Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Inhaled Steroids, Sex and Emphysema Index – Clinical Parameters with Impact on the Effectiveness of Valve Implantation in Patients with Severe Emphysema
Authors Polke M, Brugger J, Rötting M, Polke N, Brock J ![]() , Schuler S, Richter I, Eberhardt R, Herth FJF
, Schuler S, Richter I, Eberhardt R, Herth FJF ![]() , Gompelmann D
, Gompelmann D
Received 10 February 2022
Accepted for publication 19 May 2022
Published 20 June 2022 Volume 2022:17 Pages 1423—1430
DOI https://doi.org/10.2147/COPD.S361256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Markus Polke,1 Jonas Brugger,2 Matthias Rötting,3 Nilab Polke,1 Judith Brock,1 Stefanie Schuler,1 Ines Richter,1 Ralf Eberhardt,1,4,5 Felix JF Herth,1,5 Daniela Gompelmann1,5,6
1Pneumology and Critical Care Medicine, Thoraxklinik at University of Heidelberg, Heidelberg, Germany; 2Institute for Medical Statistics, Center for Medical Statistics, Informatics and Intelligent Systems, Medical University Vienna, Vienna, Austria; 3Medizinische Klinik V, Klinikum Fulda, Fulda, Deutschland; 4Pneumologie & Internistische Intensivmedizin, Asklepios Klinik Barmbek, Hamburg, Deutschland; 5Translational Lung Research Center Heidelberg (TLRCH, German Center for Lung Research (DZL), Heidelberg, Germany; 6Department of Internal Medicine II, Division of Pulmonology, Medical University of Vienna, Vienna, Austria
Correspondence: Markus Polke, Pneumology and Critical Care Medicine, Thoraxklinik at University of Heidelberg, Heidelberg, Germany, Email [email protected]
Aims and Objectives: Many patients with chronic obstructive lung disease suffer from emphysema. Valve implantation may be a reasonable method in patients presenting advanced emphysema and absent interlobar collateral ventilation (CV). However, other clinical parameters influencing the effectiveness of endoscopic lung volume reduction (ELVR) are not well known.
Methods: COPD patients with advanced emphysema who received valve implantation in 2016 were retrospectively analyzed. The following characteristics were collected prior to valve implantation: age, sex, body mass index, presence of allergies, use of inhaled corticosteroids (ICS), lung function parameters, diffusion capacity, 6-minute walk distance (6-MWD), blood gases, COHb, smoking history, and emphysema index (quantitative multi-detector computed tomography). Three months following valve implantation, lung function parameters, diffusion capacity, 6-MWD and blood gases were measured. In this analysis, we evaluated the impact of these variables on an increase in FEV1 and 6-MWT as well as a decrease in RV three months after valve implantation.
Results: Overall, 77 COPD patients (57% male, mean age 66, mean FEV1 32%, mean RV 259%) who underwent valve therapy were enrolled. At 3-month follow-up, patients experienced a mean FEV1 increase of 0.09 ± 0.21 L, a mean RV decrease of 0.42 ± 1.80 L and a mean improvement of 8.3 ± 57 m in the 6-MWT. Overall, ICS, sex and emphysema index had an impact on the outcome following ELVR: ICS medication was associated with inferior FEV1 outcome. The higher the emphysema index, the less the RV reduction. Sex was a predictor for change of FEV1 (%), RV (L), and 6-MWT: male patients seem to benefit less than female patients from valve implantation.
Conclusion: These findings suggest that ICS, emphysema index and sex are clinical parameters that may be associated with inferior outcome following ELVR. Further studies have to confirm these results to improve patient selection and clinical outcome of ELVR.
Keywords: COPD, emphysema, valve implantation, lung volume reduction
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death and expected to become the leading cause of death in the world in around fifteen years.1 Many patients with COPD suffer from emphysema and disease severity depends on its extent.2 The main causes of emphysema are environmental or occupational exposure to substances and alpha-1 anti-trypsin (AAT) deficiency.3 Endoscopic lung volume reduction (ELVR) and lung volume reduction surgery (LVRS) may be beneficial in some of these individuals. In patients with upper lobe-predominant emphysema, lung volume reduction surgery can minimize hyperinflation and thus lead to improvements in lung function, exercise capacity, and quality of life and is associated with survival benefits.4 However, LVRS is associated with a risk of morbidity and mortality. Therefore, an alternative and less invasive method of lung volume reduction was invented: endoscopic lung volume reduction (ELVR). Besides some other interventional methods, endoscopic valve implantation is the best studied technique, resulting in lobar atelectasis of the emphysematous lung lobe and thus in a reduction of symptoms and improvement of long-term outcomes.5–8
Although the valve implantation is a minimally invasive therapy, it can be associated with complications. The most frequent complication in valve implantation is pneumothorax in around a quarter of patients.5,6,8 The prevalence of COPD exacerbations, pneumonia, hemoptysis and death were not significantly higher than in control groups.5,6,8
For successful valve therapy, patient selection is crucial. Besides lung function testing, other assessments such as high resolution computed tomography (HRCT), perfusion scintigraphy, cardiopulmonary exercise testing and echocardiography are recommended for patient selection and predict outcome following valve treatment.7 In particular, the absence of interlobar collateral ventilation (CV) that can be assessed by multi-detector computed tomography (MDCT) scan or invasive Chartis® measurement is an important prerequisite for a successful valve implantation in patients with heterogenous or homogeneous emphysema.5 Furthermore, the lower the lobe attenuation volume (LAV) of the target lobe to LAV of the target lung, the lower the 6-minute walk distance, and the lower the vital capacity (VC), the better the outcome, following valve implantation.9,10 Moreover, the residual volume (RV) seems to be a predictor of the outcome; patients with severe air trapping and thoracic hyperinflation were shown to have a superior response to endoscopic valve therapy.10
These different findings suggest that critical patient selection is crucial for the outcome of intervention. Inclusion criteria and different exclusion criteria such as incomplete fissure or missing target lobe must be taken into account.11 Although certain criteria have been identified, there is still a huge variability in the outcome, but evidence for this is not provided in the literature. The more predictors for a successful endoscopic lung volume reduction with are known, the more precise is the patient selection. Therefore, we looked for further clinical parameters that might predict the effectiveness of valve implantation in severe emphysema.
Methods
The aim of this retrospective analysis was to evaluate clinical parameters as predictors for the outcome following endoscopic valve implantation in patients with severe emphysema. The database was queried for patients with severe emphysema, who were treated with endoscopic valve therapy at Thoraxklinik at the University of Heidelberg. The information entered into the database included baseline characteristics, treatment procedures, outcome and complications. All patients gave written informed consent for the scientific use of their medical records acquired during hospitalization. Data collection was performed with respect to the privacy of the subject, patient data confidentiality and compliance with the Declaration of Helsinki. The local ethics committee of Heidelberg approved the protocol of this trial (S-202/2017).
Subjects, Procedure and Data Collection
Patients who were treated with valve therapy at Thoraxklinik of the University Heidelberg in 2016 were enrolled in this specific analysis. Prior to valve implantation, medical history, physical examination, body plethysmography, measurement of diffusion capacity, 6-MWD, laboratory test, MDCT and perfusion scintigraphy were recorded in a routine clinical care setting.
All patients received a complete occlusion of the target lobe by one-way valves under general anesthesia according to current best practice recommendations.11 Thereby, the target lobe was defined as an emphysematous destroyed lung lobe (assessed by software analysis [YACTA, yet another CT analyzer]) completely separated by interlobar fissures from adjacent lung lobes. In cases where the CT fissure analysis was not sufficient to exclude significant CV, additional Chartis® measurement was performed to quantify the extent of CV. In the absence of CV, the one-way valves were placed.
To assess the clinical outcome following valve therapy, improvements in forced expiratory volume in 1 second (FEV1; L and %), residual volume (RV; L and %) and 6-minute walk distance (6-MWD; m) were assessed from baseline to 3 months following valve implantation.
Evaluation of Efficacy Predictors
The following variables were considered as predictors for the outcome following valve treatment: age, sex, body mass index (BMI), FEV1 (L and %), RV (L and %), transfer factor for carbon monoxide (TLCO SB; %), 6-MWD, eosinophil count, base excess (BE), long-term oxygen therapy (LTOT) (yes/no), domiciliary non-invasive ventilation (NIV; yes/no), smoking history (py), inhaled glucocorticosteroids (ICS; yes/no), oral glucocorticosteroids (yes/no) and emphysema index assessed by YACTA software analysis (%).
Statistical Analysis
For each of the predictive parameters we fitted a linear model with the value of the outcome variable at 3 months after therapy as the dependent variable and its baseline value as well as the respective predictive parameter as the explanatory variables. We fitted these models for each of the 5 outcome parameters (FEV1 [L], FEV1 [%], RV [L], RV [%], 6-MWD [m]). We computed p-values for the predictive parameters in each model. For each outcome variable, we fitted another multivariable linear model with its value at 3 months after therapy as the dependent variable and its baseline value as well as the predictive parameters that had a p-value smaller than 0.1 in their respective baseline model as the explanatory parameters and again computed p-values and estimates. The results of these multivariable linear models are presented in tabular form in the results section. Differences in outcomes between baseline and month 3 were computed with paired t-tests. The significance level for the latter models was set to α = 0.05; however, no correction for multiple testing was applied, therefore all p-values are of descriptive, hypothesis-generating character. Statistical analysis was performed using R, version 3.6.1 or higher.
Results
In this specific analysis, 77 patients (57% male, mean age 66 ± 15 years) who underwent valve therapy due to severe emphysema were enrolled. Prior to valve implantation, the mean FEV1 was 0.86 L ± 0.25 L (32.1% ± 8.6%), and the mean RV was 5.8 L ± 1.32 L (258.6% ± 53.6%). All the patients stopped smoking (47 ± 25 py). The emphysema index assessed by quantitative CT scan was found to be 35.3% ± 9.8%. The patient characteristics prior to valve treatment are summarized in Table 1.
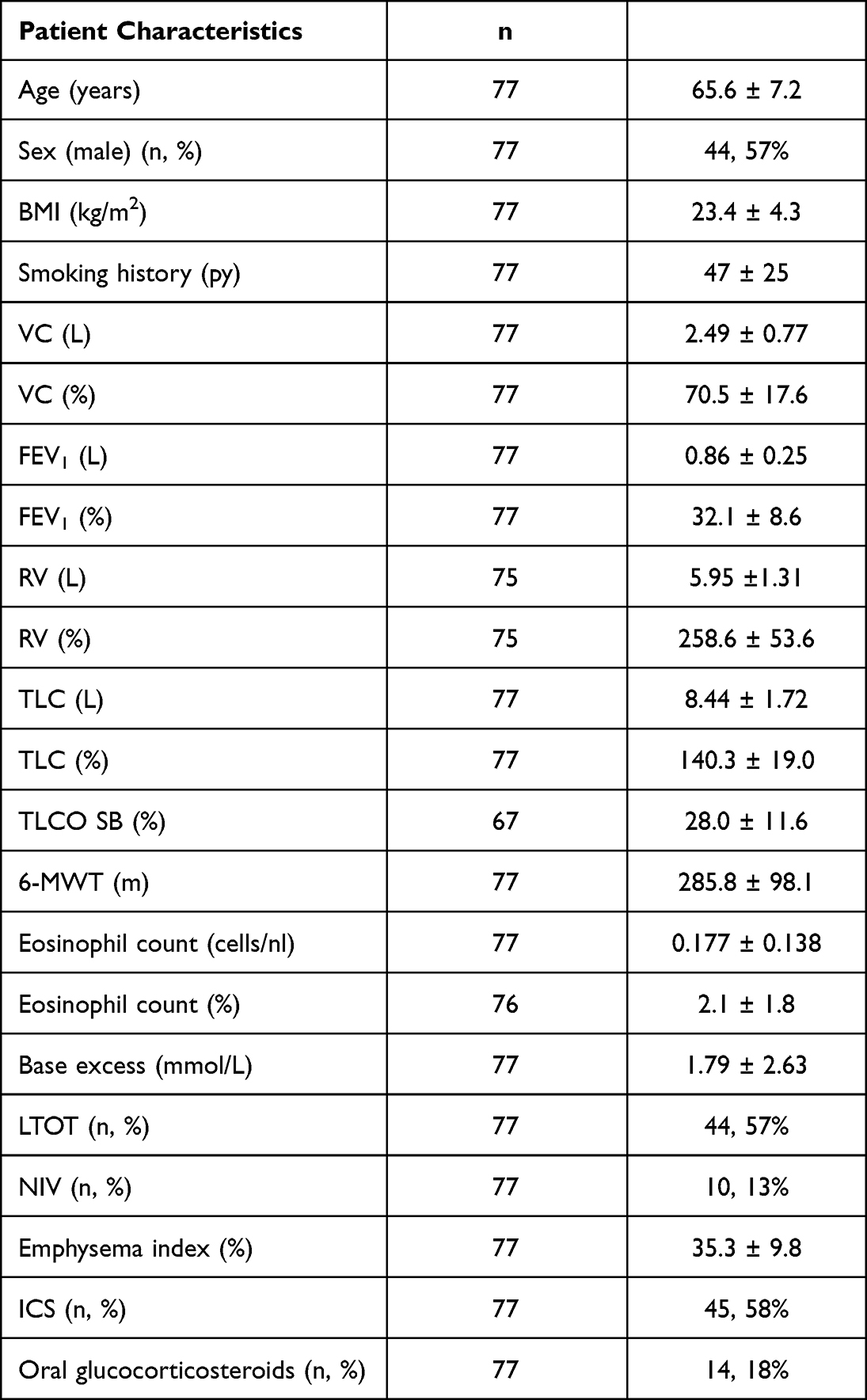 |
Table 1 Patient Characteristics Prior to Valve Implantation |
Twenty-eight patients received one-way valves in the left lower lobe, 23 patients in the left upper lobe, 16 patients in the right lower lobe and 8 patients in the right upper lobe. In one patient, the right upper lobe and middle lobe and in another patient only the middle lobe was occluded by valves.
Clinical Outcome Following Valve Therapy
Three months following valve implantation, patients experienced a mean FEV1 improvement of 0.09 ± 0.21 L (p < 0.001) and 3.8 ± 8.2% (p < 0.001). Moreover, a mean RV reduction of 0.66 ± 1 L (p < 0.001) and 31.7 ± 47.1% (p < 0.001) was detected. The 6-MWT revealed a mean increase of 8 ± 57 m (p = 0.25). Radiological follow-up confirmed a complete lobar atelectasis in 22% of the patients. After valve implantation, 10% of the patients experienced a pneumothorax as anticipated complication.
Predictors for Successful Valve Implantation
Fev1 (L)
In the univariate model, only ICS and BE were associated with a change in FEV1 (L) (p < 0.1) (Table 2). However, only ICS remained significant in the multivariable model (p = 0.026) (Table 3). ICS use was associated with lower FEV1 improvement at 3-months follow-up (−0.12 L compared to non-ICS).
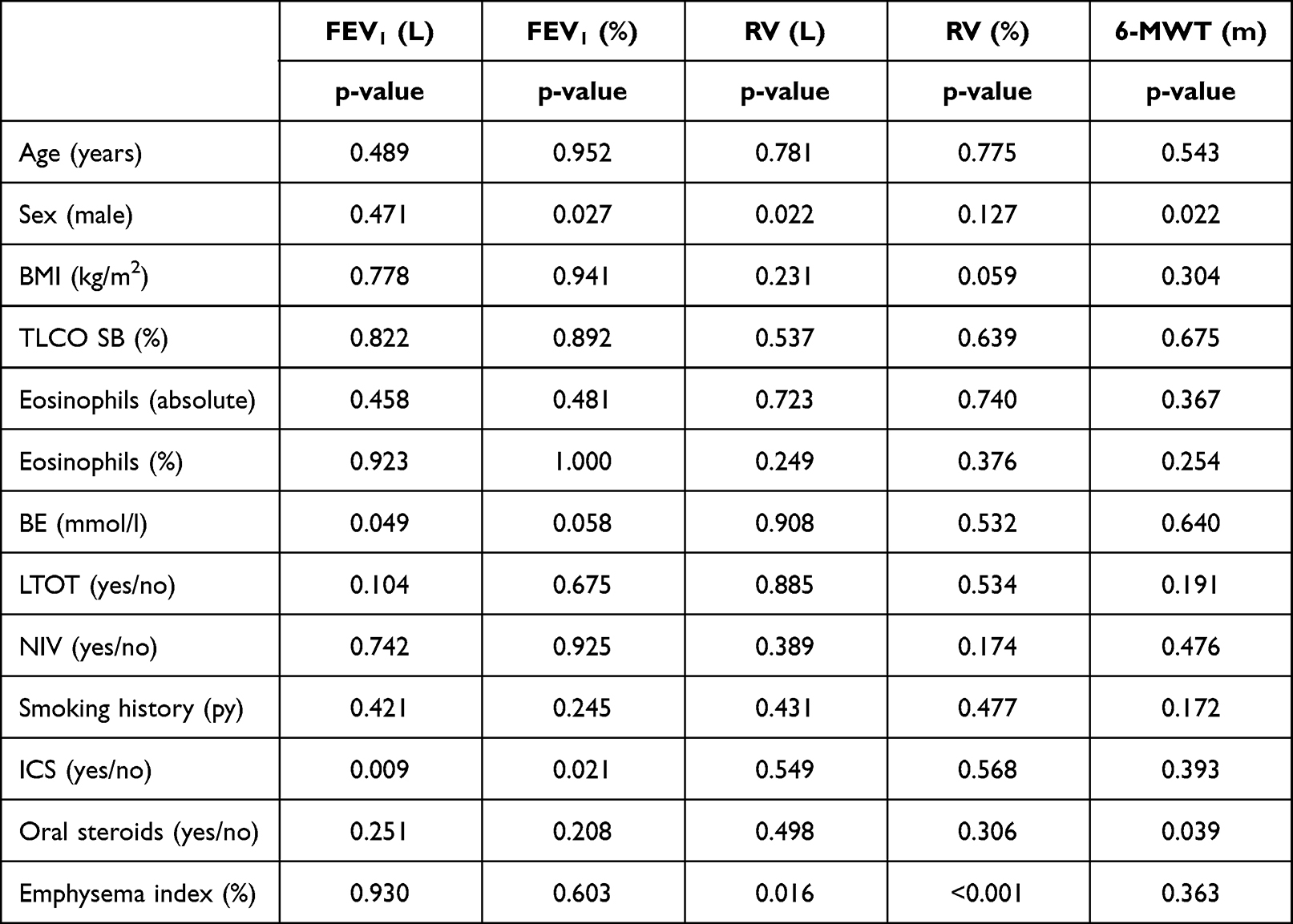 |
Table 2 Results of the Univariate Models for the 5 Outcome Parameters |
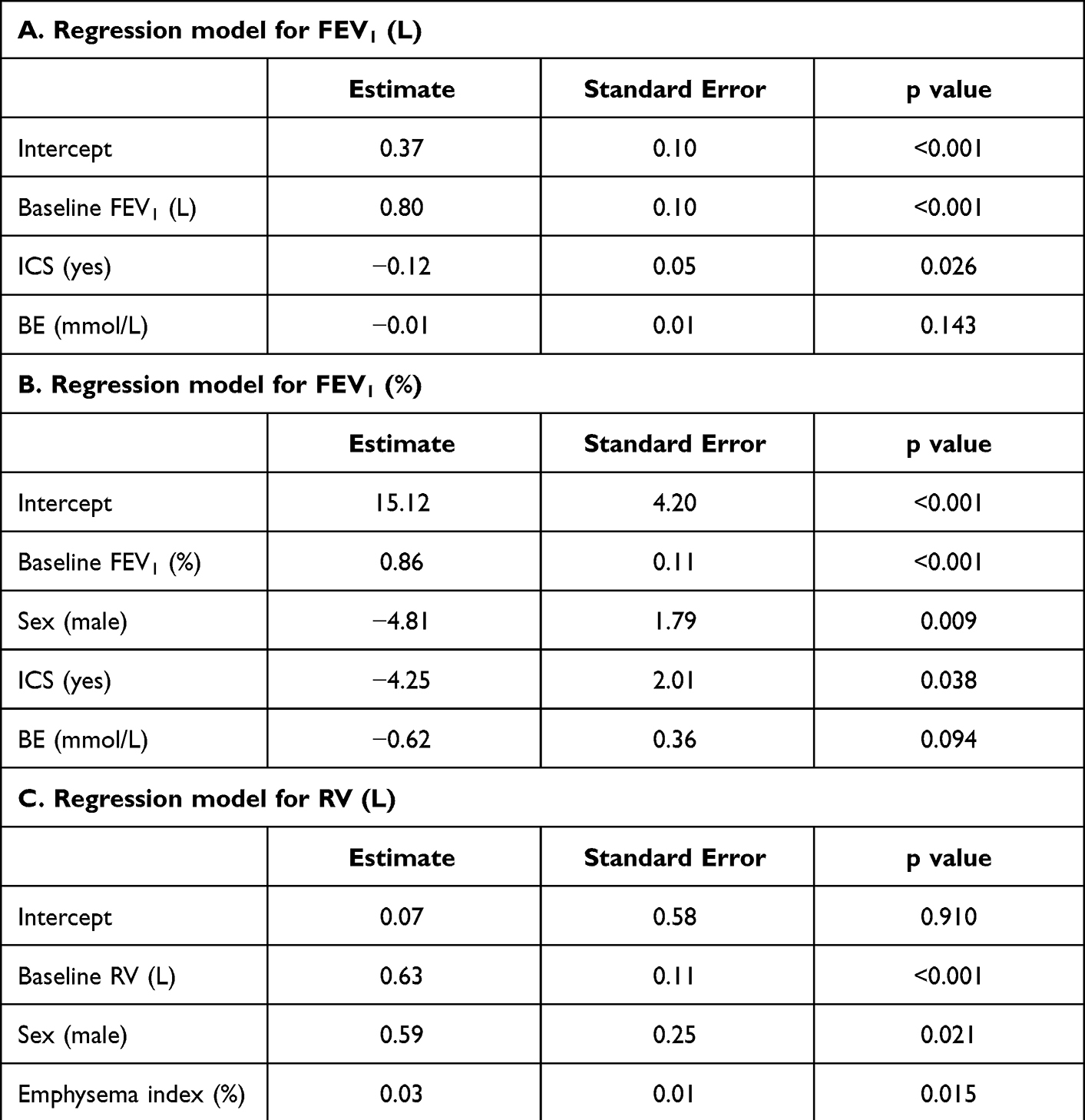 |
Table 3 Multiple Linear Regression Models for Outcome Parameters. Only Parameters That Were Significant in the Univariate Linear Models (P < 0.01) are Mentioned in the Table for Each Outcome Parameter |
Fev1 (%)
In the univariate linear model, sex, ICS and BE were associated with a change in FEV1 (%) (p < 0.1) (Table 2). Sex and ICS remained significant in the multivariable model (p = 0.009 and p = 0.038 respectively) (Table 3). Male patients on average had 4.81% less FEV1 (%) than female patients 3 months after therapy. Patients with ICS on average had 4.25 less FEV1 (%).
RV (L)
Sex and the emphysema index assessed by quantitative CT analysis were associated with RV (L) change in the univariate (p < 0.1) and in the multivariable model (p = 0.021 and p = 0.0125, respectively) (Tables 2 and 3). Male patients on average experienced less RV reduction compared to female patients. Patients with a higher emphysema index had an inferior hyperinflation reduction.
RV (%)
In the univariate linear model, BMI and the emphysema index were associated with RV change (p < 0.1) whereby only the emphysema index remained significant in multivariable model (p = 0.0013, respectively) (Tables 2 and 3). The higher the emphysema index, the less the RV (%) reduction.
6-MWD (m)
In the univariate model, sex and oral glucocorticosteroids were associated with 6-MWD change (p < 0.1) (Table 2). In the multivariable model, sex was still a significant predictor for the outcome (Table 3). Male patients achieved a 26.5 m less 6-MWD than female patients 3 months following valve implantation.
Discussion
Endoscopic valve therapy is an established therapeutic approach in selected patients with advanced emphysema.12,13 Since the first valve implantation in 2003, various trials evaluated the efficacy, and investigated different predictors for outcome and adverse events.5,6,8,14 So far, heterogeneous emphysema distribution, absent interlobar collateral ventilation, low VC and high RV are known as predictors for superior outcome following valve therapy. Despite the consideration of all these predictors, the response to valve therapy remains highly variable. Therefore, the evaluation of further predictors for successful outcome may improve patient selection with the aim of increasing the proportion of patients with an excellent outcome and excluding those patients who do not benefit from this invasive procedure that can be associated with adverse events.
In this analysis, we focused on clinical parameters beyond lung function parameters and radiological parameters and evaluated their impact on the outcome following valve treatment. This analysis reports for the first time that female sex is associated with improved outcome following valve implantation. Women experienced a greater FEV1 improvement, RV reduction and 6-MWD increase. It is known that men and women may respond differently to various therapies, but the results of different trials are controversial.15,16 Moreover, men and women differ in the outcomes of acute COPD exacerbations and hospitalizations, whereby women have a survival advantage, whereas men have an increased risk for in-hospital mortality.15–17 The reasons behind the differences are still unknown and further investigations are needed.
The use of ICS was found to be another predictor for the outcome following valve therapy, whereby patients using ICS had an inferior outcome. A possible explanation for this phenomenon may be the disease severity and COPD exacerbation frequency. An indication for ICS in COPD patients is an increased exacerbation frequency. Presumably, patients who are using ICS may have an advanced stage of the disease, more exacerbations, and thus a poorer prognosis. A specific COPD phenotype may also play a role. Due to the mechanism of action of valve therapy, it may also be possible that particularly patients with severe emphysema but only mild chronic bronchitis, less sputum and a reduced number of exacerbations will experience a superior response to valve therapy.
Emphysema index assessed by MDCT scan was significantly associated with RV reduction, whereby a surprisingly higher emphysema index led to a less RV reduction. This finding was contrary to our expectation as we assumed that the higher the emphysema index, the better the outcome. However, a retrospective study by Theilig et al also revealed that the total lung emphysema score does not predict a beneficial outcome of ELVR.18 In this study, the authors described no association between the total lung emphysema score and ELVR outcome, whereby the authors only focused on FEV1 improvement but not on RV reduction. A possible explanation for the inverse association between the total emphysema index and RV reduction may be the reduced elastic recoil and the severe static hyperinflation of the whole lung that leads to an inferior outcome after occlusion of one of the emphysematous destroyed lung lobes. This hypothesis can be supported by the fact that only the emphysema heterogeneity but not the total lung emphysema score or the emphysema score of the target lobe has an impact on the ELVR outcome.10,18
Summarizing, the results of this study provide evidence that patients with already very advanced disease associated with a high emphysema index and who are already on ICS medication may benefit less from endoscopic valve therapy. Therefore, these parameters should be considered in selecting suitable patients for ELVR, especially borderline cases.
Moreover, important findings in this study were not only the identification of sex, ICS use and emphysema index as predictors for ELVR outcome but also the fact that other clinical parameters like age, BMI, smoking status, the eosinophil count, LTOT or NIV have no impact on the ELVR outcome.
The major limitation of this study is its retrospective design and the small population size. Therefore, further prospective studies are necessary to investigate the impact of the clinical variables on ELVR outcome. Furthermore, it must be emphasized that the patient cohort is a preselected population with advanced emphysema and thus the results may not apply to patients with milder disease.
In conclusion, this study revealed that a high emphysema index, male sex and ICS were associated with less benefit. This result suggests that disease severity has an impact on ELVR outcome. Further studies have to confirm these results to improve patient selection and clinical outcome of ELVR.
Disclosure
Prof. Dr. Ralf Eberhardt reports personal fees from Olympus and Pulmonx, outside the submitted work. Prof. Dr. Daniela Gompelmann reports personal fees from Pulmonx, Olympus, Böhringer Ingelheim, Novartis, Chiesi, Astra Zeneca, Berlin Chemie, and Grifols, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Quaderi SA, Hurst JR. The unmet global burden of COPD. Glob Health Epidemiol Genom. 2018;3:e4. doi:10.1017/gheg.2018.1
2. Shaker SB, Stavngaard T, Hestad M, Bach KS, Tonnesen P, Dirksen A. The extent of emphysema in patients with COPD. Clin Respir J. 2009;3(1):15–21. doi:10.1111/j.1752-699X.2008.00102.x
3. Devasahayam J, LaFreniere K, Naik R. Chronic emphysema. [Updated 2021 Aug 9]. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539910/.
4. Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume- reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348:2059–2073.
5. Klooster K, ten Hacken NH, Hartman JE, Kerstjens HA, van Rikxoort EM, Slebos DJ. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. doi:10.1056/NEJMoa1507807
6. Kemp SV, Slebos DJ, Kirk A, et al. A multicenter randomized controlled trial of Zephyr endobronchial valve treatment in heterogeneous emphysema (TRANSFORM). Am J Respir Crit Care Med. 2017;196:1535–1543. doi:10.1164/rccm.201707-1327OC
7. Herth FJF, Slebos DJ, Criner GJ, Valipour A, Sciurba F, Shah PL. Endoscopic lung volume reduction: an expert panel recommendation - update 2019. Respiration. 2019;97(6):548–557. doi:10.1159/000496122
8. Valipour A, Slebos DJ, Herth F, et al.; IMPACT Study Team. Endobronchial valve therapy in patients with homogeneous emphysema. Results from the IMPACT Study . Am J Respir Crit Care Med. 2016;194(9):1073–1082. doi:10.1164/rccm.201607-1383OC
9. Eberhardt R, Gompelmann D, Herth FJ, Schuhmann M. Endoscopic bronchial valve treatment: patient selection and special considerations. Int J Chron Obstruct Pulmon Dis. 2015;10:2147–2157. doi:10.2147/COPD.S63473
10. Gompelmann D, Hofbauer T, Gerovasili V, et al. Predictors of clinical outcome in emphysema patients with atelectasis following endoscopic valve therapy: a retrospective study. Respirology. 2016;21(7):1255–1261.
11. Polke M, Rötting M, Sarmand N, et al. Interventional therapy in patients with severe emphysema: evaluation of contraindications and their incidence. Ther Adv Respir Dis. 2019;13:1753466619835494. doi:10.1177/1753466619835494
12. Slebos DJ, Shah PL, Herth FJ, Valipour A. Endobronchial valves for endoscopic lung volume reduction: best practice recommendations from expert panel on endoscopic lung volume reduction. Respiration. 2017;93(2):138–150. doi:10.1159/000453588
13. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD; 2022.
14. Toma TP, Hopkinson NS, Hillier J, et al. Bronchoscopic volume reduction with valve implants in patients with severe emphysema. Lancet. 2003;361(9361):931–933. doi:10.1016/S0140-6736(03)12762-6
15. Aryal S, Diaz-Guzman E, Mannino DM. Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. Int J Chron Obstruct Pulmon Dis. 2014;14(9):1145–1154.
16. Cydulka RK, Rowe BH, Clark S, Emerman CL, Rimm AR, Camargo CA. Gender differences in emergency department patients with chronic obstructive pulmonary disease exacerbations. Acad Emerg Med. 2005;12(12):1173–1179. doi:10.1197/j.aem.2005.06.025
17. Patil SP, Krishnan JA, Lechtzin MD, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Intern Med. 2003;163(10):1180–1186. doi:10.1001/archinte.163.10.1180
18. Theilig DC, Huebner RH, Neumann K, Poellinger A, Doellinger F. Selecting patients for lobar lung volume reduction therapy: what quantitative computed tomography parameters matter? Rofo. 2019;191(1):40–47. doi:10.1055/a-0638-0058
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.