and meta-analysis of observational studies. PLoS One. 2020;15(2):e0228533. doi:10.1371/journal.pone.0228533
35. Luyster FS, Strollo PJ
36. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
37. Singareddy R, Vgontzas AN, Fernandez-Mendoza J, et al. Risk factors for incident chronic insomnia: a general population prospective study. Sleep Med. 2012;13(4):346–353. doi:10.1016/j.sleep.2011.10.033
38. Sweetman A, Lack L, Bastien C. Co-Morbid Insomnia and Sleep Apnea (COMISA): prevalence, consequences, methodological considerations, and recent randomized controlled trials. Brain Sci. 2019;9(12):371. doi:10.3390/brainsci9120371
39. Kessler RC, Coulouvrat C, Hajak G, et al. Reliability and validity of the brief insomnia questionnaire in the America insomnia survey. Sleep. 2010;33(11):1539–1549. doi:10.1093/sleep/33.5.1539
40. Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17(4):241–254. doi:10.1016/j.smrv.2012.09.005
41. Australian Bureau of Statistics. Internet activity, Australia; cat no 8153.0. Available from: https://wwwabsgovau/statistics/industry/technology-and-innovation/internet-activity-australia/latest-release.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.