Back to Journals » Psychology Research and Behavior Management » Volume 17
Influencing Factors Associated with Psychological Capital Among Ischemic Stroke Patients: A Latent Profile Analysis
Authors Zhang Y ![]() , Liu Z, Wang X
, Liu Z, Wang X ![]() , Gu Y
, Gu Y
Received 29 July 2024
Accepted for publication 13 November 2024
Published 26 November 2024 Volume 2024:17 Pages 4043—4052
DOI https://doi.org/10.2147/PRBM.S482943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Yang Zhang,1 Zhiyan Liu,1,2 Xianmei Wang,1 Ying Gu2
1School of Nursing, Guizhou Medical University, Guiyang, People’s Republic of China; 2The Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China
Correspondence: Zhiyan Liu; Xianmei Wang, School of Nursing, Guizhou Medical University, No. 9, Beijing Road, Guiyang, Guizhou, 550025, People’s Republic of China, Email [email protected]; [email protected]
Background: China has the highest incidence of stroke worldwide because of a high rate of recurrence of ischemic stroke, which has significant negative impacts on the physical and mental health of patients. However, little research has been devoted to the psychological capital of ischemic stroke patients.
Purpose: To investigate the psychological capital of ischemic stroke patients, and uses latent profile analysis to identify the potential profiles of the psychological capital among patients as well as to explore heterogeneity within subgroups and the factors influencing it.
Methods: A survey was distributed among and completed by 427 ischemic stroke patients from November 2023 to March 2024. Four types of questionnaires were administered: the Psychological Capital Questionnaire (PCQ-26), Perceived Stress Scale (CPSS), Athens Insomnia Scale (AIS), and a general information questionnaire.
Results: Three latent profiles of the psychological capital of ischemic stroke patients were identified: the deficient psychological capital group(19.7%), medium psychological capital group(52.5%), and affluent psychological capital group(27.9%). Compared with the deficient psychological capital group, the results of a disordered multi-classification logistic regression analysis showed that the factors influencing the participants of the medium psychological capital group were their marital status (married OR = 1.081, 95% CI: 1.163– 7.468, p = 0.023), perceived stress (OR = − 0.2, 95% CI: 0.769– 0.872, p < 0.001), and insomnia (OR = − 0.273, 95% CI: 0.696– 0.833, p < 0.001). The factors influencing the affluent psychological capital group were perceived stress (OR = − 0.334, 95% CI: 0.664– 0.773, p < 0.001) and insomnia (OR = − 0.46, 95% CI: 0.56– 0.712, p < 0.001).
Conclusion: Three potential categories of psychological capital in ischemic stroke patients were identified. Sex, marital status, education, perceived stress, and insomnia were found to be associated with psychological capital in stroke patients. Future research should explore other determinants of psychological capital in ischemic stroke patients to formulate interventions that can improve their psychological capital.
Keywords: ischemic stroke, psychological capital, perceived stress, insomnia, latent profile analysis
Introduction
Ischemic stroke (IS) is a leading cause of disability and mortality worldwide, and imposes a significant burden on public health systems.1 It is influenced by various factors, including age, genetics, lifestyle, hypertension, diabetes, obesity, and atrial fibrillation. The rate of recurrence of stroke among patients within a year is 17%, while IS has a rate of rate of recurrence of 41% within five years.2,3 Advances in the prevention, early detection, and treatment of IS have led to improved patient outcomes and reduced mortality rates. However, the burden imposed by stroke in developing countries remains large because of limited resources and uneven access to healthcare.4,5 According to the systematic analysis provided by the Global Burden of Disease Study, China is the largest contributor to global neurological disability-adjusted life years (DALYs),6 which implies that the country has the highest incidence of stroke in the world. The high rate of recurrence of ischemic stroke has a significant negative impact on the physical and mental health of patients. A study of 919 patients with stroke found that poor wellbeing was prevalent in 279 of them (30.4%), while almost all patients reported abnormal fatigue.7 Therefore, developing positive psychological conditions in patients can contribute to the treatment of the diseases afflicting them and improve the quality of nursing care.
The psychological capital (PsyCap) is the positive developmental state of an individual that helps them cope with stress, and can be viewed as a self-regulating process of mobilizing one’s resources to manage challenging situations.8 To improve the motivation of stroke patients for treatment is the focus of clinical staff, because the long rehabilitation duration of stroke, some patients are easily to lose confidence in the later treatment.1 PsyCap as a positive psychological resource for stroke patients, the higher level of PsyCap, the more resilience patients are, the more willing they are to choose challenging rehabilitation tasks, and the more hope they are to devote their energy to managing stroke disease even when they encounter obstacles. This positive psychological resource can enhance stroke patients’ level of self-efficacy, promoting active patient participation in the management of stroke disease, which in turn improves the efficacy of treatment for stroke patients.9 Which means that individuals with a higher level of PsyCap have more flexible cognitive behavioral models, and are more likely to receive support from outside sources when dealing with intense stress.10 Thus, there is a need to focus on stroke patients’ PsyCap and the influence factors in order to identify patients with low level of PsyCap and lay the foundation for intervention.
The structure of the PsyCap of individuals is not completely uniform owing to their different cognitive levels.11 The psychological capital questionnaire (PCQ-26) was developed by Zhang et al,12 based on the theory of psychological capital developed by Luthans, and has been widely used in different contexts.13,14 There are no uniform standard that distinguish between different level of PsyCap and complex factors influencing PsyCap may be subject to heterogeneity between groups. The majority of previous studies on PsyCap of stroke patients have relied on variable-centered analyses, which is limited to exploring the correlation between variables and ignoring the existence of heterogeneity among individuals and may therefore draw over-generalized conclusions based on overall samples.15,16 On the contrary, latent profile analysis (LPA) is an individual-centered method that clusters the relevant data by using continuous explicit variables to allow for the exploration of population heterogeneity, to enable a more clarified understanding of symptom presentations.17
Clarifying the heterogeneity of PsyCap among stroke patients and the reasons for these differences may be vital for designing and implementing targeted interventions. However, there is a lack of research on PsyCap from an individualized perspective in order to visualize group heterogeneity in stroke patients. In light of this, we investigate the PsyCap of ischemic stroke patients by using LPA to identify the potential profiles of their psychological capital, and to explore subgroup heterogeneity and the factors influencing it. The results of our study will provide crucial information for nurses to develop precise strategies of intervention in case of mental health problems in stroke patients.
Materials and Methods
Design and Participants
This study used a cross-sectional design with latent profile analysis. The reporting was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (Figure S1).
From October 2023 to April 2024, patients receiving treatment and hospitalization in the neurological ward of the Affiliated Hospital of Guizhou Medical University by using convenience sampling. The criteria for the inclusion of the respondents were as follows: 1) age ≥ 18 years, 2) eligibility for the diagnostic criteria of the Chinese guidelines for the diagnosis and treatment of ischemic stroke, as confirmed by computed tomography or magnetic resonance imaging,18 and 3) informed and voluntary recruitment. The criteria for exclusion were as follows: 1) patients with acute or critical diseases, 2) patients diagnosed mental disorders, and 3) patients with language dysfunction who could not complete the questionnaire.
According to Kendall,19 the number of samples of the data needs to be at least five to 10 times the number of variables considered. 20 variables were considered in this study. Given the number of invalid samples and an expansion of the samples by 20%, the sample size was N=(20 × 10)/(1–0.2)=250. In addition, previous studies suggested a sample size of 300–1000 was recommended for LPA,20 and a minimum profile needs to include enough individuals(>30) to support generalizations,21 and the final number of samples was 427.
Data Collection
The purpose of our study was explained to the participants before they were asked to fill out the questionnaire to solicit their consent. The researchers answered any question that the participants had in detail during the survey. If the participants were unable to complete the questionnaires on their own, the researchers explained the items of the questionnaire separately to them, and filled in the questionnaire on their behalf according to their responses.
Instruments
Sociodemographic Characteristics
The sociodemographic characteristics of the participants that were collected included their sex, age, marital status, place of residence, education level, monthly income, and occupation. The disease-related information collected from them included data concerning hemiplegia, first hospitalization due to stroke (“yes” or “no”), the number of chronic diseases from which they suffered, the number of therapeutic drugs of chronic diseases, and National Institute of Health Stroke Scale(NIHSS) scores.
Psychological Capital
The psychological capital questionnaire (PCQ-26) developed by Zhang et al13 was used here. PsyCap was measured as adapted by Luthans et al.22 It contained 26 items along four dimensions: self-efficacy (seven items), resilience (seven items), hope (six items), and optimism (six items). Each item was rated on a seven-point scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). The score of PCQ-26 ranged from 26 to 182, and the PsyCap of a given participant increased with their total score. This scale is widely used, and is satisfactorily applicable to Chinese patients.23 The Cronbach’s α coefficient of the scale in this study was 0.936.
Perceived Stress
The perceived stress scale (PSS) was developed by Cohen et al24 to assess the perceived level of stress among participants. The Chinese version of the PSS (CPSS), developed by Yang and Huang,25 contains 14 items and two subscales: those related to a sense of being out of control (seven items) and a feeling of tension (seven items). Each item is rated on a five-point scale ranging from 0 (“strongly disagree”) to 4 (“strongly agree”). CPSS scoring uses two subscales, and its scores range from zero to 56. As the total score increases, so does the level of perceived stress in the corresponding participant. The reliability and validity of the CPSS have been proven, and it has been applied to stroke patients.26 The Cronbach’s α coefficient of the scale in this study was 0.828.
Insomnia
Insomnia was measured by using the Athens Insomnia Scale (AIS), which was developed as a sleep assessment tool to quantify the degree of difficulty encountered in sleeping according to the International Classification of Diseases-10th edition (ICD-10).27 The AIS contains eight items along two dimensions: the quantity and quality of sleep (five items), and daytime symptoms (three items). It uses a four-point Likert scale ranging from 0 (“no problem”) to 3 (“serious problem”), with the total score ranging from zero to 24. Higher AIS scores reflect higher levels of insomnia. Its validity and reliability have been verified in past research, and a total score above six is considered to reflect insomnia.28 The Cronbach’s α coefficient of the scale in this study was 0.878.
Statistical Analysis
Data analysis was performed by using SPSS 27.0 and Mplus 8.3 software. The scores of the participants on the 26 PsyCap items were entered for LPA, and profiles 1–5 were sequentially chosen for analysis.20 To identify the optimal number of latent profiles to fit the data, we compared several evaluation indices of each model, including the Akaike information criterion (AIC), Bayesian information criterion (BIC), sample size-adjusted Bayesian information criterion (aBIC), entropy, Lo–Mendell–Rubin likelihood ratio test (LMR), and bootstrapped likelihood ratio test (BLRT). Smaller values of the AIC, BIC, and aBIC, larger values of entropy (>0.8), and high levels of significance of the p-values of the LMR and BLRT (<0.05) were considered to represent a better model.
SPSS version 27.0 was used to compare the differences in sociodemographic characteristics between ischemic stroke patients, and their PsyCap was identified by using LPA. A chi-square (χ2) test and one-way ANOVA were used to compare the differences in the sociodemographic characteristics, perceived stress, and insomnia between profiles. The statistically significant indicators were subjected to multi-nomial logistic regression when the subgroups were compared to analyze the factors associated with the PsyCap of ischemic stroke patients. The differences were considered statistically significant at p<0.01 or p<0.05.
Ethics
This study complied with the Declaration of Helsinki and was approved by the Committee of Medical Ethics of the Affiliated Hospital of Guizhou Medical University (ethics approval number: 2024149). All the participants provided informed consent.
Results
Tests for Common Method Bias and Multicollinearity
Given that the data were collected by self-report methods, Harman’s univariate test was performed prior to data analysis using exploratory factor analysis to detect common method bias. The results showed that 16 factors had eigenvalues greater than 1, 65.85% of the variance. The first factor explained 27.51% of the variance, which was below the critical value of 40%.29 Therefore, there was no significant common method bias in this study.
For predictive analysis, multicollinearity diagnosis among observed variables was performed. The results showed that the tolerance index of each model(0.495–0.948) was less than 1, and the variance inflation factor(VIF) of independent variables were 1.055–2.018. According to the common rule of thumb that a VIF of 10 or above as a cutoff value for a large multicollinearity problem,30 the results indicate that there is no significant multicollinearity problem among the independent variables in the present study.
Participant Characteristics
The demographic characteristics and disease-related information of the ischemic stroke patients are presented in Table 1. A total of 427 participants were included in this study, and had a mean age of 60.32 years (SD=12.40; range, 20–88 years). A total of 59.95% of the patients were male, 55.5% were older than 60 years, 76.81% were married, 64.17% lived in urban areas, 35.36% had a junior high school diploma, 39.11% had a monthly income of less than 3000 yuan, and 26.93% were farmers. A majority of the ischemic stroke patients was not hemiplegic (N=292 [68.38%]), most of the participants had undergone their first hospitalization due to stroke [N=331 (77.52%)], and most of them had no chronic diseases (N=143 [33.49%]) or had only one chronic disease (N=156 [36.53%]).
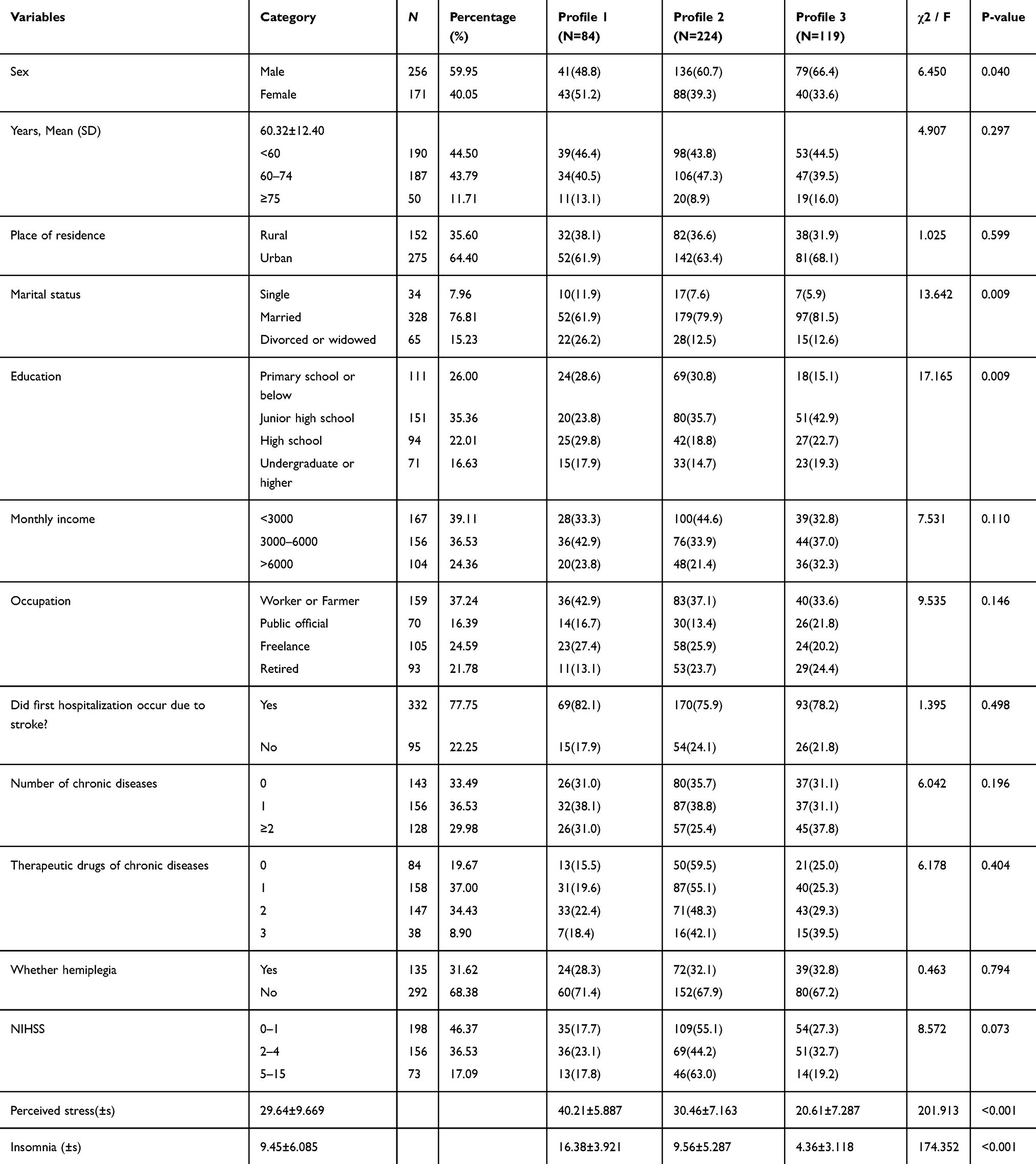 |
Table 1 General Information of Patients with Ischemic Stroke and Their Differences in Psychological Capital Latent Profile(N = 427) |
Latent Profile Analysis of Psychological Capital Among Participants
LPA was performed with 26 items as the input variables. Latent profile models 1–5 were selected for an exploratory LPA of the PsyCap of ischemic stroke patients (Table 2). The values of the AIC, BIC, and aBIC continuously decreased in all five profiles, but the entropy had the largest value in profile model 3, while the indicator for LMR was not significant in profile model 5 (p>0.05). Each indicator of profile model 4 was statistically significant, but it was considered to be too complex to be useful and thus did not provide clinical guidance. By combining the above results, we chose profile model 3 as the optimal latent profile model for ischemic stroke patients.
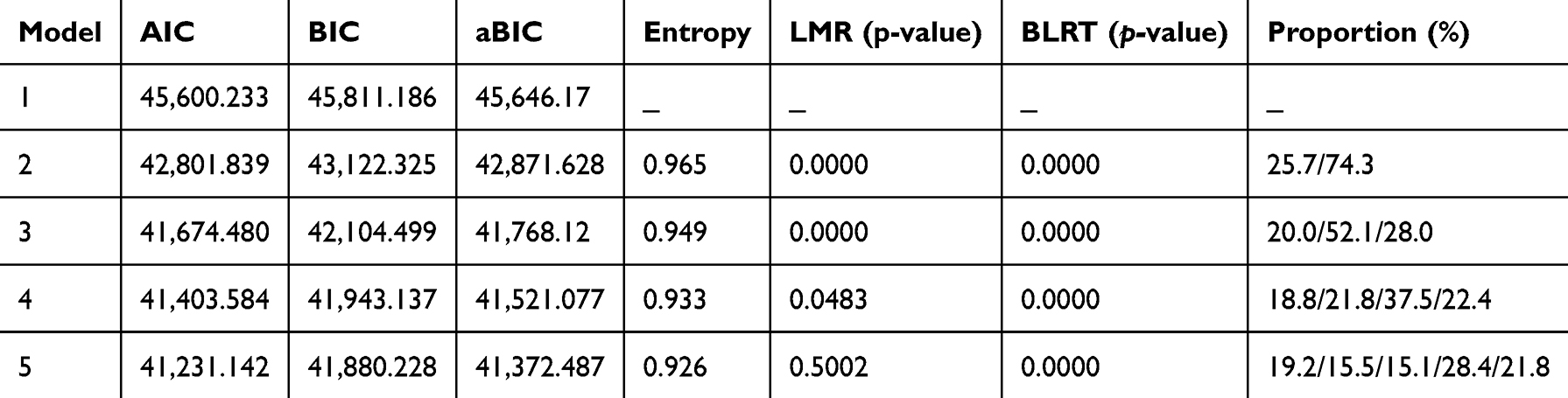 |
Table 2 Comparison of Indices of Fit Between Models |
Characterization of Psychological Capital Profile
Based on the results of latent classification, the scores of the three profiles on the 26 items of the PsyCap questionnaire are plotted in Figure 1. The total score for profile 1 was 59.80 ± 11.817, and the average score of all its items was lower than 4, indicating a low level of PsyCap. We called this profile the “deficient psychological capital group.” There were 84 ischemic stroke patients in this group (19.7%). Profile 2 had the highest proportion of participants, at 52.5%. The overall level of PsyCap of individuals in this profile (106.10 ± 10.792) was close to the moderate level of the conventional model, while the development of its items was uneven. Fluctuations were observed in both the dimensions of self-efficacy and resilience. We called this profile the “medium psychological capital group”, and it contained 224 individuals. The total score for profile 3 was 142.76 ± 11.242, and the average score of each item was above 4, but there were mild fluctuations in its dimension of self-efficacy. We called this class the “affluent psychological capital group”, and it comprised 119 patients, accounting for 27.8% of all participants.
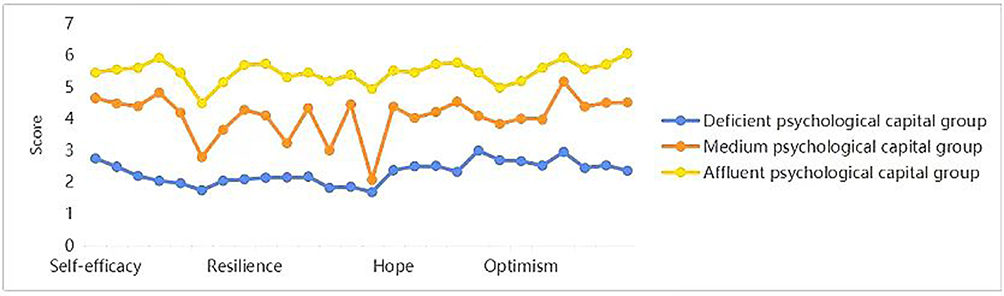 |
Figure 1 Latent profile model of psychological capital among ischemic stroke patients. |
Factors Influencing Psychological Capital Among Ischemic Stroke Patients
Sex, marital status, education, perceived stress, and insomnia were found to influence the profile of the psychological capital of ischemic stroke patients according to the results of a univariate analysis (p<0.05) (Table 1).
When profile 1 was used as the reference group, the results of disordered multi-classification logistic regression indicated that the participants’ marital status, perceived stress, and insomnia were statistically significant factors, as shown in Table 3. The factors influencing the participants of the medium psychological capital group were their marital status (married OR = 1.081, 95% CI: 1.163–7.468), perceived stress (OR = −0.2, 95% CI: 0.769–0.872), and insomnia (OR = −0.273, 95% CI: 0.696–0.833). The factors influencing the affluent psychological capital group were perceived stress (OR = −0.334, 95% CI: 0.664–0.773) and insomnia (OR = −0.46, 95% CI: 0.56–0.712).
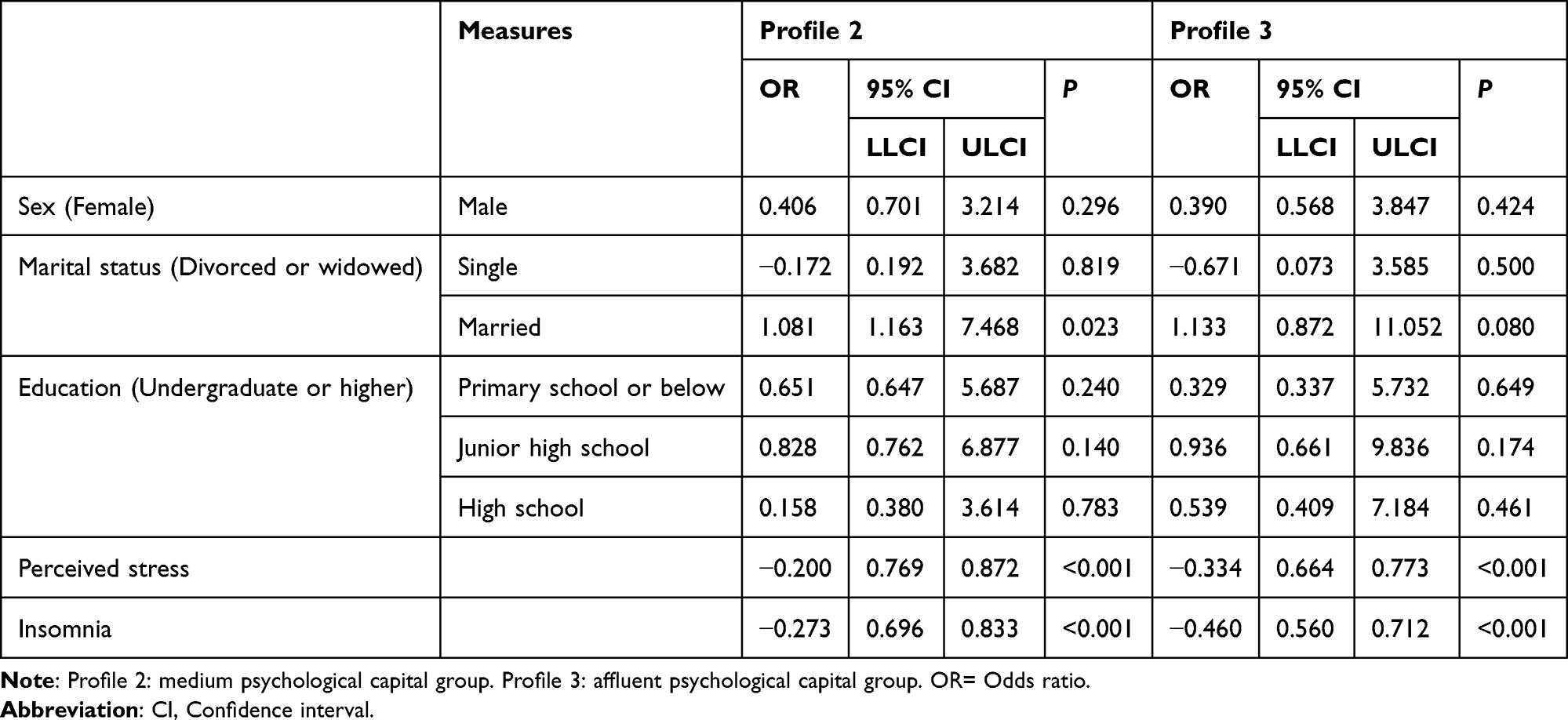 |
Table 3 Results of Multi-Nomial Logistic Regression |
Discussion
We used LPA to explore the types of PsyCap and the factors influencing them in ischemic stroke patients. We eventually classified the participants into three potential profiles: the “deficient psychological capital group”, “medium psychological capital group”, and “affluent psychological capital group.” The medium psychological capital group had the highest proportion of participants, 52.5%, with scores of 106.10 ± 10.792. These scores are lower than those reported for the PsyCap of stroke patients by He et al.15 Moreover, the affluent psychological capital group accounted for only 28% of the participants, suggesting that the PsyCap of most ischemic stroke patients in China is low. This can be attributed to the fact that stroke patients typically suffer from long-term physical and psychological health issues.31 These findings are beneficial for nurses and clinicians to better understand the heterogeneous and clustered classification of PsyCap in stroke patients, and plan more targeted interventions to improve the quality of care for them. A study by Hu et al32 on patients with coronary heart disease showed that positive psychological intervention improved the negative cognition of the individuals, helped them regulate their psychological and emotional problems, and enhanced their sense of wellbeing.
We also considered the factors influencing the latent profile of PsyCap. We found that the marital status of stroke patients in the medium psychological capital group was a more influential factor than for patients in the deficient psychological capital group. Wu and Yan found a significantly positive correlation between PsyCap and the marital status of medical staff,33 which is consistent with the findings of Bouzanjani et al.34 A husband, wife, or family is an individual’s spiritual harbor, and an important source of social support. If patients can obtain affirmation, recognition, and support from marriage, their PsyCap and self-efficacy can be enhanced. However, these results may be related to the fact that the participants of our study included a larger number of married people. Therefore, nurses should pay more attention to stroke patients who are single, divorced, or widowed, seek to alleviate their psychological stress, and encourage their family members to provide psychological support to them to enhance their PsyCap. As an important resource, PsyCap can alleviate and regulate stress among people. This is because it can help patients adapt to their stressful environment, encourage them to accept, face, and accommodate the development of the disease, and alleviate negative emotions and unfavorable mental states, such as anger, helplessness, and anxiety.
This study also found that perceived stress was an influential factor for both the medium psychological capital group and the affluent psychological capital group. Previous studies have shown that perceived stress is negatively associated with PsyCap in patients with chronic diseases.35 Studies have shown that CPSS have satisfactory internal consistency and alphas, the two-factor structure(sense of being out of control and feeling of tension) for CPSS has also been widely validated in China.36,37 A meta-analysis has also shown that perceived psychological stress is associated with an increased risk of total ischemic stroke (HR=1.40),35 which means that perceived stress not only directly affects the physical health of the individual, but also affects their mental health.38 Perceived stress is the degree to which an individual perceives a stimulus as stressful. Prather et al39 found that stress was prevalent among stroke patients, since lacking of knowledge about disease, fearing of disease progression and heavy financial burden were the main sources of stress. When individual faced perceived stress can mobilize their own internal and external resources to cope with stressful events, PsyCap as a positive psychological resource, stroke patients with lower level of PsyCap are more likely are they to experience tension and feel helpless about the future.40 As a result, they are mentally unable to come to terms with their physical condition, and have a low level of wellbeing.41 On the contrary, stroke patients with less perceived stress are more likely to have resilient and optimistic attitudes, a higher degree of acceptance of the disease and compliance with the treatment, and better wellbeing.42 Therefore, in addition to caring for the physical symptoms of patients, nurses should implement effective psychological interventions to help them, such as relaxation training, Baduanjin, and health education. This can reduce the perceived stress of patients and promote their recovery from disease.
In addition, insomnia was found to be an influential factor for the medium psychological capital group and affluent psychological capital group. The negative correlation between insomnia and PsyCap has been reported in previous studies.43 A meta-analysis showed that 14 studies on the prevalence of post-stroke insomnia or symptoms of insomnia identified 38.2% stroke patients (95% CI, 30.1–46.5).44 In China, 40% of old adults were suffered from sleep disturbance or insomnia, as defined by a cut-off score on the AIS(≥6).45,46 In the COVID-19 pandemic, a cross study have examined the prevalence of insomnia symptoms with screener of insomnia AIS and Pittsburgh Sleep Quality Index(PSQI), finally, similar results were discovered.47 According to the theory of sleep disturbance, illness depletes the PsyCap of patients, and since overall PsyCap is limited and difficult to replenish in short term, if psychological resource depletion is not replenished in time, it would cause to insomnia symptoms.48 Patients with higher levels of PsyCap will actively acquire and replenish psychological resources during the treatment period, thus maintaining the normal mental activities of patients and the insomnia symptoms will disappear.49 Du et al50 found that insomnia was negatively correlated with PsyCap among Chinese nurses, which is similar to the results of this study. In fact, stroke patients were more likely to suffer from insomnia owing to long-term treatment and emotion disorders.
Limitations
This study has several limitations that should be noted. First, the list of influential factors considered here was not exhaustive. Second, the sample was limited to patients in Guizhou, China, and the results may vary when patients from different geographical areas of the country are considered. Third, this study used a cross-sectional design, because of which the relevant causal relationships were not verified. Therefore, multi-center longitudinal clinical studies with large sample sizes are needed in future research to clarify the causal relationships between the variables considered, so that precise interventions can be developed and implemented.
Conclusion
In summary, this is study to use LPA to identify three profiles of the psychological capital of stroke patients: deficient, medium, and affluent. Patients belonging to different profiles were found to differ in terms of their sex, marital status, education, perceived stress, and insomnia. Comparisons between these groups of stroke patients can help medical staff better understand the factors influencing them, and can provide a theoretical basis for developing helpful interventions.
Data Sharing Statement
The dataset supporting the conclusions of this study can be shared with the corresponding author via e-mail.
Funding
This study was supported by the Science and Technology Fund Project of the Guizhou Provincial Health Commission (gzwkj2022-489).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brief report on stroke prevention treatment in China Writing Group. Brief report on stroke prevention treatment in China, 2021. Chin J Cerebrovasc Dis. 2023;20(11):783–793.
2. Chen Y, Wright N, Guo Y, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0·5 million Chinese adults. Lancet Glob Health. 2020;8(4):e580–e590. doi:10.1016/S2214-109X(20)30069-3
3. Feigin VL, Nichols E, Alam T, GBD 2016. Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
4. Kim AS, Cahill E, Cheng NT. Global stroke belt: geographic variation in stroke burden worldwide. Stroke. 2015;46(12):3564–3570. doi:10.1161/STROKEAHA.115.008226
5. Zheng H, Wu K, Wu W, et al. Relationship between the cumulative exposure to atherogenic index of plasma and ischemic stroke: a retrospective cohort study. Cardiovasc Diabetol. 2023;22(1):313. doi:10.1186/s12933-023-02044-7
6. Feigin VL, Stark BA, Johnson CO. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
7. Damsbo AG, Kraglund KL, Buttenschøn HN, et al. Predictors for wellbeing and characteristics of mental health after stroke. J Affect Disord. 2020;264:358–364. doi:10.1016/j.jad.2019.12.032
8. Hcy H, Chui OS, Chan YC. When pandemic interferes with work: psychological capital and mental health of social workers during COVID-19. Soc Work. 2022;67(4):311–320. doi:10.1093/sw/swac035
9. Virga D, Baciu L, Lazăr T-A, Lupsa D. Psychological capital protects social workers from burnout and secondary traumatic stress. Sustainability. 2020;12(6):2246. doi:10.3390/su12062246
10. Fredrickson BL. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am Psychol. 2001;56(3):218–226. doi:10.1037//0003-066x.56.3.218
11. Youssef-Morgan CM, Luthans F. Psychological capital and well-being. Stress Health. 2015;31(3):180–188. doi:10.1002/smi.2623
12. Zhang K, Zhang S, Dong Y. Positive psychological capital: measurement and its relationship to mental health. Stud Psychol Behav. 2010;8(1):58–64.
13. Yuan Z, Zhang X, Wang F, et al. Levels of psychological capital among nurses: a systematic review and meta-analysis. Int Nurs Rev. 2023;70(1):89–96. doi:10.1111/inr.12803
14. Hazan-Liran B, Miller P. Psychological capital’s mediation of anxiety-related patterns of thinking and academic adjustment among university students. J Am Coll Health. 2023;1–11. doi:10.1080/07448481.2023.2232867
15. He Y, Wang Y, Xie J, et al. Analysis of the mediating effect of psychological capital on the perception of social support and patient motivation in convalescent stroke patients. J Nurs. 2023;30(7):65–70.
16. Li XY. Correlation Between Positive Psychological Capital, Care-Dependent, Self-Care ability and Quality of Life in Stroke patients Gansu. University of Chinese Medicine.; 2024.
17. Chang H, Wang X, Wang Z. Latent profile analysis of successful aging among empty nesters in Guiyang, China. Aging Mental Health. 2024;28(4):667–674. doi:10.1080/13607863.2023.2265851
18. Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin J Neurol. 2018;51(9):666–682.
19. Kendall M. Kendall’s Advanced Theory of Statistics. Edward Arnold. Halsted Press; 2004.
20. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equ Model. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
21. Sherman NW. Statistics in Kinesiology. Vincent, Brigham Young University, Weir, Des Moines University; 2015:100–102.
22. Luthans F, Bruce JA, James BA, et al. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. 2007;3(60):541–572. doi:10.1111/j.1744-6570.2007.00083.x
23. Lv G, Zhao X, Xu X, Hou F, Li P. Gender-based differences in the relationships among social support, positive psychological capital, and sleep quality in patients implanted with pacemakers: a moderated mediation model. J Cardiovasc Nurs. 2022;37(1):79–85. doi:10.1097/JCN.0000000000000745
24. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
25. Yang TZ, Huang HT. An epidemiological study on stress among urban residents in social transition period. Chinese J Epidemiol. 2003;24(9):760–764.
26. Guo L, Wei M, Namassevayam G, et al. Is sleep quality a moderated mediator between perceived stress and depression among stroke patients? Front Public Health. 2023;11:1284197. doi:10.3389/fpubh.2023.1284197
27. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. 2000;48(6):555–560. doi:10.1016/s0022-3999(00)00095-7
28. Niu S, Wu Q, Ding S, Wu L, Wang L, Shi Y. Comparison of three measures for insomnia in ischemic stroke patients: Pittsburgh Sleep Quality Index, insomnia severity index, and Athens insomnia scale. Front Neurol. 2023;14:1118322. doi:10.3389/fneur.2023.1118322
29. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
30. Kutner M, Nachtsheim C. Applied Linear Regression Model. Neter J. 2004.
31. Feske SK. Ischemic Stroke. Am J Med. 2021;134(12):1457–1464. doi:10.1016/j.amjmed.2021.07.027
32. Hu YY, Jiang X, Mao FY, et al. Effect of positive event recording based on positive psychology on healthy behaviors and readmission rate of patients after PCI: a study protocol for a prospective, randomized controlled trial. Trials. 2022;23(1):1013. doi:10.1186/s13063-022-06964-9
33. Wu CX, Yan WJ. A study on the relationship between medical Staff’s psychological capital and their marital satisfaction. Chin J Health Psychol. 2017;25(2):207–210.
34. Allahyari Bouzanjani A, Bahadori P, Nikoonam P. Nurses’ empathetic behaviors: the direct and indirect effect of their spiritual orientation. J Relig Health. 2021;60(1):134–152. doi:10.1007/s10943-019-00966-9
35. Zou J, Liu Y. Perceived stress, positive psychological capital and health literacy in patients with multiple chronic conditions: a structural equation modelling. J Clin Nurs. 2024. doi:10.1111/jocn.17201
36. Deng Q, Ruoyu HU, Wang J, et al. Validity and reliability of the Perceived Stress Scale among cancer survivors. Chin Ment Health J. 2018;32:15–20.
37. She Z, Li D, Zhang W, et al. Three versions of the perceived stress scale: psychometric evaluation in a nationally representative sample of Chinese adults during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(16):8312. doi:10.3390/ijerph18168312
38. Booth J, Connelly L, Lawrence M, et al. Evidence of perceived psychosocial stress as a risk factor for stroke in adults: a meta-analysis. BMC Neurol. 2015;15(1):233. doi:10.1186/s12883-015-0456-4
39. Prather JG, Stanfill AG. An integrative review of the utilization of the perceived stress scale in stroke recovery. J Neurosci Nurs. 2023;55(2):65–71. doi:10.1097/JNN.0000000000000695
40. Gyawali P, Chow WZ, Hinwood M, et al. Opposing associations of stress and resilience with functional outcomes in stroke survivors in the chronic phase of stroke: a cross-sectional study. Front Neurol. 2020;11:230. doi:10.3389/fneur.2020.00230
41. Zheng WK, Heng CN, Tan YL, et al. Relationship among insomnia symptoms, neuroticism, anxiety symptoms and psychological capital in patients with COVID-19. Chin Ment Health J. 2024;38(2):151–157.
42. Du J, Wu C, Zheng W-K, et al. Insomnia and anxiety among COVID-19 patients in China: the chain mediating effect of psychological capital and self-esteem. BMC Nurs. 2024;23(1):221. doi:10.1186/s12912-023-01563-8
43. Lundh LG, Broman JE. Insomnia as an interaction between sleep-interfering and sleep-interpreting processes. J Psychosom Res. 2000;49(5):299–310. doi:10.1016/s0022-3999(00)00150-1
44. Baylan S, Griffiths S, Grant N, et al. Incidence and prevalence of post-stroke insomnia: a systematic review and meta-analysis. Sleep Med Rev. 2020;49:101222. doi:10.1016/j.smrv.2019.101222
45. Lu L, Wang SB, Rao W, et al. The prevalence of sleep disturbances and sleep quality in older Chinese adults: a comprehensive meta-analysis. Behav Sleep Med. 2019;17(6):683–697. doi:10.1080/15402002.2018.1469492
46. Zhong BL, Zhou DY, He MF, et al. Mental health problems, needs, and service use among people living within and outside Wuhan during the COVID-19 epidemic in China. Ann Transl Med. 2020;8(21):1392. doi:10.21037/atm-20-4145
47. Zhang QQ, Li L, Zhong BL. Prevalence of insomnia symptoms in older Chinese adults during the COVID-19 pandemic: a meta-Analysis. Front Med Lausanne. 2021;8:779914. doi:10.3389/fmed.2021.779914
48. Wang MF, Shao P, Wu C, et al. The relationship between occupational stressors and insomnia in hospital nurses: the mediating role of psychological capital. Front Psychol. 2023;13:1070809. doi:10.3389/fpsyg.2022.1070809
49. Stephan Y, Sutin AR, Bayard S, Križan Z, Terracciano A. Personality and sleep quality: evidence from four prospective studies. Health Psychol. 2018;37(3):271–281. doi:10.1037/hea0000577
50. Du J, He SZ, Li MJ, et al. The relationship between psychosocial job stressors and insomnia: the mediating role of psychological capital. Nurs Open. 2023;no 2:1693. doi:10.1002/nop2.1693
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unveiling Psychological Capital Profiles and Their Impact on Quality of Life in Breast Cancer Patients: A Latent Profile Analysis
Cui C, Liu H, Wang L
Cancer Management and Research 2025, 17:2429-2440
Published Date: 22 October 2025
The Relationship Between Midwives’ Psychological Capital and Core Competency: A Latent Profile Analysis
Ni S, Zhang A, Zhu Z, Jiang L, Li L, Xue X, Wang J, Li L, Fan X, Xu M
International Journal of Women's Health 2026, 18:585765
Published Date: 27 February 2026