")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Informing the State of Process Modeling and Automation of Blood Banking and Transfusion Services Through a Systematic Mapping Study
Authors Elhaj SA, Odeh Y , Tbaishat D, Rjoop A , Mansour A, Odeh M
Received 26 October 2023
Accepted for publication 9 January 2024
Published 1 February 2024 Volume 2024:17 Pages 473—489
DOI https://doi.org/10.2147/JMDH.S443674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shaima’ Abdallah Elhaj,1 Yousra Odeh,1,2 Dina Tbaishat,1,3,4 Anwar Rjoop,5,6 Asem Mansour,1 Mohammed Odeh1,7,8
1Cancer Care Informatics Research, King Hussain Cancer Center (KHCC), Amman, Jordan; 2Faculty of Information Technology, Philadelphia University, Amman, Jordan; 3College of Technological Innovation, Zayed University, Dubai, United Arab Emirates; 4Library and Information Science Department, University of Jordan, Amman, Jordan; 5Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 6Department of Pathology, Blood Bank, King Abdullah University Hospital, Irbid, Jordan; 7College of Arts, Technology and Environment, University of the West of England, Bristol, UK; 8Global Academy for Digital Health, Bristol, UK
Correspondence: Mohammed Odeh, University of the West of England, Frenchay Campus, Coldharbour Lane, Bristol, BS16 1QY, UK, Tel +44 (0)117 9656261, Email [email protected] Yousra Odeh, Philadelphia University, Jarash Road, P.O.Box 19392, Amman, Tel +96 (2) 64799000, Fax +96 (2) 64799040, Email [email protected]; [email protected]
Purpose: The current state of the art in process modeling of blood banking and transfusion services is not well grounded; methodological reviews are lacking to bridge the gap between such blood banking and transfusion processes (and their models) and their automation. This research aims to fill this gap with a methodological review.
Methods: A systematic mapping study was adopted, driven by five key research questions. Identified research studies were accepted based on fulfilling the following inclusion criteria: 1) research studies should focus on blood banking and transfusion process modeling since the late 1970s; and 2) research studies should focus on process automation in relation to workflow-based systems, with papers classified into categories in line with the analysis undertaken to answer each of the research questions.
Results: The search identified 22 papers related to modeling and automation of blood banking and transfusion, published in the period 1979– 2022. The findings revealed that only four process modeling languages were reported to visualize process workflows. The preparation of blood components, serologic testing, blood distribution, apheresis, preparation for emergencies, maintaining blood banking and transfusion safety, and documentation have not been reported to have been modeled in the literature. This review revealed the lack of use of Business Process Modeling Notation (BPMN) as the industry standard process modeling language in the domain. The review also indicated a deficiency in modeling specialized processes in blood banking and transfusion, with the majority of reported processes being described as high level, but lacking elaboration. Automation was reported to improve transfusion safety, and to reduce cost, time cycle, and human errors.
Conclusion: The work highlights the non-existence of a developed process architectural framework for blood banking and transfusion processes, which is needed to lay the groundwork for identifying and modeling strategic, managerial, and operational processes to bridge the gap with their enactment in healthcare systems. This paves the way for the development of a data-harvesting platform for blood banking and transfusion services.
Keywords: blood banking, blood transfusion, blood banking process model, blood banking process automation, blood transfusion process model, blood transfusion process automation, Systematic Mapping Study, Blood Banking and Transfusion Services
Introduction
Blood banking and transfusion (BB&T) centers, having varying levels of process complexity, necessitate the qualitative and efficient operationalization of technological and system support to bridge the gap between the world of blood banking and transfusion services on the one hand, and the world of systems and technology on the other.1,2 Therefore, before developing and deploying computer-based information management systems to manage BB&T business processes, it is vital to visualize the workflow through business process modeling (BPM).3–8 Visualizing business processes using the modeling approach can help BB&T stakeholders to gain a clear understanding of the entire BB&T process.3–6 This clarity is crucial for identifying bottlenecks, gaps, risks, redundancies, and inefficiencies within the current BB&T system. Understanding and identifying risks using the BPM visualization allows blood bank centers to develop strategies for risk mitigation and compliance with safety standards.3 BPM of BB&T processes makes it easier for different stakeholders, including healthcare professionals, administrators, and IT people, to communicate effectively and thus to improve BB&T operations continuously. It also serves as a common language, facilitating discussion and collaboration among multidisciplinary teams.3,4,6
Hammer and Champy (1993) defined a business process as “a collection of activities whose final aim is the production of a specific output that is of value to the customer”.9 A business process has a goal and is affected by events occurring in the external world or in other processes. The BPM approach is used to attain visual depictions of business processes in order to gain and communicate better understanding of business processes before technologically enacting them. Therefore, BPM is considered a necessary practice to provide rapid knowledge transfer to relevant stakeholders through standardized process models, documentation and visualization for intraprocess and interprocess communications, knowledge exchange for process improvement,10,11 and information modeling of data consumed and produced by the respective processes.4–8,10,11
Over the past decade, the need to highly automate healthcare processes has been recognized by many healthcare providers, aiming to attain higher levels of efficiency, productivity, reliability, and cost-effectiveness of healthcare services.12 BB&T services are a key complex functional and operative part of the national healthcare systems, along with the increasing number of deployed BB&T national centers, and the stringent quality requirements of both timely and safe delivery of blood product to recipients. Accordingly, there are complex processes underlying BB&T, with complex relationships between them. Such processes will be modeled, communicated, improved, and validated to seek approval by the stakeholders before they can be enacted as BB&T services. However, several questions remain unanswered. Which BB&T processes have been identified in the literature and which have not? Which of these processes have been modeled, and which have not? Which processes have been automated, and to what extent has automation been achieved? These questions formed the motivation for this research. To provide scientifically informed answers to these questions, a rigorous methodological approach ought to be adopted to systematically study the state of the art in process modeling and automation of BB&T services.
In this research, we applied the systematic mapping study (SMS)13 method for studying and classifying the literature on BB&T process modeling and automation, as presented in Defining the Research Questions, followed by analysis of this SMS BB&T literature and research questions in Overview of Studies and Answering the Research Questions, respectively. A critical reflective discussion stemming from the SMS BB&T analysis of results is presented in Results and Discussion, before the conclusions are drawn in the final section, with further current and future research directions briefly conveyed.
Methods
This section describes the application of the SMS method to the process modeling and automation of BB&T services. This research is concerned with developing a systematic map of the literature related to the process modeling and automation of BB&T services. Such a literature map needs to be driven by the research questions. However, this literature map needs to be comprehensive, unbiased, and methodologically rigorous; and, thus, the outcomes of analyzing such a map are expected to draw the landscape of process modeling and automation of BB&T services, and to identify and reflect on gaps or uncovered areas, with directions for further research. Two well-known methods, the systematic mapping study (SMS)13 and the system literature review (SLR),14 are obvious contenders to embark on this process, given that the above rationale for this research anticipated the outcomes to start with. However, our research questions are broad and are aimed at discovering trends in process modeling and automation of BB&T services in general, and anticipate that the analysis of such trends could lead to solutions or directions being proposed to fill in the gaps in this research area. This explains our rationale behind embarking on the SMS method and applying it to the process modeling and automation of BB&T services.
Petersen et al define an SMS as “a method to build a classification scheme and structure a software engineering field of interest”.13 SMS is undertaken through an exhaustive search and provides analysis of all studies in the literature. In general, the SMS process is comprised of five stages or phases, having identified the research scope, which are: 1) defining the research questions, 2) developing the literature searching and keywording criteria, 3) establishing the relevance of research papers to research questions (literature repository), 4) searching for relevant papers, screening papers, and keywording of abstracts (screening), and 5) extracting data and mapping to analyze and answer the research questions.15 The adapted SMS process diagram for this research is shown in Figure 1.
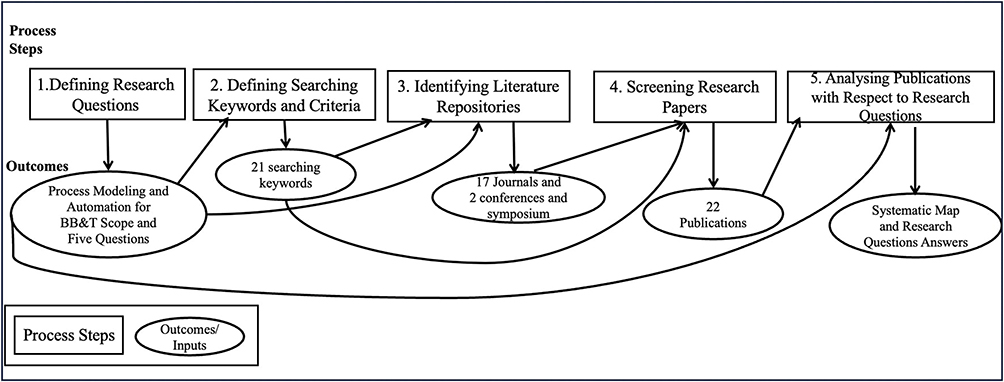 |
Figure 1 The systematic mapping study research process. |
Defining the Research Questions
Over the past few decades, the role of BPM in discovering, characterizing, diagnosing, creating, and enacting processes has been driving the development of automated workflow management systems.3 Blood banks and transfusion centers, among other key components of healthcare systems, operate critical processes including blood collection, blood processing, blood storage, and blood distribution, to produce blood components for transfusion. To date, no clear map of such BB&T processes exists to draw the landscape of which processes have been identified and modeled, and which process modeling methods and notation have been utilized. Such processes, when modeled and enacted with automation, result in complicated services involving multiple human and non-human role-players (eg, ordering physicians, nurses, lab technicians, porters, and blood donors) that do not necessarily interact in co-located spaces and may be fully geographically dispersed. Also, multiple functional procedures of BB&T processes should be enacted in the respective healthcare computer information systems to ensure the delivery of blood products to the right recipients, both qualitatively and in a timely manner. Accordingly, the following research questions have been formulated to guide the application of the adapted SMS process in relation to the process modeling and automation of BB&T services:
RQ1: Which process modeling languages and notation have been used in the process modeling and automation of BB&T services?
RQ2: Which processes of BB&T services have been modeled in the literature?
RQ3: Which BB&T processes are yet to be process modeled?
RQ4: To what extent have BB&T processes been automated?
RQ5: What are the gained impacts of process modeling and automation of BB&T services?
Defining Search and Keywording Criteria
A literature search was conducted to gather all studies on BB&T in general. Since the topic of this paper covers the two fields of “blood banking and transfusion” and “process modeling”, the derived keywords have been divided as shown in Table 1. The Boolean operators “AND” and “OR” were used in forming the search expressions.
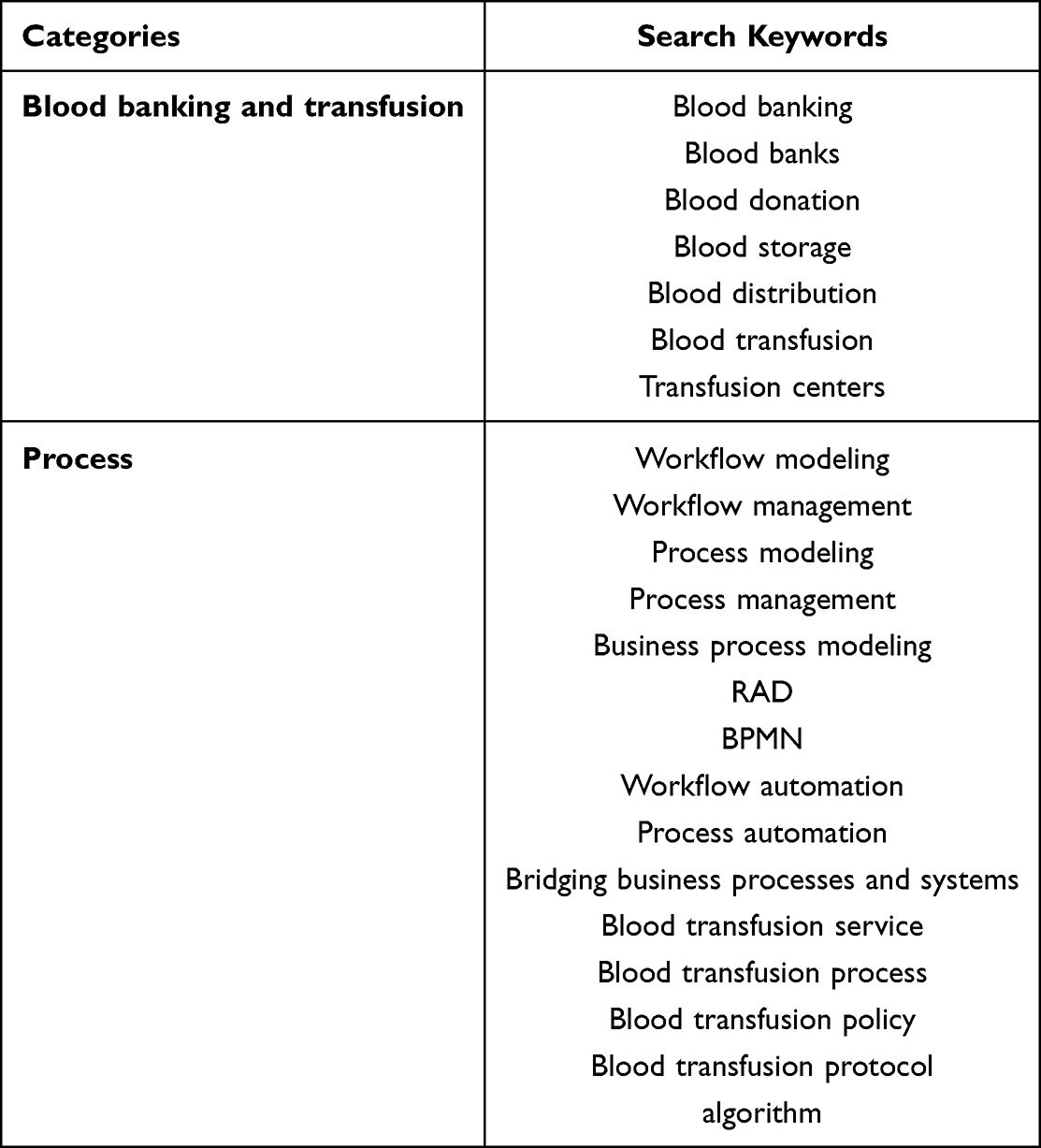 |
Table 1 Keywords Used in the Process Modeling and Automation of BB&T Services for the Systematic Mapping Study |
Identifying the Research Literature Repositories and Associated Research Papers
The development of electronic research literature repositories, along with search engines, has advanced rapidly and has yielded a set of prime electronic databases powered by electronic indexing and search engines. The most notable repositories (or databases) that combine the diverse interests in the fields of process modeling and automation of BB&T were identified to represent the electronic search space for this BB&T SMS:
- PubMed (https://pubmed.ncbi.nlm.nih.gov/)
- Web of Science (https://clarivate.com/webofsciencegroup/solutions/web-of-science/)
- IEEE (https://www.ieee.org/)
- ACM (https://www.acm.org/)
- Google Scholar (https://scholar.google.com/)
- Science Direct (https://www.sciencedirect.com/)
- Mendeley (https://www.mendeley.com/?interaction_required=true)
Furthermore, only journal papers that are indexed in Scopus and identified as being relevant to the domain of process modeling and automation of BB&T services were included. These journals are published in the English language, with a publication year between 1979 and 2022, since the interest in graphical process modeling research began to be exposed in the relevant domain in the late 1970s and early 1980s.16 The following journals were included in the systematic mapping literature search:
- Journal of Pathology Informatics
- Transfusion
- Transfusion Medicine and Hemotherapy
- Annals of Laboratory Medicine
- Annals of the Romanian Society for Cell Biology
- Anesthesia and Analgesia
- Transfusion and Apheresis Science
- American Journal of Clinical Pathology
- Laboratoriumsmedizin
- Vox Sanguinis
- Journal of the Operational Research Society
- Health Policy
- Computers in Biology and Medicine
- ACM SIGSIM Simulation Digest
- International Journal of Electronic Business Management
- Procedia Technology
- PLoS ONE
In addition, Procedia Computer Science and The International Council on Systems Engineering (INCOSE) were searched for their prime one conference and one symposium, respectively. Mendeley was used as the searching and reference management tool for this SMS.
Screening Research Papers
The screening process for assessing the relevance of papers to this research is comprised of the following:
Inclusion Criterion I
Articles that focus on BB&T graphical process modeling and/or automation since the late 1970s.
Inclusion Criterion II
Articles that focus on process automation since the late 1970s and early 1980s, when workflow-based systems started to emerge, with application to process modeling and process automation.8
Inclusion Criterion III
Articles published in Scopus-indexed journals, conferences, or symposiums.
Exclusion Criterion I
Publications that focus only on cord blood banks or general health services.
Exclusion Criterion II
Publications that discuss mathematical or stochastic modeling of BB&T processes without graphical process modeling.
Analysis of Results
Overview of Studies
The total number of papers returned after applying the searching keywords in the selected repositories was 40. After applying the inclusion and exclusion criteria mentioned in Screening Research Papers, this resulted in 18 papers being excluded and 22 papers being included in this SMS. Nine publications, representing about 41% of the overall publications, discussed process modeling without automation; 11 publications, representing 50% of the overall publications, discussed automation without process modeling; and two publications, representing about 9.1%, discussed both process modeling and automation. Figure 2 shows the subject distribution of publications on the process modeling and automation of BB&T in this SMS.
 |
Figure 2 Subject distribution in the selected publications. |
Furthermore, the number of publications and the associated percentages of publications per year of publications are presented in Table 2, which shows that studies on process modeling and automation of BB&T services have increased sharply since 1979, with a marked increase in 2007–2008, when the number of publications in the targeted subjects peaked (at three publications/year).
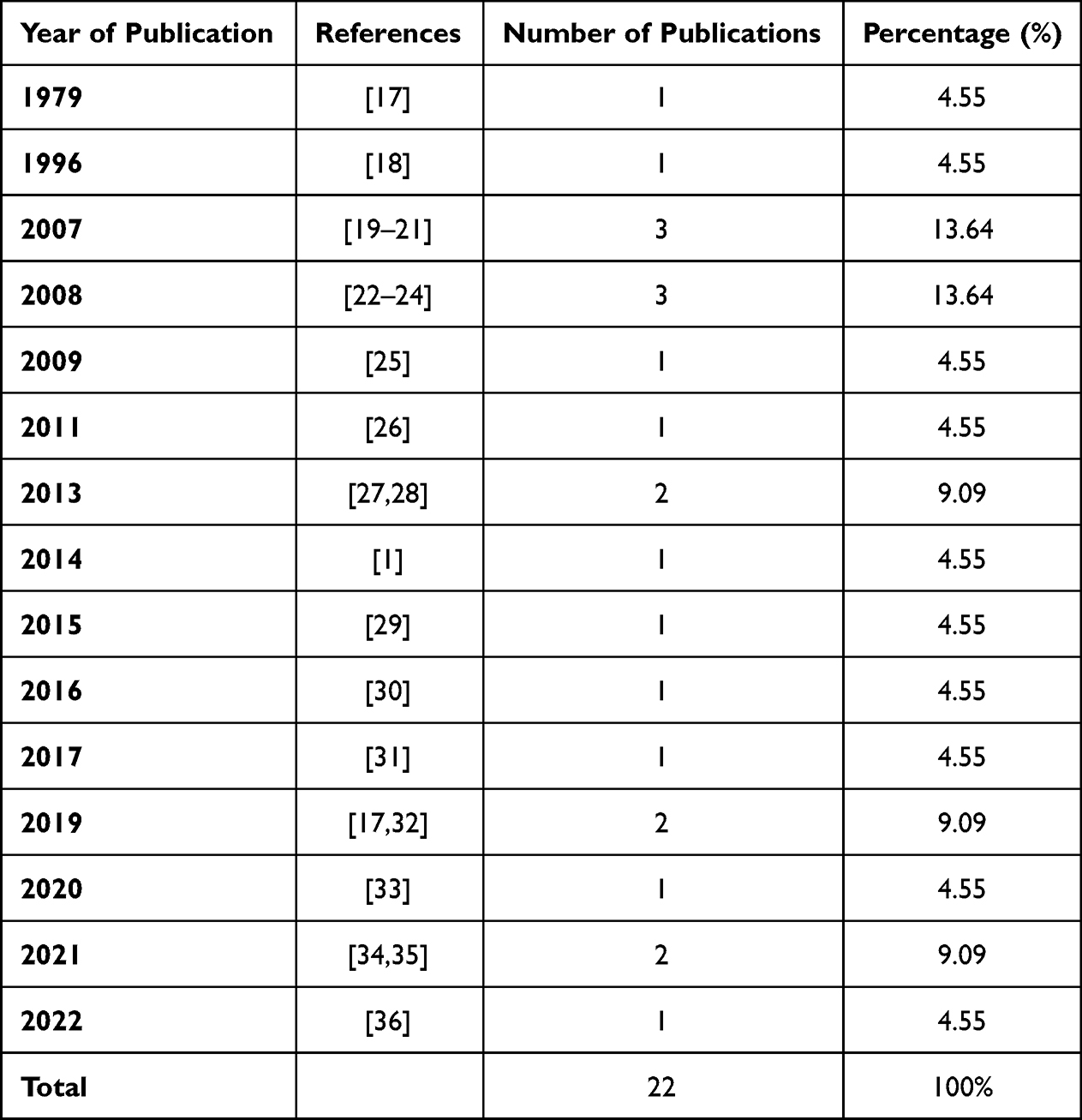 |
Table 2 Publication Tendency of Process Modeling of Blood Banking and Transfusion (BB&T) Services, Sorted by Year |
Moreover, the papers were classified according to the sources of publications, as shown in Figure 3. There were three sources of publications: journals, conferences, and symposiums. Journals were the most common source of publication, accounting for 90.90% of the total publication types, whereas conference and symposium publications covered less than 10% of the publications (4.55% each). It is logical to conclude that the interest in BB&T process modeling and automation from several journals reflects the significant role of process modeling and automation in empowering the BB&T services.
 |
Figure 3 Types of publications included in the systematic mapping study. |
Notably, most of the publications emerged from the journal Transfusion, which is associated with the Association for the Advancement of Blood & Biotherapies (AABB). This could be attributed to the large society contributing to this association, which has a distinguished role in mentoring and educating members in the field and is an accreditation body for banks internationally. This means that such leadership is important for the desired advancement in the field of BB&T process modeling and automation of services.
Answering the Research Questions
RQ1: Which process modeling languages and notation have been used in the process modeling and automation of BB&T services?
Table 3 provides the distribution of research papers and shows the details of the statistics regarding this classification. Unfortunately, most of the studies do not mention modeling languages, except for those that report on the BB&T processes modeled using four process modeling languages or notations. First, Yet Another Workflow Language (YAWL),1 an XML-based1 workflow language used for modeling business and healthcare processes, has been used to process model the fields of blood donation, processing, and transfusion.1 However, the modeled processes in YAWL are shown in high-level process modeling representation, where interactions between involved roles and their associated activities are not supported.1 Also, the notation used in YAWL is very limited. This leads to a deficiency in the representation of key BB&T process aspects necessary for modeling related workflows, especially since BB&T processes are complex, with a high level of interacting roles.
 |
Table 3 Process Modeling Languages and Notation Used for Process Modeling of Blood Banking and Transfusion (BB&T) Services |
Second, Unified Requirements Modeling Language (URML), initially reported in 2010 with a proposed meta-model, was used to model the activities, starting from the physician’s request for a blood transfusion, to collecting blood.27,37 URML37 claims to attend to two key shortcomings of earlier modeling languages such as UML and SysML, namely 1) not providing comprehensive interdisciplinary visualization of requirements and system models, and 2) the lack of integrated modeling solutions with process traceability.
In a workflow, a task can have four different states: disabled, enabled, running, or finished (DERF). DERF is the third modeling language that was proposed as a multilevel meta-modeling approach to specify a domain-related process workflow language, where its routes are specified using routing predicates and transformation rules.30 Modelers can specify their own workflow modeling language to create a common ground between all stakeholders. This provides an opportunity to enrich the specifications of healthcare processes with flexibility to enable evolution in the current area of process modeling languages. WebDPF30 was applied with an alignment of interaction design in a case study of blood transfusions, being a safety-critical operation, in associated hospitals, for the development of a simulation tool that allows users to connect between their user interfaces and track the state of execution of a blood transfusion workflow. However, updating a process metamodel in workflow language needs to be rigorously managed as it may lead to dependency and inconsistency in pairing or relating to, for instance, the BB&T concept hierarchy, which is a potential concern when adopting the WebDPF approach. For example, if concept “A” is removed from a BB&T process metamodel, then all concepts paired with “A” must be removed unless there is a set of new transformation rules, and hence the issues of dependency and consistency should be pre-emptively managed.
Fourth, Business Process Modeling Notation (BPMN),38 an industry standard in BPM (unlike WebDPF) proposed by the Object Management Group in 2010, with more than 100 predefined process notations, has not been purely adopted in modeling BB&T processes, except in 2008 and late 2018, as per the current landscape of the literature. As reported in 2008,23 BPMN was utilized to model the implementation of radio frequency identification (RFID) in relation to the analysis of blood pack handling processes for blood acquisition, blood examination, and pack inventory, which may suggest extending such work to derive related data models to inform quantitative and qualitative evaluation for the related key performance indicators (KPIs), and hence contributed to data-driven process improvement in BB&T. However, the case study was limited to the application of one process in relation to blood donation in hospitals, which is not representative enough in the virtual domain of BB&T.23 In other research, conducted in late 2018, BPMN was utilized in a cancer care center to model blood and marrow transplant (BMT) laboratory processes.7 This resulted in deriving process-based specimen states,7 with process versus states tracking, which informed the discovery of informational entities10 that can be utilized to inform the basis for developing information and data models/databases for the concerned BMT laboratory workflow. This may allow a reduction in the requirements of the engineering process cycle time, and hence the whole software development process cycle time.4 However, such a process-modeling based approach highlights the absence of a comprehensive evaluation framework for informing the completeness, correctness, and consistency of derived data entities and states for the BMT laboratory in that cancer care organization.7,10
In conclusion, BPMN,38 which is the industry standard for BPM, was, surprisingly, found not to have been widely adopted in modeling BB&T processes, let alone process blueprinting of BB&T services. In addition, no process architectural modeling of the BB&T domain has been attempted using any process architecture modeling languages, methods, or frameworks. This concludes the answer to the first research question.
RQ2: Which processes of BB&T services have been modeled in the literature?
To answer this research question, a map of modeled processes of BB&T services is presented in Table 4, classified into seven categories of process types. It is observed that nearly half of the research studies reported in this BB&T SMS were related to more than one BB&T process category, and the remaining studies encompassed a single category of BB&T workflow process. The process of “High-level model of blood bank workflow” encompassed 35% of modeled workflow processes, followed by the “Blood processing” and “Blood storage” categories, which occupied 20% and 15%, respectively, of the total modeled BB&T process.
 |
Table 4 Process Modeling of Blood Banking and Transfusion (BB&T) Services in the Systematic Mapping Study |
Regarding the individual processes in these seven process categories, “High-level model of blood bank workflow” appeared as the most frequently modeled process, followed by blood donation, cross-matching, and blood storage (10% each). Further details on the modeled BB&T processes and their categories in each of the BB&T SMS papers are detailed in Table 5. In Table 5, “Blood group” has recorded the highest percentage in the BB&T automated processes literature. It was also observed that the focus has been on critical processes with the greatest safety impact and automation potential (high-level processes). These processes are also the most strictly regulated by professional organizations; they are technical processes whose performance ought to be measured.1
 |
Table 5 Automatic Blood Banking and Transfusion (BB&T) Processes Identified in the Systematic Mapping Study |
RQ3: Which BB&T processes are yet to be process modeled?
The AABB standard, an international standard for BB&T processes, was utilized as the guide to inform which BB&T processes have not yet been modeled, stemming from answering RQ2. The following are key BB&T processes that have not been reported as process modeled in the SMS BB&T surveyed literature:
- Preparation of blood components: This is an essential blood banking process that was surprisingly identified within the category of “not process-modeled”. In this process, the donated blood is separated into different components (red blood cells, plasma, platelets, and cryoprecipitate) through several steps using different methods.2 Blood bank technicians typically use centrifugation for separation; however, apheresis is used in some cases.2 Some other activities may also be performed in this process, depending on the diseases of the patients receiving the transfusion. This critical process encompasses several activities, such as filtration and irradiation, which are aimed at reducing the number of leukocytes in the blood or inactivating them, or aimed at decreasing transfusion reactions, especially in immunocompromised patients.2,40,41
- Serologic testing: This embodies a set of testing procedures with reference to serologic testing, the pathways of rejection of infected blood, and communication with an infected blood donor. These tests have not been reported as process-modeled despite being critical health and safety requirements for blood donor screening, and of critical concern for informing the existence of most common transfusion-transmitted infections in the donor blood samples.2 The tests required during the screening of infections vary worldwide depending on the epidemiologic status of each country. In Jordan, for instance, these tests are conducted to detect HBsAg, anti-HBc, anti-HCV, HIV, and syphilis.42
- Blood distribution: The SMS BB&T surveyed literature focused on modeling the technical parts of this process category, ignoring the strategic and managerial dimensions in BB&T centers. The strategic and managerial dimensions of this process involve managing transporting blood components from blood banks to the patients, who can be in other departments, hospitals, or health institutions, and transporting blood from the main distribution centers to peripheral blood banks. This transportation must strictly follow formal policies and instructions to ensure that blood units are safely conserved and delivered to the right patient, taking into consideration changes in the atmospheric temperature or any other factors during transportation.43
- Apheresis: This is a significant process involved in separating and collecting one blood component from whole blood, while returning the remaining blood components to the donor or the patient’s bloodstream using an automated apheresis machine.2
- Preparation for emergencies: This process relates to planning and managing internal disasters such as fire and smoke, as well as external disasters such as earthquakes.44
- Maintaining BB&T safety: This is a quality control process that is concerned with defining, applying, and monitoring safety metrics, and other quality measures and procedures.44
- Documentation: This process is concerned with capturing all essential information required to properly guide and operate BB&T processes and services.44
Given the above findings regarding the missed BB&T modeled processes compared to the highly comprehensive processes for BB&T documented in the 33rd edition of Standards for Blood Banks and Transfusion Services (BBTS Standards), published by AABB,44 several concerns arise, as follows. First, the AABB BBTS Standards comprise a large number of BB&T processes that are not widely reported in an automation context or designed in the form of process models in the BB&T literature. This indicates shortcomings in the current BB&T literature with regard to BPM and automation. Second, there is missing evidence clearly demonstrating BB&T processes at different levels of abstraction and operative dimensions from strategic, managerial, and operational sides in this SMS, even through the AABB BBTS Standards. For instance, according to the AABB BB&T requirements, BB&T should have emergency operation policies, processes, and procedures in place to respond to the effects of internal and external disasters,44 which is a requirement for emergency preparedness. However, there are no details provided on the operational, management, or strategic fronts. If this process is to be automated, then more links to related key processes, such as testing for infectious diseases and donor recruitment, will need to be established. These connections might have affected how the world responded to the recent COVID-19 outbreak, which caused a global blood shortage. This further reinforces the finding in this SMS that a BB&T process architecture is needed to methodologically model and develop a comprehensive blueprint depiction for BB&T processes (at different levels of abstraction and operative dimensions) and showing their interdynamic relationships.
RQ4: To what extent have BB&T processes been automated?
Automating the BB&T processes refers to the implementation of advanced technologies and software systems to run and optimize some aspects of BB&T management that cover operations or tasks from donation to transfusion.
Applying the SMS process to the BB&T literature in this research led to the identification of six process categories (blood donation, blood processing, infection screening, blood storage, blood transfusion, post-transfusion, and administrative processes) with reference to automation of BB&T processes, where each process automation category embodies several related processes along with their associated goals. The modeled BB&T processes in the SMS BB&T literature (resulting from answering RQ2) appear to have been automated. However, such automation appeared fragmented and was only applied to some activities of some key reported SMS BB&T processes. For example:
- The registration of specimens and printing tags for blood samples are activities of the blood donation process are yet to be fully automated.26
- The process of blood processing, including automatic activities such as group typing, subgroup typing, antibody screening, cross-matching, results entry, results reporting, and sending screening results from the laboratory to the blood bank, is yet to be fully automated.18,19,26,28,29,32,34,35,39
- The process of blood storage is commonly discussed in the literature, especially the automation of controlling the availability of blood units, checking the site of storage, and controlling the temperature of refrigerators.26,35
- The process of blood transfusion automation has also been discussed in the literature. This has been achieved by automating the entry and inquiry of electronic test orders, reading the identity of patients from their wristbands, verifying the matching of patient identity with the prescribed blood product, and calculating the number of ordered units.26,30,36
- The last BB&T process that has been automated is the administrative process that includes tracking, workflow management, control of workstation quality, and real-time monitoring.26,36
Although it appears that significant efforts have been exerted to automate core BB&T processes, there are still BB&T processes that have not been process modeled, as deduced from answering RQ3, yet automated processes were represented in solo systems (ie, no computer information system has been largely developed to automate the total BB&T process, as per the AABB44 guidelines), for example, the Ortho AutoVue® for blood processing and the VISION Max system for cross matching.29,35 However, a comprehensive system to automate BB&T processes may not rationally be possible to achieve in the absence of a blueprint of BB&T processes (or a process architecture) to incorporate strategic, management, and operative dimensions of the BB&T domain.
RQ5: What are the gained impacts of process modeling and automation of BB&T services?
BB&T process modeling and automation contributed to addressing a set of critical quality requirements, as shown in Table 6, with citations to literature sources. Table 7 depicts the distribution of the automation and non-automation of BB&T process modeling, with a reflective analysis of the literature discussed below.
 |
Table 6 Gained Impact of Process Modeling and Automation of Blood Banking and Transfusion (BB&T) Processes |
 |
Table 7 Percentage of Process Modeling and Automation of Blood Banking and Transfusion (BB&T) Processes |
Significant findings have been reported in the literature with regard to improving the reliability of BB&T processes.19,26,29,32,36 Reliability in a blood bank means “ensuring that the right patient receives the right amount of the right blood component at the right time”.26 Workflow modeling has assisted in highlighting current activities of blood banks, with delays in delivering blood to site for transfusion in emergency situations. This pitfall can cause further problems in relation to overordering and overstocking to guarantee the availability of blood for transfusion under emergency conditions.19,26 Therefore, automation of the remote release of unmatched blood was implemented as a functional unit in virtual blood banks, which allows immediate allocation of compatible blood. This is associated with real-time monitoring and controlling capabilities of the blood inventory.26 A virtual blood bank is an online platform that runs an information technology-based system that keeps track of donations, transfusions, and blood inventory. Through the automation of processes such as donor management, blood testing, blood distribution, sample tracking, and transfusion management, it helps healthcare organizations to optimize the BB&T processes.26 Automation has enhanced the bidirectional traceability and reporting of inventory cassette records regarding their expiry date, availability, interpretation of results, and validation.29 Bar codes and computer-based systems have contributed to reducing human errors during labeling and data transcription.26,29,36 Also, automated algorithms have enhanced the execution of standard procedures and interpretation of results which, in turn, have led to stronger safety systems in blood banks.26,29,36 Moreover, automation has contributed to improving transfusion safety.29 Systems have been implemented for analyzing and improving blood bank processes. For example, the Ortho AutoVue Innova is an automated analyzer for blood banks that has resulted in 45% faster reporting time than manual procedures.29 Another example is the VISION MAX system; the first attempt to operate this system resulted in a 97.9% concordance rate between manual and automatic cross-matching.32 Also, automatic cross-matching resulted in a shorter turnaround time (from 23.3 min to 19.1 min) and lower risk priority number (from 1435 to 229), with reduced errors. The test cost per unit was reduced from 2.70 USD to 1.44 USD.32
With regard to improving cost-effectiveness in BB&T processes, several researchers have reported their findings.22,23,25,28,32 Workflow analysis has contributed information about decreasing costs and time cycles after automating manual methods. For example, the RFID technology was utilized in handling blood pack product supply processes.23,25 Noticeable cost effectiveness is reported in the reduction of direct labor costs, and operation time for the work of ABO/Rh(D) typing and unexpected antibody screening.28 Process models in blood product pack supply were designed, for example using BPMN,23 and employed to analyze, identify pain points, and re-engineer the existing processes to demonstrate the use of RFID in future processes.23,25 In another work, automating BB&T processes led to significant improvements in process effectiveness with regard to increasing throughput and safety, and reducing labor costs.23,25 Such results contribute to information on compliance with service-oriented architecture principles in information systems, and are anticipated to serve as a reference blueprint guideline for further development in blood product pack handling.23 Cost reduction is feasible to increase return on investment cost in the blood bank payback period and hence to enrich investment plans.25
Based on using computer simulation models to inform cost-effective management practices in blood banks, researchers22 have highlighted the need for: 1) hospitals to revisit their policies in blood unit ordering, reservation, scheduling, and delivery; and 2) cost-effective management practices in blood bank processes through the integration of policies from different blood bank centers.
Another necessary cornerstone BB&T quality requirement is adherence to and compliance with policies.24,26,34 BPMs and automation have assisted in ensuring the compliance of complex BB&T processes with their respective guidelines and regulations. For example, in virtual blood banks, BB&T domain experts employed BPMs to design a workflow model of the essential activities in relation to the development of the process of remote release of unmatched blood.26 This model contributed to informing estimates of transfusion turnaround time of these activities before and after the operation of the remote release, which resulted in reducing associated risks, blood wastage, and time-lag, and increasing resource utilization aligned with requirements in policies.26 As a result of such automation, clinicians were informed about the progress of antibody screening in a timely fashion. This contributes to reducing the demand for unmatched blood and facilitates timely decision making in emergency transfusion situations.
Furthermore, various technologies were adopted and reported in automating one of the complex BB&T processes, namely blood processing. As blood processing requires repetitive, time-consuming steps, human error is the most highly safety-critical requirement to avoid in preparing blood components. Automation contributes to increasing efficiency through reducing procedural errors that are usually generated because of manuals steps followed by humans. Also, automation contributed to reducing the blood component processing time from respective units.34 Flowcharts were used to specify and simulate the demand and supply-related processes in hospital blood banks, which are described as stochastic in nature.24 The use of flowcharts, as a tool to represent a business process, informed the extent of meeting policies in front-office existing systems. These flowcharts contributed to deriving decision rules that were evaluated in terms of cost to optimize the selection of inventory level, distribution policy, resource allocation, and supply shortages due to poor management in scheduling. One outcome of this was the suggestion to revisit policies that involve variable factors in relation to compliance with policies.24
Results and Discussion
Although BB&T is a rich domain in the literature, with significant research articles in many of its related subfields, this SMS applied to process modeling and automation of BB&T services revealed only 22 journal, conference, and symposium articles. Accordingly, this draws on the underdevelopment in the field of process modeling and automation of BB&T services. Such an assertion has been demonstrated by the absence of process modeling of key BB&T processes, such as preparation of blood components, serologic testing, blood distribution, apheresis, preparation for emergencies, maintaining BB&T safety, and documentation. These are notable examples of health and safety-critical process-related requirements that have not been modeled; and hence, this raises the concerns regarding the missed impact of process validation through BPM for better process improvement and automation support. Consider, for example, the process of “preparation of blood components”, which involves separating the components of the whole blood into packed red blood cells, fresh frozen plasma, and cryoprecipitate. These represent the final products that are used in the transfusion process. Not only that, but this process includes significant activities such as filtration and irradiation that are required to reduce the leukocytes in the blood to avoid transfusion reactions, especially in cancer patients.2 This is further evidence of the significance of such findings relating to process modeling validation, management and control, automation, quality management, etc.
Furthermore, this SMS revealed the diverse utilization of BPM notation; and among the 22 SMSs, only one study followed BPMN,40 the industry standard BPM language that also allows BPMN process models to be translated to or enacted as web services using WS-BPEL Web-Services Business Process Execution Language.23 The use of BPMN would increase the degree of automation of BB&T processes to enable concerned stakeholders to monitor the execution of process flows to improve attainment of the quantitative and qualitative BB&T specified KPIs. This provides a direction for the BB&T community to orchestrate efforts and educate their community research groups to make substantial shifts in utilizing BPMN as the process modeling language for BB&T processes, in a step towards bridging the gap between the world of BB&T and the individual healthcare systems, which are very widely geographically dispersed.
Although this SMS revealed a substantive set of BB&T modeled processes, such as blood donation, processing, storage and distribution, transfusion, and post-transfusion, only one research study reported the utilization of BPMN as the industry standard for BPM.23 That paper modeled the storage process based on a specific information management approach, and resulted in the inclusion of activities related to other processes, such as cross-matching, which is related to blood processing. On the other hand, modeling the monitoring of refrigerator temperature, which is a critical activity in blood storage, was missed in that study.23
Furthermore, BB&T process modeling and automation is increasingly being adopted as an approach for optimizing BB&T processes and improving the quality of blood products with higher safety levels and compliance with protocols and policies.26,34 BB&T process modeling can be extended to evaluate the potential benefits and costs of extending the lifetime of blood, aligned with predicting the impact of blood shortages, under central managerial control.24 A further noticeable impact of BB&T process modeling and automation has been observed in relation to the role of applying a requirements engineering approach to the BB&T domain without being formally mentioned as an approach. For example, the activity of requirements elicitation was accomplished by experts in the domain identifying hazard-driven mitigating requirements to show how problems can be addressed by the respective BB&T actors,27 with identified hazards to respective use cases and mitigating requirements.
Moreover, communication between multidisciplinary teams can be improved because BPM creates a common workflow language without delving into systems and software engineering languages and technologies, for example when BB&T domain specialists need to relate which step in a BB&T practical transfusion process requires specific automation services.
Besides the above, BB&T process modeling may be utilized in educating and training specialists involved in BB&T-related complex processes, for example, in explaining a transfusion medicine billing guide.31
Finally, analysis of the results of this SMS on BB&T process automation revealed that most of the modeled processes have been automated, from blood donation registration to post-transfusion. However, this automation is fragmented, which implies fragmented BB&T workflows processes. This aligns with the observations of Wittmann et al,19 Dada et al,39 and Shin et al,28 who discussed the automation of several activities of blood processing (genotyping, cross-matching), whereas Cheng and Wilkinson29 and Chung et al,32 for example, discussed the automation of only one activity of blood processing (cross-matching). Therefore, these fragmented views of automation need to reflect on the absence of both reference BB&T process models and an integrated framework linking these processes together. BB&T automation can have significant impacts on the quality management of the BB&T processes and services by eliciting the quality requirements, improving the quality of the processes, and improving adherence to policies and guidelines. Owing to the high volume of labor and potential for human error, busy blood banks can put patient safety at risk. Automation performs consistently, decreases the need for labor, and eliminates human manual errors. In addition, automation helps to maintain a balance between personalization in patient care and standardization.45,46 However, there is still a large gap in identifying holistic BB&T processes, their relationships, and their association with the whole quality requirements of these processes, such as usability and portability, metrics and KPIs, let alone the limited types of quality requirements reported in the literature, such as reliability, safety, efficiency, and cost-effectiveness.
Conclusion
This paper has reported on the research undertaken to inform the current state of process modeling and automation of BB&T services using a methodological research design driven based on the SMS method. This resulted in only 22 research articles that fulfilled the orchestrated SMS research process with a set of search and keywording criteria, inclusion and exclusion criteria, and a set of five research questions to direct drawing the landscape of process modeling and automation of BB&T services. This landscape has been portrayed with the non-existence of a holistic blueprint of BB&T processes, within a process architectural framework, where BB&T processes are methodologically identified and network-modeled, along with their associated interrelationships.
Such a process architectural framework lays the groundwork for future research on identifying and modeling the strategic, managerial, and operational processes for bridging the gap between BB&T processes and their enactment in corresponding healthcare systems. This, however, is anticipated to develop a data harvesting and analytics platform for BB&T services, to be reflectively optimized from the incremental execution of BB&T process cycles from inception to completion. Therefore, a virtual organizational model of the processes of BB&T services appears to be a necessity to bridge the gap between such virtual process architectural organizational models (spanning geographically dispersed locations of healthcare systems) and the enactment of their computer-based systems to achieve higher degrees of automation, for a consequent optimization of BB&T processes and their automated services. Virtual organizational models help in representing and structuring the integration of complex BB&T interconnected processes that should share information through computer-based systems.26 For example, the automation of these complex processes within a virtual organization facilitates monitoring blood inventory, tracking donor information to ensure the safety of blood products, and reducing human errors.
A further corollary of this SMS is that the field of process modeling and automation of BB&T services is far from being developed; there is an absence of process modeling of key BB&T process categories such as “Preparation of blood components”, “Serologic testing”, and “Blood distribution”, as notable examples of missing critical health-and-safety process requirements.
Furthermore, the BB&T process modeling research output has demonstrated the deviation of the BB&T research community from the BPMN industry standard of process modeling, as only one of the 22 studies utilized BPMN. This reflects on the loss of standardized mapping of BPMN models to further standard environments such as WS-BPEL, with automatic generation of BB&T web services for the automatic monitoring and controlling of BB&T processes.
Acknowledgments
The authors are grateful to King Hussain Cancer Centre, Amman, Jordan, Philadelphia University, Amman, Jordan, Zayed University, Dubai, UAE, University of Jordan, Amman, Jordan, Jordan University of Science and Technology, Irbid, Jordan, King Abdullah University Hospital, Irbid, Jordan, and Global Academy for Digital Health, UK for research support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, writing, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article will be submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grants from any party or sector.
Disclosure
This study was conducted prior to the development of the Process Architectural Framework for Blood Banking and Transfusion (PArch.BB&T), filed as patent number (JO-P-2023-103) at the Jordanian Patent Office, part of the Ministry of Industry and Trade. The authors declare that the research was conducted in the absence of any commercial or financial relationships. The authors report no conflicts of interest in this work.
References
1. Hazzazi N, Wijesekera D, Hindawi S. Formalizing and Verifying Workflows Used in Blood Banks. Procedia Technol. 2014;16:1271–1280.
2. Harmening D. Modern Blood Banking & Transfusion Practices.
3. Ould M. Business Process Management. Swindon, UK: BCS; 2018.
4. Odeh M, Kamm R. Bridging the gap between business models and system models. Inf Software Technol. 2003;45:1053–1060.
5. Tbaishat D, Odeh Y, Tbakhi A, Odeh M Deriving Object-based Business Process Architectures Using Role-based Business Process Models: a Reverse-Engineering Approach Applied to the Cell Therapy and Applied Genomics in a Cancer Care Organisation. In:
6. Odeh Y, Tbaishat D, AlOkaily A, et al. Informing Business Process Models Adherence to Protocols via Business Process Modelling: the Case of Cell Therapy and Applied Genomics in Cancer Care. In:
7. Odeh Y, Tbaishat D, Sharma S, Aburub F, Tbakhi A, Odeh M Using Business Process Models to Inform Deriving State Transition Diagrams: applied to BMT Lab in a Cancer Organization. In:
8. Odeh Y, Green S, Odeh M Deriving Goal-Oriented Models from Business Process Models: applied to Cancer Care Organization. In:
9. Hammer M, Champy J. Reengineering the Corporation.
10. AbuRub F, Tbaishat D, Odeh Y, Odeh M, Deriving Information Needs from Process Models: the Of Cell Therapy and Bone Morrow Transplant Workflow in Cancer Care Organisation. In:
11. AbuRub F, Odeh M, Beeson I. Modelling Non-Functional Requirements of business Processes. Inf Software Technol. 2007;49(11–12):1162–1171. doi:10.1016/j.infsof.2006.12.002
12. Mohapatra S. Business Process Automation. New Delhi: PHI Learning Private Limited; 2009.
13. Petersen K, Feldt R, Mujtaba S, Mattsson M Systematic mapping studies in software engineering. In:
14. Littell J, Corcoran J, Pillai V. Systematic Reviews and Meta- Analysis. New York, USA: Oxford University Press; 2008.
15. Fauzi SSM, Bannerman PL, Staples M Software Configuration Management in Global Software Development: a Systematic Map. In:
16. Johannesson P, Perjons E. Design Principles for Process Modelling in Enterprise Application Integration. Inform Syst. 2001;26(3):165–184. doi:10.1016/S0306-4379(01)00015-1
17. Krog G, Rieneck K, Clausen F, Steffensen R, Dziegiel M. Blood group genotyping of blood donors: validation of a highly accurate routine method. Transfusion. 2019;59:3264–3274.
18. Cheng G, Chiu D, Chung A, et al. A Novel System For Providing Compatible Blood To Patients During Surgery: “Self-Service” Electronic Blood Banking By Nursing Staff. Transfusion. 1996;36:347–350. doi:10.1046/j.1537-2995.1996.36496226151.x
19. Wittmann G, Frank J, Schramm W, Spannagl M. Automation and Data Processing with the Immucor Galileo® System in a University Blood Bank. Transfusion Med Hemother. 2007;34:5.
20. Katsaliaki K, Brailsford SC. Using Simulation To Improve The Blood Supply Chain. Journal of the Operational Research. Society. 2007;58:219–227.
21. Li BN, Chao S, Chui Dong M. SIBAS: a Blood Bank Information System And Its 5-Year Implementation At Macau. Computers in Biology and. Medicine. 2007;37:588–597.
22. Katsaliaki K. Cost-effective practices in the Blood Service Secto’r. Health Policy. 2008;86:2–3. doi:10.1016/j.healthpol.2007.11.004
23. Chiang J. An Investigation of Business Process Management on the application of RFID ~ On the Case of Medical Blood Pack Handling. Int J Electronic Business Manage. 2008;6:174–183.
24. Cohen MA, Pierskalla WP. Simulation of blood bank systems. ACM SIGSIM Simulation Digest. 1979;10:14–18.
25. Davis R, Geiger B, Gutierrez A, Heaser J, Veeramani D. Tracking Blood Products In Blood Centres Using Radio Frequency Identification: a Comprehensive Assessment. Vox Sanguinis. 2009;97:50–60. doi:10.1111/j.1423-0410.2009.01174.x
26. Wong K. Virtual Blood Bank. J Pathol Informatics. 2011;16. doi:10.4103/2153-3539.78039
27. Berenbach B, Rea D, Schneide F Process Modelling For Requirements Engineering: a Medical System Case Study. In:
28. Shin K, Kim H, Chang C, Lee E. Economic And Workflow Analysis Of A Blood Bank Automated System. Ann Lab Med. 2013;33(4):268–273. doi:10.3343/alm.2013.33.4.268
29. Cheng YW, Wilkinson JM. An Experience Of The Introduction Of A Blood Bank Automation System (Orth:O Autovue Innova) In A Regional Acute Hospital. Transfus Apheresis Sci. 2015;53:58–63. doi:10.1016/j.transci.2015.03.007
30. Barendregt R, Lamo Y, Rabbi F. A Bottom-up Approach for Synchronous User Interaction Design and Workflow Modelling. Procedia Comput Sci. 2016;98:340–347. doi:10.1016/j.procs.2016.09.051
31. Jhang J, Francis R, Winkler A. How do we perform and bill for blood bank physician consultative services? Transfusion. 2017;57:2311–2318. doi:10.1111/trf.14264
32. Chung H, Hur M, Choi S, et al. Benefits of VISION Max automated cross-matching in comparison with manual cross-matching: a multidimensional analysis. PLoS One. 2019;14(12):12. doi:10.1371/journal.pone.0226477
33. Jalali A, Lonsdale H, Zamora L, et al. Machine Learning Applied to Registry Data: development of a Patient-Specific Prediction Model for Blood Transfusion Requirements During Craniofacial Surgery Using the Pediatric Craniofacial Perioperative Registry Dataset. Anesthesia Analg. 2020;132:160–171.
34. Aliaga P, Labata G, Aranda A, et al. Improvement of blood processing and safety by automation and Pathogen Reduction Technology. Transfusion Med Hemother. 2021;48:5.
35. Kiruthika S, Sakthi P, Kaviya M. Blood Bank Monitoring and Blood Identification System Using Iot Device. Annals of the Romanian Society for Cell. Biology. 2021;25:182–192.
36. Passwater M, Huggins YM, Delvo Favre ED, Mukhtar F, Pelletier JP. Adding automation and independent dual verification to reduce wrong blood in tube (WBIT) events. Am. J. Clin. Pathol. 2022;158(2):212–215. doi:10.1093/ajcp/aqac031
37. Helming J, Koegel M, Schneider F, et al. Towards a Unified Requirements Modeling Language. In:
38. Object Management Group. BPMN 2.0 (2010). Available from: https://www.omg.org/spec/BPMN/2.0/About-BPMN.
39. Dada A, Beck D, Al Amiri A, Huver K. Management Of Immunohaematological Testing And Workflow Using Automated Technologies In Routine Blood Banks. LaboratoriumsMedizin. 2008;32:70–77. doi:10.1515/JLM.2008.016
40. Bahar B, Tormey C. Prevention of Transfusion-Associated Graft-Versus-Host Disease With Blood Product Irradiation: the Past, Present, and Future. Archives of Pathology & Laboratory. Medicine. 2018;142:662–667.
41. Shapiro M. The filter blood or universal leukoreduction: what is the answer? Crit Care. 2004;8(Suppl 2):27. doi:10.1186/cc2453
42. Ministry of Health. Home page - Ministry of Health; 2021 Available from: http://moh.gov.jo/Pages/viewpage.aspx?pageID=288.
43. World Health Organization. Design Guidelines for Blood Centers. Switzerland: World Health Organization Regional Office for Western Pacific; 2010.
44. American Association for the Advancement of Blood and Biotherapies (AABB). Standards for Blood Banks and Transfusion Services; 2018.
45. Gupte SC. Automation in Blood Centre: its impact on Blood Safety. Asian J Transfus Sci. 2015;9:S6–S10.
46. Pérez Aliaga AI, Labata G, Aranda A, et al. Improvement of blood processing and safety by automation and pathogen reduction technology. Transfusion Med Hemother. 2021;48:290–297. doi:10.1159/000516696
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.