Back to Journals » Journal of Pain Research » Volume 19
Initial Exploration of a Music-Based Telehealth Support for Medically-Complex Chronic Pain Patients
Authors Hunt AM ![]() , Schug S, Maitin A, Peluso A, Patel A, Bailey J
, Schug S, Maitin A, Peluso A, Patel A, Bailey J
Received 21 October 2025
Accepted for publication 24 May 2026
Published 16 June 2026 Volume 2026:19 571972
DOI https://doi.org/10.2147/JPR.S571972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Andrea McGraw Hunt,1 Seran Schug,2 Asher Maitin,3 Arianna Peluso,4 Aarsh Patel,4 James Bailey5
1Department of Music, Rowan University, Glassboro, NJ, USA; 2Department of Sociology and Anthropology, Rowan University, Glassboro, NJ, USA; 3Lewis Katz School of Medicine, Temple University, Philadelphia, PA, USA; 4Rowan-Virtua School of Osteopathic Medicine, Stratford, NJ, USA; 5Neuromusculoskeletal Institute, Rowan-Virtua School of Osteopathic Medicine, Stratford, NJ, USA
Correspondence: Andrea McGraw Hunt, Department of Music, Rowan University, 237 Wilson Hall, 201 Mullica Hill Road, Glassboro, NJ, 08028, USA, Tel +1 856 256 4032, Email [email protected]
Purpose: Music interventions for chronic pain harness multiple therapeutic mechanisms, including self-efficacy and social connectedness. Many patients cannot access face-to-face music therapy due to health conditions and/or socioeconomic barriers. We sought patient input on an initial session protocol to determine whether a telehealth support group would benefit patients unable to attend in-person group music therapy.
Patients and Methods: In collaboration with an osteopathic clinic, we conducted two cohorts (N = 3 unique participants) of the Virtual Chronic Pain Support Group to develop session protocols and assess utility of outcome measures. We obtained ongoing participant feedback through check-in surveys and adjusted session format in response. Thematic analysis of focus group data at the conclusion of each cohort identified patients’ perceived benefits and suggestions for future groups. Lastly, we examined the feasibility of survey data collection methods and measures.
Results: Participants reported they experienced pain relief, social support, and gained knowledge and insight into managing their pain and other stressors using music. They preferred small group sizes and participant-centered psychoeducation, with song sharing and music imagery central to each session. Furthermore, patients supplemented sessions by listening to recordings of the sessions’ music and imagery experiences and group-curated playlists. They reported that the quantitative outcome measures were relevant to their pain experiences and needs.
Conclusion: The groups were accessible and provided patients meaningful social connections, valuable psychoeducation, and self-management resources for chronic pain. This pilot study suggests that this telehealth protocol can be a lifeline for isolated patients facing barriers to in-person therapy. Furthermore, participants’ descriptions of increased mind-body awareness during the music interventions highlight their potential for restoring positive interoception. Participant-centered group telehealth could significantly expand access of music intervention resources to chronic pain patients. Further research with diverse patient communities is needed to optimize approaches for this challenging population.
Keywords: chronic pain, music therapy, music intervention, telehealth, peer support
Introduction
Chronic pain affects one in five adults in America,1 including as many as 41% of U.S. veterans, and is associated with impacts on range of mobility, daily activities, anxiety, depression and poor perceived health.2,3 With continuing concern for opioid abuse, there is a greater need for adjunctive interventions for patients experiencing chronic pain and using opioids.4 Studies have shown that coordinated interventions across modalities using multiple treatment strategies are effective for managing chronic pain,5 in contrast to isolated treatment options such as surgery, physical therapy, behavioral interventions, or alternative therapies6 (a broad category of interventions aside from those already listed). Thus, current best practices for chronic pain management involve a personalized biopsychosocial approach acknowledging the complex interaction of sociocultural, psychological, and physiological factors on pain.7
Moving patients to non-pharmacological, interdisciplinary approaches requires a well-supported tapering period and an acceptance that pain may not be eliminated completely; the focus thus shifts to minimizing the impact of pain on patients’ quality of life.5 Practitioners have shown a growing interest in using music as an alternative and adjunctive approach to pain management, but they require more evidence of its effectiveness to support recommending its use.8 Clinicians and researchers must also address the racial and socioeconomic disparities that exist in accessing treatments/supports and the harms that result from opiate medications in treating acute/chronic pain. For example, recent research examining experiences of Black American adults who are coping with chronic osteoarthritis pain found that lack of access, time, and knowledge of resources impeded respondents’ ability to engage in self-management practices.9 Additional barriers to accessing a full range of treatment options include inadequate clinician knowledge and guidance, unconscious bias, lack of pain management specialists, limited access to different therapeutic modalities, siloed health systems, limited insurance coverage, and limited evidence supporting alternative pain treatments.5 Our clinical experience supports these observations, as we work with patients whose ability to attend supplementary in-person services and supports is restricted due to their lack of mobility because of pain/disability, lack of time due to the demands of managing one’s own chronic health conditions and/or caregiving for others, and lack of financial resources. Though prescribing rates for opioids have decreased over the past 10 years, they are still commonly prescribed for chronic pain,10 and addiction, abuse, and misuse of opioids among pain patients remain a primary concern.7
Music listening and the creation of music is a pleasurable activity that can affect mood, cognition, and sensory awareness, providing a basis for its use as an accessible intervention for pain.8 Music listening has been widely studied to address pain management, with proven reductions in self-reported pain, emotional distress, and opioid use.11–16 Researchers have sought to identify neural correlates of these effects, and found that engaging with music may affect dopaminergic pathways in the mesolimbic striatal system, which is correlated with an individual’s perception of reward, reinforcement, and motivation.8,17–19 Though research on the neural mechanisms of music’s effects on chronic pain has been limited, neuroimaging has shown large-scale overlap between music and pain processing networks in the brain, involving somatosensory and prefrontal areas, the amygdala and cingulate cortex, and the insula.8 Additionally, the default mode network has been implicated in resting-state fMRI of fibromyalgia patients who experienced reduced pain while listening to preferred relaxation music.20
Though evidence for the effects of music-based interventions for chronic pain continues to grow, translating this research to clinical application has been limited to research settings,8 limiting access to patients who are in proximity to labs conducting such work. Telemedicine has been shown to provide continuous care and monitoring for patients who endure chronic pain, limiting the need for patients to attend in-person activities. Thus telemedicine saves time on and the need for travel, as well as offers cost-cutting solutions for patients of lower socioeconomic demographics.21 Telemedicine also provides greater access to care for patients living in rural communities who may experience geographic barriers to accessing treatments.22 Lastly, telemedicine has been shown to empower patients through engagement and education of their care by accessing education resources and tools through telemedicine platforms.21–25 Patients report they are generally satisfied with their telemedicine visits, which is enhanced by the other cost-cutting and time-saving measures.26
Combining the accessibility of telemedicine with group music therapy sessions could help patients overcome barriers to treatment (such as travel, costs, lack of access, limited mobility, and stress), in order to reap the known benefits of music therapy for chronic pain. One case study showed that music therapy conducted on a virtual platform did not diminish its effectiveness: after the conclusion of an eight-week in-person music therapy group, the patients, who were female veterans in the Greater Boston area, requested continuation of care virtually after the lead music-therapist moved out of the area. The group evaluated the additional five telehealth music therapy sessions, stating that the online platform was overall effective and not a deterrent from engagement in treatment.27 The COVID-19 pandemic also forced practitioners to utilize telemedicine approaches for a wide range of populations, such as music therapy support groups for chronic pain.28 Cephas et al found that telehealth sessions offered participants opportunities to exert agency in their treatment and self-efficacy, which allowed participants to learn about and develop new coping skills for pain, a finding supported by research indicating that perceived music choice and control over music in music listening interventions–that is, the mechanism of cognitive agency–had analgesic benefits.29 Cephas et al’s work reported on group sessions using live and recorded music through the use of streaming or music videos, lyric sharing using sound, and screen sharing over zoom, in an effort to replicate in-person sessions halted during the pandemic. Furthermore, the use of the chat feature provided another way participants could spontaneously interact with the music and each other during music experiences. Participants also benefited from psychoeducation about ways to use music listening on their own to manage pain outside of sessions.28 Although more research is needed to support music therapy through telehealth platforms, studies have already shown positive benefits towards the conversion of music therapy to a more convenient and accessible telehealth outlet.
Group music-making helps chronic pain patients through the mechanisms of social connections and self-efficacy.30,31 Many cross-sectional studies show that social support is associated with lower levels of anxiety, depression, and pain related distress in pain patients.32–39 Additionally, the related concept of greater social connectedness (ie, a greater sense of belonging and ability to connect with others) is also correlated with lower anxiety and, consequently, lower levels of pain.40 Given the challenges many chronic pain patients face attending in-person sessions, we wondered if telehealth music therapy groups could also support these mechanisms. Synchronized, live music-making over video platforms is not technologically feasible; however, given the success of telehealth sessions using streamed music for active listening and guided imagery,27,28,41 telehealth music therapy for groups of chronic pain patients has potential to provide accessible, effective supports for chronic pain patients. Group work would support social connections with peers, incorporate learning coping skills for pain management outside of group meetings, and promote self-efficacy.
We sought to leverage these advantages of music therapy and telehealth delivery to support chronic pain patients in need of accessible adjunctive supports to manage their pain. We developed an initial group protocol that included psychoeducation, directed music imagery (MI), and patient-selected song-sharing. Our psychoeducation component followed the example in previous research initially addressing the neurological interaction of music and pain perception.31 We intended the song sharing portion of the session to promote interaction among group members, leading to peer support. Finally, we planned to adapt the Bonny Method of Guided Imagery and Music (GIM), which is a music-centered approach that uses curated classical music to correspond with imaging and verbal processing.42 This approach has been shown to improve overall quality of life and well-being in patients with post-traumatic stress disorder (PTSD), depression, fibromyalgia, cancer, and rheumatoid arthritis.43,44 GIM includes a continuum of techniques ranging from supportive to intensive psychotherapy. In a group application for telehealth, a supportive form of music imagery (MI) would involve a directed imagery experience based upon the participants’ interests and needs. Whereas previous research on telehealth group music therapy has shown promise for pain patients,28 this application did not include MI; and whereas individual MI delivered via telehealth has shown promise for pain patients, as of yet there has been no research on a group application for pain patients.41
In light of these promising outcomes and remaining clinical needs, we undertook two series of telemedicine music therapy groups with the primary aim to collaborate with participants to develop a feasible, acceptable, and accessible peer support telehealth protocol. We sought participant feedback throughout each series to ensure we addressed and supported patients’ needs and preferences in the group structure and intervention delivery. In this paper, we share our findings from this initial project, including the resulting session protocol and participant reactions. As a secondary aim, we collected quantitative and qualitative outcome measures to evaluate the appropriateness and potential of these tools to evaluate participant responses to the support group. This information will help us design larger studies.
Materials and Methods
Study Design
This is an initial, exploratory project to gain participants’ input on developing a feasible and acceptable session protocol and to test relevance of selected measures. The design will inform future research involving larger samples suitable for inferential analysis. This is a mixed method-program evaluation, convergent parallel design;45 we utilized participant feedback to increase relevance and accessibility of programming; working at the “consult” level of Participatory-Action Research.46
Participants
The intervention was designed for adults aged 18 and older taking opioids for moderate to severe pain or who are diagnosed with opioid use disorder secondary to treatment of chronic pain. The Rowan University and Virtua Health Institutional Review Boards (PRO-2024-64) reviewed the study protocol and assured its compliance with U.S. federal regulations (45 CFR 46) and international ethical codes (The Declaration of Helsinki). Upon approval, we recruited participants from the Rowan-Virtua Neuromusculoskeletal Institute (NMI) who met the inclusion criteria: namely, adults (age 18 and over) at risk for opioid use disorder who had been experiencing chronic pain for at least three months, who were interested in using music for adjunctive pain management, who were able to access the sessions via Zoom from a private location and with reliable internet connection, and who could communicate in English. We excluded patients who were not at risk for opiate use disorder, lacked reliable internet connection for Zoom sessions, had moderate to profound hearing loss, and were diagnosed with a severe psychiatric disorder or cognitive impairment. Patients were referred by the PI directly and also self-referred in response to flyers posted in clinical areas and announcement emails sent to NMI patients. The Co-PI/music therapist screened patients via a telephone interview to assure eligibility for the group, and if patients were eligible and available, study staff consented patients. The consent process included patients meeting with study staff in person to review the requirements of the study and to answer questions. Participants’ informed consent included permission to publish de-identified data and direct quotes provided in the study. Participants who consented to enroll in the study then signed and retained hard copies of the consent form, which included an acknowledgement that data collected from the study would be publishable.
Support Group Intervention
The first author and Co-PI (a board-certified music therapist and certified practitioner in the Bonny Method of Guided Imagery and Music) provided two series of weekly sessions over Zoom to eligible pain patients. The first cohort met for five sessions, one hour each, to quickly assess initial acceptability and feasibility of the intervention. After receiving feedback from participants in the first cohort to lengthen the session time and increase the number of sessions, the second cohort met for six sessions, 90 minutes each.
First Cohort
The session structure for the first two weeks of the first cohort included time for greeting group members and checking in, doing any troubleshooting with the Zoom platform, followed by sharing positive music experiences over the past week, a brief interactive psychoeducation presentation by the music therapist about the effects of music experiences on pain, and then either participants sharing a favorite song with the group or the music therapist leading a directed MI experience.
Song sharing involved participants requesting a preferred song they wanted to introduce to the other group members, and the sharing usually included telling personal anecdotes about the song’s importance. The group often engaged in discussion after listening to the song, sharing about their reaction to it or how their relationship to the song has changed over time.
When the group took part in music and imagery (MI), the music therapist integrated elements of Bonny Method of Guided Imagery and Music into the intervention, beginning with a brief relaxation exercise and then streaming one music selection while describing a scene chosen by the group members. Usually, the scene was nature-based and included prompts to engage with the scene with multiple senses–imagining seeing, smelling, hearing, and touching. Music selections ranged from short classical pieces related to the GIM repertoire or ambient tracks, such as selections by Daniel Kobialka.47 This part of the session lasted approximately 10 minutes, after which participants shared their reactions to the experience. Sessions often closed with participants describing their personal goals for using music to support their pain needs over the next week. Both participants stated they preferred to access music online through YouTube, thus the therapist created a private playlist for the group that included each piece of music used in every session, including music from the MI portion. After every session, the therapist emailed links to this playlist and the psychoeducational material from the session to the participants.
Second Cohort
Feedback from the check-in surveys and final focus group was overwhelmingly positive, with participants requesting a longer session length and longer series of sessions. Thus we extended each meeting time from 60 to 90 minutes and met weekly for 6 weeks. The elements of the session structure remained consistent, with the addition of more participant involvement in the psychoeducation segment in response to questions arising from participants’ specific pain and other health conditions. During this series, we recorded the MI portions of two sessions and shared those recordings with group members for their use outside of sessions. The therapist included these links along with the YouTube playlist for this cohort’s music over the six weeks of sessions in post-session emails to the participants.
Qualitative Measures
After each cohort’s series of sessions, a member of the research team facilitated a focus group with the participants over Zoom. The meeting lasted an hour and addressed questions relating to participants’ experiences as group members, their opinions on the group, and their recommendations for future sessions (see Figure 1). We recorded and transcribed these groups for thematic analysis.
Figure 1 Focus Group Questions. Figure 1 continued.
Quantitative Measures
For the purposes of this project, we wanted to explore feasibility and acceptability of administering gold-standard measures with this population. We selected standardized measures relating to pain experience and quality, general health, and psychosocial impact of pain and self-efficacy for coping with chronic pain. Surveys were administered via Qualtrics, where participants received links via Email and text at each data collection point.
The Pretest survey asked participants to provide demographic information, including age, ethnicity, race, and educational background. The survey then included several measures from the PROMISⓇ bank of measures (Patient Reported Outcome Measurement Information System), specifically:48
● SF-3a Pain Intensity
● SF-4a Pain Interference
● 5a Neuropathic Pain Quality
● SF4a Psychosocial Illness Impact – Positive
● 4a Self-efficacy for Managing Chronic Conditions – Managing Symptoms
● Global Health v.1.2
Investigator-created, biweekly check-in surveys asked participants to rate their pain severity and tolerability before and after each session, with an additional open-ended comment added to the second cohort’s survey where participants could add any further feedback. The second cohort’s check-in survey included several additional items, asking participants to rate the helpfulness of the music interventions and whether and how often they used recordings of the MI interventions outside of sessions. The posttest survey repeated the pretest measures and also asked patients to state in their own words what factors impacted their pain in the previous 7 days. We conducted descriptive analysis of these data to determine trends in responses.
Results
Recruitment
Recruitment proved to be challenging, despite outreach to staff and physicians at the NMI, flyers posted in clinical areas, and the PI’s direct encouragement with eligible patients. For the first cohort, we screened four patients; one did not meet eligibility criteria and another did not complete the enrollment process, leading to two patients enrolling in the study. Participants in the first cohort included: a Black male, age between 60 and 70, with a high school degree, experiencing neuropathic pain, and a white female, age between 60 and 70, with an associate’s degree, experiencing neuropathic pain. For our second cohort, the two original participants continued in the group, and we screened four new patients: two did not meet eligibility criteria, one did not complete the enrollment process, and one enrolled in the group. The second cohort included the original two participants and the new member, a white male, aged between 40 and 50, with some college education, also experiencing neuropathic pain. With the first cohort consisting of two patients and the second consisting of three (though one member only attended one session), our recruitment fell short of our anticipated N of 8–10 per cohort.
Qualitative Feedback from Focus Groups
Our thematic analysis of the two focus group discussions revealed four overarching major themes: Self-efficacy, Structure and Music Techniques, Social Connections, and Practical Applications, comprised of thirteen sub-themes (indicated in italicized font within the text), several of which included multiple subcodes (indicated in italicized font). We provide example quotes for each main theme and some sub-themes within the summary below and present the main themes and sub-themes with brief definitions and example quotes from the focus groups in Table 1.
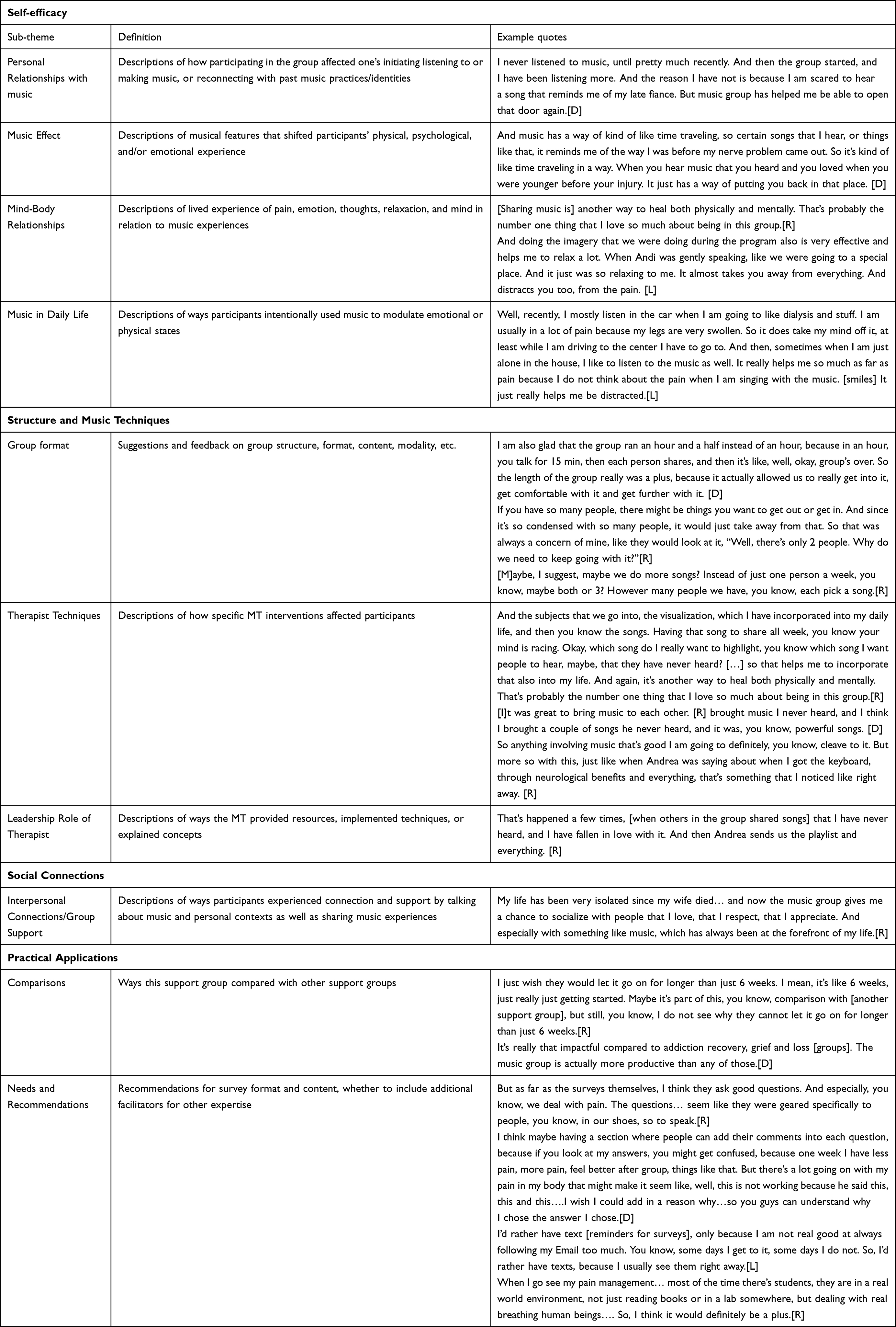 |
Table 1 Qualitative Themes |
Self-Efficacy
In this primary theme, participants described ways their engagement with the group supported their increased awareness of the music’s effect on their body, pain experience, and self, and incorporating this awareness into daily living. First, two out of the three participants shared a marked difference between their Personal Relationships with Music prior to taking part in the groups compared to after. Prior to the music therapy groups, these participants had limited their listening to or making music due to physical and/or emotional pain. By contrast, while they were taking part in the music therapy groups, these participants initiated listening to and/or making music for the first time in years. One participant vividly described reconnecting with his musician identity that had been lost due to his chronic pain:
I’m still learning the piano thanks to [D]. And that’s something I’ve wanted to do for a very long time, and now that I’m able to do it, and what it led to was me for the first time in 30 years, picking up my drumsticks. I never thought I would do it again […] now I’m back to practicing my rudiments on a daily basis [.] And it makes me also know that I didn’t dream it all. Sometimes I look back in my life thinking maybe I just dreamt it, it wasn’t really me. … It’s something I never thought I would do again…. But this was something very positive that also came out of being in this group. [R]
All participants described experiencing different effects of music (Music Effect) as a catalyst to shift one’s physical, psychological, and/or emotional experience, eg, using upbeat music to motivate physical movement or dance, to shift one’s mood, or intentionally elicit positive memories. This theme often related to specific techniques used in the group:
And doing the imagery that we were doing during the program also is very effective and helps me to relax a lot. When Andi was gently speaking, like we were going to a special place. And it just was so relaxing to me. It almost takes you away from everything. And distracts you too, from the pain. [L]
The Music Effect theme also emerged in tandem with descriptions of how group members intentionally used Music in Daily Life to attain different emotional or physical states. Participants then often described how they chose music according to specific attributes, such as tempo, timbre, etc, to support pain relief or avoid exacerbating pain.
When pain is at its worst, there’s some music I’ll avoid because I don’t want to move, and sometimes certain music can make you want to just get up and move around, and I know I can’t. So I try to avoid it sometimes. [R]
In addition to descriptions of the effects of the dynamic qualities of music, participants also reported their awareness of Mind-Body Relationships: their lived experience of pain, emotion, thoughts, relaxation, and mind in relation to the music experiences and that their immersion in the music experience could help them manage their pain. The participants often described the interplay between thoughts, emotions, conscious awareness, and bodily states along with their use of Music in Daily Life or along with Techniques they experienced in the sessions.
[M]usic just has a way of…it distracts you as well as…it’s kind of like a crutch to help you through physical or emotional pain. And it’s just so much more powerful than just words, you know. And the group was absolutely amazing. I could tell that my pain was… not that my pain was better, but it helped me process something else instead of the pain, which was a huge plus. [D]
Structure and Music Techniques
This primary theme encompasses feedback and suggestions regarding the group format and the therapist’s techniques and role employed in the sessions. With respect to Group Format, participants expressed their preferences regarding the length of sessions, how sessions were structured, group size, accessibility of sessions, and privacy. Nearly all participants shared that in terms of Structure-time a 90-minute-long session was much better than 60 minutes, noting that even with the longer sessions, the therapist needed to manage the time so that participants could share longer pieces of music without concern of needing to cut them short. Participants in the second cohort suggested reorganizing the elements of the session to allow participants to share their individual songs before the MI portion of the session to allow time to hear the entire song. All participants expressed sadness and disappointment with the limited Number of sessions, saying they wanted the group to continue indefinitely. Participants highlighted the Accessibility of the groups, sharing that they liked the convenience and ease of using Zoom. Two of the participants had previous experience using Zoom for other group support sessions, therefore they were familiar and comfortable with the platform. At times participants joined the sessions from public locations (like a bookstore cafe) or from a hospital bed; in the second focus group, participants shared they were not overly concerned about Privacy in these situations, though the therapist checked with participants at the time to ensure everyone consented to these situations, and that participants were using headphones/earbuds so that audio from the call could not be overheard by non-group members. The second cohort discussed how the ideal Group size would be small (no more than five members) to allow time for each participant to share and be heard.
Related to the Group Format, participants described how they benefited from each of the specific Therapist Techniques the music therapist employed in the session, which could reinforce their self-efficacy (MI/Relaxation with music, Selecting and listening to a song together, Teaching about research or other narratives related to participant needs).
She’d ask us where we want to go, and then we would, like, I picked Hawaii. And she would set the scene. Just in a soft voice, plus she had the music playing. And she would just speak the whole time, most of the time. Kind of getting you in the mood, so to speak. For, you know, to listen to and relax with the music. And it was very effective. [L]
The participants also often described the Leadership Role of the therapist, including ways the therapist implemented techniques and things the therapist did or explained that enhanced the mind-body effects of the music experiences.
The guided imagery was amazing, because it totally… it helps you with your pain. You’re focused on, you know, from your head to your feet. Then you go somewhere else. She was very good at describing the small things as well as the big things. And it really…it just puts you in a different place and a different frame of mind.[D]
Social Connections
This main theme included themes and subthemes related to the importance of members’ interactions in the context of the support group: Interpersonal Connections and Group Support. These themes were central to the participants’ description of the benefits they experienced in terms of their pain and overall well-being. Participants shared the value of both discussing music and their personal contexts (Interpersonal connections-Talk) and sharing music experiences (Interpersonal connections-Music) with peers during the sessions.
Being able to sit and talk with someone about something that I love so much as music, and especially in, you know, dealing with pain, that was a great idea…. And learning to play that and all the connections and everything to it, talking about the music that we love to hear. The last time we were on, in fact, [L] suggested a song that is now my first thing in the morning song. “Good Day” I think it is called. And, you know, being able to talk to other people about music instead of just the usual, you know, my friends, my inner circle, whatever. And especially dealing with pain and how it’s associated with pain, I thought, was a great idea. [R]
Practical Applications
The final primary theme included subthemes related to the practical experience and outcomes of participating in the group. One unexpected subtheme that emerged included Comparisons between this group with other support groups participants had experienced previously or currently. One participant [D] spoke about the holistic role the group played in addressing not only their pain needs, but other co-occurring needs.
And, you know, like addiction recovery is very dear to my heart. I’ve been clean for 14 years now. Grief and loss is very important to me. …. And I honestly would trade both [addiction recovery and grief] groups for the music group, because the music group covers all avenues, mental and physical pain. Whereas each of the other groups don’t. [D]
Finally, in the theme of Needs and Recommendations, we asked participants about the accessibility, utility, and relevance of the surveys, and for any other concerns or recommendations they had. Most participants preferred to receive the survey links via text message, and they all stated that they found the length of the surveys very manageable. They also stated the surveys addressed relevant needs and concerns they have. One participant requested that the survey include a space to comment about their pain ratings over the previous two weeks, as they felt that these ratings might not reflect the positive effects of the music group; rather, their pain may have worsened for other reasons.
Aside from the surveys, participants recommended spending more time in the sessions to listen to songs members share with the group; this could mean members could share more than one song within each session, or members could choose longer songs to share without fear of running out of time before the session ended. As group members D and R discussed this in the focus group, D shared:
Yeah, it’s very important to be able to express how that song makes you feel and why it makes you feel that way. So putting it somewhere in the middle would probably be better.
Finally, when asked about welcoming a medical student in future groups who would assist with providing psychoeducation about the physiology of chronic pain and related conditions, participants in the second focus group expressed enthusiasm.
Therapist Themes
In this section, the first author/interventionist (AMH) writes from her personal perspective to consolidate themes in response to the focus group data.
After we analyzed the focus group data, I reviewed my session notes and considered the participants’ qualitative themes in the context of my experience as the facilitator of the group sessions. The most resonant themes I found included the participants’ strong desire for social connection, their pre-existing and evolving musical identities, finding a shared language in the group to describe and explore the pain experience, group bonding and solidarity over music and pain experiences, and the transformational power of the music for each participant.
Social Connection and Belonging
Early in the first series of sessions, it became clear that these participants greatly needed this group for social contact, as the members emphasized that any interruption in sessions had to be rescheduled that week to maintain the weekly connection. For all of the participants, their medical conditions combined with their pain had caused significant social isolation, further exacerbated by COVID-19 lockdowns and restrictions, and from which they never really recovered a few years later. For R, at least, this led to further mobility limitations, exacerbated by being ill with COVID; together these prevented him from attending concerts and other social gatherings he dearly missed. In L’s case, her comorbidities required ongoing and time-consuming treatments and appointments, leaving her with little energy and time to attend social gatherings. D was managing full-time caregiver responsibilities on top of his treatment schedule and pain condition. Some participants also shared how their pain diminished their sex lives, too, robbing them of physical intimacy on top of the social isolation from friends and family.
Individual Relationships with Music and Musical Identities
Before taking part in the support group, each participant had unique, strong relationships and identification with music in some way. Whether it was a history of playing music, attending concerts, connecting to a spiritual tradition, or relating to important people and life events, music was incredibly important to each person regardless of any musical training or performing experience. Pain also interfaced directly with these musical relationships and identities. In negative ways, pain interfered with playing music or attending concerts, or certain music associated with major losses caused emotional pain, causing participants to avoid freely listening to music on the radio or TV. Such interference further exacerbated difficulty regulating emotions when in pain. In positive ways, listening to music could be a safe haven from emotional and physical pain, providing support, distraction, and connection with others. Thus, even if experiencing music was sometimes emotionally or physically difficult for these participants, they knew that music could be beneficial for their pain experience, and they were drawn to this support group.
As group members shared, talked about, and experienced music over the course of several weeks, each of them rediscovered their previous musical self in a new way and/or formed new relationships with music and developed another part of their musical identities. For example, R began learning to play a new instrument to him, the keyboard, while at the same time feeling motivated to begin practicing drumming again. Other group members shared their eagerness at learning about new music from others and hearing how this music was meaningful to their peers. The MI portion of the session almost always involved introducing the members to music unfamiliar to them, and in each case the participants shared the positive associations they had with the music and the imagery experiences they underwent with it. In some cases, music that had been emotionally painful in the past for members became enjoyable and positive once it was shared in the context of the group. Thus, the group members reconnected with and expanded their musical identities along with their emotional and social spheres and capabilities.
Shared Language Around the Pain Experience
In the original concept of the group structure, I had planned to provide psychoeducation around how music can support pain relief; I drew from the latest published literature to select topics and led discussion around those topics with the group members. These discussions often led participants to raise questions I had not anticipated nor was I prepared to address them. Therefore, I would look up research on these questions and return the following week with additional information. Ultimately, the process evolved to the point where the participants directed the psychoeducation portion of each session, and I responded to their interests. For example, R described to us how playing his keyboard on his own helped with his “fibro-fog”; I researched and then provided evidence to support his anecdotal experience showing the possible mechanism of that action.49 This led to me understanding their pain and music experiences more deeply, making connections between participants’ experiences with music and pain that even they were not aware of or understanding until we explored them. Therefore, through our collaboration, the sessions validated participants’ experiences, while also finding a shared language about pain among group members, using music as a vehicle.
Song Sharing for Connection and Emotional Healing
The group emphasized the importance of song sharing and describing memories and feelings associated with these songs. This was particularly powerful for D given he had been avoiding listening to the radio for years so he would not inadvertently hear any songs that would remind him of his deceased partner; but when participants and he shared and reminisced about songs from his young adulthood, D shared he found himself emotionally and even physically connecting to music again–recalling how his body felt when he first heard that music, prior to the onset of his pain condition. The group resonated with the concept of music from their past as a “time machine”, where participants felt they could travel back to experiencing their bodies from before their pain conditions began. In addition, participants appreciated hearing music they had never heard before, and listened to songs they especially liked outside of sessions via the running playlist. For example, R described how a song that L had shared was his “new favorite”, and he chose to listen to it every morning to help him start his day.
Music and Imagery for Relaxation and Restoration
I had intended for the MI portions of the sessions to include positive, pain-free body awareness within the images that the participants wanted to experience. In these images, I described our bodies moving freely in peaceful scenes. For example, every MI experience began with a breath-based relaxation induction and mental body scan, from head to toe. Following the request of the participants, I started playing the music selection and guided the participants to feel their bodies standing firmly, sensing the ground under their feet. In one scene, I then described walking along an uphill path as a nature scene unfolded around them. I emphasized feeling the ground with each step, the ease of the gentle ascent, and breathing in the clean air. When we reached the scenic lookout in the imagery, I described the physical sensation of sitting on a large flat boulder, feeling the hardness of the rock, and relaxing in a comfortable position. Toward the end of the music selection, I guided the participants to imagine standing up and gently walking again, still aware of the sensations of each step. In each session, participants reported that they felt physical relief and emotional calm after the MI experiences, providing a much-needed “break”. We discussed how these breaks were beneficial, and I had a sense they were also opening participants to be less at odds with their bodies–because they could experience the capabilities and strengths of their bodies for a while through their imagination.
Limitations of Music for Pain
Sometimes music cannot address severe pain, or it can exacerbate certain types of pain. Having myself recovered from a severe, painful illness several months before working with this group, I knew firsthand that music could not help every pain situation. The group found solidarity and commiseration sharing about such experiences and how they cope with them. These discussions included naming the ways they work to regulate their emotions, and shift their attention and body awareness to gain more control over the pain until it subsides. For example, R shared once that during extreme pain flares, he would “close off” all other stimuli he was experiencing, and also strive to manage his emotional state so it would not exacerbate his pain. Though we discussed this topic several times, none of the participants reported worsening pain or related symptoms during or after the support sessions.
Feasibility of Quantitative Measures
Given our aim to assess the feasibility and utility of the measures, and the very small sample size of the groups, we present the quantitative results for trend observation only. We assessed trends in ratings across individual cases to verify that participants did not report worsening symptoms during the study and to corroborate their responses as a group with the focus group data. For this section, we refer to participants A, B, and C, however these initials are not linked to the initials used in reporting the focus group data in the subsequent section. Not all participants completed the entire survey at both data points, limiting our ability to make comparisons. Only Participant B completed both pre-tests and post-tests in both cohorts; Participant A completed only the pretest in both cohorts. Participant C completed the pre- and post-test surveys for cohort 2 only. PROMIS48 ratings in the pre- and post-tests were within expected ranges for patients with varying pain conditions. We calculated T-scores for each measure and, for measures with available cut-off scores, determined categorical ranges (eg, severe, moderate, good) for the participants’ scores. In cases where we obtained complete pre- and post-test scores, we calculated the difference between T-scores; PROMIS48 guidelines state that a change of 5 to 7 points in individual T-scores suggests “meaningful change”.
Given the available data, we compared complete pre-/post-test datasets for pain intensity (SF-3a), pain interference (SF-4a), and neuropathic pain quality (5a) (Table 2). The patients’ ratings of pain intensity and quality shifted slightly across cohorts. Participant A’s Pain Intensity scores were in the Mild range at pretest in both cohorts, whereas participant B’s ratings were in the Severe range, and C’s ratings were in the Moderate range; these ranges did not change for Participant B and C at posttest. In cohort 1, Participant B showed a decrease in pain intensity and interference from pre-test to post-test, with a meaningful change of reduced pain intensity at posttest in both cohorts. Participant C had no change in pain intensity or interference from pretest to posttest. All participants rated their pain as neuropathic at pretest (causing sensations such as burning, tingling, or stabbing); however, there were no meaningful changes from pre-test to posttest in either cohort.
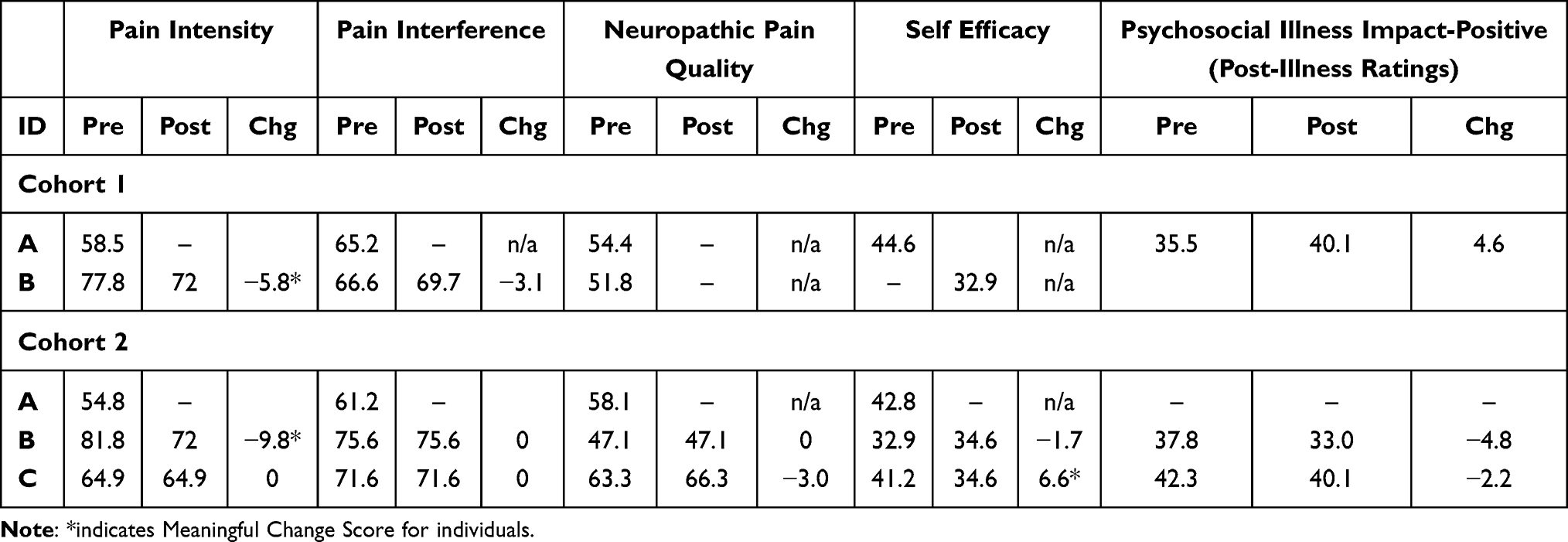 |
Table 2 Individual Pre- and Post-Test T Scores on PROMIS Pain Intensity, Interference, Self-Efficacy, Psychosocial Illness Impact-Positive Scales |
We obtained incomplete data in the Self-efficacy scale (4a) (Table 2), with additional missing pre-test responses from Participant B in the first cohort. When comparing this participant’s pre- and post-test responses for cohort 2, they showed a slight increase in their confidence in managing their symptoms (higher scores indicate more confidence). In contrast, Participant C’s ratings indicated a meaningful decrease in confidence managing symptoms from pre-test to posttest in cohort 2.
In response to the SF4a Psychosocial Illness Impact items (Table 2), participants rated the degree to which they were comfortable with themselves, their connection with their friends, their ability to adjust to change, and feeling their lives are meaningful–these ratings related to two data points, reflecting on their perceptions from before the onset of the pain condition, and since the onset of the pain condition. Table 2 displays the T-scores for ratings since the pain condition began. Whereas participants indicated that their pain condition often had a negative impact on these phenomena at the start of the study, with meaningful differences between these points for Participants A and B, there were few changes in ratings post-illness onset across pre- and post-test surveys.
Responses to Global Health v.1.2 (Table 3) had the same response patterns as the other measures. This scale results in two scores, Global Physical Health and Global Mental Health, with single item ratings of general health and ability to carry out usual social activities/roles. Overall, Participant B’s ratings indicated both poor physical and mental health, according to PROMIS cut-off scores; the physical health scores did not change at posttest for cohort 2, however the mental health scores slightly (but not meaningfully) improved. Participant A’s physical health scores fell in the Fair range at both cohorts’ pre-tests, and Participant C’s physical scores also fell in the Fair range at pre-test in cohort 2. This pre-test score resulted in the only meaningful change score across all Global Health subscales, where Participant C’s physical health ratings moved from Fair to Poor health range. Whereas this participant’s mental health ratings worsened slightly between pre- and post-test, the difference was not meaningful. In terms of general health, Participant A rated their health the highest as “Good” at both pre-tests, along with Participant C in cohort 2. Participant C downgraded this rating to “Fair” at post-test, consistent with their other ratings on the scale. Participant B reported their health as “Poor” at pretest and at both cohort’s post-tests. Participant B and C rated their ability to participate in social activities and roles as “Poor” across datapoints, whereas Participant A reported their ability as “Good” at pre-test for cohort 1, and “Fair” at pre-test for cohort 2.
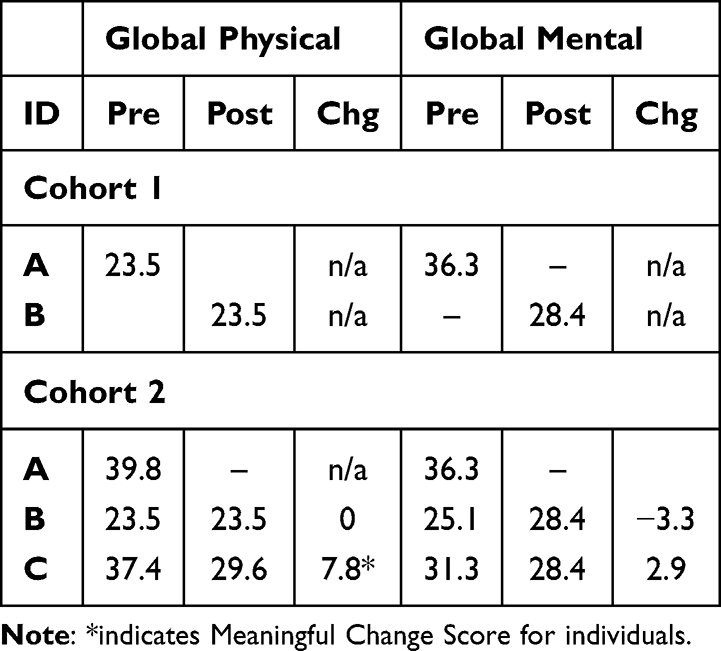 |
Table 3 Individual Pre- and Post-Test T Scores on PROMIS Global Health Scale |
Figures 2 and 3 include the obtained responses from the biweekly check-in surveys for both cohorts regarding pain severity and pain tolerance before and after sessions. Responses were incomplete at times, with no responses beyond the second check-in survey in cohort 2. In cohort 1, Participant A reported a decrease in pain severity following the intervention, with a corresponding increase in pain tolerance following that week’s session (rating a 0 pre-session and 4 after the session). In cohort 2, Participants B and C reported a decrease in pain severity from before to after sessions at both check-in surveys. Participant B reported an increase in pain tolerance following intervention at both check-ins whereas Participant C reported a decrease in pain tolerance following intervention at both check-ins.
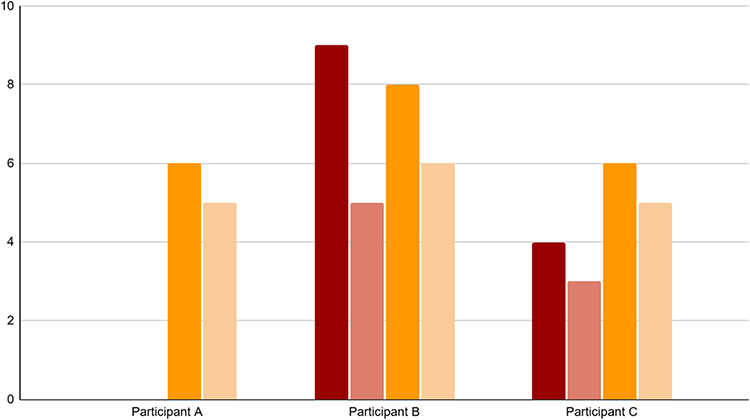 |
Figure 2 Pain Score Ratings (0= no pain, 10 = worst pain); before sessions at check-in 1 (dark red), after sessions at check-in 1 (light red); before sessions at check-in 2 (dark yellow), after sessions at check-in 2 (light yellow). |
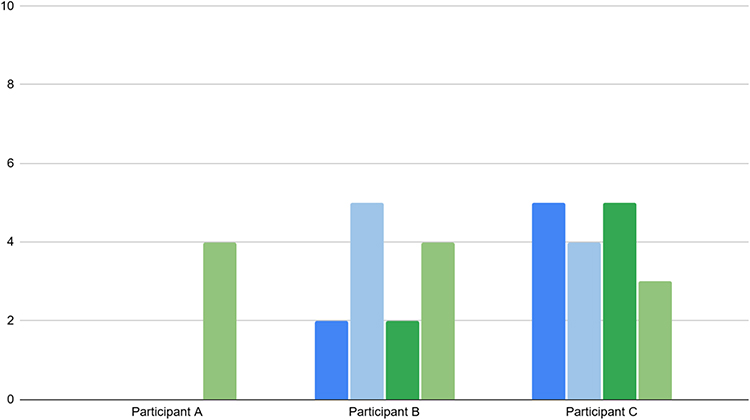 |
Figure 3 Pain Tolerance Ratings (0 = no tolerance, 10 = most tolerance): Before sessions at check-in 1 (dark blue), after sessions at check-in 1 (light blue); before sessions at check-in 2 (dark green), after sessions at check-in 2 (light green). |
The check-in surveys also asked participants to indicate their preferences regarding session length and to indicate which parts of the session were their favorite, which parts were their least favorite, and any suggestions for changing the session. The surveys for cohort 2 also asked participants to rate the helpfulness of group sharing about music for pain and the MI intervention, as well as how often participants used the recordings of the MI intervention outside of sessions. These responses are summarized in Table 4. Participants rated the session length as either “about right” or “too short”. Participant A, who only responded to the check-in for cohort 1, focused their comments on playing music and discussing the songs, whereas Participants B and C focused their comments on the benefits of MI for their pain, which corresponded to their high ratings on the helpfulness of MI. Participant B rated the helpfulness of group discussion high as well (8/10), however Participant C commented across both check-in surveys in cohort 2 that they disliked long discussion around members’ personal history with music and wanted more direct discussion about using music for pain management.
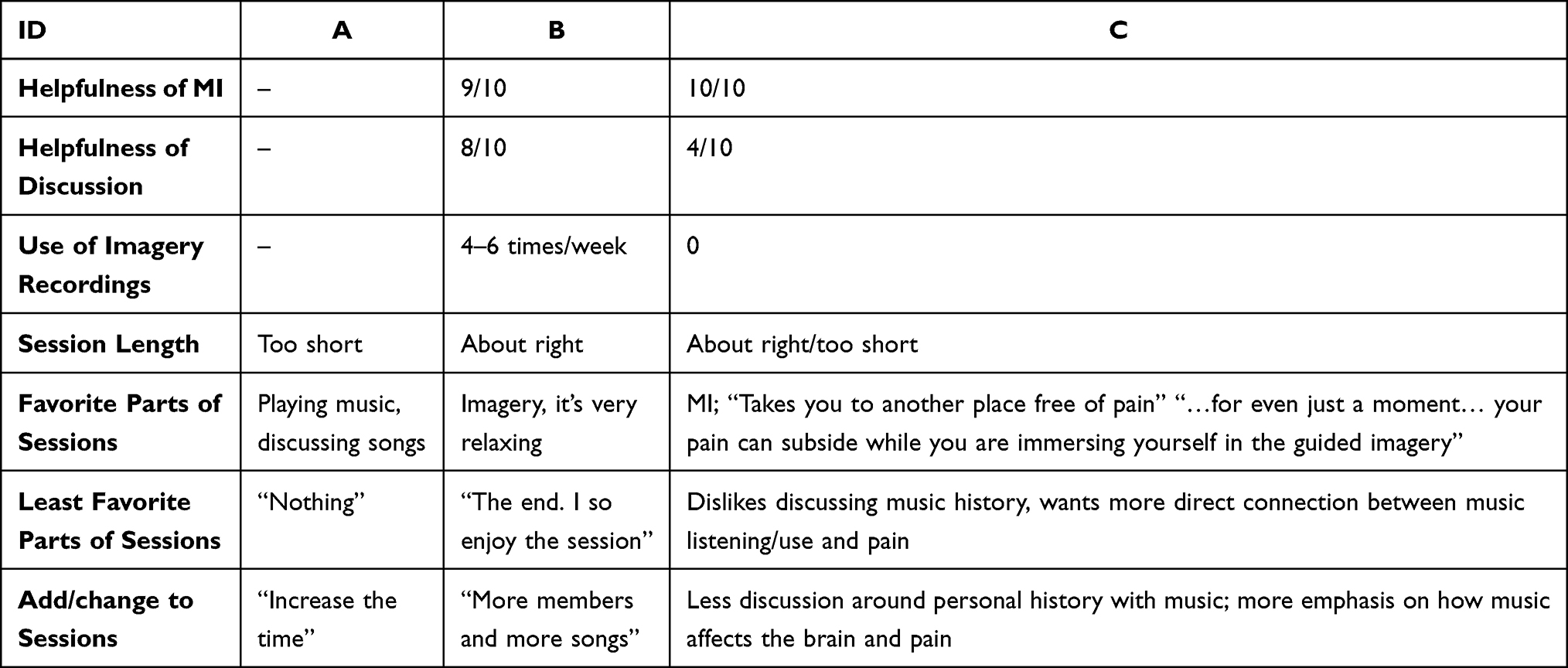 |
Table 4 Summary of Check-in Survey Ratings and Responses to Session Structure |
In summary, according to the guidelines set by PROMIS,48 the only meaningful changes in scores included participant B’s decreased pain intensity ratings from pretest to posttest (cohorts 1 and 2), and Participant C’s decreased ratings of self-efficacy and physical health (cohort 2). However, according to the submitted check-in surveys, all participants reported trends of decreasing pain following the intervention, whereas Participants A and B reported an increase in pain tolerance following the intervention. Contrarily, despite highly rating the helpfulness of MI, Participant C reported a decrease in pain tolerance after the intervention, results that could reflect their worsening health condition as reported in the Global Health measure, or could be an error in their understanding of the survey item given their free response to the open-ended comment on the survey. Participants also stated that their favorite parts of the sessions included song sharing and MI, and they indicated their desire for longer sessions, more information and discussion about using music for pain relief.
Discussion
Here, we discuss both the practical and theoretical implications of this initial data collection, focusing on our aims to develop a participant-focused approach for a telehealth support group and the feasibility of data collection and use of the selected measures. We note that the qualitative themes from the focus groups reflect our findings from our background literature search, indicating that self-efficacy in music experiences, social connection, and accessibility related to the group structure, measures, and data collection procedures are significant and relevant to the needs of these patients. Table 5 presents our synthesis of themes from our review of the literature with specific interventions of the protocol, the themes derived from the focus group data and therapist reflections, and the quantitative trends and comments from check-in survey responses. We found that these themes overlapped and enhanced one another, leading to practical and theoretical implications for practice and future research.
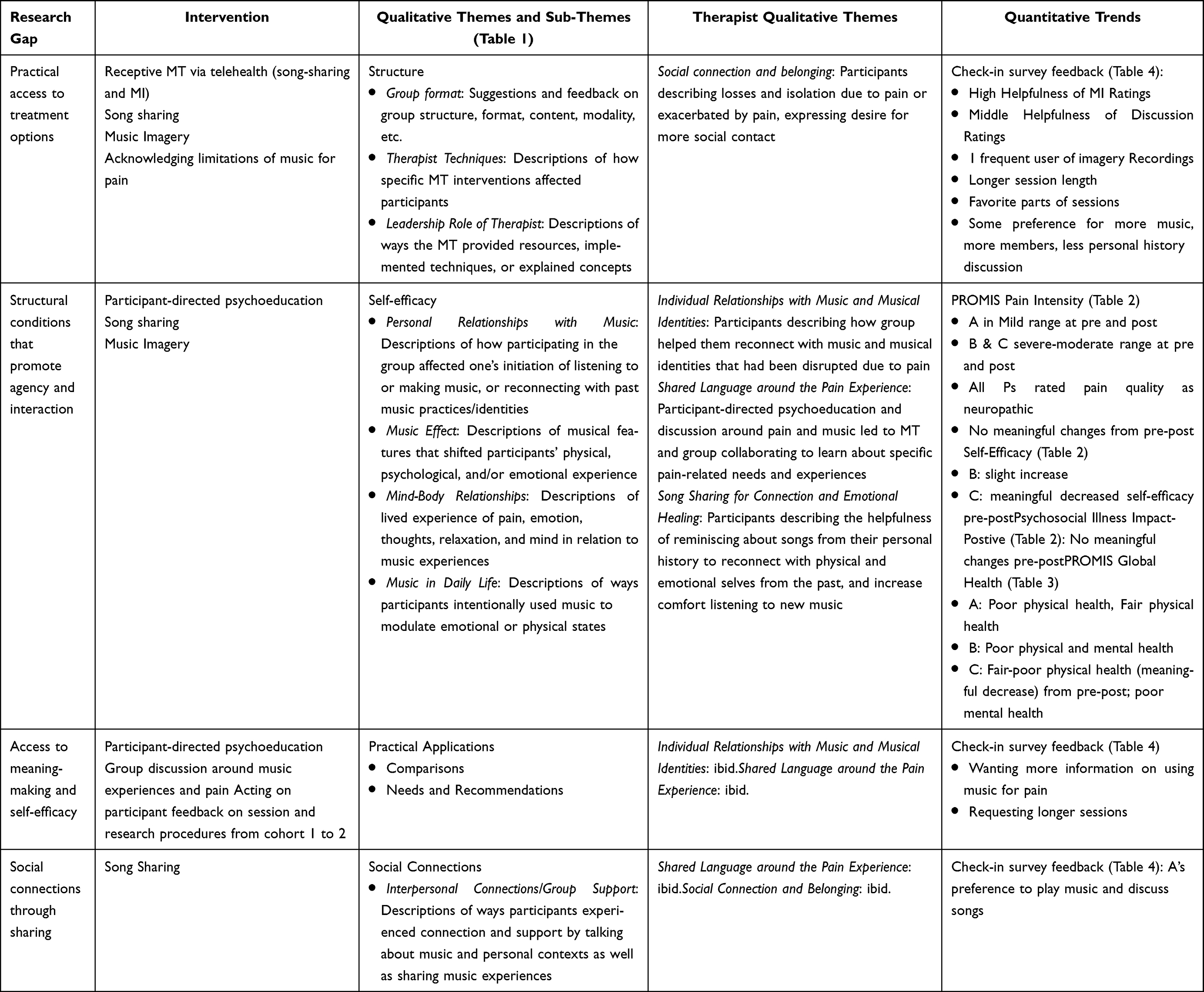 |
Table 5 Synthesis of Themes: Research Gap, Telehealth Interventions, Qualitative Themes, and Quantitative Trends |
At a very practical level, the participants’ enthusiasm and endorsement of the support groups indicate the model is worthy of further investigation and development. These participants face significant challenges in their physical and mental health that imposed barriers on even meeting in person for the consenting process, let alone completing all the steps of the enrollment process. Based on what participants shared during sessions, the likelihood that they would regularly attend an in-person support group was very low; in contrast, the participants expressed great disappointment in the limited number of Zoom sessions and desired that they continue for much longer than 5–6 weeks. Thus the telehealth option provided an accessible opportunity for patients who can be difficult to reach and support.
We had initially included psychoeducation as part of the group structure with the intention of providing participants information about their pain condition to support their self-efficacy in managing their pain. As the group format evolved, with participants directing the topics for psychoeducation through their questions and descriptions of their pain experience, this intention shifted to the participants taking more control over the information they wanted and, thus, enacting self-efficacy within the group structure. In so doing, the participants educated us on their experiences and how music interacts with their pain in their day-to-day lives. This led to a much more egalitarian relationship between the music therapist and the group members, though the therapist’s role as the information-bearer remained. As topics and questions evolved from session to session, the music therapist had to gather information from outside her knowledge base, requiring her to attempt to decipher medical research that was beyond her scope of practice. At the completion of the second cohort, the music therapist felt that it would be most effective and ethical to have a medical practitioner assist with the psychoeducation piece in future cohorts.
Our use of receptive music therapy interventions that did not require additional materials such as instruments or supplies allowed for much easier access for participants to join the groups from different locations than their homes, and our approach did not inhibit the effectiveness or interaction with the materiality of the music. Other music therapy telehealth models have worked well with live music, though with some limitations of simultaneous music-making, requiring interventions that can work with audio lag.27,28 Whereas our participants did not express interest in live music-making together, future cohorts may desire it. We will remain open to participant feedback and explore this possibility.
Over the course of this project, we determined a clinical need to expand access to patients who are unable to use opioid medication. With our initial aim focused on reducing opioid use, we excluded at least one patient who desired to participate in the group, and became aware of other potentially eligible patients who had a similar need. Such patients also need adjunctive treatment options, and this intervention could benefit them. Therefore, future studies should address this treatment gap.
The telehealth delivery model raised interesting practical and ethical implications. We found that extending the reach of music therapy services to patients in their own living spaces not only increased accessibility for our participants but also helped garner their trust; this was the case in other applications of telehealth music therapy.27 However, we also encountered situations that tested participants’ confidentiality and privacy when one patient wanted to join the session from a public cafe, and another patient joined the session from her dialysis bay. As each of these situations arose, the group discussed the need to protect privacy and confidentiality, and gained all attendees’ verbal agreement to proceed with the session. Participants are, ultimately, the only ones who can be responsible for managing privacy on their end by ensuring that no one out of view of the camera is overhearing the session, and even if they are wearing headphones in a treatment setting, that they do not reveal private or confidential information within earshot of others. Music therapists retain responsibility for establishing clear inclusion criteria for programs, managing any internet interruptions during sessions, and abiding by all legal and ethical requirements inherent in telehealth services.
The data collection process proved to be challenging; the participants shared in the focus groups that some preferred to access the surveys through their emails, while others preferred receiving reminders and links through text messages. However, when we implemented both options, we still had incomplete responses. Thus, we need to continue refining our data collection procedures. Furthermore, our trend analysis of the incomplete measures, particularly the PROMIS48 measures, did not clearly mirror the participants’ qualitative descriptions of benefit from the intervention. In contrast, the check-in surveys appeared to more generally reflect the participants’ descriptions of beneficial effects of the intervention. Whereas the PROMIS pain scales have been extensively tested and validated, they are relatively new compared to other pain scales, therefore additional research needs to establish their long-term reliability, responsiveness to change, and applicability to chronic pain patients.50 To best detect participants’ response to the intervention, in future studies we will investigate multiple formats for assessing participants’ individual pain experiences.
Though this is a very small dataset, our initial findings also revealed some theoretical and conceptual implications to consider for future iterations of this intervention. These considerations include possible mechanisms of action and potential research approaches that could shape the design of future studies.
The focus group themes echoed findings from previous research that showed belonging and social inclusion as important mechanisms in chronic pain treatment in general and in studies on music therapy for chronic pain;8,30,31,51–53 Whereas previous research on group music therapy emphasized active music making in their interventions, our study implemented receptive interventions delivered via telehealth. Similar to the previous music therapy studies, our participants experienced significant loss around their social lives resulting from their chronic pain and comorbidities, and also shared how this group provided a much-needed social connection. The telehealth delivery method did not impede these connections, rather it enabled them to establish and develop among these participants. This benefit of telehealth has been reported in other studies as well.28
Unique to this project, however, are the social benefits of receptive music therapy methods delivered via telehealth. The participants’ emphasis on sharing preferred songs with each other in tandem with sharing about their pain experiences highlighted the importance of finding language and understanding around challenging circumstances in order to be understood. In this vein, author Elaine Scarry wrote about the inexpressibility of pain that exacerbates its isolating effects, especially when facing chronic pain.54 Sharing songs in this support group context also provided an opportunity for participants to engage in cognitive agency in their pain management via sustained attention to each selection and the meaning it held for their peers. Sustained attention to self-selected, familiar music for pain management is a component of the Cognitive Agency mechanism; this involves top-down processing in moderating pain. Often, participants shared songs that carried strong personal meanings, memories, and pleasant experiences. Research indicates that these deeper connections to music have an even stronger analgesic effect and may indicate another cognitive mechanism of Meaning Making and Enjoyment.49 These participants may have also engaged these mechanisms by using music as a mediator for making sense of and telling a story about themselves and their world of pain. Altogether, the participants’ song sharing supported several important phenomena: bridging participants’ embodied experience with language to integrate their emotional, physical, and spiritual pain, taking agency over their pain experience through selecting preferred music, and in experiencing personally meaningful and enjoyable music for themselves as well as sharing with others.
The participants’ enthusiasm for the MI intervention is reflected in their reports of how the imagery experience provided a respite from their pain long after the session. Whereas the participants requested imaginal scenes in relaxing places, away from day-to-day stressors and problems, the music therapist often directed the guiding to support a positive, pain-free connection to the body by invoking body awareness and imagining unhindered, gentle movement. Research shows that body awareness (versus body dissociation) is important in healing from physical and psychological trauma, including chronic pain.55 Chronic pain patients often use body dissociation to cope with pain, however research shows this has been detrimental for patients.56 Whereas previous researchers emphasized active music therapy techniques to help chronic pain patients restore a positive relationship with their bodies through singing, instrument playing, and movement,31 MI can also facilitate increased body awareness with directed imaging to help patients mentally rehearse pain-free movements and body sensations that could be disrupted due to the chronicity of their pain. Just as many approaches such as yoga, mindfulness meditation, and Feldenkrais can facilitate the mind-body connection, MI affects somatosensory regions along with the insula, a critical structure that integrates sensory and affective perception and forms part of the interoceptive neural network.57–59 Thus there could be a neurological basis for MI interventions to improve patients’ mind-body awareness that would be interesting for future study.
Therefore, with a feasible trial protocol in place, it is possible to design future studies to examine both the efficacy and the mechanistic roles of music interventions designed for limitations of telehealth–that is, using listening-type interventions rather than live, synchronized music. The telehealth delivery model can recruit patients from many locations and could be ideal for a multicenter trial; this would support a suitably-powered clinical trial, which is often difficult to achieve in music-based intervention studies. The trial could include head-to-head comparisons of the effects of a non-music support group against a group involving music interventions such as MI and song sharing, and perhaps directly compare MI against verbal-only guided imagery. If these next studies continue to show promising results, including qualitative data indicating subjective phenomena relating to the music interventions and pain relief, then we can begin to study neurological mechanisms of MI interventions that facilitate beneficial body awareness for pain, perhaps involving biometrics through mobile apps and self-reports to track longitudinal responses and outcomes.
We note several important limitations of this report. First, this is a very small dataset involving three unique participants, and with inconsistent completion of the quantitative measures. Whereas we may have found some trends in ratings of pain intensity, interference, and quality, as well as pain severity and tolerance, we cannot conclude that these are the result of the telehealth intervention. The mixed and incomplete responses to the PROMIS48 measures indicate the need for further investigation to determine whether participants faced difficulty with the data collection process or with the measures themselves. Furthermore, all these measures are based on perceived effects of the intervention, and do not indicate clinical efficacy. In addition, participants self-selected to participate in the study based on their personal interest in music interventions for pain, thus we cannot rule out selection bias.
Given these initial outcomes, we have started a third cohort to obtain additional data to finalize the group protocol and structure in advance of larger trials in different settings. We have included patients who were previously excluded due to health conditions that contraindicate opiate medications, resulting in higher recruitment numbers. In response to participant feedback, we will evaluate the feasibility of this larger group size (N of 6) and a longer series of weekly sessions. We have also included a medical student to assist with the patient-directed psychoeducation component of the sessions. With more participants, we will undertake a deeper analysis of feasibility and utility of quantitative measures for this intervention, as well as a more holistic qualitative analysis of the focus group interview, integrating both video and transcript data into the analysis. These analyses will help us determine the final group protocol and measures for future feasibility studies in different settings.
Conclusion
When combined with the accessibility of telehealth delivery, receptive music therapy techniques such as song sharing and MI in a support group format can be vital tools in supporting chronic pain patients who may not be able to undertake face-to-face music therapy due to limited mobility, chronicity of health conditions, or other barriers. Participants in these initial groups reported that the song sharing, MI, psychoeducation, and group support within the telehealth delivery model promoted their ability to manage their pain within and outside of sessions, improved their personal relationships with music, and provided meaningful social support and shared knowledge about how music can support them in managing their pain and other stressors. This model provides a cost-effective and accessible way to support patients in great need but who are also difficult to reach and treat. Patients who undertake telehealth music support may ultimately elect to attend face-to-face music therapy sessions once their health or other circumstances allow; otherwise, they can remain connected to an online support system that could reduce social isolation and provide pain management tools.
In sum, advances in video conferencing, music streaming and sharing, and biometrics hold great potential for extending and advancing greatly needed music-based support to medically, socially, and economically isolated patients with chronic pain. Such support has the potential to reduce the risk of opioid use and dependence while improving the quality of life for many patients via feasible, cost-effective delivery models. Furthermore, research into the mechanisms of these interventions will continue to inform the refinement of MI techniques and selecting music for listening interventions. With these advances in technology and delivery models, practitioners can bridge a substantial treatment gap using a proven non-pharmacological and patient-centered approach.
Acknowledgments
The authors wish to extend gratitude to the Rowan-Virtua SOM Music Medicine Club, Dr. Jeffrey Powers, Chris Malcolm Lynsung, Eva Attotta, Rachel Caldwell, and Nesha Daneshwar for their support on this project and in final preparations of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):328–24. doi:10.1097/j.pain.0000000000002291
2. Bruun K, Bye-Møller L, Vaegter HB. High-impact chronic pain. International Association for the Study of Pain, 2023. Available from: https://www.iasp-pain.org/resources/fact-sheets/high-impact-chronic-pain/.
3. Sherry TB, Roth CP, Bhandarkar M, Hepner KA. Chronic Pain Among Service Members: using Administrative Data to Strengthen Research and Quality Improvement. RAND Corporation. 2021. Available from: https://www.rand.org/pubs/research_reports/RRA1160-1.html.
4. Nonopioid therapies for pain management. CDC; 2025. Available from: https://www.cdc.gov/overdose-prevention/hcp/clinical-care/nonopioid-therapies-for-pain-management.html.
5. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain. MMWR. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
6. Zhang Y, Wu B, Qin P, Cheng Y, Chen Y. Alternative therapies in chronic non-cancer pain management: a scoping review of randomized controlled trials. Complement Ther Med. 2025;90:103154. doi:10.1016/j.ctim.2025.103154
7. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;10289(397):2082–2097. doi:10.1016/S0140-6736(21)00393-7
8. Sihvonen AJ, Pitkäniemi A, Särkämö T, Soinila S. Isn’t there room for music in chronic pain management? J Pain. 2022;23(7):1143–1150. PMID: 35124251. doi:10.1016/j.jpain.2022.01.003
9. Booker S, Herr K, Tripp-Reimer T. Black American older adults’ motivation to engage in osteoarthritis treatment recommendations for pain self-management: a mixed methods study. Int J Nurs Stud. 2021;116:103510. doi:10.1016/j.ijnurstu.2019.103510
10. Pristell C, Byun H, Huffstetler AN. Opioid prescribing has significantly decreased in primary Care. Am Fam Phys. 2024;110(6):572–573.
11. Bradt J, Dileo C, Myers-Coffman K, Biondo J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev. 2021;10(10). doi:10.1002/14651858.CD006911.pub4
12. Fu VX, Oomens P, Klimek M, Verhofstad MHJ, Jeekel J. The effect of perioperative music on medication requirement and hospital length of stay. Ann Surg. 2020;272(6):961–972. doi:10.1097/SLA.0000000000003506
13. Homel P, Lonner B, Shepp J, Lichtensztejn M, Loewy J. Music therapy increases comfort and reduces pain in patients recovering from spine surgery. Am J Orthoped. 2017;46(1):13–22.
14. Lee JH. The effects of music on pain: a meta-analysis. J Music Ther. 2016;53(4):430–477. doi:10.1093/jmt/thw012
15. Lin CL, Hwang SL, Jiang P, Hsiung NH. Effect of music therapy on pain after orthopedic surgery-a systematic review and meta-analysis. Pain Pract. 2020;20(4):422–436. doi:10.1111/papr.12864
16. Yangoz ST, Ozer Z. The effect of music intervention on patients with cancer-related pain: a systematic review and meta-analysis of randomized controlled trials. J Adv Nurs. 2019;75(12):3362–3373. doi:10.1111/jan.14184
17. Speranza L, Pulcrano S, Perrone-Capano C, Di Porzio U, Volpicelli F. Music affects functional brain connectivity and is effective in the treatment of neurological disorders. Rev Neurosci. 2022;3(7):789–801. doi:10.1515/revneuro-2021-0135
18. Putkinen V, Seppälä K, Harju H, Hirvonen J, Karlsson HK, Nummenmaa L. Pleasurable music activates cerebral µ-opioid receptors: a combined PET-fMRI study. Eur J Nucl Med Mol Imaging. 2025;52(10):3540–3549. doi:10.1007/s00259-025-07232-z
19. Stefano GB, Zhu W, Cadet P, Salamon E, Mantione KJ. Music alters constitutively expressed opiate and cytokine processes in listeners. Med Sci Monit. 2004;10(6):MS18–27.
20. Garza-Villarreal EA, Jiang Z, Vuust P, et al. Music reduces pain and increases resting state fMRI BOLD signal amplitude in the left angular gyrus in fibromyalgia patients. Front Psychol. 2015;6(1051):1051. doi:10.3389/fpsyg.2015.01051
21. Qin J, Chan CW, Dong J, Homma S, Ye S. Telemedicine is associated with reduced socioeconomic disparities in outpatient clinic no-show rates. J Telemed Telecare. 2024;30(9):1507–1515. doi:10.1177/1357633X231154945
22. Uscher-Pines L, Sousa J, Raja P, Mehrotra A, Barnett M, Huskamp HA. Treatment of opioid use disorder during COVID-19: experiences of clinicians transitioning to telemedicine. J Subst Abuse Treat. 2020;118. doi:10.1016/j.jsat.2020.108124
23. El-Tallawy SN, Perglozzi JV, Ahmed RS, et al. Pain management in the post-COVID era-an update: a narrative review. Pain Ther. 2023;12(2):423–448. doi:10.1007/s40122-023-00486-1
24. Ghai B, Malhotra N, Bajwa SJS. Telemedicine for chronic pain management during COVID-19 pandemic. Indian J Anaesth. 2020;64(6):456–462. doi:10.4103/ija.IJA_652_20
25. Areias AC, Costa F, Janela D, et al. Long-term clinical outcomes of a remote digital musculoskeletal program: an ad hoc analysis from a longitudinal study with a non-participant comparison group. Healthcare. 2022;10(12):2349. doi:10.3390/healthcare10122349
26. Gofeld M, Smith KJ, Djuric V, Motlani F, Baldor D. Chronic pain management during the COVID-19 pandemic: can telemedicine replace in-person consultation? A prospective clinical study. Interv Pain Med. 2023;2(2):100252. doi:10.1016/j.inpm.2023.100252
27. Vaudreuil R, Langston DG, Magee WL, Betts D, Kass S, Levy C. Implementing music therapy through telehealth: considerations for military populations. Disabil Rehabil Assist Technol. 2022;17(2):201–210. doi:10.1080/17483107.2020.1775312
28. Cephas AS, Sofield S, Millstein A. Embracing technological possibilities in the telehealth delivery of interactive music therapy. Nord J Music Ther. 2022;31(3):214–227. doi:10.1080/08098131.2022.2040579
29. Howlin C, Rooney B. Cognitive agency in music interventions: increased perceived control of music predicts increased pain tolerance. Eur J Pain. 2021;8(25):1712–1722. doi:10.1002/ejp.1780
30. Low MY, Lacson C, Zhang F, Kesslick A, Bradt J. Vocal music therapy for chronic pain: a mixed methods feasibility study. J Altern Complement Med. 2020;26(2):113–122. doi:10.1089/acm.2019.0249
31. Bradt J, Norris M, Shim M, Gracely EJ, Gerrity P. Vocal music therapy for chronic pain management in inner-city African Americans: a mixed methods feasibility study. J Music Ther. 2016;53(2):178–206. doi:10.1093/jmt/thw004
32. Wilson JM, Colebaugh CA, Flowers KM, Meints SM, Edwards RR, Schreiber KL. Social support and psychological distress among chronic pain patients: the mediating role of mindfulness. Pers Individ Dif. 2022;190(111551):111551. doi:10.1016/j.paid.2022.111551
33. Cano A. Pain catastrophizing and social support in married individuals with chronic pain: the moderating role of pain duration. Pain. 2004;110(3):656–664. doi:10.1016/j.pain.2004.05.004
34. Du S, Hu Y, Bai Y, et al. Emotional distress correlates among patients with chronic nonspecific low back pain: a hierarchical linear regression analysis. Pain Pract. 2019;19(5):510–521. doi:10.1111/papr.12772
35. Nicholas MK, Coulston CM, Asghari A, Malhi GS. Depressive symptoms in patients with chronic pain. Med J Aust. 2009;190(S7):S66–70. doi:10.5694/j.1326-5377.2009.tb02473.x
36. Zheng X, Wang Y, Jin X, et al. Factors influencing depression in community-dwelling elderly patients with osteoarthritis of the knee in China: a cross-sectional study. BMC Geriatr. 2022;22(1):453. doi:10.1186/s12877-022-03117-0
37. Zyrianova Y, Kelly BD, Gallagher C, et al. Depression and anxiety in rheumatoid arthritis: the role of perceived social support. Ir J Med Sci. 2006;175(2):32–36. doi:10.1007/BF03167946
38. Matthias MS, Hirsh AT, Ofner S, Daggy J. Exploring the relationships among social support, patient activation, and pain-related outcomes. Pain Med. 2022;23(4):676–685. doi:10.1093/pm/pnab306
39. Cano A, Leong L, Heller JB, Lutz JR. Perceived entitlement to pain-related support and pain catastrophizing: associations with perceived and observed support. Pain. 2009;147(1–3):249–254. doi:10.1016/j.pain.2009.09.023
40. Baumgartner JN, Haupt MR, Case LK. Chronic pain patients low in social connectedness report higher pain and need deeper pressure for pain relief. Emotion. 2023;23(8):2156–2168. doi:10.1037/emo0001228
41. Story KM, Robb SL, Bravata DM, Damush TM, Bair MJ. Telehealth engaged music for pain outcomes: a music and imagery proof-of-concept study with veterans. J Music Ther. 2024;61(3):288–310. doi:10.1093/jmt/thae011
42. Bonny HL. Music and Consciousness: The Evolution of Guided Imagery and Music. Barcelona Publishers; 2002.
43. Jerling P, Heyns M. Exploring guided imagery and music as a well-being intervention: a systematic literature review. Nord J Music Ther. 2020;29(4):371–390. doi:10.1080/08098131.2020.1737185
44. McKinney CH, Honig TJ. Health outcomes of a series of bonny method of guided imagery and music sessions: a systematic review. J Music Ther. 2017;54(1):1–34. doi:10.1093/jmt/thw016
45. Creswell J. Research Design: Qualitative, Quantitative and Mixed Methods Approaches. Pearson Education Inc; 2015.
46. Vaughn LM, Jacquez F. Participatory research methods – choice points in the research process. J Participatory Res Meth. 2020;1(1). doi:10.35844/001c.13244
47. Kobialka D. Discography Daniel. 2025.
48. HealthMeasures. PROMIS (Patient-Reported Outcomes Measurement Information System). HealthMeasures website. 2023. Available from: https://www.healthmeasures.net/explore-measurement-systems/promis.
49. Howlin C, Rooney B. The cognitive mechanisms in music listening interventions for pain: a scoping review. J Music Ther. 2020;57(2):127–167. doi:10.1093/jmt/thaa003
50. Robinson CL, Phung A, Dominguez M, et al. Pain scales: what are they and what do they mean. Curr Pain Headache Rep. 2024;28(1):11–25. doi:10.1007/s11916-023-01195-2
51. Vetere G, Williams G, Ballard C, et al. The relationship between playing musical instruments and cognitive trajectories: analysis from a UK ageing cohort. Int J Geriatr Psychiatry. 2024;39(2):e6061. doi:10.1002/gps.6061
52. Bullington J. Embodiment and chronic pain: implications for rehabilitation practice. Health Care Anal. 2009;17(2):100–109. doi:10.1007/s10728-008-0109-5
53. Livesey L, Morrison I, Clift S, Camic P. Benefits of choral singing for social and mental wellbeing: qualitative findings from a cross-national survey of choir members. J Public Mental Health. 2012;11(1):10–26. (). doi:10.1108/17465721211207275
54. Scarry E. The Body in Pain: The Making and Unmaking of the World. Oxford University Press; 1985.
55. Laricchiuta D, Garofalo C, Mazzeschi C. Trauma-related disorders and the bodily self: current perspectives and future directions. Front Psychol. 2023;14(1166127):1166127. doi:10.3389/fpsyg.2023.1166127
56. Price CJ, Thompson EA. Measuring dimensions of body connection: body awareness and bodily dissociation. J Altern Complement Med. 2007;13(9):945–953. doi:10.1089/acm.2007.0537
57. International Association for the Study of Pain. More on body awareness and chronic pain. RELIEF News International Association for the Study of Pain. 2021.
58. Dai R, Toiviainen P, Vuust P, Jacobsen T, Brattico E. Beauty is in the brain networks of the beholder: an exploratory functional magnetic resonance imaging study. Psychol Aesthetics Creativity Arts. 2024. doi:10.1037/aca0000681
59. Parma C, Doria F, Zulueta A, et al. An overview of the bodily awareness representation and interoception: insights and progress in the field of neurorehabilitation research. Brain Sci. 2024;14(4):386. doi:10.3390/brainsci14040386
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Music Intervention on Pain, Mood, Sleep, and Heart Rate Variability in Patients with Chronic Pain: A Randomized Controlled Trial
Wang B, Yu F, Ma Y, Zhao H, Wu W, Zheng Y
Journal of Pain Research 2026, 19:584043
Published Date: 23 March 2026