Back to Journals » Patient Preference and Adherence » Volume 19
Influencing Factors of Exercise Behavior in Patients with Type 2 diabetes:A Systematic Review of Qualitative Studies
Received 9 July 2025
Accepted for publication 21 October 2025
Published 5 November 2025 Volume 2025:19 Pages 3435—3451
DOI https://doi.org/10.2147/PPA.S552727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Zhu Han, Li Wang
School of Nursing, Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning, People’s Republic of China
Correspondence: Li Wang, School of Nursing, Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning, People’s Republic of China, Email [email protected]
Background: Exercise is an critical component of diabetes health management. Long-term regular exercise can improve blood glucose levels and prevent or control diabetes-related complications. When facing exercise decision-making, patients are often full of confusion and hesitation, and may refuse to participate, thus affecting the effect of blood glucose control.
Purpose: The objective of this review was to systematically evaluate and integrate qualitative research on factors influencing exercise behaviour and exercise experience in diabetes patients to provide references for formulating management strategies to improve patients’ exercise compliance.
Patients and Methods: PubMed, Web of Science, Embase, PsycINFO, CINAHL, Scopus, CNKI, VIP, Wanfang and SinoMed were searched for qualitative studies or mixed methods studies concerning qualitative research on exercise influencing factors or experience in diabetes patients from the establishment of the database to March 2025. The quality evaluation of the included studies was critically conducted using an established tool after study selection.And then extract and analyse the data, using a systematic review and thematic synthesis approach to analyse the data.
Results: A total of 32 studies were included, using thematic analysis, 11 interrelated themes were identified. Among them, exercise stimulates positive emotions and makes exercise a habit; perceiving the benefits of exercise; external support system; correct understanding of exercise; suitable exercise mode serves as promoting factors, obstacle factors including limitations due to personal conditions or concerns about adverse events caused by exercise; lack of knowledge related to exercises or misconceptions about it; being restricted by external conditions; incomplete support system; personal emotions and psychosocial factors; cultural restrictions and other reasons.
Conclusion: The influencing factors of exercise behavior are complex and have a profound impact on patients’ exercise compliance. Medical staff should clarify the four core dimensions that affect patients’ exercise behavior, enhance patients’ exercise-related knowledge through health education and other methods, encourage patients to choose exercise methods that are suitable for themselves, and encourage family members or peers to participate with patients, and promote patients’ active participation in exercise by exerting their autonomy, thereby achieving more ideal health outcomes.
Keywords: diabetes mellitus, exercise, qualitative research, systematic review
Introduction
Diabetes is one of the fastest growing global medical emergencies in the 21st century. Type 2 diabetes (T2D) accounts for more than 90% of all diabetic patients.1 Diabetes raises the risk of microvascular compliance as well as macrovascular compliance.2 Diabetes and the associated compliance also reduce people’s quality of life.3 As a result, T2D, a disease with a high incidence rate, poses a serious threat to people’s physiology and psychology, as well as a significant societal burden.
Physical activity increases insulin sensitivity by enhancing free fatty acid oxidation, skeletal muscle mitochondrial function, and serum adiponectin levels.4,5 Exercise also helps the body produce irisin, which can work on the muscles, liver, and adipose tissue of the human body, so improving blood glucose control.6 However, since many patients are affected by multiple factors, the exercise participation rate among T2D patients is still at a low level. They demonstrate a poor willingness to engage in the initial test as well as difficulty adhering to regular exercise over time. Related research found that more than 96% of patients with T2D had fewer than 2 times of physical activity per week.7 Only 23.8% of persons with diabetes met aerobic, 10.9% met muscle-strengthening, and 6.2% met both physical activity guidelines.8 Consequently,the proportion of long-term exercise adherence still needs to be improved.
Although there have been many qualitative research on the experience of exercise decision-making. For example, Crews et al9 summarized the many factors that affect patients’ exercise behavior, but most of them were cross-sectional studies. Maudet-Coulomb et al10 clarified the positive effects of various exercise interventions on patients’ physical activity levels, physiological indicators, self-efficacy, and other psychological aspects. Whereas quantitative studies focus on correlations, qualitative research is crucial for designing patient-centered interventions as it uncovers lived experiences and complex decision-making processes. Meanwhile, there has been no systematic review on the factors that promote or hinder patients’ exercise in everyday life. In order to systematically explain the experience and cognition of T2D patients’ exercise decision-making, thoroughly analyze the reasons why patients refuse to exercise or find it difficult to maintain exercise, and summarize the experiences of successful persisters, this study employs a systematic review and thematic synthesis method to integrate and analyze pertinent qualitative interview.This study can provide valuable references for the development of targeted exercise intervention strategies in clinical practice.
Materials and Methods
Search Strategy (Figure 1)
Figure 1 presents the article selection.The research strategy incorporated three concepts of interest: (1) Type 2 Diabetes Mellitus; (2) exercise or physical activity; (3) qualitative studies. Boolean terms (AND/OR) were used to combine medical subject headings (MeSH) terms and other keywords. Firstly, identified MeSH terms, and then researched papers across different databases, the electronic research strategy was (qualitative research OR qualitative* OR experience OR feelings OR interview OR phenomeno* OR ethnographic research OR grounded theory) AND (exercise OR training OR physical activity OR exercis*) AND (diabetes mellitus OR diabetes). The search method was adapted to fit each database. The search strategy had no year limit, but it was confined to studies published in English or Chinese. All references were imported into EndNote 21 to check for duplication and relevancy.
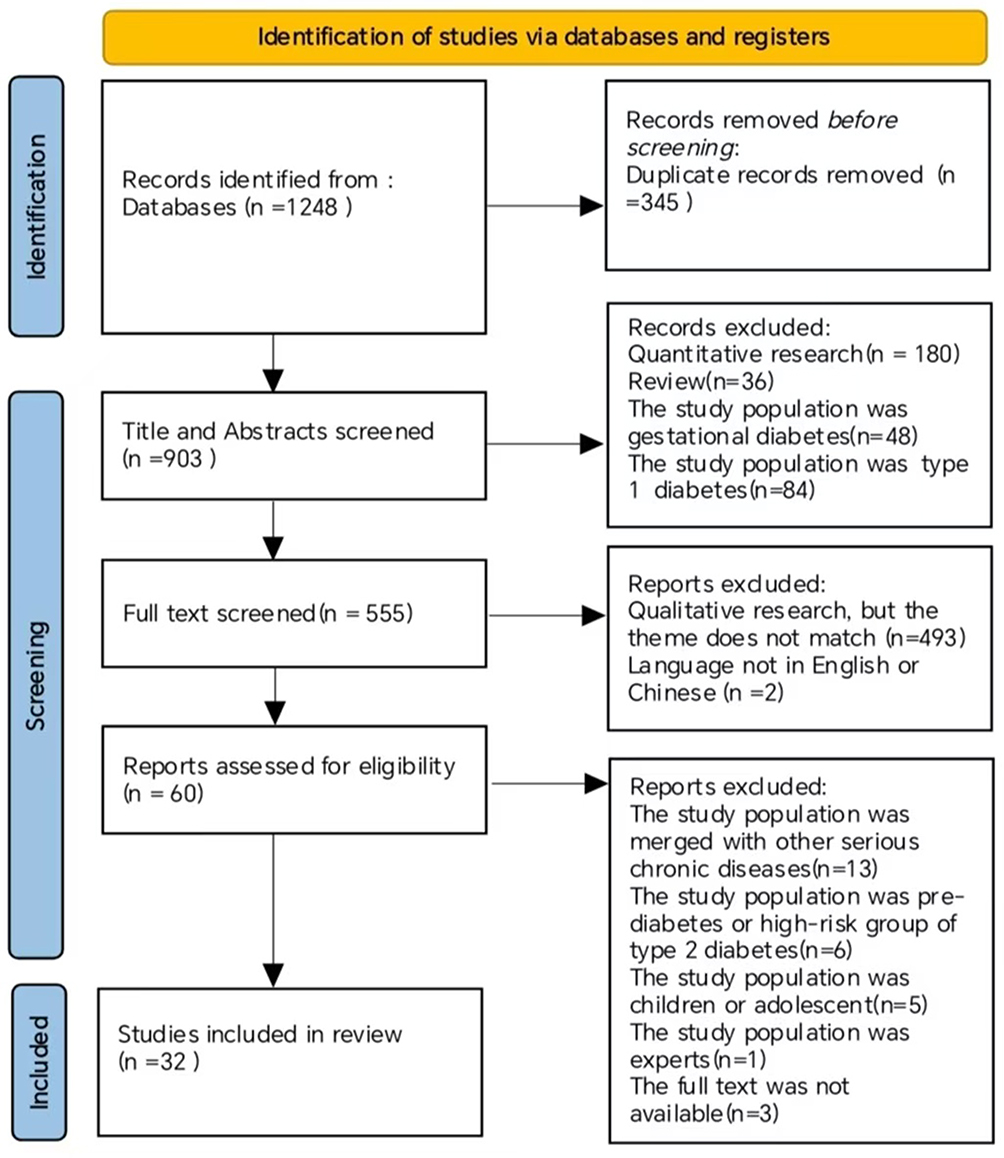 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram. |
Inclusion and Exclusion Criteria
Studies were included if they:
- Studies involved participants with T2D over the age of 18;
- Outcomes were the views, perceptions, experiences, and barriers or contributing factors to exercise;
- Qualitative studies or mixed methods studies which reported qualitative results.
Studies were excluded if:
- Participants with pre-diabetes, high risk of diabetes or gestational diabetes;
- Participants had severe chronic diseases;
- The full text was not available;
- Non-English or Chinese papers.
Quality Assessment (Table 1)
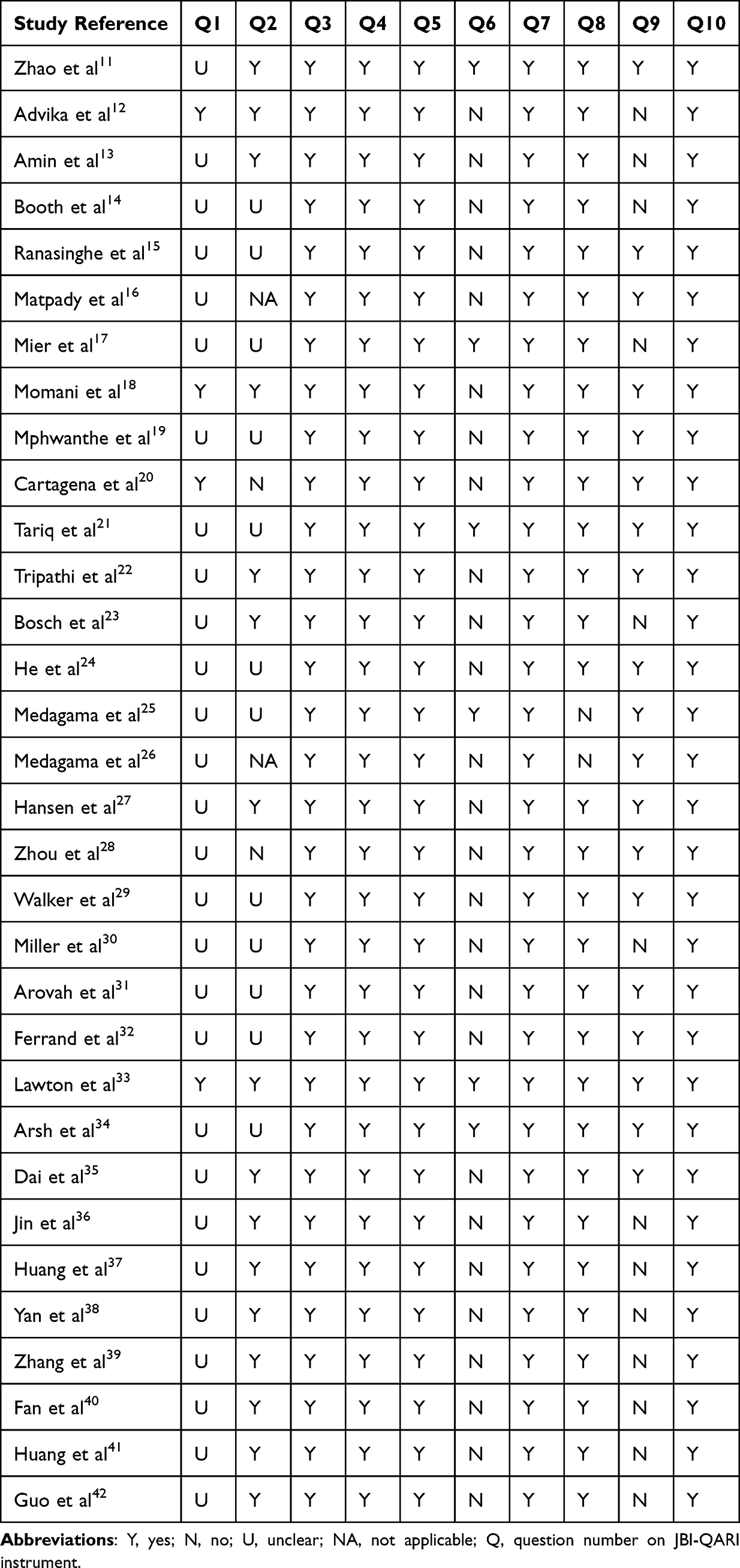 |
Table 1 Quality Appraisal of Studies Using JBI-QARI Instrument |
The JBI Critical Appraisal Checklist for Qualitative Research (JBI-QARI)43 was used to assess the quality of included studies.11–42 The JBI-QARI includes ten criteria: philosophical perspective, methodology, data collection, representation and analysis of data, interpretation of results, researcher reflexivity, ethical approval, and data analysis. Each criterion offers response options of “yes”, “no”, “unclear”, or “not applicable.” Quality assessment was conducted separately by Zhu Han and Li Wang, and inconsistencies were discussed and resolved between Zhu Han and Li Wang. Studies were reviewed based on the results of the quality assessment, but no studies were omitted due to their quality.
Data Extraction and Synthesis (Table 2)
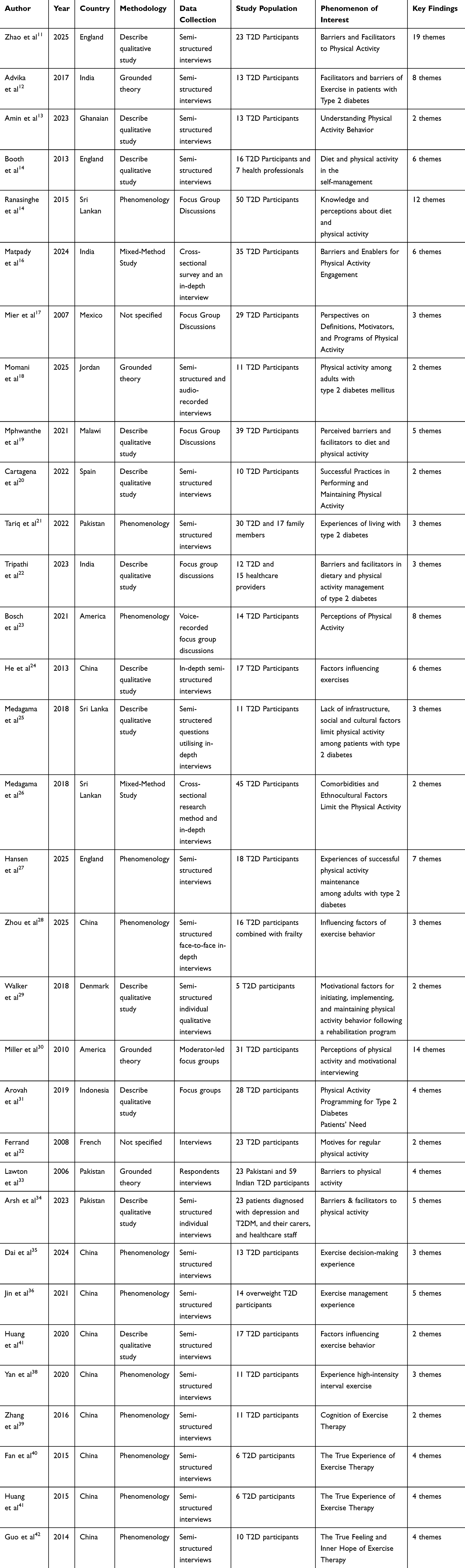 |
Table 2 Specific Information of the Included Studies |
The first author extracted data of the included studies, while the second author reviewed the results. The extracted data contained precise information about the author, year of publication, country of study, study methodology, data collection methods,sample size, phenomena relevant to the review questions, and results. The data were synthesized using the thematic synthesis approach, bringing together common data from studies that offered information on patients’ viewpoints on physical activity. As the primary purpose of this research was to discover factors impacting patients’ exercise behavior, categories were grouped into overarching themes, which represented the review’s consolidated conclusions. The findings were then classified into subthemes line by line, and specific quotes that represent the subthemes were identified. Furthermore, the categories had been repeatedly revised and refined. Critical reflection was engaged during the categorizing process.
Results
Study Description and Data Synthesis results (Table 3)
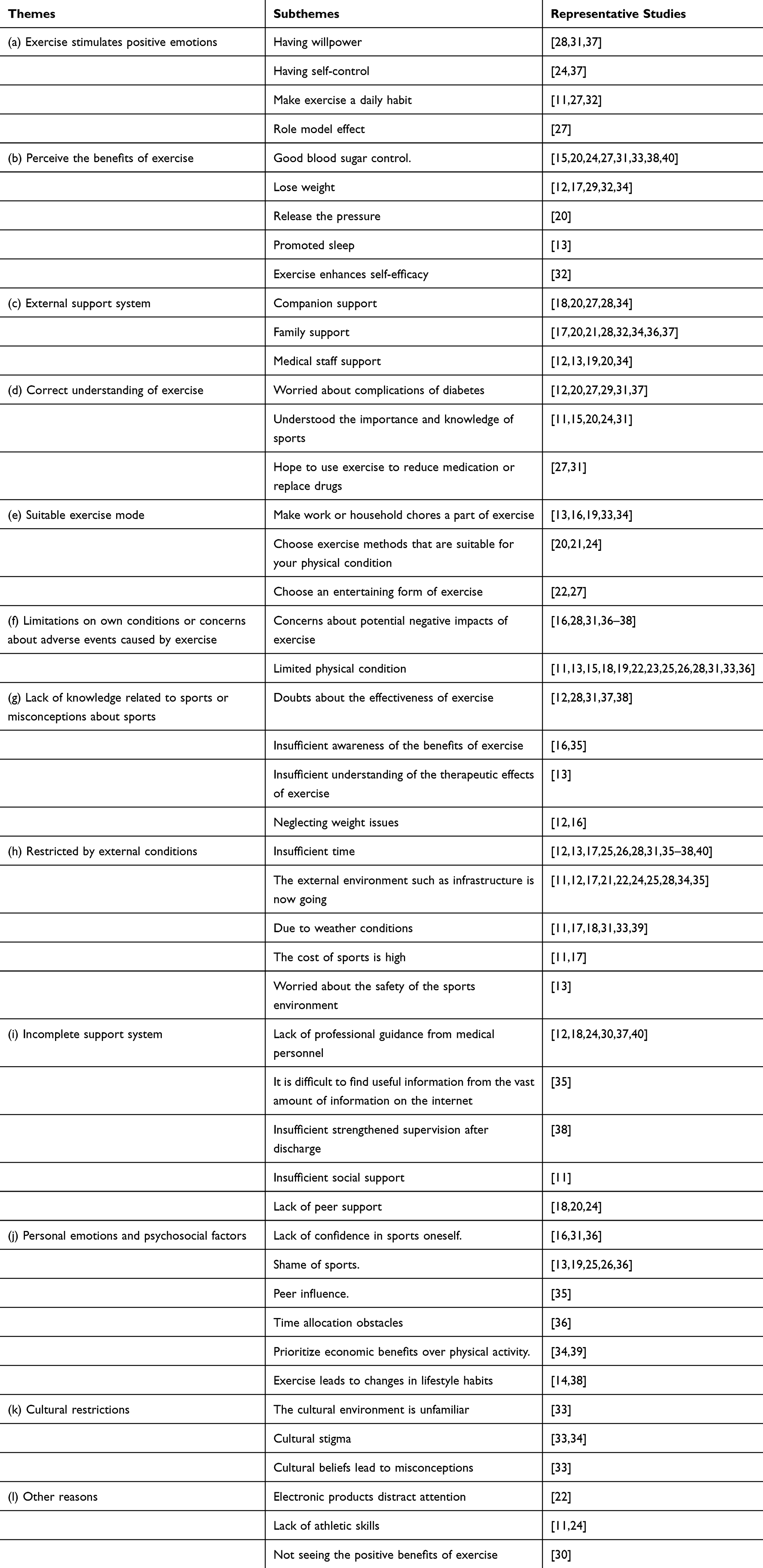 |
Table 3 Data Analyse results of the Included Studies |
The included studies were published between 2005 and 2025, involving 14 countries: England (n=4), India (n=3), Ghanaian (n=1), Sri Lankan (n=3), Mexico (n=1), Jordan (n=1), Malawi (n=1), Spain (n=1), Pakistan (n=2), America (n=2),China (n=10), Denmark (n=1), Indonesia (n=1) and French (n=1). In total, there were 682 patients and 39 participants related to patients across all studies, 30 studies used qualitative research methodologies, while 2 studies used a mixed-method approach. Interrelated subthemes were identified and detailed.
Theme 1 Exercise Stimulates Positive Emotions or Makes Exercise a Habit
According to research, patients with strong willpower are more likely to maintain exercise routines in the long term,28 and people with good self-control can actively alter their exercise tactics when the external environment is limited:
I am always very busy with my work, and cannot afford enough time for exercises. But I think out a way. I usually get off the bus one stop prior to my destination, and then choose to walk home after work. I think it suits me because it will not take up too much of my time.28
After completing the internalization phase of exercise behavior, patients can make their own decisions to continue exercising without being pushed to do so, and incorporate exercise as a habit into their daily lives, making it an important component of self-identity. One participant explained:
If I skip exercising for a few days, I feel uncomfortable and itchy, I want to exercise, it’s become a habit, and even if I’m lazy for a few days, I feel bad if I skip exercising for too long.11
Some patients have successfully reduced the cognitive burden generated by continual decision-making by creating detailed workout regimens in advance.27 The exemplary role helps patients improve their exercising self-efficacy. One participant expressed:
The BBC showed a documentary called Fixing Dad… Here’s this guy, a bit older than me, type 2 diabetic … he changed the way he eats and he exercises more. And his diabetes is put into remission. And I was like. ‘Oh? Well! If he can do it, I can do it!’ And that is what started my journey.27
Theme 2 Perceive the Benefits of Exercise
To begin, in terms of psychology,many participants reported that physical activity helps reduce blood glucose levels and promotes weight management. For instance,one said:
I believe exercises help modify blood glucose. Sometimes, I measured my blood glucose after walking for half an hour after dinner. Two-hour post-prandial blood glucose level always ranges between 7 and 8 mmol/l. Hyper glucose level does not happen;24
Another explained: “It would really be motivating. You want to get into a loop where you eat right because you are exercising and you are exercising because you are losing weight”.29 It has also improved sleep quality.13 Secondly, exercise significantly improves patients’ mental health. Patients experience less anxiety and depression after exercising, as well as increased inner satisfaction and enjoyment of the activity. One patient explained:
Well-being. That’s it, sometimes you’re in a bad mood for whatever or sometimes without any reason, and when you go out walking and when you get home, it’s gone.20
Furthermore, exercise helps boost the immune system and improve overall health. Improving patients’ health status effectively boosts their self-efficacy, resulting in a positive feedback loop.32
Theme 3 External Support System
Mutual encouragement, support, and monitoring among peers effectively increase passion for exercising:
When for some reason I miss my walking routine, let’s say for 1 or 2 days, many people will ask me: ‘where have you been?’, in a way that makes me happy because it means that many people care for me.31
Participants said that this form of encouragement, together with other physiological and psychological benefits, prompted them to continue exercising. Good family support also provides essential guarantees for patients to continue exercising:
For the past few days, my son has accompanied me for a walk. He offers to go for a walk, and we walk for about 30 minutes. Usually, he is busy at night, so we can’t go for a walk then. However, when he has time, he asks me to go for a walk with him, which I do.21
Professional advice and favorable incentives from medical professionals have a substantial impact on patients’ exercise compliance. One participant said: “When you say, physical activity is told (advised/prescribe) by the doctor, it means a lot, whenever a doctor says anything, I do what he suggests, you can say (ask) why (I follow the doctors’ advice) but because he knows everything about me (my disease condition) … even if he told me to run for a while, I cannot ignore that “.29 Another said:”The nurses told me more about it (exercise) than the doctor did. The nurses are much closer to patients than doctors are and we tend to listen to them more”. As a result, it is worth emphasizing that nursing staff and patients interact frequently, therefore the advice given by nurses to patients has a significant impact. This frequent contact not only improves the effectiveness of health recommendations, but it also fosters a stronger trust relationship.
Theme 4 Correct Understanding of Exercise
Many patients are concerned about the long-term risks of diabetes, therefore they prioritize the health benefits of exercise. One participant expressed:
I was terrified of getting my foot chopped off. I thought: ‘Oof, this is really really serious what can happen there!’ Chronic, progressive disease that leads to heart attack, stroke, amputations, and blindness! Once I read that, that was it, and I thought: ‘I need to do something about this!27
Some patients aim to cut their medication dosage or even replace it entirely with diet and exercise. For instance, one participant shared:
The first thing the diabetic nurse said was:’right, I will put you on metformin’. I said, ‘OK’, but I then said, ‘No!’. And I [have] successfully since managed [to control my diabetes] with just diet and exercise. […] Going on medication is like giving into it. It’s an ongoing battle with my diabetic nurse around medication.27
Furthermore, patients can clarify relevant exercise knowledge with support from medical staff or self-learning online.20,24
Theme 5 Suitable Exercise Mode
Patients include household tasks or professional activities into their daily exercise routines. One say:
I briskly walk as part of my exercise. I also go to Lilongwe river to wash my clothes either two or three times a week and I wash for over 40 minutes. I even wash my wife’s clothes which I also consider as part of my exercise and it’s really helping me,
Another stated: “I do farm a lot and my work involves carrying heavy metals, because I am a welder. So, I do physical activity through work”.19 Some patients choose exercise regimens that are appropriate for their physical abilities and health situation. For example, because of the patient’s advanced age or bronchitis, walking was chosen as a type of exercise.20,24 Patients’ ability to continue for an extended period of time is also influenced by their workout style. When patients engage in recreational exercise, the enjoyment and happiness they get serve as a motivator for further participation. One participant shared: “The joy, the actual psychological aspect of the biking – being out in the air is genuinely motivating. I just love being out in the air”.27
Theme 6 Adverse Events Caused by Personal Health Limitations or Concerns About Exercise
Diabetes causes decline of body function, which restricted the physical activity.15 The patient’s ability to complete certain movements is limited due to other illnesses such as vision problems, gout, breathing problems, chest pain, resulting in the inability to complete certain forms of exercise. One participant explained:
I can’t exercise like the strong guys [healthy people]. At my age, my hypertension doesn’t allow me to exercise. My heart beats too fast... my knee [arthritis] doesn’t allow me. [hurts when I exercise].13
Another explained: “I have gout and my weight is very high, it’s difficult for me to walk even 50 steps. I somehow manage to do my routine”.22 Due to prior experiences, patients frequently worry that their initial conditions (such hypoglycemia, or unforeseen circumstances like exercise-related injuries) may worsen as a result of exercise. They actively lower their activity intensity or avoid exercise as a result of this worry.16 For instance,one participant said: “I dare not go out for exercise now. I fell last month and have been walking slowly and carefully lately”.28
Theme 7 Lack of Knowledge Related to Sports or Misconceptions About Sports
Some patients feel that exercise cannot or only temporarily improves blood glucose levels, and that it may raise physical stress and the risk of unpleasant events such as perspiration, elevated heart rate, and dyspnea after exercise.33 One said: “Exercise is beneficial for physical health, but medication is important. People at this age still need to rely on medication to control themselves.” Another stated:
After exercising, it seems that there hasn’t been any improvement in the body, and I feel like it’s mostly the medication and diet control that works, and exercise doesn’t change those symptoms (blood glucose, fatigue);28 or even if wanting to continue exercising, a lack of professional advice leads to a misunderstanding of the optimum exercise time and intensity.13 They are also unable to forecast the precise advantages of exercise, raising concerns about their own decision-making procedures:
I am advised to do exercise, and I walk for 15 to 30 minutes a day, I do not know whether it is sufficient to control diabetes or not. 16 Some patients have a limited grasp of obesity issues, and some patients with a familial history of obesity see obesity as a typical occurrence, lacking the motivation to control their weight through exercise. For example, one participant explained: “Everyone in my family is well built as I am. It is not like I gained weight in the middle I have always been on the heavier side from when I was young”.12
Theme 8 Restricted by External Conditions
A large number of studies found that due to the increased pressure of social roles and the significant burden of work and family responsibilities, patients’ disposable time is significantly reduced, making it difficult to ensure regular exercise arrangements, resulting in insufficient exercise time for themselves. Exercise is also limited by the patient’s living conditions and infrastructure. If the patient’s living environment lacks handy exercise facilities or walking trails, their willingness to exercise will decline. Some participants noted that the expense of fitness equipment or facilities is a deterrent to exercising. One participant said:
Currently, playing table tennis is very costly. It’s very expensive. A bucket of balls costs over 70 yuan for 12 balls, and it’s gone after playing three times. Each time, the venue fee is 50 yuan. Just thinking about it, it’s already very expensive.11
At the same time, weather conditions might make it difficult for patients to exercise, with extreme weather conditions such as high heat, severe cold, and pollution directly impeding outdoor activities.11,33 Furthermore, some patients are concerned about their personal safety during evening exercise and in distant regions, which reduces their motivation to exercise. One participant expressed: “It is not safe to exercise outside [especially] at dawn.The recent [serial] killings of women makes me fear going out early in the morning to exercise”.13
Theme 9 Incomplete Support System
Due to their busy daily schedules, medical staff have neglected to provide exercise guidance to patients; or, if they have provided relevant guidance to patients, it is too abstract, leaving patients with some doubts about the specific implementation process; in some cases, medical staff only inform patients of the importance of exercise, lacking effective communication with patients and personalized guidance.14,18,30 When confronted with a plethora of online information, patients struggle to identify the best workout method for themselves.35 Due to a lack of professional supervision, some patients struggle to continue regular exercise for an extended period of time after discharge, resulting in a steady decrease in compliance.38 Some patients have difficulties sticking to their fitness regimen due to a lack of peer or group motivation. One participant expressed: “I am not doing exercise every day because no one is walking with me, I like walking with others”.18
Theme 10 Personal Emotional Factors
Some patients are concerned about physical exercise due to age or a lack of trust in their athletic ability, therefore they intentionally avoid sports activities,16,31 Chronic illness can reduce patients’ quality of life by generating negative feelings such as despair and anger, losing tolerance with therapy (including exercise), and, ultimately, decreasing patients’ exercise compliance.40 Patients’ decision-making behavior is frequently influenced by their peers, and if people around them stop exercising, the patient’s inclination to continue exercising decreases.35 The patient’s sense of guilt due to their incapacity to learn might also become a barrier to their movement.19,26 Furthermore, some patients value economic rewards (such as the sense of accomplishment that comes from earning money) over health management and consciously choose to discontinue exercise.34
Theme 11 Cultural Restrictions
Cultural elements that impede patient movement can be divided into two categories: individual cognitive level and society cultural level. For example, when patients migrate to foreign cultural contexts and have inadequate English proficiency, they frequently avoid outdoor activities out of fear of being unable to successfully seek aid in the event of an unforeseen crisis. A typical case demonstrates that a patient experienced limb spasms when walking exercise on the advice of a doctor, but owing to language issues, they were unable to access timely care, leading to a chronic phobia of going out alone.33 Furthermore, some patients’ disease attribution influences their athletic motivation, such as attributing diabetes to God’s will rather than their own behavior, so diminishing the initiative for lifestyle change.33 At the social cultural level, including the phenomenon of sports stigmatization: certain forms of exercise (such as cycling and walking) are labeled as’symbols of poverty’,34 or running on the road is considered unconventional behavior,21 leading to psychological resistance; gender cultural constraints: traditional culture prohibits physical exposure between the opposite sex, and the lack of supporting facilities (such as same-sex coaches and single-sex sports venues) further hinders the development of fitness, swimming, and other activities.33
Theme 12 Other Reasons
Excessive use of electronic gadgets, such as mobile phones, televisions, and laptops, can lead to a sedentary lifestyle: “I come back from the office and lie down; I watch my social media profile etc. without noticing when it’s time for dinner. Then I skip my evening walk”;22 some patients, despite their want to exercise, face challenges in real implementation due to a lack of exercise abilities, making it difficult for them to sustain regular exercise habits. One participant shared: “I once tried to play table tennis. But when I went to the venue, no one was willing to play with me because I am just a beginner”.22 When exercise time conflicts with personal preference periods (such as the “afternoon exercise routine”), patients’ inclination to exercise decreases significantly;36 alternatively, after abandoning their old habits, patients frequently struggle to adapt to the new exercise routine owing to laziness.14 Furthermore, patients’ exercise compliance and motivation may suffer as a result of a misunderstanding of the benefits of exercise. One participant stated: “I played basketball every day. And when I do that I never lose weight. So it’s all a turn off to me”.16
Discussion
This study revealed four core dimensions that affect exercise behavior of diabetes patients through systematic review and thematic synthesis. The first aspect to consider is knowledge and cognitive factors: It is manifested in the patient’s mastery of sports and diabetes management knowledge, as well as the positive feedback formed through practice, such as the perceived improvement of exercise on blood sugar control. Another key point is structural barriers and social support systems: involve objective constraints such as economic costs, time arrangements, environmental accessibility, and subjective support resources such as family support, peer encouragement, and guidance from medical personnel. Notably, in terms of selecting exercise methods, choosing exercise methods that are suitable for one’s own health condition or have fun can significantly increase the likelihood of long-term persistence. The final consideration is personal motivational factors: including intrinsic driving forces such as strong autonomy and the habit of exercising, as well as hindering factors such as emotional disorders such as exercise shame; The modern lifestyle challenge of excessive use of electronic devices squeezing out exercise time; Shortcomings in individual abilities.
Patients with exercise knowledge often have higher exercise compliance. Under the theoretical framework of the health belief model, patients’ health behavior decisions can be influenced by two key cognitive factors: the perception of the benefits of adopting healthy behaviors, and the judgment of potential serious consequences of diseases such as death, disability, and long-term health problems.44 These cognitive factors not only encourage patients to actively adopt healthy behaviors or seek treatment, but also have an impact on their long-term treatment compliance. Multiple studies have provided empirical support for this: Zhu et al45 found that there is a significant correlation between patients’ mastery of exercise knowledge and exercise compliance. Patients who have sufficient mastery of exercise knowledge are better able to follow exercise advice and improve their exercise compliance; Mwimo et al46 further confirmed that the level of belief and knowledge of T2D patients can effectively predict their practice of physical activity. As mentioned, when patients observe that their blood glucose levels are effectively controlled after exercise and their weight gradually decreases, these positive changes significantly enhance their motivation to continue exercising; at the same time, when patients are fully aware of the severity of complications of diabetes (such as diabetes foot), exercise is regarded as an important intervention to reduce such risks. On the contrary, some patients who lack exercise knowledge believe that the increased heart rate and shortness of breath caused by exercise will increase the burden on the body and avoid exercise. Therefore, medical staff should popularize patients’ exercise knowledge such as the positive effects of exercise and specific exercise intensity and correct patients’ misconceptions about exercise through various forms such as health education lectures, distribution of promotional brochures, and online science popularization. Besides, actively guiding patients to pay attention to the short-term and long-term benefits of exercise, and providing targeted health guidance through evaluating their understanding of the severity of the disease, is essential for long-term changes in exercise behavior.
For external objective conditions and support systems, social support theory suggests that informal or formal support systems from family members, peers, or healthcare professionals can serve as external motivators that can be leveraged through emotional support or professional guidance. This can enhance an individual’s ability to cope with various environmental challenges.47 And professional guidance from healthcare professionals can help patients have a more accurate understanding of the disease, making them more willing to follow exercise plans and having a positive impact on their physical and mental health. Further research reveals that perceived social support is an important predictor of physical activity levels,48 however, time constraints and health status limitations constitute the main obstacles to achieving compliance.49 At the practical level, the following adaptive strategies can be adopted to cope with environmental barriers: in the face of extreme weather conditions, it is recommended to adjust the exercise period to a climate suitable morning or evening, or switch to indoor exercise, such as using treadmills and other fitness equipment; time limited patients can use their fragmented time for exercise, such as using stairs instead of elevators or walking instead of transportation. These small activities do not take up a lot of time and can increase physical activity. Even without professional equipment, patients can creatively utilize household items for strength training. It is particularly noteworthy that medical personnel should focus on building a social support network, encouraging patients to establish exercise partnerships with their families and peers, and include peer mentorship components in exercise programs. This sociable exercise not only provides supervision and support, but also enhances the enjoyment and sustainability of exercise. This comprehensive support strategy promotes the formation and maintenance of healthy behaviors from three levels: cognitive, emotional, and behavioral.
In terms of the choice of exercise mode, some patients are afraid of exercise because they have limited physical function due to diabetes or other chronic diseases, or because they are worried that exercise may aggravate the primary disease, induce hypoglycemia, fall and other adverse events. Conversely, there are also patients who actively seek suitable forms of exercise despite facing physical limitations, such as converting daily work or household activities into exercise opportunities. The level of interest of patients in rehabilitation activities is closely related to their treatment participation and long-term compliance, some patients tend to choose sports projects with strong interest, and maintain their long-term participation enthusiasm through the pleasant experience during the exercise process. According to the theory of behavioral motivation, when patients develop an intrinsic interest in a rehabilitation activity, their likelihood of actively participating significantly increases.50 Kanai et al51 found through a large sample study that through three years of continuous incentive measures, patients’ exercise participation and long-term persistence have been significantly improved. These research results indicate that stimulating patients’ interest in activities is an important strategy for increasing their participation and long-term persistence. Therefore, it is recommended that patients choose appropriate forms of exercise based on their own health status, and medical staff need training to develop personalized exercise prescriptions and provide targeted health guidance for patients based on individual physical and cultural differences.
Research has shown that aerobic exercise can promote the secretion of more cortisol, endorphins, and dopamine in the human body, the changes in bodily function caused by these substances after exercise are not only effective in reducing stress reactions, but also closely related to the pleasurable experience brought by exercise.52 In the field of health behavior research, willpower and habits are two key elements for long-term adherence to healthy behavior. Willpower is not only the initial driving force for people to start a healthy behavior, but also helps individuals resist various temptations and cope with setbacks in the process of maintaining healthy behavior; habit, on the other hand, is a relatively fixed and automated behavioral pattern, and its persistence contributes to the long-term maintenance of healthy behavior, as healthy behaviors gradually become habits, people no longer need to rely on strong willpower to drive their execution.53 As mentioned earlier, patients with strong willpower are often able to persist in healthy behaviors for a long time. Some patients integrate exercise into their daily lives, making it a habit, and once they stop exercising, they will feel uncomfortable However, there are also some patients who find it difficult to change their existing lifestyle habits, making it difficult to integrate exercise into their daily lives. Therefore, when habits are formed, people’s dependence on willpower when performing healthy behaviors will significantly decrease. Social cognitive theory suggests that when observers see role models succeed, they can predict that they will also achieve similar success after performing the same behavior, thereby enhancing their motivation to imitate and promoting individual behavior change and growth.54 In summary, medical personnel should actively help patients develop exercise habits and introduce them to successful cases around them to enhance patients’ self efficacy in persisting in exercise. Patients themselves should also balance the relationship between earning money and exercising, consciously resist the temptation of addiction to electronic products, and strive to develop exercise habits.
Limitations
This study also has certain limitations due to pragmatic reasons, as only articles in English and Chinese were included and literature in other languages was not included, which may affect the comprehensiveness of the analysis results. Meanwhile, the literature that meets the inclusion criteria does not involve ethnographic research. Subsequent research can expand multilingual literature retrieval to explore the key factors affecting patient exercise compliance in depth, thereby provide more comprehensive evidence-based support for optimizing clinical intervention strategies.
Conclusion
This review clarified many promoting and hindering factors that affect physical activity of T2D patients in daily life. Understanding the reasons why patients refuse or find it difficult to maintain exercise, as well as their successful experiences in maintaining exercise, can assist nurses to identify patients’ individual nursing needs and adopt relevant promotion plans. The patients’ opinions and experiences of the current literature can be classified into personal factors, external factors. Personal factors include the patient’s level of knowledge, perception of benefits, physical condition, choice of exercise style, cultural factors; external factors include objective conditions, support systems, and other factors should also be considered. In future nursing, attention should be paid to the objective conditions and inner experiences of patients, identifying factors that affect exercise compliance from multiple perspectives, and then developing targeted exercise promotion plans from multiple dimensions, evaluating the effectiveness of the plans, and making timely modifications to further enhance compliance.
Acknowledgments
Thank you to all the authors and participants of the original research paper, it was their research that made this study possible. At the same time, we would like to express our gratitude to the funding provided by the Liaoning Provincial Department of Education.
Funding
This research was supported by the Basic Research Project of Liaoning Provincial Department of Education (Grant No. LJKFR20220254).
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Global action plan for the prevention and control of nonconnunicable diseases 2013-2020(EB/OL). 2013. Available from: https://www.who.int/publications/i/item/9789241506236.
2. Khan RMM, Chua ZJY, Tan JC, Yang Y, Liao Z, Zhao Y. From pre-diabetes to diabetes: diagnosis, treatments and translational research. Medicina. 2019;55(9):546. doi:10.3390/medicina55090546
3. Wicaksana AL, Hertanti NS. Concept analysis of diabetes-related quality of life. Health Qual Life Outcomes. 2025;23(1):27. doi:10.1186/s12955-025-02354-2
4. Berg AH, Scherer PE. Adipose tissue, inflammation, and cardiovascular disease. Circ Res. 2005;96(9):939–949. doi:10.1161/01.RES.0000163635.62927.34
5. Slentz CA, Tanner CJ, Bateman LA, et al. Effects of exercise training intensity on pancreatic beta-cell function. Diabetes Care. 2009;32(10):1807–1811. doi:10.2337/dc09-0032
6. Perakakis N, Triantafyllou GA, Fernández-Real JM, et al. Physiology and role of irisin in glucose homeostasis. Nat Rev Endocrinol. 2017;13(6):324–337. doi:10.1038/nrendo.2016.221
7. Hermann G, Herbst A, Schütt M, et al. Association of physical activity with glycaemic control and cardiovascular risk profile in 65 666 people with type 2 diabetes from Germany and Austria. Diabet Med. 2014;31(8):905–912. doi:10.1111/dme.12438
8. Onufrak S, Saelee R, Zaganjor I, et al. Physical activity according to diabetes and metropolitan status, U.S. 2020 and 2022. Am J Prev Med. 2024;66(6):1008–1016. doi:10.1016/j.amepre.2024.01.023
9. Crews RT, Schneider KL, Yalla SV, Reeves ND, Vileikyte L. Physiological and psychological challenges of increasing physical activity and exercise in patients at risk of diabetic foot ulcers: a critical review. Diabetes Metab Res Rev. 2016;32(8):791–804. doi:10.1002/dmrr.2817
10. Maudet‐Coulomb É, Martin‐Krumm C, Tarquinio C, Mino J-C. Adapted physical activity interventions and motivational levers: what benefits for type 2 diabetics? A systematic review. Health Sci Rep. 2024;7(3):e1644. doi:10.1002/hsr2.1644
11. Zhao X, Duaso M, Ghazaleh HA, Guo X, Forbes A. Barriers and facilitators to physical activity in people with young-onset (Aged 18-40 years) type 2 diabetes: a qualitative study. J Clin Nurs. 2025;34(6):2386–2399. doi:10.1111/jocn.17691
12. Advika TS, Idiculla J, Kumari SJ. Exercise in patients with type 2 diabetes: facilitators and barriers - A qualitative study. J Family Med Prim Care. 2017;6(2):288–292. doi:10.4103/2249-4863.219998
13. Amin M, Kerr D, Atiase Y, Yakub Y, Driscoll A. Understanding physical activity behavior in ghanaian adults with type 2 diabetes: a qualitative descriptive study. J Funct Morphol Kinesiol. 2023;8(3):127. doi:10.3390/jfmk8030127
14. Booth AO, Lowis C, Dean M, Hunter SJ, McKinley MC. Diet and physical activity in the self-management of type 2 diabetes: barriers and facilitators identified by patients and health professionals. Prim Health Care Res Dev. 2013;14(3):293–306. doi:10.1017/S1463423612000412
15. Ranasinghe P, Pigera AS, Ishara MH, Jayasekara LM, Jayawardena R, Katulanda P. Knowledge and perceptions about diet and physical activity among Sri Lankan adults with diabetes mellitus: a qualitative study. BMC Public Health. 2015;15:1160. doi:10.1186/s12889-015-2518-3
16. Matpady P, Maiya AG, Saraswat PP, et al. Barriers and enablers for physical activity engagement among individuals from India with type 2 diabetes mellitus: a mixed-method study. J Phys Act Health. 2024;21(5):519–527. doi:10.1123/jpah.2023-0574
17. Mier N, Medina AA, Ory MG. Mexican Americans with type 2 diabetes: perspectives on definitions, motivators, and programs of physical activity. Prev Chronic Dis. 2007;4(2):A24.
18. Momani A, Al-Marzouqi Z, Abu-Shhadeh A, et al. Physical activity among adults with type 2 diabetes mellitus in Jordan: a qualitative study. Ther Adv Endocrinol Metab. 2025;16:20420188251315658. doi:10.1177/20420188251315658
19. Mphwanthe G, Carolan M, Earnesty D, Weatherspoon L. Perceived barriers and facilitators to diet and physical activity among adults diagnosed with type 2 diabetes in Malawi. Glob Public Health. 2021;16(3):469–484. doi:10.1080/17441692.2020.1805784
20. Vilafranca Cartagena M, Arreciado Marañón A, Artigues-Barbera E, Tort-Nasarre G. Successful practices in performing and maintaining physical activity in adults with type 2 diabetes mellitus: a qualitative study. Int J Environ Res Public Health. 2022;19(21):14041. doi:10.3390/ijerph192114041
21. Tariq O, Rosten C, Huber J. Experiences of living with type 2 diabetes in Pakistan: the role of culture and family in physical activity. Int J Equity Health. 2022;21(1):103. doi:10.1186/s12939-022-01706-4
22. Tripathi D, Vikram NK, Chaturvedi S, Bhatia N. Barriers and facilitators in dietary and physical activity management of type 2 diabetes: perspective of healthcare providers and patients. Diabetes Metab Syndr. 2023;17(3):102741. doi:10.1016/j.dsx.2023.102741
23. Vanden Bosch M, Wesley E, Strouse S. Perceptions of physical activity in middle-aged women with type 2 diabetes. West J Nurs Res. 2021;43(7):640–648. doi:10.1177/0193945920973151
24. He W, Zhang Y, Zhao F. Factors influencing exercises in Chinese people with type 2 diabetes. Int Nurs Rev. 2013;60(4):494–500. doi:10.1111/inr.12046
25. Medagama A, Galgomuwa M. Lack of infrastructure, social and cultural factors limit physical activity among patients with type 2 diabetes in rural Sri Lanka, a qualitative study. PLoS One. 2018;13(2):e0192679. doi:10.1371/journal.pone.0192679
26. Medagama A, Galgomuwa M. Comorbidities and ethnocultural factors limit the physical activity of rural sri lankan patients with diabetes mellitus. J Diabetes Res. 2018;2018:4319604. doi:10.1155/2018/4319604
27. Blicher-Hansen J, Chilcot J, Gardner B. Experiences of successful physical activity maintenance among adults with type 2 diabetes: a theory-based qualitative study. Psychol Health. 2024;39(3):399–416. doi:10.1080/08870446.2022.2063863
28. Zhou Y, Lu HH, Sun X, et al. Influencing factors of exercise behavior in older patients with type 2 diabetes mellitus combined with frailty: a qualitative study. Geriatr Nurs. 2025;62(Pt A):138–144. doi:10.1016/j.gerinurse.2025.01.017
29. Walker KC, Valentiner LS, Langberg H. Motivational factors for initiating, implementing, and maintaining physical activity behavior following a rehabilitation program for patients with type 2 diabetes: a longitudinal, qualitative, interview study. Patient Prefer Adherence. 2018;12:145–152. doi:10.2147/PPA.S150008
30. Miller ST, Marolen KN, Beech BM. Perceptions of physical activity and motivational interviewing among rural African-American women with type 2 diabetes. Womens Health Issues. 2010;20(1):43–49. doi:10.1016/j.whi.2009.09.004
31. Arovah NI, Kushartanti BW, Washington TL, et al. Type 2 diabetes patients’ need for physical activity programming: a qualitative study at a Yogyakarta hospital clinic. Kesmas. 2019;13(4):169–175. doi:10.21109/kesmas.v13i4.1942
32. Ferrand C, Perrin C, Nasarre S. Motives for regular physical activity in women and men: a qualitative study in French adults with type 2 diabetes, belonging to a patients’ association. Health Soc Care Community. 2008;16(5):511–520. doi:10.1111/j.1365-2524.2008.00773.x
33. Lawton J, Ahmad N, Hanna L, et al. ‘I can’t do any serious exercise’: barriers to physical activity amongst people of Pakistani and Indian origin with Type 2 diabetes. Health Educ Res. 2006;21(1):43–54. doi:10.1093/her/cyh042
34. Arsh A, Afaq S, Carswell C, et al. Barriers & facilitators to physical activity in people with depression and type 2 diabetes mellitus in Pakistan: a qualitative study to explore perspectives of patient participants, carers and healthcare staff. Mental Health Phys Act. 2023:110542. 10.1016/j.mhpa.2023.100542.
35. Dai X, Li Z, Qin YL, et al. Qualitative research on exercise decision-making experience of type 2 diabetes patients. J Hunan Normal Univer. 2024;21(3):179–183. doi:10.3969/j.issn.1673-016X.2024.03.034
36. Jin CY, Lu XF. Qualitative study on exercise management experience of overweight diabetes patients. General Nursing. 2024;22(16):3103–3106. doi:10.12104/j.issn.1674-4748.2024.16.033
37. Huang, CY. Qualitative study on the true feelings of diabetes patients on exercise therapy. General Nursing. 2015;9:848–850. doi:10.3969/j.issn.1674-4748.2015.09.041
38. Yan HM, Zhang C, Wang YJ, et al. Qualitative study on high-intensity intermittent exercise experience of type 2 diabetes patients. Chin J Pract Nurs. 2020;36(24):1870–1875. doi:10.3760/cma.j.cn211501-2020113-00140
39. Zhang QZ, Wang X. Qualitative research on diabetes patients’ cognition of exercise therapy based on PMT theory. China Health Nutrition. 2016;26(17):370.
40. Fan B, Liu SQ, Huang F. Qualitative study on the true feelings of diabetes patients on exercise therapy. General Nursing. 2015;13:1158–1160. doi:10.3969/j.issn.1672-1888.2015.13.005
41. Huang LJ, Yang XN, Li SM, et al. Qualitative study on the influencing factors of exercise behavior in young and middle-aged patients with type 2 diabetes. Integrat Chin Western Med Nurs. 2020;6(8):59–63. doi:10.11997/nitcwm.2008012
42. Guo ML, Cheng M. Qualitative research on diabetes patients’ understanding of exercise therapy and their inner hope. J PLA Nurs. 2014;22:9–12,16. doi:10.3969/j.issn.1008-9993.2014.22.003
43. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z. editors. JBI Manual for Evidence Synthesis. In: JBI. 2024.
44. Alyafei A, Easton-Carr R. The Health Belief Model of Behavior Change. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024.
45. Zhu Y, Cheng K, Wang H, et al. Exercise adherence and compliance and its related factors among elderly patients with type 2 diabetes in China: a cross-sectional study. Patient Prefer Adherence. 2022;16:3329–3339. doi:10.2147/PPA.S374120
46. Mwimo JL, Somoka S, Leyaro BJ, Amour C, Mao E, Mboya IB. Knowledge, attitude and practice of physical activity among patients with diabetes in Kilimanjaro region, Northern Tanzania: a descriptive cross-sectional study. BMJ Open. 2021;11(9):e046841. doi:10.1136/bmjopen-2020-046841
47. Acoba EF. Social support and mental health: the mediating role of perceived stress. Front Psychol. 2024;15:1330720. doi:10.3389/fpsyg.2024.1330720
48. Morowatisharifabad MA, Abdolkarimi M, Asadpour M, Fathollahi MS, Balaee P. Study on social support for exercise and its impact on the level of physical activity of patients with type 2 diabetes. Open Access Maced J Med Sci. 2019;7(1):143–147. doi:10.3889/oamjms.2019.016
49. Alhomaid TA, Alkhalifah KA, Aljudayi AS, Alharbi OA, Aladwan AA, Alresheedi FA. Type of exercise and factors contributing to exercise adherence among diabetes patients in Saudi Arabia. Cureus. 2025;17(6):e86146. doi:10.7759/cureus.86146
50. Helou AY, Bittencourt JC. Navigating the complex terrain of motivated behavior: a bibliometric and neuroscientific perspective. Front Behav Neurosci. 2024;18:1363856. doi:10.3389/fnbeh.2024.1363856
51. Kanai M, Onozato N, Fujisawa Y, et al. Ongoing incentives’ 36-month effect on physical activity in a Japanese insurance-based health-promotion program. Prev Med. 2025. doi:10.1016/j.ypmed.2025.108327
52. Heijnen S, Hommel B, Kibele A, Colzato LS. Neuromodulation of Aerobic Exercise-A Review. Front Psychol. 2016;6:1890. doi:10.3389/fpsyg.2015.01890
53. Arlinghaus KR, Johnston CA. The Importance of Creating Habits and Routine. Am J Lifestyle Med. 2018;13(2):142–144. doi:10.1177/1559827618818044
54. Ginis KA, Nigg CR, Smith AL. Peer-delivered physical activity interventions: an overlooked opportunity for physical activity promotion. Transl Behav Med. 2013;3(4):434–443. doi:10.1007/s13142-013-0215-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combined Nutrition with Exercise: Fueling the Fight Against Sarcopenia Through a Bibliometric Analysis and Review
Zeng Y, He X, Peng X, Zhao L, Yin C, Mao S
International Journal of General Medicine 2024, 17:1861-1876
Published Date: 3 May 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025