Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Inhaled Corticosteroid Therapy in Bronchiectasis is Associated with All-Cause Mortality: A Prospective Cohort Study
Authors Håkansson KEJ ![]() , Fjaellegaard K, Browatzki A, Dönmez Sin M, Ulrik CS
, Fjaellegaard K, Browatzki A, Dönmez Sin M, Ulrik CS ![]()
Received 18 March 2021
Accepted for publication 1 June 2021
Published 16 July 2021 Volume 2021:16 Pages 2119—2127
DOI https://doi.org/10.2147/COPD.S311236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Kjell EJ Håkansson,1 Katrine Fjaellegaard,2,3 Andrea Browatzki,4 Melda Dönmez Sin,1 Charlotte Suppli Ulrik1,5
1Department of Respiratory Medicine, Copenhagen University Hospital - Hvidovre, Hvidovre, Denmark; 2Department of Respiratory Medicine, Zealand University Hospital Næstved, Næstved, Denmark; 3Institute of Regional Health Research, University Southern Denmark, Odense, Denmark; 4Department of Respiratory Medicine, North Zealand Hospital, Hillerød, Denmark; 5Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Kjell EJ Håkansson
Respiratory Research Unit 237, Copenhagen University Hospital - Hvidovre, Kettegård Allé 30, 2650, Hvidovre, Denmark
Email [email protected]
Background and Objective: Prescribing inhaled corticosteroids (ICS) for bronchiectasis (BE) in the absence of obstructive lung disease is controversial. Studies investigating ICS therapy and impact on morbidity and mortality in BE are sparse.
Methods: This study comprises all patients with BE managed at respiratory outpatient clinics at two university hospitals in the Capital Region of Denmark 2014– 2015. Baseline data were obtained from patient medical records, and patients were followed until April 2020.
Results: Out of 264 patients, 122 (46%) were prescribed ICS with no demographic differences between users/non-users of ICS. Among patients prescribed ICS, 21% did not have a concomitant diagnosis of asthma or COPD. Patients prescribed ICS had lower lung function (median FEV1 65.2 vs 80.9%pred, p< 0.001) and a higher symptom burden in terms of cough (p 0.028), sputum production (p < 0.001) and dyspnea (p < 0.001). Pseudomonas-positive sputum cultures were more common in ICS-treated patients (6.5 vs 20%, p 0.010), as were previous severe exacerbations (41% vs 21%, p < 0.001). In terms of mortality, high-dose ICS use was associated with increased mortality in multivariable Cox regression adjusted for age, sex, FEV1 and concomitant asthma/COPD (HR 4.93 [95% CI 1.73– 14.0], p 0.003).
Conclusion: In this cohort, close to one out of five patients with BE were prescribed ICS despite having no concomitant diagnosis of asthma or COPD. Overall, ICS treatment was associated with higher morbidity and mortality, though causation is difficult to establish.
Keywords: follow-up cohort, descriptive study, all-cause mortality, ICS, non-cystic fibrosis bronchiectasis
Introduction
Patients with non-cystic fibrosis bronchiectasis (BE) experience severely reduced quality of life (QoL) as well as increased morbidity and mortality.1,2 Non-cystic fibrosis BE is radiologically defined as permanent, pathological enlargement of airways, often as a result of intrinsic airway pathology.3 A vicious vortex of chronic bronchial inflammation, reduced mucociliary clearance and structural lung damage has been proposed as the driving pathological mechanism in BE.4 While long-term antibiotics have shown promise in some patients,5 the role of anti-inflammatory drugs as a treatment in BE is still unclear.
Due to the suspected involvement of bronchial inflammation, the use of anti-inflammatory drugs has been proposed as a treatment for reducing symptoms and exacerbation frequency.6 Corticosteroids, statins and macrolides have all been suggested as feasible agents.7–9 So far, only long-term macrolide treatment has shown effectiveness in reducing exacerbation burden in certain groups of BE patients, though novel therapies, such as the dipeptidyl peptidase 1-inhibitor brensocatib, have shown promising results.7,10
Inhaled corticosteroids (ICS) are the anti-inflammatory cornerstone of asthma therapy, and an add-on treatment for COPD patients with evidence of eosinophilic inflammation.11,12 According to the 2018 Cochrane review of ICS treatment for BE, results from most randomized, placebo-controlled trials have been disappointing in terms of effects on most endpoints such as pulmonary function and exacerbation frequency.13 As such, the ERS Guidelines for Management of Bronchiectasis advice against prescribing ICS to patients with BE, unless otherwise indicated by either an asthma or COPD diagnosis.3 Additionally, ICS treatment in asthma and COPD is associated with common side effects such as oral candidiasis, dysphonia and, in some cases, systemic corticosteroid effects.14 However, the rate of adverse events from ICS treatment of BE is largely unknown.3
In the present study, using a 5-year prospective cohort based on two university hospital respiratory outpatient clinics, we aimed to assess the change in prevalence of ICS treatment in patients with HRCT-verified BE over time and the association between ICS treatment and all-cause mortality. Furthermore, we aimed to assess treatment regimens, exacerbation burden and the prevalence of Pseudomonas aeruginosa in sputum samples.
Methods
Study Design
The present study is a descriptive prospective cohort follow-up study, designed to reflect real-world management of BE. The study was carried out at the respiratory outpatient clinics of Copenhagen University Hospital-Hvidovre, Hvidovre and North Zealand Hospital, Hillerød, Denmark.
All patients with 1) a current diagnosis of bronchiectasis (ICD-10: DJ-479) and 2) an active outpatient status between January 1, 2014 and April 30, 2015 were enrolled in the cohort. Patients were followed in electronic patient journals (EPJ) and national databases until end of April 2020. Exclusion criteria were 1) No high-resolution computer tomography (HRCT)-verified BE diagnosis and 2) patients actively declining quality control or researcher access as noted in their patient journals.
Ethics
This study and study-related access to patient journals without written consent from patients not actively opting out of researcher access was approved by the Capital Region of Copenhagen’s Ethics Committee (ref. H-1500-43-40). Data handling was approved by the Danish Data Protection Agency (ref. 2016-41-4913). The study was conducted in accordance with the Declaration of Helsinki.
Data Collection
All patient data, including concomitant diagnoses, hospital admissions, radiological findings and laboratory data were collected from the EPJ systems OPUS Arbejdsplads (CSC A/S, Denmark) at enrolment and from Sundhedsplatformen (Epic Systems Inc., USA) at follow-up. Prescription data were collected from the national Common Prescription Card (MedCom A/S, Denmark) and vital status was collected from the Danish Civil Registration System.15 Prescription data, laboratory data and microbiology data were available also for patients returned to primary care due to shared data platforms in Denmark.
Definitions
The following definitions were used during data collection:
- Asthma – Objectively confirmed diagnosis, ie, positive reversibility or positive bronchial provocation tests.
- COPD – Objectively conformed diagnosis by post-bronchodilator FEV1/FVC ratio <0.7, relevant exposure and specialist assessment.
- Pack-year – 20 cigarettes smoked daily for 1 year.
- Exacerbation – From the criteria described by Hill et al.16 Based on prescription data with the indications “for infection”, “for pneumonia”, “for acute exacerbation”.
- Moderate exacerbation – An exacerbation requiring a prescription of antibiotics or leading to hospital admission for less than 24 hours.
- Severe exacerbation – An exacerbation requiring more than 24 hours of hospital admission. Aetiologies
- Allergic bronchopulmonary aspergillosis (ABPA) – fulfilling the ABPA-Bronchiectasis-criteria as described by Agarwal et al.17
- Connective tissue disease – An active ICD-10 code of Inflammatory Polyarthropathies (M05-M14), Systemic Connective Tissue Disorders (M30-36), Inflammatory Spondylopathies (M45-46), Myositis (M60), Sarcoidosis (D86).
- Inflammatory bowel disease – An active ICD-10 code of K50-52.
- Immunosuppression – either idiopathic (Immunoglobulin A, G or M below lower limit of normal (LLN); mannose-binding lectin below LLN) or pharmacologic (Active treatment with immunosuppressant, eg, ciclosporin or known active haematological disorder, eg, chronic lymphocytic leukaemia)
- Severe childhood pulmonary disease – Anamnestic history of repeated pulmonary infections and/or hospitalization due to pulmonary disease during childhood.
- Idiopathic – Defined as the absence of any aetiologies described above.
- Rescue course of systemic corticosteroid – Prescription of at least 25 mg for prednisolone for 3 days or more.
- BE severity – Disease severity was evaluated using Bronchiectasis Severity Index (BSI) score.18
- Prescribed dose of ICS – Dose equivalents as described in the Global Initiative for Asthma 2020 guidelines.11
Outcomes
The primary outcomes were
- Change in prevalence of ICS treatment from baseline to end of follow-up.
- Association between ICS use and all-cause mortality
Secondary outcomes were
- Change in treatment regimens from baseline to end of follow-up
- Change in annual exacerbation rate from baseline to end of follow-up
- Prevalence of Pseudomonas aeruginosa in collected sputum samples during the study period.
Statistics
Continuous variables are presented as median and interquartile range (IQR). Categorical variables are presented as number (n) and percentages (%). Differences across groups were investigated using Wilcoxon rank-sum test or chi-square test of independence depending on continuous or categorical variable nature.
Bivariable and multivariable adjusted Cox regression analyses were used to estimate the association between mortality and ICS treatment when adjusted for other known risk factors. Results are presented as hazard ratios (HRs) with 95% confidence intervals (CI). Adjusted models include the following variables: age, gender, smoking status, forced expiratory volume in 1 second (FEV1) at baseline and co-existing asthma and/or COPD.
R 4.0.2 (R Foundation for Statistical Computing, Austria) was used for statistical analysis. A P-value ≤0.05 was defined as statistically significant.
Data Sharing and Availability
Data is available upon reasonable request but may require prior approval by the Danish Patient Safety Authority and the Regional Data Protection Committee of the Greater Capital Region as per Danish law.
Results
A total of 264 patients were included from the two respiratory outpatient clinics, out of 285 screened. Of the screened patients, 21 were excluded due to missing HRCT-verification of BE. In the final cohort, 165 (62%) were female, the median age was 66 (IQR 51–72) and 22 (8.8%) and 117 (47%) were current and ex-smokers, respectively, with a median pack-year history of 15.0 (IQR 2–30) (Table 1).
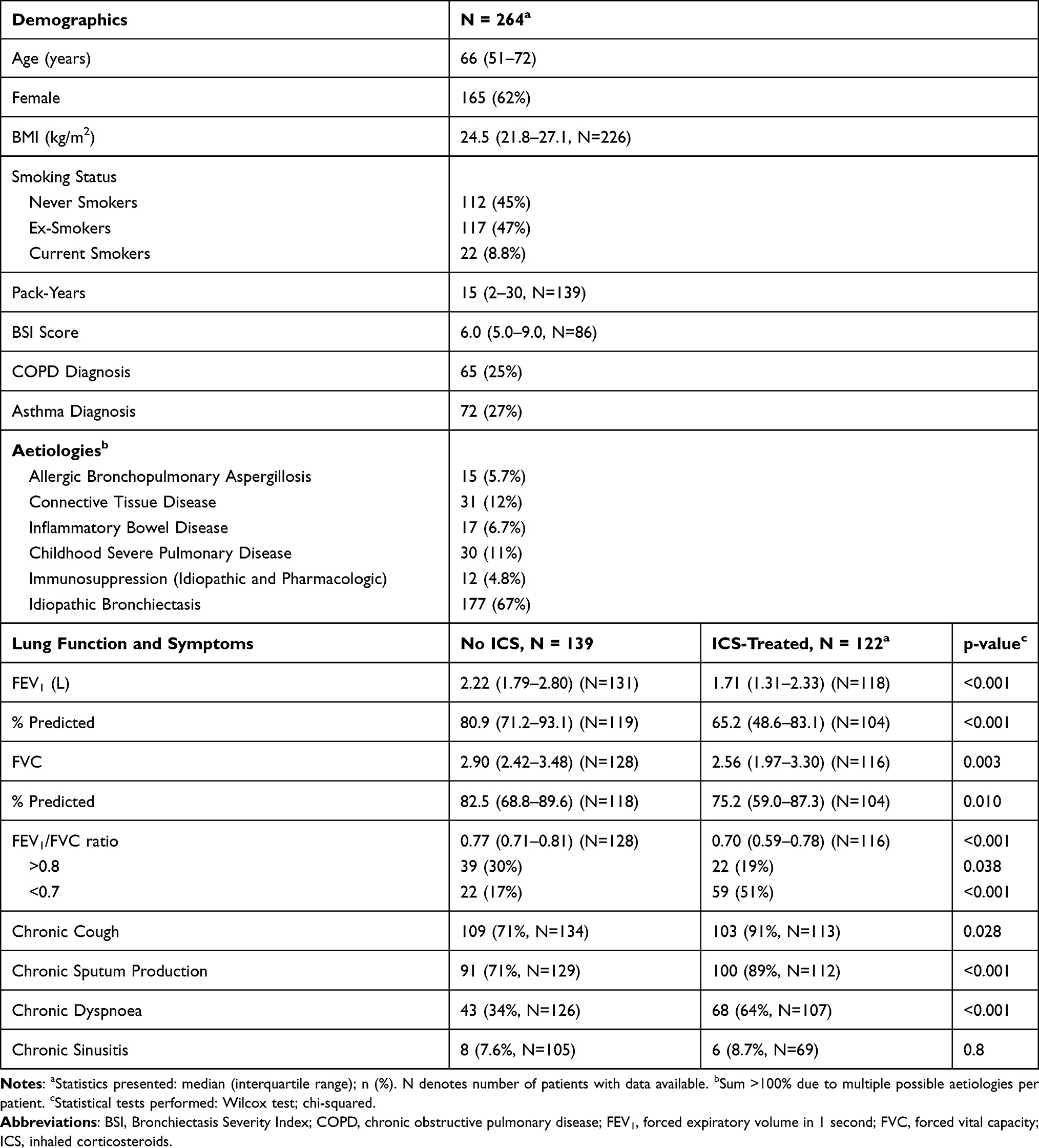 |
Table 1 Demographics, Lung Function and Symptoms of 264 Respiratory Outpatients with Bronchiectasis Followed for 5 Years at Two University Hospitals |
Regarding severity of BE, the median BSI score was 6.0 (IQR 5.0–9.0). However, BSI score was only available for roughly one-third of patients, primarily due to missing Medical Research Council scores in non-COPD patients. Twenty-seven percent and 25% had a verified asthma and/or COPD diagnosis, leaving 142 patients (54%) without known respiratory disease besides BE (Table 1).
Aetiology, Symptoms and Pulmonary Function
The most common aetiology seen was idiopathic BE (67%), followed by connective tissue diseases and a history of severe childhood respiratory disease (12% and 11%, respectively) (Table 1).
In terms of symptoms, chronic cough and sputum was reported by over 80% of the patients. When stratified by ICS treatment, chronic cough, sputum production and dyspnoea were more prevalent in the ICS-treated group (p=0.028, p <0.001 and p <0.001 respectively) (Table 1).
When stratified by ICS treatment, patients currently prescribed ICS treatment at enrolment had a considerable and significantly lower FEV1 (65.2%pred (IQR 48.6–83.1) versus 80.9%pred (IQR 71.2–93.1), p <0.001) causing a significantly lower FEV1/FVC (p <0.001) despite also having a significantly lower FVC (p=0.003) (Table 1). Excluding patients with COPD, FEV1 was lower in patients receiving ICS (77%pred (IQR 59–94) versus 83%pred (72–94), p 0.040. FEV1/FVC was lower in patients receiving ICS without concomitant COPD, when compared to patients without concomitant COPD not receiving ICS at 0.73 (0.69–0.80) versus 0.77 (0.73–0.82), p 0.004. No difference in FVC was found (data not shown).
Treatment of Bronchiectasis
In the cohort, 122 (46%) of patients were treated with ICS at enrolment. Three patients were excluded from ICS-related analyses due to missing data. Out of the patients prescribed ICS, 23 (21%) did not have concomitant asthma or COPD and among these, 35% were prescribed high-dose ICS (Table 2).
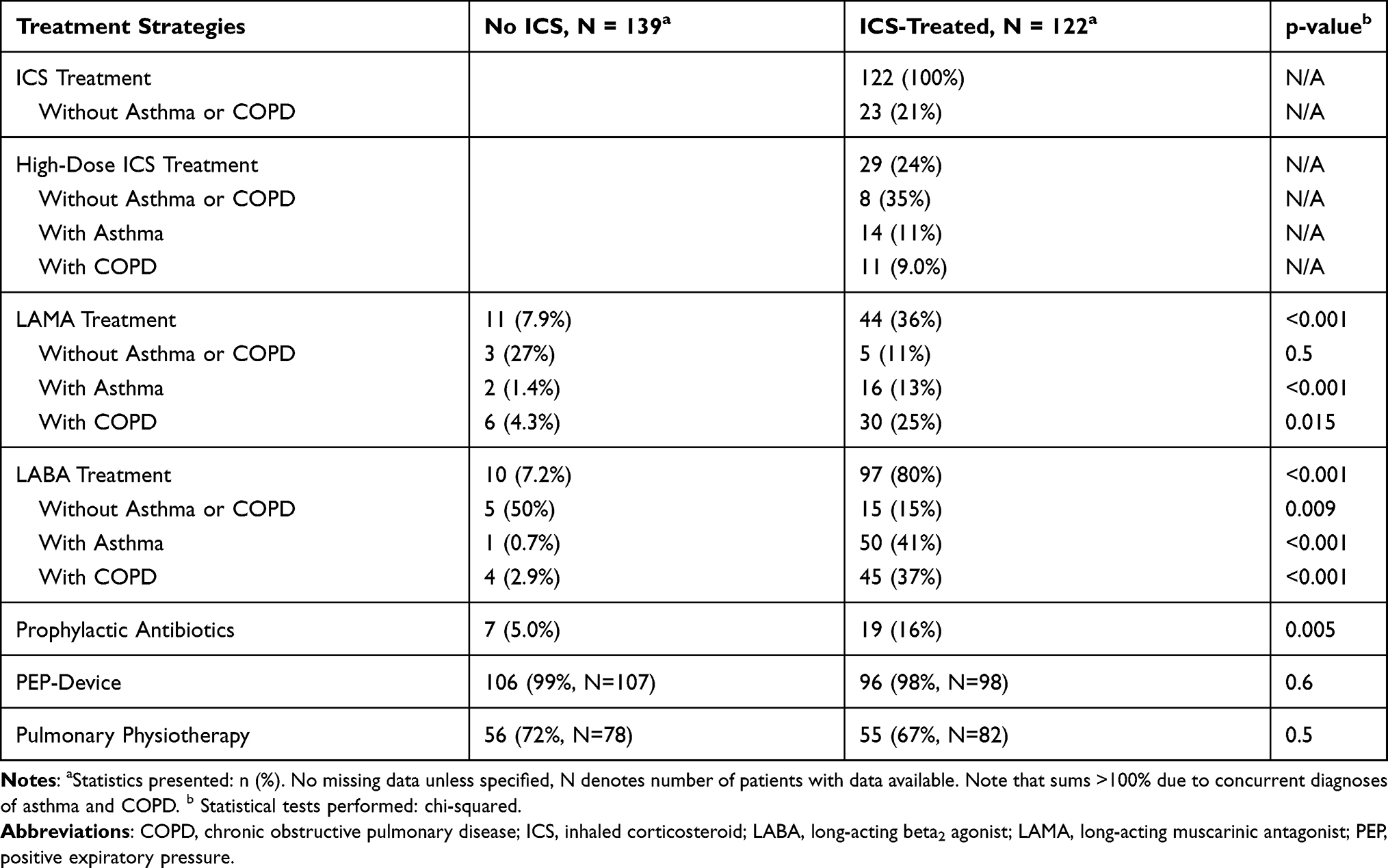 |
Table 2 Pharmacological and Non-Pharmacological Treatment Strategies in 264 Respiratory Outpatients with Bronchiectasis Followed for 5 Years at Two University Hospitals, Stratified by Treatment with Inhaled Corticosteroids |
Bronchodilators were rarely prescribed to patients without concurrent obstructive lung disease and ICS treatment, as only five and three patients, respectively, not on ICS at baseline were prescribed a long-acting beta2 agonist (LABA) or a long-acting muscarinic antagonist (LAMA), respectively (Table 2). However, 15 (11%) of patients without asthma and/or COPD were prescribed a LABA and ICS combination at baseline (data not shown).
Prophylactic antibiotics, irrespective of formulation and mode of delivery, were prescribed to 16% of patients receiving ICS compared to 5.0% among those not prescribed ICS (p 0.005) (Table 2).
Non-pharmacologic therapies such as positive expiratory pressure (PEP)-devices and pulmonary physiotherapy were offered to approximately 100% and 70%, respectively, of patients, with no significant difference between groups (Table 2).
Pseudomonas
Of all patients, 68 (26%) had positive sputum cultures during the study period, with positive cultures being slightly more common in patients receiving ICS (32% versus 21%, p 0.041). Pseudomonas aeruginosa-positive cultures were predominately seen in patients receiving ICS (20% versus 6.5%, p=0.001) (Table 3). When stratifying patients by FEV1 above or below 50%, Pseudomonas-positive sputum cultures were seen in 39% of the patients with an FEV1 below 50% and 9.3% above 50% (p<0.001, data not shown).
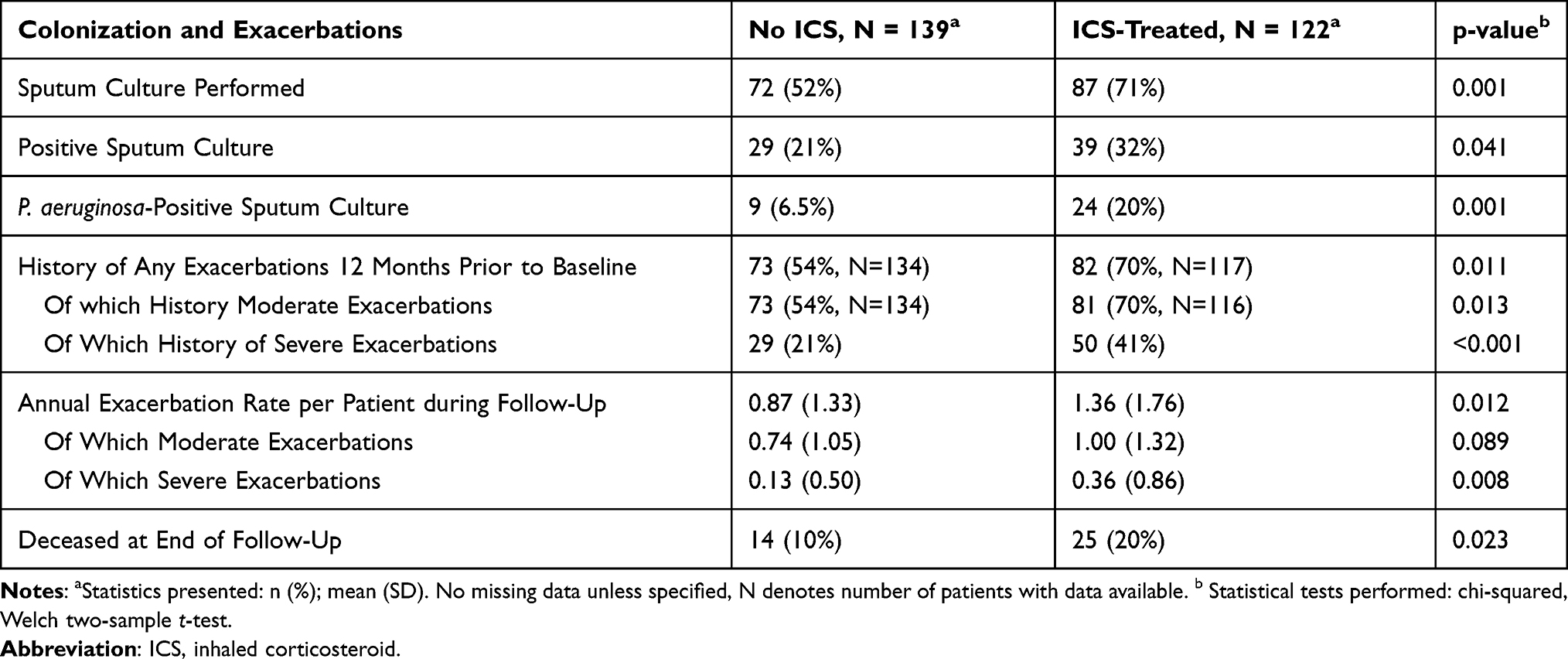 |
Table 3 Burden of Disease in 264 Respiratory Outpatients with Bronchiectasis Followed for 5 Years at Two University Hospitals, Stratified by Treatment with Inhaled Corticosteroids |
Acute Exacerbations
Having had at least one moderate exacerbation during the last 12 months prior to baseline was more common in patients prescribed ICS treatment (70% versus 54%, p 0.011). Likewise, a history of severe, exacerbations requiring hospitalization was overrepresented by patients receiving ICS (41% versus 21%, p <0.001) (Table 3).
Mortality
Being prescribed high-dose, but not low-to-moderate doses, of ICS was associated with all-cause mortality in bivariable regression (HR 4.66 (95% CI 2.12–10.3; p <0.001)). When adjusted for age, sex, smoking status, baseline FEV1 and concomitant asthma/COPD high-dose ICS treatment remained significantly associated with all-cause mortality with an HR of 4.93 (95% CI 1.73–14.0; p=0.003) (Table 4).
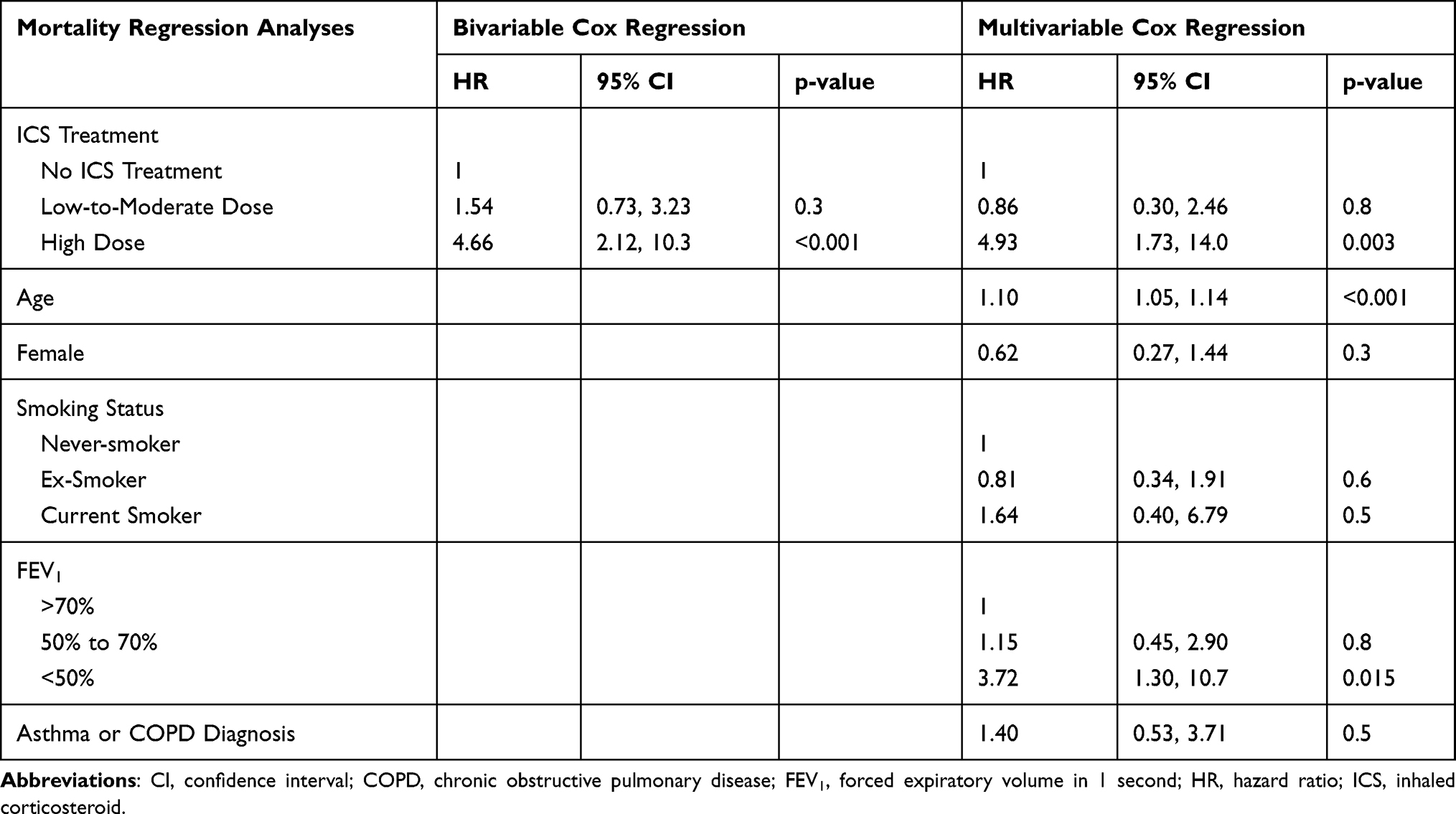 |
Table 4 HR of All-Cause Mortality in 264 Respiratory Outpatients with Bronchiectasis Followed for 5 Years at Two University Hospitals, Calculated Using Cox Regression |
Discussion
In this study, ICS treatment in BE was associated with a higher prevalence of symptoms, increased risk of all-cause mortality in multivariable Cox regression adjusted for age, gender, FEV1, smoking status and concurrent asthma/COPD. Furthermore, approximately one in five patients treated with ICS did not have concurrent asthma or COPD, and one in four ICS-treated patients without asthma or COPD received high-dose ICS.
Bronchodilator and Inhaled Corticosteroid Treatment of Bronchiectasis
As BE shares some traits with both asthma and COPD,19–21 inhaled treatment strategies have often been directly extrapolated from asthma and COPD. Clinical guidelines offer a weak recommendation towards the use of long-acting bronchodilators, citing low overall risk of adverse reactions3 in smaller or unblinded studies with mixed results.22,23 Accordingly, we found no evidence of widespread prescription in patients without concurrent asthma or COPD.
The current European Respiratory Society guidelines advise against ICS treatment for BE, unless otherwise indicated3 due to lack of clear evidence of benefit.13 We found a slightly lower prevalence of ICS treatment than previous studies,24,25 with 18% of the patients with BE were treated with ICS despite no concurrent asthma or COPD.
Symptom reduction using ICS has reported by one study by Martinez-Garcia and colleagues,26 with reduced dyspnoea scores, sputum production and improved QoL – perhaps dependent on eosinophil airway inflammation.27 In the present study, and in contrast to previous neutral studies,26,28 we have demonstrated increased prevalence of moderate and severe exacerbations in patients with BE using ICS, perhaps due to the study design with standard-of-care of the present study.
Positive Sputum Cultures
In the present cohort, Pseudomonas-positive sputum cultures were more common in patients treated with ICS, than in non-ICS users. However, this finding is possibly due to bias by indication, as sputum cultures typically only are performed when patients are experiencing exacerbations and ICS users were more prone to exacerbations in the present study. Indeed, in several other studies, no association between ICS treatment, regardless of dose, and 6-month Pseudomonas colonization has been observed.13,22,28
Previous studies have shown associations between lower FEV1 and Pseudomonas-positive sputum cultures in COPD as well as BE.29–32 Indeed, in the present study, patients with FEV1 <50% had a higher prevalence of Pseudomonas-positive sputum samples. If colonization is a marker of severe disease or a direct cause of severe disease remains unknown, as some studies have found an accelerated FEV1 decline in BE patients colonized with Pseudomonas,31 while others conclude that low FEV1 is a risk factor but does not influence FEV1 decline.32
Inhaled Corticosteroids and Mortality
The use of high-dose ICS was a significant predictor of all-cause mortality in our study, even when adjusting for both FEV1 and concurrent asthma or COPD. In COPD, positive effects on exacerbation rates in COPD with eosinophilic inflammation are seemingly well documented.33 In terms of mortality, the evidence is unclear, with the positive IMPACT trial34 contrasting a pooled analysis by Vestbo and colleagues.35 In terms of asthma, present evidence is less conflicted, with large studies showing mortality reductions in both mild-to-moderate and severe asthma.36–38
In the present study, the increased risk of mortality with high-dose ICS use was independent of concurrent asthma and/or COPD. Data on mortality and ICS use in BE is sparse and the 2018 Cochrane review by Kapur et al. does not report mortality as an outcome.13 A comparative study showed increased risk of mortality with ICS therapy compared to macrolides39 in patients with BE. Further long-term randomized studies are desperately needed to provide clinical evidence of benefit or harm with ICS use in bronchiectasis, especially considering that ICS prescription without indication from other respiratory diseases ranges from 18% in the present study and exceeding 40% in others.25
Limitations
The present study is strengthened by the national registries available in Denmark and thus no loss to follow-up in terms of our primary endpoint. However, some misclassifications regarding ICD-10-coding and missing prescription data is inevitable. Additionally, while patients were continuously enrolled in the cohort, patients with radiologic-only disease were often returned to primary care resulting in some missing 5-year follow-up data for secondary endpoints. However, as information regarding prescriptions, microbiology, biochemistry, hospitalization and death is available from national sources, most endpoints in this study should not be affected.
Adherence to ICS is not accounted for in the present study; however, 70% of the patients prescribed ICS at baseline had active prescriptions at the end of follow-up, suggesting active treatment with frequent redemptions. Remaining patients were either deceased (21%) or had no active prescriptions (9%). As such, correct exposure status during the observation period is assumed.
Reverse causation, bias by indication and/or severity cannot be completely ruled out in our findings, even after statistical correction for important markers for mortality such as FEV1. This is unfortunately primarily due to nature of the present study and is an inherent flaw in study design. Larger, prospective studies are needed to fully elucidate any possible causation between ICS use and mortality.
Conclusion
In conclusion, the present study adds to the evidence suggesting the use of one-size-fits-all ICS treatment in BE, especially in patients with no concurrent asthma or COPD, is detrimental to patient health. Particularity high-dose ICS seems to be strongly associated with adverse outcomes such as all-cause mortality, but bias by indication and severity might make it difficult to draw valid conclusions. However, there is an urgent need for practical guidelines and tools to identify which patients could benefit from ICS treatment to ensure a favourable risk–benefit ratio in this highly vulnerable patient population.
Disclosure
KEJH reports personal fees from AstraZeneca, Chiesi and TEVA outside the present work. CSU reports personal fees from AstraZeneca, Chiesi, TEVA, Novartis, GSK, Orion Pharma, Actelion, ALK-Abello, Sanofi, and Boehringer-Ingelheim outside the present work. KF, AB and MS declare no conflicts of interest with regard to the present article.
References
1. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi:10.1056/NEJMoa0805800
2. Martínez-García MA, Perpiñá-Tordera M, Román-Sánchez P, Soler-Cataluña JJ. Quality-of-life determinants in patients with clinically stable bronchiectasis. Chest. 2005;128(2):739–745. doi:10.1378/chest.128.2.739
3. Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629. doi:10.1183/13993003.00629-2017
4. Cole PJ. Inflammation: a two-edged sword--the model of bronchiectasis. Eur J Respir Dis Suppl. 1986;147:6–15.
5. Fjaellegaard K, Sin MD, Browatzki A, Ulrik CS. Antibiotic therapy for stable non-CF bronchiectasis in adults - A systematic review. Chron Respir Dis. 2017;14(2):174–186. doi:10.1177/1479972316661923
6. Mandal P, Hill AT. Bronchiectasis: breaking the cycle of inflammation and infection. Lancet Respir Med. 2013;1(1):2012–2013. doi:10.1016/S2213-2600(13)70005-5
7. Chalmers JD, Boersma W, Lonergan M, et al. Long-term macrolide antibiotics for the treatment of bronchiectasis in adults: an individual participant data meta-analysis. Lancet Respir Med. 2019;7(10):845–854. doi:10.1016/S2213-2600(19)30191-2
8. Mandal P, Chalmers JD, Graham C, et al. Atorvastatin as a stable treatment in bronchiectasis: a randomised controlled trial. Lancet Respir Med. 2014;2(6):455–463. doi:10.1016/S2213-2600(14)70050-5
9. Lasserson TJ, Holt K, Milan SJ, Greenstone M. Oral corticosteroids for bronchiectasis (stable and acute exacerbations). Cochrane Database Syst Rev. 2001. doi:10.1002/14651858.CD002162
10. Chalmers JD, Haworth CS, Metersky ML, et alL; WILLOW Investigators. Phase 2 Trial of the DPP-1 Inhibitor Brensocatib in Bronchiectasis. N Engl J Med. 2020;383(22):2127–2137. doi:10.1056/NEJMoa2021713.
11. Bateman ed ED, Hurd SS, Barnes PJ, et al.Global strategy for asthma management and prevention: GINA executive summary. European Respiratory Journal. 2008;31(1):143–178. doi:10.1183/09031936.00138707.
12. Halpin DM. Global Initiative for Chronic Obstructive Lung Disease. GOLD Report 2020. Glob Initiat Chronic Obstr Lung Dis. 2020.
13. Kapur N, Petsky HL, Bell S, Kolbe J, Chang AB. Inhaled corticosteroids for bronchiectasis. Cochrane Database Syst Rev. 2018;2018(5):485. doi:10.1002/14651858.CD000996.pub3
14. Roland NJ, Bhalla RK, Earis J. The local side effects of inhaled corticosteroids: current understanding and review of the literature. Chest. 2004;126(1):213–219. doi:10.1378/chest.126.1.213
15. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
16. Hill AT, Haworth CS, Aliberti S, et al. Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research. Eur Respir J. 2017;49(6). doi:10.1183/13993003.00051-2017
17. Agarwal R, Chakrabarti A, Shah A, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850–873. doi:10.1111/cea.12141
18. Chalmers JD, Goeminne P, Aliberti S, et al. The bronchiectasis severity index an international derivation and validation study. Am J Respir Crit Care Med. 2014;189(5):576–585. doi:10.1164/rccm.201309-1575OC
19. Ip M, Lam WK, So SY, Liong E, Chan CY, Tse KM. Analysis of factors associated with bronchial hyperreactivity to methacholine in bronchiectasis. Lung. 1991;169(1):43–51. doi:10.1007/BF02714140
20. Tsikrika S, Dimakou K, Papaioannou AI, et al. The role of non-invasive modalities for assessing inflammation in patients with non-cystic fibrosis bronchiectasis. Cytokine. 2017;99(May):281. doi:10.1016/j.cyto.2017.08.005
21. Guan WJ, Gao YH, Xu G, et al. Bronchodilator response in adults with bronchiectasis: correlation with clinical parameters and prognostic implications. J Thorac Dis. 2016;8(1):14–23. doi:10.3978/j.issn.2072-1439.2016.01.05
22. Martínez-García MÁ, Soler-Cataluña JJ, Catalán-Serra P, Román-Sánchez P, PerpiñáTordera M. Clinical efficacy and safety of budesonide-formoterol in non-cystic fibrosis bronchiectasis. Chest. 2012;141(2):461–468. doi:10.1378/chest.11-0180
23. Wong C, Chang C, Lewis C, et al. Tiotropium treatment for bronchiectasis (ROBUST): a randomized, placebo-controlled, crossover trial. In: airway Pharmacology and Treatment [Internet]. Eur Respir Soc. 2017;PA1809.
24. Visser SK, Bye PTP, Fox GJ, et al. Management of Australian adults with bronchiectasis in tertiary care: evidence-based or access-driven? Lung. 2019;197(6):803–810. doi:10.1007/s00408-019-00280-x
25. Henkle E, Aksamit TR, Barker AF, et al. Pharmacotherapy for non-cystic fibrosis bronchiectasis: results from an NTM Info & Research Patient Survey and the Bronchiectasis and NTM Research Registry. Chest. 2017;152(6):1120–1127. doi:10.1016/j.chest.2017.04.167
26. Martínez-García MA, Perpiñá-Tordera M, Román-Sánchez P, Soler-Cataluña JJ. Inhaled steroids improve quality of life in patients with steady-state bronchiectasis. Respir Med. 2006;100(9):1623–1632. doi:10.1016/j.rmed.2005.12.002
27. Aliberti S, Sotgiu G, Blasi F, Saderi L, Posadas T, Martinez Garcia MA. Blood eosinophils predict inhaled fluticasone response in bronchiectasis. Eur Respir J. 2020;56(2):2000453. doi:10.1183/13993003.00453-2020
28. Hernando R, Drobnic ME, Cruz MJ, et al. Budesonide efficacy and safety in patients with bronchiectasis not due to cystic fibrosis. Int J Clin Pharm. 2012;34(4):644–650. doi:10.1007/s11096-012-9659-6
29. Miravitlles M, Espinosa C, Fernández-Laso E, Martos JA, Maldonado JA, Gallego M. Relationship between bacterial flora in sputum and functional impairment in patients with acute exacerbations of COPD. Chest. 1999;116(1):40–46. doi:10.1378/chest.116.1.40
30. Murphy TF, Brauer AL, Eschberger K, et al. Pseudomonas aeruginosa in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2008;177(8):853–860. doi:10.1164/rccm.200709-1413OC
31. Evans SA, Turner SM, Bosch BJ, Hardy CC, Woodhead MA. Lung function in bronchiectasis: the influence of Pseudomonas aeruginosa. Eur Respir J. 1996;9(8):1601–1604. doi:10.1183/09031936.96.09081601
32. Davies G, Wells AU, Doffman S, Watanabe S, Wilson R. The effect of Pseudomonas aeruginosa on pulmonary function in patients with bronchiectasis. Eur Respir J. 2006;28(5):974–979. doi:10.1183/09031936.06.00074605
33. Oshagbemi OA, Odiba JO, Daniel A, Yunusa I. Absolute blood eosinophil counts to guide inhaled corticosteroids therapy among patients with COPD: systematic review and meta-analysis. Curr Drug Targets. 2019;20(16):1670–1679. doi:10.2174/1389450120666190808141625
34. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
35. Vestbo J, Fabbri L, Papi A, et al. Inhaled corticosteroid containing combinations and mortality in COPD. Eur Respir J. 2018;52(6):6–8. doi:10.1183/13993003.01230-2018
36. Suissa S, Ernst P, Benayoun S, Baltzan M, Cai B. Low-dose inhaled corticosteroids and the prevention of death from asthma. N Engl J Med. 2000;343(5):332. doi:10.1056/NEJM200008033430504
37. O’Byrne P, Fabbri LM, Pavord ID, Papi A, Petruzzelli S, Lange P. Asthma progression and mortality: the role of inhaled corticosteroids. Eur Respir J. 2019;54(1):1–14. doi:10.1183/13993003.00491-2019
38. Kuprys-Lipinska I, Kolacinska-Flont M, Kuna P. New approach to intermittent and mild asthma therapy: evolution or revolution in the GINA guidelines? Clin Transl Allergy. 2020;10(1):1–14. doi:10.1186/s13601-020-00316-z
39. Henkle E, Curtis JR, Chen L, et al. Comparative risks of chronic inhaled corticosteroids and macrolides for bronchiectasis. Eur Respir J. 2019;54(1). doi:10.1183/13993003.01896-2018
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.