")
Back to Journals » Infection and Drug Resistance » Volume 15
Inhaled Colistimethate Sodium in the Management of Patients with Bronchiectasis Infected by Pseudomonas aeruginosa: A Narrative Review of Current Evidence
Authors de la Rosa-Carrillo D , Suárez-Cuartín G, Golpe R , Máiz Carro L, Martinez-Garcia MA
Received 28 July 2022
Accepted for publication 2 December 2022
Published 14 December 2022 Volume 2022:15 Pages 7271—7292
DOI https://doi.org/10.2147/IDR.S318173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
David de la Rosa-Carrillo,1 Guillermo Suárez-Cuartín,2,3 Rafael Golpe,4 Luis Máiz Carro,5 Miguel Angel Martinez-Garcia3,6
1Respiratory Department, Hospital de la Santa Creu I Sant Pau, Barcelona, Spain; 2Respiratory Department, Hospital de Bellvitge, L’Hospitalet de Llobregat, Barcelona, Spain; 3CIBER de Enfermedades Respiratorias, ISCIII, Madrid, Spain; 4Respiratory Department, Hospital Universitario Lucus Augusti, Lugo, Spain; 5Respiratory Department, Hospital Ramón y Cajal, Madrid, Spain; 6Respiratory Department, Hospital Universitario y Politécnico La Fe, Valencia, Spain
Correspondence: David de la Rosa-Carrillo, Respiratory Department, Hospital de la Santa Creu I Sant Pau, Carrer Sant Quintí, 89, Barcelona, 08041, Spain, Tel +34 935565972, Email [email protected]
Abstract: International guidelines on the treatment of bronchiectasis indicate that the use of inhaled antibiotics is effective, especially in symptomatic chronic bronchial infection (CBI) due to Pseudomonas aeruginosa (PA). To date, however, no such treatment has been approved by regulatory agencies. Of the inhaled antibiotics on the market, colistimethate sodium (colistin) is one of the most used in many countries, either in its nebulized presentation or as dry powder. Among the characteristics of this antibiotic, it is worth noting that its main target is the lipopolysaccharide in the outer membrane of the cell wall of gram-negative bacteria and that it has a low rate of resistance to PA (< 1%). Most observational studies have shown that the use of colistin in patients with bronchiectasis and CBI due to PA results in a decrease in both the number and severity of exacerbations, an improvement in quality of life, a decrease in sputum volume and purulence, and a high rate of PA eradication, although there are no clear differences with respect to other inhaled antibiotics. However, the lack of randomized clinical trials (RCT) with positive results for its main variable (exacerbations) in an intention-to-treat analysis has prevented its approval by regulatory agencies as a formal indication for use in bronchiectasis. The PROMIS program, made up of two RCT with identical methodology, is currently underway. The first of these RCT (already concluded) has demonstrated a clearly positive effect on the group randomized to colistin in its main variable (number of annual exacerbations), while the results of the second are still pending. This review presents exhaustive information on the pharmacological and microbiological characteristics of colistin, the results of the studies carried out to date, and the future challenges associated with this treatment.
Keywords: colistin, nebulized antibiotics, pharmacology, chronic bronchial infection, COPD
Introduction
Most studies on the efficacy of inhaled antibiotics have generally been performed in cystic fibrosis (CF) patients, and their use in this disease is recommended by all scientific societies.1 Since inhaled antibiotics showed a remarkable improvement in the evolution of CF patients, their use was gradually extended to regular clinical practice in patients with non-CF bronchiectasis (hereafter called bronchiectasis) who had frequent isolations of Pseudomonas aeruginosa (PA), despite the lack of any formal indication in these drugs’ information leaflets. This widespread practice has created a body of evidence over time (mainly in the form of observational studies), which eventually became sufficient for the use of inhaled antibiotics in general, and colistin in particular, to be included among the recommendations of the various national and international treatment guidelines for bronchiectasis.2–4 These developments have inspired research into new molecules and new ways of dispensing inhaled antibiotics, as well as the instigation of various clinical trials whose results will emerge in the coming years.
In recent years, it has been shown that the presence of certain potentially pathogenic microorganisms (PPM), especially PA, is associated with a poorer clinical course, regardless of whether a patient’s underlying lung disease is CF, bronchiectasis, or even chronic obstructive pulmonary disease (COPD). Accordingly, concepts such as primary infection and chronic bronchial infection (CBI) have emerged, allowing a patient to be categorized as being at risk of progressive clinical deterioration and, therefore, a potential candidate for early and/or prolonged antibiotic treatment. There has been an increasing tendency to use inhaled antibiotics to treat these patients, due to their greater bioavailability at the site of infection and lower frequency of systemic side effects.
Although tobramycin has been the most widely studied inhaled antibiotic, its association with local and systemic side effects and the frequency of antibiotic resistance, as well as the clinical worsening of many patients in treatment rest periods, has motivated the search for alternative antibiotics.1 These include colistin or colomycin, an old acquaintance in the field of respiratory infections that fell into disuse due to its side effects when administered systemically. Since the end of the last century, however, there has been far-reaching research into the effectiveness and safety of nebulized colistin in patients with CF and chronic or intermittent bronchial infection by PA, giving rise to a resurgence that has now made it one of the pillars of treatment for these patients.5,6 This development led to the use of colistin in bronchiectasis patients, in both clinical practice and research.
In this article, we review various issues related to the use of colistin in bronchiectasis, such as the deleterious consequences of CBI, the recommendations of the scientific societies regarding the use of inhaled antibiotics in bronchiectasis, and the pharmacological characteristics of colistin, as well as the published scientific evidence regarding its effectiveness and safety.
Why Chronic Bronchial Infection by Pseudomonas aeruginosa and Exacerbations are Important in Bronchiectasis
CBI is one of the key elements of the “vicious vortex” hypothesis in the pathogenesis of bronchiectasis, in which bacteria induce a sustained inflammatory response that leads to further airway structural damage.7 CBI is defined as three or more consecutive positive cultures for the same PPM in a period of at least 6–12 months, with a time span between samples of at least one month.8 PA is one of the most common PPM isolated in the airway samples of bronchiectasis patients, causing chronic infection in up to 25% of them.9,10 PA rapidly adapts to the chronically infected lung by developing antibiotic resistance and forming biofilms to protect itself from the immune system and the effect of antibiotics.11,12 The eradication of PA is thus a treatment priority in bronchiectasis patients, as managing CBI by this pathogen is a major clinical challenge.2,3
The negative effects of PA infection on bronchiectasis patients have been widely studied. In fact, PA-CBI is a marker for disease severity in internationally validated scores such as the Bronchiectasis Severity Index (BSI), the FACED and E-FACED.13–15 In terms of lung function, Martinez-Garcia et al observed that chronic PA infection, frequent exacerbations, and systemic inflammation were associated with a faster worsening of the disease.16 Similarly, another study including 849 patients from the Spanish Bronchiectasis Registry (RIBRON) showed that the annual decline of the forced expiratory volume during the first second (FEV1) was faster in individuals with PA-CBI (−1.37% (52.1 mL) vs −0.37% (−24.6 mL); p <0.001), older age, increased number of previous severe exacerbations, and higher FEV1 at baseline.17
PA has also been shown to play a significant role in bronchiectasis mortality. Chalmers et al observed a mortality rate of 21.2% in bronchiectasis patients with PA-CBI in the BSI cohort,13 while Martinez-Garcia et al found that it was 48.1% in the FACED cohort.14 A Belgian study prospectively assessed mortality in 245 bronchiectasis individuals and identified a hazard ratio (HR) of 1.60 (95% confidence interval [CI] 1.27–2.00; p-value <0.0001) for mortality in patients chronically infected with PA.18 Another long-term study by Loebinger et al showed that age, St. George’s Respiratory Questionnaire (SGRQ) score, PA infection, and lung volumes and diffusion capacity were all independently associated with mortality.19 Finally, a comprehensive analysis by Finch et al, which included these and several other studies to evaluate the impact of PA on the prognosis of adult patients with bronchiectasis, observed a pooled odds ratio [OR] for mortality of 2.95 (95% CI 1.98–4.40; p-value 0.0001) for subjects with PA-CBI.10
Furthermore, PA has also shown a significant correlation with frequent exacerbations. Rogers et al stratified 107 bronchiectasis patients into three groups, according to the predominant microbiota taxon: PA, Haemophilus influenzae, and other taxa. PA predominance was the best predictor of frequent future exacerbations in this cohort.20 The aforementioned comprehensive analysis also showed that PA-CBI was significantly associated with a higher number of hospital admissions (OR 6.57; 95% CI 3.19–13.51; p-value 0.0001) and exacerbations (mean difference 0.97/year; 95% CI 0.64–1.30; p-value 0.0001), as well as poorer quality of life, as defined by the SGRQ score (mean difference 18.2 points; 95% CI 14.7–21.8; p-value 0.0001).10 It is therefore safe to consider PA infection as not only a marker of severe bronchiectasis but also a significant driver of disease progression.
Exacerbations are another key element in the pathogenesis of bronchiectasis. Both the number and severity of exacerbations have been associated with a poorer clinical prognosis in terms of quality of life, lung function decline, increased costs, and mortality.13,15,21,22 In a recent multicenter study including 651 patients, the definition of frequent exacerbator that presented the greatest predictive power for mortality was based on at least two exacerbations/year or one hospitalization/year (area under the curve [AUC]-ROC: 0.75; 95% CI: 0.69–0.81).21 Frequent exacerbations are the strongest predictors of further frequent exacerbations in the future, while 5-year mortality is higher with an increasing number of exacerbations.23 The prevention and prompt management of acute exacerbations are therefore crucial for avoiding disease progression and reducing patient mortality.
Indications of Inhaled Antibiotics in International Guidelines in Bronchiectasis
The indications for the administration of inhaled antibiotics in patients with bronchiectasis have not been well defined and thus vary between the different management guidelines; their most relevant aspects are described in Tables 1 and 2.
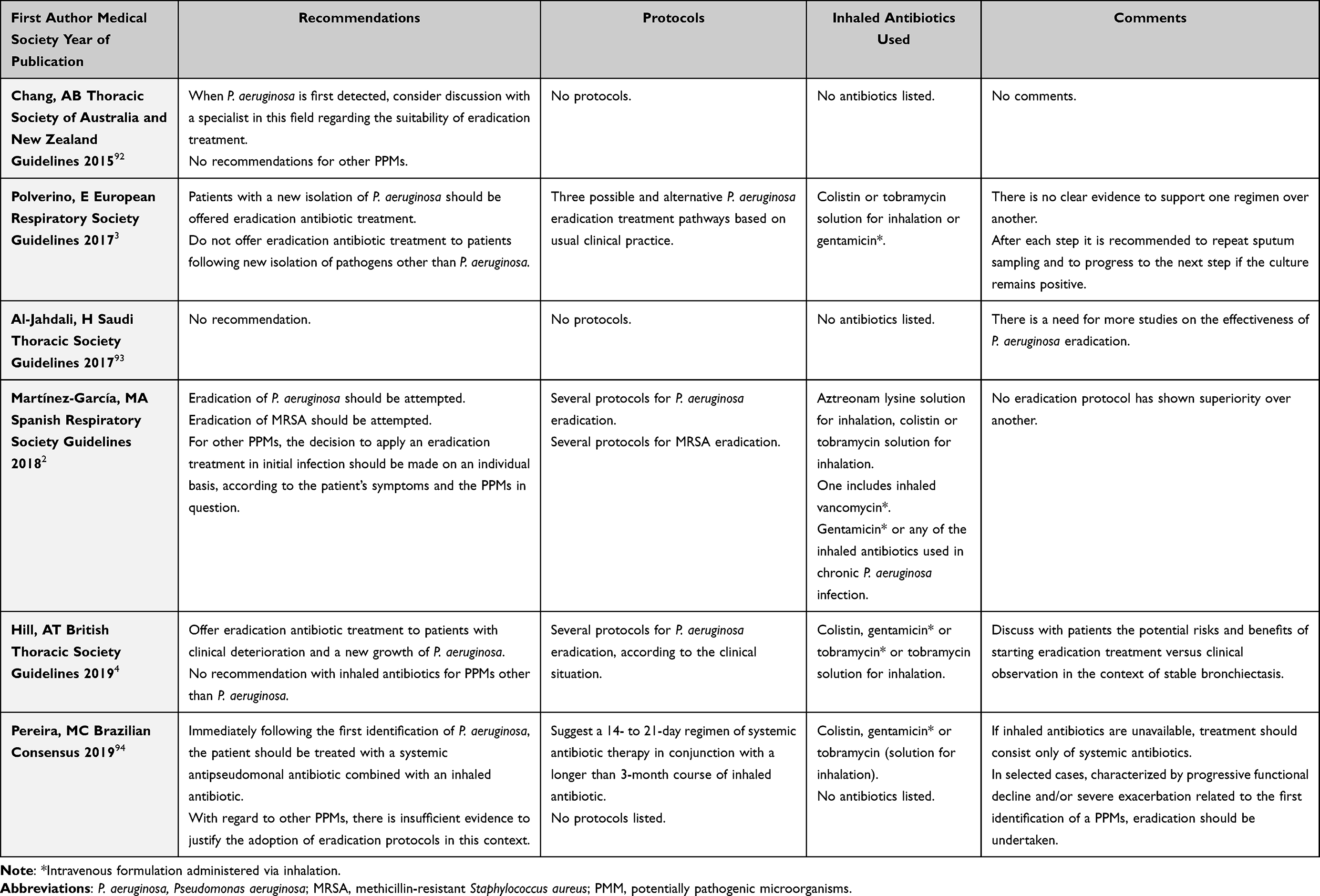 |
Table 1 Indication for Inhaled Antibiotic Treatment in Patients with Bronchiectasis and Primary Bronchial Infection (Presented in Chronological Order of Their Publication Date) |
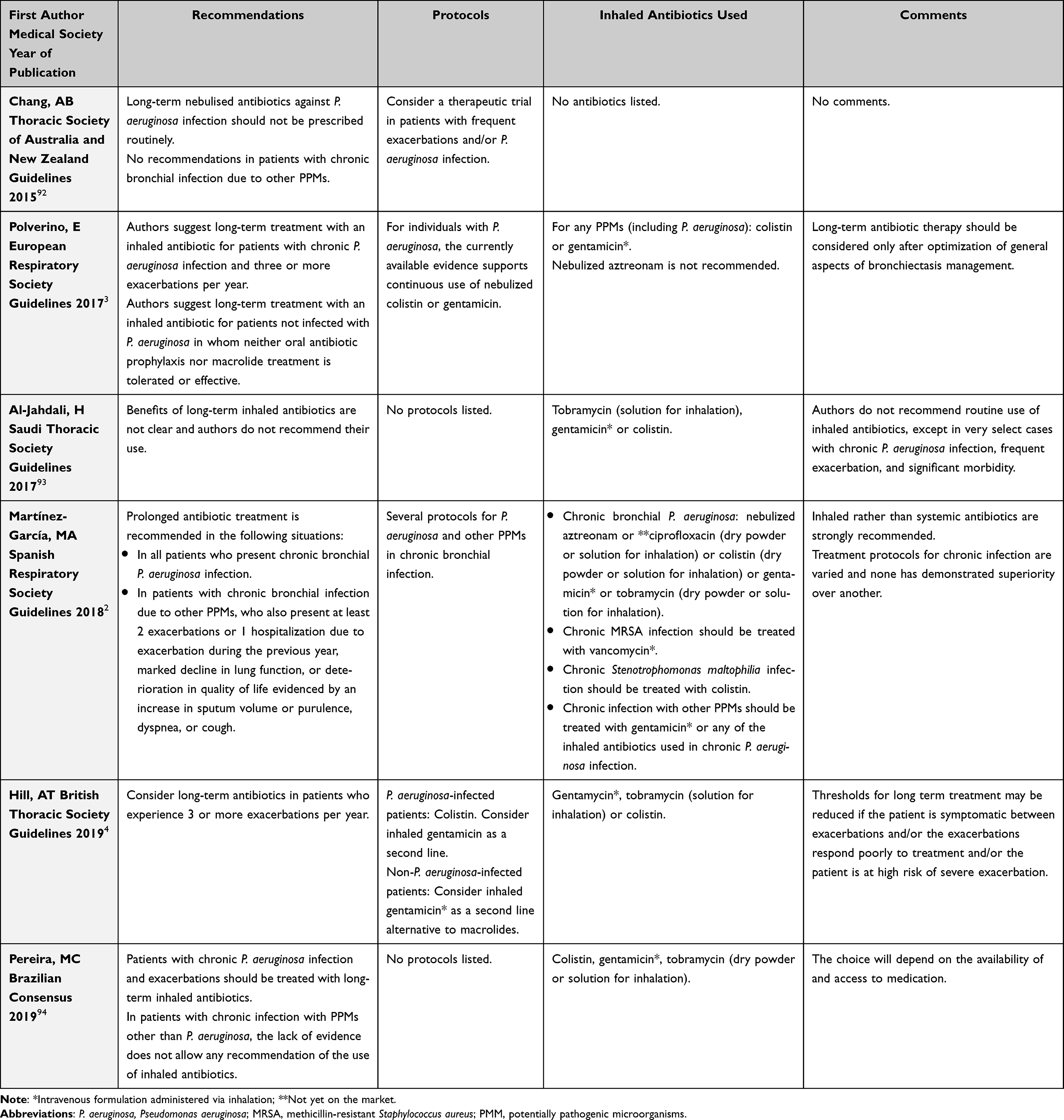 |
Table 2 Indication for Inhaled Antibiotic Treatment in Patients with Bronchiectasis and Chronic Bronchial Infection (Presented in Chronological Order of Their Publication Date) |
Due to the good microbiological results of inhaled antibiotic treatment in patients with BE and PA primary infection, most treatment guidelines include the inhaled route as a means to eradicate this microorganism. Among the different recommendations for treatment of PA primary infection, inhaled antibiotics are usually included, as a first, second, or third line of attack. The eradication of other PPMs is not generally suggested, except in the Spanish guidelines, even though their eradication protocols recommend only the use of oral or intravenous – not inhaled – antibiotics (Table 1).
As regards CBI by PA, all but one of the guidelines recommend treatment with inhaled antibiotics, although with slight variations in the type of antibiotics and the protocols to be used. In CBI by other PPMs, there is more variation in the recommendations, to such an extent that several current guidelines do not recommend any treatment for them. It should be pointed out that the Spanish guidelines stand alone in always recommending inhaled antibiotics as the first therapeutic option in patients with CBI (Table 2).
Inhaled Sodium Colistimethate
Pharmacokinetics and Pharmacodynamics
Polymyxins are a group of polypeptide antibiotics that include several different compounds, of which only polymyxin B and E (colistin) have clinical applications. Colistin is a multicomponent antibiotic made up of a complex mixture of about 30 different decapeptides. Its two main components are colistin A (polymyxin E1) and colistin B (polymyxin E2), which typically account for more than 85% of colistin, but the proportion of these constituents can vary substantially between different pharmaceutical formulations.24
There are two pharmaceutical forms of colistin: colistin sulfate, for topical and oral use, and colistin methanesulfonate (available as a sodium salt, known as sodium colistimethate, less toxic than colistin sulfate), for injection and inhalation. Sodium colistimethate (SCM) is an inactive prodrug. It is hydrophilic and polyanionic at a pH of 7.4, and it contains the colistin moiety, with a sulfomethyl group added to the primary amines of colistin. Its hydrolysis produces the active drug colistin, along with other derivatives.25 Colistin is polycationic at a pH of 7.4 and hydrophilic but, due to the presence of both lipophilic and hydrophilic groups, it has amphipathic property.24 It is advisable not to use the terms colistin and SCM interchangeably because their chemistry, pharmacokinetics, pharmacodynamics, and toxicity are different.26
There are relatively few PK and PD studies on colistin or SCM in humans, and many of these have been carried out in special populations, such as subjects with cystic fibrosis or critically ill patients. After intravenous administration to healthy volunteers, SCM has a terminal half-life of 2 hours, while the terminal half-life of the active compound colistin is 3 hours.27 After administration, SCM is partially converted to colistin by hydrolysis. The main mechanism for clearing unconverted SCM is renal excretion, but, in contrast, the renal clearance of colistin is low, due to extensive tubular reabsorption. The mechanisms for the elimination of colistin remain largely unknown, although it is believed to be eliminated by hydrolysis.24 After intravenous administration, the physicochemical characteristics of SCM and colistin predispose to low penetration into lung tissue, due to their large molecular weights and electric charge. The distribution within the lungs after parenteral administration is therefore believed to be low. In fact, studies have found that, after several dose-regimen administrations of intravenous SCM, the bronchoalveolar lavage and sputum concentrations of the active colistin drug were low,28,29 below the susceptible breakpoint of ≤ 2 mg/L established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) and the Clinical and Laboratory Standards Institute (CLSI) for P aeruginosa.30 However, other authors have found variable concentrations of colistin in the epithelial lining fluid (ELF), ranging from 1.48 to 28.9 mg/L, after intravenous administration of 2 million international units (MIU) of SCM.31
PK parameters may vary substantially in patients compared to healthy volunteers. After intravenous administration, the half-life of SCM will change depending on the volume of distribution, which is a dynamic variable, particularly in critically ill patients, where it fluctuates according to variations in albumin, the infusion of liquids, etc. Moreover, impaired renal function decreases the clearance of SCM and increases the fraction converted to colistin.32 Consequently, it is difficult to predict the PK of colistin (and, accordingly, the drug’s efficacy and toxicity) when intravenous administration is used in these populations. Dose-limiting nephrotoxicity is a significant concern with the parenteral administration of SCM. This, coupled with low lung penetration, makes intravenous SCM a suboptimal drug for treating respiratory tract infections.
As regards the PD of colistin, it can, depending on its concentration, kill susceptible strains of pathogens like PA, with a very modest post-antibiotic effect that is seen only at high, non-clinically relevant concentrations. Studies investigating the relationship between the PK and PD of colistin have evaluated several integrated PK/PD parameters, such as the peak plasma concentrations (Cmax) to minimum inhibitory concentration (MIC) ratio (Cmax/MIC), the time above the MIC (T>MIC), and the area under the concentration curve (AUC) to MIC ratio (AUC/MIC).33 Although early animal studies suggested that once-daily dosing of colistin was most effective against PA and, therefore, that Cmax/MIC might be the most useful PK/PD index for predicting activity, further studies have shown that the most predictive PK/PD index of antibacterial activity is the free (unbound) AUC to MIC ratio (fAUC/MIC), suggesting that time-averaged exposure to colistin is significant for its antibacterial activity and that the drug has both concentration- and time-dependent effects.33
Furthermore, relatively few PK and PD studies of colistin using the inhalation route have been undertaken to date, in either animal models or humans. These studies agree, however, that high levels of colistin exposure are achieved in epithelial lining fluid (ELF) and sputum after inhalation, and that these levels are much higher than after intravenous administration.29,31,34–38 Systemic exposure after SCM inhalation is low. Concentrations of SCM and colistin can be on the order of 100 to 1000 times higher in the ELF than in plasma after administration of aerosolized SCM.31 Yapa et al found that the systemic availability of SCM was low after the administration by nebulizer of 2 and 4 MIU of SCM (7.93% and 5.37%, respectively).29 Boisson et al also found that, after aerosol delivery, only about 9% of the SCM dose reached the systemic circulation.31 In contrast, a much higher systemic bioavailability (46 to 64%) have been observed in rat models after intratracheal administration.35,36 The reason for this difference is unclear, but it has been speculated that the diffusion of colistin across the bronchial epithelium is not only mediated by passive diffusion and that specific drug transporters might be implicated in the absorption of colistin – and the expression of these transporters might be different between species.34
The substantial pulmonary exposure and minimal systemic exposure observed after inhalation of SCM in humans imply that this route should be effective in maximizing the antibacterial effect in the respiratory system, while also minimizing toxicity. There are some limitations, however, in the interpretation of the PK/PD data for colistin when the inhalation route is used. Studies using sputum samples may not adequately reflect the drug concentrations in the lower respiratory tract. Consequently, reliable pharmacokinetic data are often based on the measurement of a drug’s serum concentrations, but these may also inadequately reflect pulmonary drug exposure.31,38 PK/PD targets have been defined to maximize the effect of colistin when used intravenously.30 As mentioned above, the relevant PK/PD parameter for colistin is plasma fAUC/MIC but since plasma concentrations of colistin do not reflect lung concentrations and therefore cannot be used to compare antimicrobial activity in the lungs after SCM administration in aerosol form, a specific ELF fAUC/MIC should be defined. To overcome these problems, PK-PD modeling approaches have been used, predicting a clear superiority of SCM using the inhalation route over intravenous administrations with respect to antimicrobial activity.31
Ratjen et al found that maximum colistin concentrations in the sputum of CF patients peaked 1h after inhalation of SCM, reaching levels at least 10 times higher than the MIC for PA. Significantly, mean concentrations were still above the MIC breakpoint 12h after administration.38 These results support the use of a twice-daily dosing regimen. In contrast, Athanassa et al found, in mechanically ventilated patients treated with inhaled SCM, that the median ELF colistin concentrations were above the MIC of the isolated pathogens at 1 and 4h, but decreased at 8h. The differences in the dose of SCM used in both studies (80 mg every 8h in the Athanassa study and 2 MIU – corresponding to 160 mg of SCM – every 12h in the Ratjen study) may explain these differences.
There are some other areas of uncertainty regarding the PK and PD studies of inhaled colistin. The PK parameters vary widely between studies, and even between individuals within the same study.31,37 The heterogeneity of the populations studied, with a variable degree of disease severity, could partially explain these discrepancies. Furthermore, some studies used sputum samples, which are not homogeneous, and most likely reflect drug deposits in the large rather than the smaller airways.29,38 Studies obtaining samples from the lower airways have used sampling methods (mini-bronchoalveolar lavage) that could sample different lung sections in different patients.31,37 The PK and PD variables could plausibly be different for the same drug, according to whether dry powder or solution formulations are used for administration by inhalation. Tewes et al found a lower exposure of the pulmonary epithelial lining fluid to colistin after intratracheal administration of SCM powder to rats, compared to SCM solution.36 However, they attributed this difference to faster systemic absorption of the drug after the inhalation of powder and, as mentioned above, the PK of SCM absorption might be different in humans. Even using the same formulation, the PK could be different, depending on the delivery system (ie, the design of the nebulizer), although Ratjen et al found no significant differences in sputum colistin concentrations with two different nebulizers.38 It should be mentioned that new inhalable formulations are being developed that combine colistin with other antibiotics, like ciprofloxacin and meropenem, and specific PK/PD studies will be needed with these new formulations, as well as with future nanomedicine-based delivery systems.39–41
Microbiological Properties
Colistin is active against aerobic Gram-negative pathogens such as PA, Haemophilus influenzae, Acinetobacter spp, Escherichia coli, and other Enterobacteriaceae such as Klebsiella spp, Salmonella spp, and Shigella spp. Its activity against Stenotrophomonas maltophilia, Aeromonas spp., and Vibrio spp is variable, and it is not active against some aerobic Gram-negative bacilli, such as Pseudomonas mallei, Burkholderia cepacia, Proteus spp, Providencia spp, Serratia spp, Edwardsiella spp, and Brucella spp. It does not exhibit activity against any Gram-positive or Gram-negative cocci (such as Neisseria gonorrhoeae, Neisseria meningitidis, and Moraxella catarrhalis), fungi, parasites, or against most anaerobes.42
The main target of colistin is the lipopolysaccharide (LPS) in the outer membrane of the cell wall of Gram-negative bacteria. The cationic colistin molecule fuses with the bacterial membrane through electrostatic interactions with anionic groups on the lipid A component of the LPS. Colistin then displaces Mg2+ and Ca2+ from the outer cell membrane of the bacteria, destabilizing the membrane structure and leading to the insertion of the colistin molecule into the membrane. This event results in an increase in the membrane permeability, which is followed by leakage of cell contents and bacterial death. Colistin is believed to act through additional mechanisms, such as the production of reactive oxygen species, which causes oxidative damage leading to cellular death, and the inhibition of bacterial respiratory enzymes. In addition to this direct antibacterial effect, colistin could also inhibit the endotoxin activity of the bacterial LPS, suppressing the capacity to induce shock through the release of inflammatory cytokines.43
Colistin is one of the few antibiotics that may still be useful for the treatment of infections caused by multidrug-resistant microorganisms such as A. baumannii and PA, which have a high tendency to develop multidrug-resistant and other extremely resistant strains, as colistin’s resistance mechanisms are quite rare and chromosomally encoded, making transfer difficult. Therefore, the rate of resistance against colistin in Gram-negative pathogens appears to be lower than against that of other classes of antibiotics.44,45 The primary mechanism underlying colistin resistance seems to reside in modifications to the LPS through the addition of cationic groups that reduce its negative charge, thus reducing electrostatic interactions with the positively-charged colistin. Other proposed resistance mechanisms include mutations leading to loss of LPS (with subsequent loss of the colistin target), overproduction of capsular polysaccharide that hides the colistin binding sites, and enzymatic inactivation of colistin.43,46
Colistin resistance can be acquired through colistin-heteroresistant bacteria. Heteroresistance is a form of antibiotic resistance in which a bacterial strain is composed of one minor resistant subpopulation and one largely susceptible subpopulation.47 Misclassification of heteroresistant isolates as susceptible can lead to unexplained treatment failures. Although the MIC of most bacteria from these strains is ≤ 2 mg/l, subpopulations can survive in the presence of concentrations greater than 2 mg/l of colistin, leading to amplification of the resistant subpopulations.46 This phenomenon, which has been particularly described in the case of Acinetobacter baumannii, has been attributed to bacterial exposure to suboptimal doses of colistin. It could therefore be a concern when using inhaled antibiotics, which may reach low (subinhibitory) concentrations in those areas of the lung with more severe structural damage.
In addition to mutation-based resistance mechanisms, another significant area of concern is the transfer between different bacterial species of the plasmid-mediated mcr-1 gene, which encodes colistin resistance in Gram-negative bacteria.43 The mechanism by which mcr-1 induces colistin resistance is similar to that of intrinsically resistant bacteria: ie, it decreases the electrostatic interactions between colistin and LPS.43 The dissemination of mcr-1, first described in 2015 in an E. coli strain in China,48 has now been reported worldwide. It has been found that mcr-1 alone could, without any additional resistance mechanisms, provide significant resistance to colistin in several Enterobacteriaceae.
Efficacy and Safety of Colistin in Patients with Bronchiectasis
Observational Studies
The first descriptions of the use of colomycin in patients with non-cystic fibrosis bronchiectasis date back more than 50 years. These came from small retrospective series of patients with heterogeneous clinical features, in which other inhaled antibiotics were also used and the results were inconclusive, or even contradictory.49,50 The beginning of this century saw further publications such as Montero et al,51 which included patients who received both intravenous and inhaled treatment for very different indications, including bronchial infection by PPM in patients with chronic bronchial disease. However, its retrospective design and the heterogeneity of the patients included, with several types of infection and different treatment approaches, do not allow us to draw relevant conclusions about the possible usefulness of colistin in patients with bronchiectasis.
Table 3 summarizes the most relevant observational studies in which the effectiveness and safety of inhaled colistin in patients with bronchiectasis have been specifically assessed. One of the pioneering studies in this field was that of the Australians Steinfort et al,52 which consisted of a cohort of 18 patients with either bronchiectasis or COPD, along with chronic bronchial sepsis. Their results showed that the administration of nebulized colistin reduced respiratory function loss and improved quality of life in patients with chronic lung disease colonized by susceptible multidrug-resistant PPM, with no appreciable side effects. Despite acknowledging that it was a small study with various limitations that rule out any generalizable conclusions, the authors proposed that colistin could be a useful treatment in patients with poor control of symptoms or frequent hospital admissions. They also suggested an evaluation of its effect on the rate of infectious exacerbations and sputum microbiology, including its possible role in the eradication of PA in patients with persistent colonization despite prolonged antimicrobial therapy.
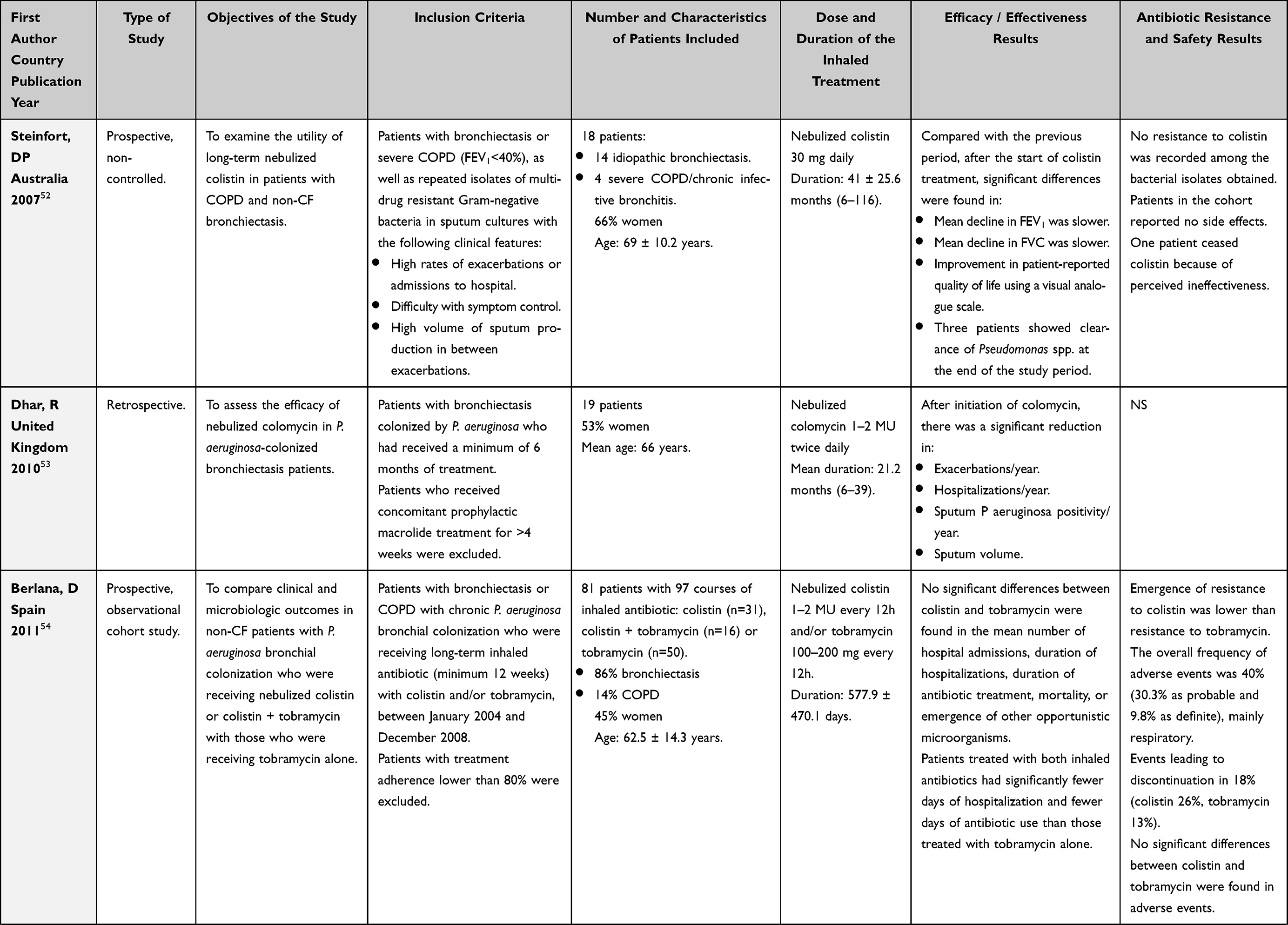 | 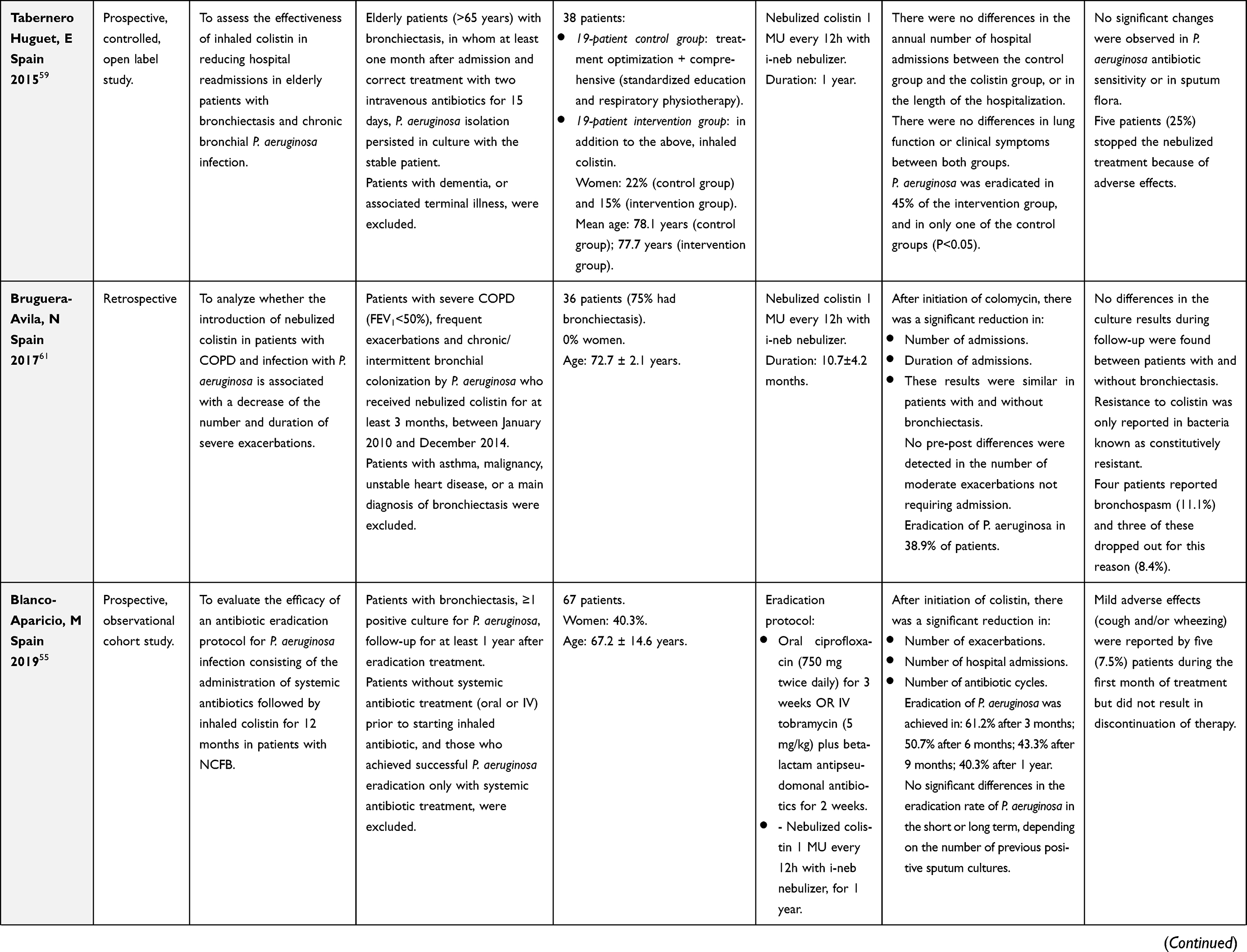 | 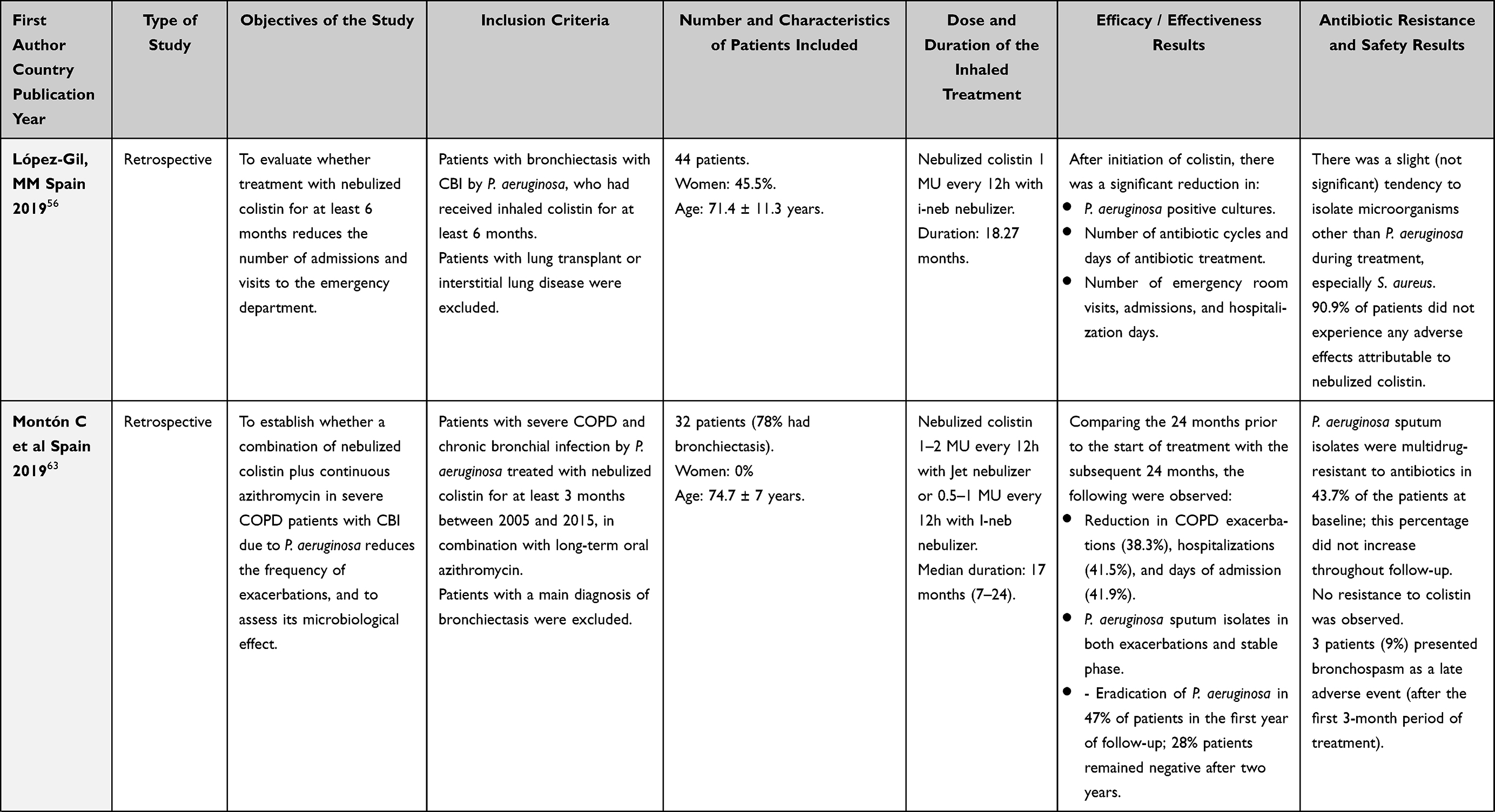 | 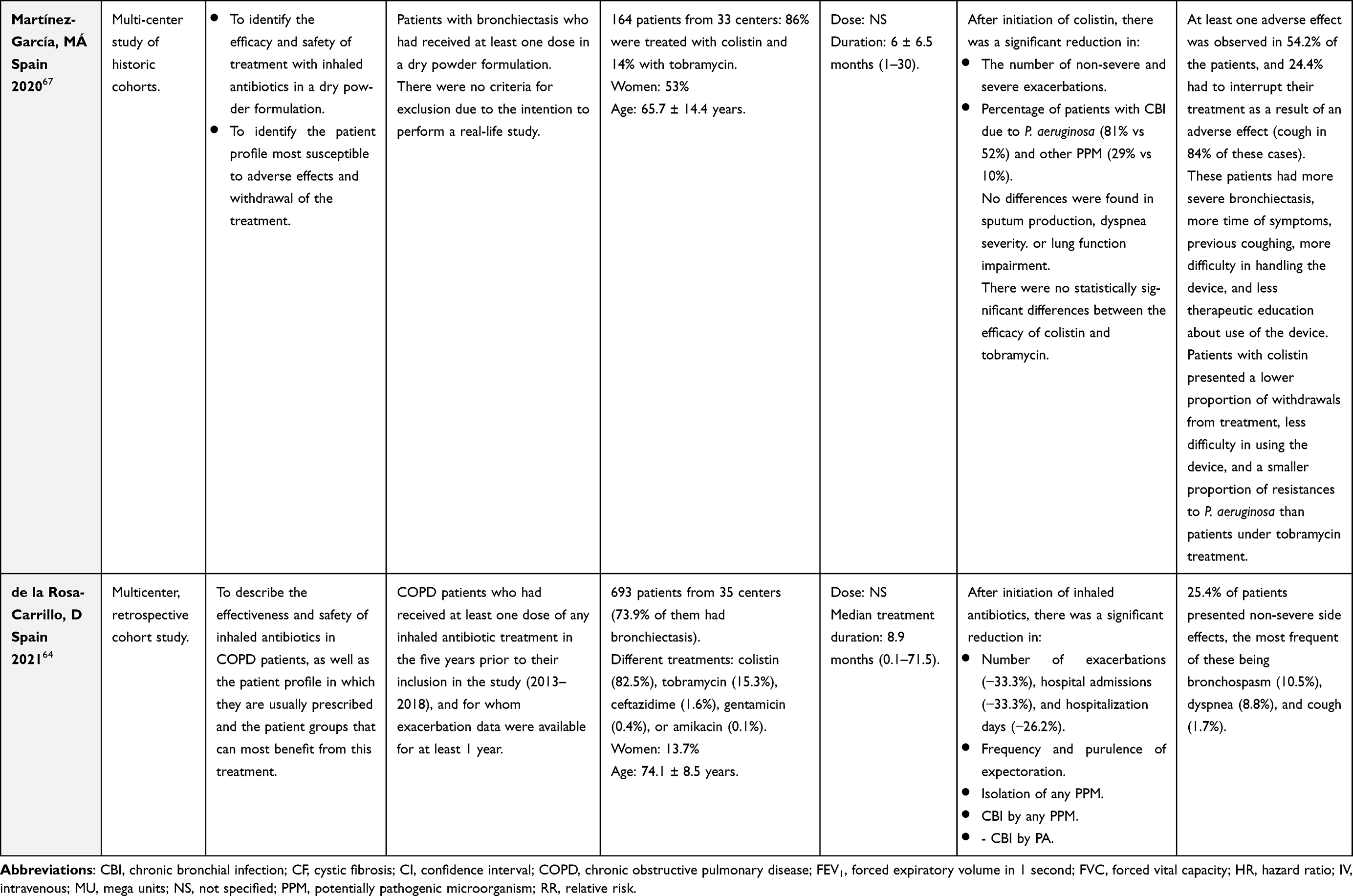 |
Table 3 Studies on the Efficacy/Effectiveness and Safety of Colistin in Bronchiectasis Patients, in Chronological Order According to the Year of Publication |
Some of these questions were addressed shortly afterwards by Dhar et al,53 who conducted a retrospective study in 19 patients in the United Kingdom affected by bronchiectasis and chronic bronchial colonization by PA. Nebulized colomycin reduced exacerbation frequency, number of hospitalizations, sputum PA positivity, and sputum volume, and it was well tolerated. These results were encouraging in this severely affected patient group and, according to the authors themselves, strengthened the need for a prospective, adequately powered, randomized controlled trial to investigate the effectiveness of this treatment more fully.
Since then, most of the observational studies on this subject have been carried out by groups of researchers from Spain. Berlana et al54 carried out a prospective, observational cohort study comparing the clinical and microbiological outcomes of treatment with nebulized colistin compared with those of various tobramycin regimens in 81 patients with bronchiectasis and PA colonization. The results with colistin were similar to those with tobramycin, as regards the mean number of hospital admissions, duration of hospitalizations, duration of antibiotic treatment, adverse events, mortality, and emergence of other opportunistic microorganisms. However, the combined use of colistin and tobramycin appeared to be associated with fewer days of hospitalization and shorter duration of antibiotic treatment.
Another clinical question regarding the use of inhaled antibiotics is their potential ability to achieve the eradication of colonizing PPMs from the airways, thus implying a reversal of the unfavorable clinical course entailed in CBI. In order to analyze the eradication rate of PA from the sputum of bronchiectasis patients treated with inhaled colistin, Blanco-Aparicio et al55 carried out a prospective study on a cohort of 67 patients who underwent a therapeutic protocol that included an initial systemic antibiotic treatment, followed by 1 year of nebulized colistin. They found a high rate of PA eradication (up to 40.3% of patients per year), even in patients with several previous positive cultures. This finding was also associated with a significant decrease in the number of exacerbations and hospitalizations after 1 year of colistin treatment, compared to the previous year. The authors therefore proposed that Pseudomonas eradication should be attempted even when PA is present in several samples of sputum.
With the evidence accumulated up to that moment, it could thus be affirmed that nebulized colistin decreases the number and severity of exacerbations and, accordingly, several groups wanted to validate this premise in their own cohorts of patients with bronchiectasis and CBI due to PA who were receiving this treatment. Thus, López-Gil et al56 carried out an observational, retrospective, and non-interventionist study in 44 patients, which showed that nebulized colistin significantly decreased the number of emergency visits, the frequency and duration of hospitalizations, and the number of positive cultures at 6 and/or 12 months. The treatment was well tolerated in almost all the patients. These results reaffirmed that treatment with nebulized colistin in these cases of severe respiratory disease seems beneficial for the patient, from the clinical and quality-of-life viewpoint.
Both the presence of bronchiectasis and the susceptibility to infections increase with age.57,58 Therefore, the elderly population with chronic airway disease constitutes a subgroup of patients potentially amenable to receiving long-term antibiotic treatment, but the usefulness and safety of inhaled antibiotic therapy in the elderly population is a controversial issue. In order to assess the effectiveness of inhaled colistin in this population, Tabernero Huguet et al59 carried out a prospective, controlled, and open label study in 39 elderly patients with bronchiectasis and CBI by PA. They compared one group receiving conventional treatment (which included education and physiotherapy training) with another that also received nebulized colistin. Significantly more patients achieved Pseudomonas eradication in the colistin treatment group, but there were no benefits in terms of clinical symptoms, lung function, or use of healthcare resources. Moreover, adverse effects were more common in this group (25% stopped the nebulized treatment because of adverse effects). Taking these results into account, it seems clear that further studies are needed to identify factors or subgroups of elderly patients that could be associated with a favorable clinical response to long-term inhaled antibiotic treatment.
Another hot topic in recent years is the association between bronchiectasis and COPD, which can be present in more than 50% of patients with severe COPD.60 Furthermore, evidence has accumulated in recent years to show that COPD patients have alterations in their lung microbiome that may result in CBI, which is associated with a higher frequency of bacterial exacerbations. This treatable trait is responsible for a true infectious phenotype that requires personalized treatment, with the use of short- or long-term antibiotic treatment in addition to the usual COPD treatment. In this respect, Bruguera-Avila et al61 carried out a retrospective study in 36 patients with a primary diagnosis of COPD (75% of whom also had bronchiectasis) who had been treated with nebulized colistin for CBI due to PA. This treatment was associated with a strong decrease in the number and duration of hospitalizations, as well as a low frequency of adverse effects. These results persisted when patients with and without bronchiectasis, or with and without persistence of PA, were analyzed separately, indicating that this treatment is effective even in COPD without bronchiectasis, or in cases in which the PPM cannot be eradicated. These same authors subsequently published an extension of this study in a larger sample of 62 patients, with the aim of describing changes in the bacteriology of sputum in relation to treatment with nebulized colistin.62 The results showed that there was no linear trend in the proportion of isolate Enterobacteriaceae, Gram-positive cocci, Haemophilus influenzae, or fungi. Isolation of Enterobacteriaceae within a year of the initial administration of nebulized colistin was associated with more ambulatory exacerbations. A similarly designed study by Montón et al63 analyzed 32 patients with severe COPD and CBI due to PA (of whom 78% had bronchiectasis), treated with a combination therapy of nebulized colistin and continuous cyclic azithromycin. This regimen reduced the number of both exacerbations and PA sputum isolates, and once again the rate of side effects was low.
On the basis of the results obtained in these single-center studies, de la Rosa et al64 published a multicenter retrospective study promoted by the Spanish Society of Pulmonology (SEPAR) to determine whether the results as regards the effectiveness and safety of inhaled antibiotics in COPD patients were similar across the country. Data from 693 COPD patients from 35 centers were analyzed; 71.7% had bronchiectasis, 46.6% presented CBI by PA, and 82.5% were treated with sodium colistimethate. As in the previous studies, there was a significant decrease after a year of treatment in the number and severity of exacerbations, PPM isolates, and bronchial symptoms. There were no differences between patients with or without bronchiectasis, and 25.4% of patients presented non-severe side effects; the results of the different prescribed antibiotics were not compared. In short, all this evidence has encouraged the more frequent inclusion of inhaled antibiotics in the therapeutic regimens of those patients with COPD and CBI, regardless of whether or not they have associated bronchiectasis.65,66
Finally, with regard to studies on new forms of administration, the retrospective multicenter study by Martínez-García et al67 evaluating the effectiveness of dry-powder inhaled antibiotics (DPIA) is worthy of note. It included 164 patients with bronchiectasis, 86% of whom received colistin. The results showed that DPIA significantly reduced the number of exacerbations, the quantity and purulence of sputum, and the isolation of pathogenic microorganisms. There were no statistically significant differences between the efficacy of colistin and tobramycin. Although there were no serious adverse effects, 40% of patients presented cough, especially those with associated COPD.
It must be taken into account that in the observational studies collected in Table 3, an overall number of only 857 patients with bronchiectasis treated with inhaled colistin were included, after the exclusion of patients who did not have bronchiectasis or received other antibiotics. Moreover, most of these patients are from Spain, following the remarkable and historic implementation of the national guidelines for the treatment of bronchiectasis, which promotes the use of inhaled antibiotic therapy in a greater number of clinical situations than other guidelines. Similar studies are therefore needed in other countries to confirm that the effectiveness and tolerance found in Spain can be extrapolated to other geographical areas and other healthcare systems.
Randomized Controlled Trials
A search in the PubMed and EMBASE databases for randomized controlled trials (RCT) or meta-analyses that include RCTs with the terms in the title or abstract nebulized OR nebulised OR inhaled OR aerosolized OR aerosolised AND colistin OR colistimethate yields 36 studies. These studies present very diverse methodologies (use of colistin alone, colistin associated with other inhaled or intravenous antibiotic treatment, different indications (ventilator-associated pneumonia,68 pneumonia due to multi-resistant microorganisms,69 CF,70 airway infections due to multi-resistant microorganisms,71 and bronchiectasis72), and different outcomes (mortality, clinical aspects, quality of life, exacerbations, and various microbiological aspects). Some meta-analyses (usually mixing RCT and observational studies) show a positive effect of inhaled antibiotics and a lower number of adverse effects than systemic antibiotics for most of these indications (although in some cases, the results are controversial, depending on the study’s methodology or the outcome studied). In general, it can be concluded that there was no clear superiority in those regimens that include inhaled colistin compared to those with other inhaled antibiotics, so further studies are recommended.
More than two decades ago, the first RCT was performed to evaluate the effect of inhaled colistin in subjects with CF by comparing it with inhaled tobramycin for 4 weeks twice daily, in 115 patients aged over 6 years. Although both treatments reduced the bacterial load, the tobramycin nebulizer solution significantly improved the lung function of patients with CF chronically infected by PA but colistin did not; however, this was a short-term study (1 month).73
In the case of bronchiectasis, colistin is the most widely used inhaled antibiotic in Spain, either alone or in combination with other drugs.74 Following the various international guidelines, its indications are diverse: the treatment of primary infection by PA and chronic bronchial infection by PA or other microorganisms. However, these same guidelines point out that there is no clear difference between the regimens used with different inhaled antibiotics.2–4
Various RCT performed with other inhaled antibiotics (ciprofloxacin,76–79 tobramycin,80 and aztreonam81) and various types of inhalers or nebulizers75 have shown conflicting results in patients with bronchiectasis, even with almost identical methodologies. The case of ciprofloxacin from the RESPIRE76,77 and ORBIT78,79 programs is paradigmatic. Each of these two programs consisted of two RCTs with identical methodologies, but only one of each pair of studies had positive results, in addition to the pooled analysis.79 There is no a clear explanation for these conflicting results, but probably the difference in the baseline characteristics, especially those related to the geographical origin, of the included individuals is one of the most accepted. However, the latest meta-analyses of the effectiveness and safety of IA that include RCT indicate a greater efficacy of inhaled antibiotics, confirming the experience in clinical practice of most physicians who use them in an appropriate selection of patients.82,83 Nevertheless, given the contradictory results mentioned above, the regulatory agencies have not yet approved any inhaled antibiotic for use in patients with bronchiectasis, pending new RCT that ratify their efficacy.
The specific case of inhaled colistin was not an exception. In 2014, the first study in the PROMIS clinical program (a therapeutic program that received FDA qualified infectious disease product and fast track designation for the prevention of pulmonary exacerbations in adults with bronchiectasis) was published to evaluate the efficacy and safety of colistin in the treatment of PA infection.72 Given this study’s negative results in the intention-to-treat population (ITT) (see below), two larger parallel RCT (PROMIS I and PROMIS II) were launched, one of which has already offered very promising results. In all of these studies, the main objective was the time to the first exacerbation (PROMIS) or the number of exacerbations (PROMIS I and II), given the importance of this factor in bronchiectasis and in its prognosis.84–87 One of the main limitations of these RCTs is the strict inclusion criteria used since usually only those bronchiectasis patients with bronchial infection by P. aeruginosa and multiple exacerbations were included. Therefore, the conclusions cannot be generalized to the usual population seen in clinical practice.
PROMIS Study (http://www.isrctn.org/ (ISRCTN49790596)
Published in 2014, this was a randomized placebo-controlled trial to assess the efficacy and safety of inhaled colistin in patients with bronchiectasis and CBI by PA.72 In all, 35 centers from UK, Russia, and Ukraine recruited patients aged at least 18 years, with confirmed bronchiectasis, at least two or more positive respiratory tract cultures for PA in the preceding 12 months, and one more PA cultured from a sputum sample taken at the screening visit.
After 21 days of oral treatment aimed at PA eradication, 144 patients were randomized to receive colistin (1 million IU; n=73) or placebo (0.45% saline; n=71) via the I-neb device, twice a day for up to 6 months. The primary endpoint was the time to the first exacerbation in an ITT population. Secondary endpoints included the time to the first exacerbation based on adherence recorded by the I-neb (per protocol population), PA bacterial density, quality of life (measured by the SGRQ), and safety parameters.
At least one exacerbation was experienced by 49% and 59% of patients during the study in the colistin and placebo groups, respectively, but there were no differences regarding the time to the first exacerbation in the colistin and placebo groups (165 (42) versus 111 (52) days; p=0.11) for the median time (25% quartile).
During the study, 77.1% of patients had an adherence >80% in both groups. It is significant that, at the level of at least 80% of adherence, the median time to the first exacerbation was significantly longer in the colistin group compared to the placebo group (168 (65) versus 103 (37) days, p=0.028).
As regards secondary objectives, evaluated in an ITT analysis, PA density was reduced after four (p=0.001) and 12 weeks (p=0.008), respectively. The total score of the SGRQ was improved after 26 weeks in the colistin group compared to the placebo group (−10.51 (95% CI: −17.87 to −3.14); p=0.006). There was no change in the mean 24-h sputum weight.
It should be stressed that the decrease in PA density and, above all, the significant improvement in the quality of life experienced by the group treated with colistin compared to the placebo group did not result in any improvement in the time to the first exacerbation. However, although statistical significance was not reached, the net difference between the groups was 54 days, which could be considered clinically significant, whereas patients with good adherence achieved a difference of 65 days (only 11 days more than in the ITT population) – a difference not much greater but statistically significant. This suggests that it is possible that the number of patients included in the study and/or the number of outcomes (exacerbations) observed were low. Moreover, although the study was multicenter, the patients came from only 3 countries (UK, Ukraine, and Russia), which could have influenced the results as it could not be a representative group. For all these reasons and given that, despite the study being statistically negative, colistin offered hope of being a well-tolerated and effective inhaled antibiotic, the PROMIS I and II studies were designed with a larger number of patients.
PROMIS I Study (Clinicaltrials: NCT03093974)
This is a Phase 3, placebo-controlled, multicenter clinical trial designed to investigate the efficacy and safety of inhaled colistin (colistimethate sodium) in bronchiectasis chronically infected with PA with at least two exacerbations requiring oral or inhaled antibiotics or one exacerbation requiring intravenous antibiotics in the previous 12 months. Patients were randomized to receive twice-daily colistin via I-neb (delivered dose of 0.3mL of 1 MIU in 1mL 0.45% saline) vs placebo (0.3mL 0.45% saline) for 12 months.
The primary endpoint was the mean exacerbation rate over 12 months. Secondary endpoints (all at 12 months) were: time to the first exacerbation, annualized number of pulmonary exacerbation-free days, number of severe exacerbations, quality of life (measured via SGRQ and QoL-B questionnaire), days of absence from work, and PA density in sputum.
Finally, 377 patients from 85 centers in 12 countries (Belgium, Netherlands, Spain, Switzerland, UK, Australia, Germany, Greece, Israel, Italy, New Zealand, Poland, and Portugal) were included, thus increasing the study’s representativity and statistical power with respect to the previous one (PROMIS). Patients were randomized – 177 to colistin via I-neb and 200 to placebo. The annual rate of exacerbations was lower in patients receiving colistin vs placebo (0.58 per patient per year vs 0.95, rate ratio (RR) 0.61; 95% CI: 0.46–0.82, p=0.001). The effect of the treatment was even greater in adherent subjects (43.5% reduction in exacerbations, p=0.0008). Moreover, the time to the first exacerbation was prolonged in the colistin group (HR 0.59, 95% CI 0.43–0.81, p=0.00074). Severe exacerbations were also reduced (RR 0.41, 95% CI: 0.23–0.74, p=0.003). The quality of life, as measured by the SGRQ, improved significantly in the colistin arm, with 4.55 points of difference vs placebo after 12 months treatment (p=0.0055). After 28 days treatment, PA density was significantly reduced in the treatment arm, p<0.00001).
No further data are available as the study was presented as an abstract at the 2021 European Respiratory Congress88 and has yet to be published at the time of writing.
PROMIS-II Study (Clinicaltrials: NCT03460704)
This study, for no data have been published at the time of writing, presents an identical methodology to the PROMIS-1 study, although the origin of the patients is different. In this case, the patients come from 12 countries (USA, Argentina, Australia, Canada, France, Germany, Greece, Israel, Italy, New Zealand, Poland, and Portugal).89
The need to present positive results in favor of colistin in an ITT population model in both studies with identical methodologies means that the scientific community is waiting expectantly for the results of this second RCT, given that, if it comes out positively in favor of colistin treatment, it may open the door for official approval from the regulatory agencies for its indication in bronchiectasis and bronchial infection due to PA – this would make colistin the first inhaled antibiotic on the market with this indication.
Safety of Inhaled Colistin
Table 3 (last column) summarizes the main findings on the safety of inhaled colistin in observational studies.52,54–56,59,61,63,64,67 Some points can be highlighted: 1. From 0% to 40% of patients had at least one side effect while used inhaled colistin. In almost all cases the side effects were mild, being the most frequent cough, bronchospasm and dyspnea; 2. The number of side effects was higher in colistin dry-powder inhalers (54.2%), being the most frequent cough (84%) that caused the interruption of treatment in 24.4% of patients. Risk factors for adverse effects were: more severe bronchiectasis, more time of symptoms, previous coughing, more difficulty in handling the device, and less therapeutic education about use of the device;67 3. Very few cases of emerging resistance of PA to colistin emerged during the studies and was lower than those emerging to tobramycin. In the same lines, no unexpected serious adverse reactions were reported and no colistin-resistant strains of PA or treatment-emergent pathogens were identified in RCTs.72,88
Future Challenges
In the light of all the above, it is evident that several challenges will have to be faced in coming years if inhaled colistin is to earn its place in the therapeutic arsenal of patients with respiratory infections. If the good results of the PROMIS program are confirmed, however, the priority should be to obtain a formal indication from the regulatory agencies for the treatment of CBI due to PA in bronchiectasis.
Further studies (preferably RCT) should also be carried out to increase our knowledge of the effectiveness and safety of inhaled colistin in different clinical situations. Its effect on bronchial infection by PPMs other than PA, such as S. aureus or the most common non-fermenting Gram-negative bacilli (A. xylosoxidans, S. maltophilia, among others), should also be analyzed. Similarly, it is necessary to deepen our knowledge of the effectiveness of colistin on CBI in conditions other than bronchiectasis and CF (eg, COPD and/or asthma). Subsequent studies should also aim to analyze the effects of colistin on primary infection by PA, in terms of its eradication rate, the optimal time to start treatment after the first isolation and the appropriateness of associating it with systemic antibiotic treatment. In this respect, there needs to be further classification of the role of biomarkers and patient genetics and endotypes in identifying the best candidates for this treatment, as well as the evaluation of its maintenance period. Furthermore, the effects of different doses of colistin, and of the nebulized and dry-powder forms, should be assessed, since this information would permit an optimization of its use and perhaps even its tolerance, without losing any effectiveness. The effect of the different inhalation devices should also be prospectively evaluated, even by making direct comparisons between them. Moreover, it would be important to know the effects of colistin on variables other than exacerbations, such as the quality of life, patient-reported outcomes, lung function, and mortality.
Such studies which would fundamentally assess the effectiveness of colistin, but others should also be undertaken to evaluate its long-term adverse effects, such as the generation of antibiotic resistance, the appearance of emerging or multi-resistant microorganisms, or unwanted effects on the lung microbiome, among others.
Inhaled antibiotics in general, and colistin in particular, are drugs whose average price is relatively high, and this factor, together with the lack of their formal indication for patients with bronchiectasis, has made some healthcare providers reluctant to authorize their use. Any future research to determine the effectiveness of this type of treatment should therefore be combined with an analysis of its cost-effectiveness and cost-utility. It is very likely that its use can be shown to reduce the high overall healthcare costs associated with the treatment of bronchiectasis, especially in patients with CBI.22 This would imply both a benefit for the patient and for the health system, and it would also make it easier to overcome any resistance to financing its treatment.
Going beyond clinical research, there is a need to carry out new pharmacological studies that analyze PK/PD parameters in humans, including the use of inhaled formulations (particularly with new combinations of colistin and other antibiotics) and of colistin with the new nanoparticles that are currently in development.90,91
Conclusions
Nebulized colistimethate sodium is a therapeutic tool that can help improve clinical control in patients suffering from respiratory infections due to PPM, particularly those with resistance or multi-resistance to systemic antibiotics. In recent decades, there has been increasing scientific evidence of the deleterious effect of CBI due to PPM in bronchiectasis patients, coupled with an increasing use of nebulized colistimethate sodium in this type of patient, leading to a growing body of evidence confirming its notable effectiveness and safety. However, it is important to recognize that whilst nebulised colistin is recommended in many guideline documents and in widespread use, there is a paucity of randomized clinical trial data to clearly demonstrate.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cantón R, Máiz L, Escribano A, et al. Spanish consensus on the prevention and treatment of Pseudomonas aeruginosa bronchial infections in cystic fibrosis patients. Arch Bronconeumol. 2015;51(3):140–150. doi:10.1016/j.arbres.2014.09.021
2. Martínez-García MÁ, Máiz L, Olveira C, et al. Spanish guidelines on treatment of Bronchiectasis in adults. Arch Bronconeumol. 2018;54:88–98. doi:10.1016/j.arbres.2017.07.016
3. Polverino E, Goeminne PC, McDonnell MJ, et al. European respiratory society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629. doi:10.1183/13993003.00629-2017
4. Hill AT, Sullivan AL, Chalmers JD, et al. British thoracic society guideline for bronchiectasis in adults. Thorax. 2019;74(Suppl 1):1–69.
5. Høiby N. Antibiotic therapy for chronic infection of Pseudomonas in the lung. Annu Rev Med. 1993;44:1–10. doi:10.1146/annurev.me.44.020193.000245
6. Littlewood JM, Koch C, Lambert PA, et al. A ten year review of colomycin. Respir Med. 2000;94(7):632–640. doi:10.1053/rmed.2000.0834
7. Flume P, Chalmers J, Olivier K. Advances in bronchiectasis: endotyping, genetics, microbiome, and disease heterogeneity. Lancet. 2018;392(10150):880–890. doi:10.1016/S0140-6736(18)31767-7
8. Martínez-García MÁ, Máiz L, Olveira C, et al. Spanish guidelines on the evaluation and diagnosis of Bronchiectasis in adults. Arch Bronconeumol. 2018;54:79–87. doi:10.1016/j.arbres.2017.07.015
9. Pasteur MC, Helliwell SM, Houghton SJ, et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med. 2000;162:1277–1284. doi:10.1164/ajrccm.162.4.9906120
10. Finch S, McDonnell MJ, Abo-Leyah H, Aliberti S, Chalmers JD. A comprehensive analysis of the impact of Pseudomonas aeruginosa colonisation on prognosis in adult Bronchiectasis. Ann Am Thorac Soc. 2015;12:1602–1611. doi:10.1513/AnnalsATS.201506-333OC
11. Chalmers JD, Hill AT. Mechanisms of immune dysfunction and bacterial persistence in non-cystic fibrosis bronchiectasis. Mol Immunol. 2013;55(1):27–34. doi:10.1016/j.molimm.2012.09.011
12. Cullen L, McClean S. Bacterial adaptation during chronic respiratory infections. Pathog. 2015;4:66–89. doi:10.3390/pathogens4010066
13. Chalmers JD, Goeminne P, Aliberti S, et al. The bronchiectasis severity index an international derivation and validation study. Am J Respir Crit Care Med. 2014;189:576–585. doi:10.1164/rccm.201309-1575OC
14. Martínez-García MA, De Gracia J, Relat MV, et al. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Eur Respir J. 2014;43:1357–1367. doi:10.1183/09031936.00026313
15. Martinez-Garcia MA, Athanazio RA, Girón R, et al. Predicting high risk of exacerbations in bronchiectasis: the E-FACED score. Int J COPD. 2017;12:275–284. doi:10.2147/COPD.S121943
16. Martínez-García MA, Soler-Cataluña -J-J, Perpiñá-Tordera M, Román-Sánchez P, Soriano J. Factors associated with lung function decline in adult patients with stable non-cystic fibrosis bronchiectasis. Chest. 2007;132:1565–1572. doi:10.1378/chest.07-0490
17. Martinez-García MA, Oscullo G, Posadas T, et al. Pseudomonas aeruginosa and lung function decline in patients with bronchiectasis. Clin Microbiol Infect. 2021;27:428–434. doi:10.1016/j.cmi.2020.04.007
18. Goeminne PC, Nawrot TS, Ruttens D, Seys S, Dupont LJ. Mortality in non-cystic fibrosis bronchiectasis: a prospective cohort analysis. Respir Med. 2014;108:287–296. doi:10.1016/j.rmed.2013.12.015
19. Loebinger MR, Wells AU, Hansell DM, et al. Mortality in bronchiectasis: a long-term study assessing the factors influencing survival. Eur Respir J. 2009;34:843–849. doi:10.1183/09031936.00003709
20. Rogers GB, Zain NMM, Bruce KD, et al. A novel microbiota stratification system predicts future exacerbations in bronchiectasis. Ann Am Thorac Soc. 2014;11:496–503. doi:10.1513/AnnalsATS.201310-335OC
21. Martinez-Garcia MÁ, Athanazio R, Gramblicka G, et al. Prognostic value of frequent exacerbations in Bronchiectasis: the relationship with disease severity. Arch Bronconeumol. 2019;55:81–87. doi:10.1016/j.arbres.2018.07.002
22. De La Rosa D, Martínez-Garcia MA, Olveira C, Girón R, Máiz L, Prados C. Annual direct medical costs of bronchiectasis treatment: impact of severity, exacerbations, chronic bronchial colonization and chronic obstructive pulmonary disease coexistence. Chron Respir Dis. 2016;13:361–371. doi:10.1177/1479972316643698
23. Chalmers JD, Aliberti S, Filonenko A, et al. Characterization of the “frequent exacerbator phenotype” in bronchiectasis. Am J Respir Crit Care Med. 2018;197:1410–1420. doi:10.1164/rccm.201711-2202OC
24. Grégoire N, Aranzana-Climent V, Magréault S, Marchand S, Couet W. Clinical pharmacokinetics and pharmacodynamics of colistin. Clin Pharmacokinet. 2017;56:1441–1460. doi:10.1007/s40262-017-0561-1
25. Antoniu SA, Cojocaru I. Inhaled colistin for lower respiratory tract infections. Expert Opin Drug Deliv. 2012;9(3):333–342. doi:10.1517/17425247.2012.660480
26. Li J, Nation RL. Comment on: pharmacokinetics of inhaled colistin in patients with cystic fibrosis. J Antimicrob Chemother. 2006;58:222–223. doi:10.1093/jac/dkl169
27. Couet W, Gregoire N, Gobin P, et al. Pharmacokinetics of colistin and colistimethate sodium after a single 80-mg intravenous dose of CMS in young healthy volunteers. Clin Pharmacol Ther. 2011;89:875–879. doi:10.1038/clpt.2011.48
28. Imberti R, Cusato M, Villani P, et al. Steady-state pharmacokinetics and BAL concentration of colistin in critically Ill patients after IV colistin methanesulfonate administration. Chest. 2010;138(6):1333–1339. doi:10.1378/chest.10-0463
29. Yapa SWS, Li J, Patel K, et al. Pulmonary and systemic pharmacokinetics of inhaled and intravenous colistin methanesulfonate in cystic fibrosis patients: targeting advantage of inhalational administration. Antimicrob Agents Chemother. 2014;58(5):2570–2579. doi:10.1128/AAC.01705-13
30. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39:10–39. doi:10.1002/phar.2209
31. Boisson M, Jacobs M, Grégoire N, et al. Comparison of intrapulmonary and systemic pharmacokinetics of Colistin Methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically ill patients. Antimicrob Agents Chemother. 2014;58(12):7331–7339. doi:10.1128/AAC.03510-14
32. Ram K, Sheikh S, Bhati RK, Tripathi CD, Suri JC, Meshram GG. Steady-state pharmacokinetic and pharmacodynamic profiling of colistin in critically ill patients with multi-drug–resistant gram-negative bacterial infections, along with differences in clinical, microbiological and safety outcome. Basic Clin Pharmacol Toxicol. 2021;128(1):128–140. doi:10.1111/bcpt.13482
33. Bergen PJ, Li J, Nation RL. Dosing of colistin – back to basic PK/PD. Curr Opin Pharmacol. 2011;11:464–469. doi:10.1016/j.coph.2011.07.004
34. Lin YW, Zhou QT, Cheah SE, et al. Pharmacokinetics/pharmacodynamics of pulmonary delivery of colistin against Pseudomonas aeruginosa in a mouse lung infection model. Antimicrob Agents Chemother. 2017;61(3):e02025. doi:10.1128/AAC.02025-16
35. Lin YW, Zhou QT, Hu Y, et al. Pulmonary pharmacokinetics of colistin following administration of dry powder aerosols in rats. Antimicrob Agents Chemother. 2017;61(11):e00973. doi:10.1128/AAC.00973-17
36. Tewes F, Brillault J, Gregoire N, et al. Comparison between colistin sulfate dry powder and solution for pulmonary delivery. Pharmaceutics. 2020;12(6):557. doi:10.3390/pharmaceutics12060557
37. Athanassa ZE, Markantonis SL, Fousteri MZF, et al. Pharmacokinetics of inhaled colistimethate sodium (CMS) in mechanically ventilated critically ill patients. Intensive Care Med. 2012;38:1779–1786. doi:10.1007/s00134-012-2628-7
38. Ratjen F, Rietschel E, Kasel D, et al. Pharmacokinetics of inhaled colistin in patients with cystic fibrosis. J Antimicrob Chemother. 2006;57(2):306–311. doi:10.1093/jac/dki461
39. Shetty N, Ahn P, Park H, et al. Improved physical stability and aerosolization of inhalable amorphous ciprofloxacin powder formulations by incorporating synergistic colistin. Mol Pharm. 2018;15(9):4004–4020. doi:10.1021/acs.molpharmaceut.8b00445
40. Mangal S, Park H, Zeng L, et al. Composite particle formulations of colistin and meropenem with improved in-vitro bacterial killing and aerosolization for inhalation. Int J Pharm. 2018;548(1):443–453. doi:10.1016/j.ijpharm.2018.07.010
41. Dubashynskaya NV, Skorik YA. Polymyxin delivery systems: recent advances and challenges. Pharmaceuticals. 2020;13(5):83. doi:10.3390/ph13050083
42. Gurjar M. Colistin for lung infection: an update. J Intensive Care. 2015;3(1):3. doi:10.1186/s40560-015-0072-9
43. El-Sayed Ahmed MAE, Zhong LL, Shen C, Yang Y, Doi Y, Tian GB. Colistin and its role in the era of antibiotic resistance: an extended review (2000–2019). Emerg Microbes Infect. 2020;9:868–885. doi:10.1080/22221751.2020.1754133
44. Khuntayaporn P, Thirapanmethee K, Chomnawang MT. An update of mobile colistin resistance in non-fermentative gram-negative bacilli. Front Cell Infect Microbiol. 2022;12:882236. doi:10.3389/fcimb.2022.882236
45. Bonyadi P, Saleh NT, Dehghani M, Yamini M, Amini K. Prevalence of antibiotic resistance of Pseudomonas aeruginosa in cystic fibrosis infection: a systematic review and meta-analysis. Microb Pathog. 2022;165:105461. doi:10.1016/j.micpath.2022.105461
46. Poirel L, Jayol A, Nordmann P. Polymyxins: antibacterial activity, susceptibility testing, and resistance mechanisms encoded by plasmids or chromosomes. Clin Microbiol Rev. 2017;30:557–596. doi:10.1128/CMR.00064-16
47. Band VI, Satola SW, Smith RD, et al. Colistin heteroresistance is largely undetected among carbapenem-resistant enterobacterales in the United States. mBio. 2021;12(1):e028810. doi:10.1128/mBio.02881-20
48. Liu -Y-Y, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168. doi:10.1016/S1473-3099(15)00424-7
49. Pino G, Conterno G, Colongo PG. Clinical observations on the activity os aerosol colimycin and of endobronchial instillations of colomycin in patients with pulmonary suppurations. Minerva Med. 1963;54:2117–2122.
50. Pines A, Raafat H, Siddiqui GM, Greenfield JS. Treatment of severe pseudomonas infections of the bronchi. Br Med J. 1970;1(5697):663–665. doi:10.1136/bmj.1.5697.663
51. Montero M, Horcajada JP, Sorlí L, et al. Effectiveness and safety of colistin for the treatment of multidrug-resistant Pseudomonas aeruginosa infections. Infection. 2009;37(5):461–465. doi:10.1007/s15010-009-8342-x
52. Steinfort DP, Steinfort C. Effect of long-term nebulized colistin on lung function and quality of life in patients with chronic bronchial sepsis. Intern Med J. 2007;37(7):495–498. doi:10.1111/j.1445-5994.2007.01404.x
53. Dhar R, Anwar GA, Bourke SC, et al. Efficacy of nebulised colomycin in patients with non-cystic fibrosis bronchiectasis colonised with Pseudomonas aeruginosa. Thorax. 2010;65(6):553. doi:10.1136/thx.2008.112284
54. Berlana D, Llop JM, Manresa F, Jódar R. Outpatient treatment of Pseudomonas aeruginosa bronchial colonization with long-term inhaled colistin, tobramycin, or both in adults without cystic fibrosis. Pharmacotherapy. 2011;31(2):146–157. doi:10.1592/phco.31.2.146
55. Blanco-Aparicio M, Saleta Canosa JL, Valiño López P, Martín Egaña MT, Vidal García I, Montero Martínez C. Eradication of Pseudomonas aeruginosa with inhaled colistin in adults with non-cystic fibrosis bronchiectasis. Chron Respir Dis. 2019;16:1479973119872513. doi:10.1177/1479973119872513
56. López-Gil Otero MM, Romero-Ventosa EY, Feijoo-Meléndez D, Casanova-Martínez C, Otero-Millán L, Piñeiro-Corrales G. Experience with nebulised colistin in patients with non-cystic fibrosis bronchiectasis colonised with Pseudomonas aeruginosa. Rev Esp Quimioter. 2019;32(3):217–223. doi:10.1056/NEJMra012519
57. Martínez-García MA, Olveira C, Máiz L, et al. Bronchiectasis: a complex, heterogeneous disease. Arch Bronconeumol. 2019;55(8):427–433. doi:10.1016/j.arbres.2019.02.024
58. Villar-‘Álvarez F, de la Rosa-Carrillo D, Fariñas-Guerrero F, Jiménez-Ruiz CA. Immunosenescence, immune fitness and vaccination schedule in the adult respiratory patient. Open Respir Arch. 2022;4(3):100181. doi:10.1016/j.opresp.2022.100181
59. Tabernero Huguet E, Gil Alaña P, Alkiza Basañez R, Hernández Gil A, Garros Garay J, Artola Igarza JL. Inhaled colistin in elderly patients with non-cystic fibrosis bronchiectasis and chronic Pseudomonas aeruginosa bronchial infection. Rev Esp Geriatr Gerontol. 2015;50(3):111–115. doi:10.1016/j.regg.2014.09.005
60. Martinez-Garcia MA, Miravitlles M. Bronchiectasis in COPD patients: more than a comorbidity? Int J Chron Obstruct Pulmon Dis. 2017;12:1401–1411. doi:10.2147/COPD.S132961
61. Bruguera-Avila N, Marin A, Garcia-Olive I, et al. Effectiveness of treatment with nebulized colistin in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2909–2915. doi:10.2147/COPD.S138428
62. Bruguera-Avila N, Garcia-Olive I, Marin A, et al. Microbiological progress in patients with bronchial infection with Pseudomonas aeruginosa treated with nebulised colistin. Respiration. 2019;97(6):501–507. doi:10.1159/000495069
63. Montón C, Prina E, Pomares X, et al. Nebulized colistin and continuous cyclic azithromycin in severe COPD patients with chronic bronchial infection due to Pseudomonas aeruginosa: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:2365–2373. doi:10.2147/COPD.S209513
64. de la Rosa Carrillo D, Martínez-García MÁ, Barreiro E, et al. Effectiveness and safety of inhaled antibiotics in patients with chronic obstructive pulmonary disease. A multicentre observational study. Arch Bronconeumol. 2022;58(1):11–21. doi:10.1016/j.arbres.2021.03.009
65. de la Rosa Carrillo D, López-Campos JL, Alcázar Navarrete B, et al. Consensus document on the diagnosis and treatment of chronic bronchial infection in chronic obstructive pulmonary disease. Arch Bronconeumol. 2020;56(10):651–664. doi:10.1016/j.arbres.2020.04.023
66. Martinez-Garcia MA, Miravitlles M. The impact of chronic bronchial infection in COPD: a proposal for management. Int J Chron Obstruct Pulmon Dis. 2022;17:621–630. doi:10.2147/COPD.S357491
67. Martínez-García MÁ, Oscullo G, Barreiro E, et al. Inhaled dry powder antibiotics in patients with non-cystic fibrosis bronchiectasis: efficacy and safety in a real-life study. J Clin Med. 2020;9(7):2317. doi:10.3390/jcm9072317
68. Xu F, He LL, Che LQ, et al. Aerosolized antibiotics for ventilator-associated pneumonia: a pairwise and Bayesian network meta-analysis. Crit Care. 2018;22(1):301. doi:10.1186/s13054-018-2106-x
69. Cui HM, Lin X, Liu YY, Shen YH. Comparison of different colistin regimens for the treatment of pneumonia caused by multidrug-resistant microorganisms: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25(16):5275–5292. doi:10.26355/eurrev_202108_26549
70. Elborn JS, Vataire AL, Fukushima A, et al. Comparison of inhaled antibiotics for the treatment of chronic Pseudomonas aeruginosa lung infection in patients with cystic fibrosis: systematic literature review and network meta-analysis. Clin Ther. 2016;38(10):2204–2226. doi:10.1016/j.clinthera.2016.08.014
71. Vardaka A, Mavroudis AD, Georgiou M, Falagas ME. Intravenous plus inhaled versus intravenous colistin monotherapy for lower respiratory tract infections: a systematic review and meta-analysis. J Infect. 2018;76(4):321–327. doi:10.1016/j.jinf.2018.02.002
72. Haworth CS, Foweraker JE, Wilkinson P, Kenyon RF, Bilton D. Inhaled colistin in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection. Am J Respir Crit Care Med. 2014;189(8):975–982. doi:10.1164/rccm.201312-2208OC
73. Hoon ME, Gallagher CG, Govan JRW. A randomised clinical trial of nebulised tobramycin or colistin in cystic fibrosis. Eur Respir J. 2002;20(3):658–664. doi:10.1183/09031936.02.00248102
74. Martinez-García MA, Villa C, Dobarganes Y, et al. RIBRON: the Spanish online bronchiectasis registry. characterization of the first 1912 patients. Arch Bronconeumol. 2021;57(1):28–35. doi:10.1016/j.arbres.2019.12.021
75. Prados C, Maiz L, Zamarron E, Alvarez-Sala R. Are inhalation devices important in antibiotic treatment? Arch Bronconeumol. 2020;56(12):771–772. doi:10.1016/j.arbr.2019.12.015
76. De Soyza A, Aksamit T, Bandel TJ, et al. RESPIRE 1: a Phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur Respir J. 2018;51(1):1702052. doi:10.1183/13993003.02052-2017
77. Aksamit T, De Soyza A, Bandel TJ, et al. RESPIRE 2: a phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur Respir J. 2018;51(1):1702053. doi:10.1183/13993003.02053-2017
78. Serisier DJ, Bilton D, De Soyza A, et al. Inhaled, dual release liposomal ciprofloxacin in non-cystic fibrosis bronchiectasis (ORBIT-2): a randomised, double-blind, placebo-controlled trial. Thorax. 2013;68(9):812–817. doi:10.1136/thoraxjnl-2013-203207
79. Haworth CS, Bilton D, Chalmers JD, et al. Inhaled liposomal ciprofloxacin in patients with non-cystic fibrosis bronchiectasis and chronic lung infection with Pseudomonas aeruginosa (ORBIT-3 and ORBIT-4): two phase 3, randomised controlled trials. Lancet Respir Med. 2019;7(3):213–226. doi:10.1016/S2213-2600(18)30427-2
80. Elborn JS, Blasi F, Haworth CS, et al. Bronchiectasis and inhaled tobramycin: a literature review. Respir Med. 2022;192:106728. doi:10.1016/j.rmed.2021.106728
81. Barker AF, O’Donnell AE, Flume P, et al. Aztreonam for inhalation solution in patients with non-cystic fibrosis bronchiectasis (AIR-BX1 and AIR-BX2): two randomised double-blind, placebo-controlled phase 3 trials. Lancet Respir Med. 2014;2(9):738–749. doi:10.1016/S2213-2600(14)70165-1
82. Brodt AM, Stovold E, Zhang L. Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review. Eur Respir J. 2014;44(2):382–393. doi:10.1183/09031936.00018414
83. Laska IF, Crichton ML, Shoemark A, Chalmers JD. The efficacy and safety of inhaled antibiotics for the treatment of bronchiectasis in adults: a systematic review and meta-analysis. Lancet Respir Med. 2019;7(10):855–869. doi:10.1016/S2213-2600(19)30185-7
84. Chen CL, Huang Y, Yuan JJ, et al. The roles of bacteria and viruses in Bronchiectasis exacerbation: a prospective study. Arch Bronconeumol. 2020;56(10):621–629. doi:10.1016/j.arbres.2019.12.010
85. Monsó E. Look at the wood and not at the tree: the microbiome in chronic obstructive lung disease and cystic fibrosis. Arch Bronconeumol. 2020;56(1):5–6. doi:10.1016/j.arbres.2019.04.017
86. Abo-Leyah H, Chalmers JD. Managing and preventing exacerbation of bronchiectasis. Curr Opin Infect Dis. 2020;33(2):189–196. doi:10.1097/QCO.0000000000000628
87. Posadas T, Oscullo G, Zaldivar E, et al. C-reactive protein concentration in steady-state Bronchiectasis: prognostic value of future severe exacerbations. data from the Spanish registry of bronchiectasis (RIBRON). Arch Bronconeumol. 2021;57(1):21–27. doi:10.1016/j.arbr.2019.12.022
88. Haworth CS, Shteinberg M, Winthrop KL, et al. RCT abstract - the efficacy and safety of colistimethate sodium delivered via the I-neb in bronchiectasis: the PROMIS-I randomized controlled trial. Eur Respir J. 2021;58(Suppl. 65):RCT4267.
89. National Library of Medicine (US). Trial in Non-cystic Fibrosis Bronchiectasis Patients With Chronic Lung Infections Treated With Colistimethate Sodium (PROMIS II)); [Feb 3, 2006; cited Jul 19, 2022]. Available from: https://clinicaltrials.gov/ct2/show/NCT03460704.
90. Falciani C, Zevolini F, Brunetti J, et al. Antimicrobial peptide-loaded nanoparticles as inhalation therapy for Pseudomonas aeruginosa infections. Int J Nanomedicine. 2020;15:1117–1128. doi:10.2147/IJN.S218966
91. Yu S, Pu X, Ahmed MU, et al. Spray-freeze-dried inhalable composite microparticles containing nanoparticles of combinational drugs for potential treatment of lung infections caused by Pseudomonas aeruginosa. Int J Pharm. 2021;610:121160. doi:10.1016/j.ijpharm.2021.121160
92. Chang AB, Bell SC, Torzillo PJ, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand thoracic society of Australia and New Zealand guidelines. Med J Aust. 2015;202(3):130. doi:10.5694/mjac14.00287
93. Al-Jahdali H, Alshimemeri A, Mobeireek A, et al. The Saudi thoracic society guidelines for diagnosis and management of noncystic fibrosis bronchiectasis. Ann Thorac Med. 2017;12(3):135–161. doi:10.4103/atm.ATM_171_17
94. Pereira MC, Athanazio RA, Dalcin PTR, et al. Brazilian consensus on non-cystic fibrosis bronchiectasis. J Bras Pneumol. 2019;45(4):e20190122. doi:10.1590/1806-3713/e20190122
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.