Back to Journals » Psychology Research and Behavior Management » Volume 16
Influence of Weight-Control Attempts as Based on Self-Perception of Macronutrient Intake Among Young Females and Its Association with Mood Disorder
Authors Alharbi MH ![]()
Received 21 April 2023
Accepted for publication 12 August 2023
Published 22 August 2023 Volume 2023:16 Pages 3319—3331
DOI https://doi.org/10.2147/PRBM.S418005
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Mudi H Alharbi
Clinical Nutrition Department, College of Applied Medical Sciences, Taibah University, Madinah, 42353, Saudi Arabia
Correspondence: Mudi H Alharbi, Email [email protected]
Background: There are a few studies on the association between macronutrients and mood, but none on weight control based on self-perception of specific macronutrients and mood.
Objective: To assess the association between anxiety and depression levels and weight-control attempts among young females based on self-perception of diet that impacts weight by limiting or boosting a certain macronutrient.
Methods: A cross-sectional survey conducted on young females (n=302) with an age range of 19 to 29. Dietary intake was measured using the Food frequency questionnaire (FFQ) and 24h-dietary recall. Anxiety and depression were measured using the Hospital Anxiety and Depression Scale (HADS) questionnaire.
Results: Analysis of the data showed a significant and inverse association of macronutrients – carbohydrates (OR 0.86; 95% CI 0.77– 0.95; p < 0.01), protein (OR 0.87; 95% CI 0.78– 0.97; p < 0.05), and fat (OR 0.79; 95% CI 0.63– 0.99; p < 0.05) – with the odds of abnormal anxiety was noted. In addition, lower omega-3 intake was significantly associated with abnormal anxiety score (OR 0.85; 95% CI 0.76– 0.97; p < 0.05) and abnormal depression score (OR 0.31; 95% CI 0.14– 0.68; p < 0.01). Increased calorie intake is associated with an increased risk of anxiety scores.
Conclusion: This preliminary study found the importance of monitoring dietary intake, especially macronutrients, among the young population to screen for any onset of mood symptoms, especially for those who are following a specific diet without any supervision. Young people should be aware of the importance of following a balanced diet and seek dietitians’ consultation.
Keywords: anxiety, depression, weight-control diet, macronutrients, self-perception of food
Introduction
Globally, anxiety and depression are the most common mental health disorders and the leading cause of life with disability and all-cause mortality.1 In the majority of cases, these two psychiatric illnesses are varyingly prevalent among the population with or without comorbidities. The prevalence of these illnesses is higher in women than men, with a ratio of 2:1.2,3 A study conducted in Tabuk in Saudi Arabia found that the prevalence of depression among young adult patients who visit primary health services has quite high rates.4 According to World Health Organization research, serious depression often first manifests in young adults between the ages of 20 and 40.5 Moreover, in Saudi Arabia, primary care visits have a high prevalence of depression as documented. It was discovered that screening for depression was substantially connected with females with more education.6 However, other studies found a higher prevalence of anxiety among young adults.7–9 It was linked to age.10 Studies suggest that the difference in risk may primarily stem from biological sex differences, mainly due to hormonal changes presented during puberty, menstruation, pregnancy, and menopause. Besides this, other confounding social and economic factors, including age-specific factors, genetic factors, race, culture, diet, education, income, self-imaging or self-perception, also potentially contribute to higher rates of depression among females.2,3 Self-perception of food may affect mood. Accordingly, dietary patterns impact mood disorders.11 Scientific evidence shows an association of dietary habits or patterns with anxiety and depression.1,12 A wholesome diet should consist of an adequate quantity of macronutrients and micronutrients.13,14 From birth to school-going age, through adolescence, to adulthood and old age, nutrient intake should support optimum growth and development and psychological stability.13 Clinical and epidemiological evidence has shown the beneficial impact of intake of micro- and macronutrients on humans’ psychological well-being, including sleep pattern, cognitive performance, and mental stability.15
In the literature, there is mixed research on combinations of macronutrients and individual macronutrients and their impact on mood disorders such as anxiety and depression. Regarding perspectives on the interplay between mental disorders and gut microbiota, studies show that diet can alter the gut microbiome and contribute to the pathophysiology of mental disorders by modulating brain-gut-microbiome interactions.16 In particular, in a number of ways, dietary fiber which exists in many foods, especially fruit and vegetables, benefits the gut microbiota and gut functions by promoting the growth of bacterial populations in the gut, and the production of beneficial metabolites such as short-chain fatty acids (SCFAs) and bioactive phenolic acids as the primary fuel source for bacterial fermentation. Because they fuel the microbiota, fermentable fibers are important contributors to mental health. In addition, these nutrients have been shown to lower anxiety and melancholy while also controlling the quantities of helpful microorganisms in the stomach.17 A recent study conducted on fiber in mood showed an association between the amount of fiber consumption and mood disorder.18 Moreover, carbohydrate-rich food improves the brain’s serotonergic function by the release of serotonin and tryptophan, which subsequently improves individuals’ cognitive performance.19 Further, inadequate intake of a type of fat which is an omega-3 predisposes individuals to psychiatric disorders such as depression.14 A high-fat diet containing omega-3 and monounsaturated fatty acids reduced anxiety scores.20 Likewise, reduced protein consumption is associated with depression and anxiety. In the context of combinations of macronutrients, a mixed diet containing low levels of carbohydrates and high levels of fat and protein is shown to have an impact on mood disorders.21 Also, a high-protein and low-fat diet increases the risk of moderate to severe depression in healthy adults.22 Similarly, a diet rich in saturated fat and sugar leads to metabolic dysfunction, which consequently increases the risk of psychiatric issues.23 A diet high in sugars also alters neurobiological brain functions, which impairs emotional processing and modifies behavior.24 A dietary intervention study reported that in young adults, increased intake (2–3 servings per day) of vegetables, nuts and seeds, fruits, protein, whole grains, and unsweetened dairy and reduced intake of refined carbohydrates, sugar, and fatty or processed foods improved depressive symptoms.25 More recent dietary modifications include a ketogenic diet consisting of a low-carbohydrate and high-fat diet, which has been proposed to have long-term benefits for overcoming anxiety disorders.26 Further, consumption of a varying composition of dietary macronutrients such as high-protein and low glycemic index27 or high or low protein content and glycemic index28 is also a part of a weight-control diet. Additionally, dietary modification including a calorie-restricted diet has been linked to weight loss and reduced depressive disorders.29
Based on these observations, it can be inferred that macronutrients have an impact on depression and anxiety. However, limited literature is available on the impact of macronutrients on young women’s mental illness or mood disorders. To date, mental illness, including mood disorders among young females, is under-researched in many countries, especially with weight-control diets. Based on the above considerations, the present study was designed to study the impact of types of macronutrients on depression and anxiety among young females who follow weight-control diets through self- perception of decreasing or increasing consumption of specific macronutrients.
The main objective of this study was to explore the association of mood status with the dietary intake of the selected macronutrient. Based on the literature review, it was hypothesized that “Reduced intake of certain macronutrients may be associated with anxiety and depression”.
Materials and Methods
This study is a part of a project that is based on a survey data collection of food consumption and mood status. The present cross-sectional study was conducted on 302 young female students or employees in Al Madinah region in 2018/2019. In this study, anxiety and depression were the dependent variables and levels of selected macronutrients were independent variables.
Sample Size Calculation
According to The General Authority for Statistics (GASTAT),30 Saudi Arabia has a total young adults population of around 37% of the country’s total population, with a 90% confidence interval, a 5% margin of error, and 10% non-response rate. The original predicted sample size of 272 was increased to 302.
Participants
A total of 302 young female students or employees in Al-Madinah region of Saudi Arabia between the ages of 19 and 29 years, who do not have any complications, have not used supplements for at least one month, do not exercise regularly, and are attempting to control weight by following a specific diet such as a low-calorie diet or low carb diet, or high protein intake specifically eat less than (<1200 kcal/day) to maintain weight, and had a specific perception of the influence of specific macronutrients on weight such as carbs etc, and were not under the supervision of dietitians. As well as those who consented to participate were included in the study. Excluded categories include pregnant and lactating women and females who are smoking, or with chronic diseases such as diabetes or hypertension or with other psychiatric morbidities. In addition, young females using antidepressants or mood-affecting drugs such as corticosteroids for the long term, also those who are suffering from pre or postmenstrual syndrome (which affects mood status) were excluded from the study. Also, the timing of the data collection was not close to exam or menstrual cycle times, which can alter mood. The study was conducted according to the declaration of Helsinki, and participants signed informed consent before participating. Out of 370 participants, only 302 participants met the study criteria. Sixty-eight participants did not complete the survey or had one of the excluding criteria.
Data Collection Process
A survey was distributed via social media such as WhatsApp and/or email and/or face-to-face. Participants filled in the survey via link. The survey consisted of sociodemographic information including age, education level, marital status, height and weight to calculate BMI. Also, health and lifestyle questions to screen the eligibility of participants included some questions about psychological factors that may affect mood. Then the diet section, which included a 24-hour dietary recall and FFQ, then self-mood assessment tool (HADS).
Dietary Intake
A food frequency questionnaire (FFQ) and a 24-hour dietary method were used to assess the intake of macronutrients. For each participant, a detailed description of food and beverage portions or sizes taken was recorded. Participants have been instructed to measure the serving size by using household measurements or by using a hand portion size guide, eg a fist, palm, thumb, handful, tennis ball, etc. Dietary intake was analyzed using Dietplan7 (Forest field Software Ltd, West Sussex, United Kingdom) in the context of fibre (g), carbohydrates (g), cholesterol (mg), monounsaturated fat (g), polyunsaturated fat (g), saturated fat (g), fat (g), calories (kcal), protein (g), sugars (g), omega-3 (g), and water (g). Food consumption from FFQ was categorized according to Alharbi and Alarifi18 into the main three categories as follows: 1) No consumption or very low consumption, 2) Low-to-moderate consumption, and 3) Moderate-to-high consumption.
Mood Assessment Tool
To determine depression and anxiety, participants were provided with a standard self-reporting questionnaire –the Hospital Anxiety and Depression Scale (HADS). This questionnaire contains 14 items to measure anxiety (7 items) and depression (7 items). The HADS questionnaire is validated universally and has a sensitivity and specificity value of above 0.7 for both anxiety and depression scores.31 The response to the questionnaire was collected from each participant via email or WhatsApp or by face-to-face interview. Based on the total score for depression and anxiety, the participants were divided into three categories – scores of 0–7 were assigned to the normal group (without depression or anxiety), and scores of 8–10 were assigned to the borderline-abnormal depression or anxiety group (borderline cases), and scores of 11–21 were assigned to the abnormal depression or anxiety group (case group).
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) software version 24.0 was used to perform statistical analysis. The collected data were computed for frequency, percentage, mean, and standard deviation. Values are displayed as mean ± standard deviation (SD) for continuous variables using ANOVA to detect differences between variables, and as percentages for qualitative variables using chi-squared testing to find differences between variables. Logistic regression was performed to analyze the relationship between the odds ratios (OR) of anxiety or depression and macronutrients. The statistical significance for all the tests was set at a level of p < 0.05.
Results
The characteristics of participants with no risk of depression (normal), borderline-abnormal depression, and abnormal depression are presented in Table 1. ANOVA analyses showed that age (F = 1.52, p > 0.05), and BMI (F = 0.46, p > 0.05) of participants were not significantly different among participants with no risk of depression. While energy or calorie intake (F = 52.73, p<0.05) was significantly different between participants with a risk of depression. Additionally, marital status (χ2= 4.41, p > 0.05), and psychological factors (χ2=6.39, p>0.0.05; χ2=8.46, p>0.0.05), showed no association with depression. On the other hand, education level (χ2=14.11, p<0.0.05), income (χ2=14.08, p<0.0.05), and types of diets (χ2=18.45, p<0.0.05) showed association with depression.
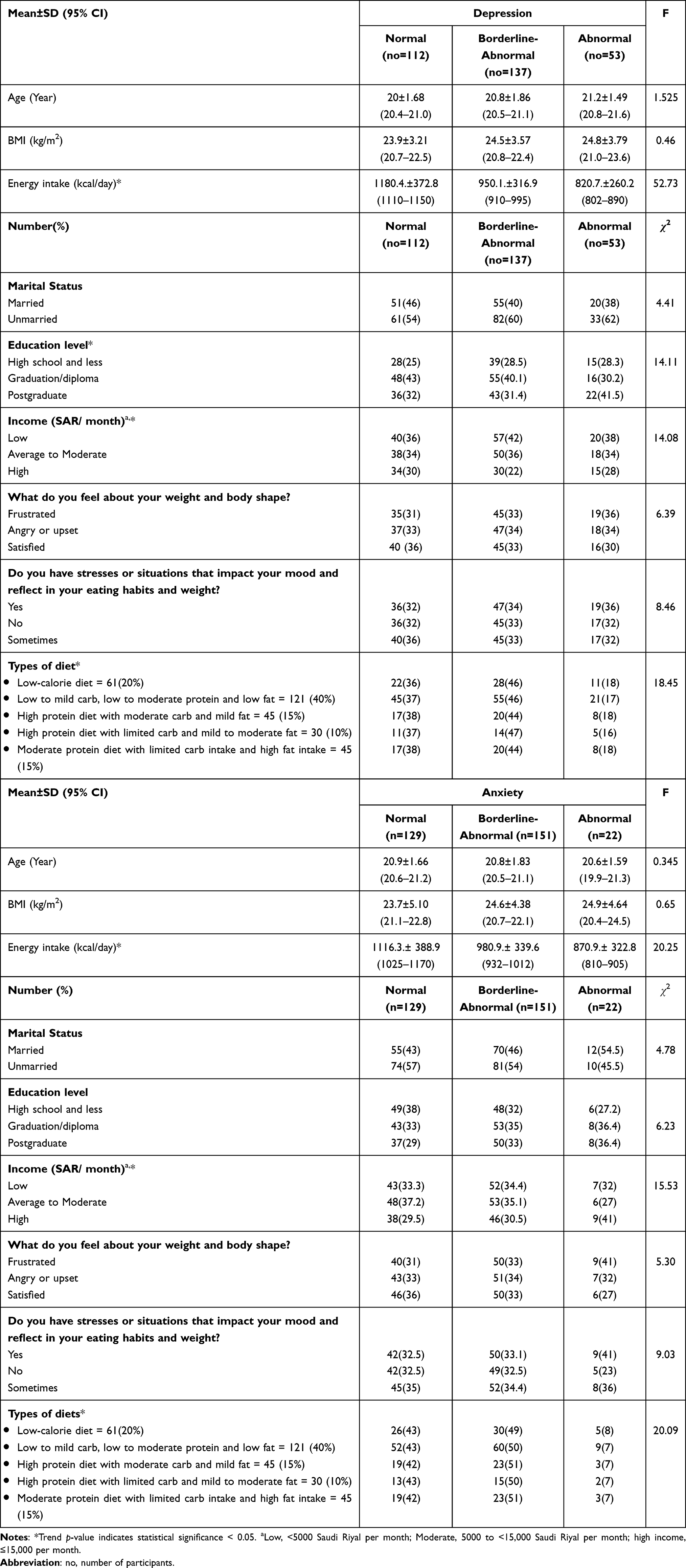 |
Table 1 Characteristics of Sample Based on Depression and Anxiety |
In the context of anxiety, ANOVA analysis revealed that age (F = 0.34, p > 0.05) and BMI (F = 0.65, p > 0.05) of participants were not significantly different among participants with no risk of anxiety. However, energy intake was significantly different between participants (F=20.25, p<0.001) with a risk of anxiety. The estimated calorie or energy intake was lower in women with abnormal anxiety (870.9±322.8 kcal) than women with borderline-abnormal anxiety (980.9±339.6 kcal) or with no anxiety (1116.3±388.9 kcal). Additionally, marital status (χ2 = 4.78, p > 0.05), education level (χ2= 6.23, p > 0.05), and psychological factors (χ2=5.30, p>0.0.05; χ2=9.03, p>0.0.05) showed no association with anxiety. In contrast, income (χ2=15.53, p<0.05), and types of diets (χ2=20.09, p<0.0.05) showed association with anxiety.
The percentage of the dietary consumption of the participants based on FFQ is presented in Figure 1.
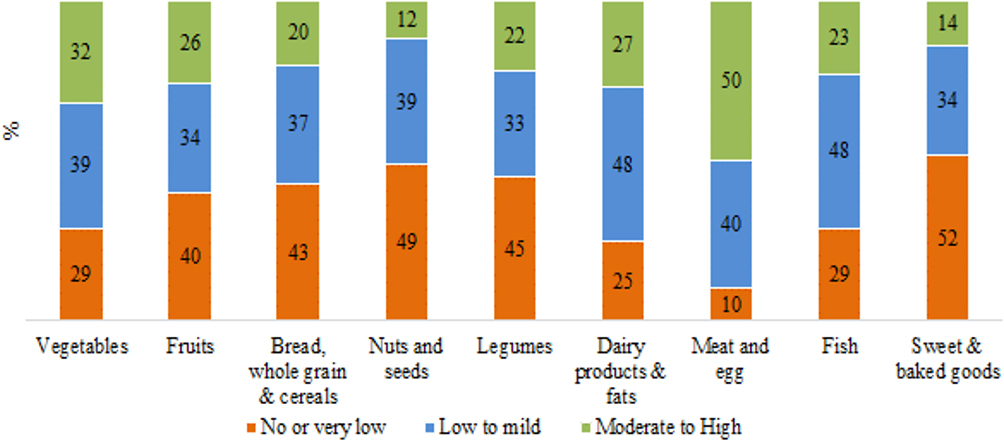 |
Figure 1 Percentage of the dietary consumption of the participants based on FFQ. Notes: Fat included animal fat and vegetable fat. Fish, mostly included tuna. |
Table 2 presents the impact of macronutrients on borderline-abnormal anxiety and abnormal anxiety as obtained from the multinomial logistic regression analysis. A significant increase in the OR for borderline-abnormal anxiety was observed for calories (OR 1.03; 95% CI 1.01–1.06; p = 0.011). A significant but inverse relation was found between borderline-abnormal anxiety and macronutrients such as carbohydrates (OR 0.89; 95% CI 0.89–0.98; p = 0.016), fat (OR 0.78; 95% CI 0.63–0.96; p = 0.011), protein (OR 0.88; 95% CI 0.80–0.97; p = 0.014), and omega-3 (OR 0.91; 95% CI 0.86–0.97; p = 0.002). The negative beta values of carbohydrates (β = −0.12), fat (β = −0.25), protein (β = −0.13), and omega-3 (β = −0.09) indicate that every single unit of increase in carbohydrates, fat, protein, and omega-3 will decrease borderline-abnormal anxiety. Likewise, a significant increase in the OR for abnormal anxiety was observed for calories (OR 1.04; 95% CI 1.01–1.06; p = 0.005). A significant but inverse relation was found between abnormal anxiety and macronutrients such as carbohydrates (OR 0.86; 95% CI 0.77–0.95; p = 0.004), fat (OR 0.79; 95% CI 0.63–0.99; p = 0.043), protein (OR 0.87; 95% CI 0.78–0.97; p = 0.011), and omega-3 (OR 0.85; 95% CI 0.76–0.97; p = 0.012). The negative beta values of carbohydrates (β = −0.15), fat (β = −0.24), protein (β = −0.14), and omega-3 (β = −0.16) indicate that every single unit of increase in carbohydrates, fat, protein, and omega-3 will reduce the risk of abnormal anxiety. Other macronutrients such as fiber (OR 1.05; 95% CI 0.99–1.12; p = 0.11), sugars (OR 0.99; 95% CI 0.98–1.01; p = 0.38), monounsaturated fat (OR 0.99; 95% CI 0.89–1.10; p = 0.84), polyunsaturated fat (OR 0.95; 95% CI 0.81–1.11; p = 0.52), and saturated fat (OR 0.96; 95% CI 0.86–1.07; p = 0.45) had no impact on anxiety. Overall, the data indicate a significant association between the risk of anxiety and macronutrients in young females.
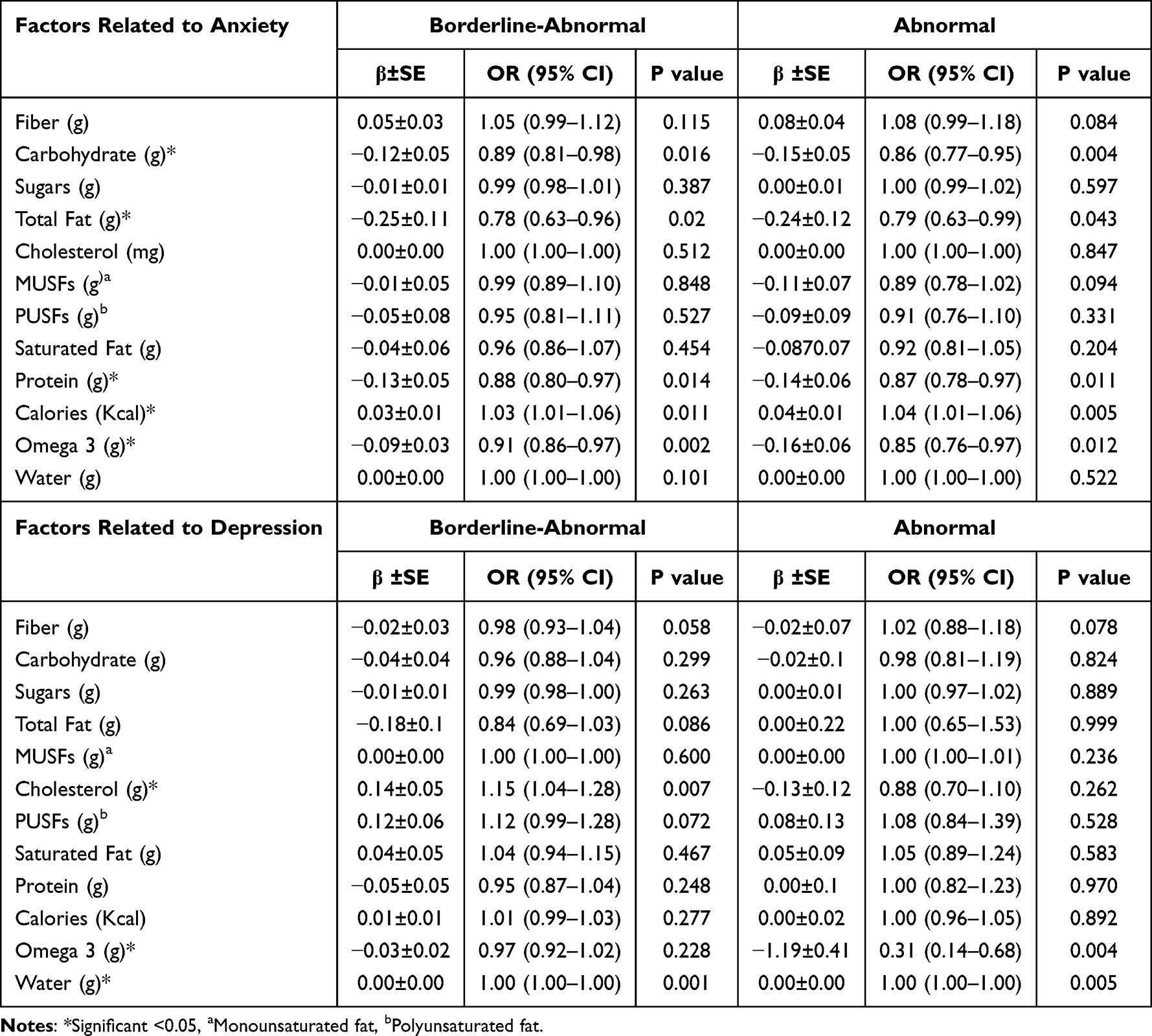 |
Table 2 Odds Ratios and 95% Confidence Intervals for Anxiety and Depression According to Macronutrients |
The impacts of macronutrients on borderline-abnormal depression and abnormal depression as obtained from the multinomial logistic regression analysis is presented in Table 2. A significant increase in the odds of borderline-abnormal depression was observed for cholesterol (OR 1.15; 95% CI 1.04–1.28; p = 0.007). Further, a significant but inverse relation was found between abnormal depression and omega-3 (OR 0.31; 95% CI 0.14–0.68; p = 0.004), indicating that every single unit of increase in omega-3 will reduce abnormal depression. Other macronutrients such as fiber (OR 1.02; 95% CI 0.88–1.18; p = 0.078), carbohydrates (OR 0.98; 95% CI 0.81–1.19; p = 0.82), polyunsaturated fat (OR 1.08; 95% CI 0.84–1.39; p = 0.52), saturated fat (OR 1.05; 95% CI 0.89–1.24; p = 0.58), and protein (OR 1.00; 95% CI 0.82–1.23; p = 0.97) had no impact on depression.
Further analysis of the case processing summary for the anxiety group showed that out of 302 female participants, 45.4% had a risk of borderline-abnormal anxiety and 17.5% had a risk of abnormal anxiety, while the remaining 37.1% had no risk of anxiety (normal). The model fit was significant (χ2 (24) = 47.482, p < 0.01), indicating the association between macronutrients and risk of anxiety. The pseudo-R2 values for three metrics, namely Cox and Snell (0.145), Nagelkerke (0.167), and McFadden (0.076), indicated a moderate relationship between dependent and independent variables. Further, the likelihood-ratio tests indicate that carbohydrates (χ2 = 8.81, p < 0.05), calories (χ2 = 9.14, p < 0.05), protein (χ2 = 7.75, p < 0.05), and omega-3 (χ2 = 17.74, p < 0.01) significantly contributed to the prediction of anxiety (Table 3).
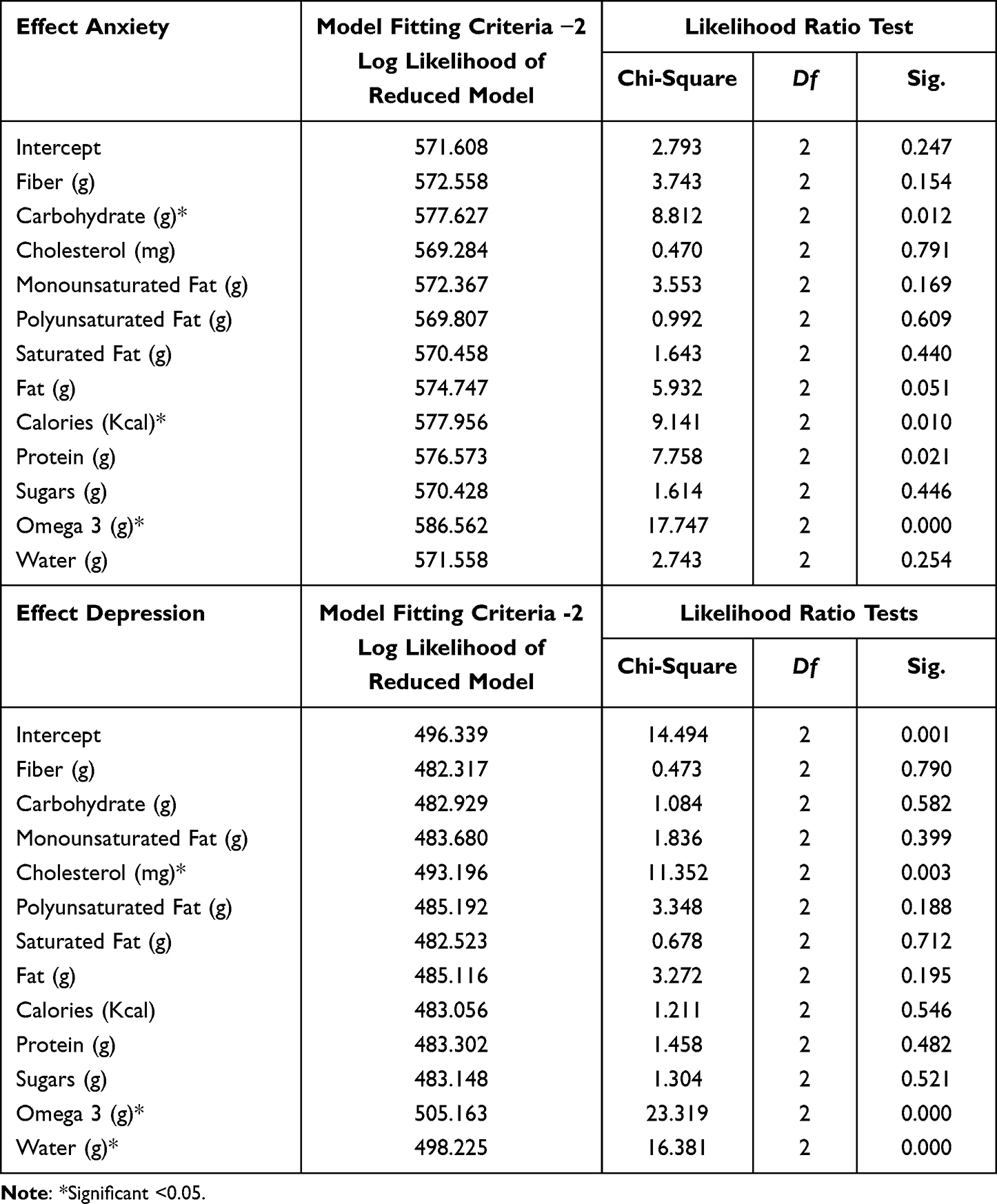 |
Table 3 Likelihood Ratio Tests for Anxiety and Depression |
Further analysis of the case processing summary for the depression group shows that out of 302 female participants, 50.0% had a risk of borderline-abnormal depression and 7.3% had a risk of abnormal depression, while the remaining 42.7% had no risk of depression (normal). The model fit was significant, as revealed by a significant chi-square value (χ2 (24) = 58.03, p < 0.01), indicating an association between selected macronutrients and the risk of depression. The pseudo-R2 values for Cox and Snell (0.175), Nagelkerke (0.209), and McFadden (0.107) suggest that 10% to 20.9% of the variation in depression could be predicted by micronutrients. Further, the likelihood-ratio tests indicate that cholesterol (χ2 = 11.35, p < 0.01) and omega-3 (χ2 = 23.31, p < 0.01) significantly contributed to the prediction of risk of depression.
Regarding the perception of the effect of specific macronutrients, about 20% of participants followed a low-calorie diet (lower in all macronutrients) and 40% of participants followed a diet with low to mild carbohydrates, low to moderate protein and low fat. A high protein diet with moderate carbohydrates and mild fat was followed by 15% and a high protein diet with limited carbohydrates and mild to moderate fat was followed by 10% of participants, and finally, about 15% followed a moderate protein diet with limited carbohydrate intake and high fat intake.
Discussion
The present cross-sectional study revealed an association of individual macronutrients, specifically carbohydrates, protein, fat, and omega 3, with anxiety and depression. In the context of macronutrients, it was found that low carbohydrate intake was associated with a risk of borderline-abnormal anxiety and abnormal anxiety. In agreement with this finding, Yarizadeh et al32 reported that after adjusting for women’s age, BMI, physical activity, and total energy intake, low carbohydrate intake was associated with mood disorders including anxiety and depression. By contrast, in a cross-sectional study, adults on a low-carbohydrate, high-fat, and high-protein diet showed no signs of mood disorders such as depression and anxiety21,33 Further, an association of carbohydrate intake with mood disorders was also noted in a mouse model. It was found that mice fed with diets high in refined carbohydrates showed anxiety and depression disorders,34 whereas dietary patterns containing complex carbohydrates provided stability to personality characteristics such as trait anxiety among females.33 Carbohydrate metabolism releases glucose in the blood, thereby stimulating the release of serotonin and tryptophan in the brain, which has a calming effect on mood. It could be posited that a healthy diet with an adequate quantity of macronutrients can prevent mood disorders. However, a diet containing healthy and complex carbohydrates such as whole grains can be beneficial in reducing symptoms of anxiety.
In the context of protein, low protein intake was associated with a risk of borderline-abnormal anxiety and abnormal anxiety. About 40% of participants consumed a moderate to high protein diet accompanied by mild to moderate consumption of other macronutrients such as carbohydrate and fat. In line with the present study, Khanna and Aeri35 found that reduced protein intake, in particular low consumption of protein-rich foods such as milk and legumes, increased depression and anxiety among adolescent boys and girls. Likewise, in a mouse model, a low-protein diet was associated with behavioral changes such as memory loss and anxiety.36 Pooyan et al22 noted reduced symptoms of depression after intake of a high-protein diet in healthy adults. In addition, a ten-year follow-up study concluded that protein-rich food can improve mood and behavior.37 The possible link between the association of protein intake and depression is attributed to high levels of tryptophan and serotonin, which have a positive effect on mood. In relation to this, in a cross-sectional study, tryptophan intake reduced depressive symptoms among young and middle-aged women.38
The findings of the present study showed an association between lower fat intake and risk of borderline and abnormal anxiety scores, which was in concordance with studies supporting the association of fat or lipids with anxiety disorder. According to Nakajima et al,39 in a high-fat diet, lipid composition containing saturated fatty acid is the deciding factor in mood changes, including those related to anxiety. Although the association of anxiety with unsaturated (mono- and poly-) and saturated fat could not be established in the present study, a cross-sectional study showed that saturated fatty acids increased anxiety, while other fatty acids including MUFAs, oleic acid, alpha-linolenic acid, and polyunsaturated fatty acids (PUFAs) reduced anxiety among women.20 The present study also showed an association of higher cholesterol with the risk of borderline-abnormal depression. In the literature, the association between cholesterol and depression is not yet conclusive. However, a disturbance in the lipid profile has been observed in the population suffering from major depressive disorders.40 In addition, outcomes varied among types of population, such as children, young adults, and the elderly. However, studies that show an association base their arguments on the fact that cholesterol contributes to depression by altering the inflammatory profile and serotonergic receptor function, and by interfering with the hypothalamic-pituitary-adrenocortical (HPA)-axis, thereby contributing to depression.41 In the present study, the type of cholesterol contributing to depressive symptoms was not identified. Nevertheless, in one study, the depressive mood among young adolescent boys was associated with higher levels of low-density lipoprotein (LDL), but the authors did not find this association significant in young girls.41 In a meta-analysis review consisting of 11 case-control studies with a heterogeneous population, elevated triglyceride and decreased high-density lipoprotein (HDL) showed an association with first episodes of major depressive disorder (MDD).42
Omega-3 is related to the proper functioning of neurons. In the present study, omega-3 intake had an impact on borderline-abnormal anxiety, abnormal anxiety, and abnormal depression. Lower omega-3 was associated with the risk of depression and anxiety. However, in the literature, researchers have reported inconsistent results regarding the impact of omega-3 on mental disorders.43 A decreased level of omega-3 fatty acids is known to increase the rate of depression.44 In an intervention study, supplementation of omega-3 fatty acids lowered the depression rate.45 An accepted dose of 1–2 g/day for a normal person without mood disorders and 9.6 g/day for patients with mood disorders is recommended to prevent incidences of mood disorders.44 Liu et al46 reported that reduced levels of omega-3 could alleviate depressive disorders in people who suffer from a severe anxiety disorder. Further, in the present study, the association of anxiety and depression with a type of omega-3 was not addressed. However, Jacka et al47 found that docosahexaenoic acid (DHA), a type of omega-3 found in fish, was effective in reducing depression and anxiety among women of ages ranging from 20–93 years. It is acknowledged that DHA plays a role in hippocampal neurogenesis and potentially prevents depression.48 Su et al49 found that in a heterogeneous population across 11 countries, omega-3 treatment was effective in reducing anxiety symptoms. However, contrary to studies supporting the effect of omega-3 in reducing mood disorders, a pool study of 31 clinical trials showed no impact of omega-3 on depression or anxiety symptoms. Further, the dose of an omega-3 supplement ranging from 0.95 g/d to 1.1 g/d for a duration of 6 months to 12 months had little or no effect on the prevention of depression or anxiety symptoms.50 Yet scientific evidence has shown that omega-3 fatty acids, proteins, and certain vitamins and minerals are the precursors of intracerebral neurotransmitters such as dopamine, glutamate, aspartate, and serotonin, which affect mood and aggression in individuals.44 Overall, from the study, it can be gathered that any decrease in macronutrients may directly affect the behavior of individuals.
Further, in the context of a weight-control diet containing a low-calorie and low carbohydrate diet, a poor diet containing low amounts of healthy macronutrients such as carbohydrates from whole grains or omega-3 fats can lead to poor mental health via multiple biological pathways including hormonal or inflammatory pathway.51 On the contrary, certain studies report benefits of a calorie-restricted diet in reducing depression score, however, those studies were mainly performed on obese people who took recommended dietary intervention to reduce body weight.29 Besides, with respect to the gut microbiome, emerging evidence indicates that the relationship between dietary pattern and depression or anxiety is bidirectional and is linked to gut microbiota.52 A diet containing vegetables, dietary fiber, milk and milk products is shown to improve microbiome diversity and mental health.53 Thus, it can be argued that planning of a weight control diet based on self-perception of macronutrients and without any guidance from a diet expert can have a negative effect on the gut microbiota and subsequent mood.
The present study has certain limitations. First, FFQ and the 24-hour dietary recall method and participants’ reports on portion sizes are subject to error. In addition, biochemical data may be beneficial in this case. The study was limited to young female students and professionals who worked in Al Madinah region. Also, sex-specific differences in depression and anxiety have been reported. Thus, this data cannot be generalized to men. A standard questionnaire was used to measure anxiety and depression; therefore, extending the outcomes to subjects with clinically diagnosed depression or anxiety may not be applicable. Despite these limitations, the study validates the impact of individual macronutrients on depression and anxiety, especially among those who attempt to follow a weight-control diet based on controlling the amount of macronutrient intake to lose weight or to maintain weight. To strengthen the outcomes and its applicability to a larger population, certain recommendations for future research are outlined. Research to identify the contribution of types of omega-3 fatty acids and lipid composition to anxiety and depression should be done. Further, dietary interventions involving supplements for omega-3 or protein supplements should be conducted. Since anxiety and depression peak in early adulthood, a similar study on males in the same age category will highlight any sex-specific association between macronutrients and anxiety or depression. Thus, several studies conducted in Saudi Arabia4–10 have revealed that young Saudi women suffer from considerable rates of anxiety and depression. Probably one of the main issues that young Saudi women need to be aware of is adhering to a diet to lose weight under professional supervision. Further studies will include the female population from other cities of Saudi Arabia.
Conclusion and Implications for Research and Practice
Based on the outcomes, the present study showed an effect of weight management which is based on self-perception of specific macronutrients on mood. This study found an inverse association of macronutrients with the odds of depression and anxiety among young females who attempt to follow a weight-control diet. A lower dietary intake of carbohydrates, protein, and fat was associated with an increased risk of borderline-abnormal and abnormal anxiety scores. In addition, lower dietary intake of omega-3 was associated with an increased risk of both abnormal depression and abnormal anxiety scores. Thus, the findings of the present study have clinical implications. The results indicate the importance of profiling macronutrient intake in young females to predict the onset of symptoms of depression and anxiety. The awareness should be raised among young females to follow a balanced diet. However, they also should be aware of the effect of limited or increased specific diets or macronutrients without any consultation from dietitians. The practitioners should do a regular mood screening for young females who have a self-perception of the effect of a specific macronutrient on weight.
Finally, the study is important since there is a lack of research on this topic, if not internationally, then in the region. Because the importance of food and/or micro-macronutrients in the mind, mood, and cognitive function is well understood, it also has long-term health or physical and psychological repercussions, especially if the problem is not addressed. Continued reductions in any of the macronutrients for no medical cause may have significant physiological, physical, and psychological consequences if not compensated for, burdening countries and costing a lot of money to treat. This is a preliminary study; further investigations will include populations from other Saudi cities.
Abbreviations
BMI, Body Mass Index; MDD, Major Depressive Disorder; FFQ, Food frequency questionnaire; HADS, Hospital Anxiety and Depression Scale; Kg, kilograms; m, Meters; g, grams; SPSS, Statistical Package for the Social Sciences; ANOVA, Analysis of Variance; OR, Odds Ratios; PUFAs, Polyunsaturated Fatty Acids; MUFAs, Monounsaturated fatty, acids; HPA, Hypothalamic-Pituitary-Adrenocortical; LDL, Low-Density Lipoprotein; HDL, High-Density Lipoprotein; DHA, Docosahexaenoic Acid.
Data Sharing Statement
Data will be made available on request.
Ethics Approval and Consent to Participate
This study was carried out in accordance with the Declaration of Helsinki and a consent form was obtained from all participants before starting the questionnaire. This study was approved by the ethics committee of applied medical sciences at Taibah university no CLN201806.
Acknowledgments
I would like to thank the participants and all of those who voluntarily helped with the distribution of the study questionnaire throughout Al Madinah region.
Funding
No funding to declare.
Disclosure
The author declares that they have no competing interests.
References
1. Ljungberg T, Bondza E, Lethin C. Evidence of the importance of dietary habits regarding depressive symptoms and depression. Int J Environ Res Public Health. 2020;17(5):1616. doi:10.3390/ijerph17051616
2. Adwas A, Jbireal J, Azab A. Anxiety: insights into signs, symptoms, etiology, pathophysiology, and treatment. S Afr J Med Sci. 2019;2:80–91.
3. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
4. Al Balawi MM, Faraj F, Al Anazi BD, Al Balawi DM. Prevalence of depression and its associated risk factors among young adult patients attending the primary health centers in Tabuk, Saudi Arabia. Open Access Maced J Med Sci. 2019;7(17):2908. doi:10.3889/oamjms.2019.789
5. Organization WH. Conquering Depression: You Can Get Out of the Blues. WHO Regional Office for South-East Asia; 2001.
6. Abdulmajeed IA, Ferwana MS, Ur Rahman S, Al-Qadhi W. Adult depression screening in Saudi primary care: prevalence, instrument and cost; 2014.
7. Aljurbua FI, Selaihem A, Alomari NA, Alrashoud AM. A cross-sectional study on generalized anxiety disorder and its socio-demographic correlates among the general population in Saudi Arabia. J Fam Med Prim Care. 2021;10(10):3644.
8. Amr M, Amin TT, Saddichha S, et al. Depression and anxiety among Saudi University students: prevalence and correlates. Arab J Psychiatry. 2013;44(473):1–14. doi:10.12816/0000092
9. Alahmadi AM. Prevalence of anxiety among college and school students in Saudi Arabia: a systematic review. J Health Inform Dev Ctries. 2019;13(1):1.
10. Aloraini MI, Mohammad SM, Hejazi MS, et al. Prevalence of generalized anxiety disorder among Saudi youth during COVID-19 pandemic in Saudi Arabia. Int J Med Dev Ctries. 2020;4(12):2322–2327. doi:10.24911/IJMDC.51-1605818315
11. Weng -T-T, Hao J-H, Qian Q-W, et al. Is there any relationship between dietary patterns and depression and anxiety in Chinese adolescents? Public Health Nutr. 2012;15(4):673–682. doi:10.1017/S1368980011003077
12. Li Y, Lv M-R, Wei Y-J, et al. Dietary patterns and depression risk: a meta-analysis. Psychiatry Res. 2017;253:373–382. doi:10.1016/j.psychres.2017.04.020
13. Savarino G, Corsello A, Corsello G. Macronutrient balance and micronutrient amounts through growth and development. Ital J Pediatr. 2021;47(1):109. doi:10.1186/s13052-021-01061-0
14. Muscaritoli M. The impact of nutrients on mental health and well-being: insights from the literature. Front Nutr. 2021;8:656290. doi:10.3389/fnut.2021.656290
15. Constantin E-T, Fonseca S. The effect of food on mental health. Rev Int Educ Saúde e Ambient. 2020;3:1–17. doi:10.37334/riesa.v3i2.36
16. Horn J, Mayer DE, Chen S, Mayer EA. Role of diet and its effects on the gut microbiome in the pathophysiology of mental disorders. Transl Psychiatry. 2022;12(1). doi:10.1038/s41398-022-01922-0
17. Cronin P, Joyce SA, O’Toole PW, O’Connor EM. Dietary fibre modulates the gut microbiota. Nutrients. 2021;13(5):1655. doi:10.3390/nu13051655
18. Alharbi MH, Alarifi SN. Gender-based differences in the consumption of food rich in fibre and its relationship with perceived mood status: a Cross-Sectional Study. Healthcare. 2022;10(4):730. doi:10.3390/healthcare10040730
19. Dye L, Lluch A, Blundell J. Macronutrients and mental performance. Nutrition. 2000;16(10):1021–1034. doi:10.1016/S0899-9007(00)00450-0
20. Fatemi F, Siassi F, Qorbani M, Sotoudeh G. Higher dietary fat quality is associated with lower anxiety score in women: a cross-sectional study. Ann Gen Psychiatry. 2020;19(1):14. doi:10.1186/s12991-020-00264-9
21. Ebrahimpour-Koujan S, Keshteli AH, Afshar H, Esmaillzadeh A, Adibi P. Adherence to low carbohydrate diet and prevalence of psychological disorders in adults. Nutr J. 2019;18(1):87. doi:10.1186/s12937-019-0513-8
22. Pooyan S, Rahimi MH, Mollahosseini M, et al. A high-protein/low-fat diet may interact with Vitamin D-binding protein gene variants to moderate the risk of depression in apparently healthy adults. Lifestyle Genom. 2018;11(1):64–72. doi:10.1159/000492497
23. Fulton S, Décarie-Spain L, Fioramonti X, Guiard B, Nakajima S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol Metab. 2022;33(1):18–35. doi:10.1016/j.tem.2021.10.005
24. Jacques A, Chaaya N, Beecher K, Ali SA, Belmer A, Bartlett S. The impact of sugar consumption on stress driven, emotional and addictive behaviors. Neurosci Biobehav Rev. 2019;103:178–199. doi:10.1016/j.neubiorev.2019.05.021
25. Francis HM, Stevenson RJ, Chambers JR, Gupta D, Newey B, Lim CK. A brief diet intervention can reduce symptoms of depression in young adults – a randomised controlled trial. Matsuoka YJ, ed. PLoS One. 2019;14(10):e0222768. doi:10.1371/journal.pone.0222768
26. Włodarczyk A, Cubała WJ, Wielewicka A. Ketogenic diet: a dietary modification as an anxiolytic approach? Nutrients. 2020;12(12):3822. doi:10.3390/nu12123822
27. Zhu R, Fogelholm M, Larsen TM, et al. A high-protein, low glycemic index diet suppresses hunger but not weight regain after weight loss: results from a large, 3-years randomized trial (PREVIEW). Front Nutr. 2021;8(June):1–14. doi:10.3389/fnut.2021.685648
28. Larsen TM, Dalskov S-M, van Baak M, et al. Diets with high or low protein content and glycemic index for weight-loss maintenance. N Engl J Med. 2010;363(22):2102–2113. doi:10.1056/nejmoa1007137
29. Patsalos O, Keeler J, Schmidt U, Penninx BWJH, Young AH, Himmerich H. Diet, obesity, and depression: a systematic review. J Pers Med. 2021;11(3):1–19. doi:10.3390/jpm11030176
30. (GASTAT) TGA for S. Saudi youth in numbers; 2020. Available from: https://www.stats.gov.sa/sites/default/files/saudi_youth_in_numbers_report_2020en.pdf.
31. Stern AF. The Hospital Anxiety and Depression Scale. Occup Med. 2014;64(5):393–394. doi:10.1093/occmed/kqu024
32. Yarizadeh H, Setayesh L, Askarpour M, Keshavarz SA, Mirzaei K. The relationship between low carbohydrate diet score and mental health in overweight and obese women. Qom Univ Med Sci J. 2020;14(2):47–54. doi:10.29252/qums.14.2.47
33. Kose J, Fezeu LK, Touvier M, et al. Dietary macronutrient intake according to sex and trait anxiety level among non-diabetic adults: a cross-sectional study. Nutr J. 2021;20(1):78. doi:10.1186/s12937-021-00733-1
34. Santos CJ, Ferreira AVM, Oliveira AL, Oliveira MC, Gomes JS, Aguiar DC. Carbohydrate-enriched diet predispose to anxiety and depression-like behavior after stress in mice. Nutr Neurosci. 2018;21(1):33–39. doi:10.1080/1028415X.2016.1213529
35. Khanna P, Aeri BT. Association of quantity and quality of protein intake with depression and anxiety symptoms among adolescent boys and girls (13–15 Years) studying in public schools of Delhi. J Nutr Sci Vitaminol. 2020;66(Supplement):S141–S148. doi:10.3177/jnsv.66.S141
36. Sato H, Tsukamoto-Yasui M, Takado Y, et al. Protein deficiency-induced behavioral abnormalities and neurotransmitter loss in aged mice are ameliorated by essential amino acids. Front Nutr. 2020;7:23. doi:10.3389/fnut.2020.00023
37. Wolfe AR, Arroyo C, Tedders SH, Li Y, Dai Q, Zhang J. Dietary protein and protein-rich food in relation to severely depressed mood: a 10 year follow-up of a national cohort. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):232–238. doi:10.1016/j.pnpbp.2010.11.011
38. Suga H, Asakura K, Kobayashi S, Nojima M, Sasaki S. Association between habitual tryptophan intake and depressive symptoms in young and middle-aged women. J Affect Disord. 2018;231:44–50. doi:10.1016/j.jad.2018.01.029
39. Nakajima S, Fukasawa K, Gotoh M, Murakami-Murofushi K, Kunugi H. Saturated fatty acid is a principal cause of anxiety-like behavior in diet-induced obese rats in relation to serum lysophosphatidyl choline level. Int J Obes. 2020;44(3):727–738. doi:10.1038/s41366-019-0468-z
40. Broncel M, Serejko-Banb K. Is there a link between cholesterol level and the risk of developing depression. Open Med J. 2016;3(1):1.
41. Kim EJ, Hong J, Hwang J-W. The association between depressive mood and cholesterol levels in Korean adolescents. Psychiatry Investig. 2019;16(10):737–744. doi:10.30773/pi.2019.03.24
42. Wei Y-G, Cai D-B, Liu J, et al. Cholesterol and triglyceride levels in first-episode patients with major depressive disorder: a meta-analysis of case-control studies. J Affect Disord. 2020;266:465–472. doi:10.1016/j.jad.2020.01.114
43. Larrieu T, Layé S. Food for mood: relevance of nutritional omega-3 fatty acids for depression and anxiety. Front Physiol. 2018;9:1047. doi:10.3389/fphys.2018.01047
44. Rao TSS, Asha MR, Ramesh BN, Rao KSJ. Understanding nutrition, depression and mental illnesses. Indian J Psychiatry. 2008;50(2):77–82. doi:10.4103/0019-5545.42391
45. Freeman MP, Hibbeln JR, Wisner KL, et al. Omega-3 fatty acids: evidence basis for treatment and future research in psychiatry. J Clin Psychiatry. 2006;67(12):1954–1967. doi:10.4088/jcp.v67n1217
46. Liu JJ, Galfalvy HC, Cooper TB, et al. Omega-3 polyunsaturated fatty acid (PUFA) status in major depressive disorder with comorbid anxiety disorders. J Clin Psychiatry. 2013;74(7):732–738. doi:10.4088/JCP.12m07970
47. Jacka FN, Pasco JA, Williams LJ, Meyer BJ, Digger R, Berk M. Dietary intake of fish and PUFA, and clinical depressive and anxiety disorders in women. Br J Nutr. 2013;109(11):2059–2066. doi:10.1017/S0007114512004102
48. Kang JX, Gleason ED. Omega-3 fatty acids and hippocampal neurogenesis in depression. CNS Neurol Disord Drug Targets. 2013;12(4):460–465. doi:10.2174/1871527311312040004
49. Su KP, Tseng P-T, Lin P-Y, et al. Association of use of omega-3 polyunsaturated fatty acids with changes in severity of anxiety symptoms: a systematic review and meta-analysis. JAMA Netw Open. 2018;1(5):e182327. doi:10.1001/jamanetworkopen.2018.2327
50. Deane KHO, Jimoh OF, Biswas P, et al. Omega-3 and polyunsaturated fat for prevention of depression and anxiety symptoms: systematic review and meta-analysis of randomised trials. Br J Psychiatry. 2021;218(3):135–142. doi:10.1192/bjp.2019.234
51. Firth J, Gangwisch JE, Borsini A, Wootton RE, Mayer EA. Food and mood: how do diet and nutrition affect mental wellbeing? BMJ. 2020;369:m2382. doi:10.1136/bmj.m2382
52. Bear TLK, Dalziel JE, Coad J, Roy NC, Butts CA, Gopal PK. The role of the gut microbiota in dietary interventions for depression and anxiety. Adv Nutr. 2020;11(4):890–907. doi:10.1093/advances/nmaa016
53. Uemura M, Hayashi F, Ishioka K, et al. Obesity and mental health improvement following nutritional education focusing on gut microbiota composition in Japanese women: a randomised controlled trial. Eur J Nutr. 2019;58(8):3291–3302. doi:10.1007/s00394-018-1873-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025