")
Back to Journals » Journal of Pain Research » Volume 16
Influence of TRPV1 on Thermal Nociception in Rats with Temporomandibular Joint Persistent Inflammation Evaluated by the Operant Orofacial Pain Assessment Device (OPAD)
Authors Leite-Panissi CR, De Paula BB , Neubert JK, Caudle RM
Received 7 February 2023
Accepted for publication 5 May 2023
Published 15 June 2023 Volume 2023:16 Pages 2047—2062
DOI https://doi.org/10.2147/JPR.S405258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Keith
Christie RA Leite-Panissi,1 Bruna B De Paula,2 John K Neubert,3 Robert M Caudle2
1Department of Psychology, School of Philosophy, Science and Literature of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil; 2Department of Oral and Maxillofacial Surgery, University of Florida, Gainesville, FL, USA; 3Department of Orthodontics, University of Florida, Gainesville, FL, USA
Correspondence: Robert M Caudle, Department of Oral and Maxillofacial Surgery, University of Florida, Gainesville, FL, USA. PO Box 100416. 1395 Center Drive, Gainesville, FL, 32610, USA, Tel +1 352-273-6767, Fax +1 352-392-7609, Email [email protected]
Background:
Methods: We characterized the thermal orofacial sensitivity for cold, neutral, and hot stimuli during the development of TMD using the OPAD behavior test. In addition, we evaluated the role of transient receptor potential vanilloid 1 (TRPV1) expressing nociceptors in rats with persistent TMJ inflammation. The experiments were performed in male and female rats with TMJ inflammation induced by carrageenan (CARR). Additionally, resiniferatoxin (RTX) was administered into the TMJs prior CARR to lesion TRPV1-expressing neurons to evaluate the role of TRPV1-expressing neurons.
Results: We evidenced an increase in the number of facial contacts and changes in the number of reward licks per stimulus on neutral (37°C) and cold (21°C) temperatures. However, at the hot temperature (42°C), the inflammation did not induce changes in the OPAD test. The prior administration of RTX in the TMJ prevented the allodynia and thermal hyperalgesia induced by CARR.
Conclusion: We showed that TRPV-expressing neurons are involved in the sensitivity to carrageenan-induced pain in male and female rats evaluated in the OPAD.
Keywords: temporomandibular disorder, acute pain, TRPV1, operant assay, orofacial pain
Introduction
Temporomandibular disorder (TMD) has a multifactorial etiology, including biological and psychological inducers, which can lead to an inflammatory phenomenon. TMD involves the temporomandibular joint (TMJ), masticatory muscles, and associated structures and is characterized by acute or chronic pain.1 The symptoms of TMD include mandibular deviation during the opening, limited mandibular movements, headache, and TMJ pain. However, TMJ pain is the main reason patients seek treatment.2 The TMJ pain may be derived from its internal derangement during TMD, leading to an inflammation of the synovial membrane.3,4 This inflammation promotes macrophage/microglia activation in the TMJ, resulting in an increase in proinflammatory cytokines and chemokines followed by hyperexcitability of the nociceptive neurons.5–7
Indeed, the development of persistent pain in the TMJ involves an inflammatory cascade that includes proinflammatory cytokines, chemokines, and matrix metalloproteinases released in limbic structures. For example, TMJ inflammation increased transient receptor potential vanilloid 1 (TRPV1) expression in the hippocampus,8 and matrix metalloproteinases in the hippocampus and amygdala,9 suggesting a central sensitization driven by neuroinflammation. Emotional disorders have also been widely linked to the development of TMD.10,11
Joint inflammation can lead to highly responsive articular nociceptors for mechanical stimulation,12,13 which involves an increase in TRPV1.14 The transient receptor potential family of cation channels is involved in the perception of hot and cold temperatures and pain.15 The subtype TRPV1 is activated by heat (≥ 43°C), low pH, and capsaicin.16 In this perspective, Neubert et al17 demonstrated intracisternal treatment with resiniferatoxin (RTX), used as a lesioning agent that acts by opening the TRPV1 ion channel causing cytotoxicity and selectively deleting TRPV1-expressing neurons,18,19 blocked heat nociception at 48°C and 55°C in mice evaluated using the operant orofacial pain assessment device (OPAD). TRPV1 is expressed in the nerves and synovial lining cells of the TMJ.20 Also, it has been shown that many TMJ TRPV1-immunoreactive nerves are labeled with the neuropeptide calcitonin gene-related peptide that is involved in the mechanisms of nociception and inflammation in this orofacial structure.20 Within this perspective, TRPV1 antagonists were developed as pharmacological alternatives to treat chronic pain.21,22 In particular, when orally administered, A-784168 and A-795614 TRPV1 antagonists could to block thermal hyperalgesia induced by complete Freund’s adjuvant (CFA) in rats.23 Further, Ghilard et al24 have shown that acute or chronic administration of a TRPV1 antagonist results in a significant attenuation of both ongoing and movement-evoked nociceptive behaviors in a bone cancer pain model in mice.
Pain from inflammatory and neuropathic origins are the two most common types of chronic or persistent pain. In addition, TMJ-associated inflammation is one of the reasons for the pain reported by patients with temporomandibular disorders.25 Inflammation can occur in the synovial membrane (ie, synovitis) or the capsule (ie, capsulitis). It may result from local trauma, infection or degeneration, changes in collagen formation, or systemic polyarthritis, such as rheumatoid arthritis.26 Among patients with TMDs, about 80% present signs and symptoms of joint disease.27,28 It is noteworthy that among the categories for diagnosing TMD, including arthritis, arthralgia and arthrosis, the masticatory muscle pain is the most common.1,26,29 Therefore, the knowledge of the underlying pathobiology of TMJ diseases would benefit a substantial proportion of patients with TMDs.
TMJ inflammation is often produced in animals’ models through the intra-articular administration of carrageenan (CARR), CFA, mustard oil, formalin, or adenosine triphosphate (ATP).30,31 Notably, persistent inflammation in the TMJ induced by CFA correlates with anxiety-like behavior and pain responses.32 Although TMD can be evaluated from physical and psychological perspectives,13,33 therapies considering these two optics are still not applicable to clinical practice because of the lack of direct clinical and experimental evidence. Thus, approaches including this relation between persistent orofacial pain and anxiety behavior can contribute to the understanding of the role of TMD in emotional responses.
To assess pain in animal models, some tests usually employed to evaluate sensitivity originating in other body regions were adapted for the orofacial area. In particular, mechanical sensitivity is frequently assessed by applying a von Frey filament to the orofacial region. This procedure involves visual anticipatory cues because the animal’s eyes are unshielded. Furthermore, the researcher’s definition of a painful response may be as varied as a head withdrawal threshold to freezing which consists of attentive immobility and is also used to evaluate responses of fear and anxiety.17 To overcome these limitations and expand knowledge in orofacial pain, our group validated and characterized an operant assessment paradigm in rats with both hot30–35 and cold36 stimuli as well mechanical stimuli.37 We also evaluated this system using different pain models, including capsaicin-induced neurogenic inflammation,38 carrageenan-induced inflammation,33 and menthol-induced sensitization.35,36 For example, capsaicin-induced orofacial pain decreased the animals’ tolerance to push mechanical stimulus to achieve the reward, and prior treatment with morphine can alter this effect on OPAD.39 Also, through this operant assay, it was evidenced that intracisternal injection of the alpha2-adrenoreceptor agonist clonidine produced a dose-dependent increase in the licks, contacts, and reward intake in male and ovariectomized females injected with CARR in the TMD region. Interestingly, these parameters were not affected in ovariectomized females previously treated with estradiol.40 Another benefit is that this assay can measure pain over extended periods (1 to 2 months) without losing sensitivity.41,42
This study aimed to characterize thermal orofacial sensitivity during the development of TMJ inflammation using this operant behavior assay in male and female rats since evidence has suggested a sex difference in the development of pain sensitivity.43,44 In addition, we wanted to evaluate the role of TRPV1-expressing neurons in the nociceptive responses of rats (male and female) with persistent TMJ inflammation.
Methods
Animal Care
Experiments were performed with hairless male and female Sprague-Dawley rats (Charles River, Raleigh, NC) weighing 250–300g. Rats were housed in pairs at 22°C and 31% humidity-controlled rooms with a 12-hour light/dark cycle (lights on from 6 am-6 pm). Water and standard laboratory chow were available ad libitum when animals were not being tested, and animal weights were recorded weekly. The behavioral sessions were performed between 8 am and 12 pm. The experiments were carried out in compliance with the Association for Assessment and Accreditation of Laboratory Animal Care and with the University of Florida’s Institutional Animal Care and Use Committee (IACUC number approval 201408528).
Operant Orofacial Pain Assessment Device (OPAD)
The methods described by Anderson et al34 were used in this study. Rats were trained on the OPAD (Stoelting, Co., Wood Dale, IL) to press their faces into Peltier devices whose temperature could be heated or cooled to aversive temperatures. If they performed this task, they received access to a rewarding bottle filled with diluted sweetened condensed milk (1:2, milk: water). Food-fasted male and female rats (15 ± 1 hour) were trained until consistent behavior was observed at a neutral temperature (32°C). Measures include the number of reward bottle activations (licks), facial contact stimuli (face contacts) and lick/face ratio (number of licks divided by the number of facial contacts within a session). The lick/face ratio is used as a pain index as the number of licks per facial contact with the stimulus decreases when an animal experiences pain, even when the total number of licks remains constant.17 About six sessions (three times a week for two weeks) are sufficient to train rats to lick about 2000 licks during an 11-minute session.35 Following training, baseline measurements were obtained for three temperatures (21°C, 37°C, and 42°C) within a single session. This was accomplished by ramping the temperature several times throughout an 11 min session (Figure 1). The room temperature was maintained at 22°C ± 1°C for all behavioral tests. Rats were divided into three treatments: I: PBS, rats submitted to PBS intra_TMJ injections (n = 6–9); II: CARR, rats submitted to CARR intra_TMJ injections (n = 4–6); III: RTX + CARR, rats submitted to RTX followed 1 week by carrageenan (n = 4–6).
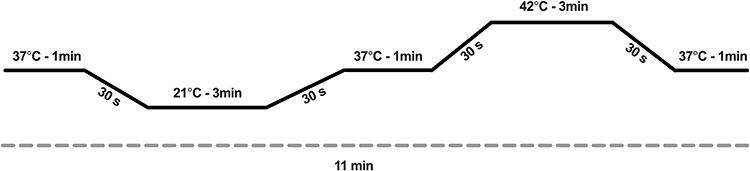 |
Figure 1 Temperature ramping of the thermode during testing sessions. |
TMJ Administration of the Carrageenan (CARR)
To examine the nociceptive behavior in rats with TMJ inflammation, rodents received CARR administration bilaterally in their TMJs one day after training on the OPAD. Briefly, rats were anesthetized by 2.5% isoflurane inhalation followed by bilateral intra-articular administration with 50µL of 1% CARR (C1867, Sigma-Aldrich, St. Louis, MO) in phosphate-buffered saline solution. Doses of CARR were based in previous studies.33,45 According to studies of Barretto et al,45 intra-articular injections with 50µL of 1% CARR in rats promoted an inflammatory infiltrate that was mainly centered in the retrodiscal region of the TMJ. The PBS group was injected with 50 µL of 0.9% phosphate-buffered saline solution. A 30 G ½” needle attached to a 1 mL plastic syringe was used for the injection. The zygomatic arch and the condyle were palpated to locate the TMJ for the injection. The needle was inserted immediately below the posteroinferior border of the zygomatic arch and advanced anteriorly to contact the edge of the posterolateral condyle.46 The same 11 min ramping protocol was repeated during different stages of temporomandibular inflammation. In this way, the nociceptive behavior was evaluated 1, 3, 5, 8, and 10 days after CARR administration into TMJ (Figure 2). At the end of the protocol, the rats were euthanized by 2.5% isoflurane inhalation followed by decapitation.
 |
Figure 2 Measuring nociception with the OPAD at 21°C, 37°C, and 42°C. (A) Licking contacts (Licks); (B) Facial contacts (Stimulus Contacts) and (C) Lick/Face ratio (L/F) during a training session in female (n = 12) and male (n = 12) rats. Data are expressed as the means ± the S.E.M. *P < 0.05 Bonferroni’s test compared to 37°C at the same sex. #P < 0.05 Bonferroni’s test compared to female group at the same temperature. |
TMJ Administration of the Resiniferatoxin (RTX)
The methods of Neubert et al17 were adapted for this study. Briefly, bilateral TMJ administration was achieved by injection of 50 μL RTX (250 ng, 0.25% Tween-80 in PBS, 0.05% ascorbic acid, kindly provided by Dr. Michael Iadarola). For this procedure, the skin overlying the TMJ was disinfected with Betadine. The zygomatic arch and the condyle were palpated to locate the TMJ. The needle was inserted immediately below the posteroinferior border of the zygomatic arch and advanced anteriorly to contact the edge of the posterolateral condyle.46 RTX was injected slowly by a 30 G ½” needle attached to a 1 mL plastic syringe. Rats recovered 1-week before behavioral testing. To evaluate the role of TRPV1 expressing neurons on nociceptive behavior in the OPAD in rats with TMJ inflammation, rodents received the RTX one day after training on the OPAD, and one week later, they were submitted to CARR bilaterally in the TMJs. The same 11 min ramping protocol was repeated during different stages of temporomandibular inflammation. Thus, the nociceptive behavior was evaluated 1, 3, 5, 8 and 10 days after CARR administration into TMJ. At the end of the experiment, the rats were euthanized by 2.5% isoflurane inhalation followed by decapitation.
Statistical Analysis
Statistical analyses were performed, including Student's t-test, One-way and Two-way repeated measures ANOVAs to evaluate the effects of temperature or treatment on the reward licking outcome measure. A general linear model for multivariate analysis was used to assess the effects of time and treatment on nociceptive behavior. When significant differences were found, post-hoc comparisons were made using Dunnett or Bonferroni’s test. All data in this study showed a normal distribution of scores as detected by Shapiro–Wilk and Kolmogorov–Smirnov tests. *P < 0.05 was considered significant in all instances.
Results
Rats were trained in the OPAD test at a constant neutral temperature of 37°C, and the number of licks, contacts, and lick/face ratio during the test were evaluated. The lick/face ratio represents an aversive score in the OPAD test.34,35 After baseline measurements with the cold/hot ramp as described in the methods (Figure 1), our results show that the number of licks is higher at 37°C compared to 21°C and 42°C in both female and male rats (p < 0.05; Figure 2).
Similarly, the lick/face ratio (L/F) is increased at 37°C compared to 21°C and 42°C in both female and male rats (p < 0.05; Figure 2). Moreover, the number of contacts is higher at 21°C compared to 37°C and 42°C in both female and male rats (p < 0.05; Figure 2). Additionally, the number of licks by male rats was lower compared to female rats at 21°C (p < 0.05; Figure 2); however, this difference was not found at 37°C and 42°C (p > 0.05). Moreover, the number of contacts and L/F at all temperatures between female and male rats did not differ (p > 0.05).
The effects of CARR-induced TMJ inflammation on the licks, contacts and aversive score are presented in Figure 3. CARR injections intra_TMJ bilaterally led to a reduction in the L/F ratio on Day 5 in females and Day 1 and 10 in males at 21°C compared to baseline and their respective PBS groups (p < 0.05).
 |
Figure 3 Effects of Carrageenan (CARR)-induced temporomandibular joint inflammation on orofacial sensibility at cold, neutral, and hot temperatures evaluated by the OPAD test (n = 6–9 per group). (A) Experimental design diagram; (B) Licks, (C) Face contact and (D) Lick/Face ratio in females at 21°C; (E) Licks, (F) Face contact and (G) Lick/Face ratio in males at 21°C; (H) Licks, (I) Face contact and (J) Lick/Face ratio in females at 37°C; (K) Licks, (L) Face contact and (M) Lick/Face ratio in males at 37°C; (N) Licks, (O) Face contact and (P) Lick/Face ratio in females at 42°C; (Q) Licks, (R) Face contact and (S) Lick/Face ratio in males at 42°C in the control period (Baseline) or after phosphate buffered saline solution saline (PBS, 0.9%, 50 μL) or carrageenan (CARR, 1% phosphate buffered saline solution, 50 μL) administration into the temporomandibular joint in male and female rats. Data are expressed as the means ± the S.E.M. *P < 0.05 Dunnett’s test compared to the respective Baseline. #P < 0.05 Bonferroni’s test compared to the respective PBS group. Abbreviations: S.E.M, standard error means; RT, ramping temperature. |
At 37°C, the number of face contacts was increased on days 1 and 5 in females and days 1 and 3 in males compared to baseline and their respective PBS groups (p < 0.05). However, there was a reduction in the L/F ratio on Days 1, 3, 5, and 8 in females and Days 1 and 3 in males at 37°C compared to baseline and their respective PBS groups (p < 0.05).
At 42°C, CARR-induced TMJ inflammation decreased the L/F ratio on day 1 in males compared to baseline (p < 0.05).
As shown in Figure 4, the role of TRPV1-expressing neurons in TMJ inflammation was evaluated following the administration of RTX into the TMJs. RTX prevented the changes in the number of licks, number of face contacts, and on the L/F ratio induced by TMJ treatment with CARR at 21°C, 37°C, and 42°C in male and female rats. Moreover, prior RTX increased the number of face contacts on Day 3 in females at 37°C compared to baseline during CARR-induced TMJ inflammation.
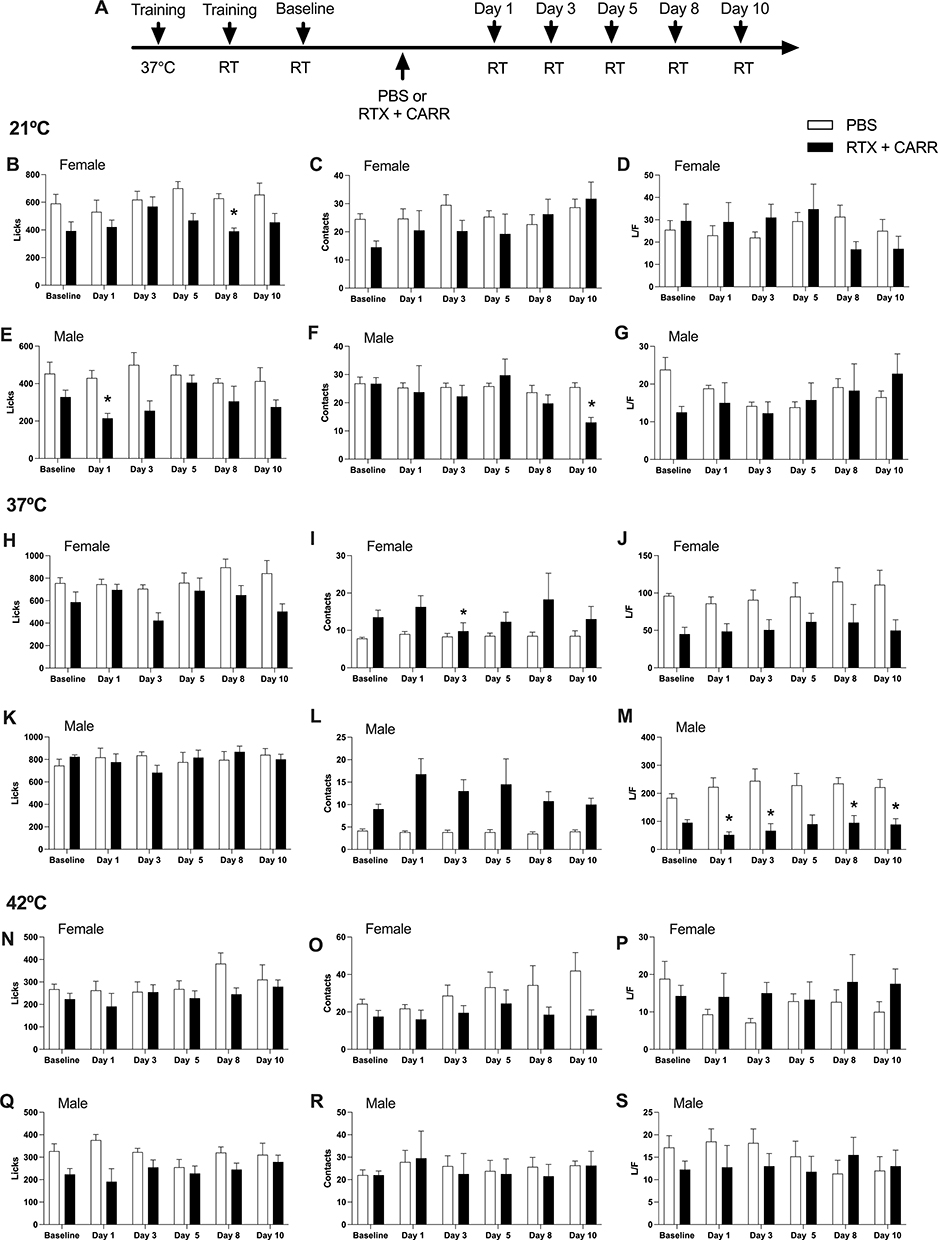 |
Figure 4 Effects of lesion of TRPV1 receptors on temporomandibular joint inflammation on orofacial sensitivity at cold, neutral and hot temperatures evaluated by the OPAD test (n = 4–6 per group). (A) Experimental design diagram; (B) Licks, (C) Face contact and (D) Lick/Face ratio in females at 21°C; (E) Licks, (F) Face contact and (G) Lick/Face ratio in males at 21°C; (H) Licks, (I) Face contact and (J) Lick/Face ratio in females at 37°C; (K) Licks, (L) Face contact and (M) Lick/Face ratio in males at 37°C; (N) Licks, (O) Face contact and (P) Lick/Face ratio in females at 42°C; (Q) Licks, (R) Face contact and (S) Lick/Face ratio in males at 42°C in the control period (Baseline) or after phosphate buffered saline solution saline (PBS, 0.9%, 50 μL) or after resiniferoxitoxin (RTX, 250 ng, 50 μL) followed 1 week by carrageenan (CARR, 1% phosphate buffered saline solution, 50 μL) administration into the temporomandibular joint in male and female rats. Data are expressed as the means ± the S.E.M. *P < 0.05 Dunnett’s test compared to respective Baseline. Abbreviations: S.E.M, standard error means; RT, ramping temperature. |
In addition, RTX promoted a reduction in the L/F ratio on day 10 at 21°C compared to the CARR group, while RTX promoted an increase in the L/F ratio on day 5 at 37°C (Figure 5).
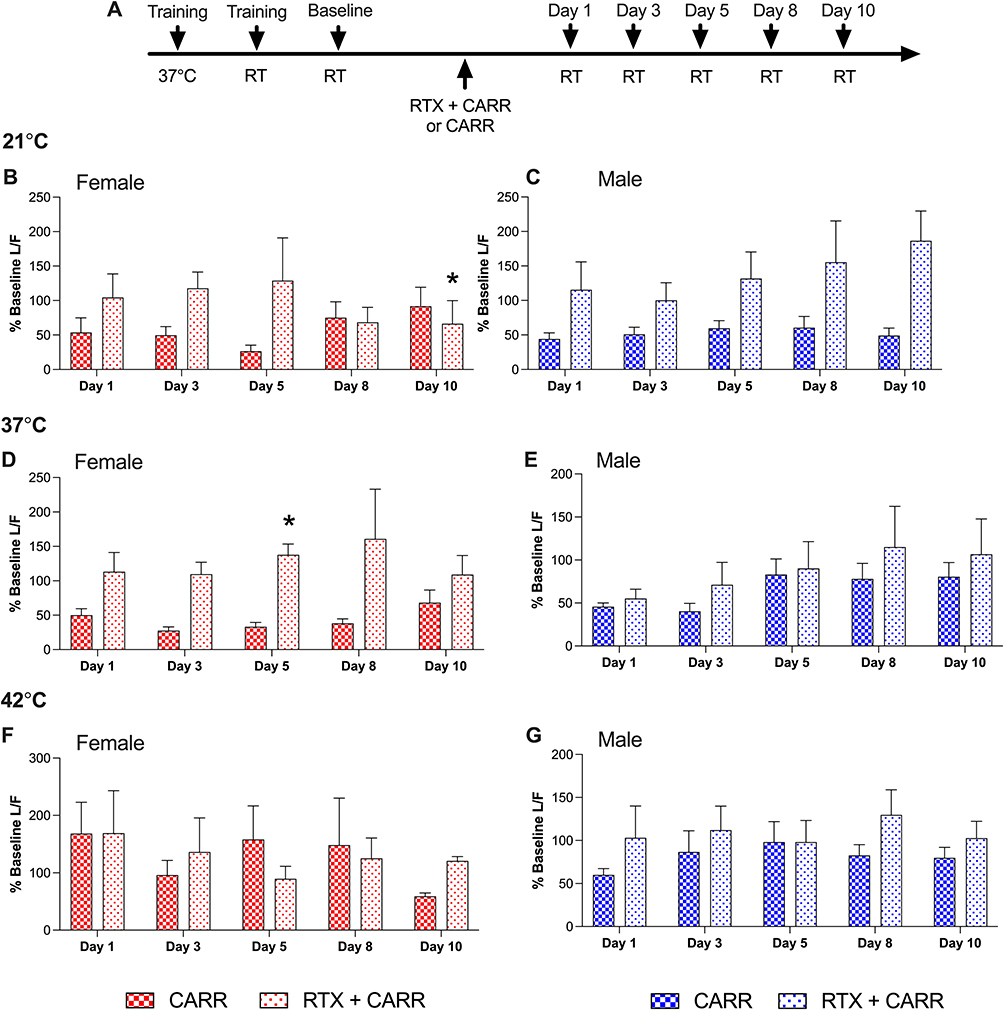 |
Figure 5 Effects of the RTX on the aversive score in CARR-induced tempomandibular inflammation at cold, neutral and hot temperatures evaluated in the OPAD test (n = 4–6 per group). (A) Experimental design diagram; (B) Lick/Face ratio in females at 21°C; (C) Lick/Face ratio in males at 21°C; (D) Lick/Face ratio in females at 37°C; (E) Lick/Face ratio in males at 37°C; (F) Lick/Face ratio in females at 42°C; (G) Lick/Face ratio in males at 42°C as a percent baseline (% Baseline L/F) for males and females that received carrageenan (CARR, 1% PBS, 50 μL) administration into the temporomandibular joint (TMJ) or that received pre-treatment intra-articular (TMJ) resiniferoxitoxin (RTX, 250 ng, 50 μL) followed 1 week by CARR. Data are expressed as the means ± the S.E.M. *P < 0.05 Bonferroni’s test compared to the respective to CARR group. Abbreviations: S.E.M, standard error means; RT, ramping temperature. |
The values of Fs and Ps for each data are described in Tables 1–5.
 |
Table 1 Statistical Analyses of the Pain Measures During Training of All Rats at 21°C, 37°C, and 42°C in the Orofacial Operant Pain Assessment Device (OPAD) |
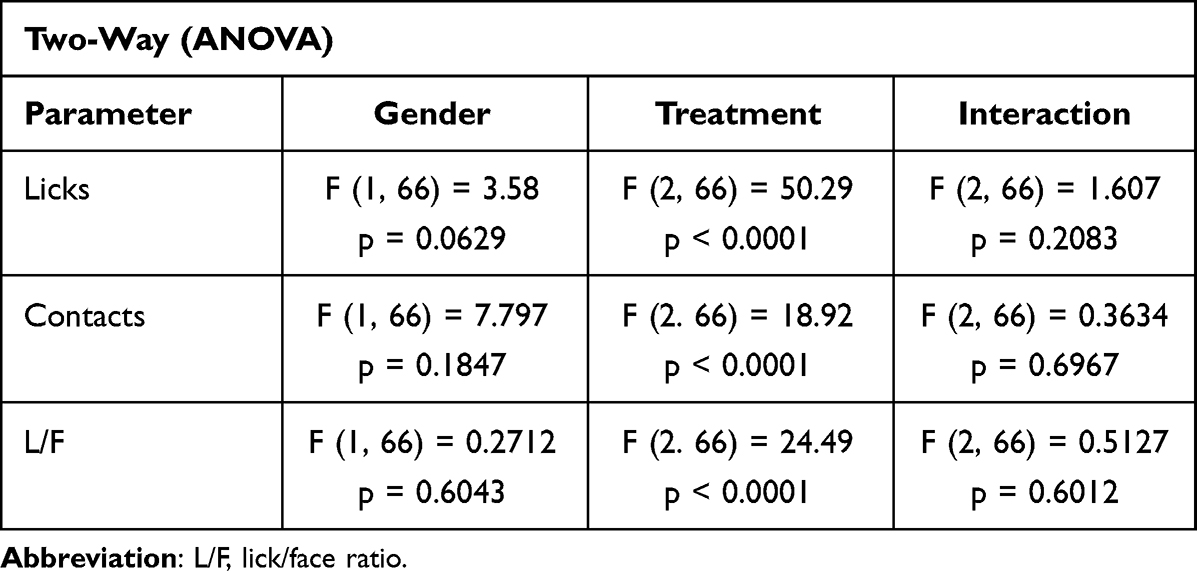 |
Table 2 Statistical Analyses of the Pain Measures During Training of Female and Male Rats at 21°C, 37°C, and 42°C in the Orofacial Operant Pain Assessment Device (OPAD) |
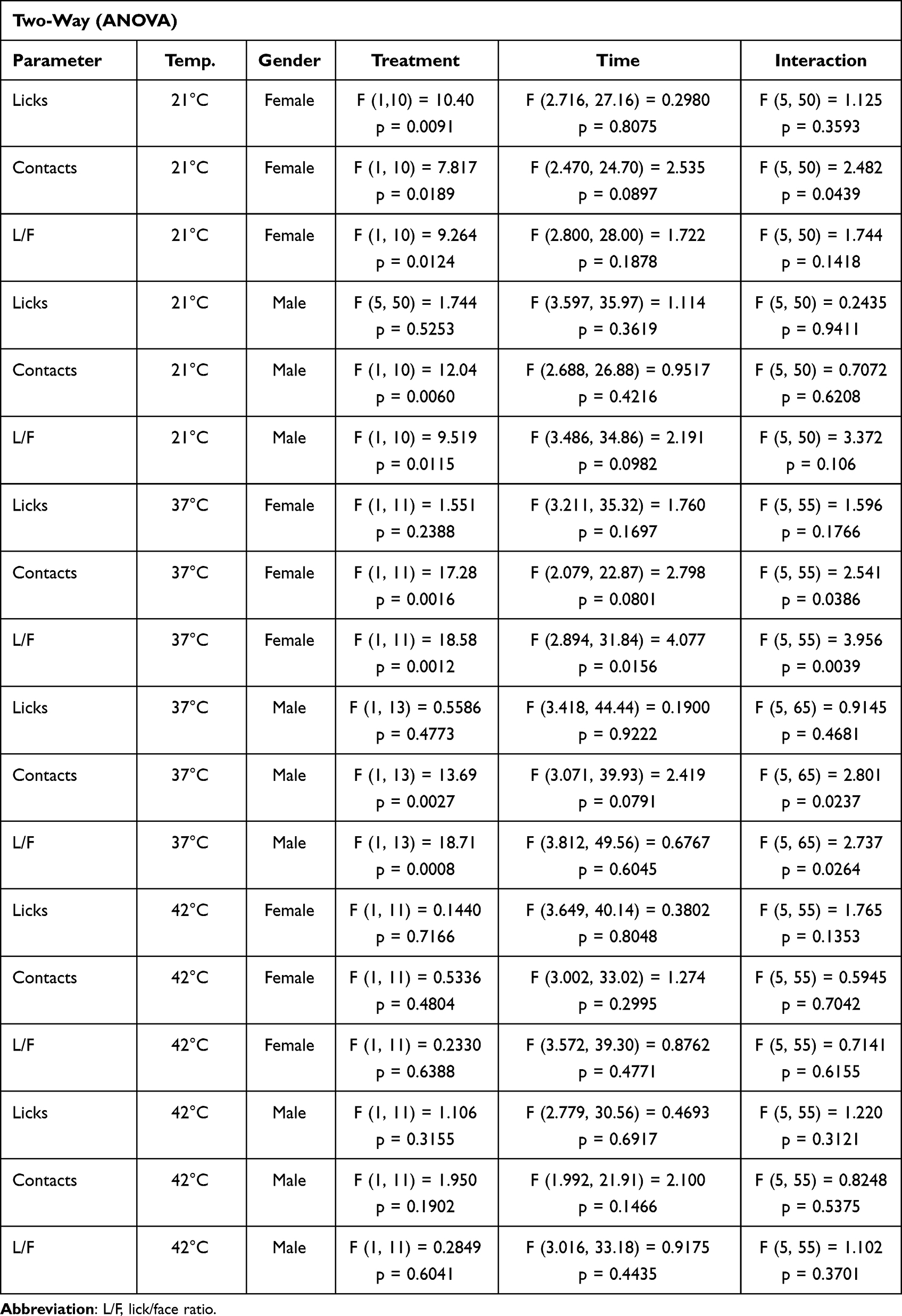 |
Table 3 Statistical Analyses of the Behavioral Parameters of Rats at 1-, 3-, 5-, 8- and 10-Days Following Carrageenan (CARR) or PBS Intra-Temporomandibular Joint Administration |
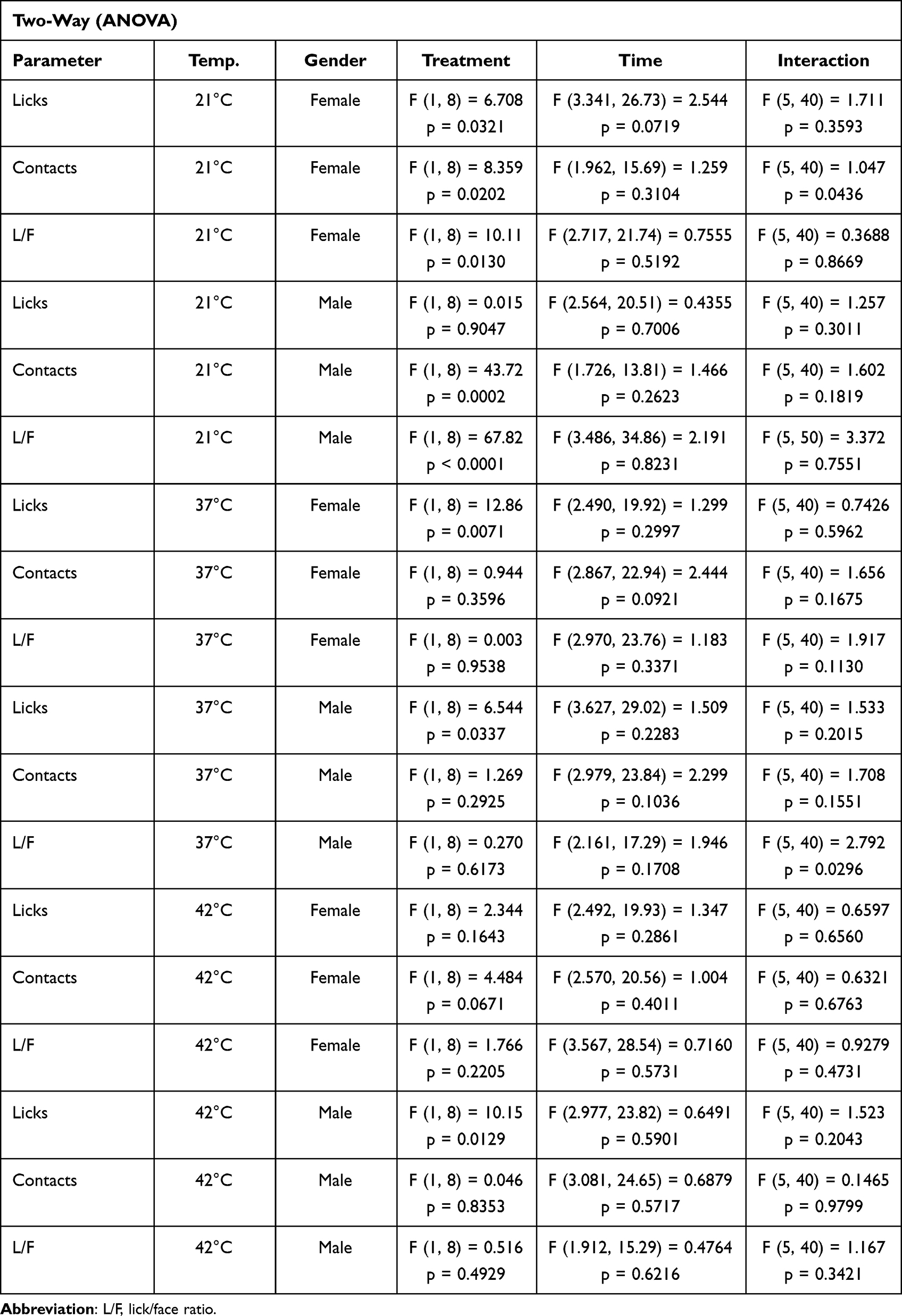 |
Table 4 Statistical Analyses of the Behavioral Parameters of Rats at 1-, 3-, 5-, 8- and 10-Days Following Carrageenan (CARR), Resiniferatoxin (RTX) + CARR or PBS Intra-Temporomandibular Joint Administration |
 |
Table 5 Statistical Analyses of the Aversive Score of Rats at 1-, 3-, 5-, 8- and 10-Days Following Carrageenan (CARR), Resiniferatoxin (RTX) + CARR Intra-Temporomandibular Joint Administration |
Discussion
The present results show that persistent inflammation in the TMJ- altered orofacial sensitivity as evaluated by the OPAD. In particular, intra_TMJ injections of CARR reduced the lick/face contact ratio (L/F) at cold (21°C) and neutral (37°C) temperatures in female and male rats. However, at the hot temperature (42°C), persistent inflammation of TMJ promoted a reduction in L/F just on Day 1 in male rats. The pre-administration of RTX prevented these effects on male and female rats, indicating that TRPV1-expressing neurons were involved in the allodynia and hyperalgesia induced by CARR.
Moreover, we evidenced that when the stimulus is at an uncomfortable temperature the rats adopt a strategy of many short stimulus contacts rather than a few sustained contacts to access the reward solution. Our group have already published similar data in a previous study in the OPAD assay.35
It is important to explain that the hyperalgesia phenomenon consists of an increased pain sensation evoked by a stimulus that usually causes pain. While allodynia is described when a non-painful stimulus induces pain. In the present results, we can suggest that TMJ inflammation promoted thermal hyperalgesia as evidenced by the reduction of the L/F ratio at 21°C and 42°C, and mechanical allodynia due to the decrease in L/F at 37°C, considering that 37°C is not a noxious stimulus. The involvement of TRPV1 in thermal hyperalgesia associated with inflammatory response has been shown in previous reports.47,48 Intrathecal injections of a TRPV1 antagonist suppressed the allodynia and hyperalgesia induced by intra-plantar injections of CARR.49 Mainly, inflammatory responses can induce enhancement of trigeminal and dorsal root ganglia neuronal excitability, resulting in increasing TRPV1 receptor expression.49,50 TRPV1 receptors are activated by noxious heat (> 42°C),17 and hyperalgesia and allodynia can result from sensitization of this receptor.51 In addition, previous reports have demonstrated that CARR, mustard oil, or CFA promoted TRPV1 sensitization.47,48 Since intra_TMJ injections of CARR mediated an increase in the number of contacts and a reduction of L/F at both cold and neutral temperatures, and these effects were prevented by RTX lesions of TRPV1-expressing neurons,17 we can hypothesize that the TRPV1-expressing neurons could be sustaining central sensitization which leads to allodynia and cold hyperalgesia. Therefore, killing off the TRPV1 neurons prevents central sensitization. Alternatively, the loss of TRPV1 primary afferent fibers prevents transmission of these sensory modalities from the face.
Similar to our results, Honda et al52 demonstrated that facial capsaicin injection significantly decreased the head-withdrawal reflex threshold to cold stimulation of the lateral facial skin, and this effect was reversed by local injection of a TRPV1 antagonist. Indeed, TRPV1 is widely expressed in nociceptive primary sensory neurons of the trigeminal ganglia.53 Previous studies showed an increased TRPV1 expression associated with the initial stages of force-induced orthodontic pain and an increased co-expression of TRPV1/CGRP in the trigeminal neurons. On the other hand, the antagonism of TRPV1 has been shown to have an analgesic effect in CARR-, CFA-, capsaicin- or acid-induced inflammatory pain.23,54–57 Our data consistently show increased mechanical allodynia in a persistent phase of CARR-induced inflammatory pain and the blocking of these effects after RTX treatment, indicating that TRPV1 is sensitized by CARR-induced inflammation.
TRPV1 receptors are found in sensory nerve fibers that innervate the face and mouth, including TMJ.20 There is growing evidence that TRPV1 receptors play a significant role in orofacial pain. Indeed, TRPV1 receptors have been found to be upregulated during TMD,8,9 and the activation of TRPV1 per se is able to induce pain. For example, TRPV1 activation induced by capsaicin injection into the masseter muscle led to acute pain in healthy human subjects evidenced by increase in the amplitude of the jaw-stretch reflex.58 While CFA-induced acute pain was reduced by blocking TRPV1 receptors in the masseter muscle in mice evaluated in the mouse grimace scale and face wiping behavior tests.59 These results, along with our results, suggest that TRPV1 contribute to development and maintenance of TMD. Consistently, Neubert et al60 found that perineural RTX injections inhibits CARR-induced inflammatory nociceptive processes in a dose- and time-dependent manner in rats.
Due to previous studies which showed that hot temperature is more aversive than cold in the OPAD35 and also that intra-plantar injections of CARR caused thermal hyperalgesia in mice,61 the lack of a statistically significant effect of CARR on nociceptive measures at 42°C was unexpected in this study. Additionally, we show that CARR-induced allodynia at 37°C lasted longer in females than males, while males showed greater peak allodynia than females, suggesting that females and males have a different form of sensitization during TMJ inflammation. In line with this finding, Tonsfeldt et al62 have demonstrated that gamma-aminobutyric acid (GABA) signaling is modulated in the ventrolateral periaqueductal gray (PAG) by persistent inflammation differently in female and male rats. The ventrolateral PAG and its descending circuit are sexually dimorphic, providing a substrate for the differential responses to pain and opioid analgesia observed in males and females.63 In addition, females and males can also differ in response to drug treatments and pain models. Notably, the report demonstrated that male mice could utilize 5-hydroxytryptamine (5-HT) and noradrenaline to decrease nociceptive responses when treated with agents that alter these neurotransmitter systems, while female mice cannot.
On the other hand, in rats without TMJ inflammation, we did not observe a difference in the aversive score (L/F) when comparing male and female rats. However, a previous report has shown that female rats are more sensitivity to cold stimulation than male rats.62
Considering that TMD involve pain upon palpation of the TMJ and/or masticatory muscles, mechanical stimuli is an important parameter in the translation of the TMD symptomatology in humans to the animal models. Here, the metal tubing of the thermode in the OPAD was positioned in a way that it was in contact with trigeminal nerve dermatomes (maxillary or mandibular) and, at least in part, masseter muscle.38,63,64 However, due to orofacial pain assessment used here, our results have thermal stimulation influence, not mechanical, as widely discussed in previous studies.38 In this way, our findings corroborated clinical studies that showed that TMD patients have a reduced pain threshold and tolerance to thermal stimuli.65–68 Despite that, further studies involving the joint mechanical sensitivity are needed to explore the advantages of using OPAD to evaluate both CARR-induced allodynia and hyperalgesia.
In conclusion, we showed that persistent inflammation of the TMJ induces allodynia and hyperalgesia effects in male and female rats using an operant orofacial pain assessment device. Moreover, prior RTX in the TMJ prevented these effects, suggesting that TRPV1-expressing neurons were involved in the allodynia and hyperalgesia during CARR-induced TMJ inflammation.
Abbreviations
5-HT, 5-hydroxytryptamine; ATP, adenosine triphosphate; CARR, carrageenan; CFA, Complete Freund’s adjuvant; GABA, gamma aminobutyric acid; L/F, lick/face ratio; OPAD, operant orofacial pain assessment device; PAG, periaqueductal gray; RTX, resiniferatoxin; TMD, temporomandibular disorder; TMJ, temporomandibular joint; TRPV1, transient receptor potential vanilloid 1.
Data Sharing Statement
The raw data supporting the development of this article can be directed to the corresponding author.
Ethics Statement
The animal study was reviewed and approved by the Association for Assessment and Accreditation of Laboratory Animal Care and with approval by the University of Florida’s Institutional Animal Care and Use Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
CRALP was granted a research fellowship from Fundação de Amparo à Pesquisa do Estado de São Paulo, Brazil (FAPESP grant number #2014/15891-0), and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq grants number #309215/2019-6, #306424/2022-3).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Schiffman E, Ohrbach R, Truelove E, et al. International RDC/TMD consortium network, international association for dental research; orofacial pain special interest group, international association for the study of pain. diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
2. Pihut M, Pac A, Gala A. Frequency of occurrence of the pain form of the temporomandibular disorders and gender distribution. Folia Med Cracov. 2021;61(2):25–33.
3. Ibi M. Inflammation and Temporomandibular Joint Derangement. Biol Pharm Bull. 2019;42(4):538–542. doi:10.1248/bpb.b18-00442
4. Jia M, Lv Y, Xu Y, Gong Z. A comparative analysis of NLRP3-related inflammatory mediators in synovial fluid in temporomandibular joint osteoarthritis and internal derangement. BMC Musculoskelet Disord. 2021;22(1):229. doi:10.1186/s12891-021-04092-0
5. Kellesarian SV, Al-Kheraif AA, Vohra F, et al. Cytokine profile in the synovial fluid of patients with temporomandibular joint disorders: a systematic review. Cytokine. 2016;77:98–106. doi:10.1016/j.cyto.2015.11.005
6. Wang GYF, Shi XQ, Wu W, Gueorguieva M, Yang M, Zhang J. Sustained and repeated mouth opening leads to development of painful temporomandibular disorders involving macrophage/microglia activation in mice. Pain. 2018;159(7):1277–1288. doi:10.1097/j.pain.0000000000001206
7. Shinoda M, Hitomi S, Iwata K, Hayashi Y. Plastic changes in nociceptive pathways contributing to persistent orofacial pain. J Oral Biosci. 2022;64(3):263–270. doi:10.1016/j.job.2022.07.001
8. Wu YW, Bi YP, Kou XX, et al. 17-Beta-estradiol enhanced allodynia of inflammatory temporomandibular joint through upregulation of hippocampal TRPV1 in ovariectomized rats. J Neurosci. 2010;30(26):8710–8719. doi:10.1523/JNEUROSCI.6323-09.2010
9. Nascimento GC, De Paula BB, Gerlach RF, Leite-Panissi CRA. Temporomandibular inflammation regulates the matrix metalloproteinases MMP-2 and MMP-9 in limbic structures. J Cell Physiol. 2021;236(9):6571–6580. doi:10.1002/jcp.30341
10. Kmeid E, Nacouzi M, Hallit S, Rohayem Z. Prevalence of temporomandibular joint disorder in the Lebanese population, and its association with depression, anxiety, and stress. Head Face Med. 2020;16(1):19. doi:10.1186/s13005-020-00234-2
11. Fillingim RB, Slade GD, Greenspan JD, et al. Long-term changes in biopsychosocial characteristics related to temporomandibular disorder: findings from the OPPERA study. Pain. 2018;159:2403–2413. doi:10.1097/j.pain.0000000000001348
12. Hornung RS, Benton WL, Tongkhuya S, Uphouse L, Kramer PR, Averitt DL. Progesterone and allopregnanolone rapidly attenuate estrogen-associated mechanical allodynia in rats with persistent temporomandibular joint inflammation. Front Integr Neurosci. 2020;14:26. doi:10.3389/fnint.2020.00026
13. Nascimento GC, Leite-Panissi CRA. Time-dependent analysis of nociception and anxiety-like behavior in rats submitted to persistent inflammation of the temporomandibular joint. Physiol Behav. 2014;125:1–7. doi:10.1016/j.physbeh.2013.11.009
14. Joseph J, Qu L, Wang S, et al. Phosphorylation of TRPV1 S801 Contributes to modality-specific hyperalgesia in mice. J Neurosci. 2019;39(50):9954–9966. doi:10.1523/JNEUROSCI.1064-19.2019
15. McKemy DD. TRPM8: the cold and menthol receptor. In: Liedtke WB, Heller S, editors. TRP Ion Channel Function in Sensory Transduction and Cellular Signaling Cascades. Boca Raton (FL): CRC PressTaylor & Francis Group, LLC; 2007.
16. Caterina MJ, Schumacher MA, Tominaga M, Rosen TA, Levine JD, Julius D. The capsaicin receptor: a heat-activated ion channel in the pain pathway. Nature. 1997;389(6653):816–824. doi:10.1038/39807
17. Neubert JK, King C, Malphurs W, et al. Characterization of mouse orofacial pain and the effects of lesioning TRPV1-expressing neurons on operant behavior. Mol Pain. 2008;4:43. doi:10.1186/1744-8069-4-43
18. Olah Z, Szabo T, Karai L, et al. Ligand-induced dynamic membrane changes and cell deletion conferred by vanilloid receptor 1. J Biol Chem. 2001;276(14):11021–11030. doi:10.1074/jbc.M008392200
19. Karai L, Brown DC, Mannes AJ, et al. Deletion of vanilloid receptor 1-expressing primary afferent neurons for pain control. J Clin Invest. 2004;113(9):1344–1352. doi:10.1172/JCI20449
20. Ioi H, Kido MA, Zhang JQ, et al. Capsaicin receptor expression in the rat temporomandibular joint. Cell Tissue Res. 2006;325(1):47–54. doi:10.1007/s00441-006-0183-7
21. Gunthorpe MJ, Chizh BA. Clinical development of TRPV1 antagonists: targeting a pivotal point in the pain pathway. Drug Discov Today. 2009;14(1–2):56–67. doi:10.1016/j.drudis.2008.11.005
22. Lima CK, Silva RM, Lacerda RB, et al. LASSBio-1135: a dual TRPV1 antagonist and anti-TNF-alpha compound orally effective in models of inflammatory and neuropathic pain. PLoS One. 2014;9(6):e99510. doi:10.1371/journal.pone.0099510
23. Cui M, Honore P, Zhong C, et al. TRPV1 receptors in the CNS play a key role in broad-spectrum analgesia of TRPV1 antagonists. J Neurosci. 2006;26(37):9385–9393. doi:10.1523/JNEUROSCI.1246-06.2006
24. Ghilardi JR, Rohrich H, Lindsay TH, et al. Selective blockade of the capsaicin receptor TRPV1 attenuates bone cancer pain. J Neurosci. 2005;25(12):3126–3131. doi:10.1523/JNEUROSCI.3815-04.2005
25. Dahlstrom L, Carlsson GE. Temporomandibular disorders and oral health-related quality of life. A systematic review. Acta Odontol Scand. 2010;68(2):80–85. doi:10.3109/00016350903431118
26. Lund LJP, Dubner R, Sessle BJ. Dor Orofacial - Da Ciencia Básica a Conduta Clínica [Orofacial Pain - From Basic Science to Clinical Practice]. Rio de Janeiro, Brasil: Quintessence; 2002.
27. Manfredini D, Chiappe G, Bosco M. Research diagnostic criteria for temporomandibular disorders (RDC/TMD) axis I diagnoses in an Italian patient population. J Oral Rehabil. 2006;33(8):551–558. doi:10.1111/j.1365-2842.2006.01600.x
28. Plesh O, Sinisi SE, Crawford PB, Gansky SA. Diagnoses based on the research diagnostic criteria for temporomandibular disorders in a biracial population of young women. J Orofac Pain. 2005;19(1):65–75.
29. Rantala MA, Ahlberg J, Suvinen TI, Savolainen A, Könönen M. Symptoms, signs, and clinical diagnoses according to the research diagnostic criteria for temporomandibular disorders among Finnish multiprofessional media personnel. J Orofac Pain. 2003;17(4):311–316.
30. Lam DK, Sessle BJ, Cairns BE, Hu JW. Neural mechanisms of temporomandibular joint and masticatory muscle pain: a possible role for peripheral glutamate receptor mechanisms. Pain Res Manag. 2005;10(3):145–152. doi:10.1155/2005/860354
31. Roveroni RC, Parada CA, Cecilia M, Veiga FA, Tambeli CH. Development of a behavioral model of TMJ pain in rats: the TMJ formalin test. Pain. 2001;94(2):185–191. doi:10.1016/S0304-3959(01)00357-8
32. Parent AJ, Beaudet N, Beaudry H, et al. Increased anxiety-like behaviors in rats experiencing chronic inflammatory pain. Behav Brain Res. 2012;229(1):160–167. doi:10.1016/j.bbr.2012.01.001
33. Neubert JK, Widmer CG, Malphurs W, Rossi HL, Vierck CJ Jr, Caudle RM. Use of a novel thermal operant behavioral assay for characterization of orofacial pain sensitivity. Pain. 2005;116(3):386–395. doi:10.1016/j.pain.2005.05.011
34. Anderson EM, Mills R, Nolan TA, et al. Use of the Operant Orofacial Pain Assessment Device (OPAD) to measure changes in nociceptive behavior. J Vis Exp. 2013;76:e50336.
35. Anderson EM, Jenkins AC, Caudle RM, Neubert JK. The effects of a co-application of menthol and capsaicin on nociceptive behaviors of the rat on the operant orofacial pain assessment device. PLoS One. 2014;9(2):e89137. doi:10.1371/journal.pone.0089137
36. Rossi HL, Vierck CJ Jr, Caudle RM, Neubert JK. Characterization of cold sensitivity and thermal preference using an operant orofacial assay. Mol Pain. 2006;2:37. doi:10.1186/1744-8069-2-37
37. Nolan TA, Hester J, Bokrand-Donatelli Y, Caudle RM, Neubert JK. Adaptation of a novel operant orofacial testing system to characterize both mechanical and thermal pain. Behav Brain Res. 2011;217(2):477–480. doi:10.1016/j.bbr.2010.10.022
38. Neubert JK, Rossi HL, Malphurs W, Vierck CJ Jr, Caudle RM. Differentiation between capsaicin-induced allodynia and hyperalgesia using a thermal operant assay. Behav Brain Res. 2006;170(2):308–315. doi:10.1016/j.bbr.2006.03.008
39. Rohrs EL, Kloefkorn HE, Lakes EH, et al. A novel operant-based behavioral assay of mechanical allodynia in the orofacial region of rats. J Neurosci Methods. 2015;248:1–6. doi:10.1016/j.jneumeth.2015.03.022
40. Nag S, Mokha SS. Activation of the trigeminal α2-adrenoceptor produces sex-specific, estrogen dependent thermal antinociception and antihyperalgesia using an operant pain assay in the rat. Behav Brain Res. 2016;314:152–158. doi:10.1016/j.bbr.2016.08.012
41. Anderson EM, Neubert JK, Caudle RM. Long-term changes in reward-seeking following morphine withdrawal are associated with altered N-methyl-D-aspartate receptor 1 splice variants in the amygdala. Neuroscience. 2012;223:45–55. doi:10.1016/j.neuroscience.2012.07.037
42. Rossi HL, Jenkins AC, Kaufman J, Bhattacharyya I, Caudle RM, Neubert JK. Characterization of bilateral trigeminal constriction injury using an operant facial pain assay. Neuroscience. 2012;224:294–306. doi:10.1016/j.neuroscience.2012.08.015
43. Riley JL, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex differences in the perception of noxious experimental stimuli: a meta-analysis. Pain. 1998;74(2–3):181–187. doi:10.1016/s0304-3959(97)00199-1
44. Berkley KJ. Sex differences in pain. Behav Brain Sci. 1997;20(3):371–380. doi:10.1017/s0140525x97221485
45. Barretto SR, de Melo GC, Dos Santos JC, et al. Evaluation of anti-nociceptive and anti-inflammatory activity of low-level laser therapy on temporomandibular joint inflammation in rodents. J Photochem Photobiol B. 2013;129:135–142. doi:10.1016/j.jphotobiol
46. Zhou Q, Imbe H, Dubner R, Ren K. Persistent Fos protein expression after orofacial deep or cutaneous tissue inflammation in rats: implications for persistent orofacial pain. J Comp Neurol. 1999;412(2):276–291. doi:10.1002/(SICI)1096-9861(19990920)412:2<276::AID-CNE7>3.0.CO;2-9
47. Caterina MJ, Leffler A, Malmberg AB, et al. Impaired nociception and pain sensation in mice lacking the capsaicin receptor. Science. 2000;288(5464):306–313. doi:10.1126/science.288.5464.306
48. Davis JB, Gray J, Gunthorpe MJ, et al. Vanilloid receptor-1 is essential for inflammatory thermal hyperalgesia. Nature. 2000;405(6783):183–187. doi:10.1038/35012076
49. Kang SY, Seo SY, Bang SK, Cho SJ, Choi KH, Ryu Y. Inhibition of spinal TRPV1 reduces NMDA receptor 2B phosphorylation and produces anti-nociceptive effects in mice with inflammatory Pain. Int J Mol Sci. 2021;22(20):11177. doi:10.3390/ijms222011177
50. Shinoda M, Asano M, Omagari D, et al. Nerve growth factor contribution via transient receptor potential vanilloid 1 to ectopic orofacial pain. J Neurosci. 2011;31(19):7145–7155. doi:10.1523/JNEUROSCI.0481-11
51. Caterina MJ, Julius D. The vanilloid receptor: a molecular gateway to the pain pathway. Annu Rev Neurosci. 2001;24:487–517. doi:10.1146/annurev.neuro.24.1.487
52. Honda K, Shinoda M, Furukawa A, Kita K, Noma N, Iwata K. TRPA1 contributes to capsaicin-induced facial cold hyperalgesia in rats. Eur J Oral Sci. 2014;122(6):391–396. doi:10.1111/eos.12157
53. Thammanichanon P, Kaewpitak A, Binlateh T, Pavasant P, Leethanakul C. Varied temporal expression patterns of trigeminal TRPA1 and TRPV1 and the neuropeptide CGRP during orthodontic force-induced pain. Arch Oral Biol. 2021;128:105170. doi:10.1016/j.archoralbio.2021.105170
54. Gavva NR, Tamir R, Qu Y, et al. AMG 9810 [(E)-3-(4-t-butylphenyl)-N-(2,3-dihydrobenzo[b][1,4] dioxin-6-yl)acrylamide], a novel vanilloid receptor 1 (TRPV1) antagonist with antihyperalgesic properties. J Pharmacol Exp Ther. 2005;313(1):474–484. doi:10.1124/jpet.104.079855
55. Horvath G, Kekesi G, Nagy E, Benedek G. The role of TRPV1 receptors in the antinociceptive effect of anandamide at spinal level. Pain. 2008;134(3):277–284. doi:10.1016/j.pain.2007.04.032
56. Watanabe M, Ueda T, Shibata Y, Kumamoto N, Ugawa S. The role of TRPV1 channels in carrageenan-induced mechanical hyperalgesia in mice. Neuroreport. 2015;26(3):173–178. doi:10.1097/WNR.0000000000000322
57. Chen WN, Lee CH, Lin SH, et al. Roles of ASIC3, TRPV1, and NaV1.8 in the transition from acute to chronic pain in a mouse model of fibromyalgia. Mol Pain. 2014;10:40. doi:10.1186/1744-8069-10-40
58. Wang K, Arendt-Nielsen L, Svensson P. Capsaicin-induced muscle pain alters the excitability of the human jaw-stretch reflex. J Dent Res. 2002;81(9):650–654. doi:10.1177/154405910208100915
59. Wang S, Brigoli B, Lim J, Karley A, Chung MK. Roles of TRPV1 and TRPA1 in spontaneous pain from inflamed masseter muscle. Neuroscience. 2018;384:290–299. doi:10.1016/j.neuroscience.2018.05.048
60. Neubert JK, Mannes AJ, Karai LJ, et al. Perineural resiniferatoxin selectively inhibits inflammatory hyperalgesia. Mol Pain. 2008;4:3. doi:10.1186/1744-8069-4-3
61. Fattori V, Pinho-Ribeiro FA, Staurengo-Ferrari L, et al. The specialised pro-resolving lipid mediator maresin 1 reduces inflammatory pain with a long-lasting analgesic effect. Br J Pharmacol. 2019;176(11):1728–1744. doi:10.1111/bph.14647
62. Tonsfeldt KJ, Suchland KL, Beeson KA, Lowe JD, Li MH, Ingram SL. Sex Differences in GABAA Signaling in the Periaqueductal Gray Induced by Persistent Inflammation. J Neurosci. 2016;36(5):1669–1681. doi:10.1523/JNEUROSCI.1928-15.2016
63. Loyd DR, Murphy AZ. The neuroanatomy of sexual dimorphism in opioid analgesia. Exp Neurol. 2014;259:57–63. doi:10.1016/j.expneurol.2014.04.004
64. Vierck CJ, Yezierski RP, Light AR. Long-lasting hyperalgesia and sympathetic dysregulation after formalin injection into the rat hind paw. Neuroscience. 2008;153(2):501–506. doi:10.1016/j.neuroscience.2008.02.027
65. Carvajal Monroy PL, Yablonka-Reuveni Z, Grefte S, Kuijpers-Jagtman AM, Wagener FA, Von den Hoff JW. Isolation and Characterization of Satellite Cells from Rat Head Branchiomeric Muscles. J Vis Exp. 2015;101:e52802. doi:10.3791/52802
66. Cox PG, Faulkes CG. Digital dissection of the masticatory muscles of the naked mole-rat, Heterocephalus glaber (Mammalia, Rodentia). PeerJ. 2014;2:e448. doi:10.7717/peerj.448
67. Park JW, Clark GT, Kim YK, Chung JW. Analysis of thermal pain sensitivity and psychological profiles in different subgroups of TMD patients. Int J Oral Maxillofac Surg. 2010;39(10):968–974. doi:10.1016/j.ijom.2010.06.003
68. Maixner W, Fillingim R, Booker D, Sigurdsson A. Sensitivity of patients with painful temporomandibular disorders to experimentally evoked pain. Pain. 1995;63(3):341–351. doi:10.1016/0304-3959(95)00068-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.