Back to Journals » Journal of Inflammation Research » Volume 14
Insights into the Implications of Coexisting Type 2 Inflammatory Diseases
Authors McCormick JP, Lee JT
Received 6 July 2021
Accepted for publication 13 August 2021
Published 30 August 2021 Volume 2021:14 Pages 4259—4266
DOI https://doi.org/10.2147/JIR.S311640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Justin P McCormick, Jivianne T Lee
Department of Head and Neck Surgery, University of California Los Angeles David Geffen School of Medicine, Los Angeles, CA, USA
Correspondence: Jivianne T Lee
Department of Head and Neck Surgery, University of California Los Angeles, David Geffen School of Medicine, Los Angeles, CA, USA
Email [email protected]
Abstract: The role of type 2 inflammation in the pathogenesis of certain human diseases is an area of active investigation. Certain asthma, atopic dermatitis, eosinophilic esophagitis, and chronic rhinosinusitis phenotypes are characterized by a Th2 predominant inflammatory pathway and are frequently associated with comorbid conditions in patients. The purpose of this article is to review the evidence behind concurrent Th2-mediated diseases and explore how the presence of these comorbid conditions affect patient and disease outcomes.
Keywords: type 2 inflammation, Th2 inflammation, asthma, atopic dermatitis, eosinophilic esophagitis, chronic rhinosinusitis
Introduction
Inflammation is classically thought to be the body’s defense against infection or injury, thereby maintaining homeostasis.1 The inflammatory cascade is directed by the innate and adaptive immune systems, which are thought to have 3 major classes of cell-mediated effector immunity. The role of type I immunity is primarily protection against intracellular microbes, while type 3 immunity plays a protective role against extracellular bacteria and fungi.2 Recent investigations have suggested that both type I and type 3 immune responses may play a pathogenic role in some human autoimmune diseases, such as rheumatoid arthritis, multiple sclerosis, Hashimoto thyroiditis, inflammatory bowel disease, and others. Type 2 inflammation, long associated with protection against helminth infections is also suggested to play a pathogenic role in some human diseases.2
The type 2 inflammatory response is primarily driven by T-helper 2 (Th2) cells following the presentation of antigen to naïve T-cells. Complex signaling pathways drive Th2 chemotaxis toward the site of inflammation, and stimulate the production of cytokines important in the type 2 inflammatory cascade. Interleukin (IL) 4 promotes the differentiation of naïve Th cells into Th2 cells and is also vital in stimulating isotype class switching of B cells to produce IgE. IgE antibodies further advance the immune response by sensitization of basophils and mast cells. Additional signaling provided by IL-5 and IL-9 leads to eosinophil and mast cell recruitment to the site of inflammation, and IL-13 is engaged in goblet cell hyperplasia, mucus secretion, and airway responsiveness.3 Recently, investigators have recognized that type 2 inflammation may also play a pathogenic role in atopic and other inflammatory diseases.
Type 2 Inflammation in Chronic Disease States
Asthma
Asthma is a disorder resulting in chronic inflammation of the airways, leading to recurrent episodes of wheezing, chest tightness, and coughing.4 Endotype driven classification of asthma has allowed researchers to understand the molecular basis behind inflammation in different subsets of asthma. As such, treatments may be specifically targeted for the relevant molecular mechanism.5 Th2-related asthma is thought to make up about 50% of mild to moderate asthma.6 These patients also tend to be more responsive to glucocorticoid therapy and tend to exhibit local and systemic eosinophilia. However, a subset of Th2 mediated asthma patients do not show significant response to glucocorticoid therapy either due to steroid resistance or significantly high levels of Th2 inflammation that is unable to be controlled with steroids.5 This has led to the development of novel therapeutics targeting the molecular basis behind the inflammation. The advent of biologic therapies for the treatment of type 2 inflammatory diseases has significantly enhanced the outcomes of difficult to treat disease.
Eosinophilic Esophagitis
Eosinophilic esophagitis (EOE) is a disease characterized by esophageal dysfunction histologically associated with eosinophilic type inflammation. Characterized clinically with symptoms of dysphagia, heartburn, abdominal pain, and food avoidance, EOE is often initially misdiagnosed as gastroesophageal reflux disease (GERD).7 However, it is important to understand that these are two distinct clinical entities with differing pathogenesis. Although the pathophysiology of EOE continues to be investigated, it is known that chronic, Th2 mediated inflammation seems to be a major contributing factor to disease propagation.8 Genetic profiling has also suggested that EOE patients may be predisposed to the development of allergic and eosinophilic inflammation in the esophagus. The management of EOE, similar to other type 2 inflammatory diseases, relies on reducing the eosinophilic inflammation within the esophagus. Elimination diets and proton-pump inhibitors have been suggested as potential first-line therapies for the treatment of EOE; however, topical corticosteroids have been the mainstay of therapy.8 While topical steroids tend to have great success with inducing remission of EOE, relapse typically occurs within a few weeks after cessation.9,10 As with other Th2 mediated diseases, biologics targeting IL-5 and IL-13 are currently being investigated as potential treatment options. While trials have shown promise with reducing eosinophil counts and inflammatory markers, symptom improvement has been less predictable.11–14
Atopic Dermatitis (AD)
Atopic dermatitis is a chronic, relapsing inflammatory skin disease characterized by erythematous, pruritic patches. Classically considered a disease of children, it is now known that AD affects people of all ages, and it is estimated that upwards of 230 million people worldwide are diagnosed with AD.15 Genetics, environmental exposures, and immunological factors may all have a role in the pathogenesis of AD and are currently being investigated. The inflammatory profiles of AD demonstrate a Th2 dominance during the acute phases of AD development.16 Messenger ribonucleic acid (mRNA) encoding Th2-specific cytokines, IL-4 and IL-13, are greatly increased in acute lesions and may be involved in some skin barrier dysfunction further exacerbating the disease process.17 The aims of management of AD are focused on establishing persistent disease control by avoiding triggers of disease exacerbations, improving the skin condition, and reducing the inflammation. Basic therapy that all AD patients should be educated on is focused on improving skin health with hydrating topical therapies, emollients, and occlusive dressings. For mild disease, topical corticosteroids continue to be the first-line treatment. Topical calcineurin inhibitors may be used in the short term in sensitive areas. Short-term phototherapy is an option when topical measures fail to achieve disease control. Systemic treatments including immunosuppressive agents, corticosteroids, and biologics are considered when the above measures fail.15
Chronic Rhinosinusitis (CRS)
Chronic rhinosinusitis is a disease of inflammation of the nose and paranasal sinuses characterized by at least 12 weeks of nasal congestion, facial pain or pressure, nasal discharge, and impairment of the sense of smell. CRS is estimated to affect nearly 10% of the adult population and results in significantly decreased quality of life, decreased productivity, and large financial impacts for disease management.18 CRS was classically grouped based on the presence or absence of nasal polyps; however, recent understanding of the underlying inflammatory profiles (ie, endotypes) of CRS has led some to suggest revising this classification scheme.19 CRS with a Th2 endotype tends to be more associated with nasal polyps, smell loss, and allergic mucin, when compared to non-Th2 patients.20 The management of CRS is largely based on appropriate medical management with surgery reserved for patients who do not respond to maximal medical therapy. The term maximal medical therapy has been used to describe a trial of nasal saline irrigations, topical corticosteroid sprays, antibiotics, and occasionally systemic corticosteroids.21 Patients with a Th2 predominant endotype tend to be more responsive to corticosteroid therapy than non-Th2 patients, however, despite adequate surgery and appropriate medical therapy a subset of patients experience persistent disease. The introduction of biologics targeting the type 2 inflammatory pathway has shown promise in treating recalcitrant disease, similar to the other Th2 mediated diseases described above.22
Interplay Between Different Type 2 Inflammatory Diseases
As our understanding of type 2 inflammatory diseases continues to expand, the effect of co-existent diseases on patient outcomes will need to be investigated. The current evidence regarding co-morbid Th2 mediated diseases will be reviewed here-in.
Asthma and EOE
Asthma and EOE are frequently associated, and some have suggested that EOE may be the asthma of the esophagus. Asthma and EOE share many commonalities in that they are both chronic immune mediated conditions, characterized by inflammatory changes within the mucosa and submucosa with a predominant eosinophil infiltrate.23 While the relationship between asthma and EOE remains poorly understood, several database studies have sought to determine the prevalence of co-existent asthma and EOE.24 Within the United States, EOE patients were found to have co-morbid asthma 23.4–37.5% of the time.25–27 The two diseases were found to co-exist more frequently in the pediatric population.27 Other retrospective studies throughout the world have been less clear-cut, reporting that between 12–68% of patients with EOE have a history of asthma.24 Furthermore, a recent systematic review and meta-analysis by Gonzalez-Cervera et al28 found that bronchial asthma is significantly more common among EOE patients of all ages when compared to controls, with an overall odds ratio (OR) of 3.01 (95% CI 1.96–4.62). Similar ORs were found when comparing adults and children separately.
Asthma and AD
The concept of the “atopic march” has been investigated for decades, following clinical observations of co-morbid disease states such as food allergy, allergic rhinitis, and asthma progressing from atopic dermatitis. Although the interplay between AD and asthma continues to be investigated, impaired skin barrier function has been suggested as an entry point for allergen penetration and the further development of atopic disease.29 Additionally, it has since been shown that the presence of atopic dermatitis in children significantly increases the likelihood asthma development.30 Several large database studies out of the US have investigated the prevalence of co-morbid asthma in AD patients. Silverberg and Simpson31 utilized the 2007 National Survey of Children’s Health and found the lifetime and 1-year prevalence of self reported asthma to be 25.1% and 19.8%, respectively. Data from the 2012 National Health Interview Survey reported similar numbers from an adult US population (25.5% and 18.7% for lifetime and 1-year prevalences).32 More recently, a 2018 study reported a 49.8% prevalence of comorbid asthma in AD patients, and calculated a relative risk of 1.73 (95% CI 1.53–1.93).33
Asthma and CRS
While CRS is broadly categorized into two predominant phenotypes [CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP)], recent developments of CRS endotypes have allowed for better understanding of the pathogenesis of disease. CRSwNP patients with Th2 endotypes often have severe disease that is difficult to manage and frequently have comorbid lower airway disease.34 Interestingly, similar inflammatory profiles have been found in nasal polyp specimens and bronchial specimens in CRSwNP patients, indicating the existence of similar inflammation throughout the upper and lower airways in these patients.35 Surprisingly, however, Th2 cytokine concentrations were significantly higher in nasal polyps compared to bronchial specimens, leading the authors to question whether the sinus disease plays an important role in lower airway inflammation.35 Several, large studies have consistently associated asthma with CRSwNP and vice-versa. Results from the Global Allergy and Asthma Network of Excellence, multicenter, population-based survey identified strong, consistent correlations between asthma and CRS among all centers, and calculated an overall OR of 3.48 (95% CI 3.21–3.77). Among patients with CRS, some studies have suggested a 60% prevalence of comorbid lower airway disease.36 Additionally, asthma patients with comorbid CRS have been shown to have higher levels of lower airway inflammation and worse asthma control than those without CRS.37,38
EOE and AD
Although it is the most recently recognized clinical entity of the disease discussed in this manuscript, EOE research has focused on identifying frequently associated comorbid conditions in an attempt to better understand the disease process. Recent studies in the EOE literature have reported prevalence rates of AD between 7%-55% amongst EOE patients.39–42 Additionally, a recent systematic review and meta-analysis compared the frequency of atopic dermatitis between EOE patients and control subjects.28 The authors reported a pooled OR of 2.85 (95% CI: 1.87–4.34), with no significant difference noted when performing subgroup analysis including adult and pediatric patients separately. Genetic analyses have also identified common predisposing factors to EOE and AD, as polymorphisms in thymic stromal lymphopoietin and loss of function mutations in filaggrin, an epithelial differentiation gene, have been shown to increase the risk of both EOE and AD.43 Additionally, recent transcriptome analysis has suggested similar disease mechanisms between EOE and AD.43
EOE and CRS
Until 2016, no studies had specifically investigated the coexistence of EOE and CRS. Utilizing a large genealogical database, however, Padia et al44 were able to investigate this particular association. Amongst patients with CRS, the authors reported a 3.44 times increased risk of having EOE. This risk extended to first degree relatives of the CRS proband (OR 1.45; 95% CI: 1.23–1.71), regardless of whether the relative also carried a CRS diagnosis.44 Reverse comparison starting with EOE patients found that probands with EOE were 2.86 times more likely to have CRS than matched controls. Again, this increased risk was carried to EOE patients first degree relatives with OR 1.48 (95% CI: 1.25–1.76).44
AD and CRS
Despite having less studies investigating the prevalence of comorbid AD and CRS, a few studies have provided supporting data. In a large, retrospective longitudinal cohort study, Tan et al45 identified an association between a pre-morbid diagnosis of AD and the subsequent development of CRS. Similarly, Chandra et al46 reported a significantly increased prevalence of CRSwNP in patients with AD compared with a control population with hypertension. In another study, a reverse comparison was performed and demonstrated that patients with CRS were at a greater risk of developing AD compared to a control population, with a hazard ratio of 2.75 (95% CI: 1.23–6.16).47
Impact of Treatment of Comorbid Type 2 Inflammatory Diseases
As more is discovered about the impact of comorbid inflammatory diseases, researchers will be motivated to investigate how the treatment of comorbid conditions affects patient outcomes.
Although robust studies investigating the effects of concomitant asthma and EOE on disease outcomes are lacking, smaller studies have reported interesting findings. Rajan et al48 found that patients with both EOE and asthma had higher baseline tissue eosinophils than non-asthmatics. Additionally, despite other inflammatory parameters being similar, EOE asthmatics had a higher rate of non-response to anti-inflammatories compared to non-asthmatics. Another retrospective review of asthma patients concluded that the use of inhaled corticosteroids appears to be protective against EOE, speculating that control of the airway disease may be therapeutic in treating EOE, although it is difficult to make such speculations with a single retrospective study.49
Similarly, the implications of comorbid asthma and CRS have been thoroughly investigated. In studies, severe asthmatics with associated CRSwNP require more frequent oral corticosteroid usage when compared to asthmatics without CRS.50 Several other studies have suggested that treatment of CRS may optimize asthma control. Zhang et al51 demonstrated greater quality of life improvement in comorbid CRSwNP and asthma patients after endoscopic sinus surgery compared CRS patients without asthma or polyps. Additionally, Schlosser et al52 reported improved asthma control and asthma-related quality of life following sinus surgery. Despite these findings, it has also been reported that comorbid asthma and CRSwNP are more likely to require a greater number of sinus surgeries than patients with CRSwNP alone.53
The recent introduction of biologics targeting Th2 inflammation will certainly have an impact on the treatment of comorbid inflammatory diseases (Table 1). Studies have already shown promising results with the addition of biologics, with one study demonstrating a 50% reduction in outpatient office visits for atopic disease and CRS in patients with severe asthma after starting mepolizumab, an anti-IL-5 biologic.54 Omalizumab, an anti-IgE monoclonal antibody is currently approved in the US for the treatment of asthma and CRSwNP. Studies investigating the utility of omalizumab in AD have been inconclusive.55 Additionally, dupilumab, which targets the shared receptor subunit for IL-4 and IL-13, has shown good results in the treatment of asthma, AD, and CRS.56 A recent Phase 2 clinical trial has also shown promise in the management of EOE,14 results that other biologic agents have failed to produce up to this point.57 So, while it is clear that we have made great strides over the past few decades in the treatment of Th2 mediated diseases, questions still remain and further research must be conducted to better understand the epidemiological variability across these disease states.
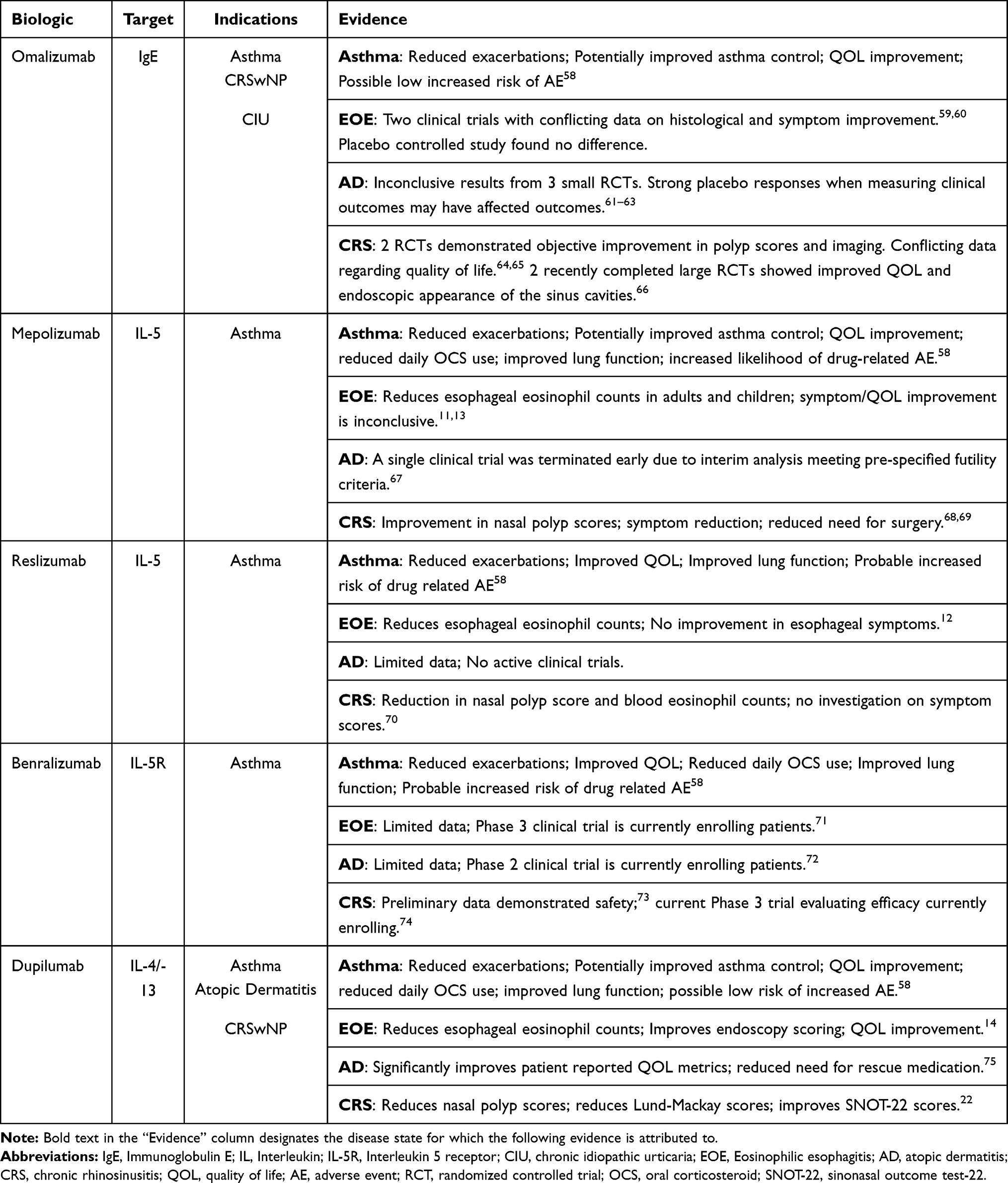 |
Table 1 Biologics in Type 2 Inflammatory Diseases |
Disclosure
Dr Jivianne Lee reports personal fees from Sanofi and Regeneron, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Chovatiya R, Medzhitov R. Stress, inflammation, and defense of homeostasis. Mol Cell. 2014;54:281–288. doi:10.1016/j.molcel.2014.03.030
2. Annunziato F, Romagnani C, Romagnani S. The 3 major types of innate and adaptive cell-mediated effector immunity. J Allergy Clin Immunol. 2015;135(3):626–635. doi:10.1016/j.jaci.2014.11.001
3. Caminati M, Pham DL, Bagnasco D, Canonica GW. Type 2 immunity in asthma. World Allergy Organ J. 2018;11:13. doi:10.1186/s40413-018-0192-5
4. Mims JW. Asthma: definitions and pathophysiology. Int Forum Allergy Rhinol. 2015;5(Suppl 1):S2–6. doi:10.1002/alr.21609
5. Fahy JV. Type 2 inflammation in asthma – present in most, absent in many. Nat Rev Immunol. 2015;15:57–65. doi:10.1038/nri3786
6. Woodruff PG, Modrek B, Choy DF, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med. 2009;180:388–395. doi:10.1164/rccm.200903-0392OC
7. Straumann A, Katzka DA. Diagnosis and treatment of eosinophilic esophagitis. Gastroenterology. 2018;154(2):346–359. doi:10.1053/j.gastro.2017.05.066
8. O’Shea KM, Aceves SS, Dellon ES, et al. Pathophysiology of eosinophilic esophagitis. Gastroenterology. 2018;154(2):333–345. doi:10.1053/j.gastro.2017.06.065
9. Schaefer ET, Fitzgerald JF, Molleston JP, et al. Comparison of oral prednisone and topical fluticasone in the treatment of eosinophilic esophagitis: a randomized trial in children. Clin Gastroenterol Hepatol. 2008;6(2):165–173. doi:10.1016/j.cgh.2007.11.008
10. Remedios M, Campbell C, Jones DM, Kerlin P. Eosinophilic esophagitis in adults: clinical, endoscopic, histologic findings, and response to treatment with fluticasone propionate. Gastrointest Endosc. 2006;63:3–12. doi:10.1016/j.gie.2005.07.049
11. Assa’ad AH, Gupta SK, Collins MH, et al. An antibody against IL-5 reduces numbers of esophageal intraepithelial eosinophils in children with eosinophilic esophagitis. Gastroenterology. 2011;141:1593–1604. doi:10.1053/j.gastro.2011.07.044
12. Spergel JM, Rothenberg ME, Collins MH, et al. Reslizumab in children and adolescents with eosinophilic esophagitis: results of a double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2012;129:456–463.e453. doi:10.1016/j.jaci.2011.11.044
13. Straumann A, Conus S, Grzonka P, et al. Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-controlled, double-blind trial. Gut. 2010;59:21. doi:10.1136/gut.2009.178558
14. Hirano I, Dellon ES, Hamilton JD, et al. Efficacy of dupilumab in a Phase 2 randomized trial of adults with active eosinophilic esophagitis. Gastroenterology. 2020;158:111–122.e110. doi:10.1053/j.gastro.2019.09.042
15. Torres T, Ferreira EO, Gonçalo M, Mendes-Bastos P, Selores M, Filipe P. Update on Atopic Dermatitis. Acta Med Port. 2019;32:606–613. doi:10.20344/amp.11963
16. David Boothe W, Tarbox JA, Tarbox MB. Atopic dermatitis: pathophysiology. In: Fortson EA, Feldman SR, Strowd LC, editors. Management of Atopic Dermatitis: Methods and Challenges. Cham: Springer International Publishing; 2017:21–37.
17. Furue M, Chiba T, Tsuji G, et al. Atopic dermatitis: immune deviation, barrier dysfunction, IgE autoreactivity and new therapies. Allergol Int. 2017;66(3):398–403. doi:10.1016/j.alit.2016.12.002
18. Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021;11:213–739.
19. Schleimer RP. Immunopathogenesis of chronic rhinosinusitis and nasal polyposis. Annu Rev Pathol. 2017;12(1):331–357. doi:10.1146/annurev-pathol-052016-100401
20. Stevens WW, Peters AT, Tan BK, et al. Associations between inflammatory endotypes and clinical presentations in chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2019;7(8):2812–2820.e2813. doi:10.1016/j.jaip.2019.05.009
21. Schwartz JS, Tajudeen BA, Cohen NA. Medical management of chronic rhinosinusitis – a review of traditional and novel medical therapies. Expert Opin Investig Drugs. 2017;26(10):1123–1130. doi:10.1080/13543784.2017.1371699
22. Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group Phase 3 trials. The Lancet. 2019;394(10209):1638–1650. doi:10.1016/S0140-6736(19)31881-1
23. Virchow JC. Eosinophilic esophagitis: asthma of the esophagus? Digestive Dis. 2014;32(1–2):54–60. doi:10.1159/000357010
24. Durrani SR, Mukkada VA, Guilbert TW. Eosinophilic esophagitis: an important comorbid condition of asthma? Clin Rev Allergy Immunol. 2018;55(1):56–64. doi:10.1007/s12016-018-8670-7
25. Mansoor E, Cooper GS. The 2010-2015 prevalence of eosinophilic esophagitis in the USA: a population-based study. Dig Dis Sci. 2016;61:2928–2934. doi:10.1007/s10620-016-4204-4
26. Dellon ES, Jensen ET, Martin CF, Shaheen NJ, Kappelman MD. Prevalence of eosinophilic esophagitis in the United States. Clin Gastroenterol Hepatol. 2014;12:589–596.e581. doi:10.1016/j.cgh.2013.09.008
27. Maradey-Romero C, Prakash R, Lewis S, Perzynski A, Fass R. The 2011-2014 prevalence of eosinophilic oesophagitis in the elderly amongst 10 million patients in the United States. Aliment Pharmacol Ther. 2015;41(10):1016–1022. doi:10.1111/apt.13171
28. González-Cervera J, Arias Á, Redondo-González O, Cano-Mollinedo MM, Terreehorst I, Lucendo AJ. Association between atopic manifestations and eosinophilic esophagitis: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2017;118:582–590.e582. doi:10.1016/j.anai.2017.02.006
29. De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132:949–963. doi:10.1038/jid.2011.435
30. Matsumoto K, Iikura K, Morita H, Saito H. Barrier dysfunction in the atopic march—how does atopic dermatitis lead to asthma in children? J Allergy Clin Immunol. 2020;145:1551–1553. doi:10.1016/j.jaci.2020.04.014
31. Silverberg JI, Simpson EL. Associations of childhood eczema severity: a US Population-Based Study. Dermatitis. 2014;25:107.
32. Hua T, Silverberg JI. Atopic dermatitis in US adults: epidemiology, association with marital status, and atopy. Ann Allergy Asthma Immunol. 2018;121:622–624. doi:10.1016/j.anai.2018.07.019
33. Silverberg JI, Gelfand JM, Margolis DJ, et al. Association of atopic dermatitis with allergic, autoimmune, and cardiovascular comorbidities in US adults. Ann Allergy Asthma Immunol. 2018;121:604–612.e603. doi:10.1016/j.anai.2018.07.042
34. Laidlaw TM, Mullol J, Woessner KM, Amin N, Mannent LP. Chronic rhinosinusitis with nasal polyps and asthma. J Allergy Clin Immunol Pract. 2021;9:1133–1141.
35. Hakansson K, Bachert C, Konge L, et al. Airway inflammation in chronic rhinosinusitis with nasal polyps and asthma: the United airways concept further supported. PLoS One. 2015;10:e0127228. doi:10.1371/journal.pone.0127228
36. Ragab A, Clement P, Vincken W. Objective assessment of lower airway involvement in chronic rhinosinusitis. Am J Rhinol. 2004;18:15–21. doi:10.1177/194589240401800105
37. Bilodeau L, Boulay M-E, Prince P, Boisvert P, Boulet L-P. Comparative clinical and airway inflammatory features of asthmatics with or without polyps. Rhinology. 2010;48:420–425. doi:10.4193/Rhino09.095
38. McHugh T, Levin M, Snidvongs K, Banglawala SM, Sommer DD. Comorbidities associated with eosinophilic chronic rhinosinusitis: a systematic review and meta-analysis. Clin Otolaryngol. 2020;45:574–583. doi:10.1111/coa.13536
39. Joo MK, Park J-J, Kim S-H, et al. Prevalence and endoscopic features of eosinophilic esophagitis in patients with esophageal or upper gastrointestinal symptoms. J Dig Dis. 2012;13:296–303. doi:10.1111/j.1751-2980.2012.00589.x
40. Mulder DJ, Hurlbut DJ, Noble AJ, Justinich CJ. Clinical features distinguish eosinophilic and reflux-induced esophagitis. J Pediatr Gastroenterol Nutr. 2013;56:263–270.
41. Slae M, Persad R, Leung AJ-T, Gabr R, Brocks D, Huynh HQ. Role of environmental factors in the development of pediatric eosinophilic esophagitis. Dig Dis Sci. 2015;60:3364–3372. doi:10.1007/s10620-015-3740-7
42. Dellon ES, Rusin S, Gebhart JH, et al. A clinical prediction tool identifies cases of eosinophilic esophagitis without endoscopic biopsy: a prospective study. Am J Gastroenterol. 2015;110(9):1347–1354. doi:10.1038/ajg.2015.239
43. Doucet-Ladevèze R, Holvoet S, Raymond F, et al. Transcriptomic analysis links eosinophilic esophagitis and atopic dermatitis. Front Pediatr. 2019;7:467. doi:10.3389/fped.2019.00467
44. Padia R, Curtin K, Peterson K, Orlandi RR, Alt J. Eosinophilic esophagitis strongly linked to chronic rhinosinusitis. The Laryngoscope. 2016;126:1279–1283. doi:10.1002/lary.25798
45. Tan BK, Chandra RK, Pollak J, et al. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2013;131:1350–1360. doi:10.1016/j.jaci.2013.02.002
46. Chandra RK, Lin D, Tan B, et al. Chronic rhinosinusitis in the setting of other chronic inflammatory diseases. Am J Otolaryngol. 2011;32:388–391. doi:10.1016/j.amjoto.2010.07.013
47. Hirsch AG, Yan XS, Sundaresan AS, et al. Five-year risk of incident disease following a diagnosis of chronic rhinosinusitis. Allergy. 2015;70:1613–1621. doi:10.1111/all.12759
48. Rajan J, Newbury RO, Anilkumar A, Dohil R, Broide DH, Aceves SS. Long-term assessment of esophageal remodeling in patients with pediatric eosinophilic esophagitis treated with topical corticosteroids. J Allergy Clin Immunol. 2016;137:147–156.e148. doi:10.1016/j.jaci.2015.05.045
49. Harer KN, Enders FT, Lim KG, Alexander JA, Katzka DA. An allergic phenotype and the use of steroid inhalers predict eosinophilic oesophagitis in patients with asthma. Aliment Pharmacol Ther. 2013;37:107–113. doi:10.1111/apt.12131
50. Canonica GW, Malvezzi L, Blasi F, et al. Chronic rhinosinusitis with nasal polyps impact in severe asthma patients: evidences from the Severe Asthma Network Italy (SANI) registry. Respir Med. 2020;166:105947. doi:10.1016/j.rmed.2020.105947
51. Zhang Z, Adappa ND, Doghramji LJ, et al. Quality of life improvement from sinus surgery in chronic rhinosinusitis patients with asthma and nasal polyps. Int Forum Allergy Rhinol. 2014;4:885–892. doi:10.1002/alr.21406
52. Schlosser RJ, Smith TL, Mace J, Soler ZM. Asthma quality of life and control after sinus surgery in patients with chronic rhinosinusitis. Allergy. 2017;72:483–491. doi:10.1111/all.13048
53. Stevens WW, Peters AT, Hirsch AG, et al. Clinical characteristics of patients with chronic rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2017;5:1061–1070.e1063.
54. Casale T, Molfino NA, Silver J, et al. Real-world effectiveness of mepolizumab in patients with severe asthma and associated comorbidities. Ann Allergy Asthma Immunol. 2021;S1081-1206(21)00382-3. doi:10.1016/j.anai.2021.05.021
55. Wollenberg A, Thomsen SF, Lacour J-P, Jaumont X, Lazarewicz S. Targeting immunoglobulin E in atopic dermatitis: a review of the existing evidence. World Allergy Organ J. 2021;14(3):100519. doi:10.1016/j.waojou.2021.100519
56. Boguniewicz M, Beck LA, Sher L, et al. Dupilumab improves asthma and sinonasal outcomes in adults with moderate to severe atopic dermatitis. J Allergy Clin Immunol Pract. 2021;9:1212–1223.e1216.
57. Muñoz-Bellido FJ, Moreno E, Dávila I. Dupilumab: a review of present indications and uses out of indication. J Investig Allergol Clin Immunol. 2021;32:2.
58. Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020;75(5):1023–1042. doi:10.1111/all.14221
59. Clayton F, Fang JC, Gleich GJ, et al. Eosinophilic esophagitis in adults is associated with IgG4 and not mediated by IgE. Gastroenterology. 2014;147(3):602–609. doi:10.1053/j.gastro.2014.05.036
60. Loizou D, Enav B, Komlodi-Pasztor E, et al. A pilot study of omalizumab in eosinophilic esophagitis. PLoS One. 2015;10(3):e0113483. doi:10.1371/journal.pone.0113483
61. Chan S, Cornelius V, Cro S, Harper JI, Lack G. Treatment effect of omalizumab on severe pediatric atopic dermatitis: the ADAPT randomized clinical trial. JAMA Pediatr. 2020;174(1):29–37. doi:10.1001/jamapediatrics.2019.4476
62. Heil PM, Maurer D, Klein B, Hultsch T, Stingl G. Omalizumab therapy in atopic dermatitis: depletion of IgE does not improve the clinical course - a randomized, placebo-controlled and double blind pilot study. J Dtsch Dermatol Ges. 2010;8:990–998.
63. Iyengar SR, Hoyte EG, Loza A, et al. Immunologic effects of omalizumab in children with severe refractory atopic dermatitis: a randomized, placebo-controlled clinical trial. Int Arch Allergy Immunol. 2013;162(1):89–93. doi:10.1159/000350486
64. Gevaert P, Calus L, Van Zele T, et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J Allergy Clin Immunol. 2013;131:110–116.e111. doi:10.1016/j.jaci.2012.07.047
65. Pinto JM, Mehta N, DiTineo M, Wang J, Baroody FM, Naclerio RM. A randomized, double-blind, placebo-controlled trial of anti-IgE for chronic rhinosinusitis. Rhinology. 2010;48(3):318–324. doi:10.4193/Rhino09.144
66. Gevaert P, Omachi TA, Corren J, et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J Allergy Clin Immunol. 2020;146(3):595–605. doi:10.1016/j.jaci.2020.05.032
67. Kang EG, Narayana PK, Pouliquen IJ, Lopez MC, Ferreira-Cornwell MC, Getsy JA. Efficacy and safety of mepolizumab administered subcutaneously for moderate to severe atopic dermatitis. Allergy. 2020;75(4):950–953. doi:10.1111/all.14050
68. Gevaert P, Van Bruaene N, Cattaert T, et al. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J Allergy Clin Immunol. 2011;128(5):
69. Bachert C, Sousa AR, Lund VJ, et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: randomized trial. J Allergy Clin Immunol. 2017;140(4):1024–1031.e1014. doi:10.1016/j.jaci.2017.05.044
70. Gevaert P, Lang-Loidolt D, Lackner A, et al. Nasal IL-5 levels determine the response to anti-IL-5 treatment in patients with nasal polyps. J Allergy Clin Immunol. 2006;118:1133–1141. doi:10.1016/j.jaci.2006.05.031
71. NCT04543409. A study of benralizumab in patients with eosinophilic esophagitis (MESSINA); 2021. Available from: https://clinicaltrials.gov/ct2/show/NCT04543409?term=benralizumab&cond=eosinophilic+esophagitis&draw=2&rank=1.
72. NCT04605094. Efficacy and safety study of the use of benralizumab for patients with moderate to severe atopic dermatitis; 2021. Available from: https://clinicaltrials.gov/ct2/show/NCT04605094?term=benralizumab&cond=atopic+dermatitis&draw=2&rank=1.
73. NCT03450083. Benralizumab effect on severe chronic rhinosinusitis with eosinophilic polyposis; 2021. Available from: https://clinicaltrials.gov/ct2/show/results/NCT03450083?term=benralizumab&cond=chronic+rhinosinusitis&draw=2&rank=2.
74. NCT04157335. Efficacy and safety study of benralizumab in patient with eosinophilic chronic rhinosinusitis with nasal polyps (ORCHID); 2021. Available from: https://clinicaltrials.gov/ct2/show/NCT04157335?term=benralizumab&cond=chronic+rhinosinusitis&draw=2&rank=3.
75. Thaçi D, Simpson L, Deleuran M, et al. Efficacy and safety of dupilumab monotherapy in adults with moderate-to-severe atopic dermatitis: a pooled analysis of two phase 3 randomized trials (LIBERTY AD SOLO 1 and LIBERTY AD SOLO 2). J Dermatol Sci. 2019;94(2):266–275. doi:10.1016/j.jdermsci.2019.02.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.