Back to Journals » Nature and Science of Sleep » Volume 14
Insomnia Partially Mediates the Relationship of Occupational Stress with Mental Health Among Shift Working Nurses and Midwives in Polish Hospitals
Authors Gustavsson K, Jernajczyk W, Wichniak A
Received 15 June 2022
Accepted for publication 11 October 2022
Published 3 November 2022 Volume 2022:14 Pages 1989—1999
DOI https://doi.org/10.2147/NSS.S375375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Katarzyna Gustavsson,1 Wojciech Jernajczyk,1 Adam Wichniak2
1Department of Clinical Neurophysiology, Sleep Medicine Center, Institute of Psychiatry and Neurology, Warsaw, Poland; 2Third Department of Psychiatry, Institute of Psychiatry and Neurology, Warsaw, Poland
Correspondence: Katarzyna Gustavsson, Department of Clinical Neurophysiology, Sleep Medicine Center, Institute of Psychiatry and Neurology, Sobieskiego 9, Warszawa, 02‐957, Poland, Tel +48 22 45 82 713, Email [email protected]
Purpose: Insufficient sleep increases sensitivity to chronic stress and may be a precursor to the deterioration of mental health and the development of burnout. The aim of our study was to verify whether symptoms of insomnia mediate the relationship of occupational stress with mental health among nurses who work shifts.
Materials and Methods: The analyses included 117 female nurses and midwives who work shifts. They filled in the 16-item Effort-Reward Imbalance Questionnaire (ERIQ) assessing occupational stress, the Insomnia Severity Index (ISI), the Patient Health Questionnaire (PHQ-9, the question about sleep was excluded from the analyses), the Generalized Anxiety Disorder Assessment (GAD-7), and the 16-item Oldenburg Burnout Inventory (OLBI) consisting of two scales – Disengagement and Exhaustion (OLBI-D and OLBI-E).
Results: Insomnia partially mediated the association of the effort-reward imbalance ratio with depression, anxiety and the exhaustion dimension of burnout. We found no association of insomnia symptoms with the depersonalization dimension of burnout, but the effort-reward imbalance ratio was associated with the depersonalization scale.
Conclusion: The results showed that occupational stress has varying degrees of influence on mental health, partly depending on the severity of insomnia symptoms among nurses and midwives who work shifts.
Keywords: mental health, night work, healthcare workers, occupational stress
Introduction
Sleep quality and stress are inextricably linked. Neurochemistry and the neural networks engaged in the stress response overlap with those regulating arousal and the sleep-wake cycle.1 Both physiological as well as cognitive and emotional arousal caused by exposure to stress may result in sleep disturbance.2 Perseverative cognition and anticipatory stress may lead to increased psychosomatic load and sustained physiological arousal.3,4 This prolonged activation involving, for example, the hypothalamic-pituitary-adrenocortical and sympathetic-adrenomedullary systems may lead to difficulty in falling asleep and maintaining it.5,6 At the same time, sleep plays an essential role in recovery from everyday stress. Good quality sleep protects against overactivation of the hypothalamic-pituitary-adrenal axis and the negative impact of stress.7
Insomnia is often caused by exposure to stress and work is its most common source.8,9 There is a significant association between occupational stress and insomnia and it may also contribute to impaired mental health.10 Chronic occupational stress may result in burnout and working conditions have been linked to depression.11,12
Healthcare workers have a higher prevalence of sleep-related problems than employees in other professions.13 Among nurses, poor quality sleep has been shown to be linked to working in a shift system.14 Working outside of the standard wake phase of the sleep-wake cycle might have an effect not only on sleep, but on other dimensions of mental health as well.15 Sleep problems are closely associated with depression and anxiety.16,17 Poor quality sleep increases vulnerability to stressful stimuli and the probability of mental health problems occurring.7,18 Sleep loss has been shown to be linked to the development of burnout among shift workers and individuals with high burnout scores experience fragmented sleep.19,20
Unlike other industries where workers engage in shift work, the nursing profession is predominantly female. Women are at a higher risk of depression and anxiety.21 Hospital nurses have been found to experience higher levels of stress and burnout than community and other non-hospital nurses.22,23 Moreover, nurses on rotating shifts report higher perceived stress than nurses on fixed day shifts.24
Few studies have examined stress, insomnia and mental health in one model. Most of the research on this topic focuses on pairs of these variables. So far, perceived stress has been shown to mediate the relationship of sleep quality with anxiety and depression25 and insomnia has been shown to mediate the association of perceived stress with anxiety.26 These results have been obtained among students. This article aims to present an analysis of data from a working sample using a recognized model of occupational stress – the Effort-Reward Imbalance Model.27 Occupational stress, measured by this model, is associated with both insomnia and increased risk of depression.10,12,28
The aim of our study was to verify whether and to what extent symptoms of insomnia mediate the relationship between occupational stress and mental health in three dimensions – depression, anxiety and burnout, among nurses and midwives who work shifts in Polish hospitals.
Materials and Methods
Ethics Statement
The study was carried out within the research project “The relationship of the work schedule and occupational stress with the quality of sleep among employees in safety-sensitive professions” which was approved by the Bioethics Committee at the Institute of Psychiatry and Neurology in Warsaw, Poland (Certificate of Approval No. 25/2018), The study was conducted in accordance with the Declaration of Helsinki.
Participation Steps
The study was performed as an online survey using a convenience sample. A link to the survey was published on eight major Polish social media groups dedicated to nurses and a website dedicated to the project. An invitation to take part in the study was also presented during a conference of the Supreme Chamber of Nurses and Midwives in Warsaw, Poland.
Due to the online setting of the survey, before taking part, participants read about the topic and aims of the project, the founding body, voluntary participation, the ability to withdraw from the survey without saving answers any time and the confidentiality and processing of sensitive personal data if they chose to submit their contact information for further participation in the project. In order to go further, they needed to check a consent statement box. All subjects included in this study provided informed consent.
Firstly, participants filled in a short questionnaire about their sex, age, length of work experience, length of experience of shift work, average number of hours worked per week, and the number of night shifts and days off in the previous four weeks. They then filled in questionnaires measuring the investigated variables.
Standardized Questionnaires
Occupational stress was measured within the framework of the effort-reward imbalance (ERI) model. The short ten-item Effort-Reward Imbalance Questionnaire (ERIQ) was used.29
The items were derived from the long version of the scale translated into Polish in the NEXT-Study.30 According to the ERI model, if perceived efforts, referring to the amount of strain caused by work demands, exceed perceived rewards, such as job security or appreciation of others, this results in a stress reaction.27,31 The ERIQ uses two scales – the effort scale of three items and the reward scale of seven. The ERI ratio is calculated as the sum of the effort score divided by the sum of the reward score and then multiplied by a correction factor to account for the unequal number of items in each scale.32 Initially, a ratio of 1 was supposed to mean a balanced work experience and values exceeding this threshold would mean a stressful work environment. However, it has been proposed that a better approach is to analyse the imbalance based on the distribution in the investigated sample and using continuous data analysis.32 We used this approach in our analysis.
The symptoms of insomnia and the degree to which they impair or distress a person’s functioning were measured using the Polish version of the Insomnia Severity Index (ISI, the scale has undergone a linguistic validation in Polish performed by three experts in sleep medicine as a part of the academic activities of the Sleep Medicine Center at the Institute of Psychiatry and Neurology in Warsaw, Poland).33
The outcome of this study, mental health, was measured in three dimensions – depression, anxiety and burnout. To screen for the presence and severity of the two most prevalent mental health disturbances – depression and anxiety, the Patient Health Questionnaire 9-item scale (PHQ-9) and the Generalized Anxiety Disorder 7-item scale (GAD-7) were used.34,35 The Polish versions of both of these scales are available through Pfizer at www.phqscreeners.com. The psychometric properties of the Polish version of the PHQ-9 were verified and the scale was shown to be effective in screening for depression among adults.36 The sleep question in the PHQ-9 was removed from the total score in the analyses so as not to inflate the correlation between depression and the insomnia measure and scores from this shortened scale (PHQ-8) were used in the analyses. Burnout was assessed with the 16-item Oldenburg Burnout Inventory (OLBI), which consists of two scales – Disengagement (OLBI-D) and Exhaustion (OLBI-E).37 The Polish version of the questionnaire was shown to have satisfactory psychometric properties and was validated for use in measuring burnout in Poland.38,39
Statistical Analyses
A priori sample size was calculated, using a method by Soper,40 to obtain the desired power level of 0.8 for a medium effect size of 0.15 and a significance level of 0.05. It was estimated that at least 97 participants would be needed to obtain adequate power in this study. The post-hoc power analyses were done using the Monte Carlo Power Analysis for Indirect Effects41 and a method described by Soper.40
The statistical analyses were conducted using SPSS software version 27.0. All the variables were continuous. Descriptive statistics (presented as mean value, standard deviation, range values) and frequency analysis were used to analyze the demographic variables. Spearman correlations were used to examine the relationships between major factors such as ERI, insomnia and mental health as well as other variables which would impact the relationships, such as age, length of work experience, length of experience of shift work, average number of hours worked per week, average number of night shifts per month and the number of days off in the previous four weeks. The statistical significance was considered to be p < 0.05.
To estimate the mediating effect of insomnia on the association between the independent variable of ERI ratio and the dependent variables of mental health, we conducted a mediation model with one mediator (Model 4) and bootstrap analyses using SPSS PROCESS v4.0.42 Mediation analysis permits the testing of hypotheses about the effect of one variable on another using a third variable – a mediator. Bootstrapping is a nonparametric approach to statistical inference that produces standard errors and confidence intervals (CIs) for each of the parameters. Bootstrapping was done with 5000 resamples and bias-corrected 95% CIs were used to investigate the indirect effects. We checked for the multicollinearity of predictors, a linear relationship between the independent variables and the dependent variable, normality of residuals, standardized residuals range and Cook’s distance.
Results
The sampling process is described in a STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow chart in Figure 1. The final sample consisted of 117 participants – 83 (70.9%) nurses and 34 (29.1%) midwives. The sample characteristics, including data on their age, work experience and schedule, are presented in Table 1. Only 49 (41.9%) worked 48 hours or less (the maximum number of hours a nurse can work without signing the opt-out clause in Poland). Eighty-three (70.9%) worked in the 12+12 hours system, three (2.6%) worked 24-hour shifts and 31 (26.5%) worked both 12+12 and 24-hour shifts. In Polish hospitals, a nurse’s shift starts between 6:00 and 8:00 in the morning or between 18:00 and 20:00 in the evening and does not follow a set shift cycle. The descriptive statistics of the investigated variables are presented in Table 1. An ERI ratio above the value of 1.0 was present among 97 (82.9%) participants. A breakdown of the values on the depression, anxiety and burnout measures according to the cut-off values of the scales can be found in Table 2.
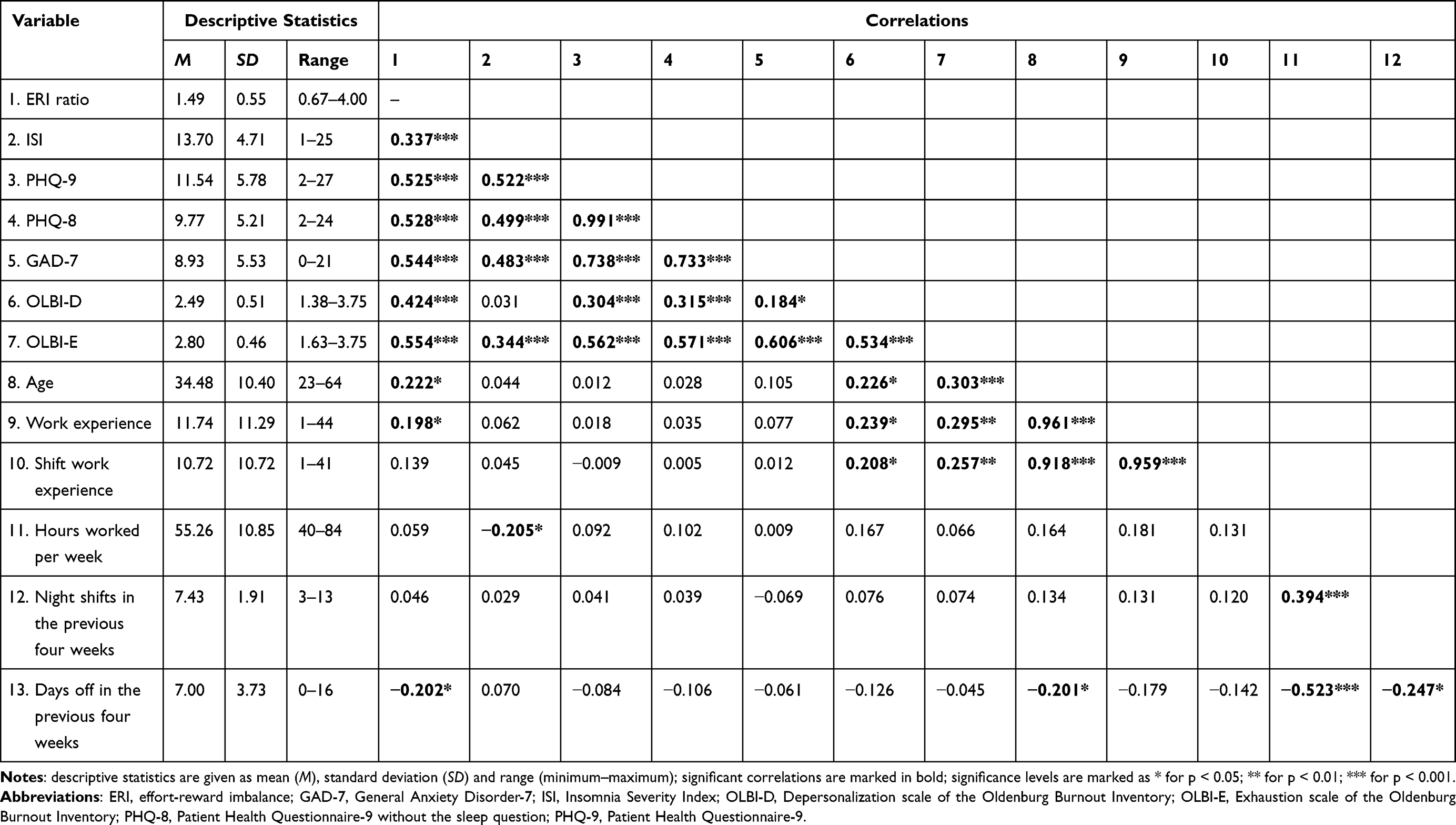 |
Table 1 Descriptive Statistics and Correlations for Study Variables (N = 117) |
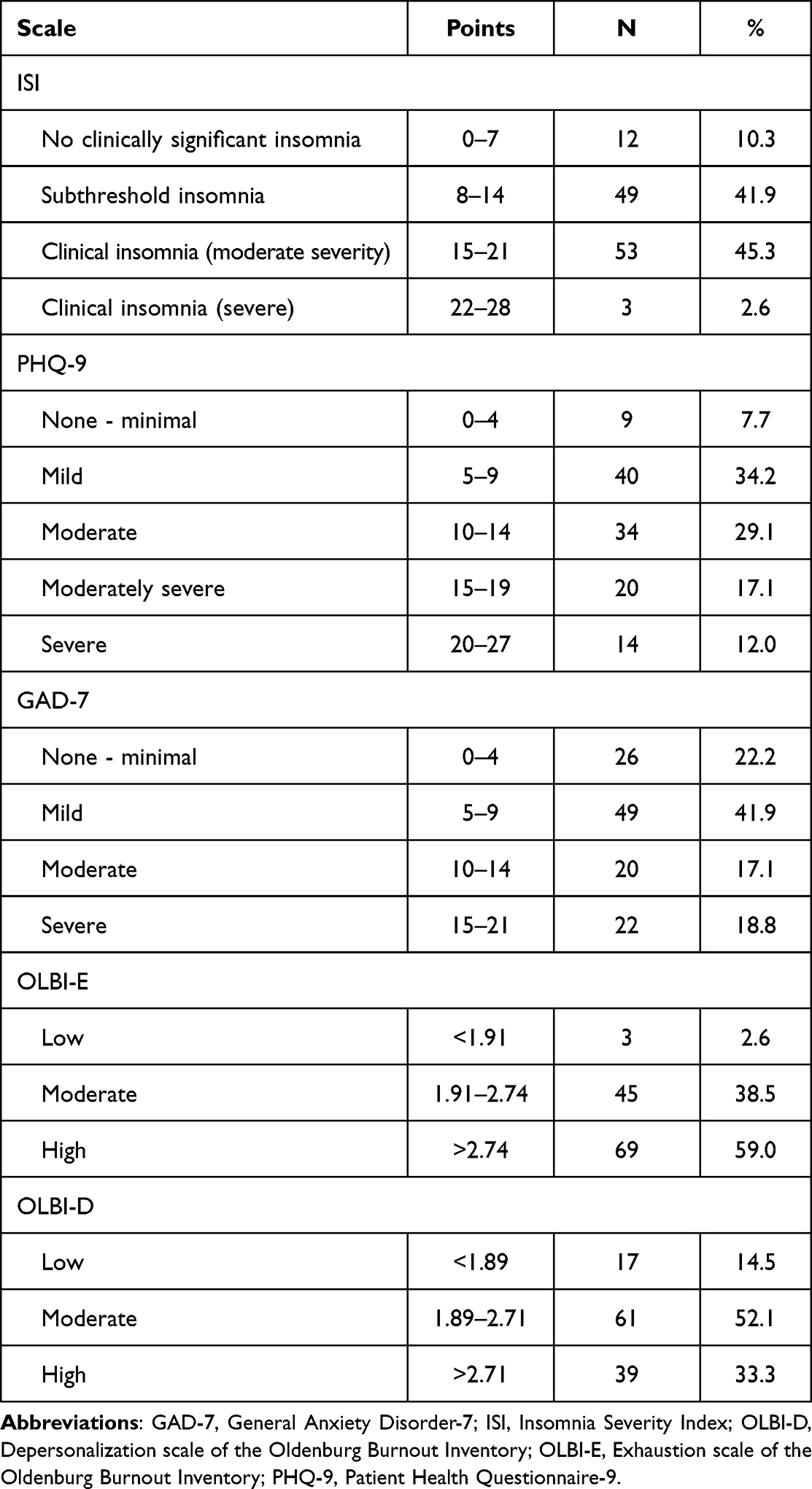 |
Table 2 Breakdown of Mental Health Scores According to the Cut-Off Values (N = 117) |
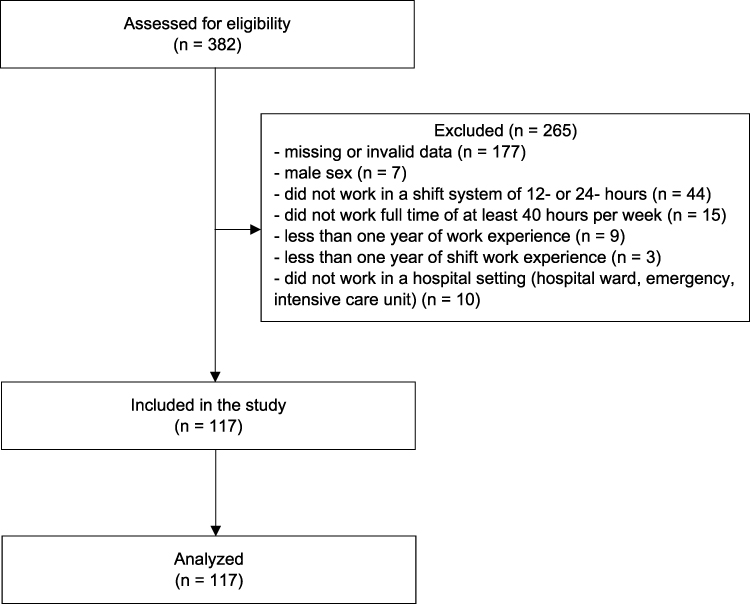 |
Figure 1 The sampling process described by a STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow chart. Notes: Adapted from von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344-9. Creative Commons. |
The correlations between the variables of interest and potential covariates are presented in Table 1. Age positively correlated with the OLBI-D (0.226, p = 0.014) and the OLBI-E (0.303, p < 0.001), therefore it was considered a covariate and entered as such in the regression models for these outcome variables. Work experience and shift work experience correlated with age at a very high level (0.961, p < 0.001; 0.918, p < 0.001 respectively), therefore only age was included in the regression analyses. The ISI did not correlate with the OBLI-D scale (p = 0.741) and a mediated regression model analysis was not performed on this outcome variable. OLBI-E correlated with the PHQ-9 at the level of 0.562 (p < 0.001) and with the GAD-7 at the level of 0.606 (p < 0.001). The OLBI-D correlated with the PHQ-9 at the level of 0.304 (p < 0.001) and with the GAD-7 at the level of 0.184 (p = 0.047). Both scales correlated with one another at the level of 0.534 (p < 0.001).
Depression
The ISI scores were entered as a mediator in the regression model, with the ERI ratio as the independent variable and the PHQ-8 scores as the dependent variable. In Step 1 of the mediation model, the regression of ERI on PHQ-8, ignoring the mediator, was significant (b = 4.5465, t(115) = 5.9196, p < 0.001). Step 2 showed that the regression of ERI on the mediator, ISI, was also significant (b = 2.6988, t(115) = 3.5833, p < 0.001). Step 3 of the mediation process showed that the mediator (ISI), controlling for ERI, was significant (b = 0.4034, t(114) = 4.5986, p < 0.001). Step 4 revealed that when controlling for the mediator (ISI), the ERI was a significant predictor of the PHQ-8 (b = 3.4578, t(114) = 4.6290, p < 0.001). The CIs for the indirect effect of insomnia did not contain 0 (95% CI [0.4395, 1.9804]). It was found that the ISI partially mediated the relationship between the ERI and the PHQ-8. The overall model accounted for 35.35% of the variance in the PHQ-8 scores (r2 = 0.3535, F(2, 114) = 31.1636, p < 0.001). Of the effect of the ERI on the PHQ-8, 23.95% was through the ISI (indirect effect of X on Y ISI Total b = 1.0887, boot SE = 0.3998). Figure 2A presents the results of the bootstrapped regression and mediation model for the effects of the ERI on the PHQ-8 through insomnia.
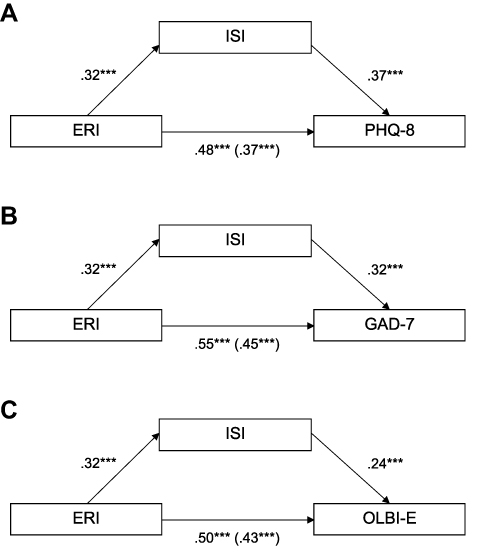 |
Figure 2 Standardized regression coefficients for the relationships between the ERI ratio and mental health as mediated by insomnia symptoms. The standardized regression coefficients between the independent and dependent variables, controlling for insomnia symptoms, are in parentheses. (A) The mediation model for the effects of the ERI on the PHQ-8 through insomnia. (B) The mediation model for the effects of the ERI on the GAD-7 through insomnia. (C) The mediation model for the effects of the ERI on the OLBI-E through insomnia. Abbreviations: ERI, effort-reward imbalance ratio; GAD-7, Generalized Anxiety Disorder-7; ISI, Insomnia Severity Index; OLBI-E, Oldenburg Burnout Inventory Exhaustion scale; PHQ-8, Patient Health Questionnaire-9 without the sleep question. Note: Significance levels are marked as *** for p < 0.001. |
Anxiety
The ISI scores were entered as a mediator in the regression model, with the ERI ratio as the independent variable and the GAD-7 scores as the dependent variable. In Step 1 of the mediation model, the regression of the ERI on GAD-7, ignoring the mediator, was significant (b = 5.5492, t(115) = 7.1528, p < 0.001). Step 2 showed that the regression of the ERI on the mediator, the ISI, was also significant (b = 2.6988, t(115) = 3.5833, p < 0.001). Step 3 of the mediation process showed that the mediator (ISI), controlling for the ERI, was significant (b = 0.3773, t(114) = 4.2029, p < 0.001). Step 4 revealed that when controlling for the mediator (ISI), the ERI was a significant predictor of the GAD-7 (b = 4.5309, t(114) = 5.9270, p < 0.001). The CIs for the indirect effect of insomnia did not contain 0 (95% CI [0.3675, 1.9627]). It was found that the ISI partially mediated the relationship between the ERI and the GAD-7. The overall model accounted for 40.08% of the variance in the GAD-7 scores (r2 = 0.4008, F(2, 114) = 38.1203, p < 0.001).
Of the effect of the ERI on the GAD-7, 18.35% was through the ISI (indirect effect of X on Y ISI Total b = 1.0183, boot SE = 0.4116). Figure 2B presents the results of the bootstrapped regression and mediation model for the effects of the ERI on the GAD-7 through insomnia.
Burnout
Exhaustion
The ISI scores were entered as a mediator in the regression model, with the ERI ratio as the independent variable, the OLBI-E scores as the dependent variable and age as a covariate. In Step 1 of the mediation model, the regression of the ERI on the OLBI-E, ignoring the mediator, was significant (b = 0.3976, t(114) = 5.8587, p < 0.001). Age was not a significant covariate (p = 0.1855). Step 2 showed that the regression of the ERI on the mediator, the ISI, was also significant (b = 2.6855, t(114) = 3.4782, p < 0.001). Age was not a significant covariate (p = 0.9320). Step 3 of the mediation process showed that the mediator (ISI), controlling for the ERI, was significant (b = 0.0203, t(113) = 2.8860, p = 0.005). Step 4 revealed that, controlling for the mediator (ISI), the ERI was a significant predictor of the OLBI-E (b = 0.3358, t(113) = 4.8529, p < 0.001). Age was not a significant covariate (p = 0.1794) in the overall model. The CIs for the indirect effect of insomnia did not contain 0 (95% CI [0.0154, 0.1271]). It was found that the ISI partially mediated the relationship between the ERI and the OLBI-E.
The overall model accounted for 31.44% of the variance in the OLBI-E scores (r2 = 0.3144 1, F(3, 113) = 17.2765, p <0.0001). Of the effect of the ERI on the OLBI-E, 15.54% was through the ISI (indirect effect of X on Y ISI Total b = 0.0618, boot SE = 0.0288). Figure 2C presents the results of the bootstrapped regression and mediation model for the effects of the ERI on the OLBI-E through insomnia.
Depersonalization
A multiple regression analysis was performed with the depersonalization dimension of burnout as an outcome and the ERI and age as predictors in order to determine if the OLBI-D could be predicted as a function of occupational stress. The overall model predicted 14% of the variability in the OLBI-D scores (r2 = 0.140, F(2, 114) = 9.264, p < 0.001). Age was shown not to be a significant predictor (b = 0.005, p = 0.293). The ERI was a significant predictor in the model explaining the OLBI-D scores (b = 0.316, p < 0.001, 95% CI [0.155, 0.478]).
Power Analysis
Using the Monte Carlo Power Analysis for Indirect Effects,41 post hoc power analyses revealed that the sample size of this study was adequate to attain a power of 0.94 for the reported mediation effects on PHQ-8 and of 0.93 on GAD-7. For OLBI-E, with the current sample size, the study had a power level of 0.76. Using a method described by Soper,40 the observed power of the regression model predicting OLBI-D scores was 0.98.
Discussion
This study showed that insomnia partially mediates the association of the ERI ratio with depression, anxiety, and the exhaustion dimension of burnout. We found no association of insomnia symptoms with the depersonalization dimension of burnout, but the ERI ratio was associated with the depersonalization scale.
Age was not a significant covariate of the relationship between the ERI ratio and both burnout dimensions. However, the sample in this study was relatively young overall and, therefore, we cannot make any conclusions on the role of age in the described models.
Our data, showing that the ratio between effort and reward at work of above the value of 1.0 was present among 97 (82.9%) participants, is consistent with previous research.43,44 A recent study among doctors and nurses by Deng et al45 shows that 78.4% had a high ERI ratio and that the sleep quality worsened as the ERI ratio increased.
Comparing our results regarding mental health to other research carried out among nurses in Poland, the burnout scores in our sample are comparable to the ones found in research by Ogińska-Bulik46 and the insomnia symptoms were higher than in a study by Andrzejewska et al47 Depression scores were much higher than in a study by Larysz and Uchmanowicz,48 even though their study overlapped the COVID-19 pandemic.
Due to the study’s cross-sectional design, no conclusions can be made about the directionality of the relationships. Mediation is most accurately established using a longitudinal design. However, according to Baron and Kelly, cross-sectional design permits the provision of initial evidence.49 Three out of four of our analyses (on PHQ-8, GAD-7, and OLBI-D) had excellent power to detect significant effects. One of the mediation models (OLBI-E) was under the desired power level, however we were still able to show significant mediation.
To the best of our knowledge, even though there is considerable research linking stress, insomnia and mental health in pairs, few studies have examined them in one model. A study among nursing students by Zhang et al25 describes how perceived stress mediates the relationship between sleep quality and anxiety and between sleep quality and depression. A later study by Manzar et al26 shows that insomnia mediates the relationship of perceived stress on anxiety, but not the other way round – insomnia did not mediate the relationship of anxiety on stress. Both of these studies were conducted among students. Our study analysed data from a working sample and focused on the occupational model of stress.
We treated insomnia as a predictor of mental health due to research showing that sleep problems are a risk for the onset of depression regardless of prior history of depression.19,28 An improvement in sleep quality is associated with a reduction in depressive symptoms.50 Targeting insomnia may be an appropriate approach to preventing mental health disorders among healthcare professionals who work shifts. Cognitive-behavioral therapy for insomnia among shift workers has been shown to improve sleep and alleviate mood, depression and anxiety symptoms.51,52
The study was conducted as an internet survey, which does not allow verification of the validity of the responses and risks the self-selection effect. Participants who took part in the study might have been individuals who were concerned about their mental health and searching for a self-diagnosis. Alternatively, we should consider the possibility of a social desirability bias, which was, to an extent, alleviated by the anonymity of the participants.53 We may also have missed people who did not have access to the internet to fill in the survey.
Another limitation in this study is that the modified version of the PHQ-9, which excluded the sleep question, has not been empirically evaluated. Even though we used mostly validated measures and theoretical models widely used in international research, the study did not include any objective assessments and the research relied only on self-report measures, which raises the issue of common method variance. It also introduces the risk of reporting bias, because some participants may have had a propensity for negative responses. There is a possibility that people scoring high on depression measures perceived their working conditions more negatively, which would point to a reverse causation. However, prospective studies show that work stress predicts depression, which is in line with our theoretical background for the models.12
The depersonalization subscale of burnout correlated with depression at a moderate level and anxiety at a low level, whereas the exhaustion subscale of burnout correlated with these two measures strongly and similar to the correlation between the two subscales themselves. This is in line with research showing that depression, anxiety, and burnout are associated with each other, but although there may be some overlap, they are not the same. Depression can develop in various contexts and be more pervasive, while burnout occurs due to occupational factors.54
The conclusions from this study are limited to only one model of work stress. Other important factors associated with work as well as work-life balance were not included. Furthermore, the sample consisted of women only. Even though the nursing population is mostly female, the generalizability of the results is limited.
Apart from factors relating to work experience and work schedule, we did not include other factors which could impact the model in this study. One such factor is chronotype, which influences sleep and mental health among shift workers and, therefore, could potentially explain a portion of the variance in the results.55 Furthermore, working in a shift system has been shown to impact a nurse’s lifestyle, such as physical activity and diet as well as family and social life,24,56 which should be taken into account in future research.
Conclusion
This study shows that insomnia partially mediates the association of the ERI ratio with depression, anxiety, and the exhaustion dimension of burnout. The results of the study prove that insomnia symptoms should be taken into account in health screenings for nurses. Employees with poor sleep quality are likely to experience burnout, depression and anxiety. Therefore, they should be identified at the early phase of mental health problems and receive appropriate intervention.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, KG, upon reasonable request.
Funding
This work was supported by the National Science Center in Poland under Grant 2019/33/N/HS6/02572.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lo Martire V, Caruso D, Palagini L, Zoccoli G, Bastianini S. Stress & sleep: a relationship lasting a lifetime. Neurosci Biobehav Rev. 2020;117:65–77.
2. Kalmbach DA, Anderson JR, Drake CL. The impact of stress on sleep: pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J Sleep Res. 2018;27(6):e12710. doi:10.1111/jsr.12710
3. Brosschot JF. Markers of chronic stress: prolonged physiological activation and (un) conscious perseverative cognition. Neurosci Biobehav Rev. 2010;35(1):46–50. doi:10.1016/j.neubiorev.2010.01.004
4. Ottaviani C, Thayer JF, Verkuil B, et al. Physiological concomitants of perseverative cognition: a systematic review and meta-analysis. Psychol Bull. 2016;142(3):231–259. doi:10.1037/bul0000036
5. Stewart NH, Arora VM. The impact of sleep and circadian disorders on physician burnout. Chest. 2019;156(5):1022–1030. doi:10.1016/j.chest.2019.07.008
6. van Dalfsen JH, Markus CR. The influence of sleep on human hypothalamic-pituitary-adrenal (HPA) axis reactivity: a systematic review. Sleep Med Rev. 2018;39:187–194. doi:10.1016/j.smrv.2017.10.002
7. Buckley T, Schatzberg A. On the interactions of the Hypothalamic-Pituitary-Adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. 2005;90(5):3106–3114. doi:10.1210/jc.2004-1056
8. Hall M, Buysse D, Nowell P, et al. Symptoms of stress and depression as correlates of sleep in primary insomnia. Psychosom Med. 2000;62(2):227–230. doi:10.1097/00006842-200003000-00014
9. Danielsson M, Heimerson I, Lundberg U, Perski A, Stefansson C, Akerstedt T. Psychosocial stress and health problems: health in Sweden: the national public health report 2012. Chapter 6. Scand J Public Health. 2012;40(9 Suppl):121–134. doi:10.1177/1403494812459469
10. Yang B, Wang Y, Cui F, et al. Association between insomnia and job stress: a meta-analysis. Sleep Breath. 2018;22(4):1221–1231. doi:10.1007/s11325-018-1682-y
11. Maslach C, Leiter M. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016;15(2):103–111. doi:10.1002/wps.20311
12. Rugulies R, Aust B, Madsen I. Effort–reward imbalance at work and risk of depressive disorders. A systematic review and meta-analysis of prospective cohort studies. Scand J Work Environ Health. 2017;43(4):294–306. doi:10.5271/sjweh.3632
13. Simonelli G, Marshall N, Grillakis A, Miller C, Hoyos C, Glozier N. Sleep health epidemiology in low and middle-income countries: a systematic review and meta-analysis of the prevalence of poor sleep quality and sleep duration. Sleep Health. 2018;4(3):239–250. doi:10.1016/j.sleh.2018.03.001
14. Flo E, Pallesen S, Magerøy N, et al. Shift work disorder in nurses – assessment, prevalence and related health problems. PLoS One. 2012;7(4):e33981. doi:10.1371/journal.pone.0033981
15. Torquati L, Mielke G, Brown W, Burton N, Kolbe-Alexander T. Shift work and poor mental health: a meta-analysis of longitudinal studies. Am J Public Health. 2019;109(11):e13–e20. doi:10.2105/AJPH.2019.305278
16. Nyer M, Farabaugh A, Fehling K, et al. Relationship between sleep disturbance and depression, anxiety, and functioning in college students. Depress Anxiety. 2013;30(9):873–880. doi:10.1002/da.22064
17. Kalmbach D, Arnedt J, Song P, Guille C, Sen S. Sleep disturbance and short sleep as risk factors for depression and perceived medical errors in first-year residents. Sleep. 2017;40(3). doi:10.1093/sleep/zsw073
18. Vandekerckhove M, Cluydts R. The emotional brain and sleep: an intimate relationship. Sleep Med Rev. 2010;14(4):219–226. doi:10.1016/j.smrv.2010.01.002
19. Cheng W, Cheng Y. Night shift and rotating shift in association with sleep problems, burnout and minor mental disorder in male and female employees. Occup Environ Med. 2016;74(7):483–488. doi:10.1136/oemed-2016-103898
20. Söderström M, Ekstedt M, Åkerstedt T, Nilsson J, Axelsson J. Sleep and sleepiness in young individuals with high burnout scores. Sleep. 2004;27(7):1369–1377. doi:10.1093/sleep/27.7.1369
21. Kessler R, Merikangas K, Wang P. The prevalence and correlates of workplace depression in the national comorbidity survey replication. J Occup Environ Med. 2008;50(4):381–390. doi:10.1097/JOM.0b013e31816ba9b8
22. Dor A, Mashiach Eizenberg M, Halperin O. Hospital nurses in comparison to community nurses: motivation, empathy, and the mediating role of burnout. Can J Nurs Res. 2019;51(2):72–83. doi:10.1177/0844562118809262
23. Muhamad Robat R, Mohd Fauzi MF, Mat Saruan NA, Mohd Yusoff H, Harith AA. Why so stressed? A comparative study on stressors and stress between hospital and non-hospital nurses. BMC Nurs. 2021;20(1):2. doi:10.1186/s12912-020-00511-0
24. Chiang SL, Chiang LC, Tzeng WC, et al. Impact of rotating shifts on lifestyle patterns and perceived stress among nurses: a cross-sectional study. Int J Environ Res Public Health. 2022;19(9):5235. doi:10.3390/ijerph19095235
25. Zhang Y, Peters A, Chen G. Perceived stress mediates the associations between sleep quality and symptoms of anxiety and depression among college nursing students. Int J Nurs Educ Scholarsh. 2018;15(1). doi:10.1515/ijnes-2017-0020
26. Manzar M, Salahuddin M, Pandi-Perumal S, Bahammam A. Insomnia may mediate the relationship between stress and anxiety: a cross-sectional study in university students. Nat Sci Sleep. 2021;13:31–38. doi:10.2147/NSS.S278988
27. Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. 1996;1(1):27–41. doi:10.1037/1076-8998.1.1.27
28. Li L, Wu C, Gan Y, Qu X, Lu Z. Insomnia and the risk of depression: a meta-analysis of prospective cohort studies. BMC Psychiatry. 2016;16(1). doi:10.1186/s12888-016-1075-3
29. Siegrist J, Wege N, Pühlhofer F, Wahrendorf M. A short generic measure of work stress in the era of globalization: effort–reward imbalance. Int Arch Occup Environ Health. 2008;82(8):1005–1013. doi:10.1007/s00420-008-0384-3
30. Kuemmerling A, Hasselhorn HM, Tackenberg P. Psychometric properties of the scales used in the NEXT-study. In: Hasselhorn HM, Mueller BH, Tackenberg P, editors. Working Conditions and Intent to Leave the Profession Among Nursing Staff in Europe. The National Institute for Working Life and the Swedish Trade Unions in Co-Operation. Stockholm: National Institute for Working Life; 2003:237–258.
31. Siegrist J, Starke D, Chandola T, et al. The measurement of effort–reward imbalance at work: European comparisons. Soc Sci Med. 2004;58(8):1483–1499. doi:10.1016/S0277-9536(03)00351-4
32. Montano D, Li J, Siegrist J. The measurement of effort-reward imbalance (ERI) at work. In: Siegrist J, Wahrendorf M, editors. Work Stress and Health in a Globalized Economy: The Model of Effort-Reward Imbalance. Springer International Publishing; 2016:21–42.
33. Morin CM. Insomnia: Psychological Assessment and Management. Guilford Press; 1993.
34. Spitzer R, Kroenke K, Williams J, Löwe B, Brief A. Measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092. doi:10.1001/archinte.166.10.1092
35. Kroenke K, Spitzer R. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–515. doi:10.3928/0048-5713-20020901-06
36. Kokoszka A, Jastrzębski A, Obrębski M. Psychometric properties of the Polish version of patient health questionnaire-9. Psychiatria. 2016;13(4):187–193.
37. Demerouti E, Bakker A. The oldenburg burnout inventory: a good alternative to measure burnout and engagement. In: Halbesleben J, editor. Handbook of Stress and Burnout in Health Care. New York: Nova Science; 2008:65–78.
38. Baka L, Cieślak R. Self-efficacy and social support and the effects of job stressors on job burnout and work engagement in teachers. Stud Psychol. 2010;48:5–18.
39. Baka Ł, Basińska BA. Psychometryczne właściwości polskiej wersji oldenburskiego kwestionariusza wypalenia zawodowego (OLBI). Med Pr. 2016;67(1):29–41. doi:10.13075/mp.5893.00353
40. Soper D Free statistics calculators; 2022. Available from: https://www.danielsoper.com/statcalc/calculator.aspx?id=9.
41. Schoemann A, Boulton A, Short S. Determining power and sample size for simple and complex mediation models. Soc Psychol Personal Sci. 2017;8(4):379–386. doi:10.1177/1948550617715068
42. Hayes A. Mediation, Moderation, and Conditional Process Analysis. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
43. Lua I, de Araújo T, Santos K, de Almeida M. Factors associated with common mental disorders among female nursing professionals in primary health care. Psicologia. 2018;31(1):1.
44. Bardhan R, Heaton K, Davis M, Chen P, Dickinson D, Lungu C. A cross sectional study evaluating psychosocial job stress and health risk in emergency department nurses. Int J Environ Res Public Health. 2019;16(18):3243. doi:10.3390/ijerph16183243
45. Deng X, Fang R, Cai Y. Evaluation of the correlation between effort-reward imbalance and sleep quality among community health workers. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-06526-w
46. Ogińska-Bulik N. Związek między wypaleniem zawodowym i wtórnym stresem traumatycznym wśród pielęgniarek pracujących w opiece paliatywnej [Relationship between burnout and secondary traumatic stress among nurses working in palliative care]. Psychiatria. Polish. 2018;15(2):63–69.
47. Andrzejewska K, Snarska K, Chorąży M, et al. Occurrence of sleep disorders among nursing staff. Medycyna Ogólna i Nauki o Zdrowiu. 2018;24(2):126–132. doi:10.26444/monz/89532
48. Larysz A, Uchmanowicz I. Sociodemographic factors and depressive symptoms among cardiac nurses: a cross-sectional study. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.723035
49. Baron R, Kenny D. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037/0022-3514.51.6.1173
50. Cunningham J, Shapiro C. Cognitive Behavioural Therapy for Insomnia (CBT-I) to treat depression: a systematic review. J Psychosom Res. 2018;106:1–12. doi:10.1016/j.jpsychores.2017.12.012
51. Järnefelt H, Härmä M, Sallinen M, et al. Cognitive behavioural therapy interventions for insomnia among shift workers: RCT in an occupational health setting. Int Arch Occup Environ Health. 2020;93(5):535–550. doi:10.1007/s00420-019-01504-6
52. Järnefelt H, Lagerstedt R, Kajaste S, Sallinen M, Savolainen A, Hublin C. Cognitive behavioral therapy for shift workers with chronic insomnia. Sleep Med. 2012;13(10):1238–1246. doi:10.1016/j.sleep.2012.10.003
53. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
54. Koutsimani P, Montgomery A, Georganta K. The relationship between burnout, depression, and anxiety: a systematic review and meta-analysis. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.00284
55. Khan WAA, Conduit R, Kennedy GA, Jackson ML. The relationship between shift-work, sleep, and mental health among paramedics in Australia. Sleep Health. 2020;6(3):330–337. doi:10.1016/j.sleh.2019.12.002
56. Ljevak I, Vasilj I, Ćurlin M, et al. The impact of shift work on psychosocial functioning and quality of life among hospital-employed nurses: a cross-sectional comparative study. Psychiatr Danub. 2020;32(Suppl 2):262–268.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Burnout Among ICU and Non-ICU Healthcare Professionals in Saudi Arabia: A Comparative Cross-Sectional Analysis
Krishna GG, Harbli NMA, Krishnan N, Ghundul LB, Aldhahri R, Aldossary AB, Margalani AO, Almeshari M, Alwadeai KS, Alshehri RA, Alkhathami AAA, Sreedharan JK, AlAhmari AD
Journal of Multidisciplinary Healthcare 2025, 18:995-1005
Published Date: 21 February 2025
“Exploring Psychosocial Interventions to Improve Mental Health Outcomes Among Healthcare Workers”: Scoping Review
Maulana I, Shalahuddin I, Eriyani T, Pebrianti S
Journal of Multidisciplinary Healthcare 2025, 18:8293-8303
Published Date: 27 December 2025