Back to Journals » Nature and Science of Sleep » Volume 13
Insomnia in Patients with Borderline Personality Disorder
Authors Vanek J ![]() , Prasko J
, Prasko J ![]() , Ociskova M
, Ociskova M ![]() , Hodny F
, Hodny F ![]() , Holubova M, Minarikova K
, Holubova M, Minarikova K ![]() , Slepecky M, Nesnidal V
, Slepecky M, Nesnidal V ![]()
Received 1 December 2020
Accepted for publication 20 January 2021
Published 22 February 2021 Volume 2021:13 Pages 239—250
DOI https://doi.org/10.2147/NSS.S295030
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Jakub Vanek,1 Jan Prasko,1– 3 Marie Ociskova,1 Frantisek Hodny,1 Michaela Holubova,4 Kamila Minarikova,1 Milos Slepecky,2 Vlastimil Nesnidal1
1Department of Psychiatry, Faculty of Medicine and Dentistry, University Palacky Olomouc, University Hospital, Olomouc, 77520, The Czech Republic; 2Department of Psychology Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University in Nitra, Nitra, The Slovak Republic; 3Institute for Postgraduate Education in Health Care, Prague, The Czech Republic; 4Department of Psychiatry, Hospital Liberec, Liberec, The Czech Republic
Correspondence: Jan Prasko
Department of Psychiatry, University Hospital Olomouc and Faculty of Medicine and Dentistry, Palacky University Olomouc, I. P. Pavlova 6, Olomouc, 77520, The Czech Republic
Email [email protected]
Objective: Both sleep disorders and BPD are prevalent in the population, and one is often a comorbidity of the other. This narrative review aims to assess contemporary literature and scientific databases to provide the current state of knowledge about sleep disorders in patients with borderline personality disorder (BPD) and clinical suggestions for managing sleep disorders in BPD patients and future research direction.
Methods: Articles were acquired via PubMed and Web of Science, and papers published between January 1980 and October 2020 were extracted. Authors made a series of literature searches using the keywords: Sleep problems, Insomnia, Nightmares, Obstructive sleep apnea, Borderline personality disorder. The inclusion criteria were: published in peer-reviewed journals; studies in humans; or reviews on the related topic; English language. The exclusion criteria were: abstracts from conferences; commentaries; subjects younger than 18 years. After an inspection of the full texts, 42 papers from 101 were selected. Secondary documents from the reference lists of the primary designated papers were searched, assessed for suitability, and included. In total, 71 papers were included in the review process.
Results: Sleep disturbance is common among patients with BPD. Nevertheless, the number of investigations is limited, and the prevalence differs between 5– 45%. Studies assessing objective changes in sleep architecture in BPD show inconsistent results. Some of them identify REM sleep changes and a decrease in slow-wave sleep, while other studies found no objective sleep architecture changes. There is also a higher prevalence of nightmares in patients with BPD. Untreated insomnia can worsen BPD symptoms via interference with emotional regulation. BPD itself seems to influence the subjective quality of sleep significantly. Proper diagnosis and treatment of sleep disorders in patients with BPD could lead to better results in therapy. Psychotherapeutic approaches can improve both sleep disorders and BPD symptoms.
Conclusion: Recognising and managing sleep disorders in patients with BPD may help alleviate the disorder’s symptoms. Treatment of people with BPD may be more effective if the treatment plan explicitly addresses sleep problems. Further research is needed to reach reliable conclusions.
Keywords: insomnia, borderline personality disorder, cognitive behavioral therapy, dialectic behavioral therapy, transference focus therapy, mentalization therapy
Introduction
Individuals with borderline personality disorder (BPD) are characterised by marked mood and affect instability, impulsivity, instability of self-concept, and impaired, unstable interpersonal relationships.1,2 The lifetime prevalence in the population of BPD is around 2.8%.3–6 Prevalence is significantly higher among individuals seeking help in healthcare; patients with BPD make up to 15–28% of patients in psychiatric outpatient clinics or hospitals, 6% of primary care visits, and 10–15% emergency room visits.7–9
Due to high levels of substance abuse,10,11 self-harm behaviour,12 lifestyle and nutrition irregularities,13,14 people with borderline personality disorder are at risk of many negative consequences for physical health15 and severe chronic diseases such as heart disease, diabetes, arthritis, and chronic sleep problems.16–18 BPD is associated with obesity which has been related to many other somatic health problems.17,19
In the aetiology of BPD, the interaction of genetic and environmental factors is considered to result in changes in brain development.20,21 Genes involved in the aetiology of BPD overlap with genes for major depression, bipolar disorder, and schizophrenia.22,23 Environmental risk factors include adverse events, childhood trauma or abuse, insecure caregiver attachments, and childhood or adolescent psychopathology.20,24 Changes in neuronal circuits associated with BPD symptoms are expected.25,26 Some authors discussed the association of BPD and affected neural areas includes regions involved in understanding the mental state of others and themselves,27,28 circuits mediating pain experience,29 reward systems, and a limbic system with circuits regulating emotions and behaviour.30
First-line treatment of patients with BPD is psychotherapy, such as dialectical behavioural therapy (DBT),31–33 transference-oriented psychotherapy (TFP),34–36 mentalisation-based therapy (MBT)37–39 and schema therapy (ST).40–42 DBT focuses on treating BPD’s observable symptoms while MBT, TFP, and ST focus on improving the patient’s understanding of their motives, feelings, and experiences. Less intensive general treatment models can help to address considerable unavailability of specialists in intensive treatment models.43,44 Comorbid BPD may interfere with treating other disorders, such as depression, obsessive-compulsive disorder, social phobia, or panic disorder. In contrast, other comorbid conditions, such as substance abuse and antisocial personality disorder, may impair treatment effectiveness in BPD patients.45,46
BPD symptoms are often associated with sleep problems.47–49 Sleep problems themselves present a significant burden and are associated with an increased risk of stressful life events, mood disorders, health, family, work, and school problems.50,51
This review was designed to summarise the current state of knowledge about sleep disorders in patients with borderline personality disorder (BPD) via assessment of contemporary literature and scientific databases and provide clinical recommendations for the management of sleep disorders in BPD patients.:
(1) How common is insomnia in patients with a borderline personality disorder?
(2) What is the etiopathogenesis of the comorbidity between insomnia and borderline personality disorders. Are there some mechanisms by which these disorders are affected?
(3) Does insomnia change during the Treatment of a borderline disorder?
(4) Do the manifestations of borderline personality disorder change during insomnia treatment?
Method
Articles were acquired via PubMed and Web of Science, and papers between January 1980 and October 2020 were extracted. Authors made a series of literature searches in PubMed and Web of Science databases, using the following keywords or items in indexed fields: Sleep problems, Insomnia, Nightmares, Obstructive sleep apnea, Borderline personality disorder. All keywords were used in all possible permutations and abstracts from the results of searches were assessed. Selected papers had to meet following inclusion criteria: (1) published in peer-reviewed journals; (2) studies in humans; or (3) reviews on the related topic; (4) English language. The exclusion criteria were: (1) commentaries; (2) abstracts from conferences; (3) subjects younger than 18 years. In the next step, the full text of eligible articles was obtained and assessed. More articles were extracted from the reference list of primary articles. After a full-text assessment of all articles by the research team, their inclusion was subjected to open discussion and decision by the research team.
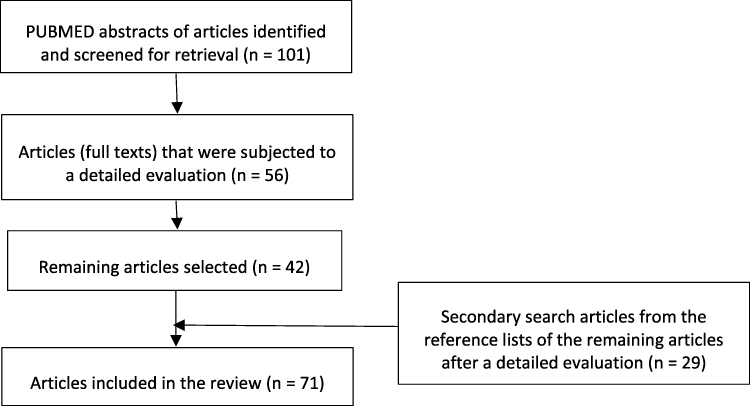 |
Figure 1 Summary of the selection process. |
Results
The total of 101 articles was nominated by primary assortment using keywords in different combinations. After the assortment, 56 papers were chosen according to the inclusion and exclusion criteria. After an inspection of the full texts, 42 papers were selected. Secondary documents from the reference lists of the primary designated papers were examined, evaluated for appropriateness, and added to the documents’ first list (n = 71). In total, 110 papers were included in the review process (Figure 1), in consistency with the PRISMA guidelines.52
Despite the high prevalence of sleep-related disorders in patients with BPD, this aspect of BPD has been neglected in clinical and research settings.53
Comorbidity of Borderline Personality Disorder and Insomnia
Bell et al compared patients with BPD and major depressive disorder (MDD) (n = 15, 10 women) to patients with MDD without current or past borderline characteristics (n = 18, 10 women) on sleep quality and duration, including delta percentage and percentage of REM sleep. No differences were seen among the groups. However, when the depressive symptoms resolved, one of the 13 dependent variables (REM latency) was significantly different. Patients with BPD-MDD showed shorter REM latency compared to patients with MDD alone.54
Benson et al obtained objective sleep values from (a) individuals diagnosed with BPD and past or current diagnosis of major depressive disorder (MDD) or bipolar disorder (BD; n = 8, all men), (b) individuals diagnosed with BPD without past/current diagnosis of MDD or past/present BD (n = 10, all men) and (c) age- and sex-matched healthy controls (n = 15, all men). Authors found no differences between BPD groups and sleep latency control group in REM. Compared to controls, both BPD groups had less total sleep, more Phase 1 sleep, and less Phase 4 sleep. However, differences in sleep between the two BPD groups were not tested.55
Some studies emphasise the connection between borderline personality disorder (BPD) and sleep disorders.47,56 Because depressive symptoms often co-occur with BPD,57,58 some researchers have examined whether the deterioration in BPD patients’ sleep quality can be explained mainly by comorbid depressive symptoms.47,54,55,59,60
Only a few studies are available on individuals with BPD and their sleep.54,59–66 They generally focused on characterising sleep in people with BPD, considering their personality peculiarities. In previous studies, a shortened latency of REM54,61 and a higher REM density54,65 were observed in BPD patients than controls. These results suggest that patients with BPD share common sleep and biological features with severely depressed patients. Even when adjusted for depression, most studies found either shortened REM latency or increased REM density in BPD. Further, Philipsen et al observed greater delta power in the sleep microstructure of NREM in BPD individuals with participants having no history or symptoms of concomitant affective disorders at the time of assessment.66
The effect of various drugs on sleep was rarely considered in previous studies; thus, although BPD individuals differ from controls, it is possible that medications further alter sleep architecture. However, individuals with BPD appear to exhibit the differences in sleep when assessed by polysomnography (PSG). The results obtained in individuals with BPD show a very heterogeneous group of poor sleepers. Philipsen et al observed that patients with BPD reported worse sleep quality than controls in the Pittsburgh Sleep Quality Index (PSQI). However, during laboratory recordings, BPD subjects did not differ from the control group in clinical sleep measurements (total awakening and sleep time, sleep latency, and sleep efficiency), while still reporting poorer sleep quality.66 In the same investigation, a lower percentage of Phase 2 was observed in patients with BPD than in healthy controls.66 Although these results are impressive, clinical sleep measurements were evaluated for only one night. Also, a phase 2 reduction was achieved only by comparing the adaptation night with the base night. This observation could be associated with the first-night effect artefact. It is possible that multiple records would show different results.
De la Fuente et al found differences in sleep patterns in patients with BPD without concomitant depression (n = 20, 14 women), patients with MDD (n = 20; 15 women), and controls (n = 20, 14 women) corresponding to age and sex.64 Contrary to the conclusions of Philipsen et al, De la Fuente et al found several other objective differences between BPD and controls. The BPD and MDD groups had lower overall sleep, longer sleep latency, and greater alertness than controls. However, the sleep of patients with BPD was characterised by the greater proportion of REM sleep and shorter Stage 3 and Stage 4 sleep than patients with MDD and controls.64,66 Furthermore, when dividing the BPD group, BPD patients with a history of MDD in the past (n = 9) showed more alertness and less slow sleep than BPD patients without such a history (n = 11). The authors concluded that while participants with BPD and MDD had similar sleep continuity, groups could be distinguished by sleep architecture.
Asaad et al compared objective and subjective sleep quality measures obtained in individuals diagnosed with BPD without comorbid depressive symptoms (n = 20, 12 women); individuals diagnosed with depressive symptoms without comorbid BPD (n = 20, 12 women), and age and gender-matched healthy controls (n = 20, 12 women). Patients in the depressed group and 45% in the BPD alone group reported significant sleep problems, while only 10% of controls reported subjective sleep problems. The researchers also used polysomnographic equipment to identify where the three groups differed. Participants with depression showed significantly reduced sleep latency, sleep efficiency, and the number of arousals than the BPD and control groups. Sleep latency and sleep efficiency were also significantly worse in the BPD group than controls, but there was no difference in the number of arousals.47
To elucidate the biological nature of depressive symptoms in BPD, de la Fuente et al examined the properties of S-EEG in 24 patients with BPD, RBD (brief recurrent depression), MDD (major depression), and controls. Patients with BPD differed in sleep continuity, especially in sleep architecture compared to RBD, MDD, and control subjects. BPD patients with or without RBD had less slow sleep events than patients with MDD and non-borderline patients with RBD. The authors conclude that although patients with BPD may have concomitant MDD, they often exhibit a specific affective syndrome associated with BPD that differs in the quality and duration of symptoms and biological substrate from MDD and non-borderline RBD.60
Many pre-2010 studies examining the relationship between BPD and sleep problems, independent of depression, were performed on small atypical samples with mixed results.59 Harty et al study expanded the literature by using a much larger sample and statistical control of depression and substance dependence. Subjective reports of sleep problems were obtained from 513 prisoners (70% men). Symptoms of BPD have been significantly associated with sleep problems even when controlled for depression. Substance dependence has been ruled out as the proximal cause of this relationship. Thus, the sleep problems associated with BPD cannot be attributed solely to the comorbid symptoms of depression.49
Despite the clinically observed comorbidity between sleep disorders and impulsivity-related disorders, such as borderline personality disorder,67 the exact relationships between the personality construct of impulsivity and insomnia have not been sufficiently investigated.
Schredl et al compared 27 untreated female BPD subjects and healthy controls. Patients showed increased sleep fragmentation, increased REM density, and decreased REM latency. The findings were independent of the comorbid post-traumatic stress disorder (PTSD) present in 33% of the patient sample. Negatively toned dreams obtained by REM awakening and nightmares have also been reported more frequently in patients – also regardless of the comorbid PTSD – dreams of specific BPD behaviours such as self-harm were rare.68
Simor & Horváth showed that sleep disorders predominate in BPD, including sleep fragmentation, slow-wave and REM sleep changes, and dysphoric dreaming. Specific sleep disorders in BPD appear to be associated with various psychopathological functioning dimensions and may have detrimental consequences for arousal and cognitive abilities.69
Selby (2013) analysed data (N = 5692) from Part II of the National Comorbidity-Replication Survey (NCS-R)70 and assessed individuals with personality disorders and sleep problems. BPD was significantly associated with all three evaluated chronic sleep problems (difficulty initiating sleep, difficulty maintaining sleep, and waking earlier than desired) and the consequences of poor sleep. The extent of the association between BPD and sleep problems was comparable to that of Axis I disorders traditionally associated with sleep problems. BPD symptoms interacted with chronic sleep problems and predicted increased social/emotional, cognitive, and self-care disorders. Sleep disorders are associated with the symptoms of BPD as well as the daily consequences of poor sleep. There may also be a synergistic effect if BPD symptoms worsen with poor sleep and lead to higher functional impairment degrees.71
Most individuals diagnosed with BPD have been exposed to severe and traumatic stressors, and therefore, often show post-traumatic stress disorder (PTSD).18 BPD is highlighted as a high-risk subgroup of PTSD due to increased insomnia and suicidal tendencies.72 In addition to the effects of comorbid depression and anxiety symptoms, emerging evidence has identified impulsivity and emotional dysregulation as possible mechanisms leading to an association between insomnia and suicide in BPD.72
Previous studies of sleep quality have shown that sleep problems are characteristic of younger individuals with borderline pathology.47,48,66,68 Philipsen et al found in a sample of 20 patients without depression that, compared to controls, patients with BPD complained of significantly reduced overall sleep quality and significantly reduced sleep time, sleep efficiency, and worse evening mood.66 Self-reported sleep quality was also significantly impaired in a study of 27 depressed patients with BPD. Patients reported significantly more sleep awakenings, awakenings, time awakenings, and overall sleep quality problems.68
Concerning the finding of shortened REM latency associated with major depression,73 four studies replicated this finding in patients with BPD compared to controls.62,65,68,74 However, four comparable studies did not find a shortened REM latency in patients with BPD than controls.55,64,66,75 Other discrepancies between findings from PSG studies on BPD and sleep are common.76 Interestingly, some PSG findings are consistent with the self-reported results, suggesting that there is convergent evidence for a relationship between borderline pathology and sleep problems in younger adults.
Prevalence of Borderline Personality Disorder and Insomnia
Asaad et al reported that 45% of 20 depressed patients with BPD complained of sleep problems compared with only 10% of controls.47 Examining a larger sample of 513 prisoners (70% men), Harty et al found that borderline pathology significantly correlated with sleep problems in the personality assessment inventory (Morey 1991).49 Asaad et al reported a mean age at 20 years, Harty et al reported a mean age of 32 years.47,49 Overall, this evidence demonstrates that severe sleep problems are common in younger adults with borderline personality pathology.
Oltmanns et al in a representative sample of older adults’ community (N = 633; mean age = 62.3 years) obtained questionnaire reports, self-reports, and informative reports on personality pathology along with an insomnia symptom questionnaire. Cross-sectional analyses revealed that symptoms from all ten DSM-IV personality disorders were significantly correlated with insomnia symptoms. However, after statistical control for major depression, body mass index, race, and gender, only borderline personality pathology remained significantly connected with insomnia.77 These results show that, in addition to other adverse health outcomes, borderline personality pathology is also uniquely associated with sleep problems in older adults.
The current findings complement the findings reported by Selby (2013), obtained from a large sample of the national comorbidity survey who were 18 years of age or older. In this study, BPD symptoms were assessed with a self-report questionnaire. This multi-method procedure provides a more thorough assessment of personality pathology and strongly suggests that the previously reported link between sleep problems and borderline symptoms exists. However, it remains unclear whether borderline pathology’s more specific characteristics are responsible for related sleep problems. Borderline symptoms are related to a person’s temperament. This form of emotional dysregulation may be different from emotional problems characterised by depression and are uniquely associated with sleep disorders. The outcomes of the regression analysis show the shared variance of the personality pathology in predicting sleep disturbances.70
Somma et al showed that the prevalence of personality disorders in their sample of 171 consecutive insomnia patients was significantly higher than the mean and median baseline estimates for any personality disorder in the general population.78
An important future research direction will be a more in-depth investigation of possible mediating and moderating effects on the relationship between borderline symptoms and sleep problems. Physical factors, such as pain, stress, and illness, affect sleep quality51,79,80 and may be more common in people with borderline pathology.
Nightmares
There is a strong association between BPD, nightmares, and subjective sleep quality.48 Patients with BPD suffer from significantly more nightmares, increased dream anxiety, and impaired sleep quality than controls.48 In the borderline group, increased dream anxiety was correlated with higher rates of early traumatic experiences and dissociative symptoms and deteriorating sleep quality. Besides, borderline patients with nightmares showed more significant psychopathology compared to patients without nightmares.48
Consequences of Comorbidity of Borderline Personality Disorder and Insomnia
Emotional Dysregulation
A borderline personality disorder is characterised by frequent shifts in affective state 80 and high impulsivity levels.81 One of the reasons for affective instability in these individuals may be insufficient persistence in the application of emotional regulation, i.e. too high flexibility of affect regulation.82
Emotional dysregulation seems to be involved in a mutually aggravating relationship between borderline personality disorder (BPD) and insomnia.48 Insomnia-related problems are common in BPD and exacerbate the core symptom of BPD - emotional dysregulation. Insomnia is induced and maintained through behaviours that disrupt the homeostatic and circadian sleep systems. However, it is unclear what alteration in homeostatic or circadian mechanisms is present in BPD and impairs emotions regulation. Fitzpatrick et al investigated whether homeostatic (i.e., sleep time abnormalities and sleep efficiency) and circadian (i.e., timing and chronotype abnormalities) characterise and exacerbate emotional dysregulation in patients with borderline personality disorders compared to healthy controls and patients with a generalised anxiety disorder. Community participants, who met the criteria for BPD, generalised anxiety disorder, or no mental disorder (healthy controls), were recruited. Participants completed emotion regulation measurements and measurements of daily homeostatic and circadian behaviour in insomnia for 14 days. The generalised anxiety disorder group showed lower sleep efficiency than healthy controls, and the time lag was significant in patients with borderline personality disorder relative to the generalised anxiety disorder group. More extended bedtime predicted increased emotional dysregulation in healthy controls but lower emotional dysregulation in the generalised anxiety disorder group. Higher sleep efficiency predicted higher emotional dysregulation in borderline personality disorder.83
Studies of sleep disorders and patients with personality disorders consistently show a relationship between personality disorders characterised by behavioral disorders and emotional dysregulation (traditionally called group B personality disorders) and poor sleep. This result is consistent with earlier studies linking insomnia to impulsive behavior, as it is a fundamental characteristic of both antisocial and borderline personality disorders. Van Veen et al examined a group (n = 112) of forensic psychiatric patients with the antisocial or borderline personality disorder or their features. Subjective sleep characteristics and impulsivity were assessed using the Pittsburgh Sleep Quality Index, the Sleep Diagnosis List, and the Barratt Impulsiveness Scale. More than half of patients (53.6%) reported poor sleep quality, and 22.3% appeared to suffer from chronic insomnia. Both poor sleep quality and chronic insomnia were significantly related to impulsivity, especially with attention’s impulsivity. This association was not significantly affected by comorbid disorders.
Active Treatment of sleep problems in these patients can improve sleep quality, mental health and physical well-being and influence the health risks associated with impulsivity by increasing self-control.84
Self-Harm
Non-suicidal self-injury (NSSI), intentional destruction, injury, or deformation of body tissue that is not socially sanctioned and is performed without conscious suicidal intent,85 is usually involved in adolescents and young adults to alleviate intense emotional states.86 It seems that NSSI may precede the combination of a reduced positive affect and an increased negative affect.87 In the early work, Gratz et al noted that low positive emotional intensity reliably distinguishes participants with a history of frequent NSSI from those with no history of NSSI.88
Research has shown a positive relationship between sleep disorders (e.g., nightmares and insomnia) and suicidal behaviour; however, the relationship between NSSI and sleeps disorders in borderline personality disorders has not been studied. A positive relationship has been confirmed in adolescents.89 Sleep disorders have been found to play a causal role in emotional dysfunction problems. In particular, sleep disorders inhibit the function of sleep in processing emotions. Notably, most individuals engage with NSSI to regulate intense emotions, and sleep disorders may increase susceptibility to NSSI by contributing to dysregulated emotions.89
Ennis et al investigated in two cross-sectional studies whether the symptoms of insomnia and nightmares were related to NSSI in a clinical sample (Study 1; N = 313) and a university sample (Study 2; N = 152). The findings showed that nightmares but not symptoms of insomnia were associated with NSSI. This pattern of findings was identical for both clinical and university samples, emphasising the robustness of the finding. Furthermore, the relationship between nightmares and NSSI was fully mediated by emotional dysregulation.90
Suicidality
While BPD features are highly associated with suicidal ideation and attempts, these behaviours could be enhanced or increased in individuals with sleep disorders.
Many studies have found an association between symptoms of insomnia and nightmares and suicidal thoughts or completed suicide in adults.91–95 As many as 10% of patients with BPD die because of suicide.96 Prospective studies report a statistically significant relative risk of suicide deaths of up to 2.4% in people with insomnia.97 Insomnia was the most common sleep disorder associated with suicide, as well as nightmares. These associations generally persisted after correcting for the severity of depression.95 Paris et al found a relationship between the intensity of suicidal thoughts and insomnia symptoms. The result that insomnia is a risk factor for suicide raises the question of the mediating variables that confer this risk.95 One of the candidate mediators is a sleep-specific cognitive impairment which often occurs in insomnia. These cognitive biases, as well as those associated with hopelessness, are potentially modifiable with Treatment.93 The dysfunctional sleep beliefs have been identified in depressed patients with insomnia.98 Treatment of insomnia with cognitive behavioural therapy for insomnia (CBT-I) reduces feelings of hopelessness once the symptoms of insomnia have resolved.99,100 Another potential mediating factor is nightmares, as nightmares have been repeatedly reported to be associated with suicidal thoughts.95,97,101 The degree to which these associations apply to patients with a borderline personality disorder is unclear.
Weibel et al compared adult patients with ADHD with control subjects and individuals with a borderline personality disorder (BPD). Patients with ADHD and BPD had higher insomnia and lower sleep quality scores than controls. Clinical groups did not differ in sleep quality, although insomnia was more severe in patients with BPD. The depression score explained most of the symptoms of sleep score variance. The symptoms of BPD mildly to highly correlated with the risk of suicide, insomnia, and nightmares.102
The DeShong & Tucker study (2019) purpose was to assess BPD symptoms’ potential indirect effect on suicide risk through insomnia and nightmares. Participants (N = 281) were recruited through Amazon’s Mechanical Turk to complete a distance study online. Participants completed an evaluation of the features and symptoms of BPD and suicidal risk (history of suicidal thoughts and features). Symptoms mildly to highly correlated with the risk of suicide, insomnia, and nightmares. In parallel models of mediation, BPD symptoms showed a significant indirect effect on suicidal risk through insomnia symptoms but not nightmares.103 The main limitation of this investigation was a non-clinical sample. Second, the study relied solely on self-assessment. Future studies would benefit from examining these relationships in the clinical population using the observational and interview methods. Features of BPD appear to be associated with an increased risk of suicide concerning sleep problems, especially insomnia symptoms. Therefore, the evaluation and treatment of sleep problems in individuals with BPD may potentially lead to a lower risk of suicide.
Substance Use Disorders
Since BPD and other psychiatric disorders are often associated with the use of drugs or other substances, it is also essential to examine the link between substance use disorders (SUDs) and insomnia. SUD can disrupt sleep and promote insomnia, which in turn can increase motivation to use substances. It has also been shown that insomnia precedes (i.e. predicts) SUD and may be present during withdrawal.104 These results emphasise the need to evaluate and treat insomnia when working with patients who represent BPD or SUD.
Mechanisms of the Comorbidity of the Borderline Personality Disorder and Insomnia
Simor & Horváth presented a qualitative and theoretical overview of empirical studies that examined the objective and subjective quality of sleep in BPD and various psychiatric conditions showing high comorbidity with this disorder. They provide a framework related to specific sleep changes to BPD pathology’s basic dimensions to elucidate inconsistencies in the various findings. Specific sleep disorders in BPD appear to be associated with various psychopathological functioning dimensions and may have detrimental consequences for alertness and cognition.69
These disorders result from the interaction of personality traits, concomitant and comorbid diseases, and environmental factors. Sleep problems are clinically relevant to BPD because they are associated with functional impairment16 and emotional dysregulation.70,105
De la Fuente et al hypothesised that depressive symptoms in BPD might have a biological substrate that is different from those in depressive disorders without comorbid BPD. It has been suggested that RBD (brief recurrent depression) overlaps with BPD which has been found to share disrupted biological substrates with major depression (MD), but the authors did not find the same biological pattern in BPD. When comparing the endocrinological data in BPD, MD and RBD, no biological links were found between BPD and RBD.60
Psychotherapeutic Strategies and Nightmares in BPD
The most researched therapeutic approach to the Treatment of nightmares is cognitive behavioural therapy. Several techniques of cognitive behavioural therapy (CBT) are useful in alleviating nightmare symptoms.106–108
Dialectical Behavioural Therapy
Dialectical behavioural therapy (DBT) is currently the only psychotherapy for BPD that specifically addresses sleep problems.70 Improving the sleep of patients with BPD can help improve their ability to cope with stressful situations, use coping skills, and improve overall energy levels and positive impact. Improving the ability to manage stress, in turn, can reduce sleep problems.109
Exposure Therapy
Narrative exposure therapy (NET) is an evidence-based method for the therapy of trauma-related psychological disorders. To study the effect of NET on sleep in patients with BPD and comorbid PTSD, Weinhold et al screened hospitalised and outpatient patients who met the criteria for inclusion of both diagnoses according to DSM-IV and had stable medication intake for at least two weeks. Patients were divided into NET (N = 13) or treatment as usual (TAU; N = 8) groups. Polysomnography and psychological questionnaires were performed before, after, and six months following up after the last therapeutic session. This pilot research aimed to investigate NET trauma therapy’s efficacy on sleep rate (total sleep time) and sleep continuity (sleep and wake efficiency) in patients with comorbid BPDs and PTSD. Compared to those who received TAU, NET participants showed a reduction in sleep latency from baseline to the end of Treatment and reduced agitation over time.18 NET is unlikely to change sleep for the worse during therapy and appears to improve sleep. These results further demonstrate the effect of baseline sleep structure on treatment success.
Persistent Nightmares in Childhood and Borderline Personality Disorder in Adolescence
Sufficient sleep in childhood is crucial for optimal cognitive and emotional functioning, and the probable relation of sleep with frontal lobe functions is particularly significant in early childhood when the brain exhibits substantial dynamic plasticity. Early behavioural disorders may be modifiable risk factors associated with future psychopathological symptoms. This supports the need to investigate childhood sleep association with mental disorders, such as BPD, during adolescence. Persistent childhood nightmares have been potentially associated with borderline personality disorder (BPD) in adolescence.110
Conclusion
Future research would recommend studies to objectively assess changes in sleep duration and sleep architecture via polysomnography on a larger sample of BPD patients, leading to a better understanding of the relationship between BPD and sleep disorders. Another possible direction is an observational study in a larger sample of BPD patients with and without sleep complaints to further clarify the actual prevalence of sleep disorders in BPD patients as literature provides a relatively wide range of prevalence.
Examination of sleep disturbance in BPD concerning waking symptoms and underlying neuronal function would shed more lights on this multifaceted disorder’s nature. The effect of insomnia on emotional dysregulation in borderline personality disorder is heterogeneous. Idiographic evaluation of the effect of insomnia on emotional dysregulation is also recommended.
It seems that proper diagnosis and treatment of sleep disorders in patients with BPD could lead to better therapy results. To date, there is little agreement concerning the sleep characteristics of BPD and several confounding factors, which makes the explanation of the results difficult. Recognising and managing dreaming and sleep disorders in patients with BPD may help alleviate the disorder’s symptoms. Treatment of people with BPD may be more effective if the treatment plan explicitly addresses sleep problems.
Clinically, monitoring for sleep problems and related disorders may be necessary for therapy, and it may be helpful to thoroughly cover aspects of sleep hygiene as a routine part of treatment for people with BPD. Screening and interventions that address insomnia and these related psychological mechanisms can offer a new way to reduce suicide risk.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Loranger AW, Janca A, Sartorius N. Assessment and Diagnosis of Personality Disorders: The ICD-10 International Personality Disorder Examination (IPDE). Cambridge: Cambridge University Press; 1997.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Ed.; Text Revision. Washington DC, USA: American Psychiatric Press; 2013.
3. Kraus G, Reynold DJ. The “A-B-C’s” of the cluster B’s: identifying, understanding, and treating cluster B personality disorders. Clin Psychol Rev. 2001;21(3):345–373. doi:10.1016/S0272-7358(99)00052-5
4. Lenzenweger MF. Epidemiology of personality disorders. Psychiatr Clin North Am. 2008;31(3):395–403. doi:10.1016/j.psc.2008.03.003
5. McGilloway A, Hall RE, Lee T, Bhui KS. A systematic review of personality disorder, race and ethnicity: prevalence, aetiology and treatment. BMC Psychiatry. 2010;10:33. doi:10.1186/1471-244X-10-33
6. Newton-Howes G, Cunningham R, Atkinson J. Personality disorder prevalence and correlates in a whole of nation dataset. Soc Psychiatry Psychiatr Epidemiol. 2020. doi:10.1007/s00127-020-01876-y
7. Zimmerman M, Rothschild L, Chelminski I. The prevalence of DSM-IV personality disorders in psychiatric outpatients. Am J Psychiatry. 2005;162:1911–1918. doi:10.1176/appi.ajp.162.10.1911
8. Zimmerman M, Chelminski I, Young D. The frequency of personality disorders in psychiatric patients. Psychiatr Clin North Am. 2008;31(3):405–420. doi:10.1016/j.psc.2008.03.015
9. Shaikh U, Qamar I, Jafry F, et al. Patients with borderline personality disorder in emergency departments. Front Psychiatry. 2017;8:136. doi:10.3389/fpsyt.2017.00136
10. Hatzitaskos P, Soldatos CR, Kokkevi A, Stefanis CN. Substance abuse patterns and their association with psychopathology and type of hostility in make patients with BPD and ASPD. Compr Psychiatry. 1999;40(4):278–282. doi:10.1016/S0010-440X(99)90128-1
11. McCann RA, Ball EM. DBT with an inpatient forensic population: the CMHIP forensic model. Cogn Behav Pract. 2000;7:447–456. doi:10.1016/S1077-7229(00)80056-5
12. Wilkins J, Coid JW. Self-mutilation in female remanded prisoners I: an indicator of severe psychopathology. Criminal Behav Mental Health. 1991;1:247–267. doi:10.1002/cbm.1991.1.3.247
13. Keuroghlian AS, Frankenburg FR, Zanarini MC. The relationship of chronic medical illnesses, poor health-related lifestyle choices, and health care utilisation to recovery status in borderline patients over a decade of prospective follow-up. J Psychiatr Res. 2013;47(10):1499–1506. doi:10.1016/j.jpsychires.2013.06.012
14. Redondo-Useros N, Nova E, González-Zancada N, Díaz LE, Gómez-Martínez S, Marcos A. Microbiota and lifestyle: a special focus on diet. Nutrients. 2020;12(6):1776. doi:10.3390/nu12061776
15. Gratz KL, Weiss NH, McDermott MJ, Dilillo D, Messman-Moore T, Tull MT. Emotion dysregulation mediates the relation between borderline personality disorder symptoms and later physical health symptoms. J Pers Disord. 2017;31(4):433–448. doi:10.1521/pedi_2016_30_252
16. Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler RC. Sleep problems, comorbid mental disorders, and role functioning in the national comorbidity survey replication. Biol Psychiatry. 2006;60(12):1364–1371. doi:10.1016/j.biopsych.2006.05.039
17. Powers AD, Oltmanns TF. Borderline personality pathology and chronic health problems in later adulthood: the mediating role of obesity. Personal Disord. 2013;4(2):152–159. doi:10.1037/a0028709
18. Weinhold SL, Göder R, Pabst A, et al. Sleep recordings in individuals with borderline personality disorder before and after trauma therapy. J Neural Transm (Vienna). 2017;124(Suppl 1):99–107. doi:10.1007/s00702-016-1536-3
19. Cruitt PJ, Boudreaux MJ, Jackson JJ, Oltmanns TF. Borderline personality pathology and physical health: the role of employment. Personal Disord. 2018;9(1):73–80. doi:10.1037/per0000211
20. Cattane N, Rossi R, Lanfredi M, Cattaneo A. Borderline personality disorder and childhood trauma: exploring the affected biological systems and mechanisms. BMC Psychiatry. 2017;17(1):221. doi:10.1186/s12888-017-1383-2
21. Fatimah H, Wiernik BM, Gorey C, McGue M, Iacono WG, Bornovalova MA. Familial factors and the risk of borderline personality pathology: genetic and environmental transmission. Psychol Med. 2019;1–11. doi:10.1017/S0033291719001260
22. Paquette AG, Marsit CJ. The developmental basis of epigenetic regulation of HTR2A and psychiatric outcomes. J Cell Biochem. 2014;115(12):2065–2072. doi:10.1002/jcb.24883
23. Sh W, Streit F, Jungkunz M, et al. Genome-wide association study of borderline personality disorder reveals genetic overlap with bipolar disorder, major depression and schizophrenia. Transl Psychiatry. 2017;7(6):e1155. doi:10.1038/tp.2017.115
24. Martín-Blanco A, Ferrer M, Soler J, et al. The role of hypothalamus-pituitary-adrenal genes and childhood trauma in borderline personality disorder. Eur Arch Psychiatry Clin Neurosci. 2016;266(4):307–316. doi:10.1007/s00406-015-0612-2
25. Perez DL, Vago DR, Pan H, et al. Front-limbic neural circuit changes in emotional processing and inhibitory control associated with clinical improvement following transference-focused psychotherapy in borderline personality disorder. Psychiatry Clin Neurosci. 2016;70(1):51–61. doi:10.1111/pcn.12357
26. Herpertz SC, Schneider I, Schmahl C, Bertsch K. Neurobiological mechanisms mediating emotion dysregulation as targets of change in borderline personality disorder. Psychopathology. 2018;51(2):96–104. doi:10.1159/000488357
27. Soloff PH, White R, Omari A, Ramaseshan K, Diwadkar VA. Affective context interferes with brain responses during cognitive processing in borderline personality disorder: fMRI evidence. Psychiatry Res. 2015;233(1):23–35. doi:10.1016/j.pscychresns.2015.04.006
28. van Zutphen L, Siep N, Jacob GA, Goebel R, Arntz A. Emotional sensitivity, emotion regulation and impulsivity in borderline personality disorder: a critical review of fMRI studies. Neurosci Biobehav Rev. 2015;51:64–76. doi:10.1016/j.neubiorev.2015.01.001
29. Ducasse D, Courtet P, Olié E. Physical and social pains in borderline disorder and neuroanatomical correlates: a systematic review. Curr Psychiatry Rep. 2014;16(5):443. doi:10.1007/s11920-014-0443-2
30. Dixon-Gordon KL, Tull MT, Hackel LM, Gratz KL. The influence of emotional state on learning from reward and punishment in borderline personality disorder. J Pers Disord. 2018;32(4):433–446. doi:10.1521/pedi_2017_31_299
31. Linehan MM. Cognitive Behavioral Therapy of Borderline Personality Disorder. New York, NY, USA: Guilford; 1993.
32. McMain SF, Links PS, Gnam WH, et al. A randomised trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. Am J Psychiatry. 2009;166(12):1365–1374. doi:10.1176/appi.ajp.2009.09010039
33. McMain SF, Chapman AL, Kuo JR, et al. The effectiveness of 6 versus 12-months of dialectical behaviour therapy for borderline personality disorder: the feasibility of a shorter treatment and evaluating responses (FASTER) trial protocol. BMC Psychiatry. 2018;18(1):230. doi:10.1186/s12888-018-1802-z
34. Kernberg OF, Yeomans FE, Clarkin JF, Levy KN. Transference focused psychotherapy: overview and update. Int J Psychoanal. 2008;89(3):601–620. doi:10.1111/j.1745-8315.2008.00046.x
35. Clarkin JF, Cain NM, Lenzenweger MF. Advances in transference-focused psychotherapy derived from the study of borderline personality disorder: clinical insights with a focus on mechanism. Curr Opin Psychol. 2018;21:80–85. doi:10.1016/j.copsyc.2017.09.008
36. Stern BL, Yeomans F. The psychodynamic treatment of borderline personality disorder: an introduction to transference-focused psychotherapy. Psychiatr Clin North Am. 2018;41(2):207–223. doi:10.1016/j.psc.2018.01.012
37. Bateman A, Fonagy P. Randomized controlled trial of outpatient mentalisation-based treatment versus structured clinical management for borderline personality disorder. Am J Psychiatry. 2009;166(12):1355–1364. doi:10.1176/appi.ajp.2009.09040539
38. Bales D, van Beek N, Smits M, et al. Treatment outcome of 18-month, day hospital mentalisation-based treatment (MBT) in patients with severe borderline personality disorder in the Netherlands. J Pers Disord. 2012;26(4):568–582. doi:10.1521/pedi.2012.26.4.568
39. Daubney M, Bateman A. Mentalisation-based therapy (MBT): an overview. Australas Psychiatry. 2015;23(2):132–135. doi:10.1177/1039856214566830
40. Giesen-Bloo J, van Dyck R, Spinhoven P, et al. Outpatient psychotherapy for borderline personality disorder: randomised trial of schema-focused therapy vs transference-focused psychotherapy. Arch Gen Psychiatry. 2006;63(6):649–658. doi:10.1001/archpsyc.63.6.649
41. Reiss N, Lieb K, Arntz A, Shaw IA, Farrell J. Responding to the treatment challenge of patients with severe BPD: results of three pilot studies of inpatient schema therapy. Behav Cogn Psychother. 2014;42(3):355–367. doi:10.1017/S1352465813000027
42. Tan YM, Lee CW, Averbeck LE, et al. Schema therapy for borderline personality disorder: a qualitative study of patients’ perceptions. PLoS One. 2018;13(11):e0206039. doi:10.1371/journal.pone.0206039
43. Crawford MJ, Thana L, Parker J, et al. Psychological Support for Personality (PSP) versus treatment as usual: study protocol for a feasibility randomised controlled trial of a low intensity intervention for people with personality disorder. Trials. 2018;19(1):547. doi:10.1186/s13063-018-2920-0
44. Zanarini MC, Conkey LC, Temes CM, Fitzmaurice GM. Randomised controlled trial of web-based psychoeducation for women with borderline personality disorder. J Clin Psychiatry. 2018;79(3):16m11153. doi:10.4088/JCP.16m11153
45. Gianoli MO, Jane JS, O’Brien E, Ralevski E. Treatment for comorbid borderline personality disorder and alcohol use disorders: a review of the evidence and future recommendations. Exp Clin Psychopharmacol. 2012;20(4):333–344. doi:10.1037/a0027999
46. Helle AC, Watts AL, Trull TJ, Sher KJ. Alcohol use disorder and antisocial and borderline personality disorders. Alcohol Res. 2019;40(1):
47. Asaad T, Okasha T, Okasha T. Sleep EEG findings in CD-10 borderline personality disorder in Egypt. J Affect Disord. 2002;1:11–18. doi:10.1016/S0165-0327(01)00357-3
48. Semiz UB, Basoglu C, Ebrinc S, Cetin M. Nightmare disorder, dream anxiety, and subjective sleep quality in patients with borderline personality disorder. Psychiatry Clin Neurosci. 2008;62:48–55. doi:10.1111/j.1440-1819.2007.01789.x
49. Harty L, Forkner RD, Thompson A, Stuewig J, Tangney JP. Are inmates’ subjective sleep problems associated with borderline personality, psychopathy, and antisocial personality independent of depression and substance dependence? J Forensic Psychiatry Psychol. 2010;21:23–38. doi:10.1080/14789940903194095
50. Healey ES, Kales A, Monroe LJ, Bixler EO, Chamberlin K, Soldatos CR. Onset of insomnia: role of life-stress events. Psychosom Med. 1981;43:439–451. doi:10.1097/00006842-198110000-00007
51. Bastien CH, Vallieres A, Morin CM. Precipitating factors of insomnia. Behav Sleep Med. 2004;2:50–62. doi:10.1207/s15402010bsm0201_5
52. Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Methods of systematic reviews and meta-analysis preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. J Clin Epidemiol. 2009;62:1006e1012. doi:10.1016/j.jclinepi.2009.06.005
53. Hafizi S. Sleep and borderline personality disorder: a review. Asian J Psychiatr. 2013;6(6):452–459. doi:10.1016/j.ajp.2013.06.016
54. Bell J, Lycaki H, Jones D, Kelwala S, Sitaram N. Effect of preexisting borderline personality disorder on clinical and EEG sleep correlates of depression. Psychiatry Res. 1983;9:115–123. doi:10.1016/0165-1781(83)90033-1
55. Benson KL, King R, Gordon D, Silva JA, Zarcone VP. Sleep patterns in borderline personality disorder. J Affect Disord. 1990;18(4):267–273. doi:10.1016/0165-0327(90)90078-M
56. Maunchnik J, Schmahl C, Bohus M. New findings in the biology of borderline personality disorder. Directions Psychiatry. 2005;25:197–215.
57. Southwick SM, Yehuda R, Giller EL. Psychological dimensions of depression in borderline personality disorder. Am J Psychiatry. 1995;152:789–791.
58. Westin D, Moses MJ, Silk NR, Lohr NE, Cohen R, Segal H. Quality of depressive experience in borderline personality disorder and major depression: when depression is not just depression. J Pers Disord. 1992;6:382–393. doi:10.1521/pedi.1992.6.4.382
59. Battaglia M, Ferini Strambi L, Bertella S, Bajo S, Bellodi L. First-cycle rem density in never-depressed subjects with borderline personality disorder. Biol Psychiatry. 1999;45:1056–1058. doi:10.1016/S0006-3223(98)00213-3
60. De la Fuente JM, Bobes J, Morlan I, et al. Is the biological nature of depressive symptoms in borderline patients without concomitant Axis I pathology idiosyncratic? Sleep EEG comparison with recurrent brief, major depression and control subjects. Psychiatry Res. 2004;129(1):65–73. doi:10.1016/j.psychres.2004.05.025
61. Reynolds CF, Soloff PH, Kupfer DJ. Depression in borderline patients: a prospective EEG sleep study. Psychiatry Res. 1985;14:1–15. doi:10.1016/0165-1781(85)90084-8
62. Battaglia M, Ferini-Strambi L, Smirne S, Bernardeschi L, Bellodi L. Ambulatory polysomnography of never-depressed borderline subjects: a high-risk approach to rapid eye movement latency. Biol Psychiatry. 1993;33:326–334. doi:10.1016/0006-3223(93)90321-4
63. Lahmeyer HW, Val E, Gaviria FM, et al. EEG sleep, lithium transport, dexamethasone suppression, and monoamine oxidase activity in borderline personality disorder. Psychiatry Res. 1998;25:19–30. doi:10.1016/0165-1781(88)90154-0
64. De la Fuente JM, Bobes J, Vizuete C, Mendlewicz J. Sleep-EEG in borderline patients without concomitant major depression: a comparison with major depressives and normal control subjects. Psychiatry Res. 2001;105:87–95. doi:10.1016/S0165-1781(01)00330-4
65. McNamara E, Reynolds CF
66. Philipsen A, Feige B, Al-Shajlawi A, et al. Increased delta power and discrepancies in objective and subjective sleep measurements in borderline personality disorder. J Psychiatr Res. 2005;39:489–498. doi:10.1016/j.jpsychires.2005.01.002
67. Bastien CH, Guimond S, St‐Jean G, Lemelin S. Signs of insomnia in borderline personality disorder individuals. J Clin Sleep Med. 2008;4:462–470. doi:10.5664/jcsm.27283
68. Schredl M, Paul F, Reinhard I, Ebner-Priemer UW, Schmahl C, Bohus M. Sleep and dreaming in patients with borderline personality disorder: a polysomnographic study. Psychiatry Res. 2012;200(2–3):430–436. doi:10.1016/j.psychres.2012.04.036
69. Simor P, Horváth K. Altered sleep in borderline personality disorder in relation to the core dimensions of psychopathology. Scand J Psychol. 2013;54(4):300–312. doi:10.1111/sjop.12048
70. Kessler RC, Merikangas KR. The National Comorbidity Survey Replication (NCS-R): background and aims. Int J Methods Psychiatr Res. 2004;13:60–68. doi:10.1002/mpr.166
71. Selby EA. Chronic sleep disturbances and borderline personality disorder symptoms. J Consult Clin Psychol. 2013;81:941–947. doi:10.1037/a0033201
72. Winsper C, Tang NK. Linkages between insomnia and suicidality: prospective associations, high-risk subgroups and possible psychological mechanisms. Int Rev Psychiatry. 2014;26(2):189–204. doi:10.3109/09540261.2014.881330
73. Giles DE, Roffwarg HP, Rush AJ. A cross-sectional study of the effects of depression on REM latency. Biol Psychiatry. 1990;28(8):697–704. doi:10.1016/0006-3223(90)90456-C
74. Akiskal HS, Yerevanian BI, Davis GC, King D, Lemmi H. The nosologic status of borderline personality: clinical and polysomnographic study. Am J Psychiatry. 1985;142:192–198.
75. Hornung OP, Regen F, Warnstedt C, et al. Declarative and procedural memory consolidation during sleep in patients with borderline personality disorder. J Psychiatr Res. 2008;42:653–658. doi:10.1016/j.jpsychires.2007.07.001
76. Fleischer M, Schafer M, Coogan A, Haßler F, Thome J. Sleep disturbances and circadian CLOCK genes in borderline personality disorder. J Neural Transm. 2012;119:1105–1110. doi:10.1007/s00702-012-0860-5
77. Oltmanns JR, Weinstein Y, Oltmanns TF. Borderline personality pathology and insomnia symptoms in community-dwelling older adults. Personal Ment Health. 2014;8(3):178–187. doi:10.1002/pmh.1259
78. Somma A, Marelli S, Giarolli LE, Maffei C, Ferini-Strambi L, Fossati A. Interview-based ratings of DSM-IV axis II/DSM-5 section II personality disorder symptoms in consecutively admitted insomnia patients: a comparison study with consecutively admitted psychotherapy patients matched on age and gender. Compr Psychiatry. 2018;87:100–106. doi:10.1016/j.comppsych.2018.09.005
79. Ashworth PCH, Davidson KM, Espie CA. Cognitive-behavioural factors associated with sleep quality in chronic pain patients. Behav Sleep Med. 2010;8:28–39. doi:10.1080/15402000903425587
80. Rosenthal MZ, Gratz KL, Kosson DS, Cheavens JS, Lejuez CW, Lynch TR. Borderline personality disorder and emotional responding: a review of the research literature. Clin Psychol Rev. 2008;28(1):
81. Links PS, Heslegrave R, van Reekum R. Impulsivity: core aspect of borderline personality disorder. J Pers Disord. 1999;13:
82. Gross JJ, Uusberg H, Uusberg A. Mental illness and well-being: an affect regulation perspective. World Psychiatry. 2017;18(2):130–139. doi:10.1002/wps.20618
83. Fitzpatrick S, Maich KHG, Carney CE, Kuo JR. Identifying specific insomnia components in borderline personality disorder and their influence on emotion dysregulation. Personal Disord. 2020. doi:10.1037/per0000395
84. Van Veen MM, Karsten J, Lancel M. Poor sleep and its relation to impulsivity in patients with antisocial or borderline personality disorders. Behav Med. 2017;43(3):218–226. doi:10.1080/08964289.2017.1313719
85. Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr Dir Psychol Sci. 2009;18:78–83. doi:10.1111/j.1467-8721.2009.01613.x
86. Bentley KH, Nock MK, Barlow DH. The four-function model of nonsuicidal self-injury: implications for assessment and psychological treatment. Clin Psychol Sci. 2014;2:638–656. doi:10.1177/2167702613514563
87. Selby EA, Joiner TE. Cascades of emotion: the emergence of borderline personality disorder from emotional and behavioral dysregulation. Rev Gen Psychol. 2009;13:219–229. doi:10.1037/a0015687
88. Gratz KL, Rosenthal MZ, Tull MT, Lejuez CW, Gunderson JG. An experimental investigation of emotion dysregulation in borderline personality disorder. J Abnorm Psychol. 2006;115:850–855. doi:10.1037/0021-843X.115.4.850
89. Bandel SL, Brausch AM. Poor sleep associates with recent nonsuicidal self-injury engagement in adolescents. Behav Sleep Med. 2020;18(1):81–90. doi:10.1080/15402002.2018.1545652
90. Ennis CR, Short NA, Moltisanti AJ, Smith CE, Joiner TE, Taylor J. Nightmares and nonsuicidal self-injury: the mediating role of emotional dysregulation. Compr Psychiatry. 2017;76:104–112. doi:10.1016/j.comppsych.2017.04.003
91. Krakow B, Schrader R, Tandberg D, et al. Nightmare frequency in sexual assault survivors with PTSD. J Anxiety Disord. 2002;16:175–190. doi:10.1016/S0887-6185(02)00093-2
92. Bernert R, Joiner T, Cukrowicz K, Schmidt N, Krakow B. Suicidality and sleep disturbances. Sleep. 2005;28:1135–1141. doi:10.1093/sleep/28.9.1135
93. Coryell W, Young EA. Clinical predictors of suicide in primary major depressive disorder. J Clin Psychiatry. 2005;66:412–417. doi:10.4088/JCP.v66n0401
94. Bernert R, Reeve J, Perlis M, Joiner T. Insomnia and nightmares as predictors of elevated suicide risk among patients seeking admission to emergency mental health facility. Sleep. 2009;32:A365–A366.
95. McCall WV. Insomnia is a risk factor for suicide - what are the next steps? Sleep. 2011;34:1149–1150. doi:10.5665/SLEEP.1222
96. Paris J. Suicidality in borderline personality disorder. Medicina (Kaunas). 2019;55(6):E223. doi:10.3390/medicina55060223
97. Fujino Y, Mizoue T, Tokui N, Yoshimura T. Prospective cohort study of stress, life satisfaction, self-rated health, insomnia, and suicide death in Japan. Suicide Life Threat Behav. 2005;35:227–237. doi:10.1521/suli.35.2.227.62876
98. Carney C, Edinger J, Manber R, Garson C, Segal Z. Beliefs about sleep in disorders characterised by sleep and mood disturbance. J Psychosom Res. 2007;62:179–188. doi:10.1016/j.jpsychores.2006.08.006
99. Carney CE, Edinger Jack D. Identifying critical beliefs about sleep in primary insomnia. Sleep. 2006;29:444–453. doi:10.1093/sleep/29.3.342
100. McCall WV, Blocker JN, D’Agostino RB
101. McCall WV, Batson N, Webster M, et al. Nightmares and dysfunctional beliefs about sleep mediate the effect of insomnia symptoms on suicidal ideation. J Clin Sleep Med. 2013;9(2):135–140. doi:10.5664/jcsm.2408
102. Weibel S, Jermann F, Weiner L, et al. Insomnia in adult attention-deficit/hyperactivity disorder: a comparison with borderline personality disorder population in a clinical setting and control participants. Compr Psychiatry. 2017;76:119–128. doi:10.1016/j.comppsych.2017.04.009
103. DeShong HL, Tucker RP. Borderline personality disorder traits and suicide risk: the mediating role of insomnia and nightmares. J Affect Disord. 2019;244:85–91. doi:10.1016/j.jad.2018.10.097
104. Provencher T, Lemyre A, Vallières A, Bastien CH. Insomnia in personality disorders and substance use disorders. Curr Opin Psychol. 2019;34:72–76. doi:10.1016/j.copsyc.2019.10.005
105. Zohar D, Tzischinsky O, Epstein R, Lavie P. The effects of sleep loss on medical residents’ emotional reactions to work events: a cognitive-energy model. SLEEP. 2005;28:47–54. doi:10.1093/sleep/28.1.47
106. Spoormaker VI, Schredl M, van den Bout J. Nightmares: from anxiety symptom to sleep disorder. Sleep Med Rev. 2006;10:19–31. doi:10.1016/j.smrv.2005.06.001
107. Lancee J, Spoormaker VI, Krakow B, van den Bout J. A systematic review of cognitive-behavioral treatment for nightmares: toward a well-established treatment. J Clin Sleep Med. 2008;4:475–480. doi:10.5664/jcsm.27285
108. Vanek J, Prasko J, Ociskova M, et al. Nightmares and their treatment. Neuro Endocrinol Lett. 2020;41(2):86–101.
109. Carlson LE, Garland SN. Impact of mindfulness-based stress reduction (MBSR) on sleep, mood, stress, and fatigue symptoms in cancer outpatients. Int J Behav Med. 2005;12:278–285. doi:10.1207/s15327558ijbm1204_9
110. Morales-Muñoz I, Broome MR, Marwaha S. Association of parent-reported sleep problems in early childhood with psychotic and borderline personality disorder symptoms in adolescence. JAMA Psychiatry. 2020;e201875. doi:10.1001/jamapsychiatry.2020.1875
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.