Back to Journals » Journal of Pain Research » Volume 16
Inhibition and Heart Rate Variability in Experimentally Induced Pain
Authors Forte G ![]() , Troisi G
, Troisi G ![]() , Favieri F
, Favieri F ![]() , De Pascalis V, Langher V, Casagrande M
, De Pascalis V, Langher V, Casagrande M
Received 21 April 2023
Accepted for publication 3 August 2023
Published 25 September 2023 Volume 2023:16 Pages 3239—3249
DOI https://doi.org/10.2147/JPR.S418238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Giuseppe Forte,1 Giovanna Troisi,2 Francesca Favieri,1 Vilfredo De Pascalis,2 Viviana Langher,1 Maria Casagrande1
1Department of Dynamic and Clinical Psychology and Health Studies, Sapienza University of Rome, Roma, 00185, Italy; 2Department of Psychology, Sapienza University of Rome, Roma, 00185, Italy
Correspondence: Giuseppe Forte; Maria Casagrande, Department of Dynamic and Clinical Psychology and Health Studies, Sapienza University of Rome, Roma, 00185, Italy, Email [email protected]; [email protected]
Introduction: Pain is a complex experience that requires executive functions (EFs) to be processed. The autonomic outcome of the neural networks involved in the cognitive evaluation of pain is reflected by heart rate variability (HRV), an index of self-regulation abilities. Although some results suggest a relationship between HRV, EFs, and pain, studies focusing on this three-way relationship are still scarce.
Objective: This study aims to investigate the relationship between pain, cognitive, and autonomic mechanisms, hypothesizing an association between resting HRV and both cognitive and motor inhibition as indices of executive functioning. This relationship was investigated after an experimental-induced pain.
Methods: Seventy-six young adults were exposed to the Cold Pressure Arm Warp to induce experimental pain. HRV was collected, and cognitive tasks were administered to assess executive performance.
Results: The results showed that (1) HRV indices significantly increased during pain stimulation, (2) cognitive inhibition was positively correlated with vagal indices and with pain parameters, (3) both inhibition tasks significantly predicted pain threshold while the performance on the Stroop Task predicted pain tolerance.
Conclusion: Results suggest a three-way relationship. Further research would focus on the role of HRV and cognitive strategies in pain management in chronic pain conditions.
Keywords: Stroop task, Go-NoGo, autonomic, pain, heart rate variability, cognition
Introduction
Pain, conceptualized as a homeostatic emotion,1 is a multidimensional experience that induces an adaptive behavioral response to re-establish the homeostatic balance.2,3 Accordingly, the integration of sensorial, physiological, and cognitive processes related to pain involves multiple brain networks.4–6 The overlapping of these neural networks would justify the influencing role of executive functions (EF) in the pain experience.7,8 Specifically, the prefrontal cortex (PFC) plays a relevant role in this interaction. PFC is involved in the modulation of various cognitive processes, including pain experience and EF.9 An increase in dorsolateral PFC activity would be associated with pain inhibitory function and a reduction in reported pain experience.10,11 PFC is also considered to be a key structure for executive control. Accordingly, the functional relationship between pain and EF may stem from shared neural networks within the PFC.11,12 Previous studies have shown that better inhibition is associated with lower sensitivity to pain11 and higher pain tolerance13 within the EF domain. Conversely, poorer control inhibition may be a risk factor for higher vulnerability to pain.14 Moreover, studies reported that chronic pain is associated with impairment in EF (for a meta-analysis, see15; for a review, see14).
Next to the association with pain experience and EF, PFC plays a central role also in the autonomic response. According to the Neurovisceral Integration Model (NIM),16 PFC is a key structure of the Central Autonomic Network (CAN)16–18 related to humans’ ability to evaluate environmental requests and adopt appropriate goal-directed behaviors. NIM suggests the importance of brain-body flexibility, assessed by heart rate variability (HRV), to adapt and respond to the environment physiologically.19–21 In the last two decades, HRV has been widely adopted as a reliable index of the individual’s ability to organize an adaptive and flexible response to environmental challenges, and the HRV indices appear to be related to different cognitive functions.18,22,23 Regarding the experience of pain, NIM suggests that the HRV and the cardiac autonomic reactivity are associated with the functional organization of some pain-related networks.16,21 An adequate reaction to pain involves the autonomic nervous system and triggers the mechanisms needed to re-establish adaptive homeostasis (ie, descending pain modulatory mechanisms24).
Starting from the evidence mentioned above, this study aims to investigate the relationship between EFs (ie, cognitive and motor inhibition), HRV, and pain sensitivity/tolerance, to understand better how cognitive and physiological parameters are related to pain perception.
Despite the theoretical evidence regarding brain–body interactions via the vagal nerve,25 only some studies focused concurrently on the relationship between pain response, central brain responses, and body activation. In this frame, an important question that remains to be investigated is the role of the heart-brain axis in pain and whether this aspect renders some individuals more susceptible to pain. Indeed, a thorough examination of these related aspects (ie, executive functions and autonomic response) in relation to experimental pain experience needs to be investigated.
This study examined the relationship between experimentally induced pain and EFs (ie, motor and cognitive inhibition) in healthy participants. A cold pressor test arm wrap (CPAW) was chosen for experimental pain induction.26 CPAW allows differentiating between three levels of pain experience: threshold, time of exposure, and tolerance. In line with the previous research, we expect an association between inhibition performance and experimental pain.11,27 However, given that EF is still related to autonomic nervous systems,20,21,23 autonomic indices (ie, HRV) and inhibition performance may predict pain tolerance and threshold. In addition, even though the previous studies provided evidence of a pain-inhibition relationship, it remains unclear if all the different components of the inhibitory domain are associated with pain. Accordingly, motor and cognitive inhibition will be tested. A better understanding of these relationships can provide a more holistic picture of the complex physiological and psychological processes implicated in pain.
Methods
Participants
The G-Power analysis (es = 0.20, alpha = 0.05, beta = 0.80; tested for planned analysis) indicated an adequate sample size of at least 75 respondents. Accordingly, seventy-six healthy young adults (47 women, 29 men; mean age = 23.17, SD = 2.34) were recruited. According to the inclusion criteria, only undergraduate students aged between 18 and 35, without any chronic pain condition, cardiovascular diseases, or psychiatric disorders – that could influence our variables of interest – were selected for this study. Inclusion and exclusion criteria were assessed during the sociodemographic and anamnestic interview. The study protocol was approved by the Local Ethical Committee of the University of Rome, “Sapienza” (Department of Dynamic and Clinical Psychology; protocol number: 0001168, 21/08/2019), according to the ethical guidelines of the Declaration of Helsinki. Each participant signed the informed consent before the experimental procedure.
Table 1 shows the main characteristics of the sample.
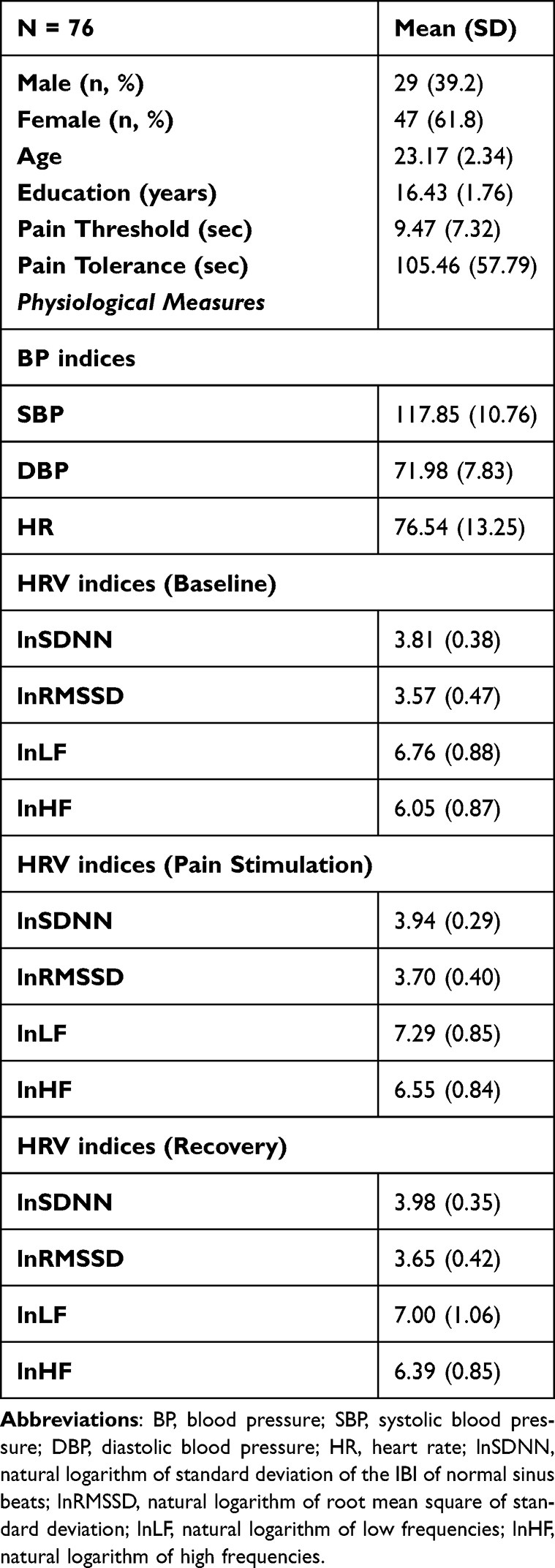 |
Table 1 Principal Demographic Characteristics, Pain, and HRV Variables of the Participants |
Measures
A face-to-face semi-structured interview was adopted to collect sociodemographic and anamnestic data. Moreover, height and weight were recorded for each participant to define body mass index (BMI). Systolic and diastolic blood pressure and heart rate were measured with an electronic device (Omron M3; HEM-7200-E, Omron Healthcare, Kyoto, Japan).
Heart Rate Variability
Heart rate Variability was collected via Firstbeat Bodyguard-2 (Firstbeat Analytics, Jyvaskyla, Finland).28 The signal was processed using Kubios HRV Analysis 3.4.3 software.29 In particular, we evaluated the HRV by considering both frequency and time domains.21 The frequency-domain analysis yielded the mean spectral power measures of the Low-Frequency (LF-HRV, 0.04–0.15 Hz) and High-Frequency (HF-HRV, 0.15–0.4 Hz) bands. The first measure indicates the influence of both vagal and sympathetic activity,30–34 whereas the latter reflects changes in the heart’s vagal control.35 The time-domain analysis yielded the standard deviation of the mean RR interval (SDNN), reflecting the variability in the recording period,23 and the root mean square of successive standard deviation (RMSSD), reflecting the vagal tone.23,34,36 We evaluated HRV during a baseline condition (Resting), task performances requiring cognitive and motor inhibition (Reactivity), and at the end of the procedure (Recovery) for each participant. HRV measures were normalized using natural logarithms.
Pain Sensitivity
The Cold Pressure Arm Wrap (CPAW;26) was adopted to induce experimental cold pain. Two 15 × 30 cm gel packs were applied to the participant’s non-dominant arm at a temperature of 0°C. The experimental procedure provided a maximum duration of stimulation of 180 seconds or immediately when the subject reached the maximum level of pain, as reported by the procedure of previous studies.11 The overall duration of CPAW was included as indices of pain exposure. During pain induction, participants rated pain intensity on a verbal rating scale, with seven levels of pain (in increasing order: “no pain”, “noticeable pain”, “bearable pain”, “moderate pain”, “intense pain”, “heavy pain” and “unbearable pain”). Pain threshold was the time interval (in sec) needed for the subject to experiment “noticeable pain”, pain tolerance was the time interval between “noticeable pain” and “unbearable pain”, and pain exposure was the time interval from “no pain” to “unbearable pain”. All three indices (pain threshold, pain tolerance, and pain exposure) were standardized into z-scores. Finally, to assess subjective pain experience as an index of pain distress, participants were invited to complete a visual analog scale (from 0 = “no pain” to 10 = “the worst possible pain”).
Inhibitory Domain of EF
Inhibition was assessed via a computerized version of the Stroop Task (cognitive inhibition)37 and the Go/NoGo Task (motor inhibition).38
Stroop Task
A computerized version of the Stroop Task37 provided the administration of colored words (Font: Courier New; Font size: 60; colors: yellow, red, blue, green), semantically referring to the colors YELLOW, RED, BLUE, and GREEN. Each word could be presented with the ink color related to its semantic meaning (Congruent Condition, eg, BLUE written in blue ink) or another color (Incongruent Condition, eg, BLUE written in red ink). The task required pressing the key corresponding to the ink color (key “A” = red; Key “S” = green; Key “K” = blue; Key “L” = yellow; each key had a label of the corresponding color) as quickly and accurately as possible. A practice block of 15 trials was presented at the beginning of the task, with feedback about their correct execution. Afterward, a block of 120 randomly presented trials (60 Congruent and 60 Incongruent) was presented. An initial fixation cross (400 ms) was presented before each trial. The target stimulus duration was 3000 ms or until the participant’s response. Reaction times and accuracy were collected. Trials with reaction times over 200 ms and correct trials were considered to calculate each participant’s mean Reaction Times (RTs) for congruent and incongruent conditions, and the Stroop Effect (mean RTs Incongruent Trials − mean RTs Congruent Trials) was computed.
Go/NoGo Task
Two geometric shapes (960 × 720 pixels) individually appeared in the center of the screen with a black background. The Go stimulus was a green circle, and the No-Go stimulus was a green triangle. An initial screen with a fixation cross (duration: 500 ms) was followed by the randomized presentation of target stimuli (Go) and non-target stimuli (No-Go). Each stimulus remained in the center of the screen for 750 ms or until the participant’s response. The task required pressing the left mouse key as quickly as possible when the green circle appeared in the screen center. When the green triangle appeared, the participant had to wait for the disappearance of the stimulus. One hundred trials divided into two blocks of 50 trials each were administered. A practice block of 12 trials, with feedback on correctness, was presented at the beginning of the experiment. The percentage of “no-go” trials was 15 in the overall task. The inappropriate responses to “no-go” stimuli were summed to define the number of False Alarms, considered the inhibition motor component.39
Procedure
Each participant underwent a single experimental session. At the beginning of the session, anamnestic data were collected, and height and weight were assessed. Then, after measuring blood pressure, resting heart rate variability (5 minutes) was recorded (ie, participants were told to relax on a comfortable chair). After resting, participants completed the Stroop Task (five minutes) and the Go/NoGo Task (five minutes). Then, after an intermediate baseline period, participants underwent the CPAW test. Finally, HRV was recorded for 5 minutes (recovery). HRV was recorded for the entire duration of the experimental session. The whole procedure took about 30 minutes.
Data Analyses
Pearson correlations were calculated to assess the association between pain indices (ie, threshold, tolerance, and time exposure), autonomic response (HRV measures), and the performance on the executive tasks (ie, Stroop effect as an index of cognitive inhibition, False Alarm as an index of motor inhibition).
Repeated-measures ANOVAs were performed to understand better the differences in the autonomic measures in the different phases of the experimental procedure of the CPAW (ie, resting, reactivity). Gender was checked as a possible confounding variable. Finally, to assess the possible predictive role of resting autonomic indices and EF domain of inhibition on pain, we performed different hierarchical linear regressions using exposure time, pain threshold, and pain tolerance, respectively, as dependent variables and three different models of prediction: Model 1 including Stroop Effect, Model 2 including both Stroop Effect and False Alarm, Model 3 including the indices of inhibition (Stroop Effect and False Alarm) and autonomic activity during resting phase (lnSDNN, lnRMSSD, lnLF, lnHF). According to the amount of conducted analysis following Bonferroni correction, a value of p < 0.02 was adopted as a significance threshold.
Results
To check for the possible confounding effect of the experimenter’s gender, 2 (participant’s gender) × 2 (experimenter’s gender) ANOVAs were carried out for each pain index. The pain threshold, sensitivity, and exposure time results showed no significant main effects and interaction considering this 2 × 2 ANOVA (all F < 1; all p > 0.40).
Moreover, to check the effective effects of pain in autonomic response, a series of repeated measures ANOVAs to test Resting and Reactivity responses were conducted and showed significant differences in HRV indices: lnSDNN (F2,94= 5.45; p = 0.02; ƞ2p= 0.10), lnRMSSD (F2,94= 7.30; p = 0.009; ƞ2p= 0.13), lnLF (F2,94= 10.04; p = 0.002; ƞ2p= 0.17) and lnHF (F2,94= 6.48; p = 0.01; ƞ2p = 0.012) indices of HRV (see Table 2). Specifically, all the indices were higher in Reactivity than in the Resting condition (see Table 2). No significant effects involving gender were found in the above analyses (all F < 1).
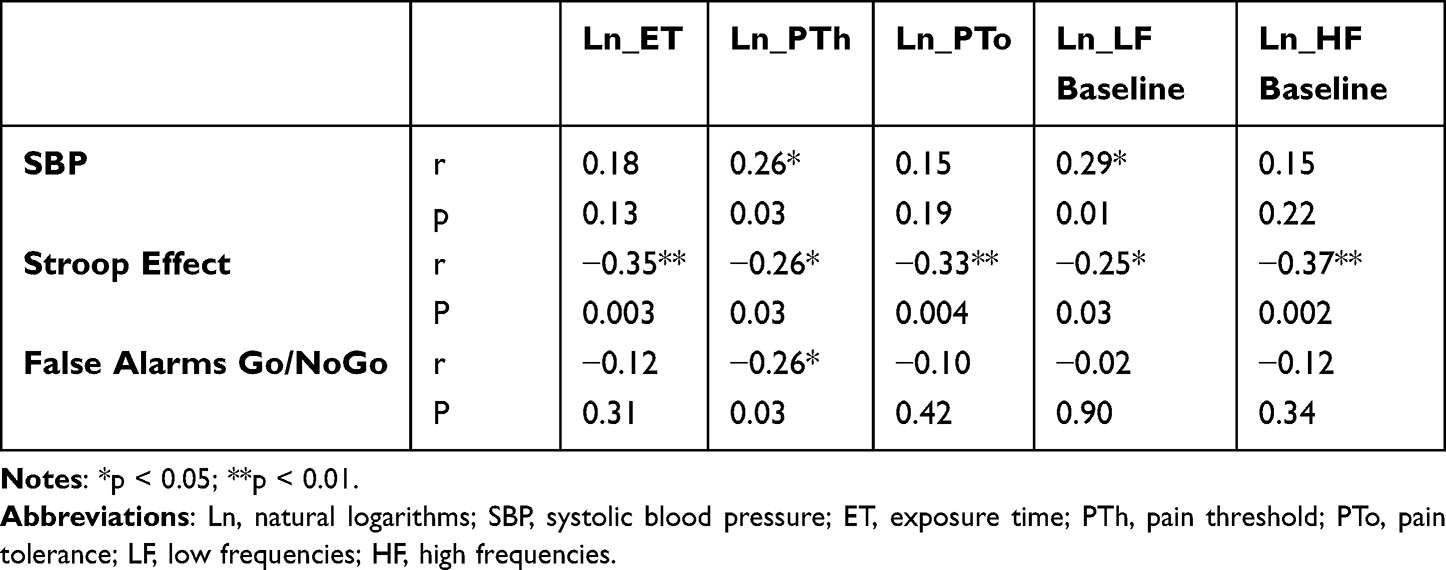 |
Table 2 Linear Correlations Among HRV, Blood Pressure, and Performance on Inhibition Tasks |
Correlation Between Executive Functions and Pain Indices
Pearson correlations reported that the Stroop Effect was significantly and negatively correlated with exposure time (r = −0.35; p = 0.003), pain tolerance (r = −0.33; p = 0.004), and pain threshold (r = −0.26; p = 0.03). Moreover, the false alarms at the Go-NoGo task negatively correlated with the pain threshold (r = −0.26; p = 0.03). These correlations indicate that better executive performance, particularly in inhibition tasks, was related to longer exposure time, higher pain tolerance, and pain threshold. However, assuming that exposure time and pain tolerance indices are influenced by pain threshold, and the correlation between the two indices and inhibition (Stroop Effect and False Alarms to Go/No-Go task) may be affected by this association, we calculated semi-partial correlations between the variables controlling for the effect of pain threshold. The correlation between the Stroop Effect and both exposure time and pain tolerance remained significant (exposure time: r = −0.26; p = 0.02; pain tolerance: r = −0.26; p = 0.02), while no significant association was reported between False Alarms to Go/No-Go and pain indices.
Correlations Between Physiological Measures and Pain Indices
A positive linear correlation was found between SBP and pain threshold (r = 0.27; p = 0.02). No other significant correlations emerged between physiological indices (blood pressure and HRV) and pain indices. Assuming that exposure time and pain tolerance indices are influenced by pain threshold, possibly affecting their association with physiological variables, we calculated semi-partial correlations between the variables controlling for the effect of pain threshold. The correlation between exposure time and pain tolerance and physiological indices reported a significant linear positive correlation between resting ln_LF and both exposure time (r = 0.25; p = 0.03) and pain tolerance (r = 0.25; p = 0.03); no other significant associations emerged between physiological and pain measures.
Correlations Between Physiological Measures and Executive Performance
Considering resting HRV indices, a significant negative correlation was found between Stroop Effect and both lnLF (r = −0.26; p = 0.02) and lnHF (r = −0.35; p = 0.02). Considering reaction times in incongruent trials, a negative linear correlation was found with lnLF (r = 0.29; p = 0.01).
Regression Analyses
Pain Threshold
A hierarchical linear regression model considered pain threshold as the dependent variable and Stroop Effect, False Alarm at Go/No-Go task, and resting HRV indices (lnSDNN, lnRMSSD, lnLF, lnHF) as predictors in three different models (see Table 3). All the models were significant (see Table 3). Model 1 (Stroop Effect) was significant (R2= 0.07; F = 4.95; p = 0.02). Model 2 (Stroop Effect and False Alarm at Go/No-Go task) was significant (R2= 0.13; F = 4.62; p = 0.01). Model 3 (inhibition indices and resting HRV indices) was significant (R2= 0.23; F = 3.03; p = 0.01). The model comparison analysis showed a significant change of R2 between Model 1 and Model 2 (p = 0.04), while no significant change between Model 2 and Model 3 (p = 0.09).
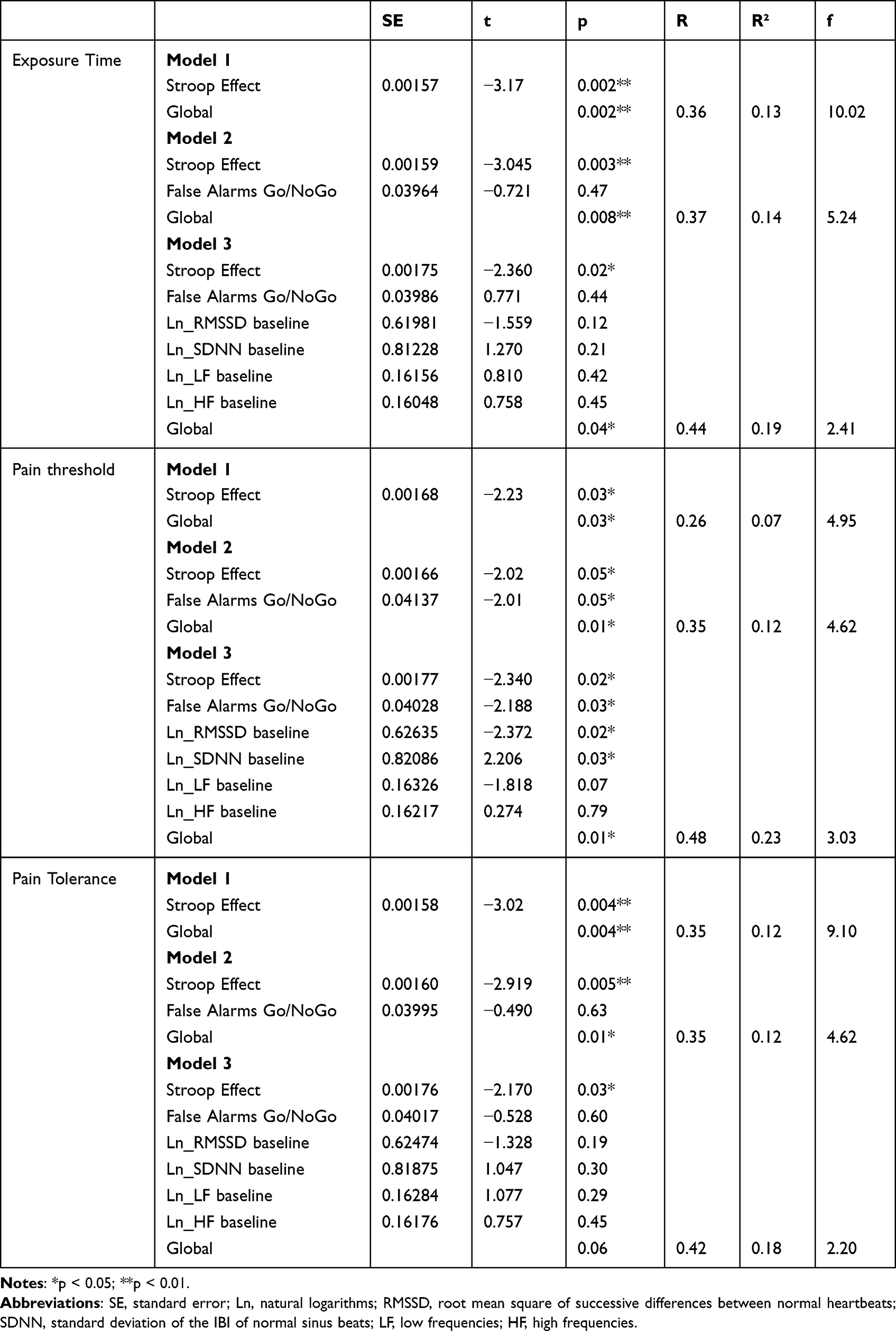 |
Table 3 Results of Regression Analyses |
Exposure Time
The hierarchical linear regression model testing the role of the Stroop Effect, False Alarm at Go/No-Go task, and resting HRV indices (lnSDNN, lnRMSSD, lnLF, lnHF) to Time Exposure reported a unique association with the Stroop Effect (see Table 3).
Pain Tolerance
The hierarchical linear regression model testing the role of the Stroop Effect, False Alarm at Go/No-Go task, and resting HRV indices (lnSDNN, lnRMSSD, lnLF, lnHF) to pain tolerance with the Stroop Effect (see Table 3).
Discussion
This study aimed to identify the association between experimentally induced pain and autonomic response as well as the relationship with EFs, particularly cognitive and motor inhibition.
Our results confirmed previous evidence, indicating an association between pain and cognitive inhibition assessed by the Stroop task.11,27,40,41 The results were confirmed for all the pain measures (ie, exposure time, pain tolerance, and pain threshold). Moreover, an association between pain threshold and false alarm to the Go-NoGo task, which did not emerge in previous studies,27 extended the results found for cognitive inhibition also to motor inhibition. This evidence suggests that different inhibition components may be involved in the capacity to tolerate pain and in determining the threshold of pain perception. Despite the functional similarity, inhibition processes assessed by the two tasks are not the same.42 The performance in the Go/No-Go task would reflect more the response inhibition associated with the activation of the middle and inferior frontal cortices,43 the pre-supplementary areas (pre-SMA), and the anterior cingulate cortex (ACC).44 The Stroop task may additionally measure informational conflict inhibition, which is dissociable from response inhibition.45 Cognitive load associated with the Stroop task performance has been related to the activation in many PFC regions.46,47
Regarding pain-related brain activity, ACC, pre-SMA, and the bilateral anterior insula are significantly activated following the nociceptive stimulation,48 whereas the PFC appears not to be involved in experimental pain perception but in pain control.49 The involvement of these neural networks would explain the results of this study. In fact, good response inhibition may be particularly related to pain threshold, while conflict inhibition may also be involved in pain tolerance and exposure time to experimentally induced pain. In light of previous studies,41,50,51 this evidence suggests that the brain regions engaged in response inhibition may also be involved in behavioral responses to pain perception due to the overlap of the neural circuits.
Interesting insight emerged considering the autonomic response assessed during pain induction as well as the predictive role of resting autonomic state in pain perception. Our results confirmed a significant relationship between the autonomic nervous system activity and pain response (for a review52). In particular, HRV changes were found during pain stimulation than in the resting phase. This pattern would suggest a functional re-organization of the heart-brain axis in response to nociceptive stimulation.53–57 Our findings highlight increased HRV parameters related to baroreflex and parasympathetic activities during painful stimulation. Although most studies reported an increase in sympathetic/baroreflex activity,57–59 few results confirmed the same trend in parasympathetic autonomic branches.60
An increase in baroreflex activity, indexed by LF-HRV, can be considered a general adaptation of the organism to experimentally induced pain.61–63 Individual characteristics, such as interoceptive awareness64 and attentional bias,65 were reported as influencing autonomic response to pain induction. However, despite a theoretical background suggesting the overlapping of the neural networks,16,66–68 no studies focused on the effects of the interaction between executive functioning and autonomic activity in the pain experience.
The hierarchical interactions emerging between executive functions, autonomic and pain processes would be explained by NIM.16 On the one hand, the autonomic response seems uniquely related to the pain threshold. On the other hand, motor inhibition represents a good predictor of the different features involved in pain experience (ie, pain threshold, pain tolerance, and exposure to pain). This pattern would suggest a dominant role of EF rather than autonomic activity in influencing pain.
Although the outcomes of the current study are promising, several limitations can be noted. First, the generalizability of this study, which focused on a sample of young adults, is low, and findings cannot be extended to different age populations. Moreover, it would be interesting to detect the autonomic-cognitive response pattern to pain experience in different populations, such as patients suffering from chronic pain. Nevertheless, this study is the first to investigate the three-way relationship between pain, HRV, and EFs; hence, further research could improve acknowledgment of this field, considering other EFs (ie, attentional control in different conditions69–71) involved in pain processing or other methods to induce acute pain.
Further studies should also consider individual differences (eg, personality traits) that could influence the reported relationship between cognitive-autonomic patterns and pain perception. Another limit could be due to the experimental pain induction. Although largely adopted, the CPAW simulates the experience of cold-related pain. Different reactions based on the origin of the pain stimulus and nociceptive reaction may affect the evidence and activate differently the networks involved. Further studies should consider this aspect and compare different pain induction experimental procedures to the findings of the present study. Finally, self-report scales could represent a limit to the measurement of pain parameters because individual characteristics influence them; further studies should find objective methods to assess pain sensitivity in order to furnish more reliable indices of pain.
Conclusions
Pain is a complex experience that all individuals experience. This study aimed to investigate some aspects of this experience, namely autonomic and cognitive influence on pain. Our results can be read from the perspective of an integrated model postulating an overlap of involved neural networks.
Specifically, summarizing results, we argue that an individual with adequate cognitive and motor inhibition and autonomic reaction to pain is more efficient in triggering mechanisms aimed to re-establish adaptive homeostasis. In these conditions, the individual will experience a more adaptive response to pain via top-down mechanisms. This study is intended to be another small step in understanding pain experiences. This evidence could be useful for understanding the mechanisms involved in pain perception in healthy populations and the field of chronic pain conditions. The three-way relationship highlighted by this study could be a starting point for better pain management in clinical populations resulting in a more satisfactory quality of life.
Acknowledgments
This paper was funded by Sapienza University of Rome (“Progetti di Ricerca Grandi”; protocol number: RG1221816C3B6C27).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Craig A, Tran Y, Siddall P, et al. Developing a model of associations between chronic pain, depressive mood, chronic fatigue, and self-efficacy in people with spinal cord injury. J Pain. 2013;14(9):911–920. doi:10.1016/j.jpain.2013.03.002
2. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
3. Koenig J, Jarczok MN, Ellis RJ, Hillecke TK, Thayer JF. Heart rate variability and experimentally induced pain in healthy adults: a systematic review. Eur J Pain. 2014;18(3):301–314. doi:10.1002/j.1532-2149.2013.00379.x
4. Melzack R. Evolution of the neuromatrix theory of pain. The Prithvi raj lecture: presented at the third world congress of world institute of pain, Barcelona 2004. Pain Pract. 2005;5(2):85–94. doi:10.1111/j.1533-2500.2005.05203.x
5. Oosterman J, Derksen LC, van Wijck AJM, Kessels RPC, Veldhuijzen DS. Executive and attentional functions in chronic pain: does performance decrease with increasing task load? Pain Res Manag. 2012;17(3):159–165. doi:10.1155/2012/962786
6. Farmer MA, Baliki MN, Apkarian AV. A dynamic network perspective of chronic pain. Neurosci Lett. 2012;520(2):197–203. doi:10.1016/j.neulet.2012.05.001
7. Apkarian AV, Bushnell MC, Treede R-D, Zubieta J-K. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–484. doi:10.1016/j.ejpain.2004.11.001
8. Seminowicz DA, Davis KD. A re-examination of pain-cognition interactions: implications for neuroimaging. Pain. 2007;130(1–2):8–13. doi:10.1016/j.pain.2007.03.036
9. Gilbert SJ, Burgess PW. Executive function. Curr Biol. 2008;18(3):R110–4. doi:10.1016/j.cub.2007.12.014
10. Lorenz J, Minoshima S, Casey KL. Keeping pain out of mind: the role of the dorsolateral prefrontal cortex in pain modulation. Brain. 2003;126(Pt 5):1079–1091. doi:10.1093/brain/awg102
11. Oosterman JM, Dijkerman HC, Kessels RPC, Scherder EJA. A unique association between cognitive inhibition and pain sensitivity in healthy participants. Eur J Pain. 2010;14(10):1046–1050. doi:10.1016/j.ejpain.2010.04.004
12. Scherder EJA, Sergeant JA, Swaab DF. Pain processing in dementia and its relation to neuropathology. Lancet Neurol. 2003;2(11):677–686. doi:10.1016/s1474-4422(03)00556-8
13. Karsdorp PA, Geenen R, Vlaeyen JWS. Response inhibition predicts painful task duration and performance in healthy individuals performing a cold pressor task in a motivational context. Eur J Pain. 2014;18(1):92–100. doi:10.1002/j.1532-2149.2013.00348.x
14. Bunk S, Preis L, Zuidema S, Lautenbacher S, Kunz M. Executive functions and pain: a systematic review. Zeitschrift für Neuropsychol. 2019;30:169–196. doi:10.1024/1016-264X/a000264
15. Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Do people with chronic pain have impaired executive function? A meta-analytical review. Clin Psychol Rev. 2014;34(7):563–579. doi:10.1016/j.cpr.2014.08.003
16. Thayer JF, Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. 2000;61(3):201–216. doi:10.1016/s0165-0327(00)00338-4
17. Benarroch EE. Pain-autonomic interactions: a selective review. Clin Auton Res off J Clin Auton Res Soc. 2001;11(6):343–349. doi:10.1007/BF02292765
18. Thayer JF, Ahs F, Fredrikson M, Sollers JJ, Wager TD. A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci Biobehav Rev. 2012;36(2):747–756. doi:10.1016/j.neubiorev.2011.11.009
19. Smith TW, Deits-Lebehn C, Williams PG, Baucom BRW, Uchino BN. Toward a social psychophysiology of vagally mediated heart rate variability: concepts and methods in self-regulation, emotion, and interpersonal processes. Soc Personal Psychol Compass. 2020;14(3):e12516. doi:10.1111/spc3.12516
20. Forte G, Favieri F, Oliha EO, Marotta A, Casagrande M. Anxiety and attentional processes: the role of resting heart rate variability. Brain Sci. 2021;11(4):480. doi:10.3390/brainsci11040480
21. Forte G, Morelli M, Casagrande M. Heart Rate Variability and Decision-Making: autonomic Responses in Making Decisions. Brain Sci. 2021;11(2):243. doi:10.3390/brainsci11020243
22. Appelhans BM, Luecken LJ. Heart rate variability and pain: associations of two interrelated homeostatic processes. Biol Psychol. 2008;77(2):174–182. doi:10.1016/j.biopsycho.2007.10.004
23. Forte G, Favieri F, Casagrande M. Heart Rate Variability and Cognitive Function: a Systematic Review. Front Neurosci. 2019;13:13. doi:10.3389/fnins.2019.00710
24. Hohenschurz-Schmidt DJ, Calcagnini G, Dipasquale O, et al. Linking pain sensation to the autonomic nervous system: the role of the anterior cingulate and periaqueductal gray resting-state networks. Front Neurosci. 2020;14:14. doi:10.3389/fnins.2020.00147
25. Thayer JF, Lane RD. Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev. 2009;33(2):81–88. doi:10.1016/j.neubiorev.2008.08.004
26. Porcelli AJ. An alternative to the traditional cold pressor test: the cold pressor arm wrap. J Vis Exp. 2014;e50849. doi:10.3791/50849
27. Bjekić J, Živanović M, Purić D, Oosterman JM, Filipović SR. Pain and executive functions: a unique relationship between Stroop task and experimentally induced pain. Psychol Res. 2018;82(3):580–589. doi:10.1007/s00426-016-0838-2
28. Palmer AR, Distefano R, Leneman K, Berry D. Reliability of the BodyGuard2 (FirstBeat) in the detection of heart rate variability. Appl Psychophysiol Biofeedback. 2021;46(3):251–258. doi:10.1007/s10484-021-09510-6
29. Tarvainen MP, Niskanen J-P, Lipponen JA, Ranta-Aho PO, Karjalainen PA. Kubios HRV--heart rate variability analysis software. Comput Methods Programs Biomed. 2014;113(1):210–220. doi:10.1016/j.cmpb.2013.07.024
30. Pomeranz B, Macaulay RJ, Caudill MA, et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol. 1985;248(1 Pt 2):H151–3. doi:10.1152/ajpheart.1985.248.1.H151
31. Cossarizza A, Chang H-D, Radbruch A, et al. Guidelines for the use of flow cytometry and cell sorting in immunological studies. Eur J Immunol. 2019;49(10):1457–1973. doi:10.1002/eji.201970107
32. Weise F, Heydenreich F, Runge U. Contributions of sympathetic and vagal mechanisms to the genesis of heart rate fluctuations during orthostatic load: a spectral analysis. J Auton Nerv Syst. 1987;21(2):127–134. doi:10.1016/0165-1838(87)90015-4
33. Saul JP, Rea RF, Eckberg DL, Berger RD, Cohen RJ. Heart rate and muscle sympathetic nerve variability during reflex changes of autonomic activity. Am J Physiol. 1990;258(3 Pt 2):H713–21. doi:10.1152/ajpheart.1990.258.3.H713
34. Laborde S, Mosley E, Thayer JF. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front Psychol. 2017;8:8. doi:10.3389/fpsyg.2017.00213
35. Porges SW. Respiratory Sinus Arrhythmia: physiological Basis, Quantitative Methods, and Clinical Implications. In: Grossman P, Janssen KHL, Vaitl D, editors. Cardiorespiratory and Cardiosomatic Psychophysiology. Springer; 1986:101–115. doi:10.1007/978-1-4757-0360-3_7
36. Shaffer F, McCraty R, Zerr CL. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front Psychol. 2014;5:1040. doi:10.3389/fpsyg.2014.01040
37. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;18(6):643–662. doi:10.1037/h0054651
38. Costantini AF, Hoving KL. The effectiveness of reward and punishment contingencies on response inhibition. J Exp Child Psychol. 1973;16(3):484–494. doi:10.1016/0022-0965(73)90009-X
39. Favieri F, Chen E, Casagrande M. Executive functions and body weight at different ages: a preliminary study. Nutrients. 2021;13(4). doi:10.3390/nu13041174
40. Marouf R, Caron S, Lussier M, Bherer L, Piche M, Rainville P. Reduced pain inhibition is associated with reduced cognitive inhibition in healthy aging. Pain. 2014;155(3):494–502. doi:10.1016/j.pain.2013.11.011
41. Zhou S, Kemp J, Despres O, Pebayle T, Dufour A. The association between inhibition and pain tolerance in the elderly: evidence from event-related potentials. Eur J Pain. 2015;19(5):669–676. doi:10.1002/ejp.588
42. Favieri F, Forte G, Pazzaglia M, Chen EY, Casagrande M. High-level executive functions: a possible role of sex and weight condition in planning and decision-making performances. Brain Sci. 2022;12(2):149. doi:10.3390/brainsci12020149
43. Bokura H, Yamaguchi S, Kobayashi S. Electrophysiological correlates for response inhibition in a Go/NoGo task. Clin Neurophysiol off J Int Fed Clin Neurophysiol. 2001;112(12):2224–2232. doi:10.1016/s1388-2457(01)00691-5
44. Gonzalez-Rosa JJ, Inuggi A, Blasi V, et al. Response competition and response inhibition during different choice-discrimination tasks: evidence from ERP measured inside MRI scanner. Int J Psychophysiol off J Int Organ Psychophysiol. 2013;89(1):37–47. doi:10.1016/j.ijpsycho.2013.04.021
45. Kalanthroff E, Goldfarb L, Henik A. Evidence for interaction between the stop signal and the Stroop task conflict. J Exp Psychol Hum Percept Perform. 2013;39(2):579–592. doi:10.1037/a0027429
46. Langenecker SA, Nielson KA, Rao SM. fMRI of healthy older adults during Stroop interference. Neuroimage. 2004;21(1):192–200. doi:10.1016/j.neuroimage.2003.08.027
47. Zysset S, Schroeter ML, Neumann J, von Cramon DY. Stroop interference, hemodynamic response and aging: an event-related fMRI study. Neurobiol Aging. 2007;28(6):937–946. doi:10.1016/j.neurobiolaging.2006.05.008
48. Qiu J. Infant pain: does it hurt? Nature. 2006;444:143. doi:10.1038/444143a
49. Salomons TV, Johnstone T, Backonja -M-M, Shackman AJ, Davidson RJ. Individual differences in the effects of perceived controllability on pain perception: critical role of the prefrontal cortex. J Cogn Neurosci. 2007;19(6):993–1003. doi:10.1162/jocn.2007.19.6.993
50. Glass JM, Williams DA, Fernandez-Sanchez M-L, et al. Executive function in chronic pain patients and healthy controls: different cortical activation during response inhibition in fibromyalgia. J PAIN. 2011;12(12):1219–1229. doi:10.1016/j.jpain.2011.06.007
51. Schmidt-Wilcke T, Kairys A, Ichesco E, et al. Changes in clinical pain in fibromyalgia patients correlate with changes in brain activation in the cingulate cortex in a response inhibition task. Pain Med. 2014;15(8):1346–1358. doi:10.1111/pme.12460
52. Kyle BN, McNeil DW. Autonomic arousal and experimentally induced pain: a critical review of the literature. Pain Res Manag. 2014;19(3):159–167. doi:10.1155/2014/536859
53. Cooper SJ. from Claude Bernard to Walter Cannon. Emergence of the concept of homeostasis. Appetite. 2008;51(3):419–427. doi:10.1016/j.appet.2008.06.005
54. Leone M, Proietti Cecchini A, Mea E, Tullo V, Curone M, Bussone G. Neuroimaging and pain: a window on the autonomic nervous system. Neurol Sci off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2006;27:S134–7. doi:10.1007/s10072-006-0588-9
55. Jänig W. Relationship between pain and autonomic phenomena in headache and other pain conditions. Cephalalgia. 2003;23(1):43–48. doi:10.1046/j.1468-2982.2003.00573.x
56. Schlereth T, Birklein F. The sympathetic nervous system and pain. Neuromolecular Med. 2008;10(3):141–147. doi:10.1007/s12017-007-8018-6
57. Del paso GAR, Garrido S, Á P, Duschek S. Autonomic cardiovascular control and responses to experimental pain stimulation in fibromyalgia syndrome. J Psychosom Res. 2011;70(2):125–134. doi:10.1016/j.jpsychores.2010.09.012
58. Midenfjord I, Polster A, Sjovall H, Friberg P, Tornblom H, Simren M. Associations among neurophysiology measures in irritable bowel syndrome (IBS) and their relevance for IBS symptoms. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-66558-w
59. Suarez-Roca H, Mamoun N, Sigurdson MI, Maixner W. Baroreceptor modulation of the cardiovascular system, pain, consciousness, and cognition. Compr Physiol. 2021;11(2):1373–1423. doi:10.1002/cphy.c190038
60. Balocchi R, Varanini M, Menicucci D, et al. Heart rate variability in subjects with different hypnotic susceptibility receiving nociceptive stimulation and suggestions of analgesia. In:
61. DEl Paso GA R, Montoro C, Muñóz Ladrón de Guevara C, Duschek S, Jennings JR. The effect of baroreceptor stimulation on pain perception depends on the elicitation of the reflex cardiovascular response: evidence of the interplay between the two branches of the baroreceptor system. Biol Psychol. 2014;101:82–90. doi:10.1016/j.biopsycho.2014.07.004
62. Laborde S, Mosley E, Mertgen A. Vagal tank theory: the three rs of cardiac vagal control functioning – resting, reactivity, and recovery. Front Neurosci. 2018;12:12. doi:10.3389/fnins.2018.00458
63. Forte G, Troisi G, Pazzaglia M, Pascalis V, Casagrande M. Heart rate variability and pain: a systematic review. Brain Sci. 2022;12(2):153. doi:10.3390/brainsci12020153
64. Pollatos O, Füstös J, Critchley HD. On the generalised embodiment of pain: how interoceptive sensitivity modulates cutaneous pain perception. Pain. 2012;153(8):1680–1686. doi:10.1016/j.pain.2012.04.030
65. Terkelsen AJ, Molgaard H, Hansen J, Andersen OK, Jensen TS. Acute pain increases heart rate: differential mechanisms during rest and mental stress. Auton Neurosci. 2005;121(1–2):101–109. doi:10.1016/j.autneu.2005.07.001
66. Benarroch EE. The central autonomic network: functional organization, dysfunction, and perspective. Mayo Clin Proc. 1993;68(10):988–1001. doi:10.1016/s0025-6196(12)62272-1
67. Smith R, Thayer JF, Khalsa SS, Lane RD. The hierarchical basis of neurovisceral integration. Neurosci Biobehav Rev. 2017;75:274–296. doi:10.1016/j.neubiorev.2017.02.003
68. Benarroch EE. Pain-autonomic interactions. Neurol Sci off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2006;27:S130–3. doi:10.1007/s10072-006-0587-x
69. Federico F, Marotta A, Adriani T, Maccari L, Casagrande M. Attention network test — the impact of social information on executive control, alerting and orienting. Acta Psychol. 2013;143(1):65–70. doi:10.1016/j.actpsy.2013.02.006
70. Spagna A, Martella D, Sebastiani M, Maccari L, Marotta A, Casagrande M. Efficiency and interactions of alerting, orienting and executive networks: the impact of imperative stimulus type. Acta Psychol. 2014;148:209–215. doi:10.1016/j.actpsy.2014.02.007
71. Spagna A, Martella D, Fuentes LJ, Marotta A, Casagrande M. Hemispheric modulations of the attentional networks. Brain Cogn. 2016;108:73–80. doi:10.1016/j.bandc.2016.07.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.