Back to Journals » Risk Management and Healthcare Policy » Volume 18
Inpatient Participation in Patient Safety Behaviors: Decision-Making Typologies from a Qualitative Study
Authors Wang C, Shi H, Du X, Peng Y, Xiao M, Zhao Q, Huang H ![]()
Received 5 May 2025
Accepted for publication 31 August 2025
Published 13 September 2025 Volume 2025:18 Pages 3029—3039
DOI https://doi.org/10.2147/RMHP.S538389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Chunni Wang,1,2 Haoning Shi,1,2 Xingyao Du,1,2 Ying Peng,1,2 Mingzhao Xiao,1,2 Qinghua Zhao,1,2 Huanhuan Huang1,2
1Department of Nursing, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Nursing Research Center, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Qinghua Zhao, Email [email protected] Huanhuan Huang, Email [email protected]
Background: Patient participation in safety behaviors has been recognized as a critical component of reducing medical errors and improving healthcare outcomes in hospitalized settings. However, there is currently a lack of research to understand the decision-making processes that drive these behaviors.
Purpose: This study aimed to identify and construct the different types of decision-making personas adopted by inpatients when thinking about participating in patient safety.
Methods: A qualitative phenomenological study was conducted at a tertiary hospital in Chongqing from October to December 2024. Inpatients meeting the inclusion and exclusion criteria were selected via purposive sampling, and semi-structured interviews were performed to explore their motivation, willingness, decision-making factors, decision-making balance, and effect evaluation during their participation in patient safety decision-making. Data were analyzed using Colaizzi’s seven-step method, facilitating the process from raw data to factual labeling and ultimately to the construction of personas dimensions. Patient characteristics were extracted and personas were constructed by artificial intelligence (AI), with the visualization of these personas achieved through a combination of character images and labels.
Results: This study developed four distinct personas that reflect the decision-making types of inpatients’ participation in patient safety, with the personas classifications as follows: self-driven decision-makers, passive collaborators, resource-limited decision avoiders, and self-assertive decision-makers.
Conclusion: The diversity of patients’ decision-making types necessitates targeted interventions, such as shared decision-making tools, simplified communication, community support provision, and trust reconstruction. Future research should also include longitudinal studies and cross-cultural validation.
Keywords: patients for patient safety, inpatients, persona, decision making, qualitative study
Introduction
Patient safety remains a global priority and persistent challenge within healthcare systems worldwide.1 It is estimated that 1 in 10 inpatients globally experiences some form of harm during their hospitalization, with such harm resulting from a range of adverse events—nearly 50% of which are preventable.2 As first-hand participants in the healthcare process, patients hold unique value as “safety sentinels”, playing a critical role in medication reconciliation,3 infection prevention,4 patient identification5 and other keys. In response, the World Health Organization has launched a series of strategic initiatives to promote patient engagement in patient safety,6,7 aiming to advocate for and advance patient safety actions at global, regional, and national levels.
Despite the global consensus on the practical value of patient participation in patient safety, the 2024 Global Patient Safety Report reveals that the participation rate in patient safety behaviors remains generally below 25% in low- and middle-income countries.8 Furthermore, existing research has largely been confined to the level of behavioral manifestations,9 such as statistics on participation frequency,10 analysis of influencing factors,11 and design of standardized intervention tools.12 These studies tend to oversimplify complex participation behaviors into a binary “yes/no” choice, with little focus on the decision-making processes underlying such behaviors. The decision-making patterns of inpatients exhibit highly contextualized variations, shaped by the interactive effects of multiple factors such as health literacy, cultural background, doctor-patient power dynamics, and characteristics specific to the hospitalization phase.13,14 While quantitative methods can capture behavioral outcomes, they struggle to unravel the implicit cognitive trade-offs and situational interactions involved in the decision-making process.15,16
Thus, this study employed qualitative methods to explore how inpatients make decisions regarding safety participation within complex clinical environments by examining their decision-making processes, and identified distinct decision-making types. The findings provide a scientific basis and actionable insights for designing targeted, effective, and implementable intervention strategies. This contributes to advancing the practice of patient engagement in safety and, ultimately, enhancing the quality and safety of healthcare services.
Materials and Methods
Study Design and Participants
This study is guided by the Transtheoretical Model and theories related to behavioral decision-making. Using a qualitative phenomenological design, it explores the decision-making process of inpatients in their participation in patient safety from five dimensions: motivation, willingness, decision-making factors, decision-making balance, and effect evaluation. Additionally, the types of decisions made by patients have been classified and profiled.
The study was conducted from October to December 2024 at a tertiary hospital in Chongqing. To ensure the depth and relevance of the findings, participants were recruited from hospitalized patients using the maximum variation purposive sampling method. The sample size was determined based on the principle of data saturation.17 The inclusion criteria were as follows: (1) age ≥18 years; (2) Inpatients in internal medicine, surgery, and gynecology departments with a hospitalization duration of more than three days; (3) informed consent and voluntary enrollment in the study. The exclusion criteria included individuals in the terminal or acute stage of their disease, as well as those with severe cognitive impairment or mental illness.
Data Collection
Interview Guide
The initial draft of the interview outline was developed following a literature review and discussions among research group members. The outline covered key aspects such as motivation, willingness, decision-making factors, decision-making balance and effect evaluation Two inpatients meeting the inclusion criteria were selected for pre-interviews.
Feedback from these pre-interviews was used to refine the draft, ultimately forming the interview outline. Core questions were as follows: (1) Are you familiar with the expression “involving patients in their own safety”? Do you believe patients should play an active role in ensuring their own safety? What is your perspective on this issue? (2) Which factors do you think would motivate you to participate actively in patient safety? Conversely, what might deter you from getting involved? (3) What benefits do you perceive in taking proactive steps to engage in patient safety practices? Are there any concerns or hesitations you have regarding these actions? (4) In what specific ways do you believe you can contribute to safeguarding your own safety? What kind of support would help you perform these tasks more effectively? (5) Do you have any recommendations for enhancing hospital initiatives to foster greater patient involvement in safety management?
Data Collection Process
All researchers involved in the study received training in qualitative research methods. Prior to each interview, the researcher introduced themselves, explained the research purpose, methodology, and assured participants that recordings would only be used for research purposes and that their privacy would be strictly protected. With the participant’s consent, basic socio-demographic information was collected, including age, gender, marital status, education level, length of hospital stays, and prior experience with safety incidents.
During the interviews, two researchers collaborated: one asked questions based on the interview outline while the other took detailed notes and provided supplementary observations. The interviewers focused on the research questions, posed targeted and open-ended questions, avoided leading inquiries, respected objective facts, and meticulously recorded key information.
Additionally, they paid close attention to the interviewees’ emotions, expressions, tone, and non-verbal cues. Each participant was interviewed for approximately 30 to 50 min. Interviews continued until no new information emerged, indicating the achievement of data saturation.17 The entire process was audio-recorded, and all recordings were transcribed verbatim within 24 hours of completion.
Data Analysis
Establishing Patient Persona Label Dimensions
The Colaizzi’s seven-step analysis method was employed to analyze the textual data, thereby completing the process from raw data collection to the construction of factual labels and personas dimensions.18,19 The specific steps are as follows: (1) Immersive comprehension of raw data: Researchers need to read each interview transcript repeatedly and thoroughly to gain an overall and generalized understanding of the interview content. (2) Extracting key statements to form factual labels: On the basis of in-depth comprehension, all meaningful and substantial statements related to patients’ participation in patient safety decision-making are identified and extracted sentence by sentence. These original and specific statements are then refined and preliminarily coded into factual labels. (3) Integrating commonalities to construct personas dimensions: In-depth analysis is conducted on the aforementioned factual labels to interpret their inherent meanings. By inducing and abstracting the core meanings they reflect, common features or patterns among different labels are identified and integrated, thus forming the personas label dimensions that can represent patients’ participation in safety decision-making (Supplementary Figure 1).
Extract Features to Construct Patient Personas
Based on the established label dimension framework, the analytical process proceeded as follows: First, researchers manually identified and extracted key themes reflecting patients’ individual characteristics, drawing on their professional expertise and in-depth contextual understanding. Subsequently, an in-depth analysis of each patient was conducted using the five dimensions of theoretical construction. By synthesizing the extracted characteristic themes, Doubao (an AI tool) was used to construct highly personalized multi-dimensional patient personas, encapsulating their unique experiences and attributes. Next, to ensure the authenticity and accuracy of these personas, the preliminarily developed individualized personas were fed back to the corresponding participants for review and validation. Necessary revisions and refinements were made based on their feedback. On this basis, all validated individual personas were analyzed to identify and aggregate patient groups exhibiting similar behavioral patterns or key characteristics, thereby constructing specific patient group personas that reflect shared features within the cohort. Finally, three experts in relevant fields were invited to independently review the persona construction process and the resulting system of individual and group personas. This review aimed to evaluate methodological rigor, result reliability, and representativeness, ensuring that the personas comprehensively and meticulously captured the diversity and complexity of the study population.
Express the Personas of Inpatients in Patient Safety Decision-Making
To visually illustrate the distinct characteristics and behavioral patterns exhibited by different inpatient groups in their participation in patient safety decision-making, this study employed a combination of character images and labels. This approach enabled a vivid, multi-dimensional presentation of various typical patient decision-making personas, thereby allowing key differences between groups to be clearly and directly manifested.
Results
Demographic Characteristic of Participants
A total of 23 hospitalized patients were deemed eligible and participated in the study (Table 1), comprising 12 women and 11 men. The participants’ ages ranged from 30 to 85 years, with a mean age of 52 years. Regarding educational background, 47.83% of the patients held a college degree. Additionally, 69.57% of the participants were married, and 82.61% were employed at the time of the study. 39.13% of the inpatients were from internal medicine, 34.78% from surgery, and 26.09% from gynecology.
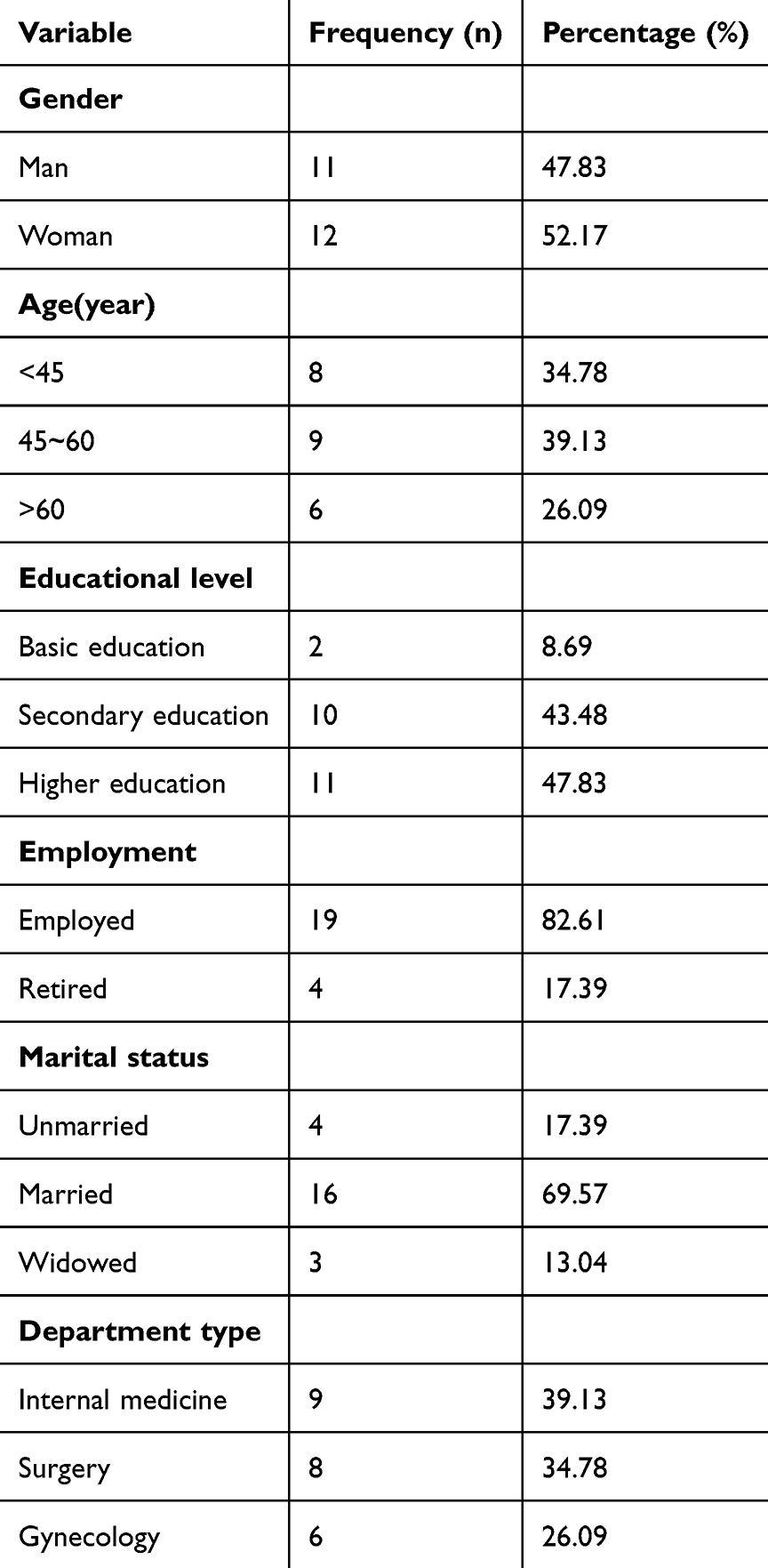 |
Table 1 Characteristics of the Participants (n=23) |
Major Themes and Categories
The codes and themes derived from the analysis have been organized, and the data in Supplementary Table 1 were interpreted using the five dimensions guided by the Transtheoretical Model and theories related to behavioral decision-making. Nineteen subthemes were identified from these five dimensions, as follows: (1) Motivation: Avoiding medical risks, Relying on medical authority, Reducing trouble, Questioning medical authority; (2) Willingness: Actively engaging, Passive acceptance with occasional doubts, Silent or perfunctory responses, Desire to assert control; (3) Decision-making factors: Cognitive ability, Psychological traits, Social support; (4) Decision-making balance: Rational risk-benefit assessment; Accepting the “default option” from providers; Low sensitivity to medical risks; Overestimating personal judgment; (5) Effect evaluation: Highly effective, Partially effective, Limited effect, Needs optimization.
Inpatient Participation in Patient Safety Decision-Making Personas
As shown in Figure 1, This study constructed four decision-making personas types regarding inpatients’ participation in patient safety, and provided detailed descriptions of the characteristics and dimensions of each type.
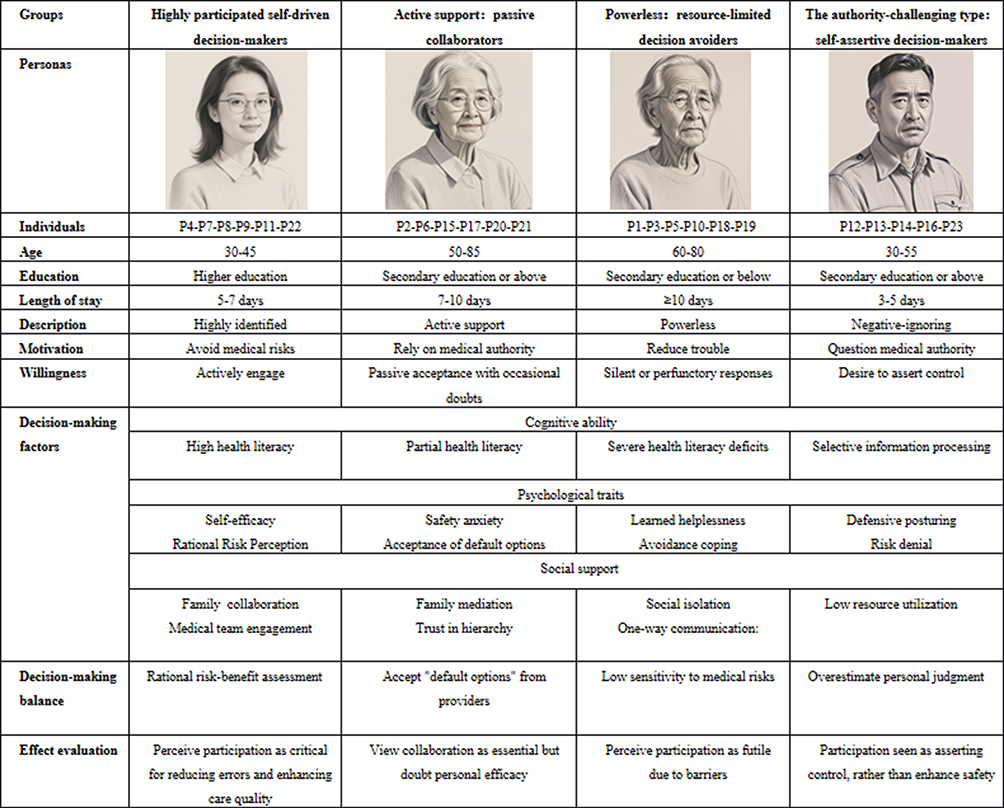 |
Figure 1 Inpatient participation in patient safety decision-making personas. |
Theme 1: Highly Participated: Self-Driven Decision-Makers
This group is predominantly composed of young women aged 30–45 years (n=6, 26.09% of the sample), with 83.3% possessing higher education qualifications (college level or above). Over 80% are employed, and 67% are married, indicating stable socioeconomic status and family support. These patients are primarily hospitalized in internal medicine (33.3%) and gynecology (66.7%) for conditions such as chronic diseases requiring long-term management. With an average hospital stay of 5–7 days, the moderate length of hospitalization allows sufficient time to familiarize themselves with medical procedures and communicate with healthcare providers. They actively participate in safety-related discussions motivated by a strong desire to avoid medical risks and a willingness to participate proactively in decision-making processes.
In the dimension of Cognitive ability, due to their relatively high educational attainment, these patients can accurately interpret medical terminology and protocols. (eg understanding antibiotic resistance). They demonstrate the ability to critically evaluate the risks and benefits of treatment options, often supported by prior health education (eg via online health platforms).
Patient 4:Before being hospitalized, I taught myself the relevant knowledge about the treatment of uterine fibroids in order to communicate better with the doctor.
In the dimension of Psychological Traits. They exhibit strong confidence in their own decision-making abilities, rooted in positive past healthcare experiences. Low anxiety levels enable calm deliberation; while fear of medical errors drives vigilance rather than avoidance.
Patient 7:Checking the details of the medicine makes me feel at ease. It’s my right. Only when confirmed clearly can I trust the treatment process.
Patient 8:I am not afraid that the doctor will think I am troublesome. Missing a detail might lead to a big mistake. I must ask clearly.
In the dimension of Social Support. Spouses or parents often assist in verifying information (eg cross-checking discharge instructions). Bidirectional communication with clinicians fosters trust and reinforces their participation.
Patient 11:During my hospital stay, my husband and parents took turns to record medical orders for me, and my friends would also help verify professional terms.
Specifically speaking, In terms of Effect evaluation They patients view their participation as a critical mechanism to reduce medical risks and improve care quality. They believe proactive behaviors—such as verifying medications, requesting treatment explanations, and reviewing test results—directly mitigate errors (eg incorrect dosages) and enhance transparency in clinical processes.
Patient 22:Before each intravenous infusion, I would check the names and dosages of the drugs with the nurse to ensure there were no mistakes.
Many report increased satisfaction with care due to their perceived autonomy and control over health outcomes.
Theme 2: Active Support: Passive Collaborators
This group is dominated by middle-aged and elderly patients (50–85 years, n=6, 26.09% of the sample), with 83.3% having secondary education or above. Most are retired (55%) or widowed (33.3%), and 77.8% are hospitalized in surgery or internal medicine for acute conditions (eg post-operative recovery). Their average hospital stay is 7–10 days, and they tend to be more accustomed to passive acceptance characterized by reliance on healthcare providers for guidance.
The primary goal of these patients is to follow medical authorities guidance and cooperate with treatment. They passively accept prescribed plans, expressing vague doubts only at critical moments, are tend to accept the default options recommended by healthcare providers while avoiding independent risk assessments.
Patient 2:I am in the hospital; they are doctors who know my condition, so I just follow their instructions.
In the dimension of Cognitive ability. These patients have limited understanding of complex medical terminology, relying on simplified explanations (eg graphical explanations). They struggle to distinguish between routine and high-risk procedures (eg conflating blood tests with surgical risks).
Patient 6:Blood glucose monitoringsounds very complicated, but when the nurse drew a curve graph to explain the range of high and low values, I understood.
In the dimension of Psychological Traits. High concern about complications (eg infections) coexists with a desire to comply, creating internal conflict. Acceptance of default options (eg “Whatever the doctor says”) reduces decision-making stress.
Patient 15:I follow doctors’ orders, but sometimes I wonder if I should ask more questions but they’re the experts.
In the dimension of Social Support, Adult children often act as intermediaries (eg translating medical terms). Trust in hierarchical structures (eg senior physicians) overrides personal judgment.
Patient 17:I do not really understand this. My daughter is studying medicine, so I usually ask her about these matters.
Specifically speaking, In terms of Effect evaluation. These patients view collaboration with medical staff as essential for safety but perceive their individual contributions as secondary to institutional protocols. While trusting clinicians to “do what’s best”, lingering doubts about personal efficacy emerge during critical moments.
Patient 20:Ask too much for fear of being criticized for being verbose. It’s safest to follow the doctor’s advice.
Theme 3: Powerless: Resource-Limited Decision Avoiders
This group consists predominantly of elderly patients (>60 years, n=6, 26.09% of the sample), with 83.3% having secondary education or below. Over 50% are widowed or living alone, and 66.7% suffer from multiple comorbidities (eg diabetes, hypertension). Primarily Hospitalized in internal medicine (83.3%), their average stay exceeds 10 days, during which they experience a decline in self-efficacy attributed to prolonged dependency (avoidance) characterized by minimal engagement in safety discussions.
The primary goal of these patients is to reduce trouble and thus avoid decision-making responsibility. They often show silently or perfunctorily in decision-making scenarios. For example, signing documents hastily without careful review.
Patient 1:At my age, I cannot handle it anymore. I will sign whatever the doctor tells me.
In the dimension of Cognitive ability, they struggle to understand medical terminology, treatment plans and the purpose of examinations. Retaining verbal instructions (eg dietary restrictions) is also challenging.
Patient 3:What does the doctor mean by electrolyte imbalance? I cannot even write all the words.
In the dimension of Psychological Traits. Long-term dependency on caregivers erodes self-efficacy (eg “I cannot manage this alone”). Rushed decisions (eg signing documents without reading) alleviate immediate stress.
Patient 5:I participate when the doctors and nurses ask me to. I do not understand that.
In the dimension of Social Support. Lack of family visits or advocacy exacerbates information gaps. Standardized nurse instructions fail to address individual needs.
Patient 10:My children all work in other places. After my spouse passed away, I lived alone. When I was hospitalized, I was unable to handle many things.
Specifically speaking, In terms of Effect evaluation. These patients exhibit low sensitivity to medical safety risks. Due to cognitive and social barriers, they perceive participation as futile, equating decision-making with confusion and prioritizing compliance to “avoid causing trouble.”
Patient 19:Doctors and nurses are very busy at work; sometimes they speak very quickly. I do not understand everything; if it is not particularly important, I will act according to my own understanding.
Theme 4: The Authority-Challenging Type: Self-Assertive Decision-Makers
This group is dominated by young and middle-aged males (30–55 years, n=5, 21.74% of the sample), with 62.5% having secondary education or above. Most are employed (80%) Hospitalized in surgery (80%), their stays average 3–5 days, marked by confrontational interactions with shorter stays often exhibit distrust due to insufficient time to establish rapport with the medical team, leading to confrontational participation.
These patients frequently question medical authority and seekcontrol over their medical decisions. Yet they also express willingness to actively participate in patient safety-related decision-making.
In the dimension of Cognitive ability. They selectively cite online content that confirms preexisting beliefs (eg distrust of therapeutic effect) and overestimate knowledge (eg equating Baidu searches with medical training).
Patient 12:I saw on the Internet that someone said this kind of antihypertensive drug would harm the liver. Is it true?
Patient 13:I feel that this atomization is of no use. Can we stop doing it.
In the dimension of Psychological Traits. They Use adversarial communication (eg questioning the rationality of the medical order) to maintain perceived autonomy and rationalize non-compliance (eg “Side effects will not happen to me”) to reduce cognitive dissonance.
Patient 14:I came to the hospital for treatment; I should not have to worry about patient safety.
In the dimension of Social Support. They avoid input from family or clinician (eg “I don’t need anyone’s help”)
Patient 16:I can be hospitalized alone and do not need the company of family members.
Specifically speaking, In terms of Effect evaluation, these Individuals tend to overestimate their judgment capabilities, viewing participation as a means to assert control rather than enhance safety. They overvalue personal judgment (eg self-diagnosis via online platforms) and dismiss clinical guidelines as “restrictive”.
Discussion
To the best of our knowledge, this is the first study to explore the decision-making types of inpatients’ participation in patient safety using qualitative research methods, and construct four distinct patient decision-making personas: self-driven decision-makers, passive collaborators, resource-limited decision avoiders, self-assertive decision-makers.
The correlations between the four types of patient personas constructed in this study and existing studies demonstrate significant cultural specificity and theoretical complementarity self-driven decision-makers align closely with the characteristics of “expert patients” proposed by Robert et al20 and their active participation behaviors are significantly associated with threat perception in the health belief model.21 Notably, the emphasis placed by this group on two-way communication shows a stronger demand for autonomy compared to the quantitative research conducted by David in the United States. This discrepancy may be linked to the rapid awakening of patients’ awareness regarding their rights to participate in patient safety in China. The behavioral patterns of passive collaborators and resource-limited decision avoiders are consistent with findings from a South Korean survey.22 This study confirms that low educational level and insufficient social support are key barriers to patient participation. However, qualitative data further reveals reveal fundamental differences in the decision-avoidance mechanisms of these two groups; the former stems from entrenched perceptions of doctor-patient power dynamics, while the latter is more constrained by the blocked information access channels. Such differences suggest that standardized patient education strategies may be ineffective, necessitating a stratified intervention approach. Within the Chinese cultural context, self-assertive decision-makers exhibit a unique characteristic of “selective trust”23 They are skeptical of the broader healthcare system while remaining dependent on specific medical staff. This contradictory psychology may arise from the collision between Confucian traditions of authority obedience and modern patients’ growing self-awareness.
The types of patient personas revealed in this study underscores the clinical necessity of stratified intervention strategies. For self-driven decision-makers, insights can be drawn form the development of Patient Decision Aids (PDA) tools in the UK.24 Under government leadership with support from medical institutions and experts, prioritizing information accuracy. By integrating disease-related content, drawing on the long-term planning of the National Health Service (NHS),25 and presenting information through diverse formats such as videos, manuals, and case demonstrations, accessible and comprehensible tools can be created. This approach effectively narrows the information gap between doctors and patients, enhancing doctor-patient communication and increasing the participation and satisfaction of inpatients. For passive collaborators, a “patient-centered” co-decision-making model is recommended. Adapting the UK “doctor-patient-nurse” co-decision-making framework while incorporating China emphasis on family involvement,26 a “doctor-nurse-patient-family” decision-making model can be constructed. Within this model, doctors, nurses, and family members assist in gathering disease-related information, but final clinical decisions rest with the patient provided they possess independent decision-making capacity. Patients’ preferences regarding family involvement in decisions should be solicited to truly realize “patient-centered”. For resource-limited decision avoiders, medical staff must adopt more patient-friendly communication, using clear and accessible language.27 Simultaneously, medical staff should also update their practice philosophies communication should involve not merely informing but also explaining, empowering patient to make treatment choices Hospital training programs should prioritize not only medical skills enhancement but also the strengthening of doctor-patient communication and shared decision-making competencies. Additionally, social support systems play a critical role: Community outreach and volunteer initiatives can promote public decision-making education breaking the “poverty cycle” of participation through sustained health literacy efforts.28 For self-assertive decision-makers, interventions should focus on restoring trust. Hospital should improve mechanisms for preventing and resolving doctor-patient disputes to rebuild trust29,30 proactively alleviate negative emotions, enhance the quality of medical services, and increase patient satisfaction. Medical staff should emphasize humanistic care, strengthen trust-building, improve communication, and enhance patient “sense of security”.
Notably, artificial intelligence (AI driven healthcare applications could significantly augment these stratified strategies by enabling more precise and dynamic patient profiling for decision support.31 By analyzing multi-source data—including electronic health records, patient-reported outcomes, and interaction patterns—AI systems could automatically identify patients’ role typologies, helping clinicians match interventions with greater efficiency. For instance, AI-powered decision aids might deliver personalized safety information tailored to cognitive abilities32 (eg simplified visuals for Resource-Poor Avoiders or detailed evidence summaries for Autonomously Driven Decision-Makers) and adapt recommendations in real time based on evolving patient needs during hospitalization.33 Such tools could bridge gaps in human resource constraints, ensuring consistent application of role-specific strategies across diverse clinical settings.34
Methodologically speaking, our research has certain advantages. By combing text with imagery, abstract interview data are transformed into concrete and easily understandable visual representations, This helps medical staff and policymakers quickly grasp core characteristics of the target population. Compared to plain text reports,35,36 visual profiling more efficiently conveys findings to non-academicstakeholders and facilitates interdisciplinary collaboration. It is not only a technological upgrade of research methods, but also a bridge connecting theoretical research and clinical practice. Its core value lies in transforming abstract data into actionable insights, ultimately achieving a “patient-centered” precision medical model. In addition, previous scholars have conducted profiling of individuals, such as self-management of cardiac rehabilitation in families of patients with coronary heart disease. Our research combined with semi-structured interviews, and visualized using AI. It generates profiles based on text data, avoiding the subjective assumptions of hand-drawn artists, and ensuring that the features are consistent with the original interview.
However, There are a few limitations to our study. Firstly, the applicability of the constructed personas is constrained by their derivation from Chinese inpatients. Further research is needed to validate their universality across different countries. Secondly, the cross-sectional design eliminates analysis of personas over time. Thirdly, although topic analysis provides depth, there is still a lack of quantitative data to validate the constructed patient decision-making personas future studies should incorporate objective measurement methods to verify the results of role classification.
Conclusion
This study identified four types of decision-making personas specific to inpatient subgroups, revealing the diversity of inpatients’ participation in patient safety decision-making. Personalized intervention strategies tailored to different patient types were proposed, enabling healthcare systems to effectively address barriers such as limited health literacy, distrust, and social isolation, thereby bridging the cognitive-behavioral gap. Future research should investigate longitudinal role transitions, evaluate role-specific interventions, and expand the sample to encompass diverse healthcare settings.
Ethics Approval and Informed Consent
This study received approval from the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (Approval No.:2024.203.02). Before enrollment, all participants were informed of the study objectives and provided written informed consent, including permission for the publication of anonymized responses/direct quotes. This study adhered to the ethical principles for medical research involving human subjects in compliance with declaration of Helsinki.
Acknowledgments
We gratefully appreciated all respondents who participated in this study. We extend our thanks to Dr. Yang Zhen from the First Affiliated Hospital of China Medical University for the invaluable writing assistance provided for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Chongqing (Project No. : CSTB2025NSCQ-GPX1118) and Key Project of Nursing Research Innovation of the First Affiliated Hospital of Chongqing Medical University (Project No. : HLPY2025-04).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Nora CRD, Beghetto MG. Patient safety challenges in primary health care: a scoping review. Rev Bras Enferm. 2020;73(5):e20190209. doi:10.1590/0034-7167-2019-0209
2. 10 Facts on Patient Safety. PSNet. Available from: https://psnet.ahrq.gov/issue/10-facts-patient-safety.
3. Wang N, Ren B, You H, et al. Assessment of medication adherence, medication safety awareness and medication practice among patients with lung cancer: a multicentre cross-sectional study. Health Expect. 2022;25(2):791–801. doi:10.1111/hex.13426
4. Kubde D, Badge AK, Ugemuge S, Shahu S. Importance of hospital infection control. Cureus. 2023;15(12):e50931. doi:10.7759/cureus.50931
5. Bell SK, Bourgeois F, Dong J, et al. Patient identification of diagnostic safety blindspots and participation in “Good Catches” through shared visit notes. Milbank Q. 2022;100(4):1121–1165. doi:10.1111/1468-0009.12593
6. Astier-Peña MP, Martínez-Bianchi V, Torijano-Casalengua ML, Ares-Blanco S, Bueno-Ortiz JM, Férnandez-García M. [The Global Patient Safety Action Plan 2021–2030: identifying actions for safer primary health care]. Aten Primaria. 2021;53(Suppl 1):102224. doi:10.1016/j.aprim.2021.102224
7. State of the world’s nursing 2020: investing in education, jobs and leadership. Available from: https://www.who.int/publications/i/item/9789240003279.
8. Global patient safety report 2024. Available from: https://www.who.int/publications/i/item/9789240095458.
9. Gültzow T, Hoving C, Smit ES, Bekker HL. Integrating behaviour change interventions and patient decision aids: how to accomplish synergistic effects? Patient Educ Couns. 2021;104(12):3104–3108. doi:10.1016/j.pec.2021.04.007
10. Street M, Dempster J, Berry D, et al. Enhancing active patient participation in nursing handover: a mixed methods study. J Clin Nurs. 2022;31(7–8):1016–1029. doi:10.1111/jocn.15961
11. Liu Y, Hu R, Li P, et al. Factors influencing Patient engagement in preventing pressure injuries: a cross-sectional study in Orthopedic inpatients. J Tissue Viability. 2025;34(3):100902. doi:10.1016/j.jtv.2025.100902
12. Li C, Xu X, He L, Zhang M, Li J, Jiang Y. Questionnaires measuring patient participation in patient safety-A systematic review. J Nurs Manage. 2022;30(7):3481–3495. doi:10.1111/jonm.13690
13. Elwyn G, Pickles T, Edwards A, et al. Supporting shared decision making using an Option Grid for osteoarthritis of the knee in an interface musculoskeletal clinic: a stepped wedge trial. Patient Educ Couns. 2016;99(4):571–577. doi:10.1016/j.pec.2015.10.011
14. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
15. Dabkowski E, Cooper SJ, Duncan J, Missen K. Investigating falls risk awareness in hospitals using the Self-Awareness of Falls Risk Measure (SAFRM): empirical research quantitative. Nurs Open. 2025;12(1):e70099. doi:10.1002/nop2.70099
16. Yuan P, Wang C, Cai Y, et al. The current status and influencing factors of hospitalized patients’ propensity to engage in patient safety: a phenomenological cross-sectional study. J Nurs Manage. 2025;2025:2701869. doi:10.1155/jonm/2701869
17. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
18. Li X, Zhang N, Yang J, Geng Z, Zhou J, Zhang J. Weight management personas of breast cancer patients undergoing chemotherapy in China: a multi-method study. BMC Med Inform Decis Mak. 2024;24(1):108. doi:10.1186/s12911-024-02515-1
19. Yang Z, Xu L, Gao Y, Zhang C, Wang A. Tailored personas for self-management in home-based cardiac rehabilitation for patients with coronary heart disease: a qualitative study. Int J Nurs Stud. 2025;163:105000. doi:10.1016/j.ijnurstu.2025.105000
20. Tattersall RL. The expert patient: a new approach to chronic disease management for the twenty-first century. Clin Med Lond. 2002;2(3):227–229. doi:10.7861/clinmedicine.2-3-227
21. Bishop AC, Baker GR, Boyle TA, MacKinnon NJ. Using the health belief model to explain patient involvement in patient safety. Health Expect. 2015;18(6):3019–3033. doi:10.1111/hex.12286
22. Choi N, Kim J, Kim H. The influence of patient-centeredness on patient safety perception among inpatients. PLoS One. 2021;16(2):e0246928. doi:10.1371/journal.pone.0246928
23. Wang Y, Liu Q, He L, Li X. Classification of the appropriate behaviors of patients for patient safety against the Chinese cultural background, based on grounded theory. Int J Occup Med Environ Health. 2020;33(3):263–272. doi:10.13075/ijomeh.1896.01525
24. Patient decision aids | making decisions about your care | NICE and the public | NICE Communities | about. NICE. Available from: https://www.nice.org.uk/about/nice-communities/nice-and-the-public/making-decisions-about-your-care/patient-decision-aids.
25. Dixon-Woods M, Baker R, Charles K, et al. Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study. BMJ Qual Saf. 2014;23(2):106–115. doi:10.1136/bmjqs-2013-001947
26. Overview | Shared decision making | Guidance | NICE; 2021. Available from: https://www.nice.org.uk/guidance/ng197.
27. Newell S, Jordan Z. The patient experience of patient-centered communication with nurses in the hospital setting: a qualitative systematic review protocol. JBI Database System Rev Implement Rep. 2015;13(1):76–87. doi:10.11124/jbisrir-2015-1072
28. Manhas KP, Olson K, Churchill K, Vohra S, Wasylak T. Experiences of shared decision-making in community rehabilitation: a focused ethnography. BMC Health Serv Res. 2020;20(1):329. doi:10.1186/s12913-020-05223-4
29. Lewandowski R, Goncharuk AG, Cirella GT. Restoring patient trust in healthcare: medical information impact case study in Poland. BMC Health Serv Res. 2021;21(1):865. doi:10.1186/s12913-021-06879-2
30. Benbenishty JS, Hannink JR. Non-verbal communication to restore patient-provider trust. Intensive Care Med. 2015;41(7):1359–1360. doi:10.1007/s00134-015-3710-8
31. Bello B, Bundey YN, Bhave R, et al. Integrating AI/ML models for patient stratification leveraging omics dataset and clinical biomarkers from COVID-19 patients: a promising approach to personalized medicine. Int J Mol Sci. 2023;24(7):6250. doi:10.3390/ijms24076250
32. Jayakumar P, Moore MG, Furlough KA, et al. Comparison of an artificial intelligence-enabled patient decision aid vs educational material on decision quality, shared decision-making, patient experience, and functional outcomes in adults with knee osteoarthritis: a randomized clinical trial. JAMA Network Open. 2021;4(2):e2037107. doi:10.1001/jamanetworkopen.2020.37107
33. Chew J, Zeng Z, Tan THB, et al. ADL+: a digital toolkit for multidomain cognitive, physical, and nutritional interventions to prevent cognitive decline in community-dwelling older adults. Int J Environ Res Public Health. 2024;22(1):42. doi:10.3390/ijerph22010042
34. Mohsen F, Ali H, El Hajj N, Shah Z. Artificial intelligence-based methods for fusion of electronic health records and imaging data. Sci Rep. 2022;12(1):17981. doi:10.1038/s41598-022-22514-4
35. Sarkhosh S, Abdi Z, Ravaghi H. Engaging patients in patient safety: a qualitative study examining healthcare managers and providers’ perspectives. BMC Nurs. 2022;21(1):374. doi:10.1186/s12912-022-01152-1
36. Raab C, Gambashidze N, Brust L, Weigl M, Koch A. Motivation for patient engagement in patient safety: a multi-perspective, explorative survey. BMC Health Serv Res. 2024;24(1):1052. doi:10.1186/s12913-024-11495-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.